Running head: PREVENTION OF VENOUS THROMBOEMBOLISM 1 Prevention of Venous Thromboembolism After Hip or Knee Replacement Molly P. Bruce Georgetown University School of Nursing and Health Studies NURO540

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Running head: PREVENTION OF VENOUS THROMBOEMBOLISM 1
Prevention of Venous Thromboembolism After Hip or Knee Replacement
Molly P. Bruce
Georgetown University School of Nursing and Health Studies
NURO540

PREVENTION OF VENOUS THROMBOEMBOLISM 2
Prevention of Venous Thromboembolism After Hip or Knee Replacement
Total hip and knee replacements are surgical procedures that are frequently performed in
healthcare. According to the Centers for Disease Control and Prevention (2014), there are
approximately 719,000 total knee replacements and 332,000 total hip replacements performed in
the United States each year. Hip and knee replacements are performed for various reasons
including development of osteoarthritis, rheumatoid arthritis, osteonecrosis, or fractures, among
many other factors (National Institute of Arthritis and Musculoskeletal and Skin Diseases, 2010).
Patients undergoing these procedures are at an increased risk for the development of venous
thromboembolisms (VTE), which is a potentially fatal complication occurring after major
orthopedic surgeries. Therefore, it is standard practice to place patients on prophylactic
anticoagulants for a minimum of ten days, though extended use of up to five weeks has been
found to be most effective (Eriksson et al., 2008).
Two anticoagulant agents currently available for the prevention of VTE include
rivaroxaban (Xarelto) and enoxaparin (Lovenox). Rivaroxaban is the newest oral anticoagulant
agent introduced for the purpose of reducing the risk of VTE in patients with atrial fibrillation or
patients who have just had knee or hip replacement surgery. Enoxaparin is a low molecular
weight heparin (LMWH) given subcutaneously and has been the standard of care in recent years
for treating hip and knee replacement patients prophylactically (Westendorf et al., 2013). Some
studies have shown rivaroxaban to be as effective as enoxaparin in the prevention of VTE, which
could be useful for prescribing physicians to consider since rivaroxaban may be more preferred
by patients due to administration route.
The purpose of this paper is to present a summary of existing literature comparing the
effectiveness of rivaroxaban to enoxaparin in the prevention of VTE. This will be done by
completing a critical appraisal of the literature including a conceptualization the problem, review
of findings, methodological rigor, strengths and limitations, and an appraisal of the strength of
evidence from included studies in order to develop an evidence-based solution to the below
PICOT question.
PICOT Question
The PICOT question being appraised is, “In adult patients who have undergone hip or
knee replacement, is rivaroxaban more effective than enoxaparin for the prevention of VTE, over

PREVENTION OF VENOUS THROMBOEMBOLISM 3
the course of a month?” The population under investigation has undergone either hip or knee
replacement, also known as arthroplasty, and has started rivaroxaban or enoxaparin either prior
to or shortly after the completion of surgery. The age of adults included ranges from 19 to 65.
The intervention under study is the use of oral rivaroxaban and it is being compared to
subcutaneous enoxaparin. Both rivaroxaban and enoxaparin are medications used to prevent the
patient from developing a VTE, or blood clot. Other terms used to describe these medications
are blood thinners or anticoagulants. Specifically, rivaroxaban is a direct factor Xa inhibitor that
interrupts intrinsic and extrinsic pathways during the coagulation cascade, thereby blocking the
formation of blood clots (U.S. National Library of Medicine, 2014). Enoxaparin is a LWMH
that binds to antithrombin III, which inactivates factor Xa and thrombin, inhibiting clot
formation (U.S. National Library of Medicine, 2014). The outcome under study includes
prevention of VTE. Venous thromboembolism includes the development of a deep vein
thrombosis (DVT) or pulmonary embolism (PE). Key words used for VTE might include blood
clot, DVT, pulmonary embolism (PE), or thromboembolism. The timing component of the
PICOT question is over the course of one month.
Significance of the Problem
Venous thromboembolisms occur in approximately 85% of patients who have undergone
major orthopedic surgery without the use of post-pharmacological prophylaxis (Westendorf et
al., 2013). Despite evidence provided in several meta-analysis studies indicating the need for
pharmacological prophylaxis after hip and knee replacement, nearly 50% of patients do not
receive extended prophylaxis after discharge (Kakkar et al., 2008). It is important for patients to
receive prophylactic anticoagulant medications to lessen the risk of VTE development, since this
is a potentially fatal complication. Without VTE prophylaxis after hip and knee replacement,
length of stay, readmission, and mortality will be negatively impacted and financial implications
will result due to the severity of VTE.
Enoxaparin and rivaroxaban are both options that have been explored for prophylaxis in
past years. While enoxaparin has been around longer, rivaroxaban has been receiving more
attention due to its route of administration and potential to be more effective at preventing VTEs.
The required length of time to take prophylactic anticoagulants most always extends past the
patient’s discharge date, given that the minimum recommended length for prophylaxis after hip
or knee replacement is ten days. Therefore, when patients are prescribed daily subcutaneous
PREVENTION OF VENOUS THROMBOEMBOLISM 4
enoxaparin, an additional responsibility is put on the patient and family to understand the
importance of administering subcutaneous enoxaparin correctly and consistently. Though it is
important for patient’s to approach rivaroxaban in the same manner, the route of administration
is by mouth, thereby not necessitating family cooperation.
Among other considerations, a study conducted by Duran et al. (2012) found rivaroxaban
to be more cost efficient than enoxaparin. According to Duran et al. (2012), rivaroxaban has a
cost savings of $511.93 per patient when compared to enoxaparin. In addition to being cost
efficient, a study completed by Lassen et al. (2008) found that gastrointestinal side effects were
mostly experienced by patients on these medications and that similar occurrence rates were
found between enoxaparin and rivaroxaban, with the greatest being 13% in patient’s taking
enoxaparin and 12% in those taking rivaroxaban (Lassen et. al, 2008). However, side effects
such as bleeding were found to be greater in rivaroxaban. Given these statistics and the
possibility of rivaroxaban being more efficacious at preventing VTEs than enoxaparin, it is
important for physicians to highly consider rivaroxaban over enoxaparin, while also taking into
consideration risks versus benefits when prescribing prophylaxis for these patients.
Search Strategy and Results
The databases used to search for articles related to the topic included CINAHL and
PubMed. Search terms used included hip or knee arthroplasty or replacement and enoxaparin
and rivaroxaban. The terms hip or knee arthroplasty or replacement were used before adding
another Boolean operator, AND, between enoxaparin and rivaroxaban to further narrow results.
Inclusion criteria included adults, English language, humans, within ten years, aged 19-65+,
rivaroxaban and enoxaparin or LMWH had to be included, and studies had to be done on patients
who underwent hip or knee replacement. Studies were excluded if inclusion criteria were not
met.
After entering appropriate keywords, Boolean operators, and inclusion/exclusion criteria,
there were 26 results on PubMed and four results on CINAHL (Figure 1). Of these results, each
article was screened for overall appropriateness and relativeness to the topic, and a total of
eleven were utilized for this article. These articles consist of eight randomized controlled trials
(RCTs) of which four were pooled-analyses, two cohort studies, and one meta-analysis. Articles

