9/22/2009 1 PMB Review Introductory remarks at Clinical Advisory Committee meetings August and September 2009 Boshoff Steenekamp REF Project Specialist Process to date • PMB Review workshops early in 2008 • 3 drafts of a PMB review consultation document • Numerous stakeholder submissions on these drafts

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

9/22/2009
1
PMB ReviewIntroductory remarks at Clinical Advisory
Committee meetings
August and September 2009
Boshoff Steenekamp
REF Project Specialist
Process to date
• PMB Review workshops early in 2008
• 3 drafts of a PMB review consultation document
• Numerous stakeholder submissions on these drafts

9/22/2009
2
Number of individuals involved
Cla
ims
cost
per
ben
efic
iary
Few Many
Low
HighClaims cost per
beneficiary
Ab
ove
-th
resh
old
ben
efit
s fo
r al
l PM
Bs
Bel
ow
-th
resh
old
ben
efit
s fo
r sp
ecif
ied
se
rvic
es a
nd
co
nd
itio
ns
Hig
h c
ost
eve
nts
co
vere
d t
hro
ugh
PM
Bs
(mo
stly
in h
osp
ital
)
CD
L an
d o
ther
co
nd
itio
ns
on
cat
ego
rica
l lis
t
Spec
ifie
dse
rvic
esDay-to-day expenses on an out-of-
pocket basis or paid from MSA
EDL
Frequently raised matters
• EDL inappropriate in current environment
– The intention of the EDL list is not to limit medicine use to drugs on this list, but simply to state that any of the drugs on the list must be covered from first Rand
• Exclusions: Annexure I
– The intention is that these conditions should excluded within the specified setting, not a general exclusion
• Challenges
– Constitutional rights, mandate of DoH & Council

9/22/2009
3
Concurrent Processes impacting on revised PMB regulations
Number of individuals involved
Cla
ims
cost
per
ben
efic
iary
Few Many
Low
HighClaims cost per
beneficiary
Ab
ove
-th
resh
old
ben
efit
s fo
r al
l PM
Bs
Bel
ow
-th
resh
old
ben
efit
s fo
r sp
ecif
ied
se
rvic
es a
nd
co
nd
itio
ns
Hig
h c
ost
eve
nts
co
vere
d t
hro
ugh
PM
Bs
(mo
stly
in h
osp
ital
)
CD
L an
d o
ther
co
nd
itio
ns
on
cat
ego
rica
l lis
t
Spec
ifie
dse
rvic
es
Day-to-day expenses on an out-of-pocket basis or paid from MSA
Proposed Essential Care Package
NHI Process
Technical analysis of economic
impact, affordability
pricing, construct,
related reforms
Clinical Advisory
committees
Drafting of Regulations
Stakeholder comments
Governance Structure
STEERING
COMMITTEE
PROJECT
MANAGER
HEALTHCARE
INTERVENTIONSREF PRICING
Participative
Co
nsu
ltat
ive

9/22/2009
4
Sources for consideration
• Existing PMB regulations
• Third draft of the PMB review consultation document
• Stakeholder comments on the consultation document relevant to the specific advisory committee
• Final submissions by committee members to the committee
Terms of reference
I. BackgroundII. Policy FrameworkIII. Composition of clinical advisory committees (CACs)IV. Criteria for evaluating a recommendationV. Role of the ChairVI. Code of conduct for CAC membersVII.Logistics
Annexure A: Clinical Advisory Committee agenda items, meeting dates, and relevant comments on the PMB review consultation documents

