Bowel Ultrasound - More Than Just A Load Of Patricia Lacy Gandor, BS, RDMS, RVT, RT Ann & Robert H. Lurie Children’s Hospital of Chicago Department of Radiology May 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Bowel Ultrasound - More Than Just A Load Of 💩💩💩💩Patricia Lacy Gandor, BS, RDMS, RVT, RT Ann & Robert H. Lurie Children’s Hospital of Chicago Department of Radiology May 2017

No Disclosures
2

Objectives
• Recognize anatomy of the gastrointestinal tract. • Identify proper technique for gastrointestinal ultrasound. • Recognize common findings seen in the emergent setting of abdominal
pain and vomiting. - Hypertrophic pyloric stenosis - Enteritis - Obstruction - Appendicitis
3
Introduction
• Ultrasound is emerging as a reliable tool for bowel interrogation. • Lack of radiation and non-invasive properties make ultrasound especially
ideal for pediatric patients. • Certain challenges accompany bowel imaging - excessive contents and gas - pain level - lack of training • Special challenges face pediatric bowel imaging - symptoms can be misleading - late presentation
4

“Gut Signature”
• The gastrointestinal tract runs from the esophagus to the rectum • The wall has a multilayered appearance called the “gut signature” - alternating hypoechoic and hyperechoic layers • The “gut signature” appearance can help differentiate normal vs abnormal
5

Gut Signature
6
• Multiple layers comprise the bowel wall (inner-outer) - mucosa - submucosa - muscularis propria - serosa
Lumen

The Pyloric Sphincter• Thin band of smooth muscle which controls
the passage of stomach contents into the duodenum.
• Can use ultrasound to view contents pass through the pylorus.
7newhealthguide.org
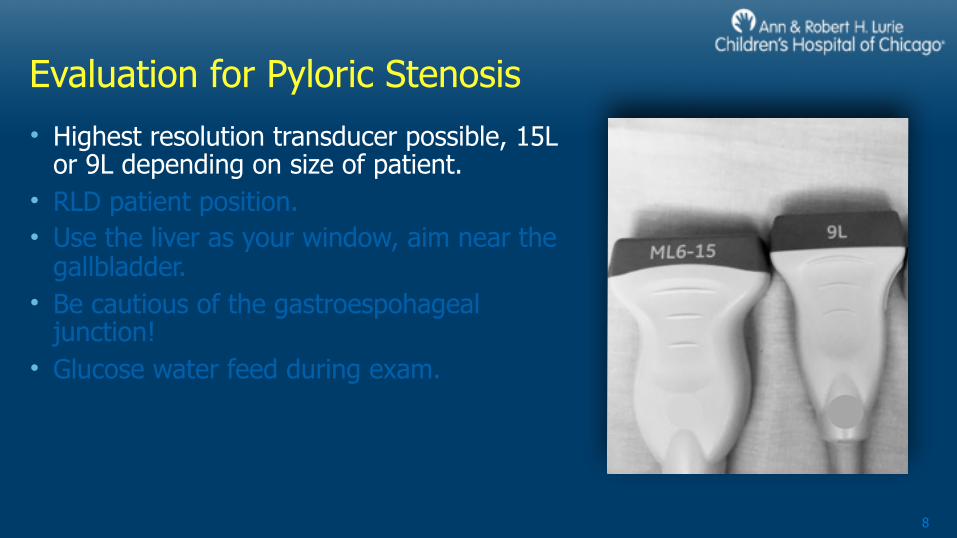
Evaluation for Pyloric Stenosis• Highest resolution transducer possible, 15L
or 9L depending on size of patient. • RLD patient position. • Use the liver as your window, aim near the
gallbladder. • Be cautious of the gastroespohageal
junction! • Glucose water feed during exam.
8

Evaluation for Pyloric Stenosis• Highest resolution transducer possible, 15L
or 9L depending on size of patient. • RLD patient position. • Use the liver as your window, aim near the
gallbladder. • Be cautious of the gastroespohageal
junction! • Glucose water feed during exam.
9
Evaluation for Pyloric Stenosis• Highest resolution transducer possible, 15L
or 9L depending on size of patient. • RLD patient position. • Use the liver as your window, aim near the
gallbladder. • Be cautious of the gastroespohageal
junction! • Glucose water feed during exam.
10
GB
pylorus