PREVENTION OF VENOUS THROMBOEMBOLISM 5
were evaluated and graded using the Rating system for the Hierarchy of Evidence for
Intervention/Treatment Questions (Figure 2).
Critical Appraisal of the Literature
Conceptualization of the Problem
The conceptual framework of the literature that was reviewed for the PICOT question
consisted of making a determination as to whether enoxaparin or rivaroxaban is more effective at
preventing VTE in hip and knee replacement patients. For these studies, each concept was
appropriately and consistently defined by detailing the differences between enoxaparin and
rivaroxaban. The doses of medications used in the studies varied in milligrams (mg) and
frequency of administration. Enoxaparin was administered in either 40mg daily or 30mg twice a
day. Rivaroxaban doses varied from 5-60mg, with the majority of studies administering 10mg
daily. The length of administration time also varied between studies, from ten to 35 days. In
addition to differentiating rivaroxaban from enoxaparin, each study also clearly defined the
concept of VTE.
It is important to note that while concepts were consistent across the majority of studies,
two of these only examined LMWH as a group, instead of enoxaparin alone. The author of one
of these studies explained that they utilized various LMWHs because hospital recommendations
were altered during the study period based on national prophylaxis guidelines for hip or knee
replacement patients (Westendorf et al., 2013). The second study included all LMWH so that
physicians could prescribe based on their preference instead of being limited to one option
(Turpie et al., 2013).
Findings
Findings from the eleven research articles that were utilized were all consistent. There
were no conflicting findings reported on development of VTE. All studies provided statistically
significant results that reported subcutaneous enoxaparin, or LMWH in general, to be associated
with higher rates of VTE when compared to oral rivaroxaban. This stayed true at varying doses
and frequencies of administration (Appendix A).
In addition to researching VTE rates with the administration of rivaroxaban and
enoxaparin, it is relevant to mention that all of the included studies also looked at safety, and
specifically rates of bleeding, for each drug. All but one of these studies reported a minimal to
moderate increase in bleeding with rivaroxaban than with enoxaparin. Fisher et al. (2007) found

PREVENTION OF VENOUS THROMBOEMBOLISM 6
that there was a dose-dependent response for bleeding with rivaroxaban (p<0.001), by showing
that in a population of 1,317 patients, bleeding occurred in “0.9%, 1.3%, 2.1%, 3.9%, and 7.0%
of patients receiving rivaroxaban total daily doses of 5, 10, 20, 40, and 60mg, respectively,
versus 1.7% of patients receiving enoxaparin (p. 931).” Westendorf et al. (2013) was the only
study that found rivaroxaban (10mg) to have a lower risk of bleeding when compared with
LMWH, 2.9% versus 7.0% (p<0.001) for 2,538 patients.
Methodological Rigor
Both experimental and nonexperimental research designs were utilized in the appraised
studies. The experimental studies consisted of eight RCTs of which four were pooled analyses,
while the two nonexperimental studies were cohort studies. In addition, a meta-analysis was
included. Of the studies included, the majority of samples were obtained internationally. The
research samples also included all appropriate candidates undergoing hip or knee replacement
being treating prophylactically for VTE, increasing representativeness and external validity of
the population under study.
A factor found in many of the research studies that negatively affected the measurement
of study variables, was the recurring incidence of inadequate venograms obtained to assess for
the development of VTE. To resolve this issue, most of the studies were able to increase the
recruitment of patients to meet the statistical power of their trials. All but two studies were
randomized and blinded, minimizing confounding variables and increasing internal validity. The
two studies that were not randomized were cohort studies, which could have negatively impacted
the internal validity of results obtained.
Strengths and Limitations
The strengths of the overall body of evidence include similarity in study populations,
inclusion of RCTs, and the utilization of ethical guidelines. The PICOT question under appraisal
specifically targets an adult population who has undergone either hip or knee replacement
surgery. These inclusion criteria were all met in the appraised research articles, which increased
the chances of determining an appropriate answer to the PICOT question. In addition, the
majority of studies included were either RCTs or pooled analyses of multiple RCTs. These
studies were not only randomized, but also double-blinded lessening the chances of bias. The
RCTs included also had large sample sizes, with the majority meeting their calculated power
analysis, increasing generalizability. Lastly, the majority of included studies mentioned

PREVENTION OF VENOUS THROMBOEMBOLISM 7
appropriate ethical considerations including the obtainment of informed consent and approval
from ethics committees.
The limitations of the body of evidence include the utilization of multiple doses and
frequencies of administration for each drug, use of LMWH instead of enoxaparin in two studies,
the inclusion of two cohort studies, and risks of bias due to connections to sponsors. The studies
under investigation included a variety of drug dosages and frequencies in administration. As
mentioned earlier, enoxaparin dosages ranged from 40mg daily to 30mg twice a day, while
rivaroxaban dosages varied from 5-60mg, with the majority of studies administering 10mg daily.
There was also not a consistent timeframe for the length of administration, ranging from ten to
35 days. These factors combined could lead to inconsistent results that are difficult to compare
to studies with varying dosages, frequencies, and timeframes. In addition, two of the studies
examined LMWH as a group instead of enoxaparin alone, which could also alter the comparison
of findings. Another limitation of the obtained body of evidence includes the utilization of two
cohort studies. Without randomization and blinding, the risk of bias is increased. Lastly, in one
of these cohort studies, Bayer Pharmaceuticals was a sponsor, and this company manufactures
rivaroxaban (Turpie et al., 2013). Many of the involved researchers had connections with Bayer
including employment, stockholders, consultants, and some obtained grants from the company,
further increasing the risk of bias in the included study. This was the same case for the meta-
analysis conducted by Nieto, Espada, Merino, and Gonzalez (2012).
Summary Statement Regarding Strength of the Evidence
After reviewing the body of existing literature, it was found that oral rivaroxaban is
superior to subcutaneous enoxaparin for preventing VTE after total hip or knee replacement. In
order to support this statement, it is important to note that the eleven studies incorporated in this
literature review each included quality, quantity, and consistency of varying degrees. The
majority of the included studies were of high quality, minimizing biases and increasing internal
validity through randomization and blinding. However, two studies were cohort studies and
were not randomized, thereby affecting quality. In addition, the majority of included studies had
a level II rating with the Rating system for the Hierarchy of Evidence for Intervention/Treatment
Questions. Quantity was appropriately addressed in each study since all studies had large sample
sizes with strong magnitude of effects. Power analyses were conducted in the majority of studies
and most of these met their calculated analysis, with the exception of the study conducted by

