Bronchoalveolar Lavage Fluid Proteome in Bronchiolitis Obliterans Syndrome: Possible Role for Surfactant Protein A in Disease Onset Federica Meloni, MD, a Roberta Salvini, ScD, b Anna Maria Bardoni, ScD, b Ileana Passadore, ScD, a Nadia Solari, ScD, a Patrizio Vitulo, MD, c Tiberio Oggionni, MD, a Mario Viganò, MD, d Ernesto Pozzi, MD, a and Anna Maria Fietta, ScD a Background: Bronchiolitis obliterans syndrome (BOS) affects long-term survival of lung transplant (Tx) recipients (LTRs), with no consistently effective treatment strategy. Identifying early markers of BOS is of paramount importance for improving graft survival. Methods: We used 2-dimensional gel electrophoresis and protein identification by mass spectrometry to compare the protein profile of bronchoalveolar lavage fluid (BALf) in two groups of LTRs: one composed of patients with BOS and the other composed of patients with good graft function at 5 years post-surgery (stable LTRs). Based on the hypothesis that only proteins of lung origin could represent reliable BOS markers, we also evaluated paired plasma samples. Proteins of interest were also assessed in the BALf of control subjects and results confirmed by dot- blot analysis. Results: Among 11 differentially expressed proteins, we identified 2 locally produced factors: peroxiredoxin II (PRXII), exclusively expressed in BOS; and surfactant protein A (SP-A), expressed consistently less in BOS patients than in stable LTRs. PRXII expression was never observed in BALf from control subjects, whereas SP-A was present in higher amounts compared with stable LTRs and BOS patients. Finally, the time course of SP-A was studied in 5 LTRs who subsequently developed BOS. A reduction in BALf SP-A content was detectable early after Tx, preceding BOS onset in 4 of 5 patients. Conclusions: Our results suggest that testing SP-A levels in BALf could predict LTR patients who are at higher risk of BOS development. J Heart Lung Transplant 2007;26:1135– 43. Copyright © 2007 by the International Society for Heart and Lung Transplantation. Bronchiolitis obliterans syndrome (BOS) is predominant cause of poor long-term survival after lung transplanta- tion (Tx). 1–3 BOS affects at least 50% of lung transplant recipients (LTRs) who survive for 5 years, and therapy is often unsuccessful once functional impairment has set in. Histologically, BOS is characterized by a fibro- proliferative process occurring within the bronchiolar wall that ultimately leads to allograft failure. 4 The exact pathogenesis of BOS and early markers of the disease are still unknown. Several alloantigen-de- pendent and -independent factors, including number and severity of acute rejection (AR) episodes, HLA mismatches, development of specific alloantibodies, isch- emia–reperfusion injury, occurrence of viral respiratory infections and gastroesophageal reflux, are thought to be involved in BOS development. 5 A few recent studies analyzed BALf to identify early markers of disease or to provide new evidence regarding its pathogenesis. Two approaches can be performed at present: one that targets specific compounds on the basis of previous in vitro or animal studies, and another that systematically examines the whole BALf protein content in different groups of patients. Using the former approach, our group and others have demonstrated that several pro- inflammatory chemokines and cytokines, metallopro- teases and neutrophil products may be linked to BOS pathogenesis. 6 –13 The latter approach has been at- tempted so far only by Nelsestuen and colleagues, who performed a retrospective global proteomic analysis of BALf extracts from LTRs by means of matrix-assisted laser desorption/ionization–time-of-flight mass spec- trometry (MALDI-TOF MS) profiles, demonstrating that From the a Department of Haematological, Pneumological and Cardiovascular Sciences, Section of Pneumology, and b Department of Biochemistry, University of Pavia, Pavia, Italy; c Pneumology Unit, ISMETT-UPMC, Palermo, Italy; and d Department of Cardiac Surgery, University of Pavia and IRCCS San Matteo Foundation, Pavia, Italy. Submitted May 18, 2007; revised July 18, 2007; accepted August 20, 2007. Supported by a grant from Fondazione Cariplo (Rif. 2003.1644/ 10.8485), Italy. Reprint requests: Federica Meloni, MD, Department of Haemato- logical, Pneumological and Cardiovascular Sciences, Section of Pneu- mology, Policlinico San Matteo, Padiglione Forlanini, Via Taramelli 5, 27100 Pavia, Italy. Telephone: 39-0382-501008. Fax: 39-0382- 422704. E-mail: [email protected] Copyright © 2007 by the International Society for Heart and Lung Transplantation. 1053-2498/07/$–see front matter. doi:10.1016/ j.healun.2007.08.009 1135

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

BODFNa
B
M
R
C
Bctrispw
FCoIU
2
1
lm24CTj
ronchoalveolar Lavage Fluid Proteome in Bronchiolitisbliterans Syndrome: Possible Role for Surfactant Protein A inisease Onset
ederica Meloni, MD,a Roberta Salvini, ScD,b Anna Maria Bardoni, ScD,b Ileana Passadore, ScD,a
adia Solari, ScD,a Patrizio Vitulo, MD,c Tiberio Oggionni, MD,a Mario Viganò, MD,d Ernesto Pozzi, MD,a
nd Anna Maria Fietta, ScDa
ackground: Bronchiolitis obliterans syndrome (BOS) affects long-term survival of lung transplant (Tx) recipients(LTRs), with no consistently effective treatment strategy. Identifying early markers of BOS is ofparamount importance for improving graft survival.
ethods: We used 2-dimensional gel electrophoresis and protein identification by mass spectrometry tocompare the protein profile of bronchoalveolar lavage fluid (BALf) in two groups of LTRs: onecomposed of patients with BOS and the other composed of patients with good graft function at �5years post-surgery (stable LTRs). Based on the hypothesis that only proteins of lung origin couldrepresent reliable BOS markers, we also evaluated paired plasma samples. Proteins of interest werealso assessed in the BALf of control subjects and results confirmed by dot- blot analysis.
esults: Among 11 differentially expressed proteins, we identified 2 locally produced factors: peroxiredoxinII (PRXII), exclusively expressed in BOS; and surfactant protein A (SP-A), expressed consistently lessin BOS patients than in stable LTRs. PRXII expression was never observed in BALf from controlsubjects, whereas SP-A was present in higher amounts compared with stable LTRs and BOS patients.Finally, the time course of SP-A was studied in 5 LTRs who subsequently developed BOS. A reductionin BALf SP-A content was detectable early after Tx, preceding BOS onset in 4 of 5 patients.
onclusions: Our results suggest that testing SP-A levels in BALf could predict LTR patients who are at higher riskof BOS development. J Heart Lung Transplant 2007;26:1135–43. Copyright © 2007 by theInternational Society for Heart and Lung Transplantation.
