5/16/19 1 1 Christine S. Yun, MSN, PNP, CPON CHOC Children’s Hospital Lauren Bristow Guidry, MSN, CPNP, CPHON Children’s Hospital Los Angeles Breaking News: Paradigm Shift in Pre-B Acute Lymphoblastic Leukemia – COG Update 2 Disclosure ▪ Christine Yun has no industry relationships to disclose. § Lauren Bristow Guidry has no industry relationships to disclose. ▪ Off label use will be discussed 3 COG Disclosure The information in this presentation is intended for educational purposes only and is solely for the use of the individual nurse learner. This information is not intended as the sole source of guidance in providing Children’s Oncology Group (COG) protocol-directed nursing care, and current COG protocols should always be consulted prior to making patient care decisions for any patient enrolled on a COG protocol. Learners should also be aware that COG protocols are research plans designed to investigate particular study questions, that recommendations for treatment and dosing are made within the context of specific research aims, and that these recommendations are intended only for use within a structured research setting. Although every attempt has been made to assure that the informational content contained herein is as accurate and complete as possible as of the date of presentation, no warranty or representation, express or implied, is made as to the accuracy, reliability, completeness, relevance, or timeliness of this content. This information may not be copied or redistributed in any form, or used for any purpose other than nursing education. 4 Objectives § Describe COG’s updated risk classifications and definitions of remission and relapse in ALL § Discuss immunotherapy versus conventional chemotherapy in the treatment of ALL patients § Identify new treatment strategies, including immunotherapy, for frontline treatment in ALL patients 5 Incidence of Childhood Cancer 6 Survival in Childhood Leukemia 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% ALL Ages 0-14 Ages 0-19 66% 92%

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

5/16/19
1
1
Christine S. Yun, MSN, PNP, CPONCHOC Children’s Hospital
Lauren Bristow Guidry, MSN, CPNP, CPHONChildren’s Hospital Los Angeles
Breaking News: Paradigm Shift in Pre-B Acute Lymphoblastic Leukemia – COG Update
2
Disclosure
▪ Christine Yun has no industry relationships to disclose.
§Lauren Bristow Guidry has no industry relationships to disclose.
▪ Off label use will be discussed
3
COG DisclosureThe information in this presentation is intended for educational purposes only and is solely for the use of the individual nurse learner. This information is not intended as the sole source of guidance in providing Children’s Oncology Group (COG) protocol-directed nursing care, and current COG protocols should always be consulted prior to making patient care decisions for any patient enrolled on a COG protocol. Learners should also be aware that COG protocols are research plans designed to investigate particular study questions, that recommendations for treatment and dosing are made within the context of specific research aims, and that these recommendations are intended only for use within a structured research setting. Although every attempt has been made to assure that the informational content contained herein is as accurate and complete as possible as of the date of presentation, no warranty or representation, express or implied, is made as to the accuracy, reliability, completeness, relevance, or timeliness of this content. This information may not be copied or redistributed in any form, or used for any purpose other than nursing education.
4
Objectives
§Describe COG’s updated risk classifications and definitions of remission and relapse in ALL
§Discuss immunotherapy versus conventional chemotherapy in the treatment of ALL patients
§ Identify new treatment strategies, including immunotherapy, for frontline treatment in ALL patients
5
Incidence of Childhood Cancer
6
Survival in Childhood Leukemia
0%10%20%30%40%50%60%70%80%90%
100%
ALLAges 0-14 Ages 0-19
66%92%

5/16/19
2
7
Prognostic factors
8
Minimal Residual Disease (MRD)§ Identification of presence or absence of residual
disease§Most important prognostic factor in childhood
ALL§Submicroscopic MRD can be measured 3 ways
Morphologic Molecular
The difference between traditional assessments of blood
cancer and MRD is like the difference between a classic
detective and a modern crime scene investigator.
9
Flow cytometry§Technique for detecting specific proteins on the
surface of cells§Quick turn around time§Detects 1:10,000 cells
10
Polymerase Chain Reaction (PCR)§Amplification of clonotypic IGH or TcR gene
rearrangement§Original clone needed§More sensitive as detects up to 1 in 100,000 cells
11
Next Generation Sequencing (NGS)
§Also known as high throughput sequencing (HTS)§Clonality and dominant sequence identification via
parallel analysis§Must have at least 500,000 cells analyzed to be
considered determinate§Sensitivity can reach up to 1 in 1,000,000 cells
12
MRD Timepoints:
End of Consolidation