PREVENTION OF VENOUS THROMBOEMBOLISM 8
Kakkar et al. (2008). Relative risk and odds ratios were utilized in the majority of the studies.
Lastly, all studies were consistent since they yielded statistically significant results showing
evidence that rivaroxaban was more efficacious at preventing VTE after total hip or knee
replacement when compared with enoxaparin.
The Rating system for the Hierarchy of Evidence for Intervention/Treatment Questions
(Figure 2) was used to rate evidence obtained from the included research studies. Of these
studies, one was rated a level one, eight were rated a level two, and two were rated as a level
four. Levels are ranked from highest evidence as level one to lowest evidence as level seven.
The average grade of all studies included combined is a level two, suggesting a fairly high level
of evidence, collectively.
Based on the review of literature and overall soundness of evidence obtained, it is
suggested that physicians consider prescribing low-dose rivaroxaban over enoxaparin for
prevention of VTE after total hip or knee replacement based on the patient and their overall risk
factors. However, it is of upmost importance that other considerations not included in the
proposed PICOT question be considered before prescribing rivaroxaban over enoxaparin due to
greater risks of bleeding while on rivaroxaban, especially with higher doses. Fisher et al. (2007)
concluded that daily doses of 5-20mg of rivaroxaban was found to be most effective at
preventing VTE and had a favorable safety balance, relative to enoxaparin. At a dose of 10mg of
rivaroxaban, Huisman et al. (2010) found that bleeding risks were 2.5% compared to 3.1% in
enoxaparin, but there was a 2-fold higher risk of developing VTE with enoxaparin compared
with rivaroxaban. Given the comparison of the nearly similar risks of bleeding to the benefit of
greater protection from VTE with low-dose rivaroxaban, it might be realistic to prescribe low-
dose rivaroxaban over enoxaparin when applicable. Regardless of the provider’s decision to
prescribe rivaroxaban over enoxaparin, patient risks versus benefits must always be taken into
consideration so that the patient can obtain the best results with the least adverse effects possible.
Clinical Recommendations
As mentioned above, it is recommended that low-dose rivaroxaban be prescribed over
enoxaparin for the prevention of venous thromboembolism after hip or knee replacement.
Venous thromboembolism development was shown to be less likely with rivaroxaban than with
enoxaparin. However, it is important to weigh patient risks versus benefits before prescribing

PREVENTION OF VENOUS THROMBOEMBOLISM 9
low-dose rivaroxaban due to higher risks of bleeding, especially with higher doses. Due to
theses risks of bleeding, certain factors should be taken into consideration before prescribing
rivaroxaban over enoxaparin. One of these considerations would be to determine whether or not
the patient has had a history of bleeding. For these patients, it might be best to prescribe
enoxaparin rather than low-dose rivaroxaban, even though the bleeding risks were shown to be
only slightly more elevated in rivaroxaban than enoxaparin. Other factors taken into
consideration should include patient preference, likeliness of compliance, and probabilities of
VTE development.
Prescription for Change
The change model used to implement the above clinical recommendations for
organizational change is the ACE Star Model of Knowledge Transformation. This model was
chosen since it includes the utilization of both old and new concepts for improving patient care.
It also is a continuous model, suggesting that knowledge transformation is a constant, endless
process (Stevens, 2004). Medications for VTE prevention are continually developed and
studied, and practice guidelines will always be evolving based on evidence-based practice, just
as the ACE Star Model suggests. This model also incorporate clinical practice guidelines that
disclose risks and benefits of different evidence-based options, which would be beneficial for the
evidence obtained in this paper. The steps applied in this model include discovering a research
question, summarizing the evidence, translating findings, integrating findings into practice, and
evaluating the overall outcomes.
Discovering Research
As mentioned previously, this topic was thoroughly researched using two databases,
PubMed and CINAHL, in order to generate knowledge on the proposed PICOT question.
Articles with various research designs including RCTs, cohort studies, and a meta-analysis were
incorporated in the search to gather evidence on the topic. This stage of discovering existing
research is necessary in order to rectify the need for change in current clinical practice (Stevens,
2004).
Summarizing the Evidence
Stevens (2004) mentions that summarizing the evidence is the first step in evidenced-
based practice, since it encompasses research findings into one meaningful statement. By

PREVENTION OF VENOUS THROMBOEMBOLISM 10
combining findings from various studies, the risk of overall findings occurring based on chance
diminishes, and reliability and reproducibility of findings is increased (Stevens, 2004). The
evidence obtained on the proposed PICOT question in this paper, suggested that VTE rates were
lessened with rivaroxaban than with enoxaparin prophylaxis. This held true for every study that
was included.
Translation of Evidence
After a summary of existing evidence is developed, it is important to translate this into a
clinical practice guideline (CPG) so that providers can easily become informed on the overall
body of evidence (Stevens, 2004). Clinical practice guidelines help assist providers in
determining the best clinical decisions for their patients by including risks, benefits, and costs.
These guidelines also clearly explain clinical recommendations and link these recommendations
to evidence obtained during research (Stevens, 2004). The CPG for the evidence obtained on the
proposed PICOT question in this review, will include the recommendation to prescribe low-dose
rivaroxaban over enoxaparin for VTE prevention. It also will include the findings of higher
bleeding rates with rivaroxaban and the importance to weigh risks versus benefits for each
patient.
Integration of Evidence into Practice
In order to integrate evidence into practice, it is important to identify key stakeholders,
barriers, and facilitators for change. Key stakeholders included in this recommendation of
implementing low-dose rivaroxaban over enoxaparin for VTE prevention in hip and knee
replacement patients, encompasses the surgeons who are completing the surgery, nurses
providing care after the procedures, and the patients and outpatient providers after discharge.
These are the main individuals who will be affected by the change, and therefore need to be
involved in the decision making process. A major barrier to change for the recommendations
made would be non-adherence to change by these providers and noncompliance by the patient.
Providers may be most comfortable with their previous standard of practice and become resistant
to change. In addition, patients may not be compliant with medication administration, and in the
case of prescribing enoxaparin, may not be adequately administering their medication as
prescribed. Lastly, the major facilitators of change would be the inpatient and outpatient

PREVENTION OF VENOUS THROMBOEMBOLISM 11
providers caring for these patients, since they have authoritative privileges for prescribing these
medications.
It is also important to have a strategy for implementing change. Lewin’s Model of
Change incorporates three steps to implement change including unfreezing, changing, and
refreezing. In the first step, the stakeholders will be recognized and pursued. A summary of the
obtained evidence will be presented to them in order to increase motivation for change. At this
time, it is important to address all questions and concerns so that the stakeholders are well
informed on the new evidence. The next step is incorporating the change itself by facilitating
and integrating the developed CPGs into practice. Lastly, the change is made permanent and
overall health outcomes, efficacy, and patient and provider satisfaction are evaluated.
Evaluating Outcomes
The last step in the ACE Star Model of Knowledge Transformation is evaluating
outcomes. To evaluate patient outcomes for VTE prevention after hip or knee replacement, both
formative and summative criteria will be included. The formative criteria to be evaluated
include medication compliance and appropriate administration by nurses and patients, number of
providers who adopt the change, and overall feasibility of recommendations made. Summative
criteria will include the occurrence of VTE with rivaroxaban as compared to enoxaparin,
bleeding rates with each drug, a cost summary, and unintended consequences. Time points for
these evaluations will take place on the day of medication course completion and subsequently
one month after this date. Venous thromboembolism development will be evaluated with
venograms. Evaluation results will be disseminated to the aforementioned key stakeholders so
that the clinical practice change can be reevaluated for effectiveness.
Conclusion
The intention of this paper was to determine a solution to the proposed PICOT question
regarding the effectiveness of rivaroxaban compared to enoxaparin for the prevention of VTE
after total hip or knee replacement surgery. This was achieved by reviewing multiple studies
completed on the topic with overall high levels of evidence. This paper included an explanation
of the PICOT question, significance of the problem, search strategy and results, critical appraisal
of the literature, conceptualization of the problem including findings, methodological rigor,
strengths and limitations, and a summary statement regarding strength of evidence from the

PREVENTION OF VENOUS THROMBOEMBOLISM 12
articles included in this review. By evaluating these criterions, it was concluded that rivaroxaban
is superior in preventing VTE after hip or knee replacement when compared with enoxaparin,
suggesting that prescribing providers should closely consider their options based on the patient
and their risk factors when interacting with this patient population.

