Scripps Clinic/Scripps Green Hospital Grand Rounds Wednesday, Sept. 2, 2009 www.scripps.org/conferenceservices Breast imaging Update 2009: Incorporating functional breast imaging Marie Tartar, M.D. Scripps Green Hospital, La Jolla CA Director, Advanced Breast Imaging Disclosures Site principle investigator: Prospective Multicenter Study of the Role of PEM in Pre- Surgical Planning for Breast Cancer, 2006-08 Sponsored by Naviscan PET Systems, San Diego Courtesy Naviscan PET Systems Courtesy Dilon BSGI vs. PEM comparison 48 y.o. female with new dx at OSF of Lt UOQ IDC (1 cm by US) 40 y.o. asx female with extensive suspicious Lt lateral microcalcifications on baseline mammo Staging: whole body PET

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
Breast imaging Update 2009:Incorporating functional breast imaging
Marie Tartar, M.D.Scripps Green Hospital, La Jolla CADirector, Advanced Breast Imaging
Disclosures
Site principle investigator: Prospective Multicenter Study of the Role of PEM in Pre-Surgical Planning for Breast Cancer, 2006-08 Sponsored by Naviscan
PET Systems, San Diego
Courtesy NaviscanPET Systems
Courtesy Dilon
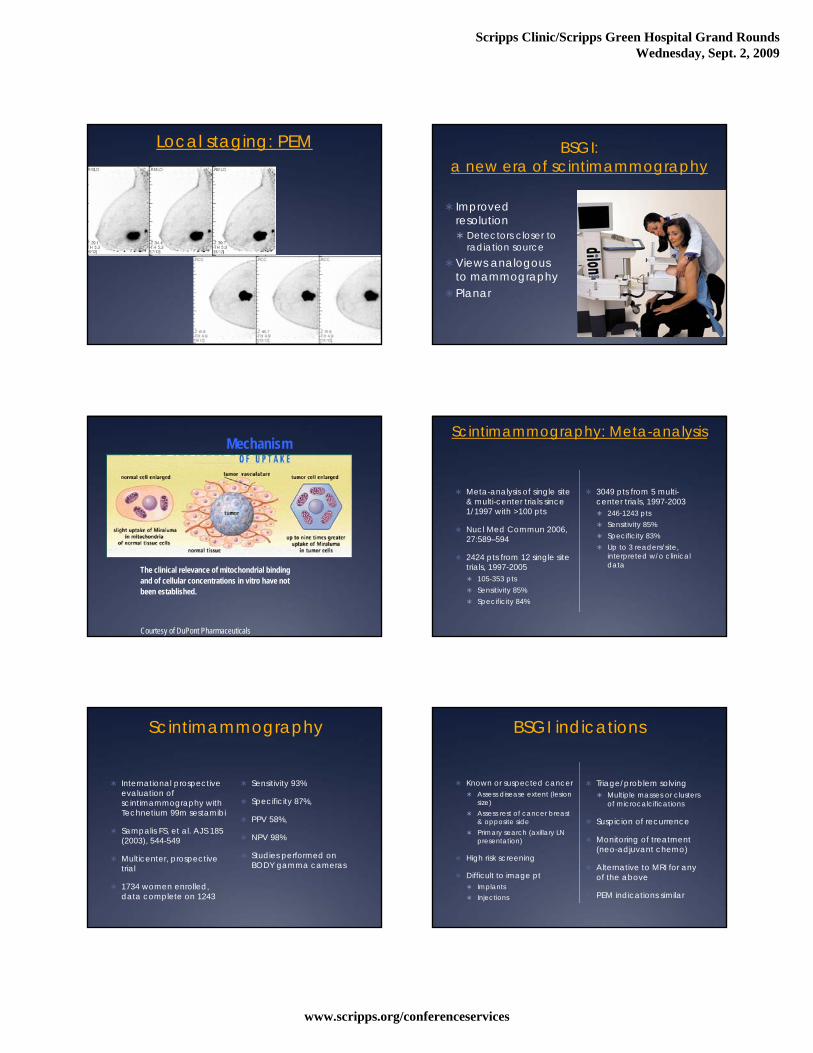
BSGI vs. PEM comparison 48 y.o. female with new dx
at OSF of Lt UOQ IDC (1 cm by US)
40 y.o. asx female with extensive suspicious Lt lateral microcalcificationson baseline mammo
Staging: whole body PET
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
Local staging: PEM BSGI: a new era of scintimammography
Improved resolution Detectors closer to
radiation sourceViews analogous
to mammographyPlanar
The clinical relevance of mitochondrial bindingand of cellular concentrations in vitro have notbeen established.
Courtesy of DuPont Pharmaceuticals
MechanismScintimammography: Meta-analysis
Meta-analysis of single site & multi-center trials since 1/1997 with >100 pts
Nucl Med Commun 2006, 27:589–594
2424 pts from 12 single site trials, 1997-2005 105-353 pts Sensitivity 85% Specificity 84%
3049 pts from 5 multi-center trials, 1997-2003 246-1243 pts Sensitivity 85% Specificity 83% Up to 3 readers/site,
interpreted w/o clinical data
Scintimammography
International prospective evaluation of scintimammography with Technetium 99m sestamibi
Sampalis FS, et al. AJS 185 (2003), 544-549
Multicenter, prospective trial
1734 women enrolled, data complete on 1243
Sensitivity 93%
Specificity 87%,
PPV 58%,
NPV 98%
Studies performed on BODY gamma cameras
BSGI indications
Known or suspected cancer Assess disease extent (lesion
size) Assess rest of cancer breast
& opposite side Primary search (axillary LN
presentation)
High risk screening
Difficult to image pt Implants Injections
Triage/problem solving Multiple masses or clusters
of microcalcifications
Suspicion of recurrence
Monitoring of treatment (neo-adjuvant chemo)
Alternative to MRI for any of the above
PEM indications similar
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
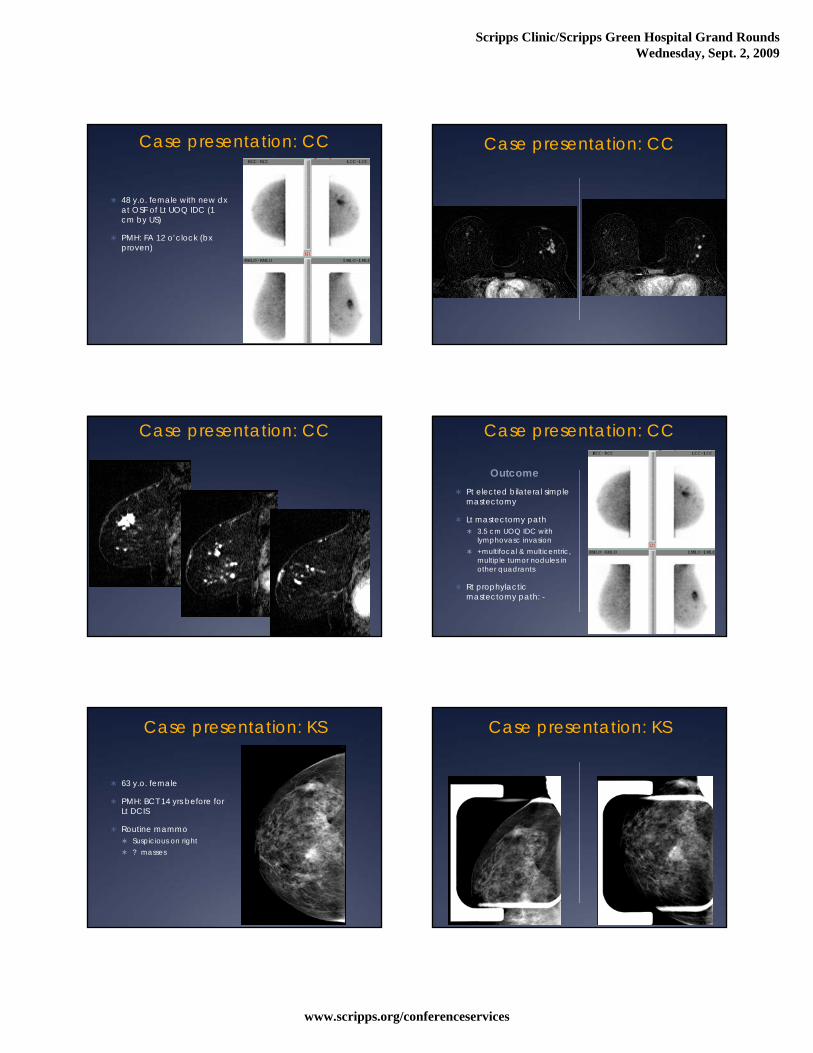
Case presentation: CC
48 y.o. female with new dxat OSF of Lt UOQ IDC (1 cm by US)
PMH: FA 12 o’clock (bxproven)
Case presentation: CC
Case presentation: CC Case presentation: CC
Outcome Pt elected bilateral simple
mastectomy
Lt mastectomy path 3.5 cm UOQ IDC with
lymphovasc invasion +multifocal & multicentric,
multiple tumor nodules in other quadrants
Rt prophylactic mastectomy path: -
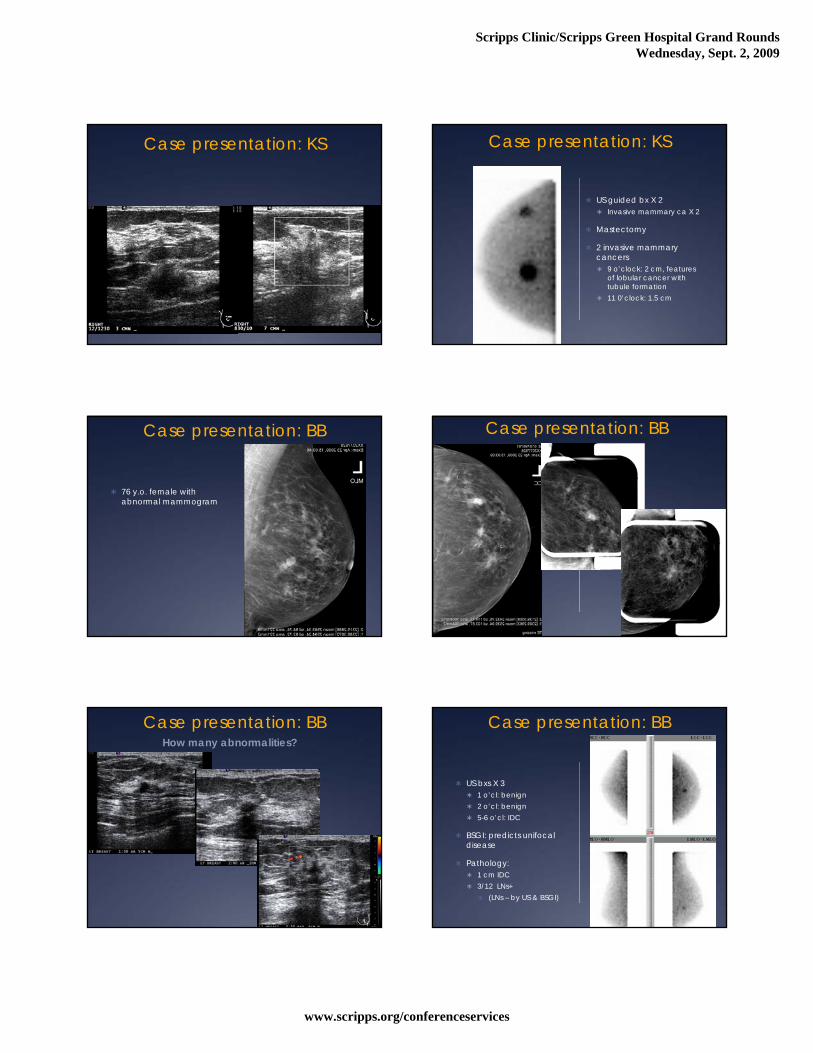
Case presentation: KS
63 y.o. female
PMH: BCT 14 yrs before for Lt DCIS
Routine mammo Suspicious on right ? masses
Case presentation: KS
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
Case presentation: KS Case presentation: KS
US guided bx X 2 Invasive mammary ca X 2
Mastectomy
2 invasive mammary cancers 9 o’clock: 2 cm, features
of lobular cancer with tubule formation
11 0’clock: 1.5 cm
Case presentation: BB
76 y.o. female with abnormal mammogram
Case presentation: BB
Case presentation: BBHow many abnormalities?