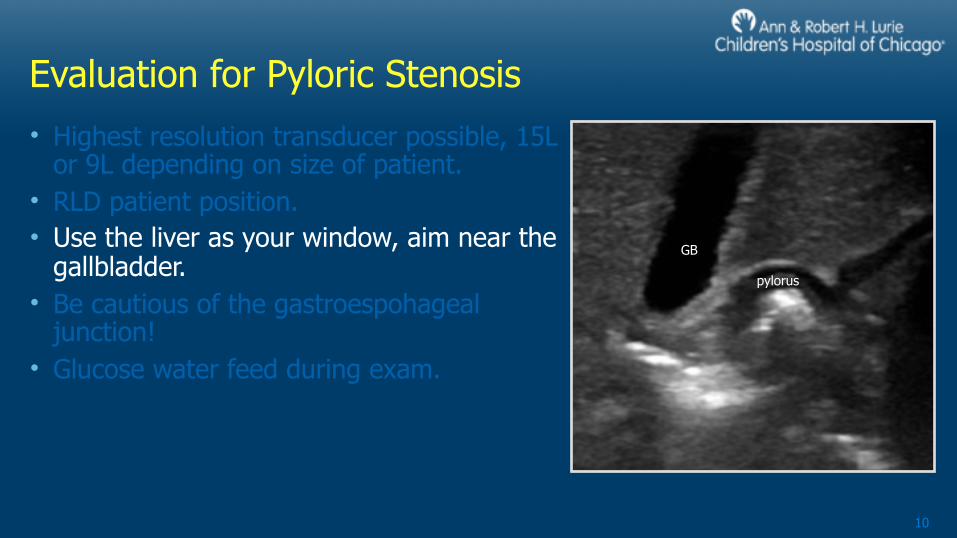
Evaluation for Pyloric Stenosis• Highest resolution transducer possible, 15L
or 9L depending on size of patient. • RLD patient position. • Use the liver as your window, aim near the
gallbladder. • Be cautious of the gastroespohageal
junction! • Glucose water feed during exam.
11
If you can see the hepatic veins, you’re probably looking at ge junction!! Feeding will run into stomach
Hepatic v.
Hepatic v.
ge junction
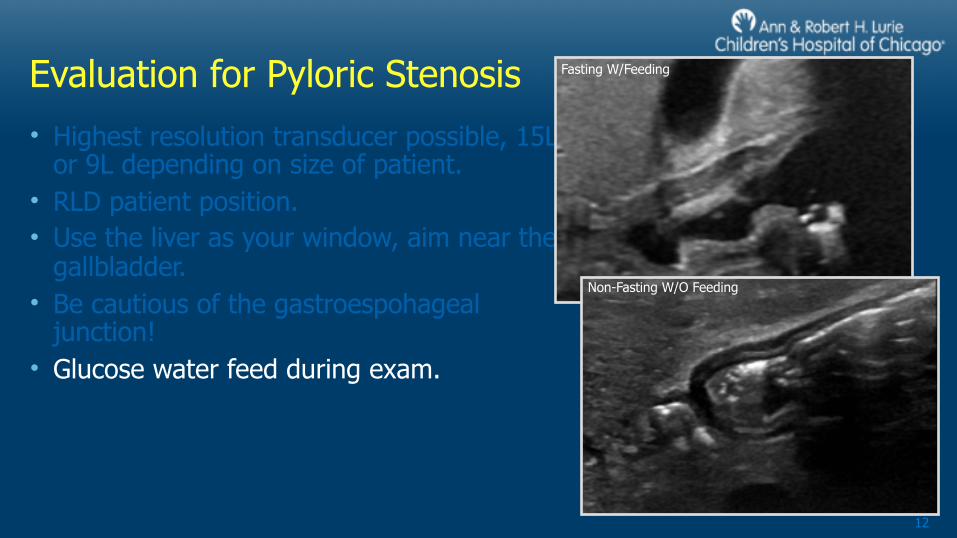
Evaluation for Pyloric Stenosis• Highest resolution transducer possible, 15L
or 9L depending on size of patient. • RLD patient position. • Use the liver as your window, aim near the
gallbladder. • Be cautious of the gastroespohageal
junction! • Glucose water feed during exam.
12
Fasting W/Feeding
Non-Fasting W/O Feeding
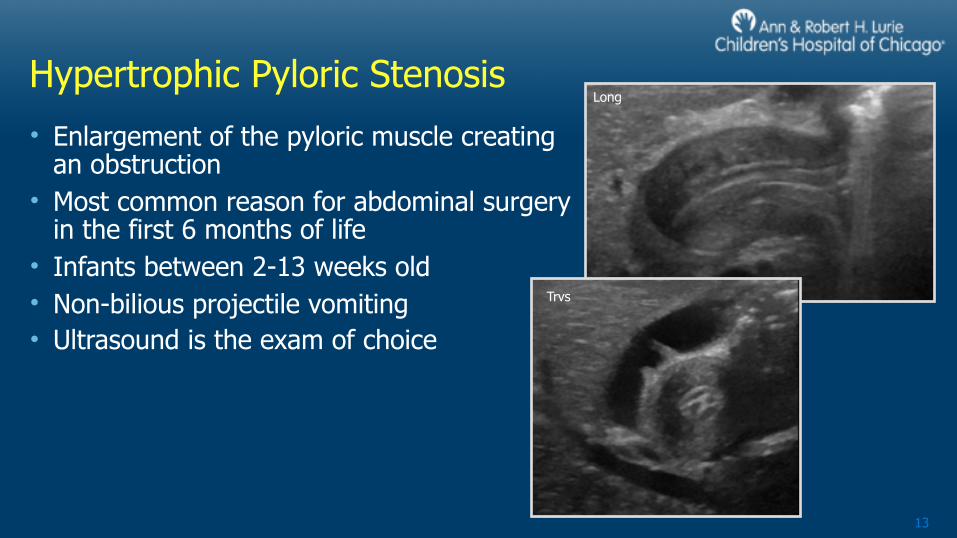
Hypertrophic Pyloric Stenosis• Enlargement of the pyloric muscle creating
an obstruction • Most common reason for abdominal surgery
in the first 6 months of life • Infants between 2-13 weeks old • Non-bilious projectile vomiting • Ultrasound is the exam of choice
13
Long
Trvs