PREVENTION OF VENOUS THROMBOEMBOLISM 13
References
Centers for Disease Control and Prevention. (2014). Inpatient surgery. Retrieved from:
www.cdc.gov/nchs/fatstates/inpatient-surgery.htm
Duran, A., Sengupta, N., Diamantopoulos, A., Forster, F., Kwong, L., & Lees, M. (2012). Cost
effectiveness of rivaroxaban versus enoxaparin for prevention of post-surgical venous
thromboembolism from a U.S. payer’s perspective. Pharmacoeconomics, 30(2), 87-101.
Eriksson, B.I., Borris, L.C., Friedman, R.J., Haas, S., Huisman, M.V., Kakkar, A.K.,… Bandel,
T.J. (2008). Rivaroxaban versus enoxaparin for thromboprophylaxis after hip
arthroplasty. New England Journal of Medicine, 358(26), 2765-2775.
Fisher, W.D., Eriksson, B.I., Bauer, K.A., Borris, L., Dahl, O.E. Gent, M.,… Haas, S. (2007).
Rivaroxaban for thromboprophylaxis after orthopaedic surgery: Pooled analysis of two
studies. Journal of Thrombosis and Haemostasis, 97, 931-937.
Huisman, M.V., Quinlan, D.J., Dahl, O.E., & Schulman, S. (2010). Enoxaparin versus dabigatran
or rivaroxaban for thromboprophylaxis after hip or knee arthroplasty: Results of separate
pooled analyses of phase III multicenter randomized trials. Circulation Cardiovascular
Quality and Outcomes, 3, 652-660.
Kakkar, A.K., Brenner, B., Dahl, O.E., Eriksson, B.I., Mouret, P., Muntz, J.,… Soglian, A.G.
(2008). Extended duration rivaroxaban versus short-term enoxaparin for the prevention of
venous thromboembolism after total hip arthroplasty: A double-blind, randomized
controlled trial. The Lancet, 372, 31-39.
Lassen, M.R., Ageno, W., Borris, L.C., Lieberman, J.R., Rosencher, N., Bandel, T.J.,
Misselwitz, F. (2008). Rivaroxaban versus enoxaparin for thromboprophylaxis after total
knee arthroplasty. New England Journal of Medicine, 358(26), 2776-2786.
Levitan, B., Yuan, Z., Turpie, A.G., Friedman, R.J., Homering, M., Berlin, J.A.,… Berkowitz,
S.D. (2014). Benefit-risk assessment of rivaroxaban versus enoxaparin for the prevention
of venous thromboembolism after total hip or knee arthroplasty. Vascular Health and
Risk Management, 10, 157-167.

PREVENTION OF VENOUS THROMBOEMBOLISM 14
Melnyk, B.M., & Fineout-Overholt, E. (2011). Evidence-based practice in nursing and
healthcare: A guide to best practice (6 ed.). Philadelphia: Lippincott Williams &
Wilkins.
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2010). What is a hip
replacement? Retrieved from:
www.niams.nih/gov/Health_Info/Hip_Replacement/hip_replacement_ff.asp
Nieto, J.A., Espada, N.G., Merino, R.G., & Gonzalez, T.C. (2012). Dabigatran, rivaroxaban and
apixaban versus enoxaparin for thromboprophylaxis after total knee or hip arthroplasty:
Pool-analysis of phase II randomized clinical trials. Thrombosis Research, 130(2012),
183-191.
Stevens, K. R. (2004). ACE Star Model of EBP: Knowledge Transformation. Academic Center
for Evidence-based Practice. The University of Texas Health Science Center at San
Antonio. Retrieved from www.acestar.uthscsa.edu
Turpie, A.G., Lassen, M.R., Davidson, B.L., Bauer, K.A., Gent, M., Kwong, L.M.,… Cushner,
F.D. (2009). Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee
arthroplasty (RECORD4): a randomised trial. The Lancet, 373, 673-680.
Turpie, A.G., Lassen, M.R., Eriksson, B.I., Gent, M., Berkowitz, S.D., Misselwitz, F.,…Kakkar,
A.K. (2011). Rivaroxaban for the prevention of venous thromboembolism after hip or
knee arthroplasty. Thrombosis and Haemostasis, 105 (3), 444-453.
Turpie, A.G., Haas, S., Kreutz, R., Mantovani, L.G., Pattanayak, C.W., Holberg, G.,… Jamal, W.
(2013). A non-interventional comparison of rivaroxaban with standard of care for
thromboprophylaxis after major orthopaedic surgery in 17,701 patients with propensity
score adjustment. Thrombosis and Haemostasis, 111, 94-102.
U.S. National Library of Medicine. (2014). Low Molecular Weight Heparins. Retrieved from:
http://livertox.nih.gov/LowMolecularWeightHeparins.htm
U.S. National Library of Medicine. (2014). Rivaroxaban. Retrieved from:
http://pubchem.ncbi.nlm.nih.gov/compound/Rivaroxaban#section=Top.
Westendorf, J.B., Lutzner, J., Donath, L., Tittl, L., Knoth, H., Radke, O.C.,… Kuhlisch, E.
(2013). Efficacy and safety of thromboprophylaxis with low-molecular-weight heparin or

