BY SROTA DAWN. M.PHARM [PHARMACOLOGY] SUBJECT - PHARMACOLOGY -∏ VELS SCHOOL OF PHARMACEUTICAL SCIENCES BRONCHITIS [PATHOLOGY & TREATMENT] 06/26/2022 1

bronchitis (pathology and treatment)by srota dawn
May 26, 2015
this presentation contains a detailed description about bronchitis ,its types, pathology,causes, treatment etc.
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

04/12/2023
1
BYSROTA DAWN.
M.PHARM [PHARMACOLOGY]SUBJECT - PHARMACOLOGY -∏
VELS SCHOOL OF PHARMACEUTICAL SCIENCES
BRONCHITIS[PATHOLOGY & TREATMENT]

04/12/20232
Chronic obstructive pulmonary disease.Bronchitis, emphysema, and asthma may
present alone or in combination.
AsthmaBronchitis
Emphysema

04/12/2023
3
DescriptionDescription
Characterized by presence of airflow obstruction
Caused by emphysema or chronic bronchitisGenerally progressive May be accompanied by airway
hyperreactivityMay be partially reversible
Characterized by presence of airflow obstruction
Caused by emphysema or chronic bronchitisGenerally progressive May be accompanied by airway
hyperreactivityMay be partially reversible

04/12/2023
4
EmphysemaEmphysema
Abnormal permanent enlargement of the air space distal to the terminal bronchioles
Accompanied by destruction of bronchioles
Abnormal permanent enlargement of the air space distal to the terminal bronchioles
Accompanied by destruction of bronchioles

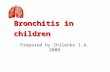
Muscle contraction
Mucosal oedema
Sticky mucusR2
R2
Bronchitis case
Normal

04/12/20236

04/12/2023
7
COPD CausesCOPD Causes
Infection Major contributing factor to the
aggravation and progression of COPDHeredity
-Antitrypsin (AAT) deficiency (produced by liver and found in lungs); accounts for < 1% of COPD cases Emphysema results from lysis of lung tissues by
proteolytic enzymes from neutrophils and macrophages
Infection Major contributing factor to the
aggravation and progression of COPDHeredity
-Antitrypsin (AAT) deficiency (produced by liver and found in lungs); accounts for < 1% of COPD cases Emphysema results from lysis of lung tissues by
proteolytic enzymes from neutrophils and macrophages

04/12/20238
TYPES OF BRONCHITIS:
CHRONIC BRONCHITIS ACUTE
BRONCHITIS

04/12/20239
Chronic bronchitis •Chronic bronchitis is
a chronic inflammation of the bronchi (medium-size airways) in the lungs.• It is generally considered one of the two forms of chronic obstructive pulmonary disease (COPD), the other being emphysema.•Chronic bronchitis It is defined clinically as a persistent cough that produces sputum and mucus, for at least three months per year in two consecutive years.

04/12/202310
Signs and symptomsBronchitis may be indicated by –
Cough (also known as a productive cough, i.E. One that produces sputum),
Shortness of breath and Wheezing.
Occasionally ,chest pains, fever, and fatigue or malaise may also occur.
Mucus is often green or yellowish green and also may be orange or pink, depending on the pathogen causing the inflammation.

04/12/202311
Causes: Tobacco smoking is the most common cause.Pneumoconiosis and long-term fume inhalation are other causes.Allergies can also cause mucus hypersecretion, thus leading to symptoms similar to asthma or bronchitis

04/12/202312
Pollution is a major cause of COPD

04/12/2023
13
Chronic Bronchitis PathophysiologyChronic Bronchitis Pathophysiology
Pathologic lung changes are: Hyperplasia of mucus-secreting glands
in trachea and bronchi Increase in goblet cells Disappearance of cilia Chronic inflammatory changes and
narrowing of small airways Altered function of alveolar macrophages
infections
Pathologic lung changes are: Hyperplasia of mucus-secreting glands
in trachea and bronchi Increase in goblet cells Disappearance of cilia Chronic inflammatory changes and
narrowing of small airways Altered function of alveolar macrophages
infections

04/12/2023
14
Chronic Bronchitis Pathophysiology
Chronic inflammation Primary pathologic mechanism causing changes
Narrow airway lumen and reduced airflow hyperplasia of mucus glandsInflammatory swellingExcess, thick mucus

04/12/2023
15
Chronic Bronchitis PathophysiologyChronic Bronchitis Pathophysiology
Greater resistance to airflow increases work of breathing
Hypoxemia and hypercapnia develop more frequently in chronic bronchitis than emphysema
Greater resistance to airflow increases work of breathing
Hypoxemia and hypercapnia develop more frequently in chronic bronchitis than emphysema

04/12/2023
16
Chronic Bronchitis PathophysiologyChronic Bronchitis Pathophysiology
Bronchioles are clogged with mucus and pose a physical barrier to ventilation
Hypoxemia and hypercapnia , lack of ventilation and O2 diffusion
Tendency to hypoventilate and retain CO2
Frequently patients require O2 both at rest and during exercise
Bronchioles are clogged with mucus and pose a physical barrier to ventilation
Hypoxemia and hypercapnia , lack of ventilation and O2 diffusion
Tendency to hypoventilate and retain CO2
Frequently patients require O2 both at rest and during exercise

04/12/2023
17
Chronic Bronchitis PathophysiologyChronic Bronchitis Pathophysiology
Cough is often ineffective to remove secretions because the person cannot breathe deeply enough to cause air flow distal to the secretions
Bronchospasm frequently develops
More common with history of smoking or asthma
Cough is often ineffective to remove secretions because the person cannot breathe deeply enough to cause air flow distal to the secretions
Bronchospasm frequently develops
More common with history of smoking or asthma

