www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0 1 Review Bordetella holmesii: an under-recognised Bordetella species Laure F Pittet, Stéphane Emonet, Jacques Schrenzel, Claire-Anne Siegrist, Klara M Posfay-Barbe Bordetella holmesii, first described in 1995, is believed to cause both invasive infections (bacteraemia, meningitis, endocarditis, pericarditis, pneumonia, and arthritis) and pertussis-like symptoms. Infection with B holmesii is frequently misidentified as being with B pertussis, the cause of whooping cough, because routine diagnostic tests for pertussis are not species-specific. In this Review, we summarise knowledge about B holmesii diagnosis and treatment, and assess research needs. Although no fatal cases of B holmesii have been reported, associated invasive infections can cause substantial morbidities, even in previously healthy individuals. Antimicrobial treatment can be problematic because B holmesii’s susceptibility to macrolides (used empirically to treat B pertussis) and third-generation cephalosporins (often used to treat invasive infections) is lower than would be expected. B holmesii’s adaptation to human beings is continuing, and virulence might increase, causing the need for better diagnostic assays and epidemiological surveillance. Introduction Bordetella holmesii, a Gram-negative bacterium was first described as a cause of bacteraemia in patients with comorbidities such as asplenia. 1,2 The bacterium was also recovered in nasopharyngeal samples in otherwise healthy individuals with pertussis-like symptoms. 3 However, debate exists as to whether B holmesii is a true respiratory pathogen or a colonising bacterium that has been identified instead of the correct disease-causing viruses or intracellular bacteria. B holmesii is possibly the leading cause of false-positive results when investigators screen symptomatic patients for whooping cough (caused by B pertussis) with use of PCR. Indeed, routine PCR does not discriminate between B holmesii and B pertussis because the target sequence typically used for clinical diagnosis (insertion sequence 481 [IS481]) is present in both genomes. The effect of this misdiagnosis is not only important for individual patients because of its potential to lead to inappropriate antimicrobial treatment and risk of invasive disease, but also for public health because it can confound the assessment of efficacy for the pertussis vaccine. 4–6 In this Review, we summarise knowledge about B holmesii and explore future research objectives. History In 1983, the US Centers for Disease Control and Prevention (CDC) recorded the first reported case of B holmesii infection, which was in a man aged 37 years with asplenia in Buffalo, NY, USA. 1 The CDC then isolated 14 additional strains in blood samples submitted from nine different states in the USA and from Saudi Arabia and Switzerland. Before identification, the bacterium was called CDC non-oxidiser group 2 (NO-2). Results of DNA- relatedness studies, 16S rDNA sequencing, guanine-plus- cytosine content analysis, and biochemical characterisation affiliated this strain to the Bordetella genus. Investigators gave the bacterium its present name in 1995 in honour of Barry Holmes, an English microbiologist and head of the British National Collection of Type Cultures, for his substantial contribution to the characterisation, classification, and identification of rare or atypical Gram- negative bacteria. 1 Microbiology Bordetella species The genus Bordetella belongs to the family of Alcaligenaceae and consists of nine species: B pertussis, B parapertussis, B bronchiseptica, B avium, B hinzii, B holmesii, B trematum, B petrii, and B ansorpii. The classic species are B pertussis, B parapertussis, and B bronchiseptica, occasionally referred to as the mammalian pathogens, by contrast with the avian species (B avium and B hinzii). The classic species are known to cause mainly respiratory infections. The latter five, added in the past two decades, are considered to be new species. B pertussis and a specific lineage of B parapertussis infect human beings exclusively, resulting in the classic symptoms of paroxysmal cough, whooping, and post- tussive vomiting. The other lineage of B parapertussis causes respiratory infection in sheep. B bronchiseptica, the ancestor of the mammalian pathogens, 7–9 is found mostly in dogs, pigs, rabbits, and cats, but has been occasionally reported in people in close contact with animals. 10–12 B avium, responsible for turkey coryza in wild or domesticated birds, 13 can sometimes infect people with underlying pulmonary diseases. 14,15 Turkey coryza can also be caused by B hinzii, 16 which has been recovered in a few patients with chronic diseases. 14,16–23 B trematum has been isolated from human cutaneous lesions and in ear infections. 24,25 First described in the environment (river sediment), 26 B petrii was anecdotally recovered in patients. 14,27–29 Finally, B ansorpii, the most recent addition to the Bordetella genus, was first described in 2005 after isolation from purulent exudate of an epidermal cyst 30 and blood samples. 31 B holmesii is the most frequently reported bacterium of these new species in the published work and seems to be the only pathogen within this group that is capable of causing disease in otherwise healthy individuals. 32 Biochemical characteristics B holmesii is a Gram-negative, rod-shaped (or predominately small coccoid and short rod shaped), slow-growing organism. Biochemically, it is non- oxidising, non-saccharolytic, urease-negative, and not haemolytic on blood agar plates (figure 1). 1 After 48 h of Lancet Infect Dis 2014 Published Online April 8, 2014 http://dx.doi.org/10.1016/ S1473-3099(14)70021-0 Department of Paediatrics, Division of General Paediatrics, Children’s Hospital, University Hospitals of Geneva (L F Pittet MD, Prof C-A Siegrist MD, K M Posfay-Barbe MD), Department of Genetics and Laboratory Medicine, Department of Medical Specialties, University Hospitals of Geneva, (S Emonet MD, Prof J Schrenzel MD), and Neonatal Immunology, Departments of Pathology- Immunology and Paediatrics (C-A Siegrist), University of Geneva, Geneva, Switzerland Correspondence to: Dr Klara M Posfay-Barbe, Children’s Hospital, University Hospitals of Geneva, 1211 Geneva 14, Switzerland [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0 1
Review
Bordetella holmesii: an under-recognised Bordetella speciesLaure F Pittet, Stéphane Emonet, Jacques Schrenzel, Claire-Anne Siegrist, Klara M Posfay-Barbe
Bordetella holmesii, first described in 1995, is believed to cause both invasive infections (bacteraemia, meningitis, endocarditis, pericarditis, pneumonia, and arthritis) and pertussis-like symptoms. Infection with B holmesii is frequently misidentified as being with B pertussis, the cause of whooping cough, because routine diagnostic tests for pertussis are not species-specific. In this Review, we summarise knowledge about B holmesii diagnosis and treatment, and assess research needs. Although no fatal cases of B holmesii have been reported, associated invasive infections can cause substantial morbidities, even in previously healthy individuals. Antimicrobial treatment can be problematic because B holmesii’s susceptibility to macrolides (used empirically to treat B pertussis) and third-generation cephalosporins (often used to treat invasive infections) is lower than would be expected. B holmesii’s adaptation to human beings is continuing, and virulence might increase, causing the need for better diagnostic assays and epidemiological surveillance.
IntroductionBordetella holmesii, a Gram-negative bacterium was first described as a cause of bacteraemia in patients with comorbidities such as asplenia.1,2 The bacterium was also recovered in nasopharyngeal samples in otherwise healthy individuals with pertussis-like symptoms.3 However, debate exists as to whether B holmesii is a true respiratory pathogen or a colonising bacterium that has been identified instead of the correct disease-causing viruses or intracellular bacteria. B holmesii is possibly the leading cause of false-positive results when investigators screen symptomatic patients for whooping cough (caused by B pertussis) with use of PCR. Indeed, routine PCR does not discriminate between B holmesii and B pertussis because the target sequence typically used for clinical diagnosis (insertion sequence 481 [IS481]) is present in both genomes. The effect of this misdiagnosis is not only important for individual patients because of its potential to lead to inappropriate antimicrobial treatment and risk of invasive disease, but also for public health because it can confound the assessment of efficacy for the pertussis vaccine.4–6 In this Review, we summarise knowledge about B holmesii and explore future research objectives.
HistoryIn 1983, the US Centers for Disease Control and Prevention (CDC) recorded the first reported case of B holmesii infection, which was in a man aged 37 years with asplenia in Buffalo, NY, USA.1 The CDC then isolated 14 additional strains in blood samples submitted from nine different states in the USA and from Saudi Arabia and Switzerland. Before identification, the bacterium was called CDC non-oxidiser group 2 (NO-2). Results of DNA-relatedness studies, 16S rDNA sequencing, guanine-plus-cytosine content analysis, and biochemical characterisation affiliated this strain to the Bordetella genus. Investigators gave the bacterium its present name in 1995 in honour of Barry Holmes, an English microbiologist and head of the British National Collection of Type Cultures, for his substantial contribution to the characterisation, classification, and identification of rare or atypical Gram-negative bacteria.1
MicrobiologyBordetella species The genus Bordetella belongs to the family of Alcaligenaceae and consists of nine species: B pertussis, B parapertussis, B bronchiseptica, B avium, B hinzii, B holmesii, B trematum, B petrii, and B ansorpii. The classic species are B pertussis, B parapertussis, and B bronchiseptica, occasionally referred to as the mammalian pathogens, by contrast with the avian species (B avium and B hinzii). The classic species are known to cause mainly respiratory infections. The latter five, added in the past two decades, are considered to be new species.
