BRIEF COMMUNITY INTERVENTION PROGRAM REFERRAL (SCHOOLS) Name of person(s) making referral: Date: Student’s Name: DOB: ☐ Male ☐ Female School: Current Grade: School/Resources: ☐ IEP* ☐ 504 ☐ YIC ☐ Other Languages Spoken in the Home: ☐ English ☐ Spanish ☐ Other: Interpreter Needed: ☐ Yes ☐ No Parent/Guardian: Signed parental release Yes ☐ Home #: Work #: Address: Email: CURRENT SCHOOL PROGRAMMING: ☐ Truancy Mediation ☐ Social Skills Instruction ☐ Tutoring ☐ Functional Behavior Assessment ☐ Behavior Intervention Plan School Case Manager and Phone Number: Other Community Partner/Agency Worker (DCFS, System of Care, JJS, Juvenile Court, LMHA): Describe school behavior interventions that have been implemented (what worked or didn’t?): REASON FOR REFERRAL: Describe student strengths, likes, dislikes, interests and any positive school involvement (sports/clubs): Reason for referral (why does student require intervention) and why they are considered at-risk (enter reason below): Attendance (days missed): GPA: Office Disciplinary referrals: Out of school suspension (days): On track for graduation: ☐ Yes ☐ No Other applicable information: PLAN/GOAL FOR STUDENT: Describe the goal for the student: Positive behaviors to increase (e.g., problem solving, communication, social skills): Risk behaviors to decrease (e.g., noncompliance, emotional outbursts, class disruptions): *Service delivery decisions must be made through the IEP process

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
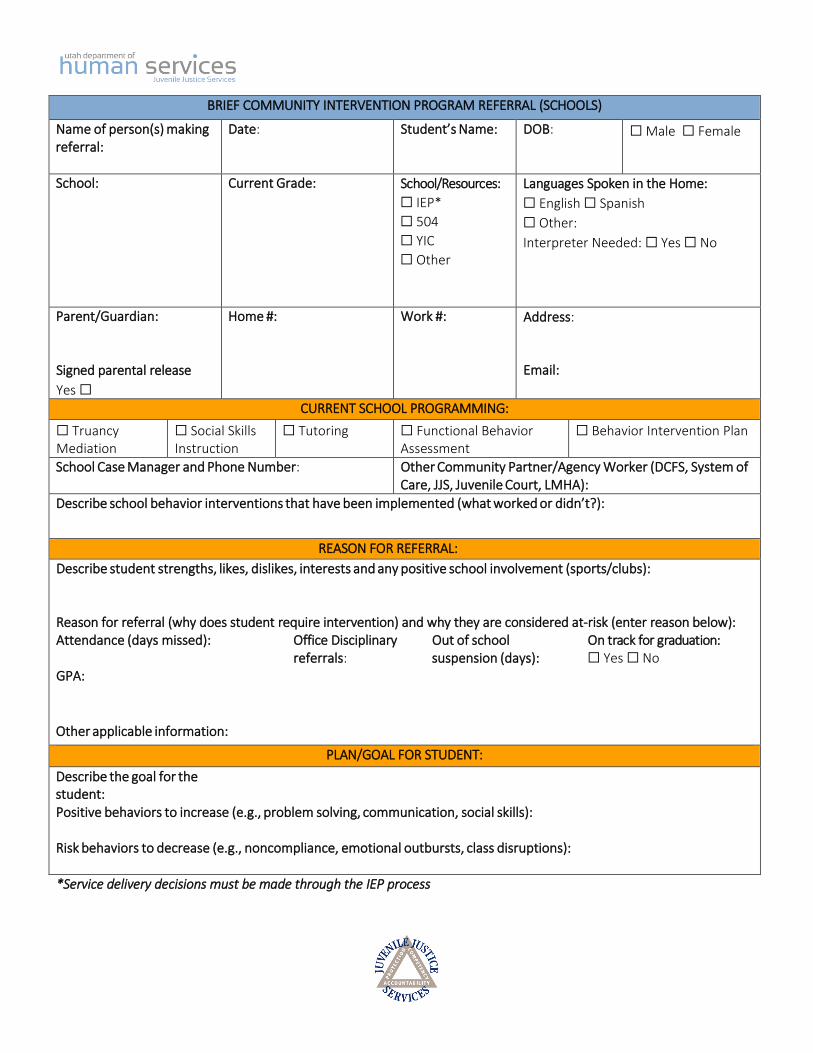
BRIEF COMMUNITY INTERVENTION PROGRAM REFERRAL (SCHOOLS)
Name of person(s) making referral:
Date: Student’s Name: DOB: ☐ Male ☐ Female
School: Current Grade: School/Resources:
☐ IEP*
☐ 504
☐ YIC
☐ Other
Languages Spoken in the Home:
☐ English ☐ Spanish
☐ Other:
Interpreter Needed: ☐ Yes ☐ No
Parent/Guardian:
Signed parental release
Yes ☐
Home #: Work #: Address:
Email:
CURRENT SCHOOL PROGRAMMING:
☐ Truancy Mediation
☐ Social Skills Instruction
☐ Tutoring ☐ Functional Behavior Assessment
☐ Behavior Intervention Plan
School Case Manager and Phone Number: Other Community Partner/Agency Worker (DCFS, System of Care, JJS, Juvenile Court, LMHA):
Describe school behavior interventions that have been implemented (what worked or didn’t?):
REASON FOR REFERRAL:
Describe student strengths, likes, dislikes, interests and any positive school involvement (sports/clubs):
Reason for referral (why does student require intervention) and why they are considered at-risk (enter reason below): Attendance (days missed):
GPA:
Office Disciplinary referrals:
Out of school suspension (days):
On track for graduation: ☐ Yes ☐ No
Other applicable information:
PLAN/GOAL FOR STUDENT:
Describe the goal for the student:Positive behaviors to increase (e.g., problem solving, communication, social skills):
Risk behaviors to decrease (e.g., noncompliance, emotional outbursts, class disruptions):
*Service delivery decisions must be made through the IEP process
Related Documents