04/12/2023
18
Chronic BronchitisClinical Manifestations
Chronic BronchitisClinical Manifestations
Earliest symptoms:
Frequent, productive cough during winter
Frequent respiratory infections
Earliest symptoms:
Frequent, productive cough during winter
Frequent respiratory infections

04/12/2023
19
Chronic BronchitisClinical Manifestations
Chronic BronchitisClinical Manifestations
Bronchospasm at end of paroxysms of coughing
Cough History of smoking Normal weight or heavyset Ruddy (bluish-red) appearance d/t
polycythemia (increased Hgb d/t chronic hypoxemia)) cyanosis
Bronchospasm at end of paroxysms of coughing
Cough History of smoking Normal weight or heavyset Ruddy (bluish-red) appearance d/t
polycythemia (increased Hgb d/t chronic hypoxemia)) cyanosis

04/12/2023
20
Chronic Bronchitis Clinical ManifestationsChronic Bronchitis Clinical Manifestations
Hypoxemia and hypercapnia
Results from hypoventilation and airway resistance + problems with alveolar gas exchange
Hypoxemia and hypercapnia
Results from hypoventilation and airway resistance + problems with alveolar gas exchange

04/12/202321
Diagnosis:

04/12/202322
Diagnosis:
A variety of tests may be performed in patients presenting with cough and shortness of breath:•Pulmonary Function Tests (PFT) (or spirometry) •A chest X-ray • chest radiography.•A sputum sample showing neutrophil granulocytes (inflammatory white blood cells) and Check for pathogenic microorganisms such as Streptococcus spp.•A blood test would indicate inflammation •High Resolution Computed Tomography (HRCT)

04/12/2023
23
COPD ComplicationsCOPD Complications
Pulmonary hypertension (pulmonary vessel constriction alveolar hypoxia & acidosis)
Pneumonia
Acute Respiratory Failure
Pulmonary hypertension (pulmonary vessel constriction alveolar hypoxia & acidosis)
Pneumonia
Acute Respiratory Failure

04/12/202324
Acute bronchitis Acute bronchitis is an inflammation of the large bronchi (medium-size airways) in the lungs that is
Usually caused by viruses or bacteria and may last several days or weeks. Characteristic symptoms :• cough, • sputum (phlegm) production, • shortness of breath • wheezing related to the obstruction of the inflamed airways. Diagnosis is by clinical examination and sometimes microbiological examination of the phlegm. Treatment For acute bronchitis is typically symptomatic. As viruses cause most cases of acute bronchitis, antibiotics should not be used unless microscopic examination of gram-stained sputum reveals large numbers of bacteria.

04/12/202325
Anti-inflammatory drugs: steroids

04/12/202326
Membrane phospholipid
Arachidonic acid
Phospholipase A2
Leukotrienes:
B’constrictor
COX-I
PGs with gastric protective effects
COX-II
PGs with inflammatory effects

04/12/202327
Membrane phospholipid
Arachidonic acid
Phospholipase A2
Leukotrienes
COX-I
PGs with gastric protective effects
COX-II
PGs with inflammatory effects
Xste
roids

04/12/2023
28
Anti-inflammatory drugs: steroids
Life-saving.Take at least 12 h to work: so start early in
severe cases.Systemic steriods: acute severe asthma.Inhaled steroids: maintenance

04/12/2023
29
Anti-inflammatory drugs: steroids
Systemic steroid: intolerance ‘Cushingoid’ features Hypertension Salt and water retention Infection
Topical steroid Hoarseness

04/12/2023
30
Anti-inflammatory drugs: cromoglycate{mast cell stabilizer}
Prevent release of histamine from mast cells
By inhaler only.Useful maintenance therapy.No role in severe episodes.Few, if any, adverse effects.

04/12/202331
Anti-inflammatory drugs: leukotriene receptor antagonists
Arachidonic acid
Leukotrienes
PGs with gastric protective effects
PGs with inflammatory effectsx
Receptors

04/12/202332
• Leukotrienes cause capillary leakiness and bronchoconstriction
• Used orally for maintenance therapy (e.g. montelukast).
• Additive with inhaled steroids.
Anti-inflammatory drugs: leukotriene receptor antagonists

04/12/2023
33
Bronchodilators

04/12/2023
34
Catecholamines, receptors and effects.
receptors vasoconstrict1 receptors increase heart rate2 receptors vasodilate and bronchodliate
• Adrenaline , 1, 2.
• Noradrenaline , 1.• Dobutamine () 1.• Isoprenaline 1, 2.• Salbutamol (1)
2.
HR, BP, Bdilate
(HR), BPHR, BPHR, (? BP)(HR), Bdilate

04/12/2023
35
2-agonists.
Salbutamol, terbutilineInhalers (of various types).Maintenance:
Regularly in more severe casesAcute severe asthmaTachycardia and tremor

04/12/2023
36
Aminophylline
Is not a catecholamine, but has analgous effects.
Narrow therapeutic range.Given by mouth or by IV infusion.Toxic:
Fatal if injected too fast. Convulsions. Tachyarrhythmia

04/12/2023
37
Antimuscarinics
Atropine is the classical antimuscarinic, and this is b’dilator.
Atropine: too many diverse effects.Ipratropium.By inhaler.Add to salbutamol.Dry mouth.

04/12/202338
Related Documents



![Infectious Bronchitis Recovered]](https://static.cupdf.com/doc/110x72/5571f3ed49795947648ec5b0/infectious-bronchitis-recovered.jpg)