B pertussis and a specific lineage of B parapertussis infect human beings exclusively, resulting in the classic symptoms of paroxysmal cough, whooping, and post-tussive vomiting. The other lineage of B parapertussis causes respiratory infection in sheep. B bronchiseptica, the ancestor of the mammalian pathogens,7–9 is found mostly in dogs, pigs, rabbits, and cats, but has been occasionally reported in people in close contact with animals.10–12 B avium, responsible for turkey coryza in wild or domesticated birds,13 can sometimes infect people with underlying pulmonary diseases.14,15 Turkey coryza can also be caused by B hinzii,16 which has been recovered in a few patients with chronic diseases.14,16–23 B trematum has been isolated from human cutaneous lesions and in ear infections.24,25 First described in the environment (river sediment),26 B petrii was anecdotally recovered in patients.14,27–29 Finally, B ansorpii, the most recent addition to the Bordetella genus, was first described in 2005 after isolation from purulent exudate of an epidermal cyst30 and blood samples.31 B holmesii is the most frequently reported bacterium of these new species in the published work and seems to be the only pathogen within this group that is capable of causing disease in otherwise healthy individuals.32
Biochemical characteristics B holmesii is a Gram-negative, rod-shaped (or predominately small coccoid and short rod shaped), slow-growing organism. Biochemically, it is non-oxidising, non-saccharolytic, urease-negative, and not haemolytic on blood agar plates (figure 1).1 After 48 h of
Lancet Infect Dis 2014
Published Online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0
Department of Paediatrics, Division of General Paediatrics, Children’s Hospital, University Hospitals of Geneva (L F Pittet MD, Prof C-A Siegrist MD, K M Posfay-Barbe MD), Department of Genetics and Laboratory Medicine, Department of Medical Specialties, University Hospitals of Geneva, (S Emonet MD, Prof J Schrenzel MD), and Neonatal Immunology, Departments of Pathology-Immunology and Paediatrics (C-A Siegrist), University of Geneva, Geneva, Switzerland
Correspondence to: Dr Klara M Posfay-Barbe, Children’s Hospital, University Hospitals of Geneva, 1211 Geneva 14, Switzerland [email protected]

2 www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0
Review
culture, B holmesii produces brown soluble pigments that differentiate it from other Bordetella and Acinetobacter species. Moraxella canis is the only other organism known to produce such a pigment.33 The lack of oxidase and haemolysing activity differentiates B holmesii from B pertussis, B bronchiseptica, and B avium. The absence of urease activity differentiates it from B parapertussis.1 As with other Bordetella species, culture of B holmesii is time consuming and difficult, and needs a special medium for transportation and culture.
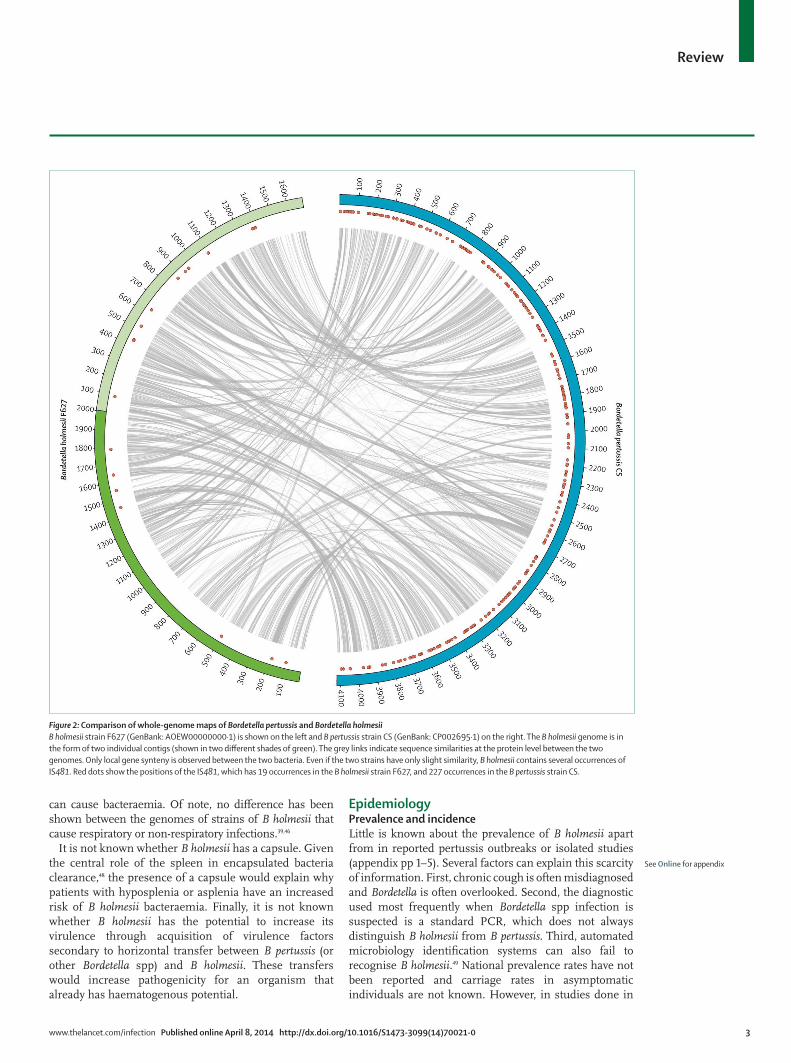
Similarity between B holmesii and other Bordetella speciesOrigin and microarrays-genomic comparisonA 99·5% gene sequence identity was shown between B pertussis’ and B holmesii’s 16S rRNA gene.32 Several techniques have been used to establish B holmesii’s similarity with other Bordetella species. Use of comparative genomic hybridisation of B holmesii strains compared with those of B pertussis on microarray showed substantial divergence between the two.34 Findings from multilocus sequence typing confirmed this divergence. However, analysis of housekeeping genes showed that B holmesii possibly acquired both its 16S rRNA gene and iron-uptake island by lateral transfer from B pertussis.34 IS481 (the sequence targeted by routine PCR for diagnosis of B pertussis) was present in high copy numbers (>50) in B pertussis, but there was only only eight to ten copies in B holmesii (figure 2).35,36 The higher copy numbers suggest that IS481 has been present in B pertussis for a longer period than it has been in B holmesii.35 Although IS481
was possibly inherited from a common ancestor of both B pertussis and B holmesii, evidence of a shared genomic site suggests horizontal transfer of this element.3,36 The B holmesii genome also contains three to five copies of IS1001-like elements, named holmesii IS1001 (hIS1001).35,37,38 Analyses of four other housekeeping genes show that B holmesii is more closely related to B hinzii and B avium (so-called avian species) than to mammalian (classic) Bordetella species.34 Results of cellular fatty acid composition analyses and multilocus sequence typing also associated B holmesii with B avium.1 Finally, draft genome sequences of B holmesii strains have enabled an updated phenogram, which shows the close relation between B holmesii and B avium.39,40
Genetic analyses of the bvgAS two-component system (the master regulator of virulence gene expression) in B pertussis, B parapertussis, and B bronchiseptica revealed that the B holmesii bvgAS system is more closely related to that of B avium than to those of the mammalian species.41 Although some areas (such as the cytoplasmic signalling domains of the bvgS histidine kinase) might be functionally interchangeable between B holmesii and B pertussis, signal perception and respective levels of activity differs between the two species.41,42
Proteins produced by B holmesii seem to be more similar to those from B bronchiseptica than to those from B pertussis.43 Link and colleagues44 reported that B holmesii produces a factor highly related to filamentous haemaglutinin (FHA), a well known adhesin essential for colonisation in other pathogenic Bordetella spp. Similar to other Bordetella spp, its production is regulated by the bvgAS virulence regulatory system. However, this protein is more closely related to that found in B avium (55% similarity) than to that in mammalian Bordetella spp.44 B holmesii does not produce a pertussis toxin,39,45,46 but this toxin is not necessary for the development of symptoms. For example, B parapertussis can cause disease without any production of the pertussis toxin. Finally, other toxins and adhesins implicated in the Bordetella pathogenesis have not been detected in B holmesii isolates, including adenylate cyclase–hemolysin toxin, Bordetella type 2 and 3 secretion systems, pertactin, and fimbrial proteins.39,40,46
Diavatopoulos and colleagues34 postulated that the recent emergence of B holmesii as a human pathogen relates to the acquisition of a 66 kilo-base-pair-long genomic island by horizontal transfer with B pertussis. Among others, this island encodes for several virulence factors, such as a siderophore capable of scavenging free iron from the extracellular environment, and several antibiotic resistance efflux pumps. This addition might enhance colonisation of the host airway through an increase in resistance to host defensins and other endogenous antimicrobial peptides.34 According to van den Akker,47 differences in lipo-polysaccharide expression between B pertussis and B holmesii (important for pathogenesis) could explain the observed clinical dissimilarity of B pertussis, which mainly infects respiratory tract epithelium, and B holmesii, which
Figure 1: Bordetella holmesii growing on a sheep-blood agar plateIsolation of B holmesii on a sheep-blood agar plate shows small shiny grey non-haemolytic colonies 24 h after incubation in 5% CO2.
www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0 3
Review
can cause bacteraemia. Of note, no difference has been shown between the genomes of strains of B holmesii that cause respiratory or non-respiratory infections.39,46
It is not known whether B holmesii has a capsule. Given the central role of the spleen in encapsulated bacteria clearance,48 the presence of a capsule would explain why patients with hyposplenia or asplenia have an increased risk of B holmesii bacteraemia. Finally, it is not known whether B holmesii has the potential to increase its virulence through acquisition of virulence factors secondary to horizontal transfer between B pertussis (or other Bordetella spp) and B holmesii. These transfers would increase pathogenicity for an organism that already has haematogenous potential.