tpameibapatveggitptpBl
ronchiolitis obliterans syndrome (BOS) is predominantause of poor long-term survival after lung transplanta-ion (Tx).1–3 BOS affects at least 50% of lung transplantecipients (LTRs) who survive for �5 years, and therapys often unsuccessful once functional impairment haset in. Histologically, BOS is characterized by a fibro-roliferative process occurring within the bronchiolarall that ultimately leads to allograft failure.4
rom the aDepartment of Haematological, Pneumological andardiovascular Sciences, Section of Pneumology, and bDepartmentf Biochemistry, University of Pavia, Pavia, Italy; cPneumology Unit,SMETT-UPMC, Palermo, Italy; and dDepartment of Cardiac Surgery,niversity of Pavia and IRCCS San Matteo Foundation, Pavia, Italy.Submitted May 18, 2007; revised July 18, 2007; accepted August 20,
007.Supported by a grant from Fondazione Cariplo (Rif. 2003.1644/
0.8485), Italy.Reprint requests: Federica Meloni, MD, Department of Haemato-
ogical, Pneumological and Cardiovascular Sciences, Section of Pneu-ology, Policlinico San Matteo, Padiglione Forlanini, Via Taramelli 5,
7100 Pavia, Italy. Telephone: �39-0382-501008. Fax: �39-0382-22704. E-mail: [email protected] © 2007 by the International Society for Heart and Lungransplantation. 1053-2498/07/$–see front matter. doi:10.1016/
t.healun.2007.08.009
The exact pathogenesis of BOS and early markers ofhe disease are still unknown. Several alloantigen-de-endent and -independent factors, including numbernd severity of acute rejection (AR) episodes, HLAismatches, development of specific alloantibodies, isch-
mia–reperfusion injury, occurrence of viral respiratorynfections and gastroesophageal reflux, are thought toe involved in BOS development.5 A few recent studiesnalyzed BALf to identify early markers of disease or torovide new evidence regarding its pathogenesis. Twopproaches can be performed at present: one thatargets specific compounds on the basis of previous initro or animal studies, and another that systematicallyxamines the whole BALf protein content in differentroups of patients. Using the former approach, ourroup and others have demonstrated that several pro-nflammatory chemokines and cytokines, metallopro-eases and neutrophil products may be linked to BOSathogenesis.6–13 The latter approach has been at-
empted so far only by Nelsestuen and colleagues, whoerformed a retrospective global proteomic analysis ofALf extracts from LTRs by means of matrix-assisted
aser desorption/ionization–time-of-flight mass spec-
rometry (MALDI-TOF MS) profiles, demonstrating that1135
adp
ttBopLBersse(aebUa
MS
TbLa
lifsofi�sopittf1T4ocits
B
BaigfpTgtpnBf
2
OeBmwgtotPC(
Ti
C
NMAT
T
T
F
SoEps
1136 Meloni et al. The Journal of Heart and Lung TransplantationNovember 2007
n increase in human neutrophil � defensins14 and aecrease in Clara cell protein/lysozyme ratio15 canredict the onset of BOS.Two-dimensional gel electrophoresis and protein iden-
ification by MALDI-TOF (2-DE/MS) has been widely usedo assess the relative abundances of proteins present inALf in several lung diseases.16–22 Therefore, by meansf this proteomic platform, we evaluated the proteinrofiles of BALf obtained from BOS patients and stableTRs to identify additional proteins possibly involved inOS pathogenesis. Furthermore, based on the hypoth-sis that only proteins of lung origin could representeliable biomarkers of BOS, we evaluated the expres-ion of 11 proteins of interest in paired BALf and plasmaamples obtained from each patient. Two proteins werexclusively produced at the lung level: peroxiredoxin IIPRXII), which was expressed exclusively in BOS cases;nd surfactant protein A (SP-A), which was less widelyxpressed in BOS. Their expression was also assessedy dot blot in all patients, as well as in healthy controls.sing this method, the time course of SP-A was alsossessed in 5 additional LTRs who developed BOS.
ETHODStudy Population
he study consisted of archived BALf samples acquiredetween January 2000 and December 2005 from 20TRs, including 9 patients with BOS (Grades 1 and 2)nd 11 with stable lung function (stable LTRs).
BOS was diagnosed according to international guide-ines.23 Samples from LTRs with acute rejection (AR) ornfections at the time of BAL collection were purpose-ully excluded from the analysis. We included BALpecimens obtained within 1 month after BOS diagnosisr at �5 years post-surgery for patients with good graftunction. A paired plasma sample was obtained from allncluded LTRs at time of BAL collection and stored at
80°C until use. Enrolled LTRs initially received atandard triple-immunosuppressive regimen consistingf cyclosporine, azathioprine and steroid. None of theseatients received induction therapy. At the time of
nclusion in this study, all LTRs were treated with aacrolimus (FK 506)–based regimen (whole bloodrough levels between 10 and 15 ng/ml), being shiftedor refractory AR, toxicities or because of a BOS Grade
diagnosis. Patients’ characteristics are summarized inable 1. Six control non-smoking subjects (mean age:4 years; 4 females) undergoing bronchoscopy forccasional upper respiratory bleeding were also in-luded in this study. None had a recent history ofnfection or was under any medical treatment at theime of analysis. Informed consent to BAL and plasma
tudy was obtained from all patients and volunteers. Rronchoalveolar Lavage
AL was performed under standard conditions.24 Briefly,total of 150 ml of warm sterile saline solution was
nstilled in 30-ml aliquots and sequentially retrieved byentle aspiration. The first aliquot collected was usedor microbiologic and virologic studies, whereas otherooled aliquots were used for cytologic assessment.hese samples were immediately filtered twice throughauze and then centrifuged at 1,500 rpm for 10 minuteso allow separation of cells and fluid (BALf). BALfrotein concentration was determined by the bicincho-inic acid (BCA) protein assay (Pierce, Rockford, IL).ALf aliquots were dialyzed, lyophilized and then used
or 2-DE studies.
-DE Electrophoresis
ur detailed 2-DE protocol for BALf has been publishedlsewhere.22 For single 2-DE experiments, 70 �g ofALf proteins were loaded, with 1 mg loaded to allowass spectrometry identification. The protein mixtureas loaded onto non-linear immobilized pH 3 to 10
radient IPG gel strips (GE Healthcare) and isoelec-ric focusing was performed (Ettan IPGphor). Sec-nd, sodium dodecylsulfate–polyacrylamide gel elec-rophoresis (SDS-PAGE) was carried out using arotean II 2-D cell apparatus (Bio-Rad, Richmond,A). Gels were stained with ammonia silver nitrate
REF; Hochstrasser) or colloid Coomassie G-250 (Bio-
able 1. Characteristics of Lung Transplant Recipients (LTRs) Enrolledn the Present study, Classified According Transplant Outcome
Transplant outcome
haracteristics Stable BOS
umber 11 9ale:female 7:4 7:2ge, years (mean � SD) 54 � 12 45 � 13x indication
Pulmonary emphysema 3 1Idiopatic pulmonary fibrosis 3 2Cystic fibrosis 1 3Pulmonary fibrosis 2 2Other 1 ES, 1 PPH 1 PEPH
ype of TxDouble 5 5Single 5 4Heart–lung 1 —
ime of BOS Grade 1 diagnosis,mm (mean � SD)
— 43 � 29
EV1 (% predicted) 81.0 � 20 69.9 � 16.3
table, stable lung function at 5 years post-transplant; BOS, bronchiolitisbliterans syndrome Grade 1 at time of BALf collection; Tx, transplantation;S, Eisenmenger syndrome; PPH, primary pulmonary hypertension; PEPH,ost-embolic pulmonary hypertension; FEV1, forced expiratory volume in 1econd.
ad). All samples were assessed in triplicate.

G
TSPqpPttpatsMe
P
Aitlbagsps
P
BabCM((nDvQSw
cBe
S
RwuePsMt
RB
WLhpNcappd
P
WpMis1aobpwsw1
The Journal of Heart and Lung Transplantation Meloni et al. 1137Volume 26, Number 11
el Image Analysis
he gels were scanned (Model 3000, Versadoc Imagingystem; Bio-Rad) and images were then imported intoDQUEST 7.1 software (Bio-Rad). Initially, we analyzedualitative or quantitative differences in BALf proteinattern, comparing two synthetic gels generated byDQUEST software, taking into account spots commono every single patient of the same study group. Theotal spot density was then determined on a singleatient’s gels and used as a measure of the spotbundance. According to recent guidelines for differen-ial proteomic research,25 only unmatched spots andpots that significantly differed in density (p � 0.05, byann–Whitney U-test) were considered differentially
xpressed in BOS patients compared with stable LTRs.
rotein Identification
ll the differentially expressed protein spots weredentified by MALDI MS (Voyager DE-PRO mass spec-rometer; Applied Biosystems, Foster City, CA) and/oriquid chromatography (LC) MSMS (Q-TOF Ultima Hy-rid Mass Spectrometer; Micromass, Toronto, ON, Can-da). The MASCOT peptide fingerprinting search pro-ram (Matrix Science, Boston, MA) and PROTEINLYNX
oftware were used, respectively. These analyses wereerformed at CEINGE Biotecnologie Avanzate, Univer-ity Federico II, Naples (Italy).
rotein Dot Blotting
ALf proteins (10 �g) were applied to nitrocellulose indot-blot apparatus (Bio-Rad). Rabbit polyclonal anti-
ody anti-human–SP-A (Santa Cruz Biotechnology, Santaruz, CA), goat anti-PRXII (R&D Systems, Stillwater,N) and horseradish peroxidase (HRP)-conjugated
Santa Cruz) goat anti-rabbit IgG or donkey anti-goat IgGR&D) were used, respectively. Enhanced chemilumi-escence was performed using the Western Blottingetection Reagent (GE Healthcare) and densitometricalues (optical density [OD] � area) determined withUANTITY ONE software (Bio-Rad). The approximate
P-A levels (nanograms per 10 �g of total proteins)ere determined by comparison with the standard
Table 2. Features of BAL in the Study Populat
Stable LTRs(n 11)
Total BAL cells (106/ml) 0.39 � 0.27Macrophages (%) 86.2 � 5.1Neutrophils (%) 2.3 � 1.8Lymphocytes (%) 11.0 � 4.2Eosinophils (%) 0.5 � 0.5Total protein (�g/ml) 0.33 � 0.26
Results expressed as mean � SD. Comparison wasLTRs, lung transplant recipients; BOS, brochiolitis
ap � 0.05, bp � 0.01, compared with stable LTRs.urve values, obtained with SP-A extracted from theALf of a patient with alveolar proteinosis, as describedlsewhere.26
tatistical Analysis
esults were analyzed using PRISM 3.0 (GraphPad Soft-are, San Diego, CA). Data relative to normally distrib-ted variables are presented as mean � SD, and differ-nces were assessed by a 2-tailed Student’s t-test.roteomic expression data are expressed as medianpot quantities, and differences were assessed using theann–Whitney U-test. p � 0.05 was considered statis-
ically significant.