Case presentation: BB
US bxs X 3 1 o’cl: benign 2 o’cl: benign 5-6 o’cl: IDC
BSGI: predicts unifocaldisease
Pathology: 1 cm IDC 3/12 LNs+
(LNs – by US & BSGI)
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
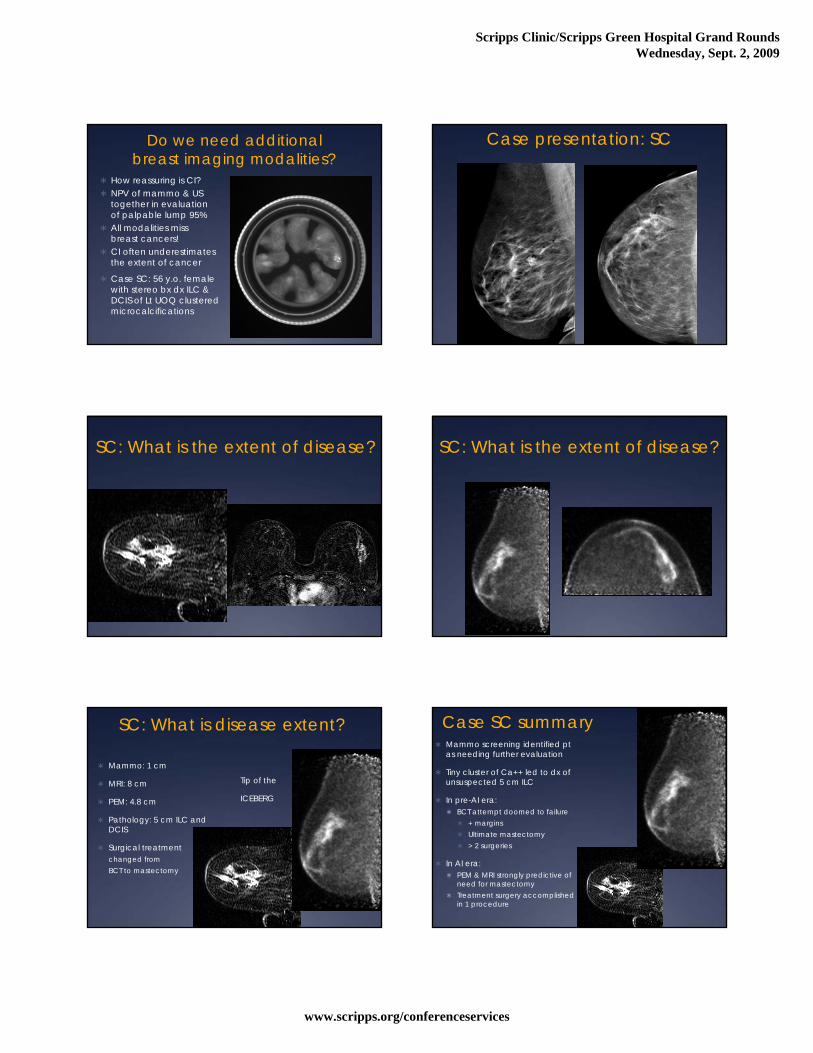
Do we need additional breast imaging modalities?
How reassuring is CI? NPV of mammo & US
together in evaluation of palpable lump 95%
All modalities miss breast cancers!
CI often underestimates the extent of cancer
Case SC: 56 y.o. female with stereo bx dx ILC & DCIS of Lt UOQ clustered microcalcifications
Case presentation: SC
SC: What is the extent of disease? SC: What is the extent of disease?
SC: What is disease extent?
Mammo: 1 cm
MRI: 8 cm
PEM: 4.8 cm
Pathology: 5 cm ILC and DCIS
Surgical treatment changed from BCT to mastectomy
Tip of the
ICEBERG
Case SC summary Mammo screening identified pt
as needing further evaluation
Tiny cluster of Ca++ led to dx of unsuspected 5 cm ILC
In pre-AI era: BCT attempt doomed to failure
+ margins Ultimate mastectomy > 2 surgeries
In AI era: PEM & MRI strongly predictive of
need for mastectomy Treatment surgery accomplished
in 1 procedure
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
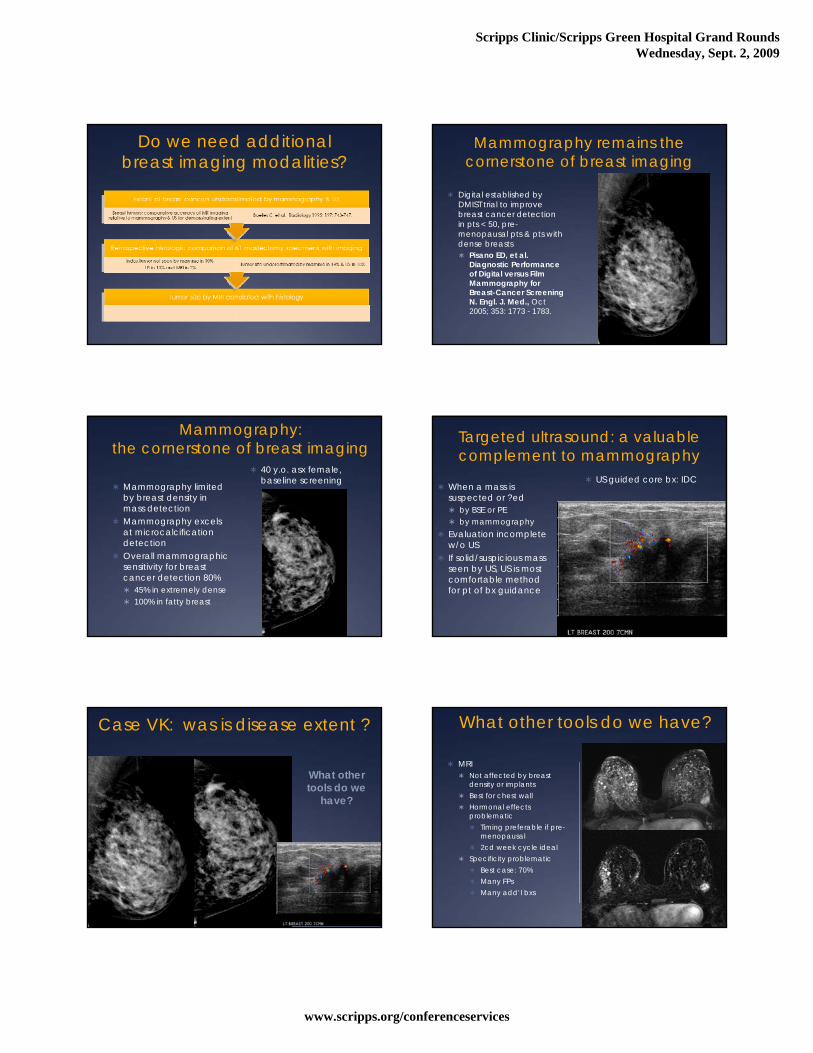
Do we need additional breast imaging modalities?
Mammography remains the cornerstone of breast imaging
Digital established by DMIST trial to improve breast cancer detection in pts < 50, pre-menopausal pts & pts with dense breasts Pisano ED, et al.
Diagnostic Performance of Digital versus Film Mammography for Breast-Cancer Screening N. Engl. J. Med., Oct 2005; 353: 1773 - 1783.
Mammography: the cornerstone of breast imaging
Mammography limited by breast density in mass detection
Mammography excels at microcalcificationdetection
Overall mammographic sensitivity for breast cancer detection 80% 45% in extremely dense 100% in fatty breast
40 y.o. asx female, baseline screening
Targeted ultrasound: a valuable complement to mammography
When a mass is suspected or ?ed by BSE or PE by mammography
Evaluation incomplete w/o US
If solid/suspicious mass seen by US, US is most comfortable method for pt of bx guidance
US guided core bx: IDC
Case VK: was is disease extent ?
What other tools do we
have?
What other tools do we have?
MRI Not affected by breast
density or implants Best for chest wall Hormonal effects
problematic Timing preferable if pre-
menopausal 2cd week cycle ideal
Specificity problematic Best case: 70% Many FPs Many add’l bxs
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
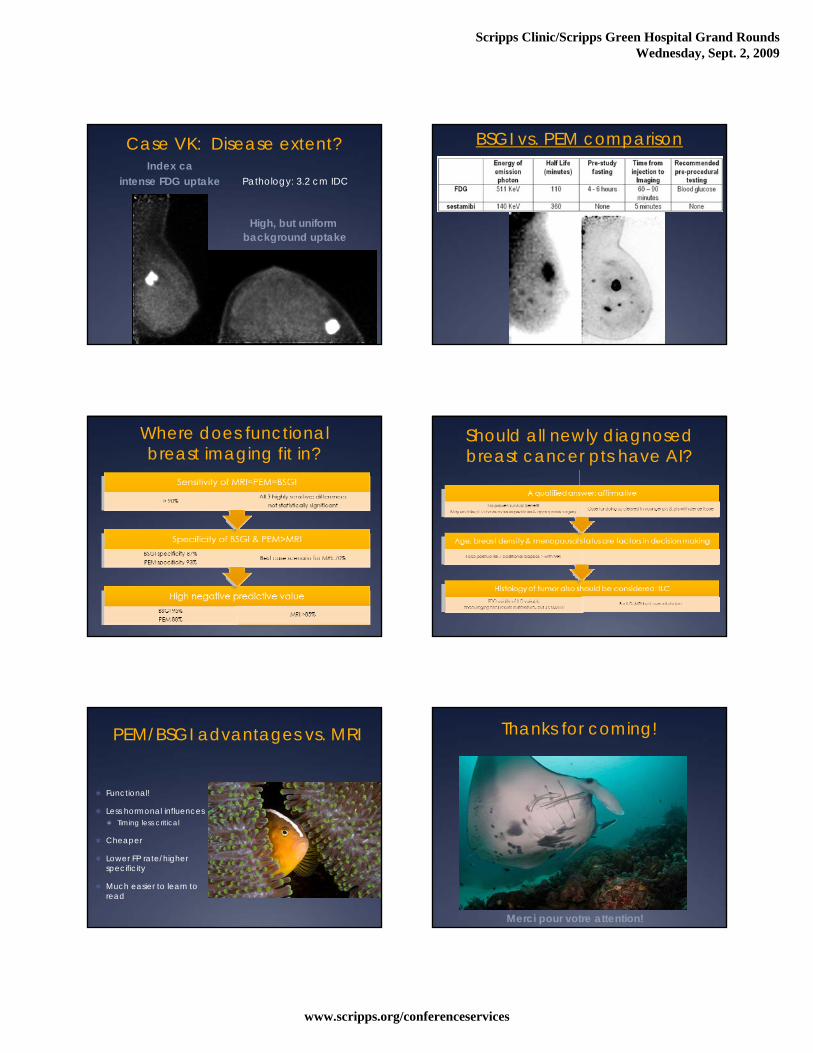
Case VK: Disease extent?Index ca
intense FDG uptake
High, but uniformbackground uptake
Pathology: 3.2 cm IDC
BSGI vs. PEM comparison
Where does functional breast imaging fit in?
Should all newly diagnosed breast cancer pts have AI?
PEM/BSGI advantages vs. MRI
Functional!
Less hormonal influences Timing less critical
Cheaper
Lower FP rate/higher specificity
Much easier to learn to read
Thanks for coming!
Merci pour votre attention!