EpidemiologyPrevalence and incidence Little is known about the prevalence of B holmesii apart from in reported pertussis outbreaks or isolated studies (appendix pp 1–5). Several factors can explain this scarcity of information. First, chronic cough is often misdiagnosed and Bordetella is often overlooked. Second, the diagnostic used most frequently when Bordetella spp infection is suspected is a standard PCR, which does not always distinguish B holmesii from B pertussis. Third, automated microbiology identification systems can also fail to recognise B holmesii.49 National prevalence rates have not been reported and carriage rates in asymptomatic individuals are not known. However, in studies done in
Figure 2: Comparison of whole-genome maps of Bordetella pertussis and Bordetella holmesiiB holmesii strain F627 (GenBank: AOEW00000000·1) is shown on the left and B pertussis strain CS (GenBank: CP002695·1) on the right. The B holmesii genome is in the form of two individual contigs (shown in two different shades of green). The grey links indicate sequence similarities at the protein level between the two genomes. Only local gene synteny is observed between the two bacteria. Even if the two strains have only slight similarity, B holmesii contains several occurrences of IS481. Red dots show the positions of the IS481, which has 19 occurrences in the B holmesii strain F627, and 227 occurrences in the B pertussis strain CS.
See Online for appendix

4 www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0
Review
Africa (Tunisia), Asia (Japan), Canada (Alberta and Ontario), Europe (Belgium, Finland, France, Romania, Switzerland, and the Netherlands), South America (Argentina and Chile), and the USA (Massachusetts, California, Colorado, Ohio, and Washington), researchers identified B holmesii in 0–29·3% of nasopharyngeal isolates from patients with pertussis-like episodes (appendix pp 1–5).3,37,38,50–65 During the 2010 pertussis outbreak in Ohio, investigators identified B holmesii in 32% of patients with Bordetella-confirmed respiratory infection.58 Almost half of the adolescents aged 11–18 years with pertussis-like illness (30 [45%] of 70 patients) had a final diagnosis of B holmesii and not B pertussis. However, since no other investigation of cause was reported in these studies, other pathogens such as viruses or intracellular bacteria could have been the true pathogenic agents in carriers of B holmesii. In Massachusetts, prevalence of B holmesii in nasopharyngeal specimens of people with whooping-cough-like episodes increased by six times over 3 years (from 0·1% in 1995, to 0·6% in 1998; p<0·001).3 Hypotheses to explain such an increase include a higher circulation rate of the bacterium, increased awareness of B pertussis by physicians, and improved laboratory detection.3,66,67
A modification of the competitive balance between B pertussis and other species secondary to the introduction of the acellular pertussis vaccine in 1996 cannot be excluded.67 Indeed, compared with the pertussis whole-cell vaccine, acellular vaccines have a lower efficacy against B parapertussis in animals.68 The introduction of acellular vaccine could have changed the competitive balance to favour non-pertussis Bordetella species, such as B holmesii, B parapertussis, or B bronchiseptica.67
Transmission and reservoirNo data are available for mode of transmission for B holmesii. Transmission is probably mostly through respiratory droplets,57 but other modes of transmission could exist, such as through the environment or blood products. B holmesii is presumed to be strictly a human pathogen because no animal reservoir has been reported as yet. However, this exclusivity has not been investigated thoroughly and might be challenged since B holmesii is closely related to the avian species of Bordetella.32,34,39,40,67 Furthermore, findings of two case reports suggested animals as potential sources of infection.69,70 B holmesii has been isolated in human sputum71,72 and could therefore be a transient pathogen of the upper respiratory tract.69 This localisation is further suggested by a case of B holmesii endocarditis that occurred 2 months after dental manipulation.73 Investigators have also detected B holmesii in two platelet concentrates. The bacterium presumably survived during platelet concentrate storage, but at too low a count for detection by routine bacterial screening.74 The duration of incubation and degree of infectivity or attack rate is not known. Finally, investigators have reported a seasonal variability.3,54,57,65
Some evidence suggests that B pertussis and B holmesii co-circulate.3,65,75 B holmesii has been isolated during several B pertussis outbreaks,57,58,65,76 and five cases of B holmesii and B pertussis coinfection were reported during the 2010 Ohio pertussis outbreak.58,65
Susceptibility factors for respiratory infection Healthy adults and adolescents seem to be at greater risk for respiratory infection with B holmesii than are younger individuals, and this age group are the most represented in published reports about B holmesii (appendix pp 1–5). In Massachusetts, 19 (83%) of 23 B holmesii respiratory infections reported were in adolescents (aged 11–19 years).3 In the Ohio pertussis outbreak, adolescents aged 11–18 years constituted about two-thirds of patients with B holmesii and only a third of patients with B pertussis (p=0·001).58 The reason why adults and adolescents seemed to be at higher risk is not clear, but it might be linked to waning immunity against B pertussis (although there is no evidence of cross-protection between the two species) or to the fact that this population is the reservoir of B pertussis in many countries. Because B holmesii possibly co-circulates with B pertussis, the increased prevalence of B pertussis infection in this age group could explain the increased risk of detection of B holmesii. However, in a whooping cough outbreak in Chile, B holmesii was equally present in all age groups. The bacterium was recovered in 13·7% of patients aged 0–7 years with pertussis-like symptoms, 8% of patients aged 10–17 years, and 8·7% of patients aged older than 18 years.63 In a recent report from Argentina, all nine B holmesii respiratory infections occurred in children, seven in infants younger than 6 months.59
Underlying conditions for invasive B holmesii infection Some categories of patients seem to be at increased risk for B holmesii infection. Asplenia (functional or anatomical) is the most frequently identified risk factor,2,75 but B holmesii infection has also been reported in patients with chronic obstructive pulmonary disease,71 ulcerative colitis,77 diabetes mellitus,1,75,77 lymphoma,1,71,78,79 common variable immunodeficiency,77 HIV infection,2 nephrotic syndrome,80,81 high-dose corticosteroid drugs,80 systemic lupus erythematosus,82,83 anorexia nervosa,84 after solid-organ transplantation,81 and in infants.2,69 The common feature between these disorders seems to be that of immune modulation, including in infants, secondary to disease or immunosuppressive therapy.85
Clinical featuresPertussis-like respiratory infection When B holmesii is isolated from respiratory samples, the corresponding presentation is similar to that of whooping cough, including low-grade fever, cough, and post-tussive vomiting. Yih and colleagues3 reported that patients infected with B holmesii presented with milder symptoms than did those with B pertussis—ie, two or fewer of the

www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0 5
Review
three classic pertussis symptoms: paroxysmal cough, whoop, and post-tussive vomiting (p<0·01). Rodgers and colleagues58 reported similar frequencies of classic features among patients infected with B pertussis or B holmesii during an outbreak. They did describe a difference in cough duration: about 70% of patients infected with B holmesii were cough-free 80 days after antibiotic treatment compared with less than 30% of patients with B pertussis. This difference could be explained by the absence of pertussis toxin in B holmesii. Bottero and colleagues59 reported milder respiratory symptoms in nine children (including seven infants younger than 6 months) infected with B holmesii—none had cyanosis or apnoea, whereas in children with B pertussis infection, 34% had cyanosis and 14% had apnoea.