ESULTSAL Features
e included a total of 26 BALf samples obtained from: 11TRs who, at a mean of 81.4 � 20.3 months post-Tx, stillad stable graft function; 9 LTRs who, at 43 � 29 monthsost-Tx, developed BOS Grade 1; and 6 healthy controls.o evidence of AR or infection was present at time of BALollection in LTRs. Total BAL cell counts, cytologic profilend protein content are summarized in Table 2. Neutro-hilic and eosinophilic alveolitis was observed in BOSatients as compared with stable LTRs. No significantifferences were observed for all other parameters.
rotein Composition of BALf
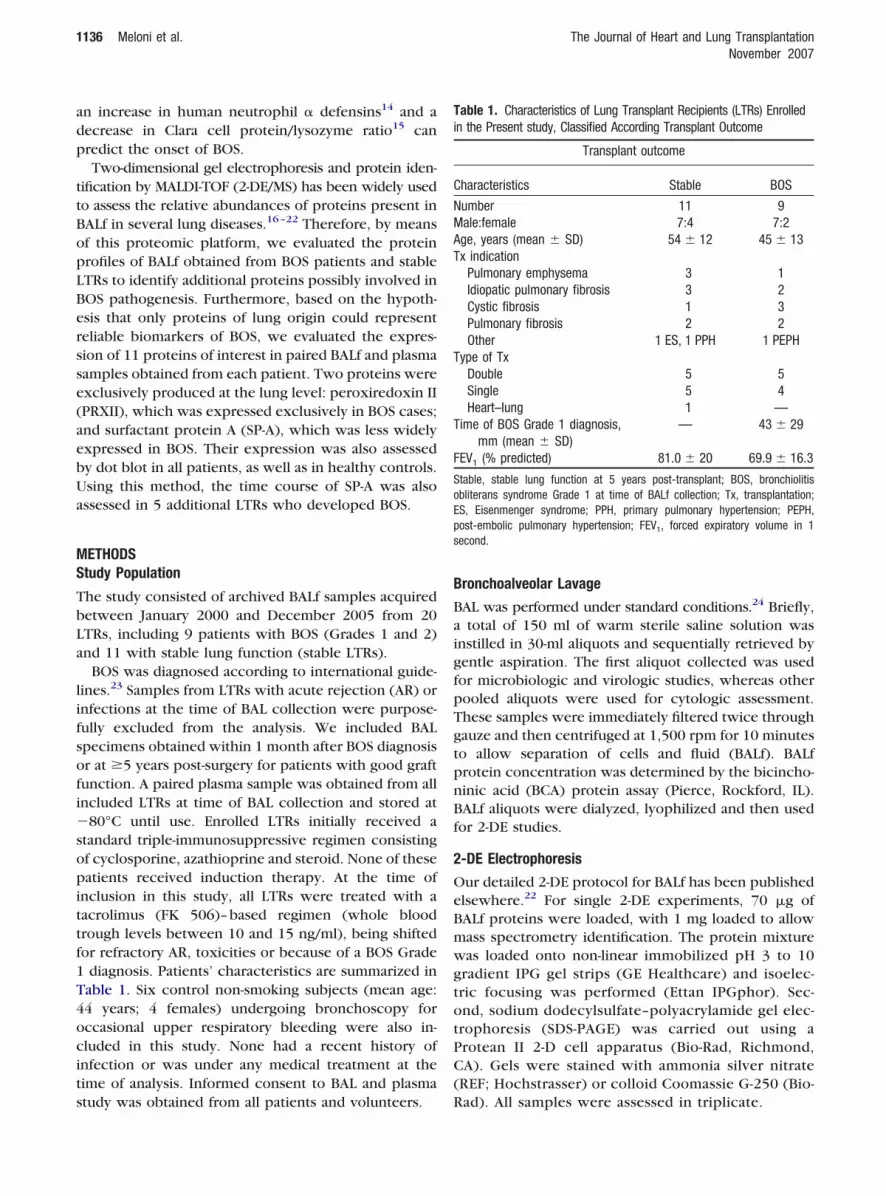
e compared the protein profile of BALf from BOSatients and stable LTRs by means of the 2-DE andALDI MS platform. Figure 1 shows the BALf Coomass-
e-stained 2-DE gels of a BOS patient (Figure 1a) and atable LTR (Figure 1b). Overall, we counted 172 and65 spots/spot-trains in the common profiles of stablend BOS LTRs, respectively. Comparative analysis dem-nstrated both qualitative and quantitative differencesetween groups (Table 3). This differential proteomicsattern was composed of 27 protein spots. Eight spotsere expressed in all BOS patients but were never ob-
erved in individual gels from stable LTRs. Another 8 spotsere exclusively present in each stable LTR. In addition,
1 spots were found to vary significantly between the two
BOS LTRs(n 9)
Control subjects(n 6)
0.38 � 0.35 0.20 � 0.1479.5 � 10.8 88.8 � 13.37.6 � 4.9b 1.7 � 1.1
11.1 � 7.0 9.5 � 7.62.9 � 4.4a —
0.45 � 0.42 0.11 � 0.09
e by Student’s t-test.terans syndrome.
ion
madobli
sBt
sprm
m4Bdlbp
pG(Bc�fl
C
AupestpPtCBdb
EC
Atafisct
S
Dbpwrs
pvsSFl
T
WfB
FfbciPspm
1138 Meloni et al. The Journal of Heart and Lung TransplantationNovember 2007
tudy groups: 7 showed significantly higher expression inOS, whereas 4 showed lower expression in BOS patientshan in stable LTRs (p � 0.05).
Mass spectrometry analysis identified 22 of these 27pots as 11 unique proteins or protein fragments. Fiverotein spots (numbered 23 to 27 in Table 3 and Figure 1)emained unidentified, even after analysis by liquid chro-atography–tandem mass spectrometry (LC-MSMS).The total quantity of each protein (including frag-ents) in the two study groups is summarized in Table
. Among proteins that were exclusively detectable inOS we identified complement C3 (C3) and peroxire-oxin II (PRXII). Both proteins were expressed at low
evels and, interestingly, one of them, PRXII, has nevereen described previously in BALf 2-DE proteome. Five
igure 1. The 2-DE patterns of bronchoalveolar lavage fluid (BALf)rom a representative lung transplant recipient (LTR) who developedronchiolitis obliterans syndrome (BOS) (A) and an LTR with stablelinical function (B). The 2-DE was performed using a non-linearmmobilized gradient pH 3 to 10, followed by 9% to 16% SDS-PAGE.rotein spots were detected by Coomassie staining. Spots showingtatistically significant differences in quantity in BOS patients com-ared with stable LTRs (Mann–Whitney U-test, p � 0.05) or un-atched spots are indicated with numbers referring to Table 3.
roteins, including �1B-glycoprotein (�1B-G), �2HS-glyco- P
rotein (�2HS-G), leucine-rich �2-glycoprotein (L-R�2-), apolipoprotein A1 (APO AI) and C-reactive protein
CRP), were expressed at a significantly higher rate inOS patients compared with stable LTRs (p � 0.05). Inontrast, four proteins, �1-anti-chymotrypsin (�1-ACT),
1-acid glycoprotein (�1-AG), haptoglobin (Hp) and sur-actant protein-A (SP-A), were expressed at a significantlyower rate in BOS than in stable LTRs (p � 0.05).