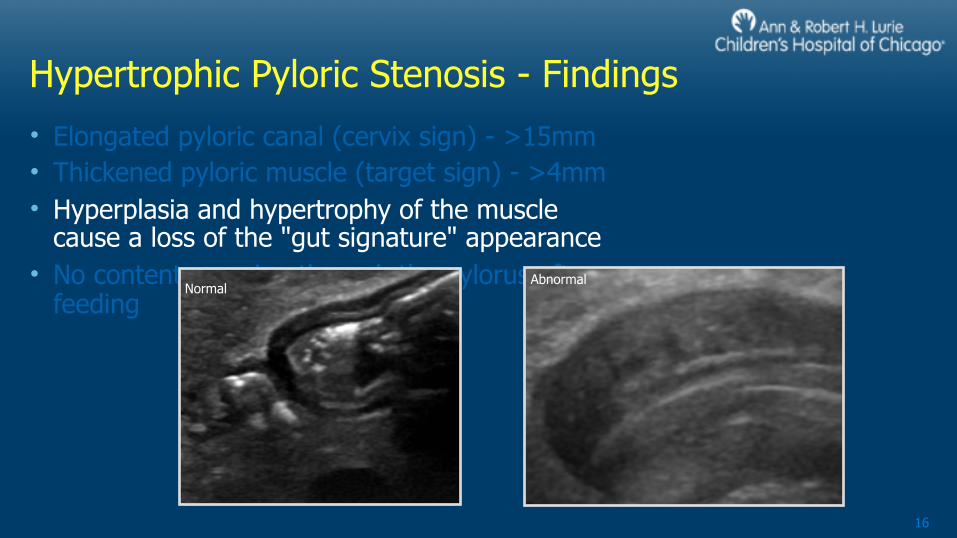
Hypertrophic Pyloric Stenosis - Findings• Elongated pyloric canal (cervix sign) - >15mm • Thickened pyloric muscle (target sign) - >4mm • Hyperplasia and hypertrophy of the muscle cause a loss of
the "gut signature" appearance • No contents passing through the pylorus after feeding
14
Normal Abnormal

