© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited http://www.grin.com -1-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-1-

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-ii-
Copyright © GRIN Verlag GmbH
All content copyright restricted. Copying and distribution prohibited. http://www.grin.com
Title Pharmaceutical Drug Promotion in Pakistan Subtitle Issues in Ethical and Non-Ethical Practices Course Pharmaceutical Marketing Author Rizwan Raheem Ahmed Year 2012 Pages 208 Archive No. V276715 ISBN (eBook) 978-3-656-70074-6 ISBN (Book) 978-3-656-70209-2 Biography of Author: Dr. Rizwan Raheem Ahmed holds B.Sc. (Hons.), M.Sc. in Applied Statistics and Master of Science (MAS) in Human Resource Management from University of Karachi. He also earned MBA (Marketing) from PAF-KIET and MBA (General Management) from Institute of Business Administration, Karachi. He also holds MS (Management Sciences) from SZABIST and M.Phil. (Financial Economics) from Hamdard University, Karachi. Dr. Rizwan earned his Ph.D. in Pharmaceutical Marketing from Hamdard University, Karachi. Dr. Rizwan Raheem Ahmed carries more than 19 years of Professional Experience at Senior Management Positions in Sales and Marketing with prestigious National & Multinational Organizations in Pharmaceutical Industry. He has been associated with Indus University since September 2013 as Professor for Business Administration & Commerce department. He has been visiting Faculty for SZABIST for several years. More than 40 Publications (Peer reviewed research articles) are on his credit in reputed National & international Journals including ISI Thomson Reuters indexed & impact factor Journals also. He is also an author of several News articles, which have published in DAWN, Karachi and Business Recorder, Karachi.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-iii-
Copyright © GRIN Verlag GmbH
All content copyright restricted. Copying and distribution prohibited http://www.grin.com
Kontakt Hauptsitz München GRIN Verlag GmbH
Nymphenburger Straße 86 80636 München
Deutschland Tel. +49 89-550559-0, Fax. +49 89-550559-10
© 2008-2014 GRIN Verlag GmbH. E-Mail: [email protected], [email protected]
GRIN Solutions
© Copyright Reserved 2014 All rights reserved. No part of this publication may be reproduced, stored, in a retrieval system or transmitted, in any form or by any means, electronic, mechanical, photocopying, reordering or otherwise, without the prior permission of the publisher. Archive No. V276715 ISBN (eBook) 978-3-656-70074-6 ISBN (Book) 978-3-656-70209-2

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-iv-
PHARMACEUTICAL DRUG PROMOTION IN
PAKISTAN: ISSUES IN ETHICAL AND NON-ETHICAL
PRACTICES
ABSTRACT
Common People and government authorities are usually concerned about the
unethical pharmaceutical marketing practices in Pakistan, therefore; the researcher
examines the unethical pharmaceutical marketing practices in Pakistan, and selected
Karachi City as Case study for this purpose and analyze the impact of unethical
marketing practices in pharmaceutical industry.
This study not only evaluates the responsible variables for the unethical
pharmaceutical marketing practices but also compare who is more responsible for
these unethical pharmaceutical marketing practices in Pakistan. This study also
examines, who has initiated these unethical pharmaceutical marketing practices in
Pakistan and who is responsible for the continuation of these practices in Pakistan.
In this study researcher focuses six variables that can be a major cause of unethical
pharmaceutical marketing practices in Pakistan i.e. Pharmaceutical marketing and
Sales personnel, doctors’ community, retail and whole sales pharmacies,
government and private hospitals personnel, government officials and patients or
their attendants’. All these six variables have been taken and gathered the data
through survey questionnaire, compile and analyze through Statistical tools like
descriptive and inferential Statistics both and conclude the main cause of unethical
pharmaceutical marketing practices in Pakistan.
In the under taken study four different hypotheses were developed and tested
through Z and F test and also analyze the data through descriptive Statistics, for the
descriptive Statistics four different parameters were developed and presented in the
form of graphs and tables. The conclusion of the study was that initially
pharmaceutical industry was responsible to introduce the unethical marketing

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-v-
practices to their customers i.e. doctors community, and hospitals and later on
unethical pharmaceutical marketing practices became the norm of the
pharmaceutical industry. Now the doctors are the main cause or reason for the
continuation of these unethical pharmaceutical marketing practices in Pakistan.
It is further concluded in the study that foreign visits are more common tools in
order to get maximum output from the doctor community and now doctors have
become more demanding and they ask themselves regarding the foreign and local
tours and conferences. Cash incentive and home appliances are another form of
unethical practices in the pharmaceutical industry. Clinic and home decoration are
also the findings of unethical pharmaceutical marketing practices in the under taken
study. However, it is also found that some demands from the doctors’ community or
the offers by the pharmaceutical companies are quite ethical genuine regarding the
scientific meeting and local & international scientific conferences.
It is further concluded that all the stakeholders are agreed that these unethical
pharmaceutical marketing practices can be stopped. They are also agreed non-
qualified doctor’s practice should be eradicated. Pharmaceutical companies should
strictly abide the rules and regulations, which are already mentioned and given in the
pharmaceutical marketing code of ethics, at the same time Pakistan Medical
Association and Pakistan Medical and Dental Association should restrict to the
doctors community to practice in the limit of ethical and moral grounds.
Governmental agencies are also responsible to enforce the prevailing laws with their
true spirit on pharmaceutical companies. If any further legislation is required in
order to stop these unethical pharmaceutical marketing practices then further
legislation should be taken place and strict laws should be made and implemented.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-vi-
A C K N O W L E D G E M E N T
My deepest gratitude and profound admiration are due firstly to my supervisor Dr.
Ahmad Saeed for his help and cooperation in the smooth completion of my Ph. D.
studies at Hamdard University.
My special thanks go to Prof. Dr. Syed Abdul Aziz, Director, Hamdard Institute of
Education and Social Sciences, Hamdard University Karachi for his encouragement
and continuous support during the research and course work.
I am also thankful to my friends, colleagues and well wishers, who constantly pray
for my success. Special thanks to Mr. Abid & Mr. Sajid who supported me
whenever they are asked for any support and help during my research work.
I would like to express my special thanks to all those who participated in this study
and whom I could not mention the names in the list of gratitude.
In last but not lease I appreciate the encouragement and countless help of my wife
during my studies and my parents who always supported me during every step of my
career.
RIZWAN RAHEEM AHMED

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-vii-
TABLE OF CONTENTS Abstract … … … … … … … … … i Acknowledgement … … … … … … … … ii Table of Contents … … … … … … … … iii Chapter I: INTRODUCTION 01 1.1 Background of the Study … … … … … 01 1.2 An Overview of Pakistani Pharmaceutical Industry … … 04 1.3 Statement of the Problem … … … … … 10 1.4 Research Hypotheses … … … … … … 10 1.5 Purpose of the Study … … … … … … 11 1.5.1 General Purpose … … … … … … 11 1.5.2 Specific Purpose … … … … … … 11 1.6 Scope of the Study … … … … … … 12 1.7 Justification … … … … … … … 12 1.8 Definition of Key Words & Phrases… … … … 13 Chapter II: REVIEW OF THE LITERATURE 16 Chapter III: RESEARCH METHODOLOGY 44 3.1 Data, Sample and Methodology … … … … 44 3.2 Total Population … … … … … … 44 3.3 Targeted Population … … … … … … 45 3.4 Sample Size … … … … … … … 46 3.5 Pharmaceutical Sales & Marketing Personnel … … 47 3.5.1 Multinational/National Pharmaceutical Personnel … … 47 3.6 Doctors Community … … … … … … 47 3.6.1 General Practitioners (Both Rural & Urban) … … … 47 3.6.2 MOs & RMOs of Public & Private Hospitals … … … 47 3.6.3 Consultants of All Specialties… … … … … 47 3.7 Hospitals … … … … … … … 47 3.7.1 Public Hospitals … … … … … … 47 3.7.2 Private Hospitals … … … … … … 48 3.8 Pharmacies … … … … … … … 48 3.8.1 Retail Pharmacies … … … … … … 48 3.8.2 Whole Sales Pharmacies … … … … … … 48 3.9 Government Officials … … … … … … 48 3.9.1 Federal/Provincial Government Officials… … … … 48 3.10 Patients or their attendants’ … … … … … 49 3.10.1 Outdoor Patients & their attendants’ … … … … 49 3.10.2 Indoor Patients & their attendants’ … … … … 49 3.11 Plan of Data Analysis … … … … … … 49 Chapter IV: DATA ANALYSIS 50 4.1 Survey Findings …. … … … … … 50

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-viii-
4.1.1 Gender … … … … … … … 50 4.1.2 Age … … … … … … … … 51 4.1.3 Experience … … … … … … … 52 4.1.4 Education … … … … … … … 52 4.1.5 Respondents … … … … … … … 53 4.1.6 Pharmaceutical Personnel… … … … … … 54 4.1.7 Consultants … … … … … … … 55 4.1.8 General Practitioners … … … … … … 56 4.1.9 RMO / MO … … … … … … … 58 4.1.10 Government & Private Hospitals Officials… … … … 59 4.1.11 Retail Pharmacies … … … … … … 60 4.1.12 Whole Sales Pharmacies … … … … … 62 4.1.13 Outdoor Patients … … … … … … 63 4.1.14 Indoor Patients … … … … … … 64 4.1.15 Government Officials (Federal & Provincial)… … … 66 4.2 Hypotheses Testing … … … … … … 67 4.2.1 Hypothesis No. 1 … … … … … … 67 4.2.2 Hypothesis No. 2 … … … … … … 69 4.2.3 Hypothesis No. 3 … … … … … … 71 4.2.4 Hypothesis No. 4 … … … … … … 73 4.3 Qualitative Analysis … … … … … … 75 4.3.1 Tools of Unethical Drug Practices… … … … … 76 4.3.2 Drug Promotion to Non-qualified Doctors … … … 77 4.3.3 Legislation for Unethical Drug Promotion … … … 78 4.3.4 Eradication of Unethical Drug Promotion … … … 79 Chapter V: SUMMARY, CONCLUSIONS AND RECOMMENDATIONS 80 5.1 Summary & Conclusions … … … … … 80 5.2 Recommendations … … … … … … 90 5.3 Suggested Areas of Further Research … … … 92 Appendix – I: 94 Questionnaire … … … … … … … … … 94 Appendix – II: 97 Cross-Tabulation … … … … … … … … 97 Appendix – III: 103 Code of Ethics for Pharmaceutical Marketing … … … … 103 Appendix – IV: 161 The New Pharma Code on Interactions with Healthcare Professionals… … 161 REFERENCES … … … … … … … … 195

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-1-
CHAPTER ONE
INTRODUCTION
1.1 BACKGROUND OF THE STUDY
Unethical marketing practices have become an essential part of the pharmaceutical
industry in Pakistan and roots are so strong that it may not be possible to reverse the
same (Parmar & Jalees, 2004). However the previous study has a limitation. It was a
case study on pharmaceutically industry in Hyderabad. In view of the findings of
that study there was a need to carry out the same on larger basis. Thus this research
has been undertaken with this objective in mind.
The phenomenon of the unethical drug practices is common worldwide but its
severity is deep rooted in developing countries. Unethical drug practices have two
dimensions. One is drug related, and other is drug promotion related. Extensive
research on drug related unethical practices has been carried out internationally.
However, the author was not able to find any empirical study on unethical drug
promotion practices except the one that was carried out by (Parmar, Jalees, 2004) in
Pakistan. Parmar and Jalees (2004) in their study observed that pharmaceutical
industry spends a substantial portion of its budget on market research but do not
carry out the research on unethical drug promotion practices. One of the reasons is
that the industry itself is indulged in this practice therefore it does not find any need
to carry out the research on this issue.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-2-
Lack of research on the subject does not mean that unethical drug promotion
practices do not exist. The pre-survey and focus groups discussions indicate that
unethical pharmaceutical marketing practices have become an acceptable norm of
the pharmaceutical diligence, and it is also well supported by more or less all the
pharmaceutical groups with the cooperation of government hospitals, private
hospitals, doctors and health allied organizations including pharmacies on patients’
interests. All the entities as discussed above appear to be corrupted; therefore, it may
not be fair to blame any one of them, including pharmaceutical industry.
Doctors and other entities as discussed above have become greedy; therefore, these
are vulnerable to Pharmaceutical industry for unethical drug promotion practices.
The Pharmaceutical companies fund nearly all symposiums and educational actions
of doctors; therefore, the industry uses the forum to pursue its goals, which at times
may not be the same as the purpose and objective of the conferences. Pakistan
Medical Journalists Association (PMJA) has published a few articles on this issue.
But this has not affected the prevailing unethical drug promotion practices (Zaidi
et.al, 1995).
The focus of the subject study was to identify the intensity and trends of unethical
drug promotion practices in Pakistan. Ascertaining the contribution of the doctors,
health related institutions and the pharmaceutical industry in promoting such
practices. Unethical marketing practices have now an integral part of drug
promotion. Unethical practices could be classified into two segments. One is related
to the medical side of the drug i.e. the trial of the drug both on animals and the
human, and registration of indications and patent period in different countries.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-3-
According to the prominent scholar and eminent physician of the country, Dr Sania
Nishtar (2007), the unreliable news of bribery and dishonesty in this pharmaceutical
circle have to be given watchful investigation. Health system of Pakistan must have
an effect with these corruption practices. These practices can entail together
supervisory body and private sector. The process of registration, authorization and
pricing criteria, procurement and sales & marketing of drugs are all involve with
these types of practices. These all bad practices has their roots for the commercial
safety of the pharmaceutical companies, who pay heavy cost and struggle to avoid
dealings for the enlistment of their products, accelerate the endorsement procedure,
and catch flattering prices of their products.
The astringent method for procuring medicines proffer money-spinning resource for
most of the bureaucrats and thus suppliers intend to pay bribes, and paying them
through excess in billing and invoicing. In Pakistan, we can find the similar
behaviors in almost every public hospital through unreliable data.
Consequently, healthcare prerequisite rely on a system, which proficiently joins
fiscal and individual assets to deliver system of check and balance, good
management and effective services. Conversely, in our country bad management and
dishonesty in health system are symptoms of a wider system trend. These issues
need be address and entails consent and right both inside and outside of the health
sector system (Nishtar, 2007).
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-4-
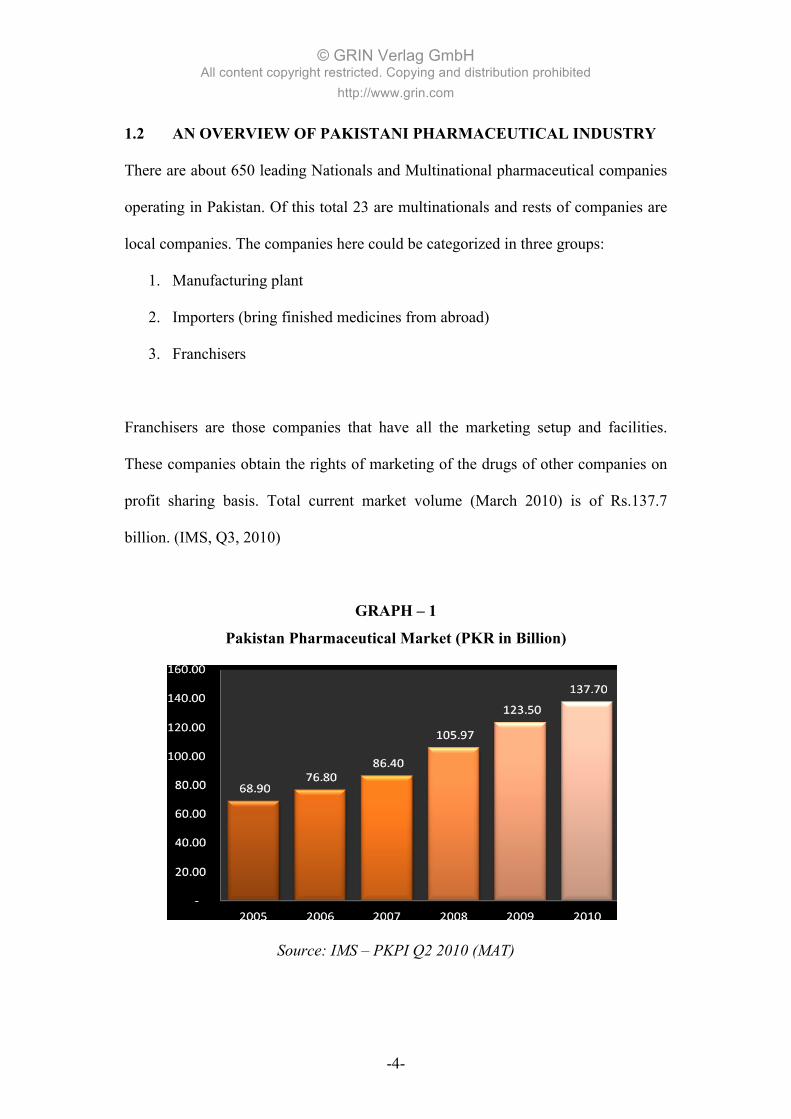
1.2 AN OVERVIEW OF PAKISTANI PHARMACEUTICAL INDUSTRY
There are about 650 leading Nationals and Multinational pharmaceutical companies
operating in Pakistan. Of this total 23 are multinationals and rests of companies are
local companies. The companies here could be categorized in three groups:
1. Manufacturing plant
2. Importers (bring finished medicines from abroad)
3. Franchisers
Franchisers are those companies that have all the marketing setup and facilities.
These companies obtain the rights of marketing of the drugs of other companies on
profit sharing basis. Total current market volume (March 2010) is of Rs.137.7
billion. (IMS, Q3, 2010)
GRAPH – 1
Pakistan Pharmaceutical Market (PKR in Billion)
Source: IMS – PKPI Q2 2010 (MAT)