omparative Analysis of BALf and Plasma 2-DE Profile
mong the 11 differentially expressed proteins, 9 aresually classified as plasma proteins, including 7 acute-hase reactants (APRs).27 Therefore, we compared thexpression of these proteins in paired BALf and plasmaamples to assess whether BALf protein variations be-ween BOS patients and stable LTRs simply mirrorlasmatic ones. As shown in Table 5, two proteins,RXII and SP-A, were not detectable at plasma levels. Allhe other proteins were present also in plasma. APO AI,3 and �1-ACT were significantly increased in plasma ofOS patients, whereas �2-HSG showed a significantecrease. No differences were noted at the plasma leveletween the two study group for all other proteins.
xpression of PRXII and SP-A in BALf Fromontrol Subjects
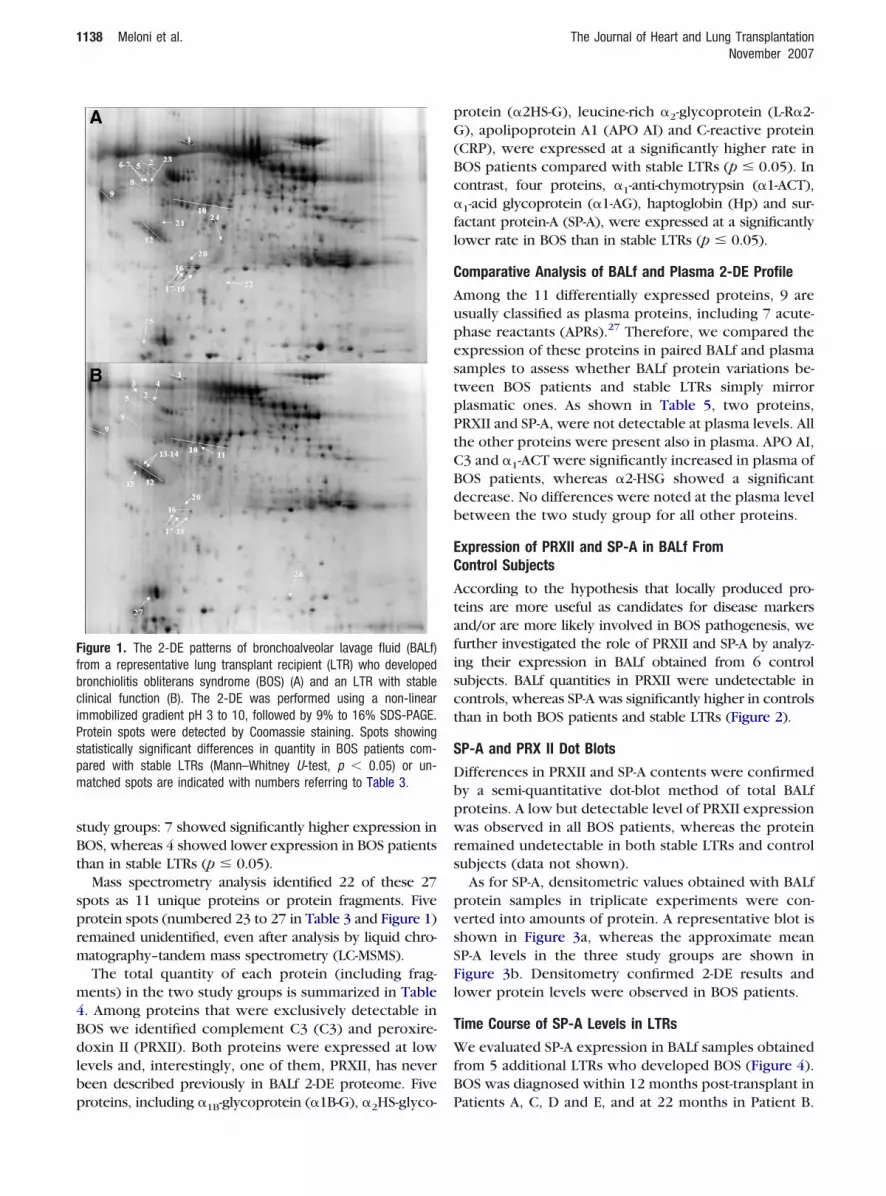
ccording to the hypothesis that locally produced pro-eins are more useful as candidates for disease markersnd/or are more likely involved in BOS pathogenesis, weurther investigated the role of PRXII and SP-A by analyz-ng their expression in BALf obtained from 6 controlubjects. BALf quantities in PRXII were undetectable inontrols, whereas SP-A was significantly higher in controlshan in both BOS patients and stable LTRs (Figure 2).
P-A and PRX II Dot Blots
ifferences in PRXII and SP-A contents were confirmedy a semi-quantitative dot-blot method of total BALfroteins. A low but detectable level of PRXII expressionas observed in all BOS patients, whereas the protein
emained undetectable in both stable LTRs and controlubjects (data not shown).
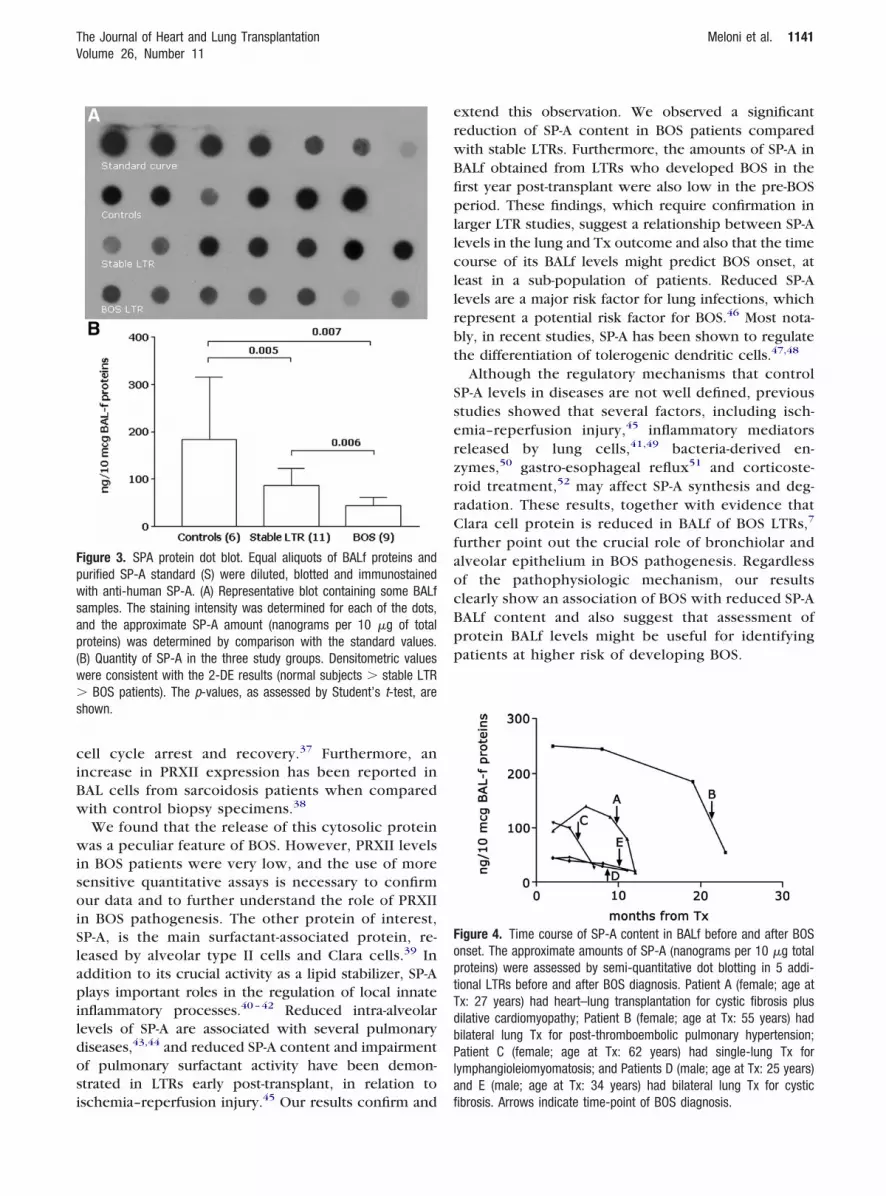
As for SP-A, densitometric values obtained with BALfrotein samples in triplicate experiments were con-erted into amounts of protein. A representative blot ishown in Figure 3a, whereas the approximate meanP-A levels in the three study groups are shown inigure 3b. Densitometry confirmed 2-DE results andower protein levels were observed in BOS patients.
