Bowel Obstruction Bowel Obstruction Tad Kim, M.D. Connie Lee, M.D.

Bowel Obstruction Tad Kim, M.D. Connie Lee, M.D..
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Bowel Obstruction
Bowel Obstruction
Tad Kim, M.D.Connie Lee, M.D.

Bowel Obstruction
Definitions• Ileus = obstruction 2/2 dysfunctional
motility of bowel
• Mechanical obstruction = 85% SB, 15% large bowel
• Simple obstruction
• Closed loop obstruction
• Strangulation

Bowel Obstruction
SBO: Etiology• Adhesion #1 (80-90% of SBO in pt’s w/prior abdominal surgery)• Hernia #2 overall - #1 cause of SBO in pts w/o prior abdominal
surgery• Tumor• Abscess• Hematoma• Annular pancreas• SMA syndrome• Congenital lesions• Gallstone ileus• Intussusception• Foreign body (bezoars, worms, etc)• Meconium ileus• Malrotation

Bowel Obstruction
Colonic Obstruction: Etiology• Cancer #1 (60%)• Volvulus (sigmoid > cecum)• Adhesions• Hernia• UC• Diverticulitis• Congenital lesions• Fecal impaction• Adynamic ileus• Hirschsprung’s• Meconium ileus• Foreign body

Bowel Obstruction
Age & DDx• Age matters!
– Neonate: meconium ileus, Hirschsprung’s, malrotation, atresia
– Child: intussusception, Hirschsprung’s– Adult: hernia, IBD, CA, diverticular disease– Elderly: CA, diverticular disease, Ogilvie’s

Bowel Obstruction
History & DDx
• Proximal obstruction: early bilious vomiting, +flatus/BM• Distal obstruction: obstipation, distension, vomiting feculent material
(2/2 bacterial overgrowth of SB contents)• Pain w/obstruction: begins as cramping pain, changes to continuous
severe pain w/strangulation & peritonitis• PMHx: remember to ask about cardiac history (arrhythmias, prior
MI, Afib - think about intestinal ischemia), IBD, gallstones, cancer• PSHx: remember to ask about ostomy output• Meds: narcotics (ileus), antipsychotics (ileus), diuretics (hypoK a/w
ileus)• ROS: recent weight loss (CA, SMA syndrome)
Bowel Obstruction
PE• Start with ABCs• Look for surgical scars• Bowel sounds • Distention: distal obstruction >> proximal• Localized tenderness: think peritonitis• Look for hernias/masses• Do a rectal exam

Bowel Obstruction
Labs• WBC (nml in uncomplicated SBO)
• CBC (anemia w/CA)
• BMP (hypoK)
• Alkalosis (a/w proximal obstruction)
• Acidosis (a/w bowel infarction)
• Amylase (may be elevated in SBO)

Bowel Obstruction
Studies
• Upright CXR: look for free air• Flat and upright/left lateral decubitus: look for
dilated bowel loops, air-fluid levels• Note: if cecal diameter >12cm, there is a risk of
perforation. At 12-14cm, the wall tension > perfusion pressure, increasing risk of necrosis
• Barium enema• UGI series w/SB follow-through• CT scan

Bowel Obstruction
SBO: Management
• NPO, NGT, Foley, IVF• Electrolyte replacement• Many partial obstructions will resolve• “Don’t let the sun set on a (complete) SBO”• Complete bowel obstruction w/concern for
strangulation/perforation requires immediate operative intervention (resuscitate first)

Bowel Obstruction
Dedouit F and Otal P. N Engl J Med 2008;358:1381
A 72-year-old woman presented with a 2-day history of abdominal pain associated with nausea and vomiting

Bowel Obstruction
Liu K and Lin B. N Engl J Med 2007;356:1152
A 48-year-old healthy woman presented with anorexia of 2 days' duration and abdominal pain in the right lower quadrant