5/16/19
3
13
Modernized COG DefinitionsRemission 1§< 1% blasts by MRD by end consolidation
♦ Early Rem-1: If you reach this level by EOI♦ Late Rem-1: If you reach this level by EOC
Consolidation failure§ ≥ 1% MRD at EOC or persistent EM disease
Note: Perform marrow when absolute phagocyte recovery (ANC + AMC) > 500/μL after day 56 of consolidation therapy
14
Modernized COG DefinitionsMarrow Relapse (must have achieved remission)
♦ Rel-M3: M3 morphology♦ Rel-M2: M2 morphology and confirmatory MRD testing
showing >5% blasts ♦ Rel-M1: M1 morphology and at least 2 tests showing
MRD >1% blasts • FISH abnormality identical to diagnosis• Flow cytogenetics with at least 1 karyotype identical to
diagnosis • PCR or NGS of Ig/TCR rearrangement that matches
diagnosis and is quantifiable as >1%• PCR or NGS of fusion gene that matches diagnosis and is
quantifiable as >1%
15
Modernized COG DefinitionsCNS Relapse (must have achieved remission)
♦ Rel-CNS 3♦ Rel-CNS 2: 2 consecutive CSF samples 1-4 weeks apart
with CNS2 status
Testicular relapse (must have achieved remission)♦ Biopsy proven relapse
OEM relapse (must have achieved remission)♦ Biopsy proven relapse
16
CytogeneticsAberration Lineage Prognostic
Significance Comments
ETV6RUNX1 t(12:21) B Lineage ALL Favorable
Ph+ t(9:22)B Lineage ALL(rarely T Lineage ALL)
Unfavorable 3-5% of childhoodALL
iamp21 B Lineage UnfavorableIntrachromosomal amplification of chromosome 21
Ph-like B Lineage Unfavorable More common in teens/adults
MLL t(4:11, 10:11) B Lineage Unfavorable Occurs 75% in age less than 1 year
Trisomy 4, 10 B Lineage Favorable EOI MRD < 0.1%
17
Risk-Directed Therapy§ “Standard” versus “high” risk per NCI§Treatment stratified based on risk of relapse§Treatment refined based on initial response
to therapy§Therapy intensified for those with persistence of
detectable MRD §Tailored therapy minimizes late effects
18
What We Have Learned §EOC MRD has prognostic significance§Ceiling effect with conventional therapy§ Less toxicity with immunotherapy vs. conventional
chemotherapy§Need for AYA/ALL collaboration
♦ COG led trials: “pediatric cancers” ages 15-25 years♦ Adult led trials: “adult cancers” ages 25-39 years
5/16/19
4
19
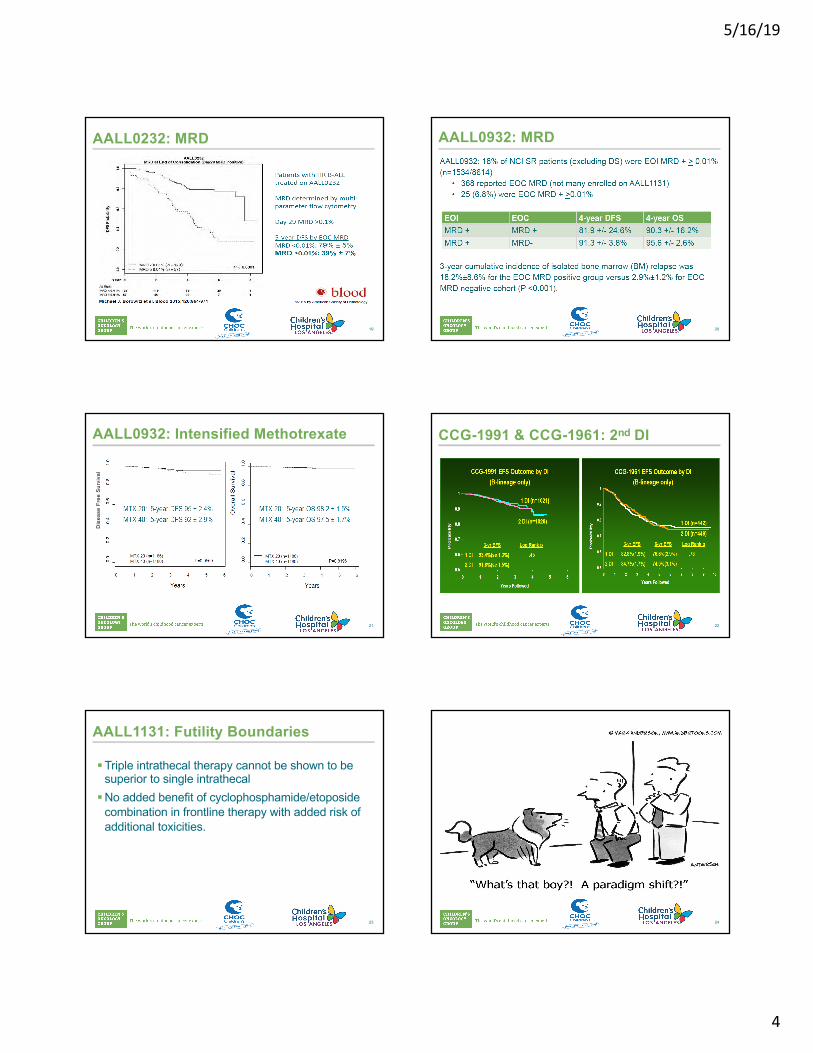
AALL0232: MRD
20
AALL0932: MRD
21
AALL0932: Intensified Methotrexate
Dis
ease
Fre
e S
urvi
val
22
CCG-1991 & CCG-1961: 2nd DI
23
AALL1131: Futility Boundaries
§Triple intrathecal therapy cannot be shown to be superior to single intrathecal
§No added benefit of cyclophosphamide/etoposide combination in frontline therapy with added risk of additional toxicities.
24
5/16/19
5
25
Breaking News§ Immunotherapy is moving upfront.
♦ In 5-7 years, CD19 or CD22 targeted immunotherapy may be standard for most B-ALL patients
♦ Subsequent trials: optimize immunotherapy (multi-antigen targeting, checkpoint inhibition, etc.)
§For the next 5-7 years, the majority of 1st relapse patients will not have received immunotherapy.♦ Need for efficacy data.
§Many/most ≥ 2nd relapses will likely receive commercial or investigational CAR T-cells
§ Long term complications of immunotherapy unknown
26
What’s New?§Immunotherapy as frontline
27
RUXOLITINIB (Jakafi)
28
§ Interferes with the JAK pathway to prevent cell reproduction
§ JAK pathway is important for cell growth and regulation
Janus Associated Kinase (JAK) Inhibitor
29
How is it used in pediatric leukemia?
§Still considered experimental§Used in Ph-like leukemia§Used in conjunction with standard chemotherapy
backbone
30
§ Similar cytogenetics as Ph+, but may not have the BCR-ABL fusion♦ May just have ABL fusions
§ May have CRLF2 mutations with or without JAK1/JAK2 mutations
§ Have similarly poorer outcomes§ More common in adolescent Hispanics§ About 10% of standard risk patients will have this marker§ About 13% of high risk patients will have this marker
What is Ph-like ALL?