9/22/2009
5
IV. Criteria for evaluating a recommendation
Submitted recommendations must comply with the principles of evidence-based medicine decision making and therefore it is crucial that sufficiently detailed information on how the evidence was obtained is provided. In addition, the criteria outlined below should be adhered to:
1. Clinical effectiveness2. Degree of discretion3. Urgency4. Cost-effectiveness/ economic evaluation5. The health benefits of the recommendation should be compared
with the next best available alternative treatment. If possible a balance sheet of the benefits, harms and major costs of recommendation should be itemised against those of the available alternative
Degree of discretion
Apply principles Apply principles Apply principles
Apply principles Apply principles Exclusion
Exclusion Exclusion Exclusion
Discretion
Med
ical
nec
essi
ty
Low Medium High
Low
Medium
High
9/22/2009
6
The health benefits
• The health benefits of the recommendation should be compared with the next best available alternative treatment. If possible a balance sheet of the benefits, harms and major costs of recommendation should be itemised against those of the available alternative
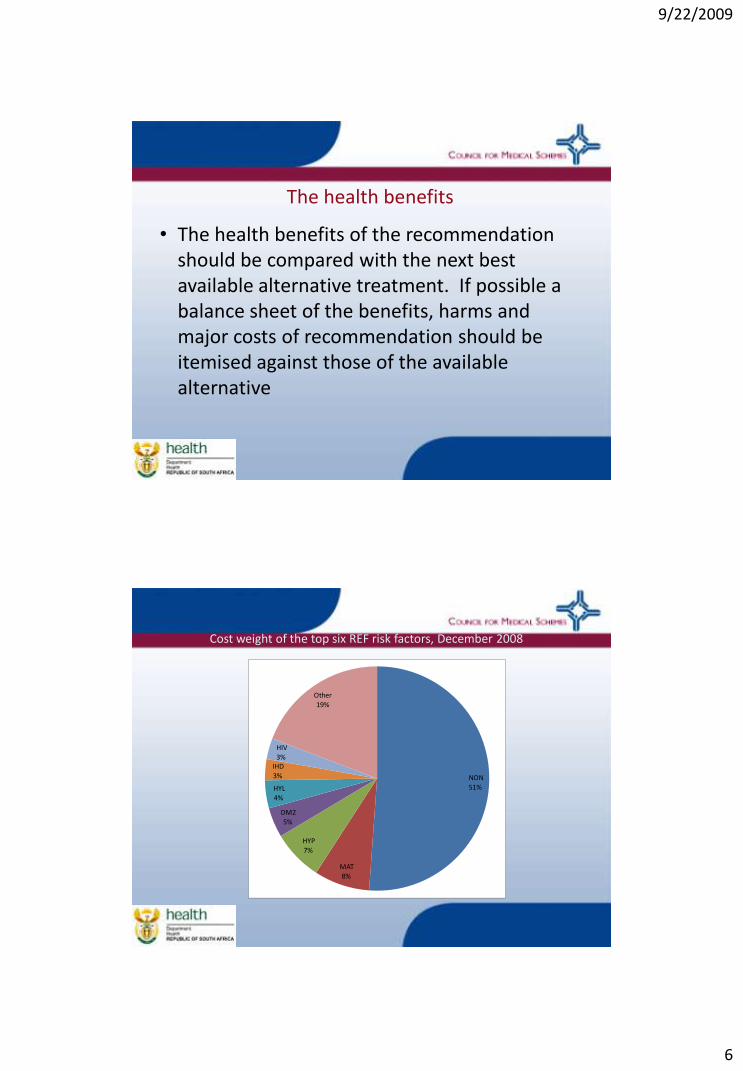
Cost weight of the top six REF risk factors, December 2008
NON 51%
MAT 8%
HYP 7%
DM2 5%
HYL 4%
IHD 3%
HIV 3%
Other19%

9/22/2009
7
CDL groups
Lifestyle diseases HYP, IHD, HYL, DM2
Other cardiac CMY, CHF, DYS
Multiple chronic diseases CC2, CC3, CC4
Psychiatric BMD, SCZ
Renal CRF
Respiratory AST, COP, BCE
Endocrine DM1, TDH, ADS, DBI
Neurologic EPL, MSS
Autoimmune RHA, SLE, CSD, IBD
Other HAE, PAR, GLC
Total REF risk factor cost load by CDL groupDecember 2008
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
R 0
R 20,000,000
R 40,000,000
R 60,000,000
R 80,000,000
R 100,000,000
R 120,000,000
R 140,000,000
R 160,000,000
R 180,000,000
R 200,000,000
Un
de
r 1
1-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
75
-79
80
-84
85
+
NON Lifestyle diseases MAT Multiple chronic diseases
Other cardiac Respiratory HIV Endocrine
Renal Neurologic Psychiatric Other
Autoimmune Population

9/22/2009
8
Cost pbpm of the REF risk factors by age and CDL groupDecember 2008
R 0
R 200
R 400
R 600
R 800
R 1,000
R 1,200
Un
de
r 1
1-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
75
-79
80
-84
85
+
Axi
s Ti
tle
NON Lifestyle diseases MAT Multiple chronic diseases Other cardiac
Respiratory HIV Endocrine Renal Neurologic
Psychiatric Other Autoimmune
Cost pbpm of the REF risk factors by age and CDL groupDecember 2008
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
R 0
R 200
R 400
R 600
R 800
R 1,000
R 1,200
Un
de
r 1
1-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
75
-79
80
-84
85
+
Axi
s Ti
tle
NON Lifestyle diseases MAT Multiple chronic diseases
Other cardiac Respiratory HIV Endocrine
Renal Neurologic Psychiatric Other
Autoimmune Population