ime Course of SP-A Levels in LTRs
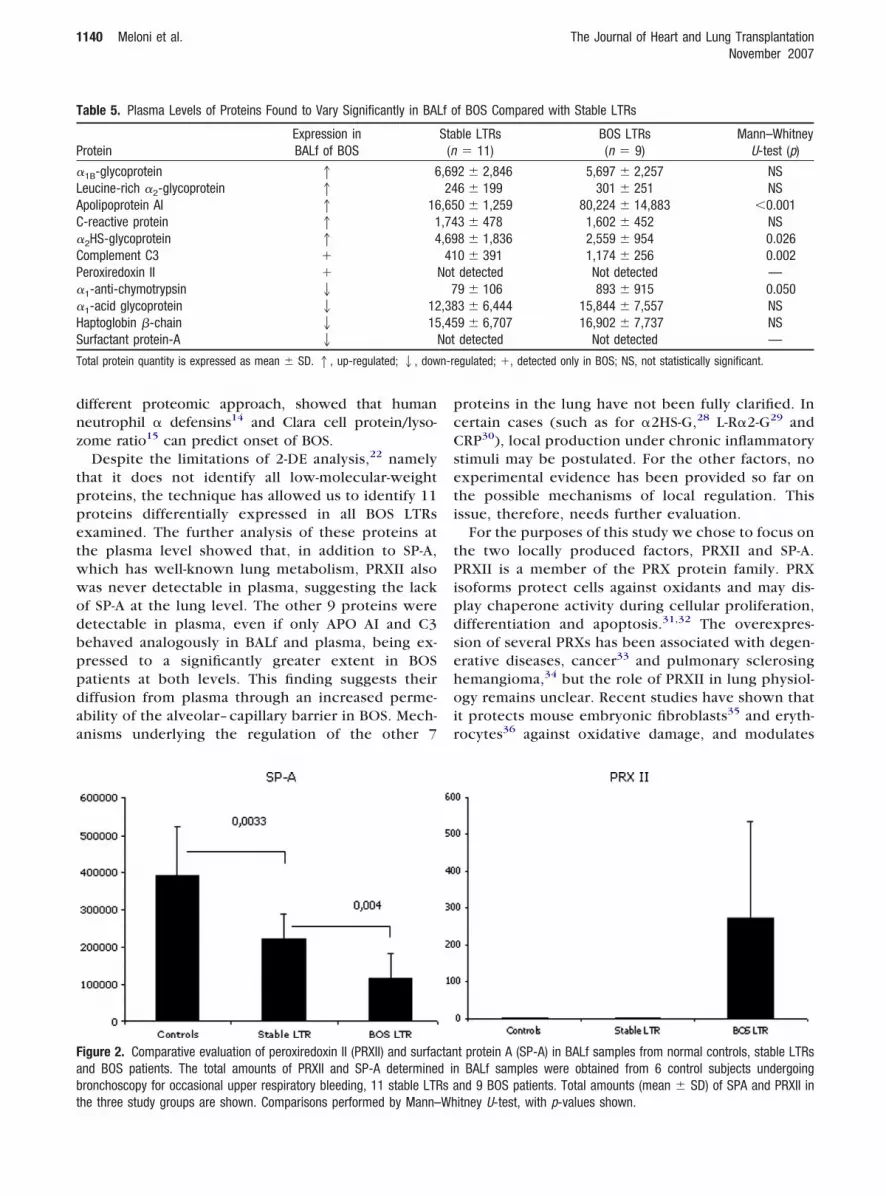
e evaluated SP-A expression in BALf samples obtainedrom 5 additional LTRs who developed BOS (Figure 4).OS was diagnosed within 12 months post-transplant in
atients A, C, D and E, and at 22 months in Patient B.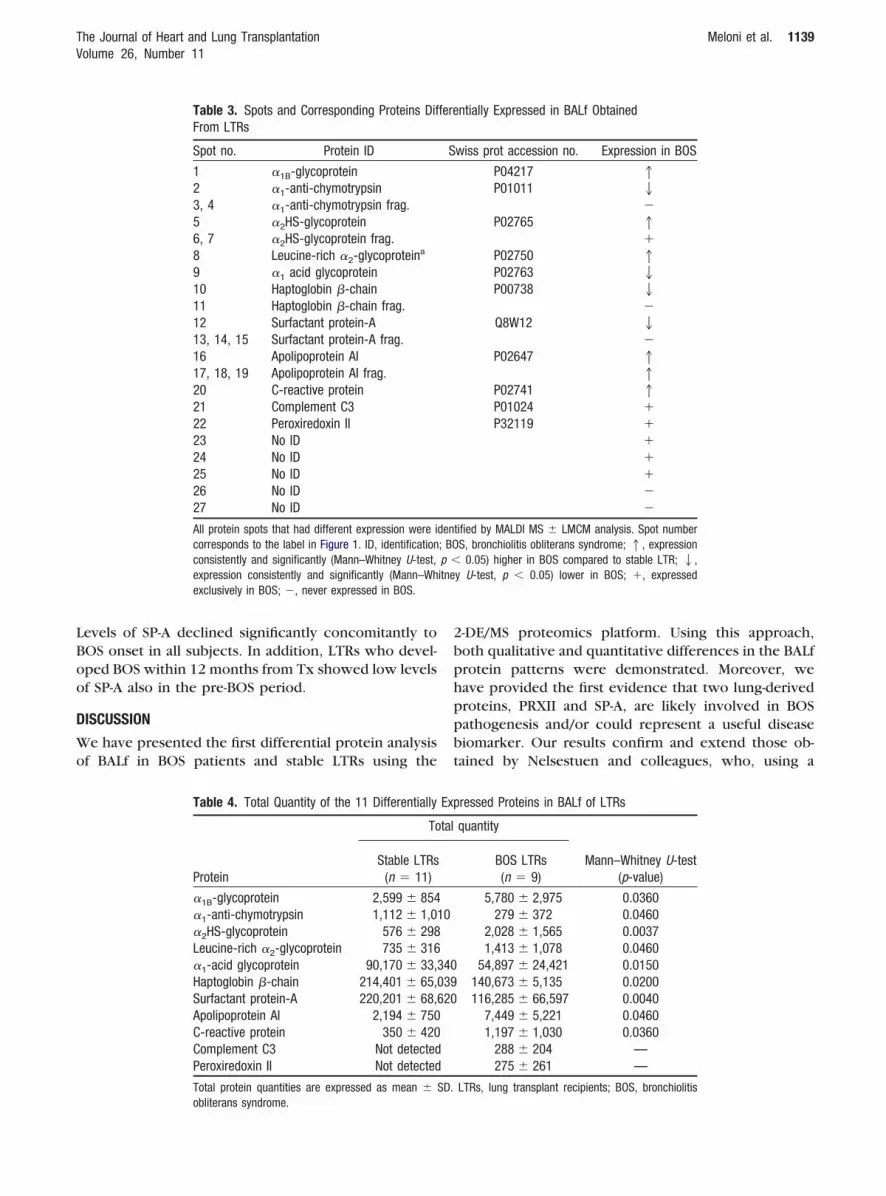
LBoo
D
Wo
2bphppbt
The Journal of Heart and Lung Transplantation Meloni et al. 1139Volume 26, Number 11
evels of SP-A declined significantly concomitantly toOS onset in all subjects. In addition, LTRs who devel-ped BOS within 12 months from Tx showed low levelsf SP-A also in the pre-BOS period.
ISCUSSION
e have presented the first differential protein analysisf BALf in BOS patients and stable LTRs using the
Table 3. Spots and Corresponding Proteins DifFrom LTRs
Spot no. Protein ID
1 �1B-glycoprotein2 �1-anti-chymotrypsin3, 4 �1-anti-chymotrypsin frag.5 �2HS-glycoprotein6, 7 �2HS-glycoprotein frag.8 Leucine-rich �2-glycoproteina
9 �1 acid glycoprotein10 Haptoglobin �-chain11 Haptoglobin �-chain frag.12 Surfactant protein-A13, 14, 15 Surfactant protein-A frag.16 Apolipoprotein AI17, 18, 19 Apolipoprotein AI frag.20 C-reactive protein21 Complement C322 Peroxiredoxin II23 No ID24 No ID25 No ID26 No ID27 No ID
All protein spots that had different expression were icorresponds to the label in Figure 1. ID, identificationconsistently and significantly (Mann–Whitney U-test,expression consistently and significantly (Mann–Whexclusively in BOS; �, never expressed in BOS.