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
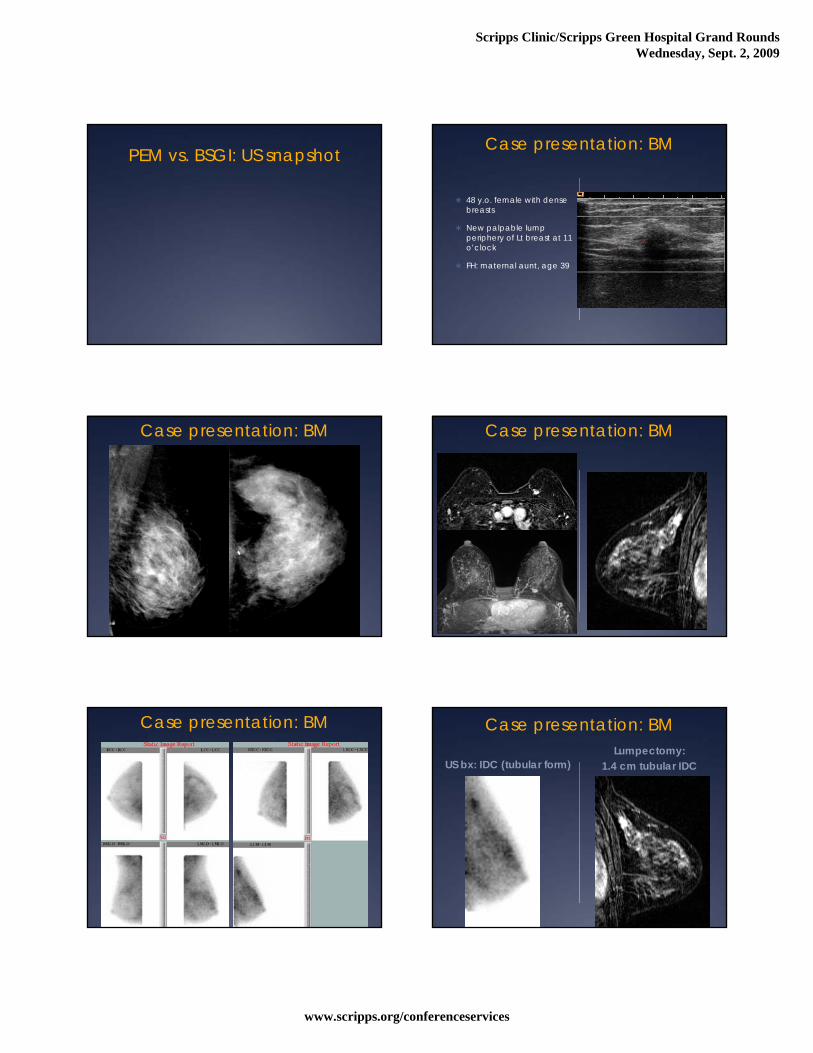
PEM vs. BSGI: US snapshot Case presentation: BM
48 y.o. female with dense breasts
New palpable lump periphery of Lt breast at 11 o’clock
FH: maternal aunt, age 39
Case presentation: BM Case presentation: BM
Case presentation: BM Case presentation: BM
US bx: IDC (tubular form)Lumpectomy:
1.4 cm tubular IDC
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
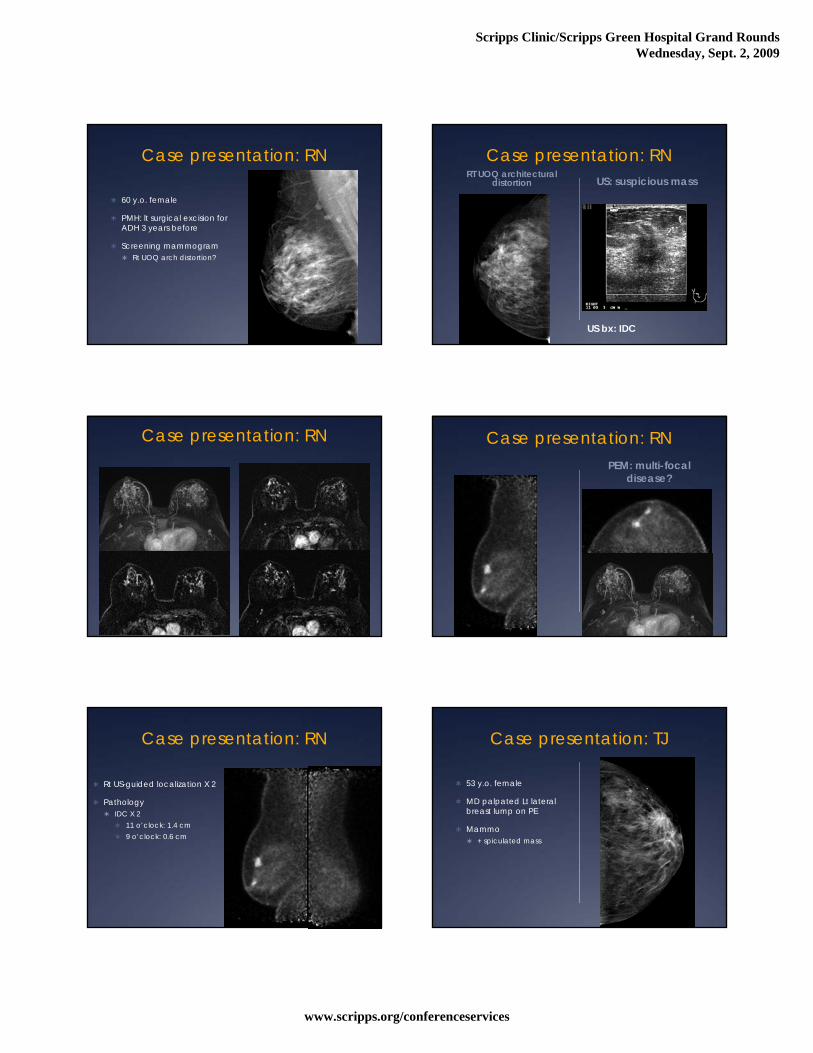
Case presentation: RN
60 y.o. female
PMH: lt surgical excision for ADH 3 years before
Screening mammogram Rt UOQ arch distortion?
Case presentation: RNRT UOQ architectural
distortion US: suspicious mass
US bx: IDC
Case presentation: RN
US bx: IDC
Case presentation: RNPEM: multi-focal
disease?
Case presentation: RN
Rt US-guided localization X 2
Pathology IDC X 2
11 o’clock: 1.4 cm 9 o’clock: 0.6 cm
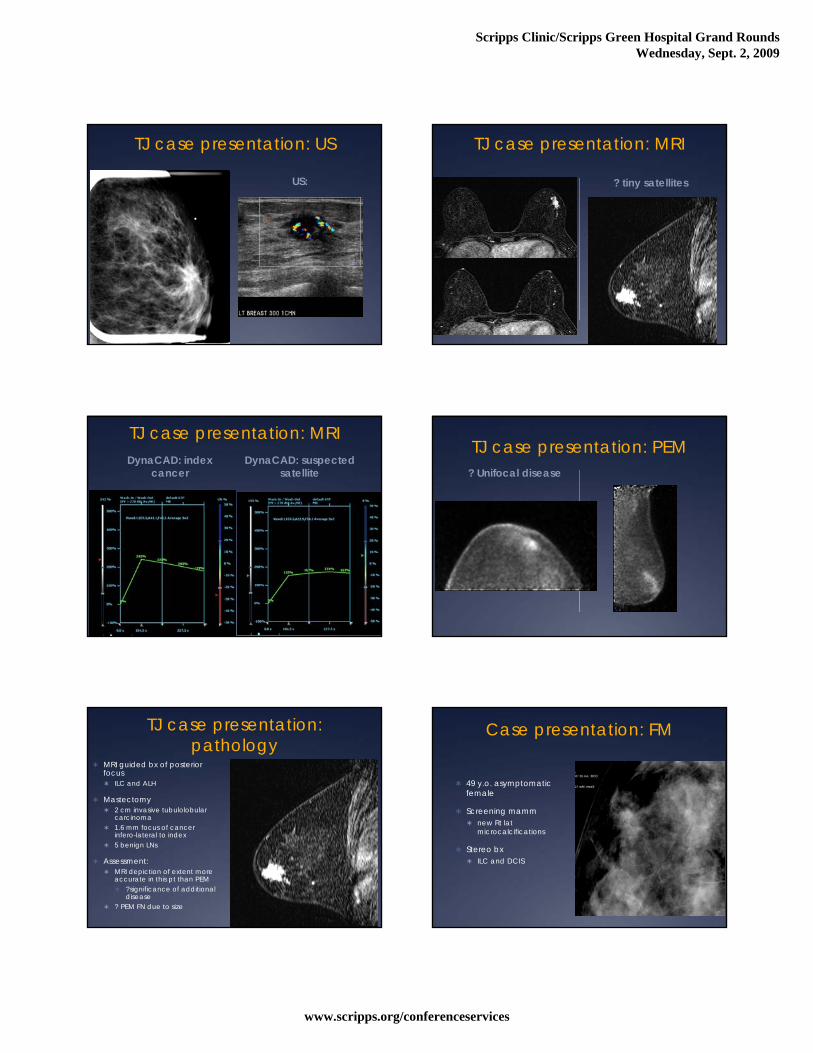
Case presentation: TJ
53 y.o. female
MD palpated Lt lateral breast lump on PE
Mammo + spiculated mass
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
TJ case presentation: US
US:
TJ case presentation: MRI
? tiny satellites
TJ case presentation: MRIDynaCAD: index
cancerDynaCAD: suspected
satellite
TJ case presentation: PEM? Unifocal disease
TJ case presentation: pathology
MRI guided bx of posterior focus ILC and ALH
Mastectomy 2 cm invasive tubulolobular
carcinoma 1.6 mm focus of cancer
infero-lateral to index 5 benign LNs
Assessment: MRI depiction of extent more
accurate in this pt than PEM ?significance of additional
disease ? PEM FN due to size
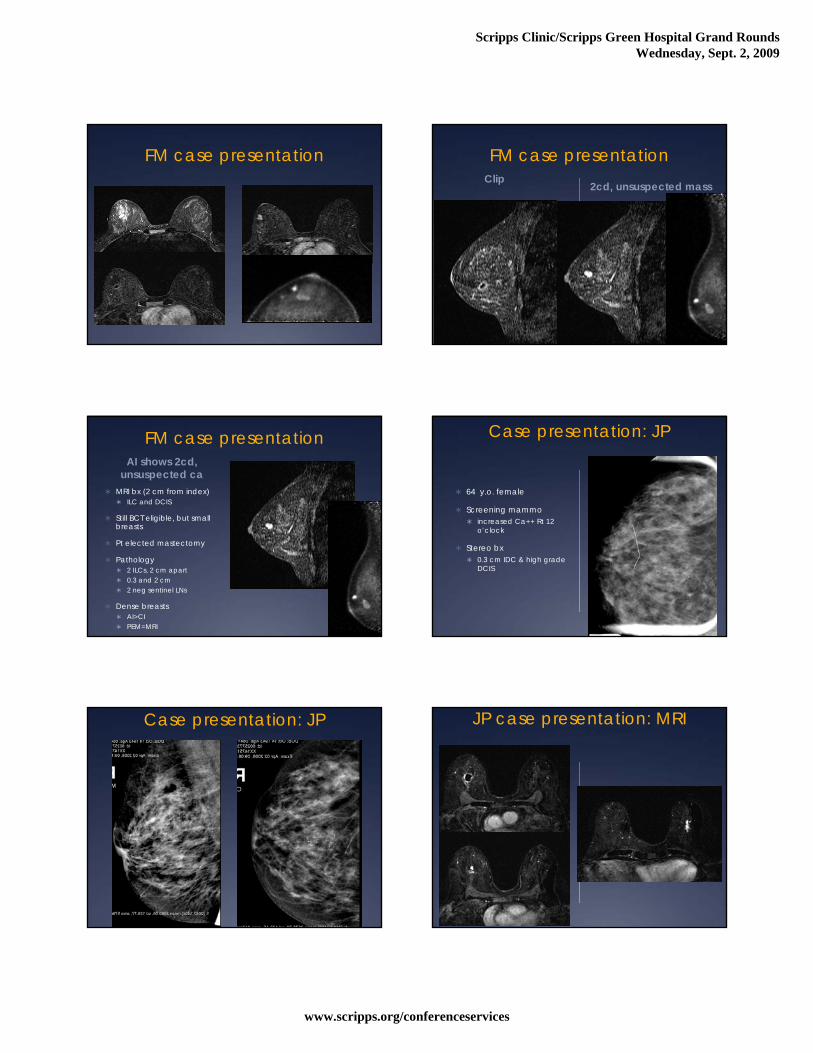
Case presentation: FM
49 y.o. asymptomatic female
Screening mamm new Rt lat
microcalcifications
Stereo bx ILC and DCIS
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
FM case presentation FM case presentationClip
2cd, unsuspected mass
FM case presentationAI shows 2cd,
unsuspected ca MRI bx (2 cm from index)
ILC and DCIS
Still BCT eligible, but small breasts
Pt elected mastectomy
Pathology 2 ILCs, 2 cm apart 0.3 and 2 cm 2 neg sentinel LNs
Dense breasts AI>CI PEM=MRI
Case presentation: JP
64 y.o. female
Screening mammo increased Ca++ Rt 12
o’clock
Stereo bx 0.3 cm IDC & high grade
DCIS
Case presentation: JP JP case presentation: MRI
