Breaking Down Barriers: Breaking Down Barriers: Providing Integrated Care for Providing Integrated Care for Individuals with Severe Mental Individuals with Severe Mental Illness and Substance Use Illness and Substance Use Disorders Disorders Ken Bachrach, Ph.D. Ken Bachrach, Ph.D. Debbie Innes-Gomberg, Ph.D. Debbie Innes-Gomberg, Ph.D. Monica Weil, Psy.D. Monica Weil, Psy.D. Martin Hernandez, MSW Martin Hernandez, MSW

Breaking Down Barriers: Providing Integrated Care for Individuals with Severe Mental Illness and Substance Use Disorders Ken Bachrach, Ph.D. Debbie Innes-Gomberg,
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Breaking Down Barriers: Providing Breaking Down Barriers: Providing Integrated Care for Individuals with Integrated Care for Individuals with
Severe Mental Illness and Substance Severe Mental Illness and Substance Use DisordersUse Disorders
Ken Bachrach, Ph.D. Ken Bachrach, Ph.D. Debbie Innes-Gomberg, Ph.D.Debbie Innes-Gomberg, Ph.D.
Monica Weil, Psy.D.Monica Weil, Psy.D.Martin Hernandez, MSWMartin Hernandez, MSW

The Mental Health Services The Mental Health Services Act Act
Proposition 63 Passed November, Proposition 63 Passed November, 20042004
Identifies 4 distinct age groups:Identifies 4 distinct age groups:
Children Children 0 -150 -15
Transition Age YouthTransition Age Youth 16-2516-25
AdultsAdults 26-5926-59
Older AdultsOlder Adults 60 +60 +

MHSA Philosophy MHSA Philosophy
Goal is to transform the mental health Goal is to transform the mental health system system
An inclusive planning processAn inclusive planning process Fund or expand programs that use proven Fund or expand programs that use proven
service modelsservice models Assure accountability by collecting data on Assure accountability by collecting data on
outcomesoutcomes Do whatever it takes to support clients to Do whatever it takes to support clients to
achieve recoveryachieve recovery

Components of MHSAComponents of MHSA
PlanningPlanning Community Services and SupportsCommunity Services and Supports
FSP and Systems DevelopmentFSP and Systems Development Prevention and Early InterventionPrevention and Early Intervention Capital Facilities and TechnologyCapital Facilities and Technology Workforce, Education and TrainingWorkforce, Education and Training InnovationInnovation
Full Service PartnershipsFull Service PartnershipsAdultsAdults
Adults who are a severe mental illness and who Adults who are a severe mental illness and who are:are:
HomelessHomeless In jailIn jail Frequent users of psychiatric hospitals or ERsFrequent users of psychiatric hospitals or ERs In institutions (IMDs, State Hospitals)In institutions (IMDs, State Hospitals) Being cared for by families but in the absence Being cared for by families but in the absence
of the family would be at risk of the above.of the family would be at risk of the above.
FSP ServicesFSP ServicesWhatever it TakesWhatever it Takes
Individualized, comprehensive treatment Individualized, comprehensive treatment and support focused on recoveryand support focused on recovery
1:15 maximum staff to client ratio1:15 maximum staff to client ratio Multi-disciplinary daily team meetingsMulti-disciplinary daily team meetings 24/7 availability for crises24/7 availability for crises Field-based service approachField-based service approach Peer support servicesPeer support services Integrated COD servicesIntegrated COD services Housing and employment assistanceHousing and employment assistance
Services Provided in Services Provided in Residential Drug and Alcohol Residential Drug and Alcohol
TreatmentTreatment Assessment & Treatment PlanningAssessment & Treatment Planning Individual and Group CounselingIndividual and Group Counseling Addiction and Recovery ServicesAddiction and Recovery Services Social ServicesSocial Services Community LinkagesCommunity Linkages Discharge PlanningDischarge Planning
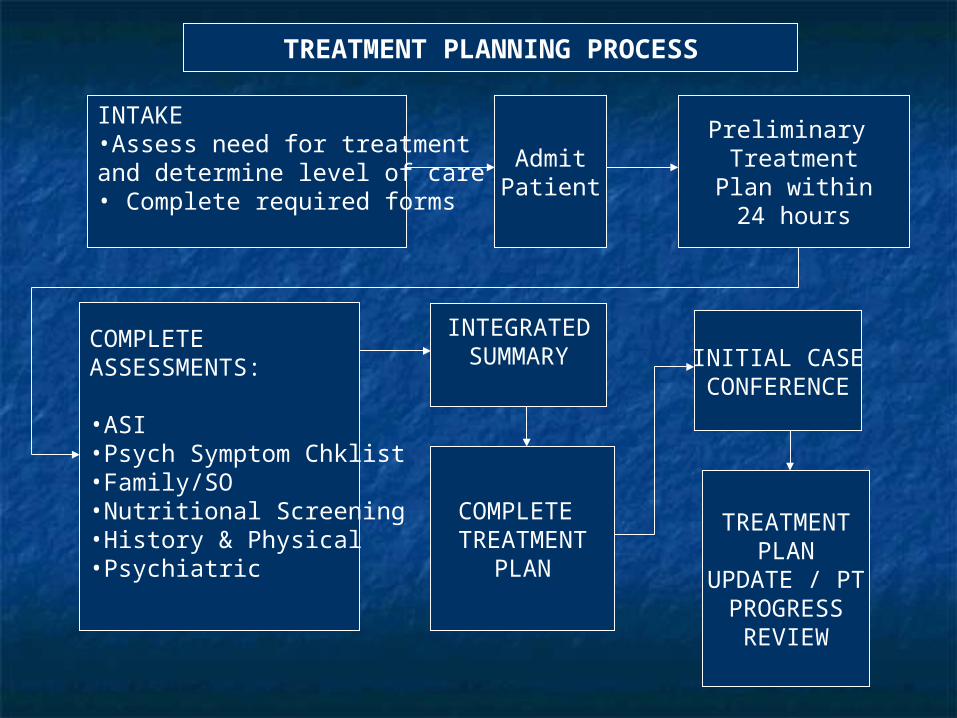
INTAKE•Assess need for treatmentand determine level of care• Complete required forms
AdmitPatient
Preliminary TreatmentPlan within24 hours
COMPLETE ASSESSMENTS:
•ASI•Psych Symptom Chklist•Family/SO•Nutritional Screening•History & Physical•Psychiatric
INTEGRATEDSUMMARY
COMPLETE TREATMENT
PLAN
INITIAL CASECONFERENCE
TREATMENTPLAN
UPDATE / PTPROGRESS
REVIEW
TREATMENT PLANNING PROCESS