Table 4. Total Quantity of the 11 Differentially
Protein
To
Stable LTRs(n 11)
�1B-glycoprotein 2,599 � 854�1-anti-chymotrypsin 1,112 � 1,0�2HS-glycoprotein 576 � 298Leucine-rich �2-glycoprotein 735 � 316�1-acid glycoprotein 90,170 � 33,Haptoglobin �-chain 214,401 � 65,Surfactant protein-A 220,201 � 68,Apolipoprotein AI 2,194 � 750C-reactive protein 350 � 420Complement C3 Not detectedPeroxiredoxin II Not detected
Total protein quantities are expressed as mean �
obliterans syndrome.-DE/MS proteomics platform. Using this approach,oth qualitative and quantitative differences in the BALfrotein patterns were demonstrated. Moreover, weave provided the first evidence that two lung-derivedroteins, PRXII and SP-A, are likely involved in BOSathogenesis and/or could represent a useful diseaseiomarker. Our results confirm and extend those ob-ained by Nelsestuen and colleagues, who, using a
ntially Expressed in BALf Obtained
wiss prot accession no. Expression in BOS
P04217 1P01011 2
�P02765 1
�P02750 1P02763 2P00738 2
�Q8W12 2
�P02647 1
1P02741 1P01024 �P32119 �
�����
tified by MALDI MS � LMCM analysis. Spot numberS, bronchiolitis obliterans syndrome; 1, expression
0.05) higher in BOS compared to stable LTR; 2,y U-test, p � 0.05) lower in BOS; �, expressed
ressed Proteins in BALf of LTRs
quantity
Mann–Whitney U-test(p-value)
BOS LTRs(n 9)
5,780 � 2,975 0.0360279 � 372 0.0460
2,028 � 1,565 0.00371,413 � 1,078 0.0460
54,897 � 24,421 0.0150140,673 � 5,135 0.0200116,285 � 66,597 0.0040
7,449 � 5,221 0.04601,197 � 1,030 0.0360
288 � 204 —275 � 261 —
LTRs, lung transplant recipients; BOS, bronchiolitis
fere
S
den; BOp �itne
Exp
tal
10
340039620
SD.
dnz
tppetwwodbppdaa
pcCseti
tPipdsehoir
T
P
�LAC�CP��HS
T n-r
Fabt
1140 Meloni et al. The Journal of Heart and Lung TransplantationNovember 2007
ifferent proteomic approach, showed that humaneutrophil � defensins14 and Clara cell protein/lyso-ome ratio15 can predict onset of BOS.
Despite the limitations of 2-DE analysis,22 namelyhat it does not identify all low-molecular-weightroteins, the technique has allowed us to identify 11roteins differentially expressed in all BOS LTRsxamined. The further analysis of these proteins athe plasma level showed that, in addition to SP-A,hich has well-known lung metabolism, PRXII alsoas never detectable in plasma, suggesting the lackf SP-A at the lung level. The other 9 proteins wereetectable in plasma, even if only APO AI and C3ehaved analogously in BALf and plasma, being ex-ressed to a significantly greater extent in BOSatients at both levels. This finding suggests theiriffusion from plasma through an increased perme-bility of the alveolar– capillary barrier in BOS. Mech-nisms underlying the regulation of the other 7
able 5. Plasma Levels of Proteins Found to Vary Significantly in BA
roteinExpression inBALf of BOS
1B-glycoprotein 1 6eucine-rich �2-glycoprotein 1polipoprotein AI 1 16-reactive protein 1 1
2HS-glycoprotein 1 4omplement C3 �eroxiredoxin II �
1-anti-chymotrypsin 2
1-acid glycoprotein 2 12aptoglobin �-chain 2 15urfactant protein-A 2
otal protein quantity is expressed as mean � SD. 1, up-regulated; 2, dow
igure 2. Comparative evaluation of peroxiredoxin II (PRXII) and surfacnd BOS patients. The total amounts of PRXII and SP-A determineronchoscopy for occasional upper respiratory bleeding, 11 stable LTR
he three study groups are shown. Comparisons performed by Mann–Whroteins in the lung have not been fully clarified. Inertain cases (such as for �2HS-G,28 L-R�2-G29 andRP30), local production under chronic inflammatorytimuli may be postulated. For the other factors, noxperimental evidence has been provided so far onhe possible mechanisms of local regulation. Thisssue, therefore, needs further evaluation.
For the purposes of this study we chose to focus onhe two locally produced factors, PRXII and SP-A.RXII is a member of the PRX protein family. PRX
soforms protect cells against oxidants and may dis-lay chaperone activity during cellular proliferation,ifferentiation and apoptosis.31,32 The overexpres-ion of several PRXs has been associated with degen-rative diseases, cancer33 and pulmonary sclerosingemangioma,34 but the role of PRXII in lung physiol-gy remains unclear. Recent studies have shown that
t protects mouse embryonic fibroblasts35 and eryth-ocytes36 against oxidative damage, and modulates
f BOS Compared with Stable LTRs
ble LTRs 11)
BOS LTRs(n 9)
Mann–WhitneyU-test (p)
2 � 2,846 5,697 � 2,257 NS6 � 199 301 � 251 NS0 � 1,259 80,224 � 14,883 �0.0013 � 478 1,602 � 452 NS8 � 1,836 2,559 � 954 0.0260 � 391 1,174 � 256 0.002detected Not detected —9 � 106 893 � 915 0.0503 � 6,444 15,844 � 7,557 NS9 � 6,707 16,902 � 7,737 NSdetected Not detected —
egulated; �, detected only in BOS; NS, not statistically significant.
t protein A (SP-A) in BALf samples from normal controls, stable LTRsBALf samples were obtained from 6 control subjects undergoing
nd 9 BOS patients. Total amounts (mean � SD) of SPA and PRXII in
Lf o
Sta(n
,6924,65,74,6941
Not7
,38,45
Not
tand ins a
itney U-test, with p-values shown.
ciBw
wisoiSlapildosi
erwBfipllcllrbt
SserzrrCfaocBpp
Fpwsap(w�s
FoptTdbPla
The Journal of Heart and Lung Transplantation Meloni et al. 1141Volume 26, Number 11
ell cycle arrest and recovery.37 Furthermore, anncrease in PRXII expression has been reported inAL cells from sarcoidosis patients when comparedith control biopsy specimens.38
We found that the release of this cytosolic proteinas a peculiar feature of BOS. However, PRXII levels
n BOS patients were very low, and the use of moreensitive quantitative assays is necessary to confirmur data and to further understand the role of PRXII
n BOS pathogenesis. The other protein of interest,P-A, is the main surfactant-associated protein, re-eased by alveolar type II cells and Clara cells.39 Inddition to its crucial activity as a lipid stabilizer, SP-Alays important roles in the regulation of local innate
nflammatory processes.40–42 Reduced intra-alveolarevels of SP-A are associated with several pulmonaryiseases,43,44 and reduced SP-A content and impairmentf pulmonary surfactant activity have been demon-trated in LTRs early post-transplant, in relation to
igure 3. SPA protein dot blot. Equal aliquots of BALf proteins andurified SP-A standard (S) were diluted, blotted and immunostainedith anti-human SP-A. (A) Representative blot containing some BALf
amples. The staining intensity was determined for each of the dots,nd the approximate SP-A amount (nanograms per 10 �g of totalroteins) was determined by comparison with the standard values.B) Quantity of SP-A in the three study groups. Densitometric valuesere consistent with the 2-DE results (normal subjects � stable LTR
BOS patients). The p-values, as assessed by Student’s t-test, arehown.