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-5-
In the year 2009 the industry realized a high degree of fluctuation in the growth rate.
One of the major reasons for such a trend was merger and acquisition, and glutting
the market by local pharmaceutical industry. However on an average the growth
rate in the year 2009-10 was about 15.4% per annum. Comparatively the growth rate
in the year 2008-09 was about 12% (IMS, Q2 & Q3, 2010).
A tough competition exists between the multinationals and nationals, day-by-day
nationals are taking up the share and in the last six years they have taken around 7%
share in value. The gap between multinationals and nationals narrows further during
2009-10 with multinationals losing another 1.7% share to nationals. At present
multinationals hold 46.9% share of the market while the nationals have captured
53.1% of the pharmaceutical business. From around 80% share in the
pharmaceutical retail market, the MNCs have lost around 29% during the last twenty
years as the nationals continue to improve their performance in the market place.
Almost an identical trend is observed in units as well, nationals having 54.05% as
compared to multinationals 45.95% (IMS, Q1 & Q2, 2010).
GRAPH – 2 Top 10 Pharmaceutical Companies (PKR in Millions)
Source: IMS – PKPI Q2 2010 (MAT)

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-6-
The overall market dynamics are tilted in favour of national companies as they are
continuously launching new products at a much faster rate than MNCs, a trend that
is becoming increasingly evident. In terms of new product market in value, the sales
contribution gap between multinational and national companies has also increased
over the last five years. The products launched before 1991 are dominated by the
multinationals while after 1991 it is shifting towards the nationals. However, the
leading 20 products of the industry are still those products, which are launched by
the MNCs between 1970 and 1990 (IMS, Q2 & Q3, 2010).
Of the total markets size of 137.7 billion, the top 20 corporations contribute around
60% of total business, 34% of market concentrated among the top 5 corporations.
The rest 40% of the market is distributed amongst 630 corporations in Pakistan. For
the purpose of calculation in terms of value, the top 15 corporations make up 54%,
top 35 corporations make up 75.09%, and top 75 corporations make up 90.91%,
while the remaining corporations are competing for approximately 9% market share
(IMS, Q1 & Q2, 2010).
The drugs prices of the national pharmaceutical companies are cheaper, as they have
choice of procuring the raw material from those countries where it is available at a
cheaper rate. The other reason for the price differential is that the national
pharmaceutical industry does not invest in research and development compare to
multinationals. Multinational companies invest a huge amount of their net profit in
R & D, therefore, when they introduce a new molecule into the market they have
already invested billions of dollars for a new product, therefore, the price of the new

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-7-
product keeps high in order to meet the total cost of the drug in a certain time period
because after patent period any company can make its Me too or imitation at cheaper
rate. So, the national companies have twice leverage to set their prices at the lower
level i.e. first they did not invest a single penny on Research & Development and
secondly they are having cheaper raw material resources (Ahmed & Jalees, 2008).
Another, important point in price difference is that national companies are not bound
to pay certain amount of profit to any other body, whereas, multinational companies
are paying certain percentage of profit to their parent companies. Moreover, national
companies do not have huge overhead expenses; in contrast, multinational
companies allocate huge overhead expenses in different fields at the beginning of
every fiscal year for every product in a certain ratio, therefore, the cost of goods
(COG) are different in national and multinational companies. In order to maintain all
these costs they are bound to set a high price, otherwise bottom line will be very low
and business would not be feasible any more.
The connection among pharmaceutical companies, doctors and health officials is
also very significant. Commissions may be the reason behind weakness of this
sector, to prevent from corruption strict rules and regulations are needed. Heavily
regulation is indispensable toward safety and protection of peoples in opposition to
inferior and unjustly price of medicines. Another reason for such regulations is to
guarantee that industrial strategies fortify the effective economic development and
improvement in the pharmaceutical sector. These two intentions at times decline
each other’s. If regulators are coercing by pharmaceutical companies, healthiness

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-8-
can be compromised. Charitable campaign and contributions both politically and
socially by pharmaceutical companies are instances of these demands offered to
doctors for stipulating fastidious medicines and specific brand. These behaviors are
very un-ethical as well as illegal in many countries. Most of the companies may
make use of underhand procedure to masquerade such bribe (American College of
Physicians, 1990, 1995-2002).
In recent years, the problem of illegal and unethical pharmaceutical practices for
marketing of medicines has acknowledged an enormous covenant of awareness,
indicating from different pharmaceuticals and doctors association who already keep
noticing of this problem. Some of them have conceded set of codes and ethical
course of action for selling of pharmaceuticals (Ahmed & Jalees, 2008).
There is another kind of practices that reflect corruption happens during clinical
trials. Many pharmaceutical companies are paid to doctors to take patients for
clinical trials. Many universities have research assessment committees who are
engaging in exposure of strategies and actions concerning divergence of interest
(Avorn & Hartley, 1982).
Furthermore, there is discussion on whether confession is adequate: must
researchers permissible to carry out studies and research for organization wherein
they contain finances?

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-9-
Pakistani pharmaceutical industry also growing at rapid pace over last many years
and reached to Rs. 137.7 Billion in 2010 (IMS Q2 2010) in this growth major chunk
came from generic drugs manufacturer or generic drugs in Pakistan.
GRAPH – 3
Generic (Copy) Drugs (% Share of Total Market)
Source: IMS – PKPI Q2 2010 (MAT)
Above graph shows that market share of generic drugs in Pakistan in continuously
increases over the years reach to 53.1% market share and likely to cross 55% market
by the end of this year. This can also validated by the number of generic drugs
making company in top ten pharmaceutical in Pakistan Getz Pharma, Hilton Pharma,
Sami Pharma & Searle are top four generic drugs making companies listed in top 10
pharmaceutical companies in Pakistan.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-10-
GRAPH – 4 Research (Branded) Drugs (% Share of Total Market)
Source: IMS – PKPI Q2 2010 (MAT)
While looking at the research drugs, market share in Pakistan continuously
decreasing compare to the local/ generic drugs making companies in Pakistan more
than 53% market share in year 2010 (IMS Q2 2010).
1 . 3 S T A T E M E N T O F T H E P R O B L E M
Is unethical drug promotion practice is common in Pakistan? Who initiated unethical
drug promotion practice in Pakistan? Who is responsible for the continuation of the
same?
1.4 RESEARCH HYPOTHESES
Based on the theoretical framework, focus group and problem statement the
following hypotheses statements have been developed:
H1o: The level of unethical drug promotion practices in pharmaceutical
industry is high (at least 4) on the scale of (5 to 1)
H1A: The level of unethical drug promotion practices in pharmaceutical
industry is less than 4 on the scale of (5 to 1)

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-11-
H20: The levels of unethical drug promotion practices are high in rural
areas.
H2A: The levels of unethical drug promotion practices are not high in rural
areas.
H30: There is no significant difference on the opinions of doctor,
pharmaceutics companies, hospitals and pharmacies on who initiated
unethical drug promotion practices in Pakistan.
H3A: There is significant difference on the opinions of doctor,
pharmaceutics companies, hospitals and pharmacies on who initiated
unethical drug promotion practices in Pakistan.
H40: The contribution of the pharmaceutical industry in continuation of
unethical drug promotion practices is higher than the doctors.
H4A: The contribution of the pharmaceutical industry in continuation of
unethical drug promotion practices is not higher than the doctors.
1.5 PURPOSE OF THE STUDY
1.5.1 General Purpose
The overall purpose of the study is to analyze the unethical pharmaceutical drug
promotion practices in Pakistan and its impact on common people of the Country.
1.5.2 Special Purpose
Most specifically the study will address the following questions:

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-12-
1. Is there any relationship between unethical pharmaceutical drug promotion
practices & under taken stakeholders i.e. pharmaceutical companies, doctors,
hospitals and pharmacies etc?
2. Who is the most responsible for these unethical pharmaceutical drug
promotions in Pakistan?
3. How common people are affected by these unethical pharmaceutical drug
promotion practices in the Country?
4. Is there any further legislation is required by the government in order to stop
these unethical practices?
5. How different stakeholders can play their role in order to stop these unethical
practices?
1.6 SCOPE OF THE STUDY
The scope of the study will be limited to all the concerned bodies of the government,
pharmaceutical companies, doctor’s community, hospitals, pharmacies and the
common people of the Country, which provides the knowledge about the unethical
drug promotion practices in Pakistan. Moreover, it will also provide the basis to the
government to take some suitable measures to stop these unethical pharmaceutical
drug promotion practices from Pakistan and to provide ease to the common people
of the Country in order to get better health facilities at nominal cost.
1.7 JUSTIFICATION
The study is justified on the following grounds:

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-13-
1. The results of the study can be used by the government and some suitable
measures and actions can be taken to improve the legislation in order to stop
unethical pharmaceutical drug promotion practices in Pakistan on the basis
of the results of the under taken study.
2. The medical facilities can be provide at nominal cost by improving the
atmosphere of unethical pharmaceutical drug promotion practices for the
common people by taking corrective measures against the responsible
stakeholders of the study.
3. To provide the knowledge of actual situation of unethical pharmaceutical
drug promotion practices to all the concerned bodies who are directly or
indirectly involved in these practices and to realize them that they should
fulfill their social responsibilities in order to improve the situation.
4. To give the awareness to the common people of the Country that in the light
of study they should play their role in order to rectify the situation.
5. The pharmaceutical ethical committees on local & multinational
pharmaceutical companies should implement the new or existing code of
conduct with its true spirit after reviewing the results of this study.
6. The concerned bodies’ of government sector should make further effective
legislation and to enforce the rules and regulations in order to stop these
unethical pharmaceutical drug promotion practices in Pakistan.
7. In the light of result of this study, the Pakistan Medical & Dental Committee
(PMDC) and Pakistan Medical Association (PMA) should make some
effective code of conduct for the doctors’ community in order to stop these
unethical pharmaceutical drug promotion practices in Pakistan.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-14-
1.8 DEFINITION OF KEY WORDS & PHRASES
• Unethical Promotion
The promotion of pharmaceutical drugs by avoiding the set of rules &
regulations, which are given by the ethical, bodies Worldwide & the local bodies
& government.
• Pharmaceutical Drugs
The medicines are being produced and sold by the pharmaceutical companies for
human beings.
• Unethical Practices
The unusual and absurd ways of marketing & selling tactics to sell the
pharmaceutical drugs.
• MNCs & Local Companies
The Multinational pharmaceutical companies, which operate more than one
Country, whereas, the companies, which are only operating in Pakistan.
• Whole Sales & Retail Pharmacies
The medicines shops, which procure the pharmaceutical drugs in bulk quantity
from distributors and fulfill the requirement of retail pharmacies, whereas, retail
pharmacies are those pharmacies where the consumers purchase pharmaceutical
drugs directly.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-15-
• Government Officials
The government servants who are employed in those Provincial or Federal
governments deportments, which are directly relevant to the pharmaceutical
drugs, pharmaceutical companies & the pharmacies.
• Public & Private Hospitals
The public hospitals are owned and run by the federal, Provincial or district
governments, whereas, the private hospitals are owned and run by the individual
or group of people.
• Indoor & Outdoor Patients
Those patients’ who are admitted in hospitals due to their illnesses are called the
indoor patients, whereas, the walk in patients or just come to the doctor and get
the prescription and go to home or called outdoor patients.
• Patients & Attendants’
The person who has suffered in any illness is known as patient, whereas, those
patients who admitted in hospital and they have been taken care by their
relatives’ or friends during the treatment are called their attendants’.
• Consultants, Medical Officers & General Practitioners
The doctors who has done post graduation after their medical graduation are
known as Consultants, whereas, those doctors who has started their career as