Bowel Obstruction
Jang M and Lee K. N Engl J Med 2008;358:e16
A 60-year-old woman presented to the outpatient clinic with vague abdominal discomfort that had developed over the previous several weeks
Bowel Obstruction
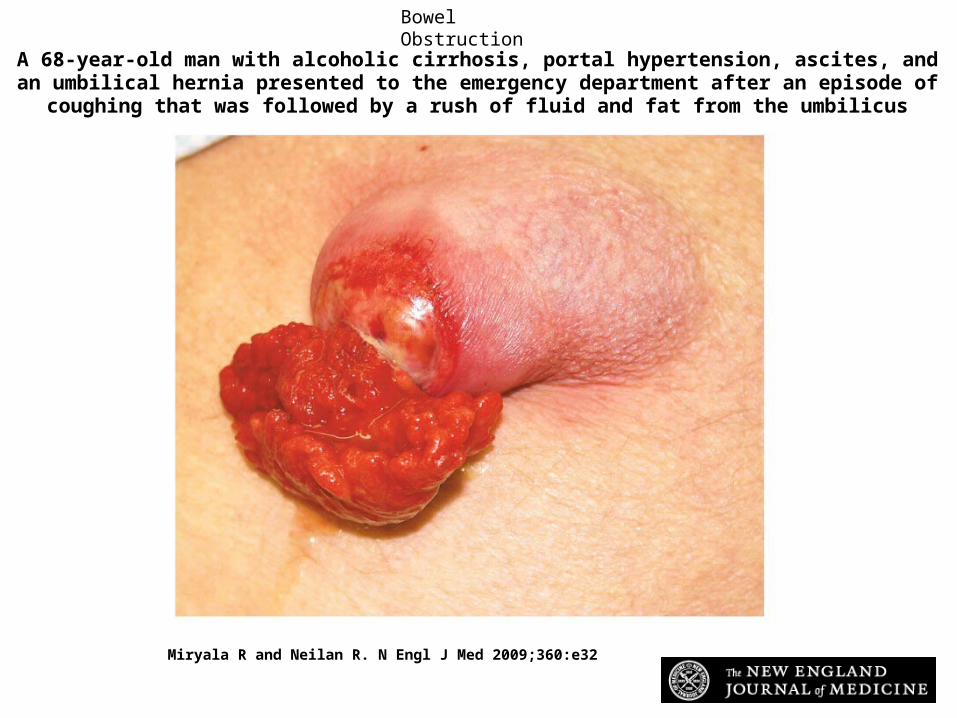
Miryala R and Neilan R. N Engl J Med 2009;360:e32
A 68-year-old man with alcoholic cirrhosis, portal hypertension, ascites, and an umbilical hernia presented to the emergency department after an episode of coughing that was followed by a
rush of fluid and fat from the umbilicus

Bowel Obstruction
Avolio L and Martucciello G. N Engl J Med 2009;360:2770
Ingested magnets

Bowel Obstruction
Rosmarin D and Tan C. N Engl J Med 2006;355:601
A 68-year-old man with chronic dysuria and increased urinary frequency presented with three weeks of weakness and fever

Bowel Obstruction
Traub S et al. N Engl J Med 2003;349:2519-2526
Radiographic Findings in Body Packers

Bowel Obstruction
Graham J and Rothwell B. N Engl J Med 2004;351:1119
An 83-year-old woman was hospitalized with nausea, vomiting, and obstipation

Bowel Obstruction
Chan D. N Engl J Med 2006;355:1714
A previously healthy 102-year-old woman was admitted with abdominal pain and a 3-day history of vomiting

Bowel Obstruction
Kurer M and Chintapatla S. N Engl J Med 2007;356:1656
A 64-year-old woman with ulcerative colitis presented with abdominal pain

Bowel Obstruction
Take Home Points• Always start with ABC, resuscitation
– Includes 2 large bore IV, Foley, NGT, monitor
• DDX is simple:– SBO: Adhesions, Bulges, Cancer, Crohn’s– LBO: CANCER, Volvulus, Diverticulitis
• Labs to assess dehydration & leukocytosis• Imaging to assess obstruction & etiology• If hypoTN/shock, “toxic”, or signs of
strangulation or ischemia, resusc & OR stat• Otherwise, for SBO, NGT & treat etiology• LBO is different: really must rule out cancer,
colonoscopy plays a larger role than w SBO
Related Documents