9/22/2009
9
Cost pbpm of the REF risk factors by age and CDL groupDecember 2008
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
R 0
R 200
R 400
R 600
R 800
R 1,000
R 1,200
Un
de
r 1
1-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
75
-79
80
-84
85
+
Axi
s Ti
tle
NON Lifestyle diseases MAT Multiple chronic diseases
Other cardiac Respiratory HIV Endocrine
Renal Neurologic Psychiatric Other
Autoimmune ICR Population
V. Role of the Chair
The Chair of each of the CACs will be appointed by the Steering committee and will be briefed by the project manager on the scope of the project.The chair will:
1. Guide the task of developing final recommendations and the process thereof.
2. Assist the team to work collaboratively and effectively together ensuring that there is balanced contribution from all members.
3. Steer the discussion according to the agenda4. Summarise the main points and key decisions from the debate,
noting any points of disagreement.5. Sign off minutes compiled the secretariat.

9/22/2009
10
VII. Logistics
1.Committee members must review the comments made by other stakeholders as listed in Annexure A and submit their final proposals at least seven days prior to the scheduled meeting.
2.The chairperson of each advisory committee must make final recommendations to the PMB Review Steering Committee by 29 September 2009.
REF data relevant to this committee
• Paediatric Asthma *
• Paediatric Epilepsy *
• Cystic Fibrosis
• Neonatal Ventilation
* REF data available

9/22/2009
11
Dec-2008AllSchemesAdmin: All Administrators
Number of beneficiaries: 7,812,388; Actual reported: 86,241
Asthma
Industry average: 112,826; Scheme-specific: 112,771
0
5,000
10,000
15,000
20,000
25,000
30,000
Un
der
1
1-4
5-9
10-1
4
15-1
9
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80-8
4
85+
Nu
mb
er
of
Ben
efi
cia
ries
Lower Bound Upper Bound ActualScheme-Specific Industry average HIGH2!LOW2!
AsthmaAllSchemesAdmin: All Administrators
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
Ja
n-2
008
Fe
b-2
00
8
Ma
r-2008
Apr-
2008
Ma
y-2
008
Ju
n-2
008
Ju
l-2008
Au
g-2
00
8
Se
p-2
00
8
Oc
t-2008
No
v-2
008
De
c-2
008
Actual
Expected
DIN
Asthma
Amount from REF by Condition Dec-2008
Diff (A-E) Expected Actual
Asthma -11,290,581 58,274,568 46,983,987

9/22/2009
12
Dec-2008
Industry average: 25,171; Scheme-specific: 25,171
AllSchemesAdmin: All Administrators
Number of beneficiaries: 7,812,388; Actual reported: 26,018
Epilepsy
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
Un
der
1
1-4
5-9
10-1
4
15-1
9
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80-8
4
85+
Nu
mb
er
of
Ben
efi
cia
ries
Lower Bound Upper Bound ActualScheme-Specific Industry average HIGH2!LOW2!
EpilepsyAllSchemesAdmin: All Administrators
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
Ja
n-2
008
Fe
b-2
00
8
Ma
r-2008
Apr-
2008
Ma
y-2
008
Ju
n-2
008
Ju
l-2008
Au
g-2
00
8
Se
p-2
00
8
Oc
t-2008
No
v-2
008
De
c-2
008
Actual
Expected
DIN
Epilepsy
Amount from REF by Condition Dec-2008
Diff (A-E) Expected Actual
Epilepsy 1,091,391 24,912,260 26,003,651

9/22/2009
13
Purpose of today’s meeting
• Consider the respective agenda items in view of – Existing regulations
– Proposals made in the 3rd draft of the PMB review document
– Stakeholder comments on the 3rd drafthttp://www.medicalschemes.com/publications/publications.aspx?catid=33&selectId=199
– Final submissions must be introduced by committee members
• No time for additional presentations or the introduction of new items