Bacteraemia Unlike B pertussis, which is a pathogen of the respiratory tract, B holmesii has been described as a cause of bacteraemia.2 Over 18 years between 1983 and 2000, the CDC identified 30 patients with B holmesii bacteraemia in 16 states in the USA.2 In 25 of 26 patients, B holmesii was the only microorganism isolated from blood samples, and researchers recovered B holmesii in more than half (54%) of patients in at least a second blood sample. In Northern Alberta, Kanji and colleagues77 identified eight cases of B holmesii bacteraemia over 5 years. In New York, Layton and colleagues86 reported on a cluster of five cases of B holmesii bacteraemia. Tartof and colleagues75 later reported an investigation of 22 cases of B holmesii bacteraemia in less than 10 months in the USA: 91% of patients had at least one underlying medical condition. Bacteraemia remains a rare presentation, but it can be severe and can even cause admission to critical care.2,75 As yet, no fatalities have been reported secondary to B holmesii bacteraemia. The clinical course is usually characterised by a non-specific febrile illness and is not typically associated with other signs, such as rash. White-blood-cell count and other routine laboratory investigation are not characteristic. B holmesii bacteraemia is generally reported in patients with risk factors such as asplenia or immunosuppression. All age groups can get B holmesii bacteraemia, but in a retrospective study by Shepard and colleagues,2 85% of patients were younger than 40 years (median age 20·5 years), and mean age was 43 years in another Canadian study.77 In a US study, the median age was 17·1 years, but the age distribution was wide (2–77 years).75
Other infection typesPneumonia with B holmesii has been described in a previously healthy 14-year-old girl and a 15-year-old boy with chronic nephrotic syndrome.80,87 Outcomes for both patients were complicated by pleural effusion. The girl had mediastinal collection, pericarditis, coagulopathy, and pulmonary fibrosis, resulting in a severe restrictive syndrome 6 months later. B holmesii bronchitis has been reported in a 2-year-old girl with asthma.72 The cough was
productive and not whooping. In a woman aged 41 years, B holmesii triggered exacerbation of chronic obstructive pulmonary disease, and she needed intubation and admission to critical care.71
Non-respiratory sites of B holmesii infection have been reported (appendix pp 6–11). There have been nine reports of patients with B holmesii endocarditis on native and prosthetic valves.1,33,71,73,82,88–90 Symptoms ranged from subacute endocarditis to septic shock with acute renal failure, usually needing valve replacement. Investigators reported on two patients with B holmesii pericarditis; one patient stayed in hospital for longer than 2 months.78,87 Researchers have also reported meningitis in two patients: a girl aged 14 years with anorexia nervosa and a woman aged 37 years with end-stage renal disease secondary to systemic lupus erythematosus.83,84 In the woman, the outcome was severe, with persistent convulsions needing continuous intravenous diazepam and mechanical ventilation.83 Septic arthritis with B holmesii, both in patients with normal and in those with prosthetic knees, has been reported;1,91,92 one immunocompetent woman aged 54 years had to get her prosthesis removed.92 Finally, B holmesii was isolated four times in the blood culture of a 67-year-old patient receiving rituximab who presented with three episodes of cellulitis and one episode of pneumonia. Later, asymptomatic nasal carriage of B holmesii was reported in the same patient.79 This severe invasive disease range has never been described for B pertussis and shows the particularity of B holmesii infections, which are ubiquitous and can go from barely symptomatic to life-threatening invasive disease. Although most patients with invasive B holmesii infection had an underlying disease, severe infections have been reported in previously healthy individuals.33,69,87
DiagnosisThe identification of B holmesii by culture from biological fluids (blood, pleural or articular fluid, or nasopharyngeal samples) is cumbersome because the mean incubation time of blood cultures to be positive is 40 h49 and the bacteria do not grow well on MacConkey agar.93 As with B pertussis, rapid specimen transfer in an appropriate transport medium is crucial to ensure optimum sensitivity.94,95 Cefalexin, an antimicrobial drug recommended for the isolation of Bordetella spp, is widely used in various Bordetella spp culture media (eg, Regan–Lowe agar), and is now recognised to have an inhibitory effect on the growth of B holmesii, which possibly explains why most laboratories did not identify B holmesii in nasopharyngeal specimens of patients with pertussis-like symptoms before 2000.96 Hence, the use of meticillin or oxacillin, instead of cephalexin, is now preferred.10 When retrieved by culture, B holmesii is usually not identified correctly by automated biochemical identification devices. Panagopoulos and colleagues49 describe several situations in which B holmesii was misidentified as Acinetobacter lwoffii by Vitek2 (bioMérieux), highlighting

6 www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0
Review
the need to take into account all the characteristics of B holmesii to limit false identification, such as its very poor growth on MacConkey agar.49
Matrix-assisted laser desorption and ionisation time-of-flight mass spectrometry (MALDI-TOF MS) of whole bacterial cells has revolutionised bacterial identification through rapid and accurate identification of most pathogens retrieved in clinical microbiology.97 For pathogens such as B holmesii, which are difficult to identify accurately with biochemical methods, MALDI-TOF MS is an ideal identification instrument. However, only a few published works report the identification of B holmesii with MALDI-TOF MS.33,85,91,93 The gold standard for identification remains 16S rDNA sequencing. However, the sequence obtained with sequencing is often very similar to that obtained for B pertussis, and further sequence analysis must be done, such as detection of B holmesii-specific genes by PCR.34
PCR is the most commonly used test for the diagnosis of B pertussis and it had a higher sensitivity compared with culture (93·5% [with the IS481 target] vs 15·2% for culture) in a study using an expanded case definition.98 PCR is less affected by previous antibiotic treatment because the organism does not need to be replicating for the test to be positive. However, PCR methods for B pertussis diagnosis are not standardised and differ widely since each laboratory defines its own assay procedure and detection limit.99–101 The most frequently used target sequence to diagnose B pertussis is IS481.100,101 More than 50 copies of IS481 are found in the B pertussis genome and its sensitivity is greater compared with single-copy target sequences with lower detection limits.51 However, false-positive results through laboratory or hospital environment contamination have been reported.51,102 In two European studies, only one in 11 and one in 24 laboratories were able to correctly identify
the B holmesii strain, and most in-house PCR assays do not discriminate B holmesii from B pertussis.100,103 In Australia, only 7% of laboratories report the ability to distinguish B holmesii from B pertussis.6 Similarly, in the USA, only two of 42 laboratories could distinguish both organisms.101 Indeed, the B holmesii genome also contains about ten copies of the IS481 sequence, which can cause false-positive B pertussis results. Occasionally, a few copies of the IS481 can be detected in B bronchiseptica.103,104 Some laboratories do a second PCR assay using another target for B pertussis to confirm results for IS481-positive specimens, but other targets can be less sensitive and lead to false-negative results.105
For diagnosis of B pertussis, Probert and colleagues51 suggested new target sequences (BP283 and BP485) that are not found in B holmesii. However, because BP283 and BP485 are single-copy target sequences, tests need to be ten times more sensitive to detect them than are tests for IS481 (table; appendix pp 12–15). Poddar112 suggests use of a beacon probe and post-PCR probe-target melting profile analysis to distinguish between B holmesii and B pertussis. This molecular assay can detect a single nucleotide change in IS481 and thus discriminate between the two species. Other researchers think that it is preferable to use a B holmesii-specific sequence (such as the hIS1001,38 BhrecA,38,52 or bhoE67), rather than to use a second B-pertussis-specific sequence (such as pertussis-toxin-S1)93 because of the risk of a false-negative B pertussis test result.93 Another difficulty is that coinfection could occur and all samples positive for B holmesii are not always B pertussis-negative.113 Since the pathogenesis for B holmesii remains still mostly unexplored, no guidelines have been established for the best anatomical site to obtain the highest yield for analysis. No specific serological testing is available for B holmesii, but even if there was, its clinical relevance would be questionable.