PREVENTION OF VENOUS THROMBOEMBOLISM 15
rivaroxaban in hip and knee replacement surgery. Thrombosis and Haemostasis, 109,
154-163.
Appendix ASummary of Primary Sources of Evidence
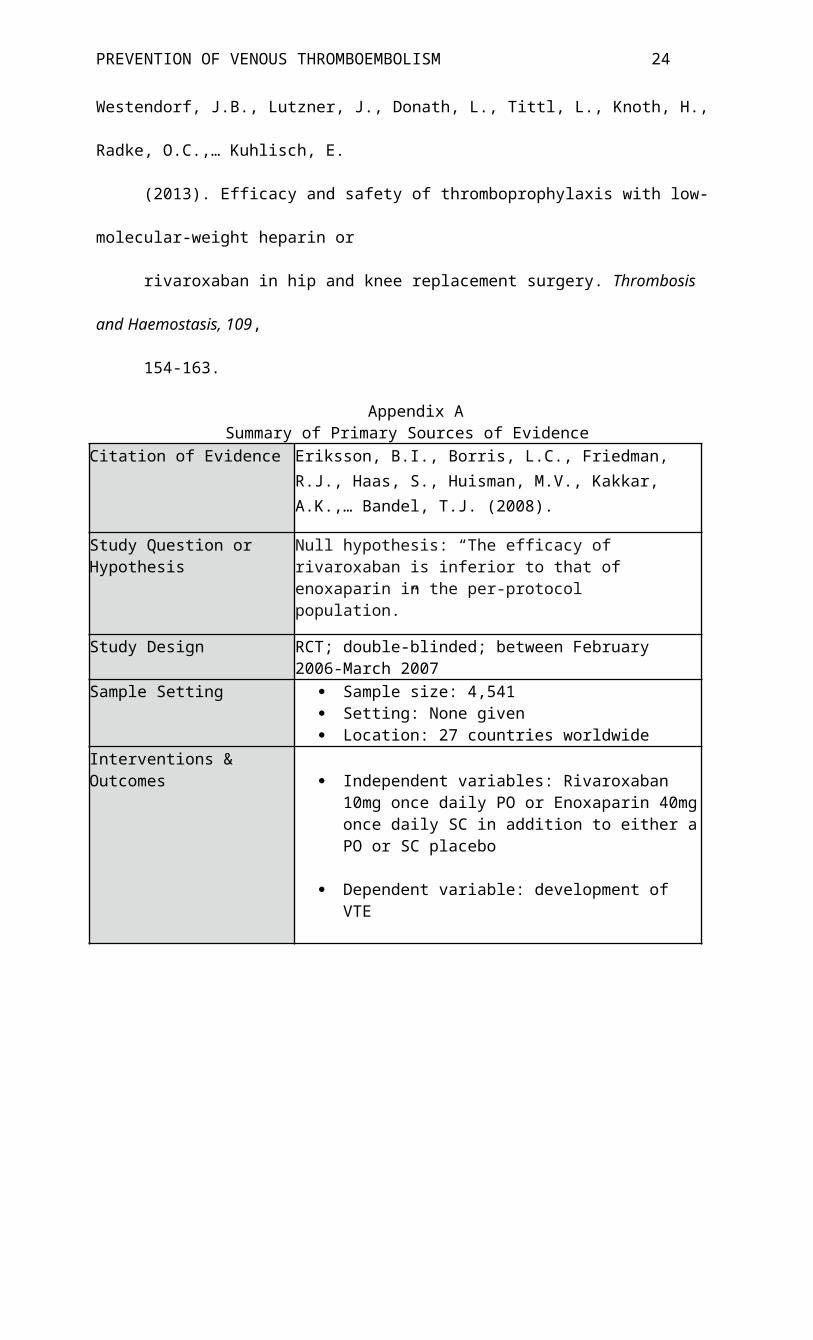
Citation of Evidence Eriksson, B.I., Borris, L.C., Friedman, R.J., Haas, S., Huisman, M.V., Kakkar, A.K.,… Bandel, T.J. (2008).
Study Question or Hypothesis Null hypothesis: “The efficacy of rivaroxaban is inferior to that of enoxaparin in the per-protocol population.”
Study Design RCT; double-blinded; between February 2006-March 2007
Sample Setting Sample size: 4,541 Setting: None given Location: 27 countries worldwide
Interventions & Outcomes Independent variables: Rivaroxaban 10mg once daily
PO or Enoxaparin 40mg once daily SC in addition to either a PO or SC placebo
Dependent variable: development of VTE
Data Collection & Analysis Data collection methods: bilateral venography done at last dose of study drug & at 36 days to screen for VTE; laboratory tests
Data analysis methods: Analysis of variance with two-sided P values, with a type I error of 5%; Mantel-Haenszel weighting with corresponding asymptotic two-sided 95% CI used to estimate difference between incidence rates in rivaroxaban group and enoxaparin group that was estimated by stratification according to country
Findings & Conclusions VTE occurred in 4/1696 (0.2%) in those taking Rivaroxaban and in 33/1678 (2.0%) in the Enoxaparin group (absolute risk reduction, 1.7%; 95% CI, 1.0 to 2.5; P<0.001) (p. 2768)
Strengths & Limitations Strengths: Trial performed under Declaration of Helsinki; protocol approved by institutional review board; informed consent obtained from patients; power analysis; adequate follow-up (only 1 patient withdrew)
Limitations: Number of valid venograms was lower than expected- more patients recruited than planned for; no information given on setting of drug administration
Implications for Practice & Research
Taking Rivaroxaban 10mg daily PO was significantly more effective than Enoxaparin 40mg SC daily for the prevention of VTE after hip arthroplasty.
Level of Evidence Level II, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)

PREVENTION OF VENOUS THROMBOEMBOLISM 16
Citation of Evidence Fisher, W.D., Eriksson, B.I., Bauer, K.A., Borris, L., Dahl, O.E. Gent, M.,… Haas, S. (2007).
Study Question or Hypothesis Is Rivaroxaban as effective as enoxaparin at preventing VTE in patients undergoing knee or hip replacement?
Study Design Pool-analysis of 2 RCTs that were both double-blinded
Sample Setting Sample size: Hip study 722; Knee study 621 Setting: Not given Location: Hip study in Europe; Knee study in North
AmericaInterventions & Outcomes Independent variables: Rivaroxaban given at 2.5, 5, 10,
20, or 30mg BID or enoxaparin 30-40mg daily; hip or knee replacement
Dependent variable: development of VTEData Collection & Analysis Data collection methods: bilateral venography 5-9 days
after surgery
Data analysis methods: Logistic regression used to analyze dose response relationship of rivaroxaban; 95% CI used to derive patient population of mean age so equal that there were equal numbers of patients in each study and equivalent numbers of male and female patients; Regression model used to rest differences in dose response relationships with rivaroxaban between hip and knee replacement groups; common odds ratio used for enoxaparin versus rivaroxaban
Findings & Conclusions VTE occurred in 16.1-24.4% of patients receiving rivaroxaban 5-60mg, and 27.8% receiving enoxaparin.
VTE with rivaroxaban occurred in 6.9-18.2% of patients in the hip study, compared to 23.3-40.4% in the knee study.
There was a flat dose response relationship with rivaroxaban for total VTE, p=0.39 (pp. 934-935)
Strengths & Limitations Strengths: Studies performed under Declaration of Helsinki and Good Clinical Practice guidelines; received consent from local ethic review committees; informed consent obtained from patients before participation; independent Data and Safety Monitoring Board monitored safety and efficacy throughout study
Limitations: Studies were not powered to detect differences between separate rivaroxaban and enoxaparin doses; specific setting of drug administration not acknowledged
Implications for Practice & Research
Rivaroxaban was found to be more effective at daily doses of 5-20mg than enoxaparin, for the prevention of VTE after a hip or knee replacement.
Level of Evidence Level II, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Citation of Evidence Huisman, M.V., Quinlan, D.J., Dahl, O.E., & Schulman, S. (2010).
Study Question or Hypothesis Are PO dabigatran and rivaroxaban as effective as enoxaparin at preventing VTE after hip or knee arthroplasty?