GroupsGroups
Educational (Addiction Education)Educational (Addiction Education) Psychoeducational (Relapse Psychoeducational (Relapse
Prevention)Prevention) Process (Recovery Issues; Men’s / Process (Recovery Issues; Men’s /
Women’s Group)Women’s Group)

Core GroupsCore Groups
Addiction EducationAddiction Education Family EducationFamily Education Relapse PreventionRelapse Prevention Self-Help OrientationSelf-Help Orientation Recovery IssuesRecovery Issues Multi-Family GroupMulti-Family Group

Residential ElectivesResidential Electives
Stress ManagementStress Management Spirituality GroupSpirituality Group Depression ManagementDepression Management Trauma Group Trauma Group (separate for men & women)(separate for men & women) Grief & LossGrief & Loss Anger ManagementAnger Management Recreational Therapy / Leisure EducationRecreational Therapy / Leisure Education

Residential Drug Treatment Residential Drug Treatment RecipientsRecipients
Often have a long history of substance Often have a long history of substance abuse and documented severe and abuse and documented severe and persistent psychiatric disorderpersistent psychiatric disorder
Often homeless or recently released Often homeless or recently released from a psychiatric hospitalization from a psychiatric hospitalization
Unable to stop their substance use on Unable to stop their substance use on an outpatient basis, but don’t meet an outpatient basis, but don’t meet criteria for a psychiatric hospitalizationcriteria for a psychiatric hospitalization

Four-Quadrant Framework for Four-Quadrant Framework for CODCOD
Source: NASMHPD, NASADAD, 1998; NY State; Ries, 1993; SAMHSA Report to Congress, 2002Source: NASMHPD, NASADAD, 1998; NY State; Ries, 1993; SAMHSA Report to Congress, 2002
Less severemental disorder/
less severe substanceabuse disorder
More severemental disorder/
less severe substanceabuse disorder
More severemental disorder/
more severe substance
abuse disorder
Less severemental disorder/
more severe substance
abuse disorder
High severity
High severity
Lowseverity