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
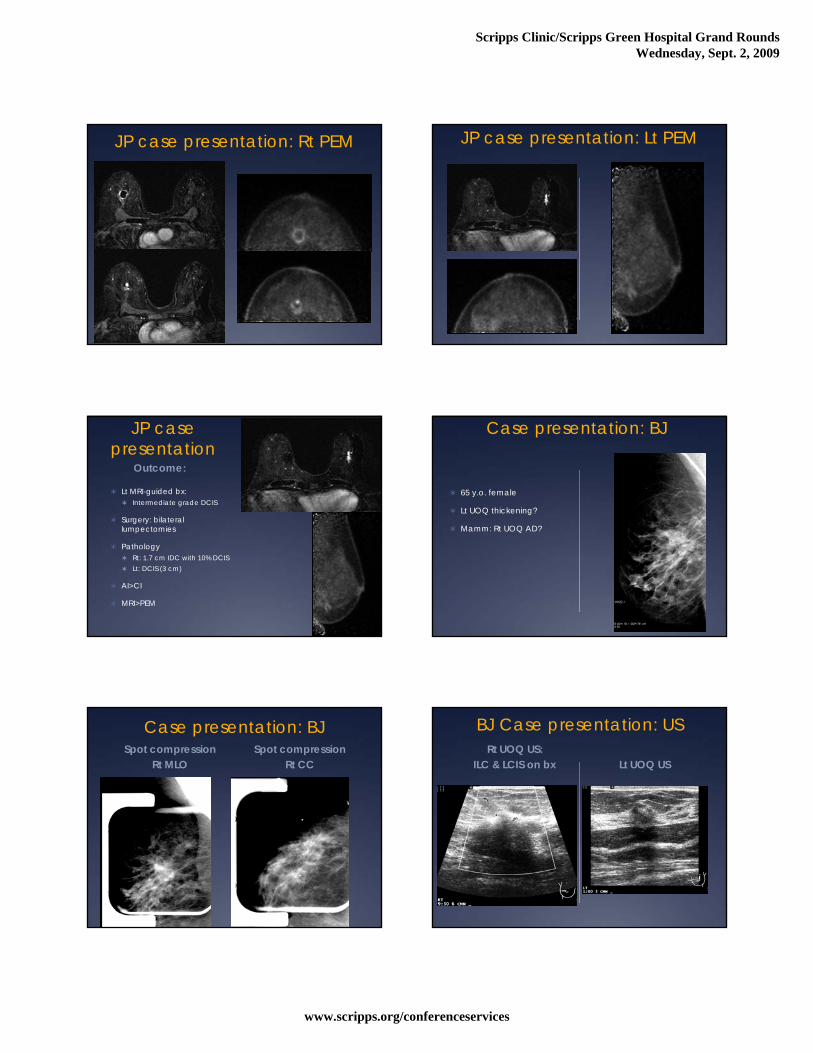
JP case presentation: Rt PEM JP case presentation: Lt PEM
JP case presentation
Outcome:
Lt MRI-guided bx: Intermediate grade DCIS
Surgery: bilateral lumpectomies
Pathology Rt: 1.7 cm IDC with 10% DCIS Lt: DCIS (3 cm)
AI>CI
MRI>PEM
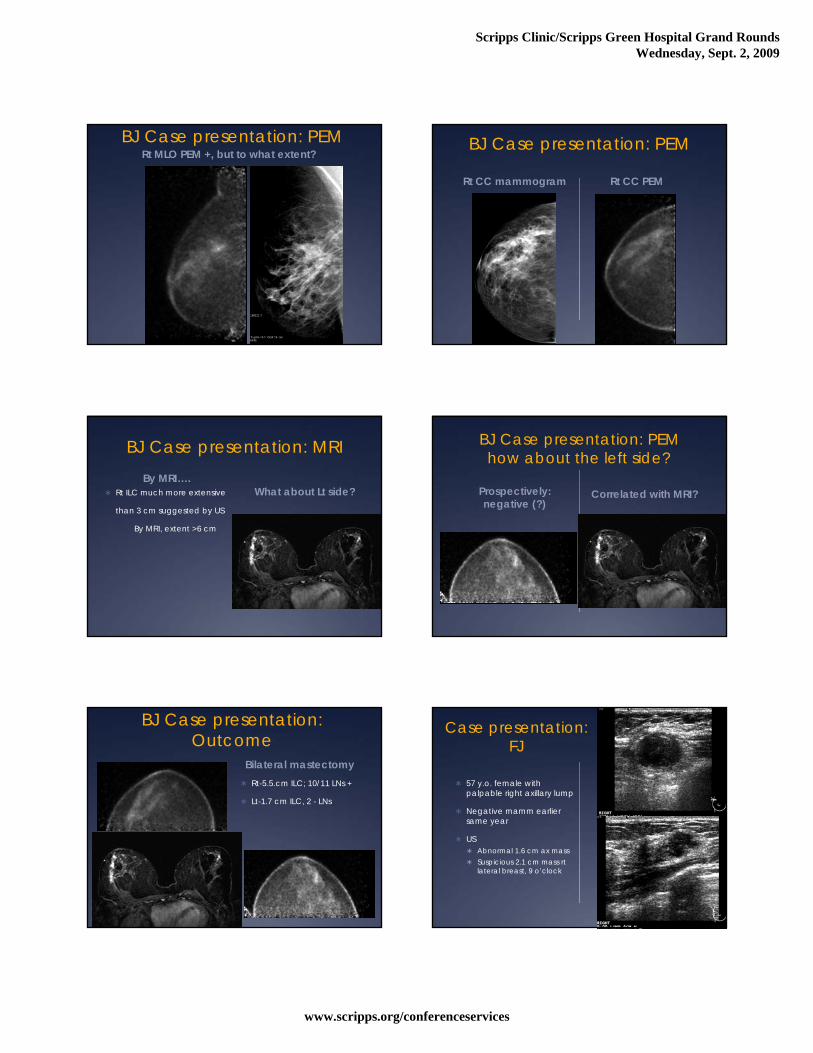
Case presentation: BJ
65 y.o. female
Lt UOQ thickening?
Mamm: Rt UOQ AD?
Case presentation: BJSpot compression
Rt MLOSpot compression
Rt CC
BJ Case presentation: USRt UOQ US:
ILC & LCIS on bx Lt UOQ US
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
BJ Case presentation: PEMRt MLO PEM +, but to what extent?
BJ Case presentation: PEM
Rt CC mammogram Rt CC PEM
BJ Case presentation: MRIBy MRI….
What about Lt side? Rt ILC much more extensive
than 3 cm suggested by US
By MRI, extent >6 cm
BJ Case presentation: PEMhow about the left side?
Prospectively: negative (?)
Correlated with MRI?
BJ Case presentation: Outcome
Bilateral mastectomy Rt-5.5.cm ILC; 10/11 LNs +
Lt-1.7 cm ILC, 2 - LNs
Case presentation: FJ
57 y.o. female with palpable right axillary lump
Negative mamm earlier same year
US Abnormal 1.6 cm ax mass Suspicious 2.1 cm mass rt
lateral breast, 9 o’clock
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
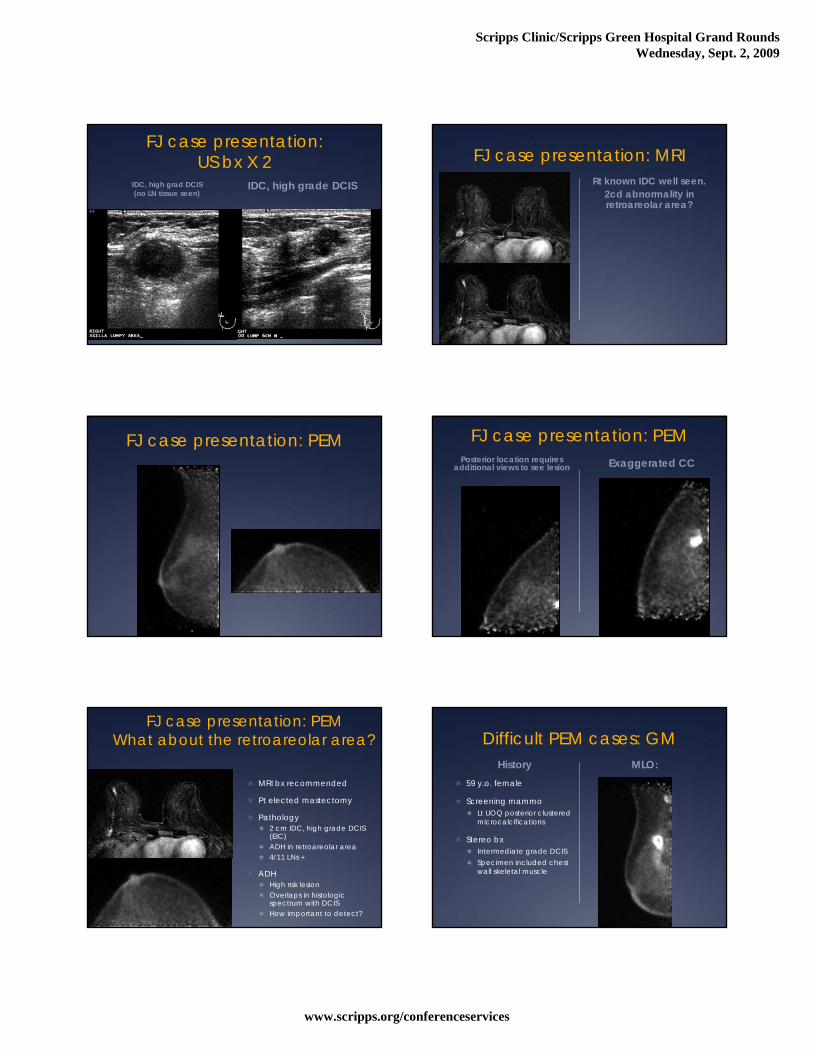
FJ case presentation: US bx X 2
IDC, high grad DCIS (no LN tissue seen)
IDC, high grade DCIS
FJ case presentation: MRIRt known IDC well seen.
2cd abnormality in retroareolar area?
FJ case presentation: PEM FJ case presentation: PEMPosterior location requires
additional views to see lesion Exaggerated CC
FJ case presentation: PEMWhat about the retroareolar area?
MRI bx recommended
Pt elected mastectomy
Pathology 2 cm IDC, high grade DCIS
(EIC) ADH in retroareolar area 4/11 LNs +
ADH High risk lesion Overlaps in histologic
spectrum with DCIS How important to detect?
Difficult PEM cases: GMHistory
59 y.o. female
Screening mammo Lt UOQ posterior clustered
microcalcifications
Stereo bx Intermediate grade DCIS Specimen included chest
wall skeletal muscle
MLO:
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
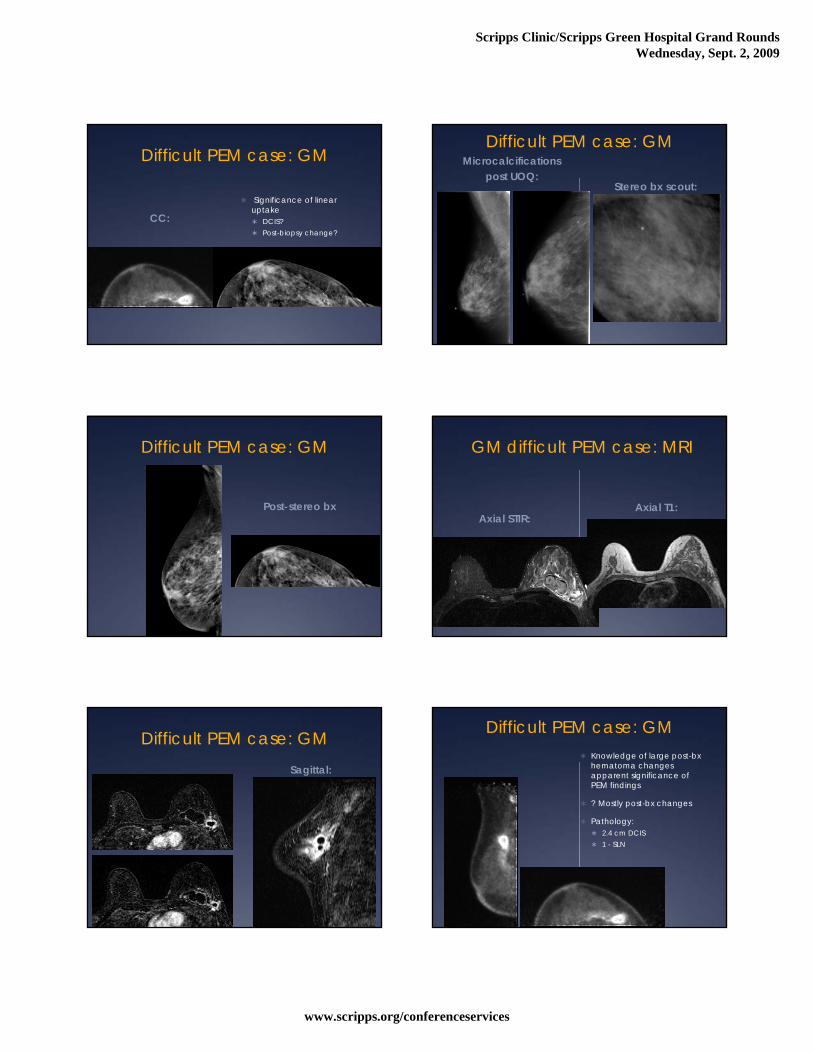
Difficult PEM case: GM
CC: Significance of linear
uptake DCIS? Post-biopsy change?