PREVENTION OF VENOUS THROMBOEMBOLISM 17
Study Design Pooled-analysis of 6 RCTs; double-blinded
Sample Setting Sample size: 18,405 total (10,220 in enoxaparin vs. rivaroxaban group from a total of 3 studies)
Setting: Not given Location(s): Not given
Interventions & Outcomes Independent variables: Enoxaparin SC 40mg once daily or 30mg BID; rivaroxaban 10mg PO daily (10-15 days in knee study and 28-35 days in hip study); hip or knee arthroplasty
Dependent variables: VTE developmentData Collection & Analysis Data collection methods: lower limb venography
Data analysis methods: Odds ratios for individual outcomes were done for each study and pooled using Mantel-Haenszel method; 95% CI; statistical calculations done with Review Manager
Findings & Conclusions When compared to rivaroxaban, enoxaparin showed a 2-fold higher risk of VTE development (1.2% versus 0.6%; OR, 2.04; 95% CI, 1.32 to 3.17; P<0.001; number needed to treat, 167)
When compared to dabigatran (220mg daily), enoxaparin had similar risks of VTE development (0.9% versus 1.1%; OR, 0.76; 95% confidence interval [CI], 0.44 to 1.31) (pp. 654-655)
Strengths & Limitations Strengths: All studies were approved by local research ethics boards; all provided informed consent; follow-up >99% in all 3 trials for enoxaparin vs. rivaroxaban group
Limitations: Study-level data used instead of patient-level data; patients were excluded if they had impaired renal function or were very old, which could decrease generalizability
Implications for Practice & Research
Enoxaparin and dabigatran had similar efficacy rates. However, when compared to rivaroxaban, enoxaparin had a significant increase in risk of VTE development. Implications were made to balance risks of bleeding with risks of VTE events when choosing prophylactic therapy after orthopedic surgery.
Level of Evidence Level II, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Citation of Evidence Kakkar, A.K., Brenner, B., Dahl, O.E., Eriksson, B.I., Mouret, P., Muntz, J.,… Soglian, A.G. (2008).
Study Question or Hypothesis Is 5 weeks of PO Ribaroxaban more effective than 2 weeks of SC Enoxaparin for preventing the development of VTE after hip arthroplasty?
Study Design RCT; double-blinded; from February 2006 to April 2007
Sample Setting Sample size: 2,509 Setting: Not given Location(s): 123 centers across 21 countries

PREVENTION OF VENOUS THROMBOEMBOLISM 18
Interventions & Outcomes Independent variables: Ribaroxaban PO daily for 31-39 days (with placebo injection for 10-14) or enoxaparin SC for 10-14 days (with placebo pill for 31-39 days)
Dependent variables: development of VTE
Data Collection & Analysis Data collection methods: Bilateral venography done to detect VTE day after last dose of medication
Data analysis methods: Used SAS version 8.2; Mantel-Haenszel weighting with corresponding asymptotic two-sided 95% CI and two-sided p value; Fisher’s exact test
Findings & Conclusions VTE occurred in 17/864 (2.0%) patients receiving rivaroxaban and in 81/869 (9.3%) in the enoxaparin group (absolute risk reduction 7.3%, 95% CI 5.2-9.4; p<0.0001) (p. 34)
Strengths & Limitations Strengths: Trial performed under Declaration of Helsinki; protocol approved by institutional review board; informed consent obtained from patients
Limitations: Adequate sample size was estimated to be 2500 patients. Of the 2,509 sampled, 776 were excluded for various reasons as shown in the article on Table 1 (no intake of study medication, indeterminate venography, no planned surgery, incorrect time interval between end of surgery and first dose of medication, etc.). In addition, 348 patients in the rivaroxaban group and 338 in the enoxaparin group did not have a venography done. However, sensitivity analyses were done.
Implications for Practice & Research
Extended use of rivaroxaban was significantly more effective than short-term use of enoxaparin in the prevention of VTE after hip arthroplasty.
Level of Evidence Level II, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Citation of Evidence Lassen, M.R., Ageno, W., Borris, L.C., Lieberman, J.R., Rosencher, N., Bandel, T.J., Misselwitz, F. (2008).
Study Question or Hypothesis Is oral rivaroxaban as efficient as subcutaneous enoxaparin for preventing VTE after total knee arthroplasty?
Study Design RCT; double-blinded; from February 2006 to November 2006
Sample Setting Sample size: 2,531 Setting: 147 centers Location: 19 countries
Interventions & Outcomes Independent variables: PO rivaroxaban 10mg daily after knee arthroplasty or SC enoxaparin 40mg daily after knee arthroplasty both for 10-14 days
Dependent variable: development of DVT

PREVENTION OF VENOUS THROMBOEMBOLISM 19
Data Collection & Analysis Data collection methods: bilateral venography between day 11-15
Data analysis methods: Mantel-Haenszel weighting used to estimate difference between incidences in rivaroxaban group and enoxaparin group; 95% CI; statistical power of 90% used with a two-sided type I error rate of 5%
Findings & Conclusions VTE occurred in 79/824 patients (9.6%) receiving rivaroxaban and in 166/878 patients (18.9%) receiving enoxaparin (absolute risk reduction, 9.2%; 95% confidence interval [CI], 5.9 to 12.4; P<0.001)
Major VTE events occurred in 9/908 patients (1.0%) in rivaroxaban group and 24/925 (2.6%) in enoxaparin group (weighted absolute risk reduction, 1.6%; 95% CI, 0.4 to 2.8; P = 0.01; relative risk reduction, 62%; 95% CI, 18 to 82; P=0.02) (p. 2779)
Strengths & Limitations Strengths: Trial performed under Declaration of Helsinki; protocol approved by institutional review board; informed consent obtained from patients; power analysis
Limitations: There were a low number of valid venograms obtained. Therefore, recruitment was increased from 2300 to 2500+ patients to meet statistical power of the trial. Comparison groups were well-balanced increasing generalizability, other than females>males in rivaroxaban group (P=0.03).
Implications for Practice & Research
Rivroxaban given in a fixed daily dose is superior to enoxaparin in preventing VTE in postop knee arthroplasty patients.
Level of Evidence Level II, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Citation of Evidence Levitan, B., Yuan, Z., Turpie, A.G., Friedman, R.J., Homering, M., Berlin, J.A.,… Berkowitz, S.D. (2014).
Study Question or Hypothesis What is the benefit-risk profile for rivaroxaban versus enoxaparin in patients who had total hip or knee arthroplasty?
Study Design Pooled-analysis of RCTs; from February 7,2006 to January 31, 2008
Sample Setting Sample size: 12,729 Setting: Not given Location(s): Not given
Interventions & Outcomes Independent variables: Rivaroxaban 10mg PO or 40mg SC enoxaparin
Dependent variables: development of VTE
Data Collection & Analysis Data collection methods: chart review
Data analysis methods: Post-hoc analysis; Kaplan-Meier rates
PREVENTION OF VENOUS THROMBOEMBOLISM 20
Findings & Conclusions Out of 10,000 patients, compared to enoxaparin, rivaroxaban was expected to be associated with 38 fewer symptomatic VTE events (95% CI: -6 to 82)
In 10,000 patients, compared with enoxaparin, rivaroxaban was associated with 98 (95% CI: 27 to 169) fewer symptomatic VTE.
The median time to onset for symptomatic VTE was 18 days for hip arthroplasty and 5 days for knee arthroplasty.
After both hip or knee arthroplasty, rivaroxaban prevented more harmful events than enoxaparin. (pp. 161-162)
Strengths & Limitations Strengths: Randomization in studies; groups under study were well-balanced with similar surgical and demographic characteristics
Limitations: Different durations of anticoagulant use were used in the four studies which could obscure results; 95% CI overlaps in the study for the hip and knee rate differences
Implications for Practice & Research
Rivaroxaban administration resulted in greater benefits than harm when compared with enoxaparin after total hip or knee arthroplasty.
Level of Evidence Level II, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Citation of Evidence Turpie, A.G., Lassen, M.R., Davidson, B.L., Bauer, K.A., Gent, M., Kwong, L.M.,… Cushner, F.D. (2009).
Study Question or Hypothesis Is rivaroxaban as effective as enoxaparin for thromboprophylaxis after total knee arthroplasty?
Study Design RCT; double-blinded; from June 2006 to October 2007
Sample Setting Sample size: 3,148 Setting: 131 centers; patient’s home after discharge Location(s): 12 countries
Interventions & Outcomes Independent variables: Rivaroxaban 10mg once daily with SC placebo or SC enoxaparin 30mg BID with PO placebo
Dependent variables: Development of VTE
Data Collection & Analysis Data collection methods: bilateral venography between days 11 and 15
Data analysis methods: Mantel-Haenszel weighting used to analyze the difference in the primary efficacy outcome between rivaroxaban and enoxaparin with corresponding asymptotic two-sided 95% CI; age, weight, and BMI were analyzed with two-way ANOVA, with georgraphical region and treatment group as fixed effects; statistical tests were done with a two-sided type I error rate of 5%