TreatmentThere is no consensus for the best treatment for B holmesii infection (appendix pp 6–11). Since diagnosis is often delayed, patients are usually treated for a B pertussis respiratory infection, or empirically according to symptoms. The in-vitro susceptibility of B holmesii to drugs has been assessed through broth microdilution,2 Epsilometer test,33,40,49,65,78–80,83,84,89–91,114 auto mated systems,73,115 agar dilution,71 and disk diffusion.33,43,70,82 Results show that broad-spectrum β-lactams, including third-generation cephalosporins, might not be the best treatment for B holmesii.2 Cefotaxime has been reported as both active43,71,89 and inactive against the bacteria.2,33,49,79,82,115,116 Resistance to ceftriaxone,84,90,116 cefotaxime, and co-trimoxazole79,116 has also been reported. Ceftazidime shows low minimum inhibitory concentrations (MICs), indicating high potency.33,49,70,71,115 Macrolides are the first-choice antimicrobials in B pertussis infections.10 However, B holmesii isolates have higher MICs for erythromycin than have isolates of
Bordetella pertussis
Bordetella parapertussis
Bordetella holmesii
Bordetella bronchiseptica
Bordetella hinzi
Bordetella petrii
IS48135–37,50,93,104,106,107 Present Absent* Present Conflicting data† ··‡ Absent
IS100110,36–38,50,53,76,106,108 Absent Present Absent Absent§ ·· Absent
IS100236,108,109 Present Present¶ Absent Absent|| ·· Absent
ptx56,76,93,106 Present Present Absent ** ·· ··
BP338552,110 Present ·· Absent Conflicting data†† Conflicting data†† ··
BP28351 Present ·· ·· ·· ·· ··
BP48551 Present ·· ·· ·· ·· ··
hIS1001106 Absent Absent Present ·· ·· ··
BhrecA38,52,56,57,111 Absent ·· Present ·· ·· ··
bhoE67 Absent ·· Present ·· ·· ··
IS=insertion sequence. BP=Bordetella pertussis. hIS=holmesii insertion sequence. *IS481107 present in some isolates of B parapertussis. †1–5 copies of IS481 reported in 2% of human isolates36,105 and 20% of animal isolates36 of B bronchiseptica. ‡IS481-like weakly present in B hinzii. §IS1001 present in 5–8% of human isolates36,106 and 31–76% of animal isolates36,108 of B bronchiseptica. ¶IS1002 present in human isolates108 but not in animal isolates of B parapertussis strains. || IS1002 present in 14% of human isolates36 and 3–6% of animal isolates36,108 of B bronchiseptica. **ptx93 present in isolates of B bronchiseptica. ††BP3385 present in some strains110 of B bronchiseptica and B hinzii.
Table: Summary of findings for different PCR strategies for diagnosis of Bordetella species105–111

www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0 7
Review
B pertussis, suggesting a lower activity against B holmesii,59 which could become an issue if B holmesii is not correctly diagnosed. Low MICs were reported for carbapenems and fluoroquinolones,2,78 which are often suggested to be the most effective antibiotics against B holmesii.2,77
Further microbiological research is needed to determine the best antimicrobial treatment, including breakpoints to be used for in-vitro susceptibility.33 The drawback is that such studies are difficult to do and severe infections caused by B holmesii are infrequent. Finally, there is a need to define whether B holmesii infections (mostly non-invasive infections) need antibiotic treatment, and when, because most reported infections are mild and uneventful.33 However, since B holmesii infection is rarely microbiologically proven, more severe infections might not have been diagnosed or reported. Bush and colleagues73 reported that two lengthy courses of active antimicrobial therapy did not eradicate a B holmesii prosthetic heart valve infection and that vegetations grew while the patient was taking chronic suppressive ciprofloxacin, showing that antibiotic treatment might not always be curative.
PreventionIn addition to standard precautions, it is not known whether other transmission-based precautions, such as droplet precautions, should be implemented in confirmed B holmesii infection.117 Also not known is whether postexposure antibiotic prophylaxis is necessary for individuals particularly at risk for invasive disease, such as those with asplenia. By contrast with B pertussis, macrolides might not be the best choice for prophylaxis because B holmesii is less susceptible to this class of antibiotics. Although several cases of B holmesii endocarditis have been reported, and some evidence indicates that B holmesii could be part of the upper respiratory-tract flora, recommended antibiotic prophylaxis for patients with prosthetic valves undergoing dental procedures is not (and probably should not be) tailored to protect against B holmesii in particular. B holmesii bacteraemia has been reported in patients receiving penicillin or co-trimoxazole prophylaxis.40,114,118,119 Finally, time-consuming and resource-consuming postexposure assessment and management for people who have been in contact with patients infected with B holmesii, as is recommended in B pertussis outbreaks, might be unnecessary.120
Genes that code for antigens present in the pertussis acellular vaccine (pertussis toxin, filamentous hemagglutinin, pertactin, or fimbriae, depending on the manufacturer) have not been recovered in the B holmesii genome,39,43 or they differ phenotypically (eg, as with filamentous hemagglutinin).44 Thus, antibodies elicited after pertussis vaccination will not target B holmesii. This selectivity was confirmed during the Ohio outbreak in which 60% of patients aged 11–18 years with B holmesii infection had been immunised with pertussis booster vaccines as adolescents compared with 44% of patients
with B pertussis.58 Although both whole-cell and acellular pertussis vaccines induce a cross-reactive T-cell response to B holmesii, neither vaccine conferred protection against B holmesii replication in mice.60
Unanswered questionsMicrobiology Many questions about B holmesii remain unanswered. For example, whether it is truly pathogenic, and whether it is really an emerging pathogen or just not recognised until recently. It is not known whether the bacterium causes a whooping cough-like illness or whether it is only incidentally detected in patients infected with other pathogens. Prospective studies should extensively investigate patients with respiratory-tract infections, so as to rule out other causes in patients in whom B holmesii was detected. Factors that could induce an increase of B holmesii’s pathogenicity are not known. This potential is feared because data have already suggested horizontal transfer of genes between B pertussis and B holmesii. Finally, an exploration of B holmesii’s virulence factors, including whether it has a capsule, could have a major effect on understanding of the ecological niche and alternative treatment options.
Epidemiology Since only a few laboratories routinely diagnose B holmesii, the actual prevalence, including how (and why) it differs from one geographic region to another, cannot be established. To improve knowledge, efforts by national reference laboratories to improve identification and centralise results in a common database are warranted. Simultaneously, these efforts could assist public health authorities to avoid reporting pseudo-outbreaks of B pertussis after using PCRs, which does not discriminate between B pertussis and B holmesii. In addition, it would be important to identify the reservoir, precise mode of transmission, and incubation period of B holmesii. Animal models, similar to those used for influenza for example, could offer vital clues and improve insight into these features.121 The introduction of acellular B pertussis vaccine in the 1990s or the implementation of booster doses in early adulthood in the 2010s might have contributed to the emergence of B holmesii, with possible effects on species equilibrium. This link should also be investigated.
Clinical care, diagnosis, and prevention B holmesii seems more likely than other Bordetella species to cause invasive diseases with long-term complications, even in previously healthy individuals. This feature needs to be confirmed in larger, prospective cohort studies. The best treatment options should also be explored. Laboratory detection of B holmesii could be improved upon by use of routine specific PCRs or sequential PCRs on nasopharyngeal and respiratory specimens. No inter-national recommendations are available, although these would be useful to further guide laboratories. With the
8 www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0
Review
development of mass spectrometry-based identi fication methods, B holmesii will possibly be identified more accurately and more frequently when retrieved by culture.33 Infection with B holmesii that is falsely recognised as a B pertussis index case often causes an investigation to give prophylactic antibiotics to contacts and uses public health resources to control these pseudo-outbreaks. The effect, beneficial or not, of such an antimicrobial prophylaxis has not been investigated.
ConclusionPhysicians should be aware of B holmesii and assess their laboratory’s ability to identify it. Further studies are needed to improve knowledge, particularly about its epidemiology. At present, the most important public health issue is related to the deleterious effect of cases of B holmesii being interpreted as a B pertussis outbreak. This mistake could lead to underestimation of the efficacy of pertussis vaccination.4–6 B holmesii might soon attract more attention because of a better understanding of its prevalence and pathogenicity, including its potential to increase the risk of invasive disease in vulnerable patients.ContributorsLFP and KMP-B searched the databases and assessed the published work; LFP, KMP-B, and C-AS wrote the text; LFP prepared the table; and DH, SE, and JS prepared the figures. All authors critically reviewed manuscript content.
Declaration of interestsWe declare that we have no competing interests.
AcknowledgmentsWe thank Rosemary Sudan for editorial assistance, David Hernandez for creating figure 2, and Martine Leplay Fontana for her help to retrieve articles.
References1 Weyant RS, Hollis DG, Weaver RE, et al. Bordetella holmesii sp. nov.,
a new gram-negative species associated with septicemia. J Clin Microbiol 1995; 33: 1–7.
2 Shepard CW, Daneshvar MI, Kaiser RM, et al. Bordetella holmesii bacteremia: a newly recognized clinical entity among asplenic patients. Clin Infect Dis 2004; 38: 799–804.
3 Yih WK, Silva EA, Ida J, Harrington N, Lett SM, George H. Bordetella holmesii-like organisms isolated from Massachusetts patients with pertussis-like symptoms. Emerg Infect Dis 1999; 5: 441–43.
4 Guiso N. Specific biological diagnoses are needed to determine the durability of pertussis vaccine-induced immunity. Clin Infect Dis 2012; 55: 1433–34.
5 Wiedermann BL. What’s wrong with acellular pertussis vaccines? Clin Ther 2013; 35: 115–18.
6 is McIntyre PB, Sintchenko V. The “how” of polymerase chain reaction testing for Bordetella pertussis depends on the “why”. Clin Infect Dis 2013; 56: 332–34.