9/22/2009
14

9/22/2009
15
Draft Asthma: Respiratory Committee
Short acting
ß2 agonists
as needed
(Only for mild
intermittent
asthma)
Low dose
ICS
(250-500 μg/day
(BDP)
equivalent
Low dose ICS
+
Long-acting ß2
agonists
OR
Leukotriene modifier
OR
ICS
(500-1000 μg/day
BDP equivalent)
Moderate dose ICS
(500-1000 ug/day
BDP equivalent)
+
agonists
OR
Leukotriene
modifier
OR
Slow -release
theophyllines
High dose ICS
(>1000 ug/day
BDP equivalent)
+
Long-acting ß2
agonists
±
Leukotriene
modifier
±
Slow-release
theophyllines
High dose ICS
+
Long-acting ß2
agonists
±
Leukotriene
modifier
±
Slow-release
theophyllines
±
Oral
corticosteroids
Diagnosis and
assessment of severity
Short-acting ß2 agonist by inhalation as needed for acute symptom relief
Implement treatment in
accordance with severity level
Mild Mild Moderate Severe
PARTLY CONTROLLED:
Check adherence and
inhaler technique
Step up treatment
UNCONTROLLED:
Check adherence and
inhaler technique
Step up treatment
Assess control
CONTROLLED:
Consider step down if
controlled
for 3 or more months
Glossary:
ICS – Inhaled corticosteroid
BDP equivalent - Beclomethasone dipriopionate equivalent
PEF – Peak expiratory flow
Applicable ICD-10 Coding:
Note:
Assessment of Asthma severity
Intermittent Chronic persistent
Severity Mild Mild Moderate Severe
Daytime symptoms ≤2 / week 3-4 / week > 4 / week Continuous
Night symptoms ≤1 / month 2- 4 / month > 4 / month Frequent
PEF ≥ 80% ≥ 80% 60 – 80% < 60%
Assessment of Asthma control
CHARACTERISTIC CONTROLLED
(All of the following)
PARTLY CONTROLLED
(Any measure present in
any week)
UNCONTROLLED
Daytime symptoms ≤2 / week ≥ 2 / week 3 or more features of partly controlled asthma in any week
Limitation of activities None Any
Nocturnal symptoms/
awakening
None Any
Need for reliever/ rescue
treatment
≤2 / week ≥ 2 / week
Lung function (PEF/FEV1) Normal <80% predicted or personal
best (if known)
Exacerbations None 1 or more per year 1 in any week

9/22/2009
16
Draft Epilepsy: Neurology committee
Absent seizures:
Ethosuximide and / or Valproate
Diagnosis
Tonic clonic or partial seizures:
First Line drugs:
Phenobarbitone, Phenytoin, Carbamazepine, Valproate, and Primidone
Control not achieved or 1st line drugs not tolerated or contraindicated
Second Line drugs:
Consider Lamitrogen, Topiramate, and Levetiracetam
Combination therapy may be required to achieve control
Consider:
Neurosurgery
Vagal Stimulator
Ketogenic diet
Control not achieved through the combination of 1st and / or 2nd line
drugs, or drugs not tolerated or contraindicated

9/22/2009
17
Applicable ICD-10 Coding:
G40 Epilepsy
•G40.0 Localization-related (focal)(partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset
•G40.1 Localization-related (focal)(partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures
•G40.2 Localization-related (focal)(partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures
•G40.3 Generalized idiopathic epilepsy and epileptic syndromes
•G40.4 Other generalized epilepsy and epileptic syndromes
•G40.5 Special epileptic syndromes
•G40.6 Grand mal seizures, unspecified (with or without petit mal)
•G40.7 Petit mal, unspecified, without grand mal seizures
•G40.8 Other epilepsy
•G40.9 Epilepsy, unspecified
•G41 Status epilepticus
•G41.0 Grand mal status epilepticus
•G41.1 Petit mal status epilepticus
•G41.2 Complex partial status epilepticus
•G41.8 Other status epilepticus
•G41.9 Status epilepticus, unspecified
Note:
1. Medical management reasonably necessary for the delivery of treatment described in this algorithm is included within this
benefit, subject to the application of managed health care interventions by the relevant medical scheme.
2. To the extent that a medical scheme applies managed health care interventions in respect of this benefit, for example
clinical protocols for diagnostic procedures or medical management, such interventions must:
a. not be inconsistent with this algorithm;
b. be developed on the basis of evidence-based medicine, taking into account considerations of cost-
effectiveness and affordability; and
c. comply with all other applicable regulations made in terms of the Medical Schemes Act, 131 of 1998
3. This algorithm may not necessarily always be clinically appropriate for the treatment of children. If this is the case,
alternative paediatric clinical management is included within this benefit if it is supported by evidence-based medicine,
taking into account considerations of cost-effectiveness and affordability.
Structure of today’s meeting
• Introduction – CMS / DoH
• Agenda items
– Regulations, Third draft proposals, Submissions & Summaries
• Lunch
• Attendance list

9/22/2009
18
THANK YOU
Related Documents