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-16-
doctor after their medical graduation in any private or government hospital, are
called Medical Officers or Resident medical doctors and finally those medical
graduates who does open their own clinics in different areas are known as
General Practitioners.
CHAPTER TWO
REVIEW OF THE LITERATURE

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-17-
The pre-survey and focus groups discussions indicate that unethical pharmaceutical
marketing practices have become an acceptable norm of the pharmaceutical
diligence, and it is also well supported by more or less all the pharmaceutical groups
with the cooperation of government hospitals, private hospitals, doctors and health
allied organizations including pharmacies on patients’ interests.
A report on practices for pharmaceutical companies has published by Lexchin J.
(1995) in Consumer International (CI). CI scrutinized that 20 main worldwide
medicines companies of the world have developed their own codes of ethics
conducts, which are highly biased in their favor.
Pharmaceutical companies exercise immoral and dishonorable marketing devices to
persuade doctors to recommend their medicines and also delicately to convince
customers to use them. The findings are based on the marketing practice of world
top most 20 pharmaceutical companies. The report contends, “Pharmaceutical
companies are advancing their medicines through patients set, student and internet
chat places to avoid the interdict on promoting excluding doctors” (Lexchin, 1995).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-18-
The authors of the report have also the opinions that the subject companies create
imprecise declares regarding protection and effectiveness of their medicines.
Moreover, the companies also offer enticements to stipulate and uphold medicines
including bribes, donations, expensive promotional gift items, free drug samples and
conferring contracts. The authors pointed out that several organizations encompass
concerned in non-aggressive policies (Lexchin, 1992, 1995).
In September 2009, Pfizer was fined US$2.9 billion dollars for deceitful marketing
practices. This was done because the company was promoting medicines for
unapproved uses or “off-label uses”. Pfizer deliberately encouraged doctors to
prescribe four medicines to treat symptoms the drugs were not approved by the FDA
to treat. The settlement also settles allegations that Pfizer induced doctors to
promote these "off-label" uses by paying for their meals and subsidizing their travel.
This is the third settlement that Pfizer has signed a “corporate integrity” agreement
(Gibbons et al., 1998).
This is just an example of the deceitful and underhanded marketing practices that
has occurred. This wrongdoing was done due to the fact that it takes approximately
US$1 billion to develop and test a new drug. In recovering their spending, the
companies want healthcare professionals to subscribe their drugs as widely as
possible (Gibbons et al., 1998).
Another example is that of Johnson & Johnson unlawfully and successfully
promoted Propulid off-label for kids regardless of inner objection complaining

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-19-
safety issues. The side effects of this drug include serious cardiac arrhythmias
including ventricular tachycardia; ventricular fibrillations have been reported in
patients taking Propulid (generic name: Cisapride). This product is no longer
available in the United States (Sibbald H., 2004).
Other companies have gotten in trouble over off-sales promotion and withholding of
critical information. In 2004, the medicine title Vioxx manufactures by the Merck &
Co. pharmaceutical company was inhibited from the market. Merck willingly
removed the medicine by reason of serious unease on cardiovascular side effects.
Allegedly the company knew that the drug may perhaps raise the probability of heart
attacks in cardiac patients from 2000 and has been charges of engineering research
outcomes to minimize the threat. In the United States, above 6,000 court cases have
been filed by public who suffer from this medicine (Boseley, S., 2006).
Again in 2004, GlaxoSmithKline (GSK) was faced a court case for preservation off-
putting data on their medicine Paxil (Paroxetine). GlaxoSmithKline decided to an
arrangement to make public regarding results of all clinical trial reviews on its
website (Sibbald H., 2004).
The case happened following a secret GSK memorandum disclosed to press
acknowledged a clinical trial in 1998 so as to wrap up paroxetine had refusal
outcome in the handling of young people. AstraZeneca faced a class action lawsuit
alleging that it was misleading in its promotion of its top-selling ulcer treatment
Nexium. The lawsuit was brought on behalf of trade union healthcare providers in

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-20-
New York who paid for the drug on behalf of their members. It demanded the return
of profits made on Nexium, which had sales of US$3.3bn. It claimed that Nexium is
an end to useful than Prilosec, AstraZeneca's older ulcer drug, which is considerably
low price as it is no more secluded from opposition by copyrighter (Tomlinson H.,
2004).
Gifts that are given by the pharmaceutical industry to healthcare professionals are
controversial. Approximately, US$11billion is spent on promotion and marketing
each year towards doctors (Gibbons et al., 1998).
A case was inspected against GlaxoSmithKline (GSK) from Italian and German
official for supposed corruption of distributing illegal gifts to doctors and other
officials, and approximate €228m from 1999 to 2002. After that, GSK has formed
marketing ethical codes for his employees, which are compulsory to all new
employees to clear an evaluation test. In 2001, a report was public and pointed out
87 employees was terminated or voluntarily departed after violation of these codes
(Boseley, S., 2006).
Charges were implicated in opposition to AstraZeneca for unsuitable use of gifts and
promotions. In a promotional campaign they invited doctors to attend this
seminar/conference free of cost, and they bear their hotel, flights and other charges
(Boseley, S., 2006).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-21-
Studies were carried out to uncover the impact of relation between physician and
medical representatives of pharmaceutical industry. Doctors meeting with
pharmaceutical representatives linked with requirements by doctors to put in
medicines to the hospital formulary and there was a change in prescribing practice
of the doctor (Tomlinson H., 2004).
Overall, residents and physicians have the same attitude towards pharmaceuticals
representatives. Physicians believed that they offer precise data regarding the
medicines that they promote. They also believe that pharmaceuticals representatives
may perhaps offer precise data on recognized or substitute medicines. On the other
hand, the majority considers that representative’s precedence the promotion of
product over the wellbeing of the patient and use unethical practices to do this
(Tomlinson H., 2004).
In the United States, once a medical student comes into school, the pursuance of
pharmaceutical companies is significant. Free promotional gift items, medical
manuals, journal subscription payments, lunches, and gifts are provided to the
medical student. These all are become a component of daily medical practice. The
sales representatives from pharmaceutical companies are good-looking, likeable and
imminent. From an early stage in the doctors’ career, the pharmaceutical companies
have an influence on the medical student (Sibbald H., 2004).
Another study (Zaidi et al., 1995) explores the connection involving in physicians
and the pharmaceutical industry. The author while criticizing the pharmaceutical

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-22-
industry observed that the industry is responsible for corrupting the medical
profession. The report further indicated that this habit is very widespread in the
urbanized countries as well as developing countries.
The author further alleged that the anticipation and requisite of physicians/doctors
has increased manifold. The attitude of doctors has changed, and some of the
commonly demanded requests are presented below:
• The doctors frequently ask for free travel and hotel accommodation.
• The doctors demands donations for various issues and threaten to not
entertain Medical Representatives, if they fail to provide the same.
• Group of doctors have formed companies. The doctors do not manufacture
the medicine in this company, but they have obtained the marketing rights
from the other companies. Subsequently these doctors heavily prescribe their
products.
• The liaison between doctors and chemists has increased tremendously. In
this kind of relationship the doctors prescribe those medicine that carry
heavy discounts, which are then shared by the doctor and chemist as per pre
agreed arrangement.
• It is a common practice of doctors asking cash for each recommendation of
medicines.
• Demand for renewal of hospitals and clinics.
Zaidi, et al., (1995) observed that in the 13th national psychiatric conference held at
Abbottabad in September, nine papers were read by different doctors; however,

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-23-
most of the papers were not on the subject issue but were mainly focused on their
experience of administrating specific drugs to the patients. Incidentally, some of the
foreign guests thought that the conference was not on psychiatric issue but it was
more on the specific drug promotion activity. Two inferences could be drawn from
this incidence. One, the doctors are so much involved in the unethical drug practices
that they did not realized what was the objective of the conference. Second is that
the doctors did not spend considerable time for developing the appropriate paper for
the conference.
Zaidi, et al., (1995) in the same report pointed out about an incidence of the 17th
International Gastroenterology conference held at Rawalpindi. In this conference
about a dozen of local doctors’ presentations were on a particular drug that belonged
to the pharmaceutical company that was sponsoring the event. The foreign delegates
became so frustrated with the proceeding that they left the conference by stating that
their purpose of the visit was to gain insight and share their views on the issue
“gastroenterology”. However, the conference appears to be one directional with
objective of promoting the drugs of the sponsoring company.
Zaidi et al. (1995) also pointed out that unethical drug practices was originally
initiated by multinationals as they were in the position to afford this unethical
practices due to huge resources at their possession. Subsequently, the local national
companies also followed the suit, and now it has become the norm of the industry.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-24-
In Nepal, a study conceded Giri, BR., Shankar, PR., (2005) also observed that
doctors recommend such drugs that are keenly promoted by representative. The
authors observed that the pharmaceutical companies use conferences and seminars
for entertaining doctors, unethical demand of traveling, and lodging etc.
According to Fisher et al., 1993, “It is immoral for research journals that issue
information on psycho-Pharmacology to recognize medicine company money for
everything. Similarly, it is unethical that the American Psychiatric Association
permits Medicines Company financially supported symposia as part of its yearly
meetings” (Fisher, Bryant & Kent, 1993).
According to the WHO Ethical Criteria for Medicinal Promotion, the nastiest
immoderation of deceptive and unprincipled promotion of drug keep on in
developing countries, where parameters for pharmaceutical industry are very weak
(American College of Physicians, 1990).
Promotion can be defined as “the information whose intention is to promote or
market a product and for itself it has an inbuilt unfairness in favor of the product in
the finest doable way. Worldwide, an enormous disparity in the funds obtainable for
promotional against existence of self-governing information (Lexchin, 1995).
Another study of Lexchin pointed out that the Companies which prop up
tranquilizers and antidepressant medicines through similes of women are nonentity
to flout the agreed product tagging, but they probably to give a well-acknowledged
setback of unsuitable stipulation of psychotropic medicines to women (Lexchin,
1992).
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-25-
The Lexchin further concluded in the study that most of the countries rely a lot on
overseas multinational pharmaceutical companies, through exports and local
production. Promotional actions must focus to parameters according to the
company’s origin country. “Promotional materials and labeling should be required
to be acceptable in both countries, i.e. to adhere to the higher of the two standards.
This would put more of an onus on governments in industrialized countries to
prevent messages with negative health consequences from being provided overseas
by multinational companies with head offices in their country” (Lexchin, 1992).
Arun Phatak studies concluded that pharmaceutical industry is already profit taking
and intends at giving utmost profit to share owners. The pharmaceutical industry is
not worried about their consumers, or else the market would not be swamped by
illogical formulations. In United States, it obtains $9.4 million to build up a fresh
medicine and catch its approval. The only approach to give back this is through
forceful promotion. An expected 20% of drug companies’ funds are used up on
marketing of drugs; and of this amount, 20% is used up on retaining and instructing
medical representatives, 30% for publicity media, and 50% for unusual schemes
which involves dinner meeting for doctors and other medical staff, printing &
publication of books and other materials (Phatak, 1998).
Arun further concluded here can be no doubt of getting a handsome profit in this
industry. The obnoxious is taking advantage by deceitful ways:

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-26-
• Imperfect and insufficient product information provided by medical
representatives. However, it is the solitary resource of information related to
drugs for most of the practitioners.
• Support for educational actions can be suitable if it is exclusive of filaments
and the event’s planners is the only decision making authority of each and
every portion of the event: Donations should be given to the institutions, and
the charges of speaker should be pay back by the proficient, not by the
pharmaceutical company.
• Funding should be handed to institutions and certified bodies not to
individual persons.
• The practitioners must worry about fake information and advertisements in
the media for drug injurious to the health. They prohibit on advertisements of
alcohol, child milk substitutes and feeding bottles are examples of this
concern. Medicine companies also publicize their drugs in research journals
and publications. It has to be making sure that incorrect information and
messages are not given, and ridiculous medicines are not promoted through
advertisements.
• The medicine companies convince doctors to recommend specific medicines
by giving gifts or payments. In Pakistan, where poverty stripe of people is
40%, the payments and gifts connection infringe the moral values of loyalty
and non-maleficence. Medicines companies like LOCOST, who do not
involve in unprincipled marketing and promotional activities of their
medicines, are capable to offer valuable and standard medicines under
common names at half price as compare to market rates (Phatak, 1998).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-27-
Daniella, & Michael studied the interaction between medicine companies’
representatives and physician in training sitting. According to them contact with
medicine companies’ representatives were widespread among locals. Most of the
trainees experienced that the connections were suitable while other think that their
own prescribing could be predisposed by gifts or relations, but were more possible
to deem that others' prescribing could be inclined. Occupant prescribing was linked
with pharmaceutical representative appointments and the accessibility of medicines
samples. A range of rules and instructive interferences come into view to sway local
mind-sets toward relations with pharmaceutical companies, though information on
the durable possessions of these interferences is inadequate. In general, locals
reported deficient exercises in this area (Daniella & Michael, 2005).
Finally they concluded that the drug industry has a noteworthy existence for the
period of placement training, has added on the whole receiving of trainees, and
come into views to control prescribing activities. Training sessions can promote
from policies and curriculum that educate residents about industry manipulate and
traditions in which to gravely assess information that they are provided.
Komesaroff and Kerridge (2002) evaluate numerous issues regarding the connection
between medical practitioners and the drug industry, highlighting that planning
between doctors and drug companies have to be transparent and obvious. They
recognize the key sources for concern and inspect ways in which unusual phases of
the medical profession are missing susceptible to sleaze. Furthermore they
recommended the points, which are as follows:

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-28-
• Drug companies and medical practitioners serve each other interests that
occasionally overlie and clash.
• There is sturdy proof that relations between drug industry and medical
practitioners manipulate the last actions in relation to clinical decision-
making as well as carry out of research.
• Present the jeopardy of concession relationships with patients and the
honesty of the research process, physicians must work out in their
communication with pharmaceutical industry.
• The basic philosophy for the behavior of physicians with respect to drug
companies must directness and lucidity.
• Evidently uttered measures should be constructed to deal with precise
problems such as traveling expenses, delivery of gifts, funding of
conferences and seminars and enduring education activities.
According to Bodenheimer (2000) and Mathieu (1999) Doctors and the drug
companies carve up a number of common interests. For example, both are anxious
with heartening effectual and accountable utilization of accessible medicines in
handling and care, their usage monitoring, and pioneering research. But both parties
have different importance and having different center of attention. Doctors are
concerned mainly in patient health care and scientific advance, while companies are
interested first and foremost in financial benefits. The resemblances and
dissimilarities between participants and their interests generate both a requirement
for dialogue and the possible for differences. The contribution for medical
knowledge and practice done by drug industry has been considerable. The cost of

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-29-
development of a fresh medicine is between US$300 to $600 million, nearly all is
provided by pharmaceutical industry. Clinical research is also luxurious: last year, in
the United States, about US$6 billion was used up on clinical research, out of which
70% came directly from drug industry. The total amount used for research and
development is still much superior. In spite of these clear mutual benefits and
interests of cooperation, both the medical profession and the community have
expressed concerns of an ethical nature. There are three main concerns:
1. The probability of connection between physicians and medicine companies
may dole out commercial purposes of industry and greedy interests of
clinicians more willingly than lawful thinking, research and educational
objectives, thus compromising the main moral compulsion of doctors to
patients, dividing the faithfulness of physicians and discouragement the
fundamental belief on which clinical relations depend.
2. The hazard that medicines promotion will unsuitably pressurize physician’s
decisions.
3. The risk that industry participation in research and development of new
drugs will lead to deformations in scientific confirmation and stop self-
governing appraisal of information.
Parmar and Jalees, 2004, developed the distinctions between ethical and unethical
drug promotions practices based on the focus group discussions. “The acceptable
norms of promoting drugs through doctors are visiting them, giving a presentation
on the merits and demerits of the drugs. Explicitly, pointing out the side effects of
drugs, giving nominal quantity of drugs sample. These gifts and give away must not

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-30-
be highly expensive and restricted to items such as dairies, calendar, year planner,
etc.” (Parmar & Jalees, 2004).
“The drugs thus prescribed to the patients on the merits of drugs with focus on the
well being of the patient will fall in the category of ethical drug promotion
practices.”
“Comparatively, unethical drug promotion practices are prescribing drugs to the
patients based on the monetary considerations, and ignoring the well being of the
patients. The commonly used monetary rewards for unethical promotion of the drugs
are discussed below” (Parmar and Jalees, 2004).
(i) Monetary Reward
The crudest type of immoral medicine promotion is financial return. In this type, the
cash payment is associated with the quantity of the medicine prescriptions by the
physicians. The rewards are given on quarterly or monthly basis.
(ii) Visits With in Country
In this category, the drug companies manage seminars and conferences for the
physicians in those cities where doctors are not domiciled. The purpose of such
arrangement may be to keep informed physicians on the current advances in the
industry, but the actual intention is to offer effusive paid medicines. The drug
companies manage the travelling expenses, accommodation expenses in posh hotels.
This paid medicine may possibly for the physicians their families. Doctors travel to

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-31-
other cities for personal reasons. The pharmaceutical firms entertain the doctors by
arranging the air traveling with lodging & boarding expenses of the doctors’
personal visits.
(iii) Foreign Visits
Drug companies organize overseas visits of the physicians. Like in country
travelling, these visits are managed in the setting of conferences and seminar, but
again actual aim is to offer paid medicines.
(iv) Gifts & Give away
a) Medical Equipments: Drug companies offer medical instruments like
stethoscope, thermometers, surgical kits and other expensive medical
equipments.
b) Personal Use Items: Drug companies provide personal use items such as
mobile, laptop, air-conditioned, and even cars.
(v) Chamber Decoration
In this category, the drug companies refurnish the physician’s clinics, as well as
provide air-conditioners, furniture, display boards, computers etc.
(vi) Home Decoration
The arrangements for the home display is alike to the physician’s clinics decorations
as mentioned above.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-32-
One author has suggested in the study (Brennan et.al, 2006), that doctors record their
attachment with medical companies. Actually, data given to the people who are most
expected to be debilitated looks most rational. Drug companies promote their
medicines to doctors, patients, and facilities for health care in turn to boost sales and
reinforce sales revenues. Literature shows many marketing models, which deal with
the control distressing: What are the conditions at which companies and peoples
select medicine for their use (Aaker & Williams; 1998, Bar-On & Parker; 2000,
Curcura, 1999; Gonul et al., 2001; Mintzes, 1998, 2002; Tutor2u, 2004; Wolfe,
2002).
In many research papers, we can easily find literature regarding the control of
Medicine Company fully funded gifts and paid education for medical students,
practicing expenses of experience and naïve doctors (Avorn et al., 1982; Curcura,
1999; Gonul et al., 2001; Stolberg & Gerth, 2000; Wazana, 2000).
Pharmaceutical companies used approximate more than 11 billion USD per year for
their marketing and promotion budget, between 5 to 8 billion USD set off to
promotion of medicines through their sales staff (Greene, 1999, 2000), and for
doctors a projected 8-13 thousand USD per year used up (Gibbons et al., 1998;
Greene, 1999, 2000; Wazana, 2000; Westfall, McCabe, & Nicholas, 1997, 1998).
Medical students, experience and naïve doctors fully confessed that listeners in
seminars and conferences latently fewer incase of lack of lunch and gifts (Steiman,
Shlipak & McPhee, 2001; Wazana, 2000).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-33-
According to an article published in New York Times, which shows the explication
of investigation by Federal Department. It engages different pharmaceutical
manufacturers for example Schering-Plough, Bristol-Myers Squibb, Johnson and
Johnson, and Wyeth (Coleman, J., Katz, E., Menzel, H., 1968)
In the course of an assessment of interrogation with doctors and managements of
drug manufacturers, the government has acknowledged unsuitable, incongruence
and unlawful promotional campaigns. It comprises of financial payback and
appreciating medical doctors to invoice intermediary payers for medicines delivered
to physicians with no cost (Harris, 2004).
In recent years, different medicines companies have pled blameworthy to elicit
accuse connecting the promotion of their medicines and even paid some fines. In
2001 TAP Company paid 875 million USD, while in 2003 Astra Zeneca paid 355
million USD. Beside this a multinational Pharmaceutical company Pfizer settled to
pay 430 million USD against fines. These all are beseech culpable to unlawful
allegation of dishonesty for heartening doctors to tab government against free
medicines, which these companies delivered to doctors (Harris, 2004).
A question has been lifted due to these problems related to unprincipled influence
those programs which could cover doctors’ stipulated observations (Avorn et al.,
1982; Curcura, 1999; Gonul et al., 2001; Wazana, 2000, Wolfe, 2002). A number of
investigation claimed that students and residents of at medical universities
considerably undervalue the control medicine organization fully funded education

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-34-
has on their prescribing practices (Steinman et al., 2001; Wazana, 2000; Waud,
1992).
A research shows that 46% of doctors stated that medical company sales and
marketing persons be fairly significant in pressurizing their set down practices
(Avorn et al., 1982). Other researchers claimed that 61 percent of residents at
medical universities affirmed that marketing and promotions by pharmaceutical
companies did not weight their own selection of medicines, on the other hand the
remaining 16 percent understood other doctors to be also uninfluenced (Steinman et
al., 2000).
In 2002, survey conducted by the journal Medical Economics found that 71% of
doctor’s respondents did not consider that accepting gifts, trips or hospitality weaken
their objectivity (Murray, 2002). Murray reports, “Indeed, many physicians found
the suggestion that they may be influenced insulting” (Murray, 2002).
For the treatment of hypertension “Chew & Colleagues” researched in year 2000, if
the sample was obtainable in the office to hand out a patient, over 90% of doctors
would distribute a sample that different from their chosen medicine options.
According to Industry estimate in 2000, 7.2 billion USD values of free medical
samples were distributed in 2000 (IMS Health, 2002).
Westfall et al. (1997) found that 96% of physicians and their staff had taken drug
samples for personal and family utilization in last year. The authors projected that

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-35-
the value of these drugs is about USD 10,000. Westfall, et al. further states: “The
use of whatever medication is available on the sample shelf (usually the more
expensive of several options) is contrary to the development of good prescribing
habits that will be necessary for success in practice”.
In 1995, Hodges observed exchanges between medical company representatives and
psychiatry residents and confine in 7 teaching hospitals in Canada. Findings
illustrated an association between the receipt of promotional marketing materials
and a conviction that conversation with the medical representatives did not pressure
doctor’s prescribing. The more promotional gift items the resident or intern had
received, the less likely he or she was to consider the medical representative
prejudiced his or her prescribing (Hodges, 1995).
In 1997, a team from University of Chicago studies advertising heading for medical
students and the students’ approach towards medical company’s representatives. The
study instituted that 90% of the students had received one or more medical books
from medical company’s representatives. The medical students whispered that the
medical company’s representatives to be obliging and edifying and also affirmed
that they felt compelled to take note to the medical company’s representatives
informational sales ground once they had received a free gift or meal (Sandberg,
Carlos, Sandberg E., & Roizen, 1997).
Wang et al. (1999) found that there was a considerable boost in doctor’s demands
for specific medicine to be placed on their hospital’s pharmacy after attending an

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-36-
educational conference/program funded by the drug manufacturing company. In
parallel Wazana (2000) reported a conclusion from 29 articles found in the peer-
reviewed literature linked attitudes towards, the connection between doctors and the
drug manufacturing industry and its outcomes on the attitudes, knowledge and
behaviors of doctors.
Haxby (1995) inspects medicines samples circulated by drug manufacturing
companies to the Oregon Health Sciences family medical clinic more than 14
months and found that the medical clinic received a total of 1117 separate visits,
ensuing in 331 different medicine samples from 43 different drug manufacturing
companies. A good number of the clinic’s health care providers confessed they
didn’t know in fact what was distributed when they signed for drug samples. A lot of
the medicine samples delivered were found to be medicines that were not stocked by
the clinic’s pharmacy and even not an approved drug at the clinic (Haxby,
Rodriguez, Zenchnich, Schuff, & Tanigawa, 1995).
These results have lead to the progress of numerous nonprofit companies focusing
the importance of doctors and drug manufacturing company’s representative contact
and on any unsuitable marketing and promotional activities. An internal medicine
doctor Goodman from New York founded one such company, No Free Lunch. The
company’s message is “Our quarrel is not with the pharmaceutical industry, but with
pharmaceutical industry promotion. The time has come to eliminate its influence
from our practices” (No Free Lunch, 2002a). The supporters and membership of ‘No
Free Lunch’ are listed as “physicians, pharmacists, dentists, nurses, physician
assistants, medical ethicists and others” (No Free Lunch, 2002a). The company
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-37-
provides indication lists from main pharmaceutical-physician studies, a forum for
concerned health care professionals and a power point presentation, which is also
downloadable on the topic of drug manufacturing company’s influence, gifts and
promotions. The site sells paraphernalia such as tee shirts and coffee mugs to hoist
income for its effort. The web site also encloses a pledge that physicians may take if
they are dedicated to being free of pharmaceutical company influence. The pledge
states:
“I, __________________, am committed to practicing medicine in the best interest
of my patients and on the basis of the best available evidence, rather than on the
basis of advertising or promotion. I therefore pledge to accept no money, gifts, or
hospitality from the pharmaceutical industry; to seek unbiased sources of
information and not rely on information disseminated by drug companies; and to
avoid conflicts of interest in my practice, teaching, and/or research” (No Free
Lunch, 2002b).
In 1999, a research was conducted by Kessenich and Westbrook focused on the
relationship of nursing and pharmaceutical sales persons’ and other reason that
could create impact on prescribing practices by taking interview from 6 Nurse
Practitioners in the New England area. According to Kessenich and Westbrook, the
Nurse Practitioners were asked about:
1. Medicine data from drug manufacturing company sales persons.
2. Basis of upcoming medicines,
3. Approval of medicines samples,
4. Providing gratis medicines samples,

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-38-
5. The professed pressure medicines samples their selections,
6. Approval of hand-outs
7. Attendance at pharmaceutical company sponsored events,
8. Concentration to drug manufacturing organization marketing campaigns
Of the sample population, 100% of the Nurse Practitioners had participated drug
manufacturing company’s funded educational programs and all of them had taken
free sample medications for their patients. 4 out of 6 Nurse Practitioners i.e. 67%
had get verbal or written communication about pharmaceutical products during
pharmaceutical company encounters for example office lunches, they believed the
accessibility of sample medications might have influenced their prescribing choices.
All 6 Nurse Practitioners had read medicine’s advertisements in medical
professional journals and 100% of the Nurse Practitioners believed that drug
manufacturing companies influenced their prescribing behaviors, “even in a
subliminal manner” (Kessenich & Westbrook, 1999).
New technique of marketing is to target the patient consumer rather than the MD,
NP, or PA. Since the early 1990’s, drug manufacturing’s companies have been
publicity directly to the consumer (DTC) through different media advertisement
such as television advertisements, billboards and gifts, mass market publications that
attract the patient to ask for specific medicine when they see their healthcare
provider (Manning & Masia, 2001). A lot of the advertisements hire popular media
personality to pitch their medicines including Olympic Gold Medalist ice skater
Dorothy Hamill advertising for the arthritis medication Celebrex and Senator Bob

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-39-
Dole extolling the virtues of Viagra. These advertisements lean to show the
medicine as the most excellent, effective and latest for the complaint. Many
conclude that if the patients’ doctor is not prescribing this medication for them, they
are not receiving the best possible recovery of their illness (Ingelfinger, 1972;
Mintzes, 1998; Mixed Reaction to Consumer Advertising, 2003). These tactics
encourage the patient to request the medical doctor or Nurse Practitioners about the
medicine and occasionally to point out the advertised medicine instead of besides
their current medications (Mintzes, 1998; Wolfe, 2002). Patient asks for precise
medicine has been acknowledged to impinge on doctor’s choice of prescription for
the patient (Mixed Reaction to Consumer Advertising, 2003; Steinman et al., 2001).
Wolfe notes, “There is evidence that many drug advertisements are not balanced or
accurate and duped gatekeepers may not adequately resist patients’ exhortations to
write a prescription” (2002, p. 525).
In general, budget for promotion on prescription medicines mounted to 15.7 billion
USD in 2000, rise from 13.9 billion USD in 1999 and only 9.2 billion USD in 1996
(National Institute for Health Care Management, 2001, 2002). An anticipated 2.5
billion USD were used up on direct to consumer advertising in 2000 up from 1.8
billion USD in 1999 and 791 million USD in 1996 (National Institute for Health
Care Management, 2002). Sales amplify of 50 medicine most profoundly advertised
to consumers were conscientious for almost 47.8% (Half) of the 20.8 billion USD
rise in spending in 2000 (National Institute for Health Care Management, 2002). In
2000, a pharmaceutical company Merck spent 161 million USD on promotion and
advertising for Vioxx, a new medicine for respite of arthritis pain. Explicitly over