7 Bjørnstad ON, Harvill ET. Evolution and emergence of Bordetella in humans. Trends Microbiol 2005; 13: 355–59.
8 Diavatopoulos DA, Cummings CA, Schouls LM, Brinig MM, Relman DA, Mooi FR. Bordetella pertussis, the causative agent of whooping cough, evolved from a distinct, human-associated lineage of B. bronchiseptica. PLoS Pathog 2005; 1: e45.
9 Parkhill J, Sebaihia M, Preston A, et al. Comparative analysis of the genome sequences of Bordetella pertussis, Bordetella parapertussis and Bordetella bronchiseptica. Nat Genet 2003; 35: 32–40.
10 Mattoo S, Cherry JD. Molecular pathogenesis, epidemiology, and clinical manifestations of respiratory infections due to Bordetella pertussis and other Bordetella subspecies. Clin Microbiol Rev 2005; 18: 326–82.
11 Ner Z, Ross LA, Horn MV, et al. Bordetella bronchiseptica infection in pediatric lung transplant recipients. Pediatr Transplant 2003; 7: 413–17.
12 Wernli D, Emonet S, Schrenzel J, Harbarth S. Evaluation of eight cases of confirmed Bordetella bronchiseptica infection and colonization over a 15-year period. Clin Microbiol Infect 2011; 17: 201–03.
13 Raffel TR, Register KB, Marks SA, Temple L. Prevalence of Bordetella avium infection in selected wild and domesticated birds in the eastern USA. J Wildl Dis 2002; 38: 40–46.
14 Spilker T, Liwienski AA, LiPuma JJ. Identification of Bordetella spp. in respiratory specimens from individuals with cystic fibrosis. Clin Microbiol Infect 2008; 14: 504–06.
15 Harrington AT, Castellanos JA, Ziedalski TM, Clarridge JE 3rd, Cookson BT. Isolation of Bordetella avium and novel Bordetella strain from patients with respiratory disease. Emerg Infect Dis 2009; 15: 72–74.
16 Vandamme P, Hommez J, Vancanneyt M, et al. Bordetella hinzii sp. nov., isolated from poultry and humans. Int J Syst Bacteriol 1995; 45: 37–45.
17 Coenye T, Goris J, Spilker T, Vandamme P, LiPuma JJ. Characterization of unusual bacteria isolated from respiratory secretions of cystic fibrosis patients and description of Inquilinus limosus gen. nov., sp. nov. J Clin Microbiol 2002; 40: 2062–69.
18 Funke G, Hess T, von Graevenitz A, Vandamme P. Characteristics of Bordetella hinzii strains isolated from a cystic fibrosis patient over a 3-year period. J Clin Microbiol 1996; 34: 966–69.
19 Arvand M, Feldhues R, Mieth M, Kraus T, Vandamme P. Chronic cholangitis caused by Bordetella hinzii in a liver transplant recipient. J Clin Microbiol 2004; 42: 2335–37.
20 Hristov AC, Auwaerter PG, Romagnoli M, Carroll KC. Bordetella hinzii septicemia in association with Epstein-Barr virus viremia and an Epstein-Barr virus-associated diffuse large B-cell lymphoma. Diagn Microbiol Infect Dis 2008; 61: 484–86.
21 Fry NK, Duncan J, Edwards MT, et al. A UK clinical isolate of Bordetella hinzii from a patient with myelodysplastic syndrome. J Med Microbiol 2007; 56: 1700–03.
22 Gadea I, Cuenca-Estrella M, Benito N, et al. Bordetella hinzii, a “new” opportunistic pathogen to think about. J Infect 2000; 40: 298–99.
23 Cookson BT, Vandamme P, Carlson LC, et al. Bacteremia caused by a novel Bordetella species, “B. hinzii”. J Clin Microbiol 1994; 32: 2569–71.
24 Vandamme P, Heyndrickx M, Vancanneyt M, et al. Bordetella trematum sp. nov., isolated from wounds and ear infections in humans, and reassessment of Alcaligenes denitrificans Rüger and Tan 1983. Int J Syst Bacteriol 1996; 46: 849–58.
25 Daxboeck F, Goerzer E, Apfalter P, Nehr M, Krause R. Isolation of Bordetella trematum from a diabetic leg ulcer. Diabet Med 2004; 21: 1247–48.
26 von Wintzingerode F, Schattke A, Siddiqui RA, Rösick U, Göbel UB, Gross R. Bordetella petrii sp. nov., isolated from an anaerobic bioreactor, and emended description of the genus Bordetella. Int J Syst Evol Microbiol 2001; 51: 1257–65.
27 Le Coustumier A, Njamkepo E, Cattoir V, Guillot S, Guiso N. Bordetella petrii infection with long-lasting persistence in human. Emerg Infect Dis 2011; 17: 612–18.
28 Fry NK, Duncan J, Malnick H, et al. Bordetella petrii clinical isolate. Emerg Infect Dis 2005; 11: 1131–33.
29 Stark D, Riley LA, Harkness J, Marriott D. Bordetella petrii from a clinical sample in Australia: isolation and molecular identification. J Med Microbiol 2007; 56: 435–37.
30 Ko KS, Peck KR, Oh WS, Lee NY, Lee JH, Song JH. New species of Bordetella, Bordetella ansorpii sp. nov., isolated from the purulent exudate of an epidermal cyst. J Clin Microbiol 2005; 43: 2516–19.
31 Fry NK, Duncan J, Malnick H, Cockcroft PM. The first UK isolate of ‘Bordetella ansorpii’ from an immunocompromised patient. J Med Microbiol 2007; 56: 993–95.
Search strategy and selection criteria
We searched PubMed and Embase for articles published from Jan 1, 1971, to Jan 31, 2014, with the term “holmesii”. We did not actively search for articles older than this date range because the first report of B holmesii was published in 1995. We also reviewed relevant references cited in these articles. We included all articles published in English, German, Spanish, Portuguese, Italian, or French.
www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0 9
Review
32 Gross R, Keidel K, Schmitt K. Resemblance and divergence: the “new” members of the genus Bordetella. Med Microbiol Immunol (Berl) 2010; 199: 155–63.
33 Jonckheere S, De Baere T, Schroeyers P, Soetens O, De Bel A, Surmont I. Prosthetic valve endocarditis caused by Bordetella holmesii, an Acinetobacter lookalike. J Med Microbiol 2012; 61: 874–77.
34 Diavatopoulos DA, Cummings CA, van der Heide HGJ, et al. Characterization of a highly conserved island in the otherwise divergent Bordetella holmesii and Bordetella pertussis genomes. J Bacteriol 2006; 188: 8385–94.
35 Reischl U, Lehn N, Sanden GN, Loeffelholz MJ. Real-time PCR assay targeting IS481 of Bordetella pertussis and molecular basis for detecting Bordetella holmesii. J Clin Microbiol 2001; 39: 1963–66.
36 Tizolova A, Guiso N, Guillot S. Insertion sequences shared by Bordetella species and implications for the biological diagnosis of pertussis syndrome. Eur J Clin Microbiol Infect Dis 2013; 32: 89–96.
37 Templeton KE, Scheltinga SA, van der Zee A, et al. Evaluation of real-time PCR for detection of and discrimination between Bordetella pertussis, Bordetella parapertussis, and Bordetella holmesii for clinical diagnosis. J Clin Microbiol 2003; 41: 4121–26.
38 Antila M, He Q, de Jong C, et al. Bordetella holmesii DNA is not detected in nasopharyngeal swabs from Finnish and Dutch patients with suspected pertussis. J Med Microbiol 2006; 55: 1043–51.
39 Tatti KM, Loparev VN, Ranganathanganakammal S, et al. Draft genome sequences of Bordetella holmesii strains from blood (F627) and nasopharynx (H558). Genome Announc 2013; 1: e0005613.
40 Planet PJ, Narechania A, Hymes SR, et al. Bordetella holmesii: initial genomic analysis of an emerging opportunist. Pathog Dis 2013; 67: 132–35.
41 Gerlach G, Janzen S, Beier D, Gross R. Functional characterization of the BvgAS two-component system of Bordetella holmesii. Microbiology 2004; 150: 3715–29.
42 Horvat A, Gross R. Molecular characterization of the BvgA response regulator of Bordetella holmesii. Microbiol Res 2009; 164: 243–52.
43 Njamkepo E, Delisle F, Hagege I, Gerbaud G, Guiso N. Bordetella holmesii isolated from a patient with sickle cell anemia: analysis and comparison with other Bordetella holmesii isolates. Clin Microbiol Infect 2000; 6: 131–36.
44 Link S, Schmitt K, Beier D, Gross R. Identification and regulation of expression of a gene encoding a filamentous hemagglutinin-related protein in Bordetella holmesii. BMC Microbiol 2007; 7: 100.