Difficult PEM case: GMMicrocalcifications
post UOQ:Stereo bx scout:
Difficult PEM case: GM
Post-stereo bx
GM difficult PEM case: MRI
Axial STIR:Axial T1:
Difficult PEM case: GMSagittal:
Difficult PEM case: GM Knowledge of large post-bx
hematoma changes apparent significance of PEM findings
? Mostly post-bx changes
Pathology: 2.4 cm DCIS 1 - SLN
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
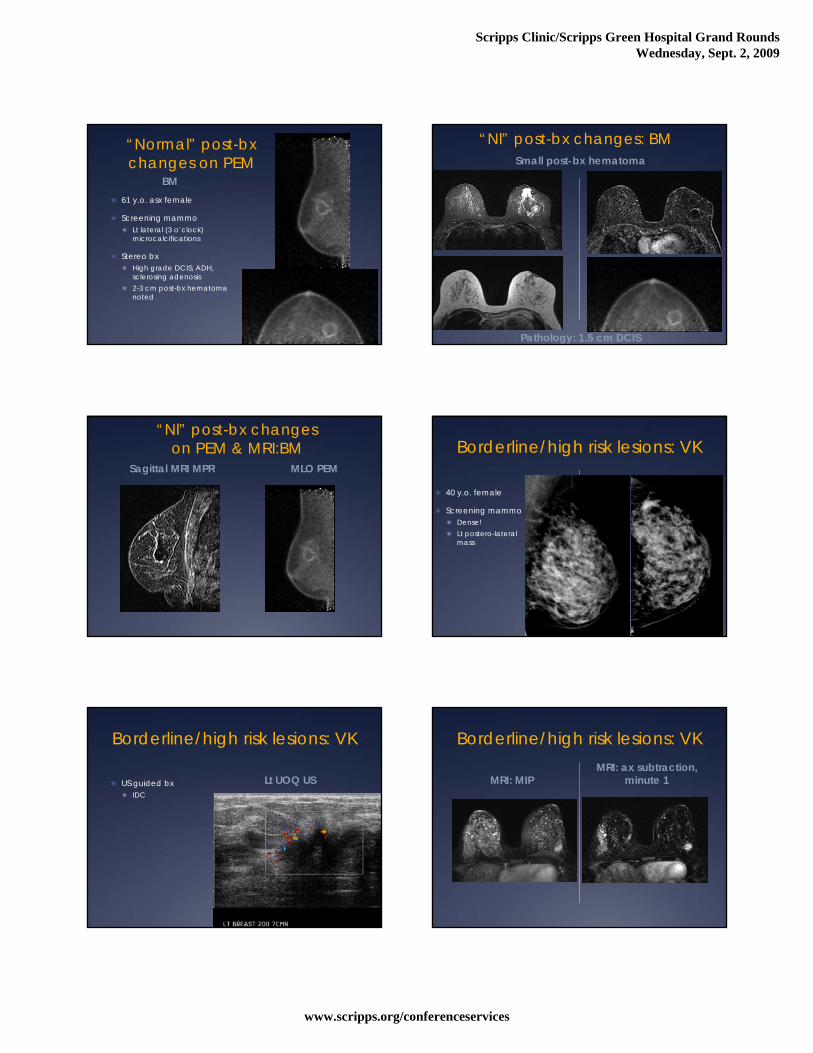
“Normal” post-bx changes on PEM
BM 61 y.o. asx female
Screening mammo Lt lateral (3 o’clock)
microcalcifications
Stereo bx High grade DCIS, ADH,
sclerosing adenosis 2-3 cm post-bx hematoma
noted
“Nl” post-bx changes: BM
Pathology: 1.5 cm DCIS
Small post-bx hematoma
“Nl” post-bx changes on PEM & MRI:BM
Sagittal MRI MPR MLO PEM
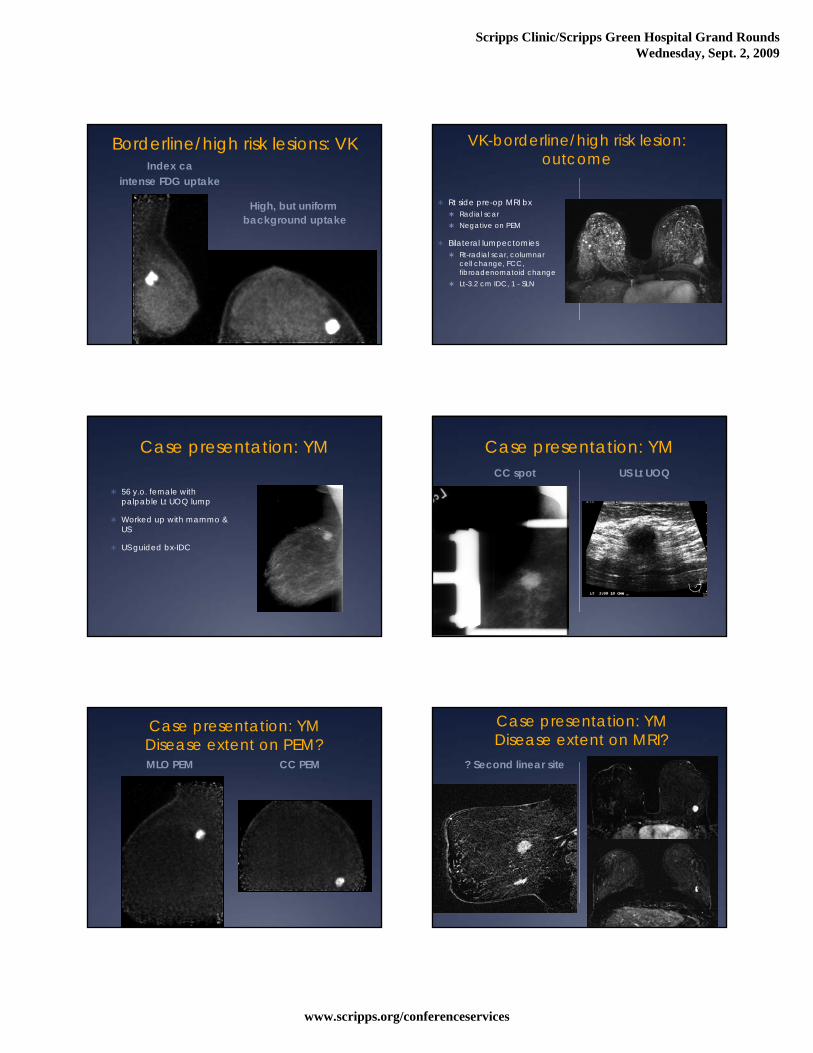
Borderline/high risk lesions: VK
40 y.o. female
Screening mammo Dense! Lt postero-lateral
mass
Borderline/high risk lesions: VK
US guided bx IDC
Lt UOQ US
Borderline/high risk lesions: VK
MRI: MIPMRI: ax subtraction,
minute 1
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
Borderline/high risk lesions: VKIndex ca
intense FDG uptake
High, but uniformbackground uptake
VK-borderline/high risk lesion:outcome
Rt side pre-op MRI bx Radial scar Negative on PEM
Bilateral lumpectomies Rt-radial scar, columnar
cell change, FCC, fibroadenomatoid change
Lt-3.2 cm IDC, 1 - SLN
Case presentation: YM
56 y.o. female with palpable Lt UOQ lump
Worked up with mammo & US
US guided bx-IDC
Case presentation: YMCC spot US Lt UOQ
Case presentation: YMDisease extent on PEM?MLO PEM CC PEM
Case presentation: YMDisease extent on MRI?
? Second linear site
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
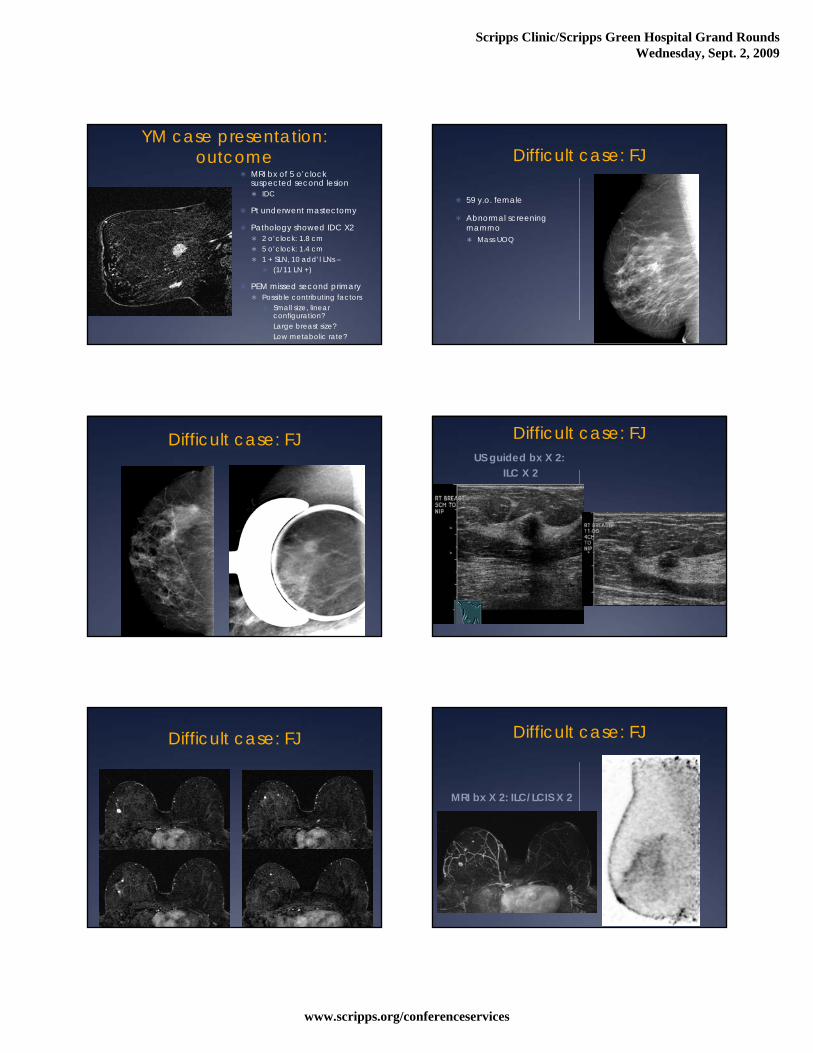
YM case presentation: outcome
MRI bx of 5 o’clock suspected second lesion IDC
Pt underwent mastectomy
Pathology showed IDC X2 2 o’clock: 1.8 cm 5 o’clock: 1.4 cm 1 + SLN, 10 add’l LNs –
(1/11 LN +)
PEM missed second primary Possible contributing factors
Small size, linear configuration?
Large breast size? Low metabolic rate?