5/16/19
6
31
5 year EFS of non-Ph-like patients = 85%
5 year EFS of Ph-like patients = 62%
32
§Generally very mild§Usually include:
♦ Pancytopenia♦ Elevated liver function
tests♦ Nausea/vomiting♦ Delayed count recovery♦ Fatigue
Adverse Events
33
Nursing Consideration
§Do not re-dose if emesis occurs
34
INOTUZUMAB OZOGAMICIN (InO)
35
Phase IISingle dose
Phase IIWeekly X3
Phase IIIWeekly X3
Comp. useWeekly X 3
Population Adult Adult Adult Pediatric
N 49 41 139 51
CR/CRp/Cri (%) 57 59 80.7 67
AST/ALT (%) 57 27 20 19
Bilirubin (%) 29 5 15 2
Post-HSCT VOD (%) 23 7 21* 52
Reference Kantarjian et al. Lancet Oncol. 2012
Kantarjian et al.Cancer 2013
Kantarjian et al.NEJM 2016
Bhojwani D et al. Leukemia 2018
MRD neg (%) 63 71 78 71
InO: Studies in R/R ALL
36
How does InO work?
Wiley Online Library, accessed 5/2/17
• CD22-directed monoclonal antibody conjugate linked to calicheamicin
• Calicheamicin is a cytotoxin that enters the cell and causes the DNA strands to break, thus causing apoptosis of the tumor cell
• CD22 is expressed in >90% of patients with ALL

5/16/19
7
37
How is InO given?
§ Intravenous§Each cycle lasts 4 weeks
♦ Give 3 doses on day 1, 8, 15♦ Fractionated doses help to reduce side effects
§Will usually have a bone marrow evaluation at the end of each cycle
38
Adverse Events§ Low emetogenic profile§Hematologic
♦ Neutropenia ♦ Thrombocytopenia
§Non-hematologic♦ Tumor lysis syndrome♦ Hepatotoxicity♦ Infusion reaction♦ Prolonged QT syndrome
39
Sinusoidal Obstruction Syndrome (SOS)
§Occurs when blood vessels in the liver become blocked or inflamed due to damage to the sinusoidal endothelial cells
§Exact pathophysiology behind why InO causes SOS is unknown
40
Signs of SOS
§Early signs♦ Weight gain from retention of water and sodium
§Other signs♦ Jaundice (elevated bilirubin), painful hepatomegaly,
transaminitis, edema, ascites§Severe signs
♦ Hypoxia, encephalopathy, pleural effusion, pulmonary infiltrates, thrombocytopenia, renal failure
41
Interventions to Prevent SOS
§Use prophylactic agents like ursodiol§Avoid hepatotoxic agents (e.g. azoles)§When proceeding to transplant
♦ Avoid conditioning regimens with dual alkylating agents♦ No more than 2 cycles of InO pre-transplant
42
BLINATUMOMAB

