BREAST Begashaw M (MD)

BREAST Begashaw M (MD). Introduction Modified sweat gland - produces milk Breast ca - most common cause of death Benign conditions discomfort confusion.
Dec 13, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

BREAST
Begashaw M (MD)
Introduction
Modified sweat gland - produces milkBreast ca - most common cause of deathBenign conditions discomfort confusion
with neoplastic disease
Anatomy
overly -2nd – 6th rib - from lateral border of sternum to anterior axillary line, between clavicle & to the 7th & 8th ribs below
Ligaments of cooper Areola contains involuntary muscles nipple covered by thick skin lactiferous ducts Lymphatics -axillary lymph nodes on the ipsilateral
side

Anatomy
Breast lumps
DDx
• Cancer
• Fibrocystic change
• Fibroadenoma
• Fat necrosis
• Duct ectasia
• lipoma
•TB

Breast cyst
Raredue to a nonintegrated involution of stroma
& epitheliumoften multiple & may be bilateralDiagnosis –aspiration/ultrasoundTreatment – Aspiraton
Fibroadenoma
Most common in women age < 30 C/F
Nodulessmooth, rubbery, discrete, well-circumscribed, non-tender, mobile
Ixs
-biopsy
-ultrasound
-FNA Treatment
_Generally conservative: serial observation
_Consider excision if size 2-3 cm & rapidly growing

Fibroadenoama
Phyllodes Tumor
_Are benign tumors
_Usually occur in women over 40 years
_large, massive tumor with unevenly lobulated surface and occasionally with ulceration of overlying skin
_Treatment – Enucleation
_ Simple mastectomy
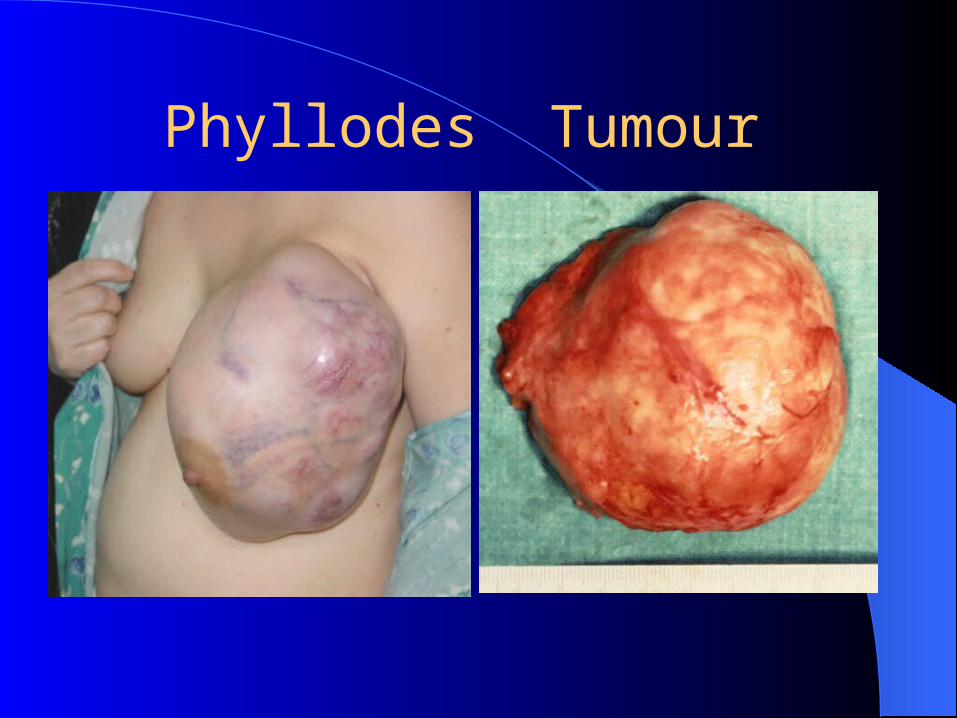
Phyllodes Tumour
Ductectasia/ periductal mastitis
is dilatation of breast ducts associated with periductal inflammation
Pathogenesis
_ Dilatation of lactiferous ducts filled with a stagnant brown or green secretiondischarge
_irritant reaction in surrounding tissue leading to periductal mastitis

Clinical presentation
-Nipple discharge
-subareolar mass
-Abscess
-Mammary duct fistula/nipple retraction Treatment
-Excision of all major ducts

Investigation of a Breast Lump

Acute mastitis
is acute inflammation of the breast Bacterial mastitis is the commonest variety of mastitis and nearly
always commences acutely associated with lactation
Causestaphylococcus aureus Clinical presentation
- Pain
- Swelling- Redness- Tenderness/hotness- abscess