45 Gerlach G, von Wintzingerode F, Middendorf B, Gross R. Evolutionary trends in the genus Bordetella. Microbes Infect 2001; 3: 61–72.
46 Bouchez V, Guiso N. Bordetella holmesii: comparison of two isolates from blood and a respiratory sample. Adv Infect Dis. 2013; 3: 123–33.
47 van den Akker WM. Lipopolysaccharide expression within the genus Bordetella: influence of temperature and phase variation. Microbiology 1998; 144: 1527–35.
48 Di Sabatino A, Carsetti R, Corazza GR. Post-splenectomy and hyposplenic states. Lancet 2011; 378: 86–97.
49 Panagopoulos MI, Saint Jean M, Brun D, et al. Bordetella holmesii bacteremia in asplenic children: report of four cases initially misidentified as Acinetobacter lwoffii. J Clin Microbiol 2010; 48: 3762–64.
50 Knorr L, Fox JD, Tilley PAG, Ahmed-Bentley J. Evaluation of real-time PCR for diagnosis of Bordetella pertussis infection. BMC Infect Dis 2006; 6: 62.
51 Probert WS, Ely J, Schrader K, Atwell J, Nossoff A, Kwan S. Identification and evaluation of new target sequences for specific detection of Bordetella pertussis by real-time PCR. J Clin Microbiol 2008; 46: 3228–31.
52 Guthrie JL, Robertson AV, Tang P, Jamieson F, Drews SJ. Novel duplex real-time PCR assay detects Bordetella holmesii in specimens from patients with pertussis-like symptoms in Ontario, Canada. J Clin Microbiol 2010; 48: 1435–37.
53 Wei Q, Robinson CC, Lovell MA, Hengartner RJ, Kelly KA, Murry KD. A cautionary tale from colorado: Bordetella holmesii circulates and can lead to false positive results in commonly-used Bordetella pertussis PCR. J Mol Diagn 2010; 12: 883.
54 Njamkepo E, Bonacorsi S, Debruyne M, Gibaud SA, Guillot S, Guiso N. Significant finding of Bordetella holmesii DNA in nasopharyngeal samples from French patients with suspected pertussis. J Clin Microbiol 2011; 49: 4347–48.
55 Norton K, Cordery R, Gleaves CA, Jensen B. Detection of Bordetella pertussis and Bordetella parapertussis by a real-time PCR in a community hospital. J Mol Diagn 2011; 13: 744.
56 Zouari A, Smaoui H, Brun D, et al. Prevalence of Bordetella pertussis and Bordetella parapertussis infections in Tunisian hospitalized infants: results of a 4-year prospective study. Diagn Microbiol Infect Dis 2012; 72: 303–17.
57 Kamiya H, Otsuka N, Ando Y, et al. Transmission of Bordetella holmesii during pertussis outbreak, Japan. Emerg Infect Dis 2012; 18: 1166–69.
58 Rodgers L, Martin SW, Cohn A, et al. Epidemiologic and laboratory features of a large outbreak of pertussis-like illnesses associated with cocirculating Bordetella holmesii and Bordetella pertussis–Ohio, 2010–2011. Clin Infect Dis 2013; 56: 322–31.
59 Bottero D, Griffith MM, Lara C, et al. Bordetella holmesii in children suspected of pertussis in Argentina. Epidemiol Infect 2013; 141: 714–17.
60 Zhang X, Weyrich LS, Lavine JS, Karanikas AT, Harvill ET. Lack of cross-protection against Bordetella holmesii after pertussis vaccination. Emerg Infect Dis 2012; 18: 1771–79.
61 Pittet LF, Emonet S, Francois P, et al. Diagnosis of whooping cough in Switzerland: differentiating Bordetella pertussis from Bordetella holmesii by polymerase chain reaction. PLoS One 2014; 9: e88936.
62 Cox HC, Jacob K, Whiley DM, et al. Further evidence that the IS481 target is suitable for real-time PCR detection of Bordetella pertussis. Pathology 2013; 45: 202–03.
63 Miranda C, Porte L, García P. Bordetella holmesii in nasopharyngeal samples from Chilean patients with suspected Bordetella pertussis infection. J Clin Microbiol 2012; 50: 1505.
64 Dinu S, Guillot S, Dragomirescu CC, et al. Whooping cough in south-east Romania: a 1-year study. Diagn Microbiol Infect Dis 2013; published online Nov 26. DOI: 10.1016/j.diagmicrobio.2013.09.017.
65 Spicer KB, Salamon D, Cummins C, Leber A, Marcon MJ. Occurrence of three Bordetella species during an outbreak of cough illness in Ohio: epidemiology, clinical features, laboratory findings, and antimicrobial susceptibility. Pediatr Infect Dis J 2014; published online Jan 17. DOI:10.1097/INF.0000000000000262.
66 He Q, Mertsola J. Factors contributing to pertussis resurgence. Future Microbiol 2008; 3: 329–39.
67 Mooi FR, Bruisten S, Linde I, et al. Characterization of Bordetella holmesii isolates from patients with pertussis-like illness in The Netherlands. FEMS Immunol Med Microbiol 2012; 64: 289–91.
68 David S, van Furth R, Mooi FR. Efficacies of whole cell and acellular pertussis vaccines against Bordetella parapertussis in a mouse model. Vaccine 2004; 22: 1892–98.
69 Morris JT, Myers M. Bacteremia due to Bordetella holmesii. Clin Infect Dis 1998; 27: 912–13.
70 Lindquist SW, Weber DJ, Mangum ME, Hollis DG, Jordan J. Bordetella holmesii sepsis in an asplenic adolescent. Pediatr Infect Dis J 1995; 14: 813–15.
71 Tang YW, Hopkins MK, Kolbert CP, Hartley PA, Severance PJ, Persing DH. Bordetella holmesii-like organisms associated with septicemia, endocarditis, and respiratory failure. Clin Infect Dis 1998; 26: 389–92.
72 Katsukawa C, Kushibiki C, Nishito A, et al. Bronchitis caused by Bordetella holmesii in a child with asthma misdiagnosed as mycoplasmal infection. J Infect Chemother 2013; 19: 534–37.
73 Bush LM, Davidson E, Daugherty J. Bordetella holmesii prosthetic valve endocarditis: a case report and review. Infect Dis Clin Pract 2012; 20: 248–53.
74 Thibault L, Nolin M, Jacques A, Daoud H, De Grandmont M, Delage G. Bacterial contamination of platelet concentrates: implication of negative culture when retesting the blood product after a positive result with the BacT/ALERT 3D. Transfusion 2012; 52: 201A.
75 Tartof SY, Gounder P, Weiss D, et al, for the Bordetella holmesii Working Group. Bordetella holmesii bacteremia cases in the United States, April 2010–January 2011. Clin Infect Dis 2014; 58: e39–43.
76 Miranda C, Wozniak A, Castillo C, et al. Presence of Bordetella holmesii in an outbreak of pertussis in Chile. Rev Chilena Infectol 2013; 30: 237–43.
77 Kanji J, Gee S, Ahmed-Bentley J, et al. Bordatella holmesii bacteremia in Northern Alberta: a 5-year case review. Can J Infect Dis Med Microbiol 2011; 22: 22A.

10 www.thelancet.com/infection Published online April 8, 2014 http://dx.doi.org/10.1016/S1473-3099(14)70021-0
Review
78 Nei T, Hyodo H, Sonobe K, Dan K, Saito R. First report of infectious pericarditis due to Bordetella holmesii in an adult patient with malignant lymphoma. J Clin Microbiol 2012; 50: 1815–17.
79 Nguyen LB, Epelboin L, Gabarre J, et al. Recurrent Bordetella holmesii bacteremia and nasal carriage in a patient receiving rituximab. Emerg Infect Dis 2013; 19: 1703–05.
80 Dörbecker C, Licht C, Körber F, et al. Community-acquired pneumonia due to Bordetella holmesii in a patient with frequently relapsing nephrotic syndrome. J Infect 2007; 54: e203–05.
81 Chambaraud T, Dickson Z, Ensergueix G, et al. Bordetella holmesii bacteremia in a renal transplant recipient: emergence of a new pathogen. Transpl Infect Dis 2012; 14: E134–36.
82 Bassetti M, Nicco E, Giacobbe DR, et al. Bordetella holmesii endocarditis in a patient with systemic lupus erythematosus treated with immunosuppressive agents. J Chemother 2012; 24: 240–42.
83 Livovsky DMM, Leibowitz D, Hidalgo-Grass C, Temper V, Salameh S, Korem M. Bordetella holmesii meningitis in an asplenic patient with systemic lupus erythematosus. J Med Microbiol 2012; 61: 1165–67.
84 Van Balen T, Nieman AE, Hermans MHA, Schneeberger PM, de Vries E. Bordetella holmesii meningitis in a 12-year-old anorectic girl. Pediatr Infect Dis J 2012; 31: 421–22.