Hypertrophic Pyloric Stenosis - Findings• Elongated pyloric canal (cervix sign) - >15mm • Thickened pyloric muscle (target sign) - >4mm • Hyperplasia and hypertrophy of the muscle
cause a loss of the "gut signature" appearance • No contents passing through the pylorus after
feeding
15
Normal Abnormal
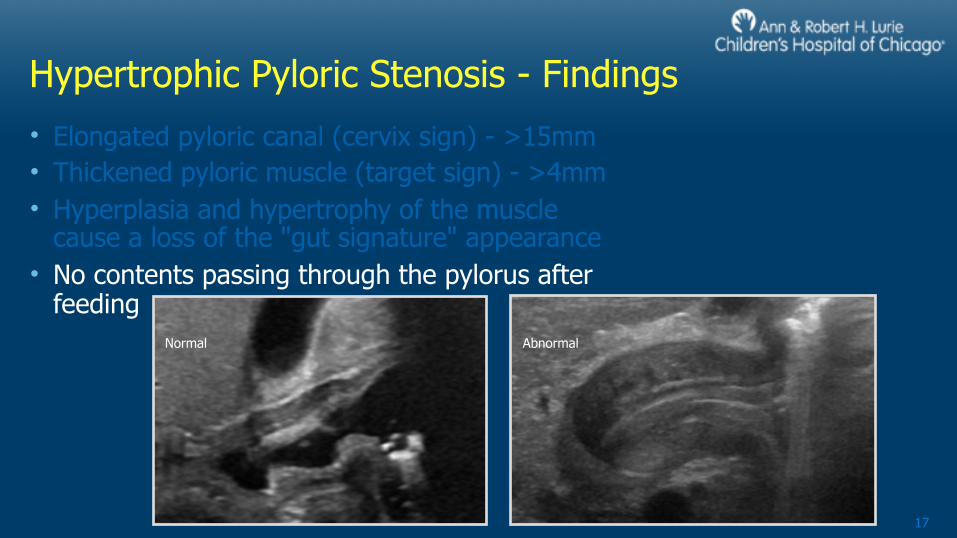
Hypertrophic Pyloric Stenosis - Findings• Elongated pyloric canal (cervix sign) - >15mm • Thickened pyloric muscle (target sign) - >4mm • Hyperplasia and hypertrophy of the muscle
cause a loss of the "gut signature" appearance • No contents passing through the pylorus after
feeding
16
NormalAbnormal
Hypertrophic Pyloric Stenosis - Findings• Elongated pyloric canal (cervix sign) - >15mm • Thickened pyloric muscle (target sign) - >4mm • Hyperplasia and hypertrophy of the muscle
cause a loss of the "gut signature" appearance • No contents passing through the pylorus after
feeding
17
Normal Abnormal

The Small Intestine• Extends from the pyloric sphincter to
ileocecal valve. • Responsible for digestion and absorption of
nutrients. • Divided into 3 sections: duodenum,
jejunum, ileum.
18
blausen.com

The Small Intestine - Normal Characteristics
• The jejunum has deep folds. • The ileum is smooth / small folds. • Normal wall has multiple layers seen and measures approx 3mm (varies
slightly with age). • Motility is rhythmic and propels the contents through the bowels.
19

The Small Intestine - Normal Characteristics
• The jejunum has deep folds. • The ileum is smooth / small folds. • Normal wall has multiple layers seen and measures approx 3mm (varies
slightly with age). • Motility is rhythmic and propels the contents through the bowels.
20

The Small Intestine - Normal Characteristics
• The jejunum has deep folds. • The ileum is smooth / small folds. • Normal wall has multiple layers seen and measures approx 3mm (varies
slightly with age). • Motility is rhythmic and propels the contents through the bowels.
21

The Small Intestine - Normal Characteristics
• The jejunum has deep folds. • The ileum is smooth / small folds. • Normal wall has multiple layers seen and measures approx 3mm (varies
slightly with age). • Motility is rhythmic and propels the contents through the bowels.
22

The Large Intestine• Extends from the ileocecal valve
to the rectum. • Responsible for water and salt
absorption. • Divided into 4 sections: - Ascending colon - Transverse colon - Descending colon - Sigmoid colon
23