Treatment
Antibiotics – cloxacillin Breast restbreast-feeding on the opposite
side only Support breast Local Heat/Analgesics

Breast abscess
If acute infection of breast doesn’t resolve with in 48 hours/tense induration Abscess
Fluctuation is a late signWhen doubt exists incision & drainageTreatment – incision & drainage

Lactational breast abscess Nonlactational breast abscess

Breast abscess drainage
Breast Carcinoma
is the commonest cause of death in middle-aged women in western countries
In our set up, increasing incidence is being observed
Risk Factors
_ Gender -99% Female
_ Age80% >40 years old
_ Prior hx of breast ca
_1st degree relative
_ Nulliparity, First pregnancy >30 years old, Menarche < 12 yrs old, Menopause >55 yrs old
_Decreased risk with lactation,Early menopause, Early childbirth
_Radiation exposure
_Obesity,Diet,Geography-western
Pathology
Arise from the epithelium of the duct system May be entirely in situ or may be invasiveGrades -Well differentiated
-Moderately
-Poorly differentiatedDuctal carcinoma -Most common Lobular carcinoma -10 %

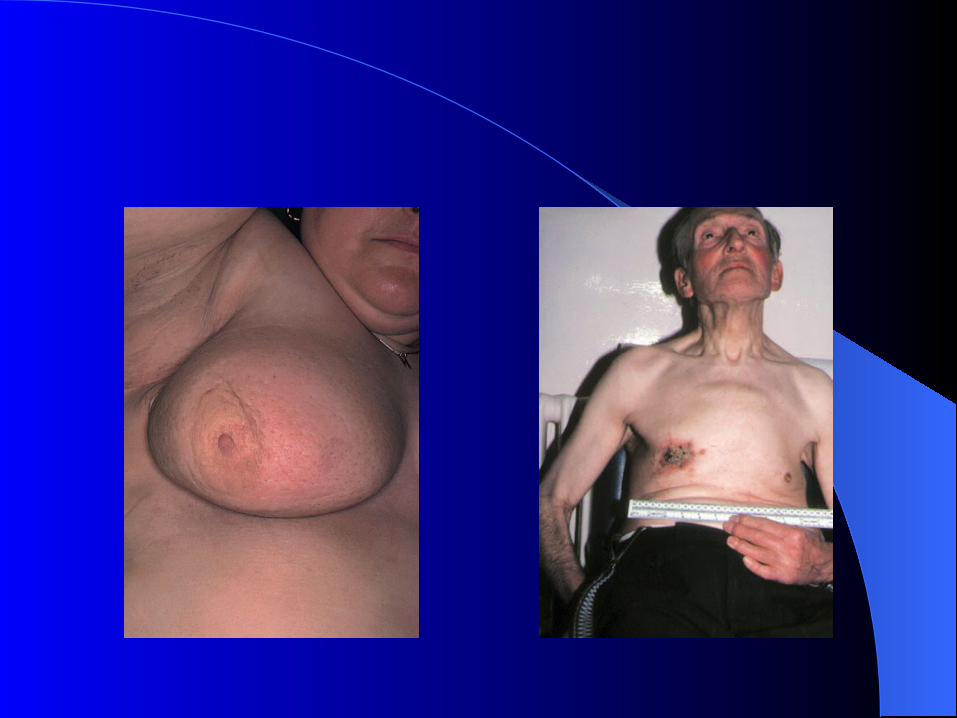
Breast cancer Locally advanced breast carcinoma