Service Delivery for CODService Delivery for COD
Consultation between systems
Generally not eligible for public alcohol/drug or mental health services
Low to Moderate Psychiatric Symptoms/Disorders
And
Low to Moderate Severity Substance Issues/Disorders
Services provided in outpatient chemical dependency or mental health system
LOW - LOW HIGH - LOW
Collaboration between systems
Eligible for public mental health services but not alcohol/drug services
High Severity Psychiatric Symptoms/Disorders
And
Low to Moderate Severity Substance Issues/Disorders
Services provided in outpatient and inpatient mental health system
LOW - HIGH
Collaboration between systems
Eligible for public alcohol/drug services but not mental health services
Low to Moderate Psychiatric Symptoms/Disorders
And
High Severity Substance Issues/Disorders
Services provided in outpatient and inpatient chemical dependency system
HIGH - HIGH
Integration of services
Eligible for public alcohol/drug and mental health services
High Severity Psychiatric Symptoms/Disorders
And
High Severity Substance Issues/Disorders
Services provided in specialized treatment programs with cross-trained staff or multidisciplinary teams
Source: Ries, 2004

FSP & Concurrent Residential Drug FSP & Concurrent Residential Drug TreatmentTreatment
A model for integrated servicesA model for integrated services Provides a safe environment to Provides a safe environment to
address substance use and mental address substance use and mental health symptoms and to create a health symptoms and to create a joint treatment planjoint treatment plan
The Pilot StudyThe Pilot Study
Purpose – To identify promising Purpose – To identify promising practices supporting integrated services practices supporting integrated services for clients with co-occurring disordersfor clients with co-occurring disorders
What added value does the FSP team What added value does the FSP team serve while an FSP client is in residential serve while an FSP client is in residential drug/alcohol treatment?drug/alcohol treatment?
What are the unique roles of the FSP What are the unique roles of the FSP team and the residential team?team and the residential team?
How do the teams work together best?How do the teams work together best?
FSP Clinical Case ConferencesFSP Clinical Case Conferences
2 weeks after an adult FSP enrollee 2 weeks after an adult FSP enrollee enters residential drug/alcohol enters residential drug/alcohol treatment, a clinical case conference treatment, a clinical case conference will be initiated by the FSP program or will be initiated by the FSP program or the Service Area District Chief.the Service Area District Chief.
Clinical case conferences continue Clinical case conferences continue every 30 days until the client is every 30 days until the client is discharged from the residential discharged from the residential program.program.

Clinical Case ConferenceClinical Case Conference
Review treatment plan- client stage Review treatment plan- client stage of recovery and intervention of recovery and intervention strategiesstrategies
Identify unique services provided by Identify unique services provided by FSP team and residential treatment FSP team and residential treatment team.team.
Ensure services are not duplicatedEnsure services are not duplicated
Case Example #1Case Example #1
Mr. Vinnie Boom BotzMr. Vinnie Boom Botz 52 year old Hispanic male who has been diagnosed 52 year old Hispanic male who has been diagnosed
with Schizoaffective Disorder and alcohol with Schizoaffective Disorder and alcohol dependence.dependence.
Long history of ETOH dependenceLong history of ETOH dependence Patient suffers from head injury as a result of Patient suffers from head injury as a result of
sustaining a beating while intoxicated and sustaining a beating while intoxicated and homeless.homeless.
Due to patient’s Organic Brain Disorder, frequent Due to patient’s Organic Brain Disorder, frequent relapse on alcohol and other substances of abuse – relapse on alcohol and other substances of abuse – patient required stabilization on the residential unit.patient required stabilization on the residential unit.

Vinnie, ContinuedVinnie, Continued
Case consultation began immediately Case consultation began immediately between FSP Case Manager, FSP clinician between FSP Case Manager, FSP clinician and residential clinician and counselor.and residential clinician and counselor.
DMH was consulted as wellDMH was consulted as well As a result, patient was given a As a result, patient was given a
neuropsychological testing battery and neuropsychological testing battery and reports were written to advocate for reports were written to advocate for patient to receive SSI.patient to receive SSI.
Patient was approved for SSI.Patient was approved for SSI.
Vinnie, Cont.Vinnie, Cont.
Patient is currently living in sober livingPatient is currently living in sober living Patient attends community meetingsPatient attends community meetings Patient continues with FSP case Patient continues with FSP case
management and therapeutic servicesmanagement and therapeutic services Patient’s SSI payments are administered by Patient’s SSI payments are administered by
a third party as he is unable to manage his a third party as he is unable to manage his own finances.own finances.
Patient is receiving dental and medical Patient is receiving dental and medical servicesservices

Vinnie, Cont.Vinnie, Cont.
Patient has a strong connection with Patient has a strong connection with residential unit and with treatment residential unit and with treatment facility.facility.
Auditory and visual hallucinations Auditory and visual hallucinations remain, but have decreased in both remain, but have decreased in both quality and quantityquality and quantity
He has been able to recognize that He has been able to recognize that his hallucinations are not reality and his hallucinations are not reality and respond more appropriately to them.respond more appropriately to them.