5/16/19
8
43
• A monoclonal antibody that is part of a new class called bi-specific T-cell receptor engaging (BITE) antibodies, which are made by linking two different monoclonal antibodies
• Targets the CD 19 antigen on B-ALL blast cells and normal B cells
• Redirects CD3+ T-cells for selective lysis of B cells
Mechanism of Action
44
How is Blinatumomab given?
§Continuous IV infusion over 28 days§Pre-medicate first cycle with dexamethasone
45
Adverse Events§Seizure§Thromboembolic event§Disseminated intravascular coagulation§Hemolysis§Neutropenia§Anemia§Thrombocytopenia
46
Adverse Events
§Nervous System/Psychiatric♦ Confusion♦ Hallucination♦ Delirium♦ Psychosis♦ Tremors
47
Adverse Events
§ Immune System ♦ Cytokine release syndrome (CRS)
• Collection of inflammatory symptoms as a result of an increase in cytokines associated with T cell engagement and proliferation
48
CRS Symptoms§ Fever§ Myalgia§ Chills/rigors§ Nausea/vomiting§ Hypo-/hypertension§ Tachycardia§ Transaminitis§ Hyperbilirubinemia
§ Headache§ Mental status changes§ Pulmonary edema§ Dyspnea§ Hypoxia § Coagulopathy§ Multiorgan failure

5/16/19
9
49
Treatment of CRS• Pre-medicate with dexamethasone for at least
the first cycle
• Tocilizumab- anti-IL-6 monoclonal antibody• IL-6 is an inflammatory cytokine
50
CHIMERIC ANTIGEN RECEPTOR (CAR) T CELLS
December 9, 2012
51
Maude S et al. Blood 2015;125:4017-4023
Mechanism of Action
§ Infuse genetically modified T cells that can recognize and eliminate malignant cells
52
CD 19 CAR T TrialsCHOP/Novartis Kymriah
NCI/KITEKTE-C19
Seattle
Co-stim. 4-1BB CD28 4-1BBN 75 21 45Feasibility (82%) 90% 93%MRD negative CR 81% 60%* 89%*12-month EFS 50% NA 50.8%CRS 47% 19% 23%Neurotoxicity (3/4) 13% 19% 21%Manufacture time 4-6 weeks 1-2 weeks 4 weeksReferences Maude, NEJM 2018 Lee, Lancet
2015Gardner, Blood 2017
53
Kymriah (tisagenlecleucel)
§Commercially available for second or greater relapsed or refractory disease
August 30, 2017
54
Adverse Events
§CRS§Hypogammaglobulinemia§Pyrexia§Febrile neutropenia§Hypotension§Decreased appetite§ Increased AST

5/16/19
10
55
Effects on the Immune System
§B cell aplasia§Hypogammaglobulinemia
56
Nursing Consideration
§Avoid corticosteroids as much as possible
57
CD 22 CAR T Cells
§Still in early phases of development§Only available as a clinical trial§Available for patients with CD 19 negative
relapses§Same toxicity profile as CD 19 CAR T cells§Often used as a bridge to transplant§ Long term cure rate still being studied
58
Final Thoughts
§Ruxolitinib♦ Still experimental♦ Used in conjunction with standard chemotherapy
§ Inotuzumab♦ In the past, used for relapsed/refractory patients as a
single agent♦ Now will be used as front line therapy in experimental
arm for HR ALL patients
59
Final Thoughts
§Blinatumomab♦ Most effective in patients with low disease burden♦ In the past, used as bridge to transplant, or even to CAR
T cells, and as combination therapy for relapsed patients♦ Now will be used as front line therapy in experimental
arm for SR ALL patients
60
Final Thoughts
§CD 19 CAR T cells♦ Higher CR rates♦ More effective in patients with high disease burden
§CD 22 CAR T cells♦ Still experimental♦ Limited Availability

5/16/19
11
61
New Frontline COG Trials
§ AALL1521- High Risk Ph-like ALL• Ruxolitinub
§ AALL1731- Standard Risk ALL• Blinatumomab
§ AALL1732- High Risk ALL• Inotuzumab
§ AALL1721- Very High Risk ALL• CD 19 CAR T cells
62
How do we choose between blinatumomab, inotuzumab, or CAR T cells for our patients???
63
Acknowledgements
§ Children’s Oncology Group-Acute Lymphoblastic Leukemia Disease Committee
§ Deepa Bhojwani, MD
64
Related Documents