schemia–reperfusion injury.45 Our results confirm and fi
xtend this observation. We observed a significanteduction of SP-A content in BOS patients comparedith stable LTRs. Furthermore, the amounts of SP-A inALf obtained from LTRs who developed BOS in therst year post-transplant were also low in the pre-BOSeriod. These findings, which require confirmation in
arger LTR studies, suggest a relationship between SP-Aevels in the lung and Tx outcome and also that the timeourse of its BALf levels might predict BOS onset, ateast in a sub-population of patients. Reduced SP-Aevels are a major risk factor for lung infections, whichepresent a potential risk factor for BOS.46 Most nota-ly, in recent studies, SP-A has been shown to regulatehe differentiation of tolerogenic dendritic cells.47,48
Although the regulatory mechanisms that controlP-A levels in diseases are not well defined, previoustudies showed that several factors, including isch-mia–reperfusion injury,45 inflammatory mediatorseleased by lung cells,41,49 bacteria-derived en-ymes,50 gastro-esophageal reflux51 and corticoste-oid treatment,52 may affect SP-A synthesis and deg-adation. These results, together with evidence thatlara cell protein is reduced in BALf of BOS LTRs,7
urther point out the crucial role of bronchiolar andlveolar epithelium in BOS pathogenesis. Regardlessf the pathophysiologic mechanism, our resultslearly show an association of BOS with reduced SP-AALf content and also suggest that assessment ofrotein BALf levels might be useful for identifyingatients at higher risk of developing BOS.
igure 4. Time course of SP-A content in BALf before and after BOSnset. The approximate amounts of SP-A (nanograms per 10 �g totalroteins) were assessed by semi-quantitative dot blotting in 5 addi-ional LTRs before and after BOS diagnosis. Patient A (female; age atx: 27 years) had heart–lung transplantation for cystic fibrosis plusilative cardiomyopathy; Patient B (female; age at Tx: 55 years) hadilateral lung Tx for post-thromboembolic pulmonary hypertension;atient C (female; age at Tx: 62 years) had single-lung Tx for
ymphangioleiomyomatosis; and Patients D (male; age at Tx: 25 years)nd E (male; age at Tx: 34 years) had bilateral lung Tx for cystic
brosis. Arrows indicate time-point of BOS diagnosis.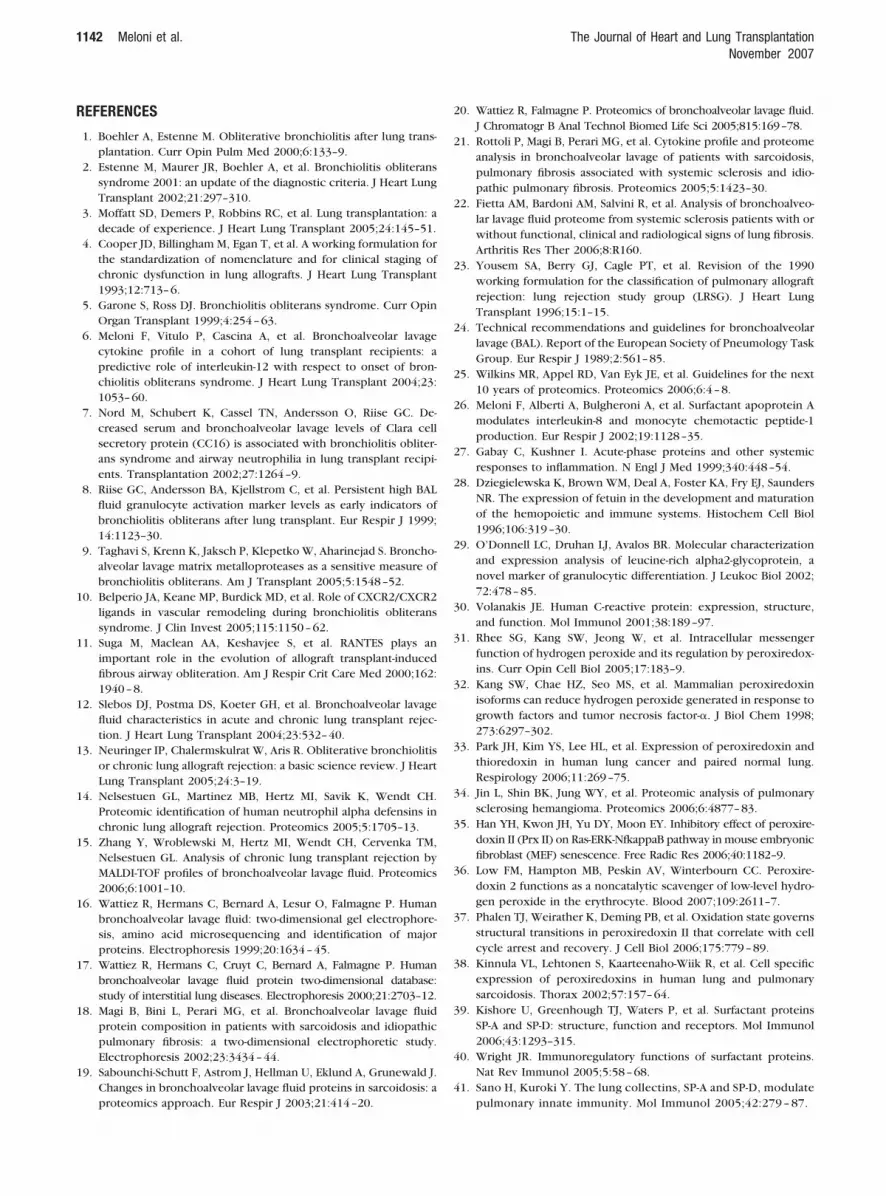
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
1142 Meloni et al. The Journal of Heart and Lung TransplantationNovember 2007
EFERENCES
1. Boehler A, Estenne M. Obliterative bronchiolitis after lung trans-plantation. Curr Opin Pulm Med 2000;6:133–9.
2. Estenne M, Maurer JR, Boehler A, et al. Bronchiolitis obliteranssyndrome 2001: an update of the diagnostic criteria. J Heart LungTransplant 2002;21:297–310.
3. Moffatt SD, Demers P, Robbins RC, et al. Lung transplantation: adecade of experience. J Heart Lung Transplant 2005;24:145–51.
4. Cooper JD, Billingham M, Egan T, et al. A working formulation forthe standardization of nomenclature and for clinical staging ofchronic dysfunction in lung allografts. J Heart Lung Transplant1993;12:713–6.
5. Garone S, Ross DJ. Bronchiolitis obliterans syndrome. Curr OpinOrgan Transplant 1999;4:254–63.
6. Meloni F, Vitulo P, Cascina A, et al. Bronchoalveolar lavagecytokine profile in a cohort of lung transplant recipients: apredictive role of interleukin-12 with respect to onset of bron-chiolitis obliterans syndrome. J Heart Lung Transplant 2004;23:1053–60.
7. Nord M, Schubert K, Cassel TN, Andersson O, Riise GC. De-creased serum and bronchoalveolar lavage levels of Clara cellsecretory protein (CC16) is associated with bronchiolitis obliter-ans syndrome and airway neutrophilia in lung transplant recipi-ents. Transplantation 2002;27:1264–9.
8. Riise GC, Andersson BA, Kjellstrom C, et al. Persistent high BALfluid granulocyte activation marker levels as early indicators ofbronchiolitis obliterans after lung transplant. Eur Respir J 1999;14:1123–30.
9. Taghavi S, Krenn K, Jaksch P, Klepetko W, Aharinejad S. Broncho-alveolar lavage matrix metalloproteases as a sensitive measure ofbronchiolitis obliterans. Am J Transplant 2005;5:1548–52.
0. Belperio JA, Keane MP, Burdick MD, et al. Role of CXCR2/CXCR2ligands in vascular remodeling during bronchiolitis obliteranssyndrome. J Clin Invest 2005;115:1150–62.
1. Suga M, Maclean AA, Keshavjee S, et al. RANTES plays animportant role in the evolution of allograft transplant-inducedfibrous airway obliteration. Am J Respir Crit Care Med 2000;162:1940–8.
2. Slebos DJ, Postma DS, Koeter GH, et al. Bronchoalveolar lavagefluid characteristics in acute and chronic lung transplant rejec-tion. J Heart Lung Transplant 2004;23:532–40.
3. Neuringer IP, Chalermskulrat W, Aris R. Obliterative bronchiolitisor chronic lung allograft rejection: a basic science review. J HeartLung Transplant 2005;24:3–19.