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-40-
Anheuser-Busch spent advertising Budweiser beer (146 million USD) or Pepsico
spent advertising its soft drink, Pepsi Cola (125 million USD). The boost in Vioxx
sales in 2000 accounted for 5.7% of the one-year rise in medicine spending in the
United States (National Institute for Health Care Management, 2001, 2002).
In the beginning of 1990, apprehension arose by American College of Physicians
related to persuasion by drug manufacturing unit’s funded institutional events and
offering for doctors and students’ recommended observations (American College of
Physicians, 1990; American Medical Association, 1991; Wazana, 2000). According
to their research they pointed out prospective persuasion from drug manufacturing
organizations might affect doctors recommended observations. Regardless the report
from past more than 10 years, and American Medical Associations and the
American College of Physicians’ suggestions so it subsist conversed among
residents & students, and after the discussion the studies demonstrated that merely
23 - 50 percent of medical residents familiar with current statement (Gibbons et al.,
1998). The information related to the manipulation that drug manufacturing
organization fully funded edification has on the recommended observations of
students and residents has consequence in a recent American College of Physicians
position statement released on March 5, 2002 (Coyle, 2002a; 2002b). According to
this, restated the necessitate in support of consciousness of the insinuation of drug
manufacturing organization fully funded edification and its control on recommended
observations and suggested that the entire doctors, student and residents has to get
teaching on this matter (Coyle, 2002b). In 2002, the existing declaration exclusively
spoken to conscientiousness who have completed their education and who have not,

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-41-
universities have to make sure that neutral edifying substance has offered and
universities course of actions be primed to recognize suitable & deplorable
connections with the drug manufacturing organizations equally for practicing
doctors and for medical students (Coyle, 2002a; 2002b).
Similar guidelines are formed from different professional medical associations
regarding relations of doctors and sales persons of pharmaceutical companies and
are recognized by Royal College of Physicians and Surgeons of Canada, Canadian
Medical Association, Academy of Medicine and American College of Physicians
and United State Medical Association (Wazana, 2000). Despite their position
regarding the influence of drug manufacturing companies, the American Medical
Association persists headed for 20 million USD in a year by advertising
comprehensive professional and personal data on all physicians working in US for
utilizing medical company’s doctors prescribing databases (Stolberg & Gerth, 2000).
Different researches have explained, and direction from U.S. Department of Health,
professional medical associations, Human Services’ Office of Inspector General
(OIG) and different industry trade associations mirrors distress that, the prospective
that the promotional efforts by pharmaceutical companies could have a unswerving
and thoughtful consequence on doctors prescribing practices, which may brunt
medical finding (Hemminki, 1975). This conflict of interest is not only receiving
substantial concentration in the media but it is also making news in the form of
enforcement actions and legislation. In consideration of the surprising costs linked
with these marketing practices approx. 90% of the 21 billion USD marketing

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-42-
finances of the drug manufacturing industry are heading for doctors, in spite of a
staged augment in direct-to-consumer advertising (Holmer, 1999). The apparent
incapability to manage increasing healthcare costs, it is not shocking that
pharmaceutical company’s gift-giving and other promotional and marketing
practices have get nearer under strict scrutiny and interest by federal and state
enforcement agencies and also self regulation by the pharmaceutical companies,
doctors and hospitals (Catlin et al., 2007).
Current study focused the suggestion of JAMA article’s related the association
between drug manufacturing companies and medical doctors and related
professionals. In April 2007, a nationwide research published in the New England
Journal of Medicine (Campbell et al., 2007) set up that in United States about 94%
of physicians stated a number of relationships with the pharmaceutical industry, and
78% receiving free medicines samples while 83% of these connections concerned
getting food in the place of work.
The investigation finally concluded that drug companies were expected to offer
payments and gifts to doctors who were recurrent recommended those companies’
medicines as compare to those who were less prescriber (PhRMA, 2002a, 2002b).
Ahmed & Jalees (2008) have conducted a study on the same topic and concluded
that both doctors and pharmaceutical companies are equally responsible for
unethical drug promotion practices in Pakistan. But most important and interesting
findings were, "basically pharmaceutical companies are responsible for initiating
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-43-
these unethical drug practices in Pakistan but now in continuation of these practices
the doctor’s community is actually responsible for these unethical drug promotion
practices in Pakistan. Now the doctors have become demanding and pharmaceutical
companies are responsible to fulfill their ethical and unethical demands. Now, this
has become an acceptable norm of the pharmaceutical industry and doctor’s
community for the promotion of drugs in unethical ways. The monetary rewards,
local and foreign visits in the name of scientific activities offered by the
pharmaceutical companies for unethical promotion of the drugs are extensively used
as a tool of promotion of their drugs".
The study further concluded, the focus groups discussions and survey findings
suggest that strong legislation must be developed, implemented and enforced by the
government. However, the regulations and legislation actually works when they are
supported by the norms and values of the society (Ahmed & Jalees, 2008).
In this particular case, these unethical practices are considered as the norms of the
pharmaceutical industry and the doctor’s community; therefore, it could only be
addressed by educating both the segments for realizing their social responsibilities
with the focus on the patients’ well being. Furthermore, there must be strong check
and monitoring by the Ministry of Health both on pharmaceutical industry and the
doctors (Ahmed & Jalees, 2008).
According to Nishtar Sania (2007), immoral practice can engage private sectors as
well as authorizing bodies and could involve drug supply chain process, which starts

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-44-
from registration, licensing and official approval of prices, sales and marketing of
medicines with procurements. This sector involved in corruption from its base in the
profitable benefits of the non-genuine drug companies, who uncover observance
with set of laws pricey and attempt to avoid rules and procedures to obtain
registration of their products, accelerate endorsement method, and obtain own
choice rates of their products.
The further conclusion of this research stated that the process of contracting for
purchase of medicines offers a well-paid supply of income for dishonest bureaucrat
and contractor through kickbacks and excess invoicing. During procurement, the
most actively fraudulent practices include conspiracy among bidders, kickbacks
from drug suppliers and bidders to minimize contest, and bribes to government
officials. They also involved in procuring below standard medicines and get money
for the suitable drugs. It is also reported that a number of medicines and other
supplies are stolen from hospital stores and are abstracted for resale. The reason
behind this is to encourage commission and corruption, which engage a lot of
medical practices such as wrong documentation, supply of medicines to ‘ghost
patients’, embed and stuffing of bills, witty book observance, additional payment for
medical supplies, extra billing and over invoicing. There is other form of
mismanagement and fraud crop up due to inadequate check and balance system; e.g.
supplies do not congregate demanding standards, partial delivery, or selling poor
standard, over date, fake and injurious medicines at lower cost. The process of
registering pharmacies can also be besmirched. Above all, the most important

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-45-
problem is violent medicines promotional and marketing strategies, which can show
the way to the unethical promotional activities.
In Pakistan, above 450 drug companies manufacture registered approximately
45,000 drugs. Such huge competition joined with hospitality based strong marketing
can lead to unprincipled marketing practices, which have the prospective influence
on medical practice and handling doctors decisions (Nishtar Sania, 2007).
A report Bowman (1988) put into noticed that drug companies are infringing moral
regulations when they test their drugs in emerging countries. Manufacturer
GlaxoSmithKline has unethically tested a breast cancer drug in India, says the
Wemos Foundation, an Amsterdam-based lobbying organization on international
health issues.
According to Bowman, M. A., & Pearle, D. L. (1988), GSK has tested an untried
medicine for breast cancer on women in India, which is also available in the
Netherlands. According to WEMOS this performance flout ethical standards.
WEMOS is initiating a campaign to encourage principled exploration in developing
countries such as India. Non developing countries are extensively used for
researching and testing products that are eventually inspired in Western countries.
GlaxoSmithKline (GSK) is tinted as the main perpetrator in a report published today
by the Centre for Studies in Ethics and Rights, based in Mumbai, India (Bowman &
Pearle, 1988).
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-46-
CHAPTER THREE
RESEARCH METHODOLOGY
3.1 DATA, SAMPLE AND METHODOLOGY
The total population, and targeted population has been given as under and on the
basis of targeted population researcher has selected sample size which has also been
elaborated as under, moreover, following research methodology will be adopted in
order to conduct this research study.
3.2 TOTAL POPULATION
The total population of undertaken study is the following:
• All Sales & Marketing Personnel of all Pharmaceutical Companies, which
are operating in Pakistan including Multinational & National Companies.
• All the doctor community whether they are General practitioner in rural or
urban area or Medical Officers & Resident Medical Officers of Government
& Private hospitals or the Consultants of all specialties whether they are
working in Government or Private Hospitals.
• All the Retail Pharmacies' of the Country.
• All the whole sales pharmacies of the Country.
• All the Public & Private Hospitals of the Country.
• All the indoor & outdoor patients & their attendants' during the data
collection time period.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-47-
• Government Offices & Officials, which are directly or indirectly involved in
order to implement & ensure the law enforcement which are related to the
subject matter of undertaken study.
3.3 TARGETED POPULATION
The targeted population of undertaken study is the following:
• Sales & Marketing Personnel of top 10 (according to IMS) Pharmaceutical
Companies, which are operating in Pakistan including Multinational &
National Companies. These top 10 players have more than 80% share of total
pharmaceutical volume, which include GSK, Abbott, Sanofi-Avantis,
Novartis, Pfizer, Merck-Serrano, Buyer-Schering, Getz, Hilton, and Bosch
Pharmaceuticals.
• The undertaken study is a case study of Karachi city; therefore, the data has
been collected from peripheral and urban areas of Karachi City. General
practitioner in rural (peripheral) and urban areas, Medical Officers &
Resident Medical Officers of Government & Private hospitals or the
Consultants of all specialties whether they are working in Government or
Private Hospitals have been taken for this study. According to IMS Karachi
city is contributing more than 35% of total pharmaceutical market of
Pakistan.
• Karachi city will be taken for the data collection of the Retail Pharmacies' of
the study. According to IMS, Karachi city is contributing more than 40% of
total pharmacies of the country.
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-48-
• Karachi city will be taken for the data collection of the wholesale
Pharmacies' of the study. According to IMS, Karachi city is contributing
more than 50% of total wholesale pharmacies of the country.
• Karachi city will be taken for the data collection of the public and private
hospitals for this study. According to IMS, Karachi city is contributing more
than 28% of total public and private hospitals of the country.
• Karachi city will be taken for the data collection of the indoor and outdoor
patients & their attendants during the data collection time period, which cater
more than 20% of total market.
• Karachi city will be taken for the data collection of government offices &
Officials, which are directly or indirectly involved in order to implement and
ensure the law enforcement, which are related to the subject matter of the
undertaken study.
3.4 SAMPLE SIZE
Probability sampling technique will be used because the research study based on
quantitative analysis. For the sampling purpose the Cluster sampling technique will
be used, another reason to use this sampling technique is, the overall population is
very much scattered and spread in a larger geographical area of the city, moreover,
the overall population is heterogeneous. Therefore, for sampling purpose different
clusters will be collected from different areas of Karachi city. Researcher has used
following six variables in order to conduct the undertaken study and to draw
statistical analysis & conclusions. The total sample of 300 has been extracted from
following six different variables.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-49-
3.5 PHARMACEUTICAL SALES & MARKETING PERSONNEL
3.5.1 Multinational / National Pharmaceuticals Personnel
Since 10 MNCs will be taken and total 60 samples have been drawn from sales and
marketing teams of these companies, so, in this way the total 60 personnel will be
taken randomly.
3.6 DOCTORS COMMUNITY
3.6.1 General Practitioners (Both Rural & Urban)
Total 30 General Practitioners have been taken from different areas of Karachi city
for sampling purpose randomly.
3.6.2 Medical Officers & Resident Medical Officers of Public & Private
Hospitals
Total 30 samples of MO & RMO have been recruited randomly.
3.6.3 Consultants of All the Specialties of Public & Private Hospitals
Total 30 consultants from Public hospitals & Private hospitals of different
specialties will be recruited randomly.
Therefore, the sample size of doctors' community will be of 90 respondents'.
3.7 HOSPITALS
3.7.1 Public Hospitals Including Provincial & Federal Hospitals

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-50-
The sample of 10 has been taken from Provincial & Federal hospitals from Karachi
City.
3.7.2 Private Hospitals
Total 15 private hospitals have been taken randomly for this study from Karachi
City.
Therefore, the sample size of Hospitals will be of 25 hospital respondents'.
3.8 PHARMACIES
3.8.1 Retail Pharmacies
Total 25 retail pharmacies have been selected from different areas of Karachi City.
3.8.2 Whole Sales Pharmacies
Total 25 wholesale pharmacies have been selected from different areas of Karachi
City.
Therefore, the sample size of total pharmacies will be of 50 respondents'.
3.9 GOVERNMENT OFFICIALS
3.9.1 Federal / Provincial Government Officials
Total 15 government officials have been taken from Karachi City.
Therefore, the sample size of Government officials will be of 15 respondents'.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-51-
3.10 PATIENTS OR THEIR ATTENDANTS'
3.10.1 Outdoor Patients & Their Attendants'
Total 30 Outdoors patients or their attendants' from Public hospitals and private
hospitals have taken randomly from different areas hospitals.
3.10.2 Indoor Patients & Their Attendants'
Total 30 Indoor patients or their attendants' from Public hospitals and private
hospitals have taken randomly from different areas hospitals.
Therefore, the sample size of Patients or their attendants' will be of 60 respondents'.
3.11 PLAN OF DATA ANALYSIS
Both descriptive and inferential statistical techniques will be used through SPSS and
Megastat. The data will be presented in tables and charts. The statistical hypothesis
will be tested with the help of z-test (involving two groups) and F-test (involving
more than two groups) of significance. The graphical analysis will also be presented
wherever it is needed.
CHAPTER FOUR