Case Example #2Case Example #2
Mr. Jimmy RodzMr. Jimmy Rodz 27 year old Hispanic male diagnosed with 27 year old Hispanic male diagnosed with
Psychotic Disorder NOS and Poly-substance abuse Psychotic Disorder NOS and Poly-substance abuse and Methamphetamine Dependenceand Methamphetamine Dependence
Has short but extensive history of abusing drugsHas short but extensive history of abusing drugs Prior to age 18, client had been doing well, Prior to age 18, client had been doing well,
enrolled in college, and wanted to be a peace enrolled in college, and wanted to be a peace officer.officer.
Mother explained that she believes that the Mother explained that she believes that the community they lived in (high drug use), possibly community they lived in (high drug use), possibly influenced his extensive drug useinfluenced his extensive drug use

Jimmy Cont.Jimmy Cont.
Prior to FSP services, he was accepting sporadic mental Prior to FSP services, he was accepting sporadic mental health services due to client’s non-compliance with health services due to client’s non-compliance with recommended treatment. recommended treatment.
Client had numerous psychiatric hospitalizations while Client had numerous psychiatric hospitalizations while he was under the influence or coming down from using.he was under the influence or coming down from using.
When enrolled into FSP services, program also enrolled When enrolled into FSP services, program also enrolled and placed in a residential drug treatment facility.and placed in a residential drug treatment facility.
Client responded well to the structured treatment and Client responded well to the structured treatment and the Co-Occurring Disorder Treatment.the Co-Occurring Disorder Treatment.
FSP Program held weekly team meeting at which client’s FSP Program held weekly team meeting at which client’s case was discussed, and bi-monthly meetings with case was discussed, and bi-monthly meetings with residential drug treatment program and FSP treatment residential drug treatment program and FSP treatment team.team.

Jimmy Cont.Jimmy Cont.
Client graduated residential drug treatment Client graduated residential drug treatment and moved on to sober living. and moved on to sober living.
He continues to received FSP services and has He continues to received FSP services and has moved to independent living. moved to independent living.
Client has strong relationship with substance Client has strong relationship with substance abuse support groups in the community. abuse support groups in the community.
Currently, client has full-time employment and Currently, client has full-time employment and is planning to enroll in college. Client is planning to enroll in college. Client continues to remain sober since entering FSP continues to remain sober since entering FSP Program and Residential Drug Treatment.Program and Residential Drug Treatment.
Lessons LearnedLessons Learned
It is important to have available short-term It is important to have available short-term residential drug treatment in the continuum residential drug treatment in the continuum of care for individuals with severe mental of care for individuals with severe mental illness and severe substance abuse illness and severe substance abuse problemsproblems
Short-term residential drug treatment can Short-term residential drug treatment can provide the opportunity to conduct a provide the opportunity to conduct a thorough assessment of the individual’s thorough assessment of the individual’s psychiatric and psychosocial functioning psychiatric and psychosocial functioning when not using substanceswhen not using substances that is rarely that is rarely possible on an outpatient basis. possible on an outpatient basis.

Lessons LearnedLessons Learned
Mental health services can be initiated or Mental health services can be initiated or continued in an environment where their continued in an environment where their effectiveness can be better evaluated, given effectiveness can be better evaluated, given the controlled environment of residential the controlled environment of residential carecare
Mental health services can be coordinated Mental health services can be coordinated during treatment and continued after leaving during treatment and continued after leaving residential care in a seamless fashionresidential care in a seamless fashion
Frequent communication between AOD and Frequent communication between AOD and DMH providers is critical to provide DMH providers is critical to provide coordinated and integrated care. coordinated and integrated care.

Next StepsNext Steps
Expand the number of AOD providers Expand the number of AOD providers who can work with FSP programswho can work with FSP programs
Continue to refine and improve Continue to refine and improve communication and coordination of communication and coordination of carecare
Evaluate the effectiveness of Evaluate the effectiveness of providing residential AOD services in providing residential AOD services in improving outcomesimproving outcomes
Related Documents