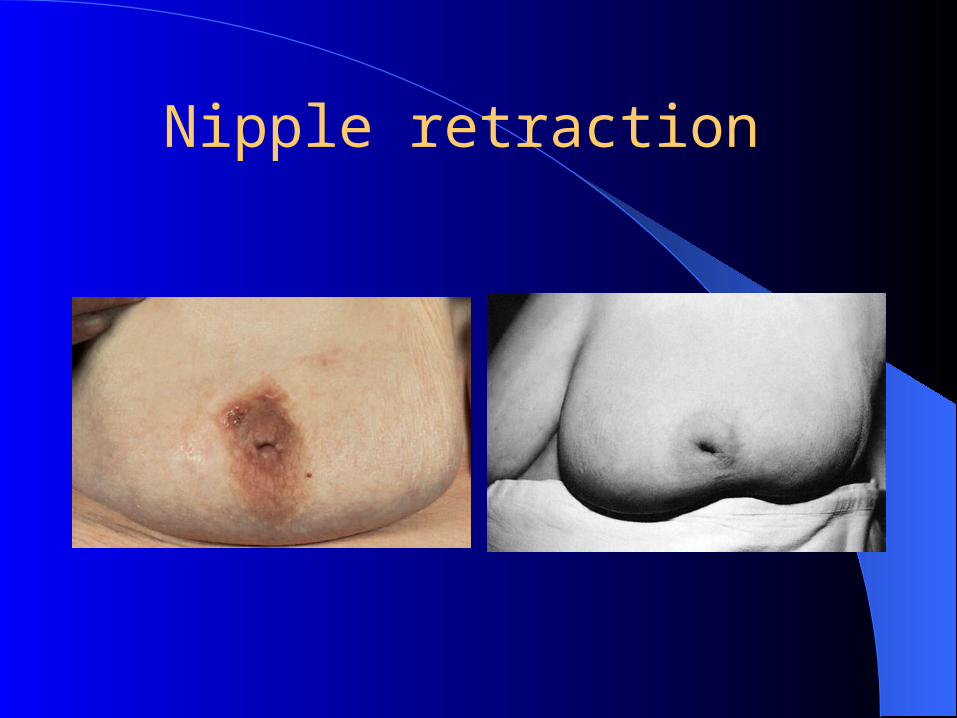
Nipple retraction

Spread
Local spread: increases in size & invades,involve skin,penetrate pectoral muscles & chest wall
Lymphatic spread
_Axillary lymph node
_Supraclavicular nodes
_Contra lateral lymph nodes Hematogenous Bone(lumbar,Femur, thoracic
vertebra, rib/skull) osteolytic) liver, lungs & brain
Clinical presentation
occurs commonly upper outer quadrant/UOQ
Local Findings
_Hard, irregular lump
_nipple retraction
_Skin involvement with peau d’ orange
_Frank ulceration & fixation to the chest wall
27
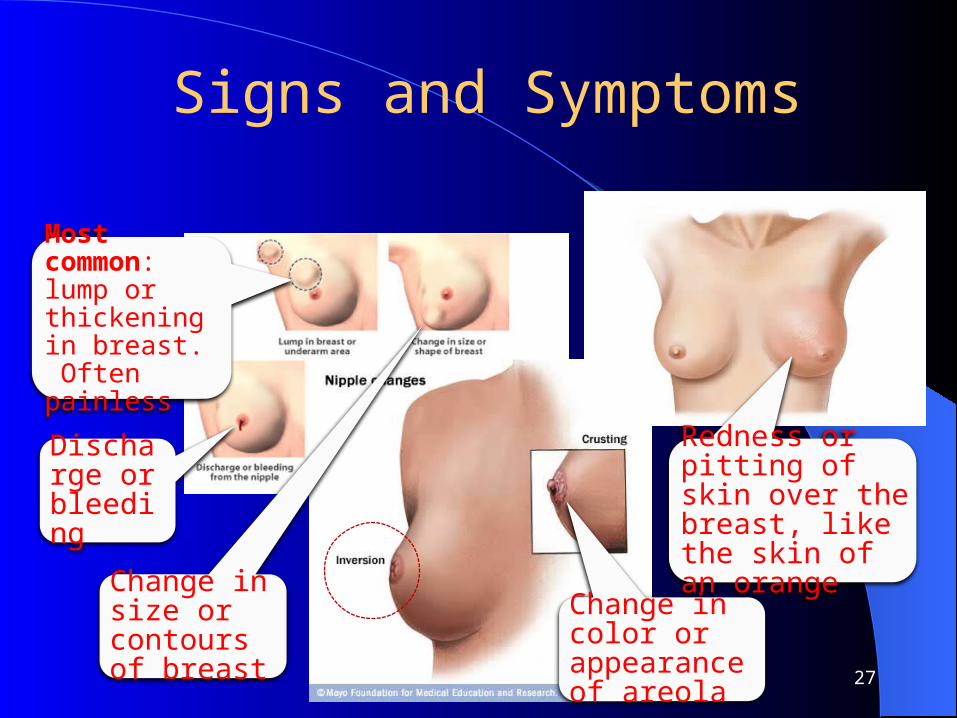
Signs and Symptoms
Most common: lump or thickening in breast. Often painless
Change in color or appearance of areola
Redness or pitting of skin over the breast, like the skin of an orange
Discharge or bleeding
Change in size or contours of breast

Signs of metastasis
_Lymph node enlargement
_Bone pain
_cough Chest x-ray, Serum alkaline phosphates &
liver ultrasound

Prognosis
- Tumor size & LN status
- Invasive & metastatic potential
- Histological grade
- Estrogen receptor status- Patient age

Treatment
Multi disciplinary
_Surgery
_Radiotherapy
_Medical therapy -Chemotherapy
-Hormonal therapy
Related Documents