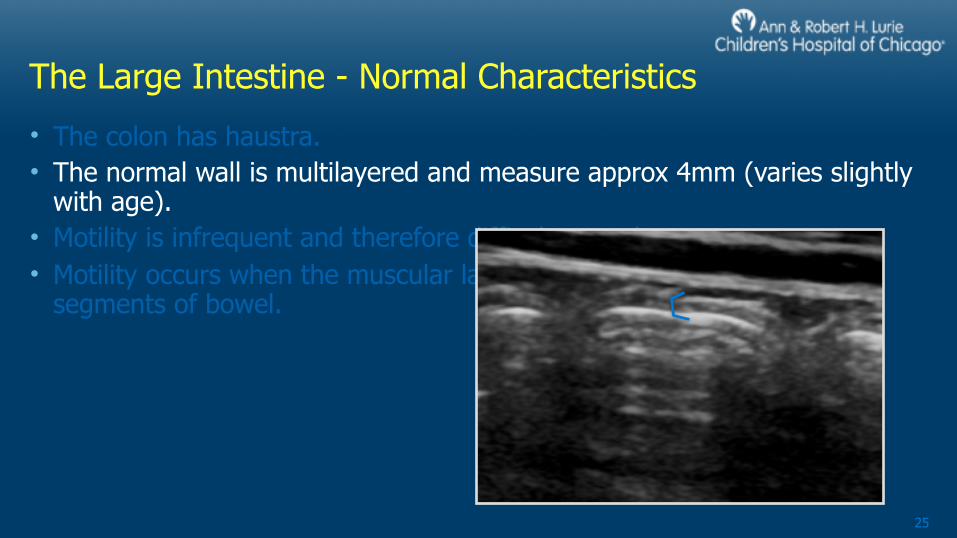
The Large Intestine - Normal Characteristics
• The colon has haustra. • The normal wall is multilayered and measure approx 4mm (varies slightly
with age). • Motility is infrequent and therefore difficult to evaluate. • Motility occurs when the muscular layer contracts and empties long
segments of bowel.
24
The Large Intestine - Normal Characteristics
• The colon has haustra. • The normal wall is multilayered and measure approx 4mm (varies slightly
with age). • Motility is infrequent and therefore difficult to evaluate. • Motility occurs when the muscular layer contracts and empties long
segments of bowel.
25

The Large Intestine - Normal Characteristics
• The colon has haustra. • The normal wall is multilayered and measure approx 4mm (varies slightly
with age). • Motility is infrequent and therefore difficult to evaluate. • Motility occurs when the muscular layer contracts and empties long
segments of bowel.
26

Technical Factors
• Highest resolution transducer • Harmonic imaging • High contrast settings - rejection - gray maps • Graded compression
27

Technical Factors
• Highest resolution transducer • Harmonic imaging • High contrast settings - rejection - gray maps • Graded compression
28

Technical Factors
• Highest resolution transducer • Harmonic imaging • High contrast settings - rejection - gray maps • Graded compression
29
Graded Compression

Imaging Planes
• Multiple slices in longitudinal and transverse.
• “Target scanning” is more accurate. • Follow colon along its path. • Use a lawn mower approach for the small
bowel.
30

Imaging Planes
• Multiple slices in longitudinal and transverse.
• “Target scanning” is more accurate. • Follow colon along its path. • Use a lawn mower approach for the small
bowel.
31