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-52-
DATA ANALYSIS
4.1 SURVEY FINDINGS
The survey findings were analyzed linearly, cross sectionally in order to have a
better comprehension and understanding between the relationship of dependent and
independent variables, moderating, and intervening variables. The empirical results
or the survey findings and interpretations of the study are discussed as below. The
total sample of 300 has been extracted from following six different variables. The
demographic information of these 300 respondents as follow:
4.1.1 Gender
TABLE 1 FEMALES MALES TOTAL
88 212 300 Major samples collected from Male respondents (Total 212, 70.67%) total samples
size responded to the research while Female doctors (Total 88, 29.33%) of sample
size.
GRAPH – 5 Gender

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-53-
The above graphical representation shows the gender recruitment of respondents in
the under taken study, which clearly demonstrate that the overwhelming majority of
respondents are male.
Following table shows the age brackets of different respondents who have
participated in the study.
4.1.2 Age
TABLE 2 < 30 30-40 40-50 > 50 TOTAL 81 76 78 65 300
It is clearly indicated from the above table the majority of respondents belongs to the
age group of less than 30 years and then followed by between 40-50 years and so on.
Following is the graphical representations of different age groups of were
participated in the study.
GRAPH - 6
Age (In Years)

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-54-
4.1.3 Experience
TABLE 3
< 5 5--10 10—15 > 15 TOTAL 47 57 67 129 300
Major respondents i.e. 129 fall under the category of more than 15 years experiences
& then followed by 67 respondents have 10-15 years of experience in their field. 57
respondents belong to 5-10 years experience and 47 respondents have less than 5
years experience. Moreover, following graph shows the distribution of experiences
according to their ages of all the respondents who have participated in the under
taken study.
GRAPH - 7
Experience (In Years)
4.1.4 Education TABLE 4
Post Graduates Graduates Intermediate Metric 105 140 33 22

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-55-
The above table shows that 140 respondents were graduates and 105 respondents
were post-graduates, whereas, only 33 respondents have received intermediate
education and 22 have obtained Matriculation certification. So, it is concluded that
majority of respondents i.e. 245 were graduate or post-graduate. Following graph
shows the pictorial diagram of this data.
GRAPH - 8
Education of Respondents
4.1.5 Respondents
TABLE 5
Consulta
nt RMO/M
O GPs Govt.
Officials Pharma.
Personnel Govt. Hosp Personnel
30 30 30 15 60 10
If we analyze the whole respondents then we come to know that there were 30
consultants and 30 MO/RMOs, & 30 general practitioners who have participated in
that study. Whereas, 60 pharmaceutical personnel have been recruited for the under
taken study. The pharmaceutical personnel were either from sales or from

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-56-
marketing. Moreover, 15 government officials were also taken as respondents for
this study and 10 hospital employees were participated in the study as well.
TABLE 6
Private Hosp. Personnel
Retail Pharmacies
Wholesale Pharmacies
Outdoor Patients
Indoor Patients
15 25 25 30 30 Moreover, 15 private hospitals personnel were also taken as respondents for this
study and 25 each retail and wholesale pharmacies taken randomly for the
undertaken study. Outdoor and indoor patients were taken 30 each. Following is the
graphical representation of the above data.
GRAPH – 9 RESPONDENTS
4.1.6 Pharmaceutical Personnel
TABLE 7 Gender Age Experience
Male Female < 30 30 – 40 40 - 50 > 50 < 5 5--10 10--15 > 15 37 23 29 20 8 3 16 16 18 10
The pharmaceutical personnel who were taken as sample for the under taken study
the further break up was as:
There were 37 males and 23 females who were participated for the study and age
bracket of less than 30 were 29 participant and 20 between 30-40 years. Only 8

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-57-
respondents were of age between 40-50 years. Whereas, the experience was less
than 5 years between 5-10 years for 16 respondents each, 18 respondents have 10-15
years experience and 10 respondents have more than 5 years experience.
TABLE 8
Education Graduate Post Graduate
25 35
As far as education was concerned all the respondents from pharmaceutical industry
were well educated, in which 25 were graduates and 35 were post-graduates.
Following is the graphical representation of all above data & tables.
GRAPH – 10
Pharmaceutical Personnel
4.1.7 Consultants
TABLE 9
Gender Age (Yrs) Experience (Yrs) Education
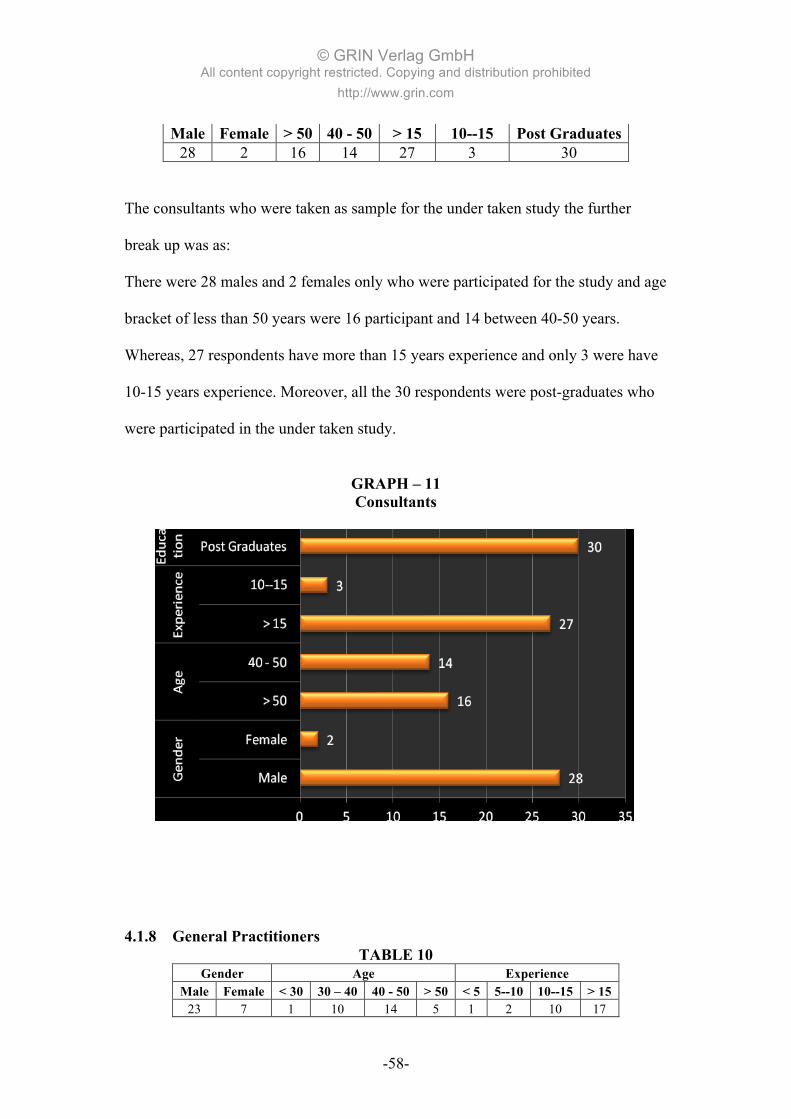
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-58-
Male Female > 50 40 - 50 > 15 10--15 Post Graduates 28 2 16 14 27 3 30
The consultants who were taken as sample for the under taken study the further
break up was as:
There were 28 males and 2 females only who were participated for the study and age
bracket of less than 50 years were 16 participant and 14 between 40-50 years.
Whereas, 27 respondents have more than 15 years experience and only 3 were have
10-15 years experience. Moreover, all the 30 respondents were post-graduates who
were participated in the under taken study.
GRAPH – 11 Consultants
4.1.8 General Practitioners
TABLE 10 Gender Age Experience
Male Female < 30 30 – 40 40 - 50 > 50 < 5 5--10 10--15 > 15 23 7 1 10 14 5 1 2 10 17

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-59-
General Practitioners who were taken as sample for the under taken study the further
break up was as:
There were 23 males and 7 females only who were participated for the study and age
bracket of less than 30 years was only 1 participant and 10 between 30-40 years, and
there are 14 respondents of age bracket 40-50 years. Whereas, 5 respondents have
more than 50 years age group. As far as experience was concerned there were two
participants who have 5-10 years experience, only 1 respondent who has less than 5
years experience. There were 10 respondents who had 10-15 years experience and
17 participants had more than 15 years experience.
TABLE 11
Education Graduation Post Graduation
28 2
There were 28 respondents who had graduation and 2 general practitioners were post
graduated who participated in the under taken study. Following is the graphical
representation of the above data.
GRAPH – 12
General Practitioners

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-60-
4.1.9 RMO / MO
TABLE 12
Gender Age Experience Education Male Female < 30 30 - 40 < 5 5--10 10—15 Graduation
12 18 25 5 15 12 3 30
RMOs / MOs who were taken as sample for the under taken study the further break
up was as follows:
There were 12 males and 18 females who were participated in the study and age
bracket of less than 30 years were 25 participants and 5 between 30-40 years. As far
as experience was concerned there were five participants who have more than 5
years experience, only 3 respondents who have between 10-15 years experience. All
30 participants were graduated who participated in the study.
GRAPH – 13 RMO / MO

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-61-
4.1.10 Govt. & Private Hospitals Officials
TABLE 13
Gender Age Experience Male Female < 30 30 – 40 40 - 50 > 50 < 5 5--10 10--15 > 15
19 6 3 6 11 5 2 1 8 14 Government and private hospitals officials who were taken as sample for the under
taken study the further break up was as follows:
There were 19 males and 6 females who were participated in the study and age
bracket of less than 30 years were only 3 participants and 6 between 30-40 years, 11
participants were between 40-50 years of age and 5 respondents were more than 50
years. As far as experience was concerned there were only two participants who
have less than 5 years experience, only 1 respondent who has between 5-10 years
experience, 8 respondents have between 10-15 years experience and 14 participants
have more than 15 years of experience.
TABLE 14
Education Intermediate Graduation Post graduation
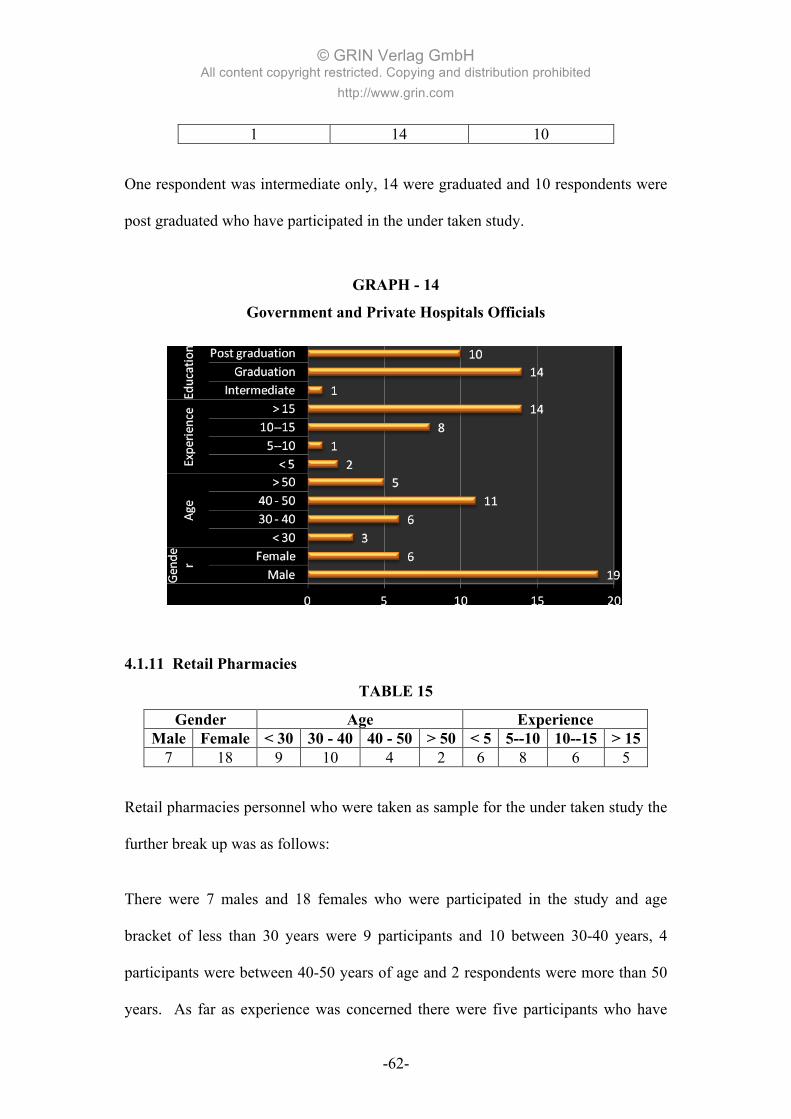
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-62-
1 14 10 One respondent was intermediate only, 14 were graduated and 10 respondents were
post graduated who have participated in the under taken study.
GRAPH - 14
Government and Private Hospitals Officials
4.1.11 Retail Pharmacies
TABLE 15
Gender Age Experience Male Female < 30 30 - 40 40 - 50 > 50 < 5 5--10 10--15 > 15
7 18 9 10 4 2 6 8 6 5
Retail pharmacies personnel who were taken as sample for the under taken study the
further break up was as follows:
There were 7 males and 18 females who were participated in the study and age
bracket of less than 30 years were 9 participants and 10 between 30-40 years, 4
participants were between 40-50 years of age and 2 respondents were more than 50
years. As far as experience was concerned there were five participants who have

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-63-
less than 5 years experience, eight respondents who have between 5-10 years
experience, 6 respondents have between 10-15 years experience and 5 participants
have more than 15 years of experience.
TABLE 16
Education Metric Intermediate Graduation Post Graduation
3 1 15 6 Three participants were matriculated, one respondent was intermediate only, 15
were graduated and 6 respondents were post graduated who have participated in the
under taken study.
GRAPH – 15 Retail Pharmacies
4.1.12 Wholesales Pharmacies