PREVENTION OF VENOUS THROMBOEMBOLISM 21
Findings & Conclusions In the modified intention-to-treat population, VTE occurred in 67/965 (6.9%) of patients who received rivaroxaban and in 97/959 (10.1%) of patients who received enoxaparin (absolute risk reduction 3·19%, 95% CI 0·71–5·67; p=0·0118)
In per-protocol population, VTE occurred in 58/864 (6.7%) patients receiving rivaroxaban and 82/878 (9.3%) patients receiving enoxaparin (weighted absolute risk reduction 2·71%, 95% CI 0·17–5·25), indicating superiority of rivaroxaban over enoxaparin (p=0.0362) (p. 1676)
Strengths & Limitations Strengths: Study done in accordance with Declaration of Helsinki & local regulations; independent ethics committees or institutional review boards approved the protocol for each center; informed consent obtained from patients before randomization; randomized; adequate power analysis
Limitations: Inadequate venograms to assess for VTEs was higher than expected in study
Implications for Practice & Research
Rivaroxaban PO 10mg was significantly superior to SC enoxaparin 30mg BID for preventing VTE after total knee arthroplasty.
Level of Evidence Level II, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Citation of Evidence Turpie, A.G., Lassen, M.R., Eriksson, B.I., Gent, M., Berkowitz, S.D., Misselwitz, F.,…Kakkar, A.K. (2011).
Study Question or Hypothesis Is enoxaparin more effective than rivaroxaban for thromboprophylaxis after hip or knee replacement surgery?
Study Design Pooled-analysis of four phase III RCT studies; between February 7, 2006 and Jaunary 31, 2008
Sample Setting Sample size: 12,729 Setting: 617 centers Location: 41 countries
Interventions & Outcomes Independent variables: enoxaparin 40mg SC daily or enoxaparin 30mg SC BID daily or rivaroxaban 10mg PO daily
Dependent variables: development of VTE
Data Collection & Analysis Data collection methods: chart review
Data analysis methods: 95% CI; Odds Ratio; Cox regression model
Findings & Conclusions 0.5% of patients (26/6183) developed of VTE as compared to 1.0% (60/6200) of patients who received enoxaparin (odds ratio 0.48 [95% CI 0.30–0.76]; p=0.001) (p. 447)

PREVENTION OF VENOUS THROMBOEMBOLISM 22
Strengths & Limitations Strengths: Randomization; Studies done under International Conference on Harmonization and Good Clinical Practice, Declaration of Helsinki, and local regulations; institutional review boards and ethics committees approved studies; written informed consent obtained before randomization
Limitations: Different intensities of prophylaxis usedImplications for Practice & Research
Rivaroxaban is more effective than LMWH for VTE prevention in patients who have undergone hip or knee replacement.
Level of Evidence Level II, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Citation of Evidence Turpie, A.G., Haas, S., Kreutz, R., Mantovani, L.G., Pattanayak, C.W., Holberg, G.,… Jamal, W. (2013).
Study Question or Hypothesis Is rivaroxaban as effective as standard-of-care for thromboprophylaxis after hip or knee replacement surgery?
Study Design Non-experimental, cohort study; from February 2009 to June 2011
Sample Setting Sample size: 17,701 Setting: 252 centers Location(s): 37 countries
Interventions & Outcomes Independent variables: Rivaroxaban or LMWH or unfractionated heparin, dabigatran, or vitamin K antagonists; hip or knee replacement surgery
Dependent variables: VTE development
Data Collection & Analysis Data collection methods: chart review
Data analysis methods: Logistic regression model used to estimate propensity score for each patient; Estimated odds ratios and CIs were calculated with a Bayesian method
Findings & Conclusions Symptomatic VTE 3 months after surgery occurred in 0.89% in the rivaroxaban group (n=8,778) and 1.35% in the standard-of-care group (n=8,635; odds ratio [OR] 0.65; 95% confidence interval [CI] 0.49–0.87), and 0.91% and 1.31% (weighted) in the propensity score-adjusted analysis (OR 0.69; 95% CI 0.56–0.85).
In comparison to the standard-of-care group, patients who receiving rivaroxaban had a significantly lower rate of VTE, 0.65% versus 1.02% (OR 0.63; 95% CI 0.45-0.89) in the safety population and 0.65% and 1.03% in the adjusted safety population (PR 0.63; 95% CI 0.49-0.81). (pp. 98-99)