Enteritis
• Inflammation of the small intestine - inner and middle layer
• Can also involve the stomach and colon
• Can be caused by numerous reasons including - viral or bacterial infection - medication induced - poor blood flow - inflammatory conditions, Crohn’s disease
32
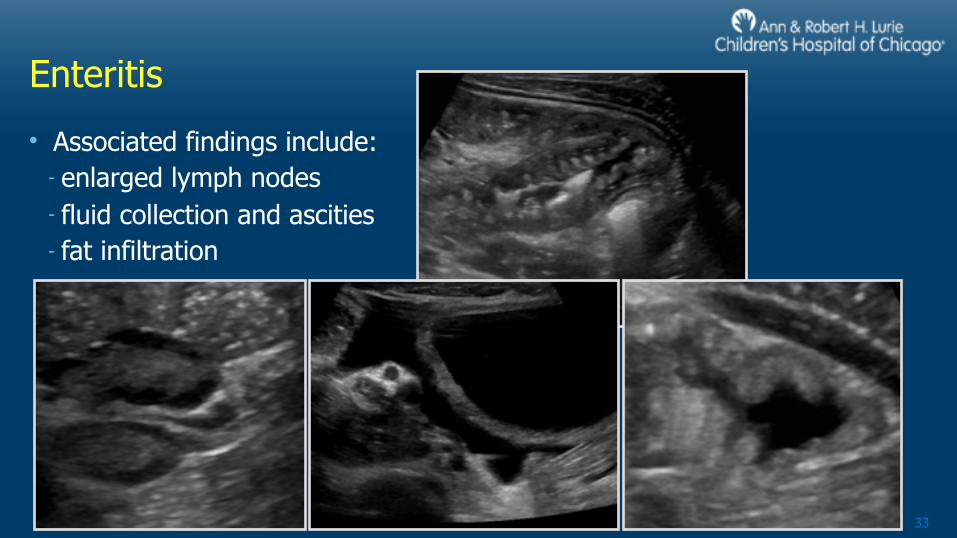
Enteritis
• Associated findings include: - enlarged lymph nodes - fluid collection and ascities - fat infiltration
33

Obstruction!!
• Can happen anywhere. • Can have many appearances. • May be complete or partial. - partial may not be seen with US. • Look for indirect signs. • Most common type of obstruction
is ileocecal intussusception.
34
electablog.com

Signs of Obstruction
• Contents do not move with bowel motility. • Dilated loops of bowel as well as collapsed loops of bowel. • Hypermotility with to-and-fro movement of bowel contents.
Potential Ischemia • Free fluid between distended loops of bowel. • Thickened bowel wall. • No motility.
35

Obstruction! Intussusception
36
• Intussusception is the most common medical emergency affecting children under 3 years old, with a peak age of 6 months - 1 year.
• More common in boys, 3:2 ratio. • It’s an invagination of one portion of
intestine into another. • Usually idiopathic, but may have a lead
point. • Look for “donut sign” in trvs and
“pseudokidney" sign in long


Appendicitis - Evaluation
• Find the ileocecal valve - Looking at the cecum in transverse - Find the location of ileum dumping into cecum near RLQ (appendix is approx 1.5cm away from ileocecal valve
• Can be in any direction around cecum • Use graded compression as well as simultaneous anterior/posterior
compression.
38
Terminal Ileum
Colon Appendix Cecum
Bladder A
V
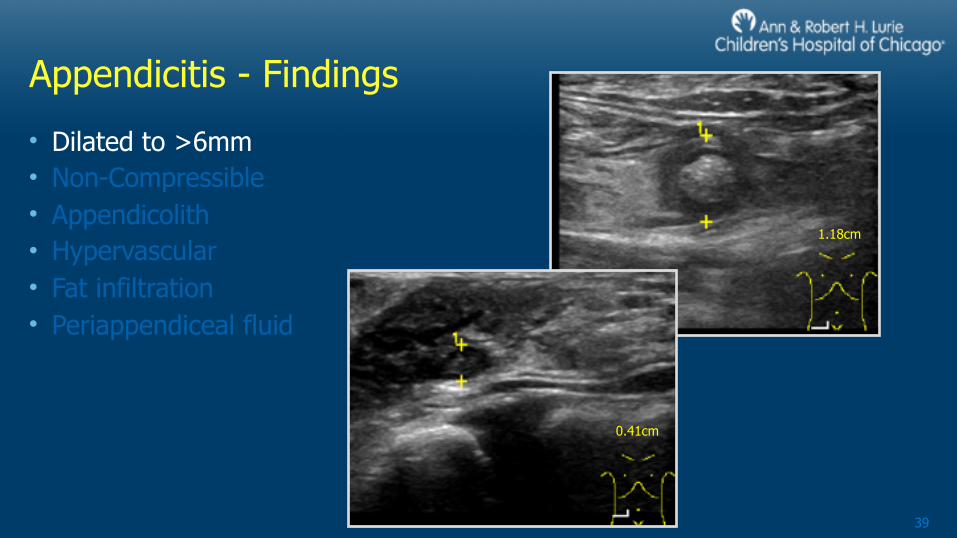
Appendicitis - Findings
• Dilated to >6mm • Non-Compressible • Appendicolith • Hypervascular • Fat infiltration • Periappendiceal fluid
39
1.18cm
0.41cm