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-64-
TABLE 17
Gender Age Experience Male Female < 30 30 – 40 40 - 50 > 50 < 5 5--10 10--15 > 15
25 0 2 4 11 8 1 2 5 17
Wholesales pharmacies personnel who were taken as sample for the under taken
study the further break up was as follows:
There were 25 males and none of female who were participated in the study and age
bracket of less than 30 years were 2 participants and 4 between 30-40 years, 11
participants were between 40-50 years of age and 8 respondents were more than 50
years. As far as experience was concerned there was only one participant who has
less than 5 years experience, 2 respondents who have between 5-10 years
experience, 5 respondents have between 10-15 years experience and 17 participants
have more than 15 years of experience.
TABLE 18
Education Intermediate Graduation Post Graduation
13 10 2 There were 13 respondents who were intermediate, 10 were graduated and 2
respondents were post graduated who have participated in the under taken study.
GRAPH – 16
Wholesale Pharmacies

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-65-
4.1.13 Outdoor Patients
TABLE 19
Gender Age Experience Male Female < 30 30 – 40 40 - 50 > 50 < 5 5--10 10--15 > 15
23 7 11 8 6 5 6 10 5 9 Outdoor patients or their attendants who were taken as sample for the under taken
study the further break up was as follows:
There were 23 males and 7 females who were participated in the study and age
bracket of less than 30 years were 11 participants and 8 between 30-40 years, 6
participants were between 40-50 years of age and 5 respondents were more than 50
years. As far as experience was concerned there were 10 participants who have
between 5-10 years of experience, 5 respondents have between 10-15 years
experience and 9 participants have more than 15 years of experience.
TABLE 20
EDUCATION Matric Intermediate Graduation Post graduation

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-66-
8 12 4 6 There were eight respondents who were Matriculated, 12 respondents who were
intermediate, 4 were graduated and 6 respondents were post graduated who have
participated in the under taken study.
GRAPH – 17
Outdoor Patients
4.1.14 Indoor Patients
TABLE 21
Gender Age Experience Male Female 30 – 40 40 – 50 > 50 5--10 10--15 > 15
23 7 8 8 14 2 7 21
Indoor patients or their attendants who were taken as sample for the under taken
study the further break up was as follows:
There were 23 males and 7 females who were participated in the study and age
bracket between 30-40 years were 8 participants and 8 between 40-50 years, and 14
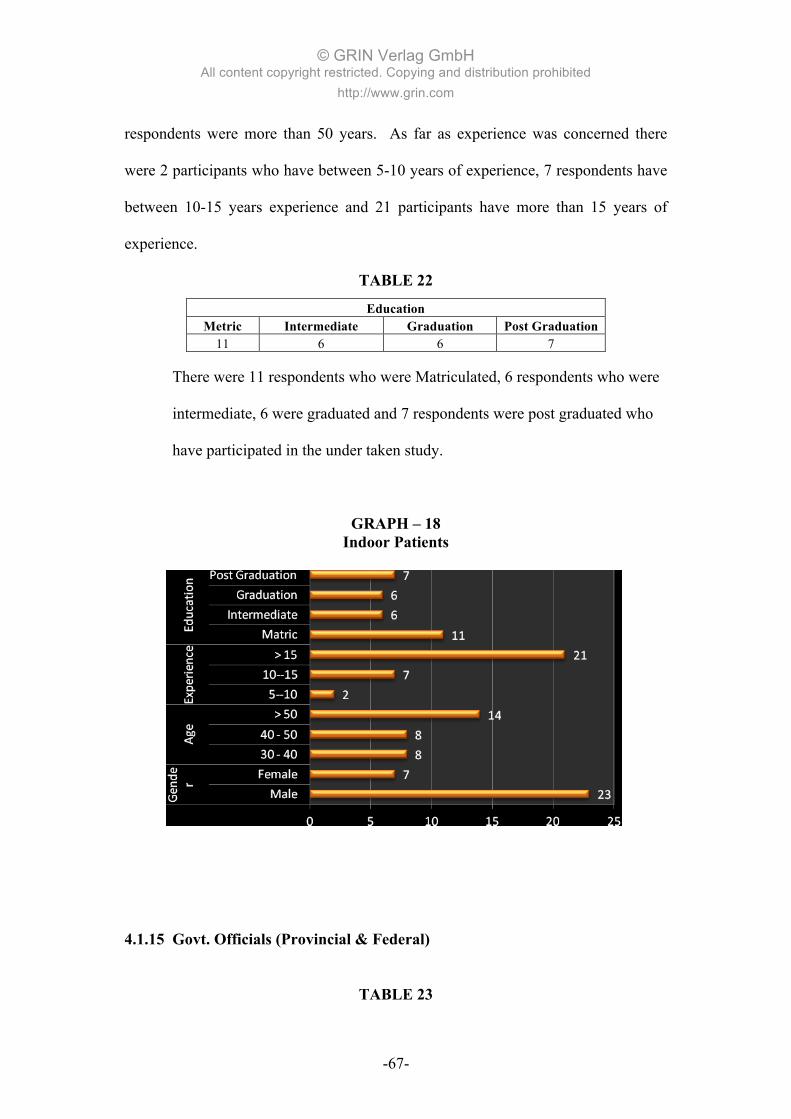
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-67-
respondents were more than 50 years. As far as experience was concerned there
were 2 participants who have between 5-10 years of experience, 7 respondents have
between 10-15 years experience and 21 participants have more than 15 years of
experience.
TABLE 22
Education Metric Intermediate Graduation Post Graduation
11 6 6 7
There were 11 respondents who were Matriculated, 6 respondents who were
intermediate, 6 were graduated and 7 respondents were post graduated who
have participated in the under taken study.
GRAPH – 18 Indoor Patients
4.1.15 Govt. Officials (Provincial & Federal)
TABLE 23

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-68-
Gender Age Experience Male Female < 30 30 - 40 40 - 50 > 50 5--10 10--15 > 15
13 2 1 5 2 7 4 2 9
Provincial and Federal government officials who were taken as sample for the under
taken study the further break up was as follows:
There were 13 males and 2 females who were participated in the study and age
bracket between 30-40 years were 5 participants and 2 between 40-50 years, and 7
respondents were more than 50 years, whereas, less than 30 years were only one
participant. As far as experience was concerned there were 4 participants who have
between 5-10 years of experience, 2 respondents have between 10-15 years
experience and 9 participants have more than 15 years of experience.
TABLE 24
Education Graduation Post Graduation
8 7
There were eight respondents who were graduated and 7 respondents were post
graduated who have participated in the under taken study.
Following is the graphical representation of Provincial and Federal government
officials who were participated in the study:
GRAPH – 19
Government Officials (Provincial & Federal)

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-69-
4.2 HYPOTHESES TESTING
Four different hypotheses were developed and tested using Z-test, simple ANOVA
and F-test. The result and interpretation of the four developed hypotheses are
presented below:
4.2.1 Hypothesis No. I
H1o: The level of unethical drug promotion practices in pharmaceutical
industry is high (at least 4) on the scale of (5 to 1)
H1A: The level of unethical drug promotion practices in pharmaceutical
industry is less than 4 on the scale of (5 to 1)
The statistical representation of the above hypothesis is presented below:

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-70-
H10: µ ≥ 4
H1A: µ ˂ 4
The above hypothesis was tested through Z-test and the summarized result is
presented below:
TABLE 25
Level of Unethical Drug Promotion Practices
Mean 4.220 Standard Deviation 0.887 Hypothesized mean 4.00 Confidence level 0.95 Critical value one tail 1.645 Critical value two tail 1.96 Z-Calculated value 4.29 N 300 confidence interval 95.% lower 4.120 confidence interval 95.% upper 4.320 p-value (two-tailed) 1.76E-05 std. error 0.051 half-width 0.100
The hypothesis relating to high level of unethical drug promotion practices (at least
4 on the scale of 5-1) was substantiated. At 95% confidence level, Z critical value is
-1.645, and Z-calculated value is 4.29 that fall in the non-critical region.
So, it is concluded that the null hypothesis is accepted because 4.29 lies in non
critical region and it is further concluded that the level of unethical pharmaceutical
marketing practices is high (at least 4) on the scale of (5 to 1).
4.2.2 Hypothesis No. 2

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-71-
Focus group discussions indicate that the level of unethical drug promotion practices
is high in rural areas. Therefore the hypothesis developed in this context is
presented below:
H20: The levels of unethical drug promotion practices are equally higher in
rural areas as compared to the urban areas.
H2A: The levels of unethical drug promotion practices are not equally
higher in rural areas as compared to the urban areas.
The statistical representation of the above hypothesis is presented below:
H20: µ1 ≥ µ2
H2A: µ1 ˂ µ2
Above test was carried out through by Z-two samples variables analysis, and the
summarized result is presented below:
TABLE 26
Level of Unethical Drug Promotion Practices In Rural Area
Rural Urban Mean 4.03 3.50 Standard Deviation 1.01 1.21 Observations 300 300 Hypothesized Mean Difference 0 Z 5.81 p-value (one-tailed, lower) 1.0000 z Critical one-tail 1.645 P(Z<=z) two-tail 0 z Critical two-tail 1.95 difference (Rural - Urban) 0.527 standard error of difference 0.091
The hypothesis relating to higher level of unethical drug promotion practices in rural
areas was substantiated. At 95% confidence level the Z-critical value taken from

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-72-
table is -1.645 and Z-calculated value is 5.81 that fall in the non-critical region.
Therefore, it is further concluded that the levels of unethical drug promotion
practices are higher in rural areas as compared to the urban areas.
TABLE 27
Unethical Practices (5 to 1) Common in Karachi Higher in Rural areas Equally higher in Urban areas
4.22 4.03 3.5
Following is the graphical representation of unethical pharmaceutical marketing
practices in overall Karachi and Urban & Rural areas, which clearly demonstrate
that according to the respondents, unethical marketing practices are more common
in rural areas as compared to the urban areas.
GRAPH – 20
UNETHICAL MARKETING PRACTICES IN KARACHI
4.2.3 Hypothesis No. III

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-73-
An important aspect is who was responsible for initiating the unethical drug
promotion practices in Pakistan. Doctor, pharmaceutical companies, hospitals,
pharmacies, Govt. Officials and Patients all have different opinions. In view of this
disparity the developed hypothesis is presented below:
H30: There is no significant difference on the opinions of doctor,
pharmaceutics companies, hospitals, pharmacies, Govt. Officials and
Patients on who initiated unethical drug promotion practices in
Pakistan.
H3A: There is significant difference on the opinions of doctor,
pharmaceutics companies, hospitals, pharmacies, Govt. Officials and
Patients on who initiated unethical drug promotion practices in
Pakistan.
The statistical representation of the above hypothesis is presented below:
H30: µ1 = µ2 = µ3 = µ4 = µ5 = µ6
H3A: µ1 ≠ µ2 ≠ µ3 ≠ µ4 ≠ µ5 ≠ µ6
The above hypothesis was tested through simple ANOVA, and the summarized
results are presented below:
TABLE 28

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-74-
Opinion on Who Initiated the Unethical Drug Promotion Practices
Groups Count Sum Average Variance Pharmaceutical company 300.00 439.00 3.59 2.62 Doctors 300.00 294.00 2.39 3.16 Hospitals 300.00 148.00 1.19 0.49 Pharmacy 300.00 140.00 1.11 0.19 Govt. Officials 300.00 140.00 2.11 1.29 Patients 300.00 140.00 2.29 2.31
Source of Variation SS df MS F P-value F crit
Bt. Groups 521.56 5.00 178.95 106.24 0.00 2.62 Within Groups 747.93 476.00 1.67
Total 1,269.48 479.00
The hypothesis relating to no significant difference of opinions on who initiated
unethical drug promotion practices in Pakistan was rejected. At 95% confidence
level and (5, 476) df the calculated F value of 106.24 is greater than F- critical
values of 2.62.
TABLE 29
Unethical Practices (5 to 1) Groups Average Variance
Pharmaceutical companies 3.59 2.62 Doctors 2.39 3.16 Hospitals 1.19 0.49 Pharmacies 1.11 0.19 Govt. Officials 2.11 1.29 Patients 2.29 2.31
GRAPH – 21 LEVEL OF UNETHICAL PRACTICES

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-75-
The above analysis also indicates that the pharmaceutical industry were found to be
the entity that has initiated unethical drug promotion practices in Karachi with a
mean of 3.59, followed by doctors with a mean of 2.39.
4.2.4 Hypothesis No. IV
In the previous hypothesis, it was found out that the pharmaceutical industry
initiated unethical drug promotion practices, in Pakistan. However, an important
issue is that who is more responsible for the continuation of this practice. Based on
the previous hypothesis the following hypothesis was developed.
H40: The contribution of the pharmaceutical industry in continuation of
unethical drug promotion practices is equal or higher than the doctors.
H4A: The contribution of the pharmaceutical industry in continuation of
unethical drug promotion practices is not equal or higher than the
doctors.
The statistical representation of the above hypothesis is presented below:

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-76-
H40: µ1 ≥ µ2
H4A: µ1 ˂ µ2
Above test was carried out through by Z-two samples variables analysis, and the
summarized result is presented below:
TABLE 30
Opinion on Who Continued the Unethical Drug Promotion Practices
Pharmaceutical Company Doctors Mean 2.94 3.81 Known Variance 3.52 2.61 Observations 300.00 300.00 Hypothesized Mean Difference 0
Z (4.39) P(Z<=z) one-tail 0.00 Z Critical one-tail 1.645 P(Z<=z) two-tail 0.00 Z Critical two-tail 1.96
The hypothesis relating to a higher contribution of pharmaceutical industry in
unethical drug promotion practices was rejected. At 95% confidence level, the Z
critical value is -1.645 and Z-calculated value is -4.39 that falls in the critical
region. So, it is further concluded that the doctor community is more responsible for
the continuation of unethical pharmaceutical practices.
TABLE 31
Pharmaceutical companies Doctors Mean 2.94 3.81 Known Variance 3.52 2.61
GRAPH – 22

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-77-
CONTINUATION OF UNETHICAL PRACTICES
Therefore, it is further concluded that the pharmaceutical companies do not have
more contribution than the doctors in order to continue the unethical pharmaceutical
marketing practices. In other words doctors’ community is more responsible for the
continuation of unethical marketing practices in the industry.
4.3 QUALITITVE ANALYSIS
The qualitative analyses of determinants such as (a) tools of unethical drug
promotion practices (b) drug promotion to the non-qualified doctors (c) Legislation
for unethical drug promotion (d) eradication of unethical drug promotion is given as
below:
4.3.1 Tools of Unethical Drug Practices