PREVENTION OF VENOUS THROMBOEMBOLISM 23
Strengths & Limitations Strengths: Written informed consent obtained in countries where necessary; study approved by European Medicines Agency and independent ethics committee or an independent review board where required; sample size
Limitations: No randomization; Bayer Pharmaceuticals sponsored the study and they manufacture rivaroxaban. Many of the researchers in the study have connections with Bayer (employees, stock holders, receive grants, consultants, etc.) which creates a conflict of interest; confounding variables not measured with propensity score design; reporting bias
Implications for Practice & Research
In unselected patients who are undergoing knee or hip surgery, oral rivaroxaban should be considered by physicians to help improve prevention of VTE.
Level of Evidence Level IV, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Citation of Evidence Westendorf, J.B., Lutzner, J., Donath, L., Tittl, L., Knoth, H., Radke, O.C.,… Kuhlisch, E. (2013).
Study Question or Hypothesis Is LMWH or rivaroxaban more efficient for thromboprophylaxis in hip and knee replacement surgery?
Study Design Non-experimental retrospective cohort study; from January 2006 to June 2011
Sample Setting Sample size: 5,061 Setting: University Clinic “Carl Gustav Carus” Location: Dresden, Germany
Interventions & Outcomes Independent variables: LMWH (fondaparinux 2.5mg) SC daily or rivaroxaban 10mg PO daily for 35 days postop
Dependent variables: development of VTE
Data Collection & Analysis Data collection methods: chart review
Data analysis methods: Fisher’s exact test or Student’s t-test and ANCOVA were used to compare differences in baseline variables; Binary data analyzed using logistic regression models; 95% CI; Length of hospital stay analyzed using Kaplan-Meier estimation; Risk for VTE modeled with Cox proportional hazard models
Findings & Conclusions Symptomatic VTE results occurred in 4.1% of patients taking LMWH and 2.1% taking rivaroxaban (p<0.001).
Patients receiving LMWH had a higher rate of distal DVT than those receiving rivaroxaban (2.5 vs. 1.1%; p=0.011). However, a reduction of VTE with rivaroxaban only found to be significant in hip surgery patients, while reduction of VTE in knee surgery patients failed to reach significance. (pp. 157-158)
PREVENTION OF VENOUS THROMBOEMBOLISM 24
Strengths & Limitations Strengths: Sampling size comparable to large RCT studies
Limitations: No randomization; Study completed at one center, decreasing generalizability; patients who were taking rivaroxaban had more risk factors for DVT (older, higher BMI, some with history of VTE) when compared to LMWH group; different LMWH were administered during observational period due to changing protocols; no information was available on development of VTE once patients were discharged; reporting bias
Implications for Practice & Research
Rivaroxaban is more effective than LMWH for VTE prevention in patients who have undergone hip or knee replacement. Switching from LMWH to rivaroxaban could be beneficial.
Level of Evidence Level IV, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Appendix B
Summary of Secondary Sources of EvidenceCitation of Evidence Nieto, J.A., Espada, N.G., Merino, R.G., & Gonzalez, T.C.
(2012).
Objective, Aim or Purpose “To compare the main efficacy and safety endpoints of the pivotal randomised clinical trials (RCTs) on venous thromboembolism (VTE) prevention after total hip (THR) or knee (TKR) replacement with the new oral anticoagulants (NAs) versus enoxaparin.” (p. 183)
Search Strategy No specific search terms given. Only states that RCTs were obtained from medical literature.

PREVENTION OF VENOUS THROMBOEMBOLISM 25
Inclusion & Exclusion Criteria Inclusion: English; patients aged 18 years-old or older; enoxaparin SC 40mg daily or 30mg BID, rivaroxaban PO 10mg daily, apixaban PO 2.5mg BID, or dabigatran PO 220mg daily; hip or knee replacement surgery
Exclusion: active bleeding, high bleeding risk, contraindications for enoxaparin, kidney failure, abnormal liver enzymes, specific medications, pregnancy or breastfeeding, planned intermittent pneumatic compression, need for continued anticoagulation, disorders preventing bilateral venography
Data Extraction & Analysis Data collection methods: review of previous studies, chart review
Data analysis methods: Chi-square test and I2 statistic was used for heterogeneity of data; random-effects model used to obtain risk-ratios and their correspondent 95% CI; funnel plot used to assess publication bias
Results, Recommendations & Implications
When comparing VTE rates to enoxaparin 40mg, rivaroxaban showed superiority (RR 0.50; 95% CI 0.34-0.73), followed by apixaban (RR 0.63; 95% CI 0.36-1.01) and dabigatran, which showed equivalence to enoxaparin (RR 1.02; 95% CI 0.86-1.20).
VTE occurred in 927/10,245 (9.1%) of patients treated with new anticoagulants (rivaroxaban, apixaban, dabigatran) and 1,223/10,276 (11.9%) treated with enoxaparin, favoring new anticoagulants (RR 0.71; 95% CI 0.56-0.90).
In patients receiving anticoagulation after hip arthroplasty, the benefit of new anticoagulants (28-39 days) was significant (RR 0.55; 95% CI 0.32-0.95). In patients who underwent knee arthroplasty (new anticoagulants for 6-14 days), the risk ratio was only slightly reduced (RR 0.80; 95% CI 0.61-1.06).
Significant heterogeneity was analyzed among trials and subgroups (Chi square test, p<0.001). (pp. 186-189)
Recommendations for Practice: Rivaroxaban, apixaban, and dabigatran showed more efficacies when compared to enoxaparin after total hip and knee replacement.
Strengths & Limitations Strengths: 10 phase III RCTs included in meta-analysis
Limitations: Mandatory bilateral venographies 24 hours after last anticoagulant dose were required, however relevant proportion of patients had venographs that were no evaluable or either did not undergo venography (26% to 35% in rivaroxaban group); 2 of the researchers in the study received fees from Bayer, the manufacturer of rivaroxaban. 1 research was an investigator in trials sponsored by Bayer creating conflicts of interest.
Level of Evidence Level I, Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions (Melnyk & Fineout-Overholt, 2011)
Legend

PREVENTION OF VENOUS THROMBOEMBOLISM 26
ABBREVIATION DEFINITION
BID Two times daily
BMI Body Mass Index
CI Confidence Interval
DVT Deep Vein Thrombosis
LMWH Low Molecular Weight Heparin
OR Odds Ratio
PO Oral
RCT Randomized Controlled Trial
RR Relative Risk
SAS Statistical Analysis System
SC Subcutaneously
VTE Venous thromboembolism
Appendix C
Figure 2. Levels of Evidence
Rating system for the Hierarchy of Evidence for Intervention/Treatment QuestionsLevel I Evidence from a systematic review or meta
analysis of all relevant RCTs.Level II Evidence obtained from well-designed
RCTs.Level III Evidence obtained from well-designed
controlled trials without randomization.Level IV Evidence from well-designed case control
and cohort studies.Level V Evidence from systematic reviews of
descriptive and qualitative studiesLevel VI Evidence from single descriptive or
qualitative studies.

PREVENTION OF VENOUS THROMBOEMBOLISM 27
Level VII Evidence from the opinion of authorities and/or reports of expert committees.
From Melnyk, B.M., & Fineout-Overholt, E. (2011). Evidence-based practice in nursing and
healthcare: A guide to best practice (6 ed.). Philadelphia: Lippincott Williams &
Wilkins.
Appendix D
Figure 1. Search Strategy
Inclusion: within
10 years, human,
English, ages 19-65
"Arthroplasty, Replacement, Knee+" OR "Arthoplasty,
Replacement, Hip+"
Cinahl: 2324 PublicationsPubMed: 12892 Publications
3 Duplicates; 27 Publications Remain
11 studies included
16 articles excluded: 8 did not include both
enoxaparin and rivaroxaban5 not related to VTE
prevention1 looked at
thromboprophylaxis on wound healing
1 did not include pharmacological
prophylaxis1 on cost effectiveness
...AND "Rivaroxaban" AND "Enoxaparin"
Cinahl: 4 PublicationsPubMed: 26 Publications

Running head: PREVENTION OF VENOUS THROMBOEMBOLISMS 28