Difficult case: FJ
59 y.o. female
Abnormal screening mammo Mass UOQ
Difficult case: FJ Difficult case: FJUS guided bx X 2:
ILC X 2
Difficult case: FJ Difficult case: FJ
MRI bx X 2: ILC/LCIS X 2
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
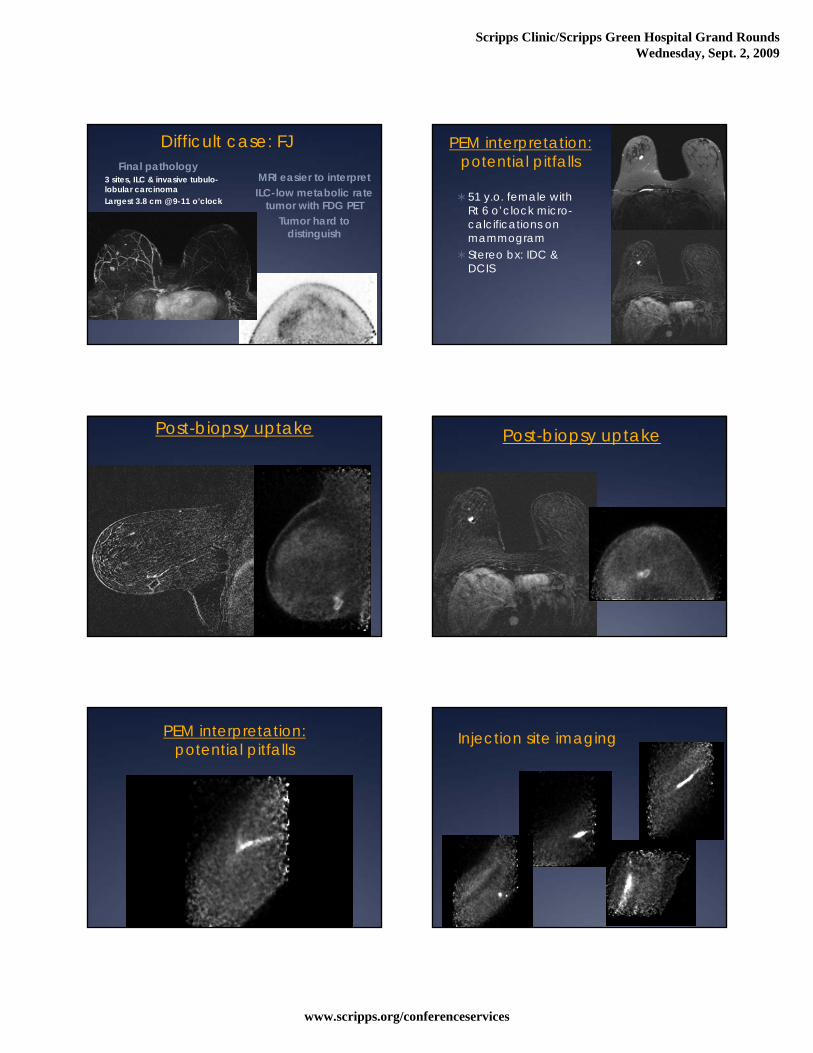
Difficult case: FJ
MRI easier to interpretILC-low metabolic rate
tumor with FDG PETTumor hard to
distinguish
Final pathology3 sites, ILC & invasive tubulo-lobular carcinomaLargest 3.8 cm @ 9-11 o’clock
PEM interpretation:potential pitfalls
51 y.o. female with Rt 6 o’clock micro-calcifications on mammogram
Stereo bx: IDC & DCIS
Post-biopsy uptake Post-biopsy uptake
PEM interpretation:potential pitfalls
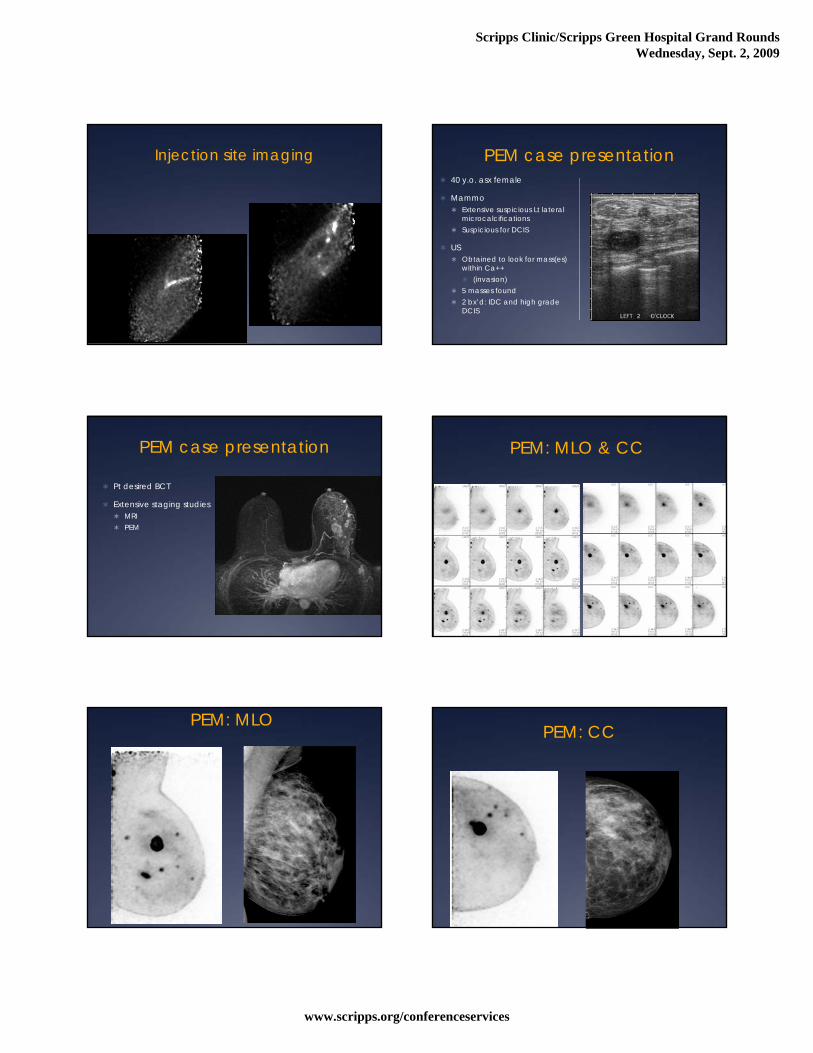
Injection site imaging
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
Injection site imaging PEM case presentation 40 y.o. asx female
Mammo Extensive suspicious Lt lateral
microcalcifications Suspicious for DCIS
US Obtained to look for mass(es)
within Ca++ (invasion)
5 masses found 2 bx’d: IDC and high grade
DCIS
PEM case presentation
Pt desired BCT
Extensive staging studies MRI PEM
PEM: MLO & CC
PEM: MLOPEM: CC
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
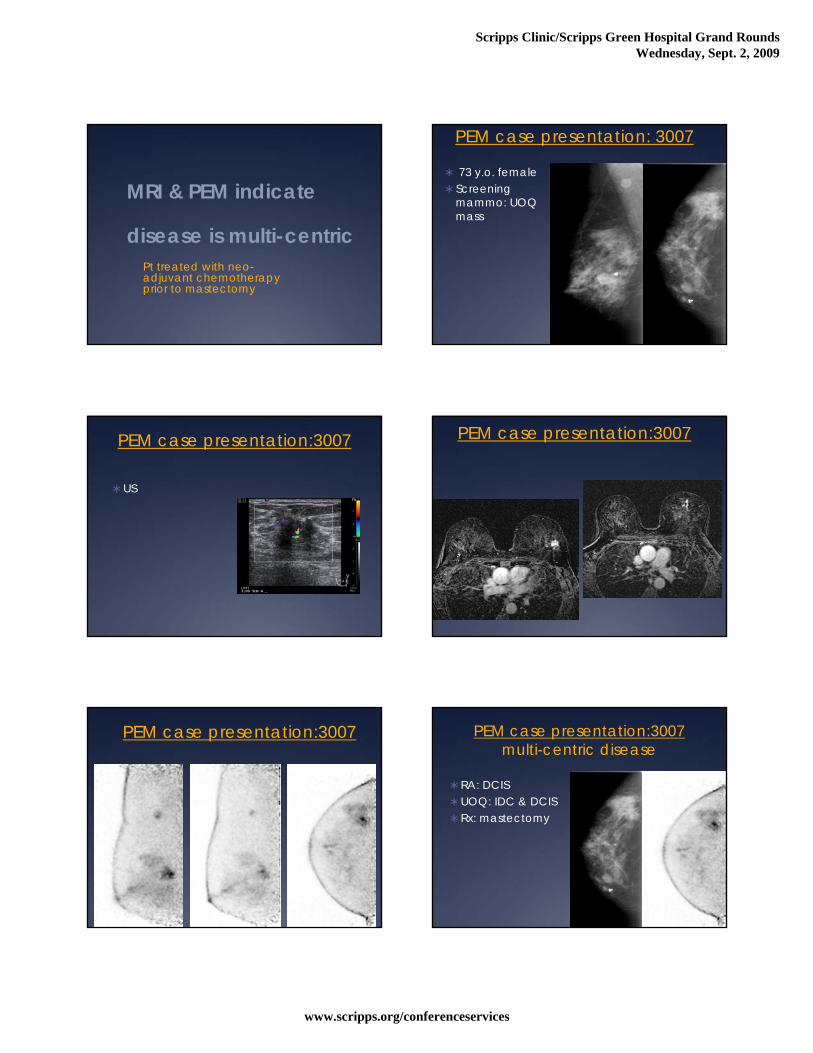
MRI & PEM indicate
disease is multi-centricPt treated with neo-adjuvant chemotherapy prior to mastectomy
PEM case presentation: 3007
73 y.o. female Screening
mammo: UOQ mass
PEM case presentation:3007