85 Allende LM, Corell A, Manzanares J, et al. Immunodeficiency associated with anorexia nervosa is secondary and improves after refeeding. Immunology 1998; 94: 543–51.
86 Layton M, Weiss D. Alert #23: Bordetella holmesii bacteremia in children. New York City, New York City Department of Health and Mental Hygiene, 2010. http://www.nyc.gov/html/doh/downloads/pdf/cd/2010/10md23.pdf (accessed Jan 23, 2014).
87 Russell FM, Davis JM, Whipp MJ, et al. Severe Bordetella holmesii infection in a previously healthy adolescent confirmed by gene sequence analysis. Clin Infect Dis 2001; 33: 129–30.
88 Clare S, Ahmed T, Singh R, Gough S. Bordetella holmesii: a rare cause of bacterial endocarditis in a post-splenectomy patient. BMJ Case Rep 2010; published online May 6. DOI:10.1136/bcr.11.2009.2459.
89 Soloaga RN, Carrion NA, Almuzara M, et al. Bordetella holmesii endocarditis in an asplenic patient. Rev Argent Microbiol 2013; 45: 86–88.
90 Stoddard JM. A case of Bordetella holmseii endocarditis in an asplenic pediatric patient. Clin Lab Sci 2013; 26: 171–74.
91 Moissenet D, Leverger G, Mérens A, Bonacorsi S, Guiso N, Vu-Thien H. Septic arthritis caused by Bordetella holmesii in an adolescent with chronic haemolytic anaemia. J Med Microbiol 2011; 60: 1705–07.
92 Abouanaser SF, Srigley JA, Nguyen T, et al. Bordetella holmesii, an emerging cause of septic arthritis. J Clin Microbiol 2013; 51: 1313–15.
93 Tatti KM, Wu KH, Tondella ML, et al. Development and evaluation of dual-target real-time polymerase chain reaction assays to detect Bordetella spp. Diagn Microbiol Infect Dis 2008; 61: 264–72.
94 Centers for Disease Control and Prevention (CDC). Outbreaks of respiratory illness mistakenly attributed to pertussis–New Hampshire, Massachusetts, and Tennessee, 2004–2006. MMWR Morb Mortal Wkly Rep 2007; 56: 837–42.
95 Loeffelholz MJ, Thompson CJ, Long KS, Gilchrist MJR. Detection of Bordetella holmesii using Bordetella pertussis IS481 PCR assay. J Clin Microbiol 2000; 38: 467.
96 Mazengia E, Silva EA, Peppe JA, Timperi R, George H. Recovery of Bordetella holmesii from patients with pertussis-like symptoms: use of pulsed-field gel electrophoresis to characterize circulating strains. J Clin Microbiol 2000; 38: 2330–33.
97 Seng P, Drancourt M, Gouriet F, et al. Ongoing revolution in bacteriology: routine identification of bacteria by matrix-assisted laser desorption ionization time-of-flight mass spectrometry. Clin Infect Dis 2009; 49: 543–51.
98 Loeffelholz MJ, Thompson CJ, Long KS, Gilchrist MJ. Comparison of PCR, culture, and direct fluorescent-antibody testing for detection of Bordetella pertussis. J Clin Microbiol 1999; 37: 2872–76.
99 Faulkner A, Skoff T, Martin S, et al. Manual for the surveillance of vaccine-preventable diseases, 5th edn. Atlanta: Centers for Disease Control and Prevention, 2011.
100 Dalby T, Fry NK, Krogfelt KA, Jensen JS, He Q, for the pertussis EQA participants. Evaluation of PCR methods for the diagnosis of pertussis by the European surveillance network for vaccine-preventable diseases (EUVAC.NET). Eur J Clin Microbiol Infect Dis 2013; 32: 1285–89.
101 Tatti KM, Martin SW, Boney KO, Brown K, Clark TA, Tondella ML. Qualitative assessment of pertussis diagnostics in United States laboratories. Pediatr Infect Dis J 2013; 32: 942–45.
102 Mandal S, Tatti KM, Woods-Stout D, et al. Pertussis pseudo-outbreak linked to specimens contaminated by Bordetella pertussis DNA from clinic surfaces. Pediatrics 2012; 129: e424–30.
103 Muyldermans G, Soetens O, Antoine M, et al. External quality assessment for molecular detection of Bordetella pertussis in European laboratories. J Clin Microbiol 2005; 43: 30–35.
104 Register KB, Sanden GN. Prevalence and sequence variants of IS481 in Bordetella bronchiseptica: implications for IS481-based detection of Bordetella pertussis. J Clin Microbiol 2006; 44: 4577–83.
105 Sloan LM, Hopkins MK, Mitchell PS, et al. Multiplex LightCycler PCR assay for detection and differentiation of Bordetella pertussis and Bordetella parapertussis in nasopharyngeal specimens. J Clin Microbiol 2002; 40: 96–100.
106 Tatti KM, Sparks KN, Boney KO, Tondella ML. Novel multitarget real-time PCR assay for rapid detection of Bordetella species in clinical specimens. J Clin Microbiol 2011; 49: 4059–66.
107 Fry NK, Duncan J, Wagner K, et al. Role of PCR in the diagnosis of pertussis infection in infants: 5 years’ experience of provision of a same-day real-time PCR service in England and Wales from 2002 to 2007. J Med Microbiol 2009; 58: 1023–29.
108 van der Zee A, Groenendijk H, Peeters M, Mooi FR. The differentiation of Bordetella parapertussis and Bordetella bronchiseptica from humans and animals as determined by DNA polymorphism mediated by two different insertion sequence elements suggests their phylogenetic relationship. Int J Syst Bacteriol 1996; 46: 640–47.
109 Roorda L, Buitenwerf J, Ossewaarde JM, van der Zee A. A real-time PCR assay with improved specificity for detection and discrimination of all clinically relevant Bordetella species by the presence and distribution of three insertion sequence elements. BMC Res Notes 2011; 4: 11.
110 Register KB, Nicholson TL, Guthrie JL. Evaluation of specificity of BP3385 for Bordetella pertussis detection. J Clin Microbiol 2010; 48: 3334–37.
111 Guthrie J, Robertson A, Tang P, Jamieson F, Drews S. A novel real-time PCR assay detects Bordetella holmesii in patients with pertussis-like symptoms in Ontario, Canada. Int J Antimicrob Agents 2009; 34 (suppl 2): S86.
112 Poddar SK. Detection and discrimination of B pertussis and B holmesii by real-time PCR targeting IS481 using a beacon probe and probe-target melting analysis. Mol Cell Probes 2003; 17: 91–98.
113 Njamkepo E, Bonacorsi S, Debruyne M, Gibaud SA, Guillot S, Guiso N. Reply to “Bordetella holmesii in nasopharyngeal samples from Chilean patients with suspected Bordetella pertussis infection”. J Clin Microbiol 2012; 50: 1506.
114 Barrado L, Barrios M, Sanz F, Chaves F. Bordetella holmesii bacteremia in a child with sickle cell disease. Enferm Infecc Microbiol Clin 2011; 29: 779–80.
115 Lam MC, Verity R, Tyrrell GJ, Arent R, Nigrin J, Forgie SE. Gram-negative bacteremia and asplenia in a well 15-year-old girl. Can J Infect Dis Med Microbiol 2008; 19: 391–92.
116 Monnier S, Therby A, Couzon B, Doucet-Populaire F, Greder-Belan A. Bordetella holmesii bacteremia in a 26-year-old patient with sickle cell disease. Med Mal Infect 2010; 40: 299–301.
117 Siegel JD, Rhinehart E, Jackson M, Chiarello L, for the Health Care Infection Control Practices Advisory Committee. 2007 Guideline for isolation precautions: preventing transmission of infectious agents in health care settings. Am J Infect Control 2007; 35 (suppl 2): S65–164.
118 Greig JR, Gunda SS, Kwan JTC. Bordetella holmesii bacteraemia in an individual on haemodialysis. Scand J Infect Dis 2001; 33: 716–17.
119 Pittet LF, Emonet S, Ansari M, et al. Bordetella holmesii bacteremia in a child with nephroblastoma. Swiss Med Wkly 2013; 143: 50S.
120 Weber DJ, Miller MB, Brooks RH, Brown VM, Rutala WA. Healthcare worker with “pertussis”: consequences of a false-positive polymerase chain reaction test result. Infect Control Hosp Epidemiol 2010; 31: 306–07.
121 Steel J, Staeheli P, Mubareka S, García-Sastre A, Palese P, Lowen AC. Transmission of pandemic H1N1 influenza virus and impact of prior exposure to seasonal strains or interferon treatment. J Virol 2010; 84: 21–26.
Related Documents