Appendicitis - Findings
• Dilated to >6mm • Non-Compressible • Appendicolith • Hypervascular • Fat infiltration • Periappendiceal fluid
40

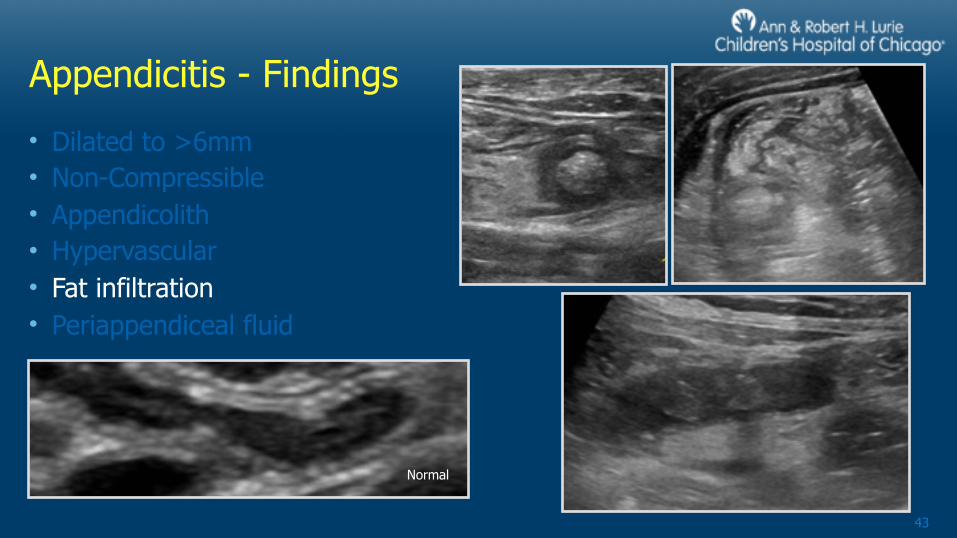
Appendicitis - Findings
• Dilated to >6mm • Non-Compressible • Appendicolith • Hypervascular • Fat infiltration • Periappendiceal fluid
41

Appendicitis - Findings
• Dilated to >6mm • Non-Compressible • Appendicolith • Hypervascular • Fat infiltration • Periappendiceal fluid
42
Appendicitis - Findings
• Dilated to >6mm • Non-Compressible • Appendicolith • Hypervascular • Fat infiltration • Periappendiceal fluid
43
Normal

Appendicitis - Findings
• Dilated to >6mm • Non-Compressible • Appendicolith • Hypervascular • Fat infiltration • Periappendiceal fluid
44

Conclusion
• Advances in sonographic resolution has opened a door in the evaluation of numerous gastrointestinal abnormalities.
• We must do out part by learning this relatively "new" exam type. • Sonography is an ideal choice because it is highly accurate, portable, not-
invasive, fast, lacks radiation, and is cost-effective.
45

References
1.Tarantino, L. (n.d.). Abdominal Ultrasound in Infectious Enteritis. Retrieved April 21, 2017, from touchophthalmology.com
2.Chao, A., & Gharahbaghian, L. (n.d.). Tips and Tricks: Clinical Ultrasound for Small Bowel Obstruction - A Better Diagnostic Tool? Retrieved April 21, 2017, from acep.org
3.Park, N. H. (2011). Ultrasonography of normal and abnormal appendix in children. World Journal of Radiology, 3(4), 85. doi:10.4329/wjr.v3.i4.85
4.Riccabona, M. (2014). Pediatric Ultrasound Requisites and Applications. Graz, Austria: Springer. Doi: 10.1007/978-3-642-39156-9
5.blausen.com staff (2014). “Medical gallery of Blausen Medical 2014”. WikiJournal of Medicine 1(2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436.N.
6.Acute Appendicitis. (2013). Retrieved April 21, 2017, from https://pedclerk.uchicago.edu/page/acute-appendicitis
46
Related Documents