US
PEM case presentation:3007
PEM case presentation:3007 PEM case presentation:3007multi-centric disease
RA: DCISUOQ: IDC & DCISRx: mastectomy
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
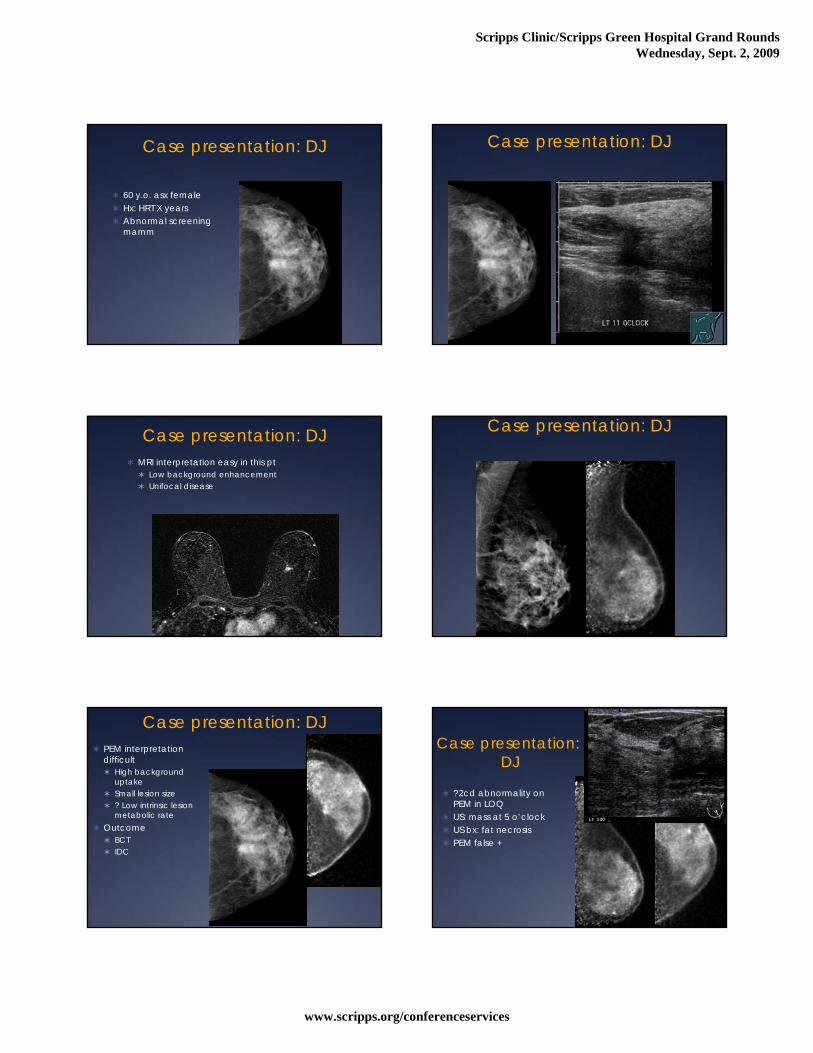
Case presentation: DJ
60 y.o. asx female Hx: HRT X years Abnormal screening
mamm
Case presentation: DJ
Case presentation: DJ MRI interpretation easy in this pt
Low background enhancement Unifocal disease
Case presentation: DJ
Case presentation: DJ PEM interpretation
difficult High background
uptake Small lesion size ? Low intrinsic lesion
metabolic rate Outcome
BCT IDC
Case presentation:DJ
?2cd abnormality on PEM in LOQ
US: mass at 5 o’clock US bx: fat necrosis PEM false +
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
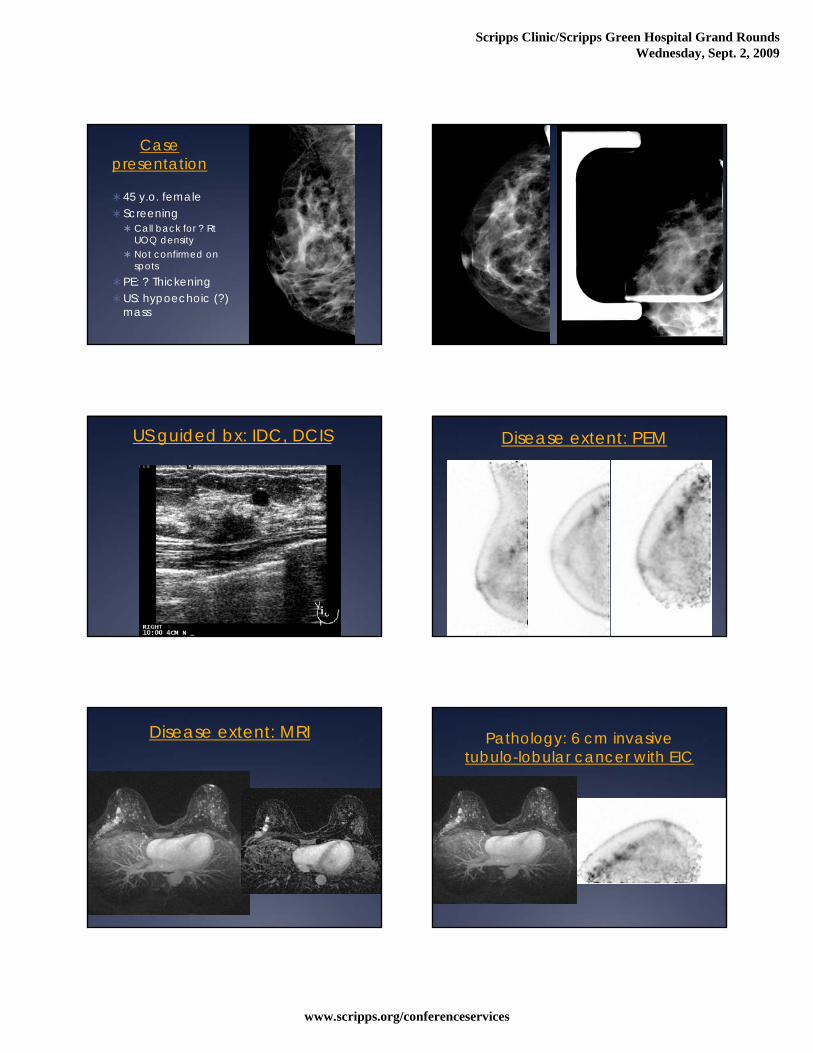
Case presentation
45 y.o. female Screening Call back for ? Rt
UOQ density Not confirmed on
spotsPE: ? ThickeningUS: hypoechoic (?)
mass
US guided bx: IDC, DCIS Disease extent: PEM
Disease extent: MRI Pathology: 6 cm invasive tubulo-lobular cancer with EIC
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
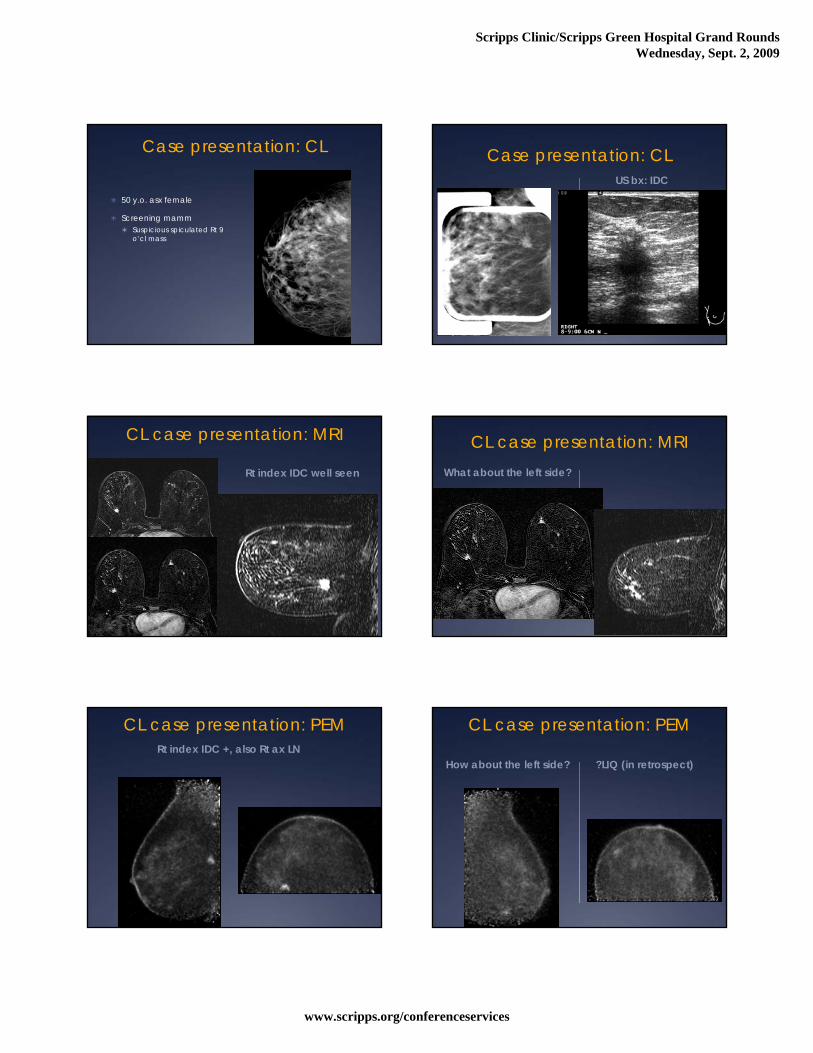
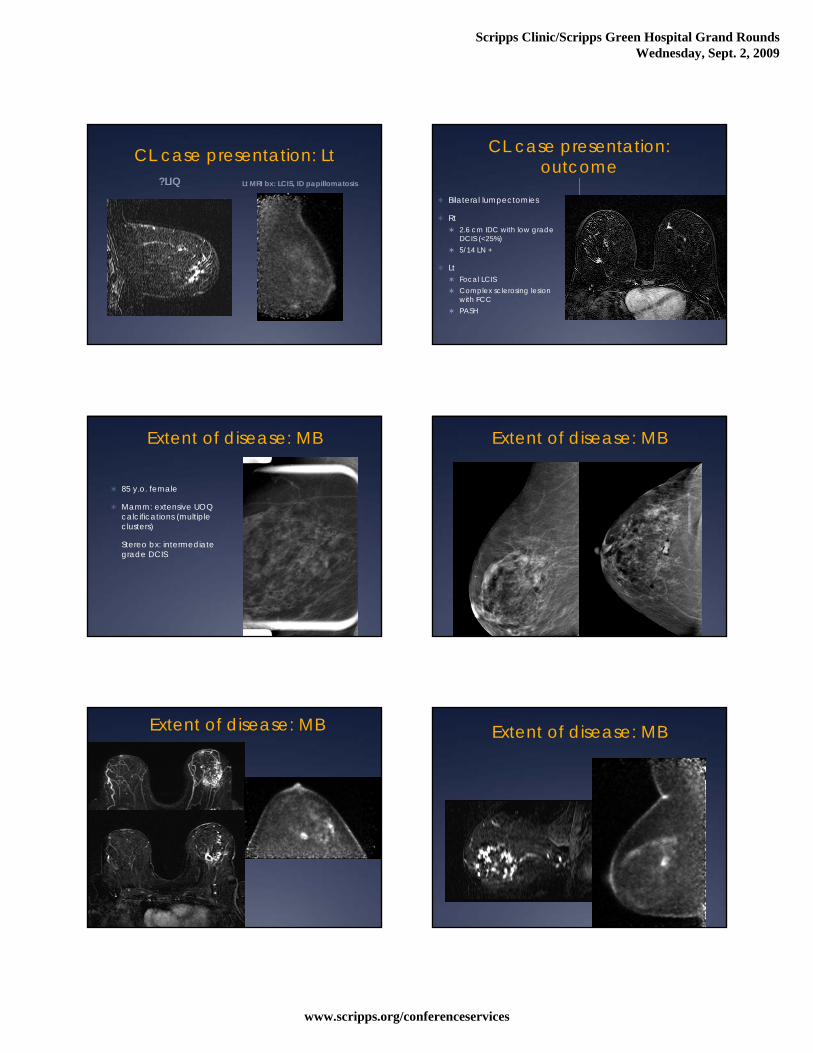
Case presentation: CL
50 y.o. asx female
Screening mamm Suspicious spiculated Rt 9
o’cl mass
Case presentation: CLUS bx: IDC
CL case presentation: MRI
Rt index IDC well seen
CL case presentation: MRIWhat about the left side?