4. Nelsestuen GL, Martinez MB, Hertz MI, Savik K, Wendt CH.Proteomic identification of human neutrophil alpha defensins inchronic lung allograft rejection. Proteomics 2005;5:1705–13.
5. Zhang Y, Wroblewski M, Hertz MI, Wendt CH, Cervenka TM,Nelsestuen GL. Analysis of chronic lung transplant rejection byMALDI-TOF profiles of bronchoalveolar lavage fluid. Proteomics2006;6:1001–10.
6. Wattiez R, Hermans C, Bernard A, Lesur O, Falmagne P. Humanbronchoalveolar lavage fluid: two-dimensional gel electrophore-sis, amino acid microsequencing and identification of majorproteins. Electrophoresis 1999;20:1634–45.
7. Wattiez R, Hermans C, Cruyt C, Bernard A, Falmagne P. Humanbronchoalveolar lavage fluid protein two-dimensional database:study of interstitial lung diseases. Electrophoresis 2000;21:2703–12.
8. Magi B, Bini L, Perari MG, et al. Bronchoalveolar lavage fluidprotein composition in patients with sarcoidosis and idiopathicpulmonary fibrosis: a two-dimensional electrophoretic study.Electrophoresis 2002;23:3434–44.
9. Sabounchi-Schutt F, Astrom J, Hellman U, Eklund A, Grunewald J.Changes in bronchoalveolar lavage fluid proteins in sarcoidosis: a
proteomics approach. Eur Respir J 2003;21:414–20.0. Wattiez R, Falmagne P. Proteomics of bronchoalveolar lavage fluid.J Chromatogr B Anal Technol Biomed Life Sci 2005;815:169–78.
1. Rottoli P, Magi B, Perari MG, et al. Cytokine profile and proteomeanalysis in bronchoalveolar lavage of patients with sarcoidosis,pulmonary fibrosis associated with systemic sclerosis and idio-pathic pulmonary fibrosis. Proteomics 2005;5:1423–30.
2. Fietta AM, Bardoni AM, Salvini R, et al. Analysis of bronchoalveo-lar lavage fluid proteome from systemic sclerosis patients with orwithout functional, clinical and radiological signs of lung fibrosis.Arthritis Res Ther 2006;8:R160.
3. Yousem SA, Berry GJ, Cagle PT, et al. Revision of the 1990working formulation for the classification of pulmonary allograftrejection: lung rejection study group (LRSG). J Heart LungTransplant 1996;15:1–15.
4. Technical recommendations and guidelines for bronchoalveolarlavage (BAL). Report of the European Society of Pneumology TaskGroup. Eur Respir J 1989;2:561–85.
5. Wilkins MR, Appel RD, Van Eyk JE, et al. Guidelines for the next10 years of proteomics. Proteomics 2006;6:4–8.
6. Meloni F, Alberti A, Bulgheroni A, et al. Surfactant apoprotein Amodulates interleukin-8 and monocyte chemotactic peptide-1production. Eur Respir J 2002;19:1128–35.
7. Gabay C, Kushner I. Acute-phase proteins and other systemicresponses to inflammation. N Engl J Med 1999;340:448–54.
8. Dziegielewska K, Brown WM, Deal A, Foster KA, Fry EJ, SaundersNR. The expression of fetuin in the development and maturationof the hemopoietic and immune systems. Histochem Cell Biol1996;106:319–30.
9. O’Donnell LC, Druhan LJ, Avalos BR. Molecular characterizationand expression analysis of leucine-rich alpha2-glycoprotein, anovel marker of granulocytic differentiation. J Leukoc Biol 2002;72:478–85.
0. Volanakis JE. Human C-reactive protein: expression, structure,and function. Mol Immunol 2001;38:189–97.
1. Rhee SG, Kang SW, Jeong W, et al. Intracellular messengerfunction of hydrogen peroxide and its regulation by peroxiredox-ins. Curr Opin Cell Biol 2005;17:183–9.
2. Kang SW, Chae HZ, Seo MS, et al. Mammalian peroxiredoxinisoforms can reduce hydrogen peroxide generated in response togrowth factors and tumor necrosis factor-�. J Biol Chem 1998;273:6297–302.
3. Park JH, Kim YS, Lee HL, et al. Expression of peroxiredoxin andthioredoxin in human lung cancer and paired normal lung.Respirology 2006;11:269–75.
4. Jin L, Shin BK, Jung WY, et al. Proteomic analysis of pulmonarysclerosing hemangioma. Proteomics 2006;6:4877–83.
5. Han YH, Kwon JH, Yu DY, Moon EY. Inhibitory effect of peroxire-doxin II (Prx II) on Ras-ERK-NfkappaB pathway in mouse embryonicfibroblast (MEF) senescence. Free Radic Res 2006;40:1182–9.
6. Low FM, Hampton MB, Peskin AV, Winterbourn CC. Peroxire-doxin 2 functions as a noncatalytic scavenger of low-level hydro-gen peroxide in the erythrocyte. Blood 2007;109:2611–7.
7. Phalen TJ, Weirather K, Deming PB, et al. Oxidation state governsstructural transitions in peroxiredoxin II that correlate with cellcycle arrest and recovery. J Cell Biol 2006;175:779–89.
8. Kinnula VL, Lehtonen S, Kaarteenaho-Wiik R, et al. Cell specificexpression of peroxiredoxins in human lung and pulmonarysarcoidosis. Thorax 2002;57:157–64.
9. Kishore U, Greenhough TJ, Waters P, et al. Surfactant proteinsSP-A and SP-D: structure, function and receptors. Mol Immunol2006;43:1293–315.
0. Wright JR. Immunoregulatory functions of surfactant proteins.Nat Rev Immunol 2005;5:58–68.
1. Sano H, Kuroki Y. The lung collectins, SP-A and SP-D, modulate
pulmonary innate immunity. Mol Immunol 2005;42:279 – 87.
4
4
4
4
4
4
4
4
5
5
5
The Journal of Heart and Lung Transplantation Meloni et al. 1143Volume 26, Number 11
2. Yang S, Milla C, Panoskaltsis-Mortari A, et al. Human surfactantprotein a suppresses T cell-dependent inflammation and attenu-ates the manifestations of idiopathic pneumonia syndrome inmice. Am J Respir Cell Mol Biol 2001;24:527–36.
3. Tagaram HR, Wang G, Umstead TM, et al. Characterization of ahuman surfactant protein A1 (SP-A1) gene-specific antibody;SP-A1 content variation among individuals of varying age andpulmonary health. Am J Physiol Lung Cell Mol Physiol 2007;292:L1052–63.
4. Heinrich S, Hartl D, Griese M. Surfactant protein A—from genesto human lung diseases. Curr Med Chem 2006;13:3239–52.
5. Casals C, Varela A, Ruano ML, et al. Increase of C-reactive proteinand decrease of surfactant protein A in surfactant after lung trans-plantation. Am J Respir Crit Care Med 1998;157:43–9.
6. Scott AI, Sharples LD, Stewart S. Bronchiolitis obliterans syndrome:risk factors and therapeutic strategies. Drugs 2005;65:761–71.
7. Hussain S. Role of surfactant protein A in innate host defense and
autoimmunity. Autoimmunity 2004;37:125–30.8. Brinker KG, Garner H, Wright JR. Surfactant protein A modu-lates the differentiation of murine bone marrow-derived den-dritic cells. Am J Physiol Lung Cell Mol Physiol 2003;284:L232– 41.
9. Rubio F, Cooley J, Accurso FJ, Remold-O’Donnell E. Linkage ofneutrophil serine proteases and decreased surfactant protein-A(SP-A) levels in inflammatory lung disease. Thorax 2004;59:318 –23.
0. Mariencheck WI, Alcorn JF, Palmer SM, Wright JR. Pseudomonasaeruginosa elastase degrades surfactant proteins A and D. Am JRespir Cell Mol Biol 2003;28:528–37.
1. D’Ovidio F, Mura M, Ridsdale R, et al. The effect of reflux and bileacid aspiration on the lung allograft and its surfactant and innateimmunity molecules SP-A and SP-D. Am J Transplant 2006;6:1930–8.
2. Hoover RR, Floros J. SP-A 3=-UTR is involved in the glucocorticoidinhibition of human SP-A gene expression. Am J Physiol Lung Cell
Mol Physiol 1999;276:L917–24.
Related Documents