CL case presentation: PEMRt index IDC +, also Rt ax LN
CL case presentation: PEM
How about the left side? ?LIQ (in retrospect)
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
CL case presentation: Lt?LIQ Lt MRI bx: LCIS, ID papillomatosis
CL case presentation: outcome
Bilateral lumpectomies
Rt 2.6 cm IDC with low grade
DCIS (<25%) 5/14 LN +
Lt Focal LCIS Complex sclerosing lesion
with FCC PASH
Extent of disease: MB
85 y.o. female
Mamm: extensive UOQ calcifications (multiple clusters)
Stereo bx: intermediate grade DCIS
Extent of disease: MB
Extent of disease: MB Extent of disease: MB
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
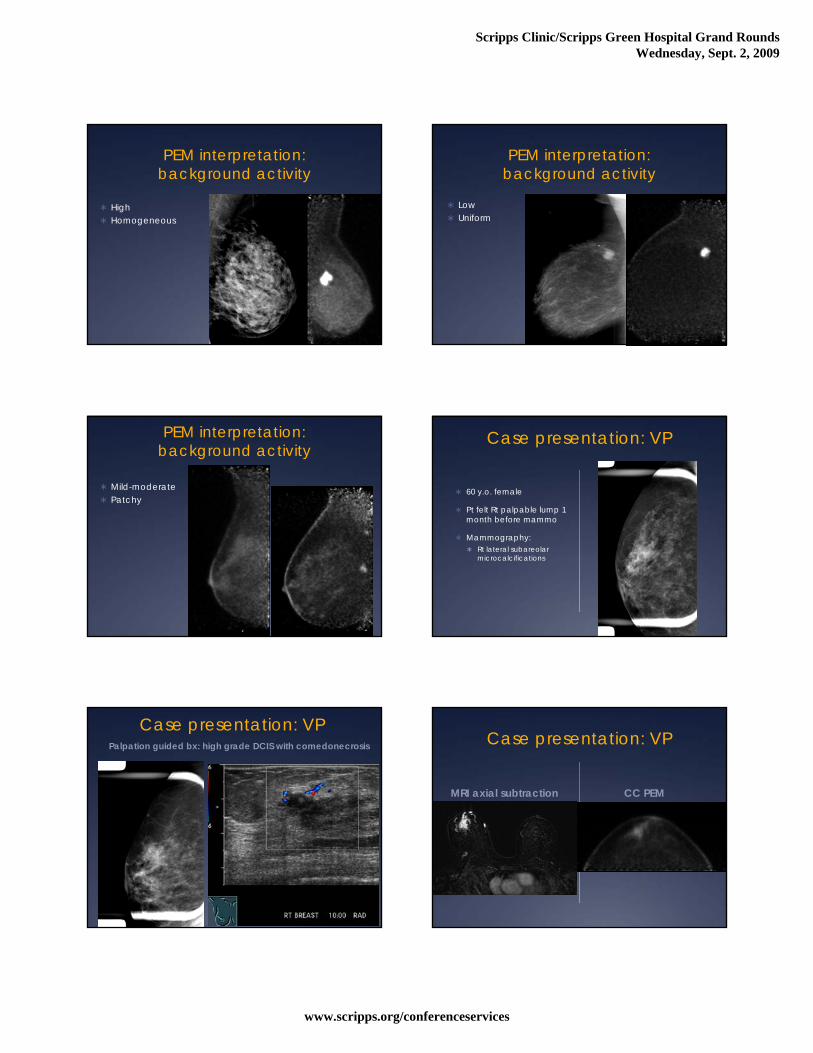
PEM interpretation:background activity
High Homogeneous
PEM interpretation:background activity
Low Uniform
PEM interpretation:background activity
Mild-moderate Patchy
Case presentation: VP
60 y.o. female
Pt felt Rt palpable lump 1 month before mammo
Mammography: Rt lateral subareolar
microcalcifications
Case presentation: VPPalpation guided bx: high grade DCIS with comedonecrosis Case presentation: VP
MRI axial subtraction CC PEM
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
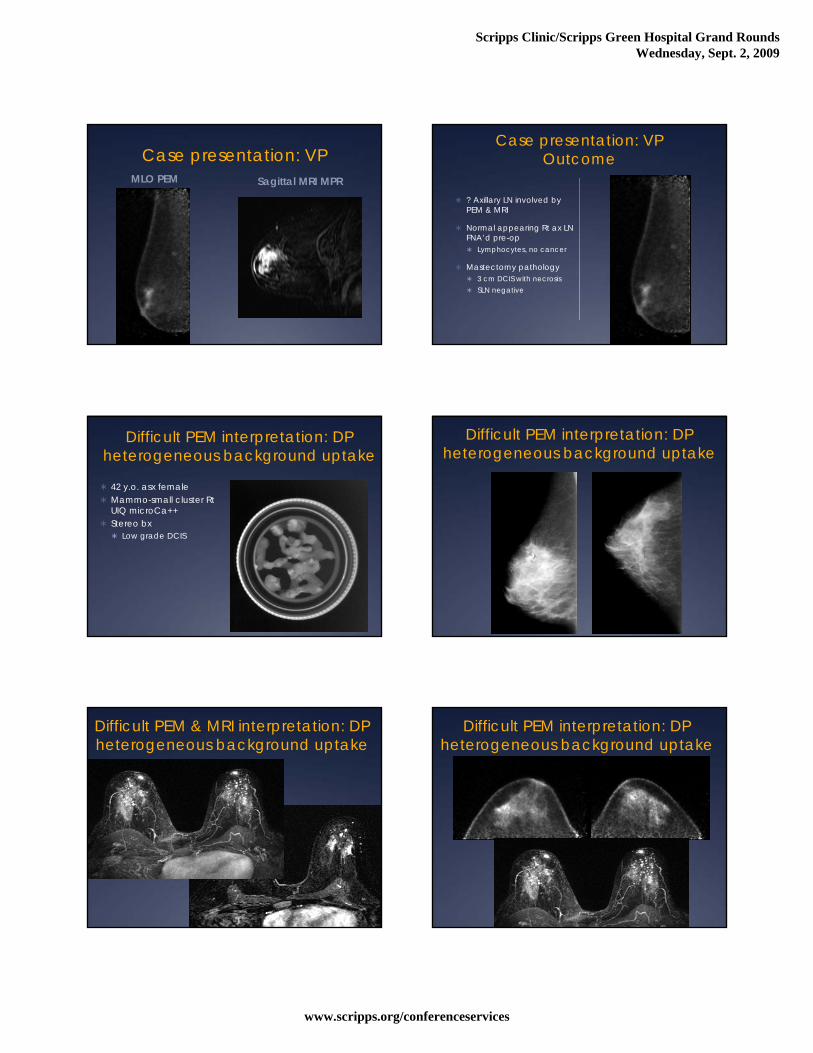
Case presentation: VPMLO PEM Sagittal MRI MPR
Case presentation: VPOutcome
? Axillary LN involved by PEM & MRI
Normal appearing Rt ax LN FNA’d pre-op Lymphocytes, no cancer
Mastectomy pathology 3 cm DCIS with necrosis SLN negative
Difficult PEM interpretation: DPheterogeneous background uptake
42 y.o. asx female Mammo-small cluster Rt
UIQ microCa++ Stereo bx
Low grade DCIS
Difficult PEM interpretation: DPheterogeneous background uptake
Difficult PEM & MRI interpretation: DPheterogeneous background uptake
Difficult PEM interpretation: DPheterogeneous background uptake
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
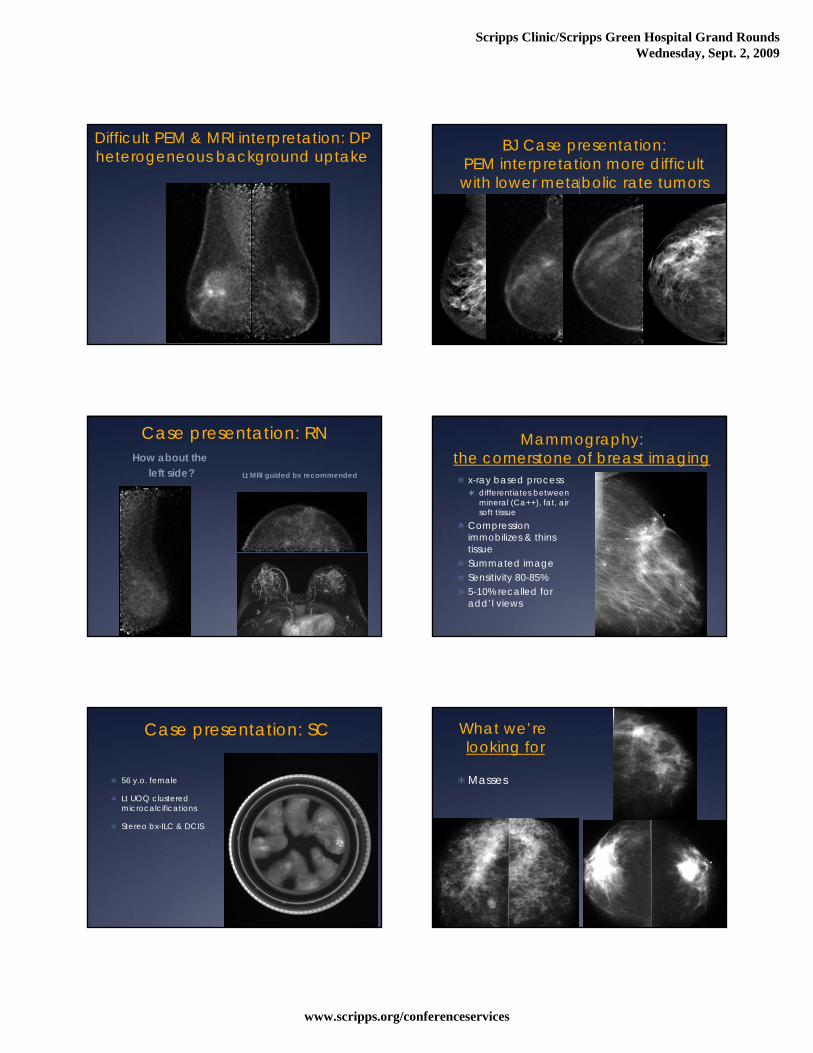
Difficult PEM & MRI interpretation: DPheterogeneous background uptake
BJ Case presentation: PEM interpretation more difficult with lower metabolic rate tumors
(e.g., ILC)
Case presentation: RNHow about the
left side? Lt MRI guided bx recommended
Mammography: the cornerstone of breast imaging x-ray based process
differentiates between mineral (Ca++), fat, air soft tissue
Compression immobilizes & thins tissue
Summated image Sensitivity 80-85% 5-10% recalled for
add’l views
Case presentation: SC
56 y.o. female
Lt UOQ clustered microcalcifications
Stereo bx-ILC & DCIS
What we’relooking for
Masses
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
What we’relooking for
Microcalcifications
Change from a prior exam…
can be the only sign of malignancy
Utility of US
Characterize mammographic or palpable masses Cystic Solid
Circumscribed Or NOT
Guide biopsies
Characterizing masses with US:margin analysis
Breast MRI basics: technique
Prone positioningDedicated breast
coilHigh field magnet 1-1.5 T magnet
Enhanced, subtracted dynamic technique
Breast MRI basics: subtraction
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
Enhancement curve:abnormal wash-out=
angiogenesis
A new tool: Breast MRI CAD
Limitations of mammography:Breast density
Generally greater in younger pts than older
Most people involute with age
Relatively little relation to weight, size
Sensitivity decreases with increasing density
newly recognized as independent risk factor for BC
Case presentation: BBHow many abnormalities?
Sonographic findings frequently non-specific
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
Case VK: was is disease extent?
MRI: MIPMRI: ax subtraction,
minute 1
Case VK: outcome
Rt side pre-op MRI bx Radial scar Negative on PEM
Bilateral lumpectomies Rt-radial scar, columnar
cell change, FCC, fibroadenomatoid change
Lt-3.2 cm IDC, 1 - SLN
Pathology: 3.2 cm IDC
Functional imaging: PET
Tracks physiologic processes using labeled biomolecule (glucose, AA, H2O)
FDG PET uses glucose analog to track glucose metabolism
Rapidly growing tumor cells have greater energy requirements/ glucose utilization than normal cells
Advantages subradiographic dz
mets in nl size LNs complements
anatomic imaging modalities
BSGI advantages/disadvantages
Advantages of BSGI No advance preparation
Cheaper radioisotope
Cheaper
No uptake period
Disadvantages of BSGI Planar
Fuzzier than PEM
No currently available biopsy capability
PEM advantages/disadvantages
PEM advantages “Sharper”
Tomographic
Biopsy capability now
Can be performed in conjunction with WB PET
PEM disadvantages Pt must fast > 4 hours
Glucose must be checked & normal
Low metabolic rate tumors variable in FDG avidity
More expensive
Case presentation: CCMulti-centric disease suggested, MRI recommended, prior Lt US targeted
Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
Does this matter?
Conventional breast imaging(mammography & US) frequently underestimate the extent of breast cancer in comparison to histology
Some difficult questions
Time for a break!High Risk Screening
BREAST IMAGING:Cancer Yield of Mammography, MR, and US in High-Risk Women: Prospective Multi-Institution Breast Cancer Screening Study
Lehman CD, et al. Radiology, Aug 2007; 244: 381 - 388.
195 women enrolled over 6 months 171 completed all
modalities within 90 days
High risk BRCA-1 (31)/BRCA-2 (36) >20% probability BRCA
16 abnormalities/bxs performed
6 cancers dx’d All 6 found by MRI Mammo found 2 US found 1 (also found by
mammo & MRI)
Whole breast screening US:the case against it
High risk screening Lehman CD, et al.
Radiology, Aug 2007; 244: 381 - 388. Cancer yield
MRI 3.5% US 0.6% Mammo 1.2%
Dense breast screening
Positron Emission Mammography: PEM
Image: courtesy of Naviscan PET Systems

Scripps Clinic/Scripps Green Hospital Grand RoundsWednesday, Sept. 2, 2009
www.scripps.org/conferenceservices
Resolution: WB PET vs. PEM Case presentation: KS
Normalized Rt CC
Case presentation: KS
Final pathology Mastectomy
2 invasive mammary cancers 9 o’clock: 2 cm, features
of lobular cancer with tubule formation
11 0’clock: 1.5 cm
Focal DCIS also in LOQ & LIQ
Whole breast screening US:
more controversial Results in elevated risk
population (n=2725) Mammographic
sensitivity alone 50% Mammo + US sensitivity
77.5% Berg WA, et al.
Combined Screening With Ultrasound and Mammography vs Mammography Alone in Women at Elevated Risk of Breast CancerJAMA. 2008;299(18):2151-2163.
High likelihood of false positives (9% PPV)
Extremely labor intensive
Related Documents