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-78-
As was discussed in the literature survey that the commonly used tools for unethical
drug practice was, monetary rewards, local visits, and foreign visits etc. The
summarized results are presented below:
TABLE 32
Monetary Rewards
Local visits
Foreign Visits
Personalized gifts
Chamber decoration
Home decoration
4.24 4.33 4.59 3.88 2.77 1.31
GRAPH 23
It was discussed in earlier section that the doctors are the ones that are responsible
for the continuation of unethical drug promotion practices. The above table and
graphs shows that foreign visits with a mean of 4.59 are more in demand and local
visits being the second. The reasons for high preferences for local visits and foreign
visits are that pharmaceutical industry could justify these expenses by linking it with
the conference.
4.3.2 Drug Promotion to Non-Qualified Doctors

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-79-
Opinions on drug promotion to non-qualified doctors were obtained. Ethically, the
firms should not promote their drugs through them. The respondents’ opinions are
presented below:
TABLE 33
Pharma Personnel Doctors Hospital Pharmacies Govt. Officials Patients
3.29 4.45 3.53 3.11 3.23 3.44
GRAPH 24
Majority of respondents’ of all the segments such as doctors, Pharmaceutical
companies, hospitals, pharmacies, Govt. Officials and Patients were strongly against
drug promotion to the non-qualified doctors. However, despite their opinions it is a
fact that the drugs are being promoted through non-qualified doctors.
4.3.3 Legislation for Unethical Drug Promotion

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-80-
Respondents’ opinions were obtained on the prospects of strong legislation against
unethical drug promotion practices. The respondents’ opinions are presented below:
TABLE 34
Pharma Personnel
Doctors
Hospital Pharmacies
Govt. Officials Patients
3.96 3.91 4.12 4.35 3.34 3.72
GRAPH 25
Inference could be drawn from the above that the majority of respondent are
strongly in the favor of making some strong legislation against the unethical drug
promotional practices in Pakistan. Although some legislation is already available but
this research showed there is no implementation of that legislation, therefore,
majority of respondent demanded that there must be strong legislation to stop this
unethical drug promotion in Pakistan.
4.3.4 Eradication of Unethical Drug Promotion

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-81-
Opinions on eradication of drug promotion in Pakistan were obtained from the
respondents’. The respondents’ opinions are presented below:
TABLE 35
Pharma Personnel
Doctors
Hospital Pharmacies
Govt. Officials Patients
1.98 2.12 1.77 1.91 2.91 2.22
GRAPH 26
Above graph shows that the majority of the respondents’ i.e. doctors, pharmaceutical
personnel, hospitals, pharmacies, Govt. Officials and Patients strongly disagree
about the opinion that the unethical drug promotion practices cannot be stopped now.
Majority of respondents’ agreed upon that these unethical practices can still be
stopped.
CHAPTER FIVE

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-82-
SUMMARY, CONCLUSIONS AND
RECOMMENDATIONS
The major findings and recommendations are discussed below:
5.1 SUMMARY & CONCLUSIONS
The researcher has concluded the overall results and found that both doctors and
pharmaceutical companies are equally responsible for unethical drug promotion
practices in Pakistan. But most important and interesting findings are, basically
pharmaceutical companies are responsible for initiating these unethical drug
practices in Pakistan but now in continuation of these practices the doctor’s
community is actually responsible for these unethical drug promotion practices in
Pakistan. Now the doctors have become demanding and pharmaceutical companies
are responsible to fulfill their ethical and unethical demands. Now, this has become
an acceptable norm of the pharmaceutical industry and doctors community for the
promotion of drugs in unethical ways. The monetary rewards, local and foreign
visits in the name of scientific activities offered by the pharmaceutical companies
for unethical promotion of the drugs are extensively used as a tool of promotion of
their drugs. The entire above conclusion is evident from the four hypotheses that
were tested through Simple ANOVA, F-tests and Z-tests.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-83-
The results of tested hypothesis and their conclusions are presented below:
1. The hypothesis relating to high level of unethical drug promotion practices
(at least 4 on the scale of 5-1) was substantiated. At 95% confidence level, Z
critical value is -1.645, and Z-calculated value is 4.29 that fall in the non-
critical region.
So, it is concluded that the null hypothesis is accepted because 4.29 lies in
non critical region and it is further concluded that the level of unethical
pharmaceutical marketing practices is high (at least 4) on the scale of (5 to 1).
It may be pointed that the level of unethical drug promotion practices as was
ascertained by (Parmar and Jalees, 2004) in their research was 3.56. The
reason could be that the study of (Parmar and Jalees) was case study of
Hyderabad, where as this study is Karachi based, and the sample drawn was
a more representative sample.
The above data clearly shows that the severity and intensity of unethical
pharmaceutical marketing practices have grown intensively in Pakistan. Now, it has
become an acceptable norm for both pharmaceutical industry and doctors’
community. Unfortunately, pharmaceutical companies are very much active in these
unethical practices; some how national and multinational companies are competing
each other in order to do these illegal and unethical pharmaceutical marketing
practices. These companies are just bothering for their profits and expansion of

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-84-
businesses. These companies are least bother about the patients’ well being and their
economic burden and care.
At the cost of the patient these companies are offering every kind of social or
scientific activities, local and international CMEs and Conferences and doctor’s
personal obligations in the form of cash, local or foreign trips, home or clinical
appliances. The doctors’ community is equally responsible for these unethical
pharmaceutical marketing practices across Pakistan by accepting all sorts of
activities whether these are ethical or unethical. So, because of both parties
cooperation the level of unethical practices has escalated beyond imagination and
crossed all limits and subsequently patients are suffering enormously.
2. The hypothesis relating to higher level of unethical drug promotion practices
in rural areas was substantiated. At 95% confidence level the Z-critical value
taken from table is -1.645 and Z-calculated value is 5.81 that fall in the non-
critical region. Therefore, it is further concluded that the levels of unethical
drug promotion practices are higher in rural areas as compared to the urban
areas.
In above hypothesis it is clearly demonstrated the level of unethical pharmaceutical
marketing practices are very high in rural areas as compared to urban areas. It does
not mean the level of unethical practices is very low in urban areas but
comparatively it is more severe in rural areas. The reason is very simple, in rural
areas there is almost zero check and balance by the regulating and law enforcing
agencies. Therefore, the pharmaceutical companies are free to offer anything to the

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-85-
doctors community in rural and suburb areas, even in slum areas of big cities the
level of unethical pharmaceutical marketing practices are very high as compared to
the main city areas. The doctors who are practicing in rural or suburb areas are very
much greedy and taking cash incentives for every prescription of medicine. They
have their attached Pharmacies with their clinics and it is very convenient to
prescribe and consume all unknown, substandard, unregistered and counterfeit drugs.
The reason is simple there is very low check and balance of regulating and law
enforcing agencies of medicines in rural and slum areas. The government drug
inspectors are also very much involved in for corruption for those areas as well.
The sale of free sample is also very common in rural and suburb areas, whereas, the
sales of free samples is illegal but due to these attached pharmacies samples are
being prescribed and sold to the patients. Another horrible fact is that almost 80%
fake doctors who do not have medical degree and medical license; they also do
illegal practice in these areas. So, there is two-dimension problem in rural areas, the
fake medicines and the fake doctors. This could be a strong reason for more
unethical practices in the rural areas as compared to the main cities. Ironically, both
pharmaceutical companies and doctors are playing with the health of poor people in
all those rural, suburbs and slum areas.
An important aspect is who was responsible for initiating the unethical drug
promotion practices in Pakistan. Doctor, pharmaceutical companies, hospitals and
pharmacies all have different opinions. In view of this disparity the developed
hypothesis is presented below:

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-86-
3. The hypothesis relating to no significant difference of opinions on who
initiated unethical drug promotion practices in Pakistan was rejected. At
95% confidence level and (5, 476) df the calculated F value of 106.24 is
greater than F- critical values of 2.62.
The above analysis also indicates that the pharmaceutical industry were
found to be the entity that has initiated unethical drug promotion practices in
Pakistan with a mean of 3.59, followed by doctors with a mean of 2.39.
The result of above hypothesis clearly demonstrated that the pharmaceutical industry
was the responsible for the cultivation of these unethical norms in Pakistan. Actually,
initially multinational companies have started these practices in big cities with
international conferences. Multinational companies have provided the opportunities
to the consultants for abroad trips in the name of international conference and
subsequently national conferences and personalized activities as well. After
emergence of national companies, the unethical practices span has increased many
folds because national companies have targeted family physicians and
comparatively junior doctors at mass level.
Another reason for phenomenal increase of unethical practices was the margin of
profits. Since the national companies have more margins and these companies have
larger field force and coverage of doctors is tremendous across Pakistan. These
national companies have diversified product portfolios and commonly used products;
therefore, their reach is also very vast to the doctors. So, they spread these unethical

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-87-
pharmaceutical marketing practices rapidly to every corner of the Country. They
also introduced new dimensions of unethical practices like cash incentives, family
trips, home appliances and foreign trips with family as well.
In the previous hypothesis, it was found out that the pharmaceutical industry
initiated unethical drug promotion practices, in Pakistan. However, an important
issue is that who is more responsible for the continuation of this practice.
4. The hypothesis relating to a higher contribution of pharmaceutical industry
in unethical drug promotion practices was rejected. At 95% confidence level,
the Z critical value is -1.645 and Z-calculated value is -4.39 that falls in the
critical region.
Therefore, it is further concluded that the pharmaceutical companies do not
have more contribution than the doctors in order to continue the unethical
pharmaceutical marketing practices. In other words doctors’ community is
more responsible for the continuation unethical marketing practices in the
industry.
The result of above hypothesis clearly shows that after initiation of pharmaceutical
marketing practices by the pharmaceutical companies, now it has become an
acceptable norm. Now, the doctors’ community thinks, this is the right of doctor to
ask their share of the profit from the pharmaceutical companies. Therefore, now,
they have become more demanding and bluntly ask for different obligations without
any hesitation. Pharmaceutical companies also fulfill their demands happily without

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-88-
asking any question, even there is a competition amongst the companies to fulfill
their demands. So, now, the doctors are asking for cash incentives for per
prescription and other lucrative incentives from the pharmaceutical companies
themselves.
Doctors clearly ask from the pharmaceutical companies, if they prescribe their
products then what sort of benefits they will be getting. They dictate and blackmail
to the pharmaceutical companies, if companies will not fulfill their demands then
they will stop their prescription and make deals with other companies. They totally
forget the patients’ stakes and their economic burden and their well-being.
The qualitative analyses of determinants such as (a) tools of unethical drug
promotion practices (b) drug promotion to the non-qualified doctors (c) Legislation
for unethical drug promotion (d) eradication of unethical drug promotion is given as
below:
a) As was discussed in the literature survey that the commonly used tools
for unethical drug practice was, monetary rewards, local visits, and
foreign visits etc. The summarized results are presented below:
It was discussed in earlier section that the doctors are the ones that are
responsible for the continuation of unethical drug promotion practices.
The Qualitative analysis shows that foreign visits with a mean of 4.59 are
more in demand and local visits being the second. The reasons for high

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-89-
preferences for local visits and foreign visits are that pharmaceutical
industry could justify these expenses by linking it with the conference.
The above qualitative analysis clearly demonstrated that the foreign visits are the
most common practice, which is being used by the pharmaceutical industry in order
to please and oblige the doctors. Whereas, the local visits are the second one tool to
oblige the doctors. Foreign and local visits are the most demanding and practicing
by the pharmaceutical industry to please or to oblige doctors for unethical marketing
practice. Initially, the multinational companies in the name of international
conferences have started foreign visits and they selected consultants from the main
cities of the Country. They were not only providing boarding, lodging, air tickets
and registration but also arrange sight seeing as well. After entrance of national
companies the quantum of foreign and local visits have increased substantially.
Local companies have also offered these visits to family physicians and junior
doctors as well. Mainly, national and multinational companies are linking these local
and foreign tours with national and international conferences. Local companies have
forwarded one step ahead and they started Continuing Medical Education (CMEs)
and in the name of CMEs these national companies arrange international tours for
doctors and their families. In those international tours these companies are providing
all sort of recreational activities to the doctors and families that is why the
international tours are in more demand by the doctors community.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-90-
b) Opinions on drug promotion to non-qualified doctors were obtained.
Ethically, the firms should not promote their drugs through them. The
respondents’ opinions are presented below:
The Qualitative analysis shows that the majority of respondents’ of all
the segments such as doctors, Pharmaceutical companies, hospitals,
pharmacies, govt. officials or Patients were strongly against drug
promotion to the non-qualified doctors. However, despite their opinions
it is a fact that the drugs are being promoted through non-qualified
doctors.
The above opinion is very logical and interesting which is obtained from doctors,
pharmaceutical companies, hospitals and pharmacies. All the respondents are very
much agreed upon that the promotion of pharmaceutical drugs should be prohibited
to the non-qualified doctors. However, the ground realities are entirely different than
their opinions because most of the pharmaceutical companies are promoting their
drugs to non-qualified doctors in order to boost up their sales, especially in rural,
suburbs, and slum areas because the major chunk of doctors are non-qualified in all
these areas. Patients’ of those areas also visit non-qualified doctors because of
unviability of qualified doctors and for economic reasons as well. All the
pharmacies of those areas freely selling their medicines to the patients on the
prescription of non-qualified doctors. Only qualified doctor’s opinion could be taken
validated because these non-qualified doctors are competitors of degree holder
doctors.
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-91-
c) Respondents’ opinions were obtained on the prospects of strong
legislation against unethical drug promotion practices. The respondents’
opinions are presented below:
Inference could be drawn from the Qualitative analysis that the majority
of respondents are strongly in the favor of making some strong
legislation against the unethical drug promotional practices in Pakistan.
Although some legislation is already available but this research showed
there is no implementation of that legislation, therefore, majority of
respondent demanded that there must be strong legislation to stop this
unethical drug promotion in Pakistan.
The above qualitative analysis clearly shows that all the respondents are agreed upon,
further legislation should be taken place in order to stop these unethical
pharmaceutical marketing practices. However, prevailing laws are more than
sufficient for the eradication of these practices, but the problem is true
implementation of these laws. The laws and code of conduct is already there for
ethical marketing practices for pharmaceutical companies. There are numerous
government bodies and agencies who are supposed to implement these laws on
pharmacies, pharmaceutical companies and doctors community but unfortunately
government officials are indulged themselves in the corruption. So, if there will be
made any new law, then who will implement that law.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-92-
d) Opinions on eradication of drug promotion in Pakistan were obtained
from the respondents’. The respondents’ opinions are presented below:
The Qualitative analysis shows that the majority of the respondents’ i.e.
doctors, pharmaceutical personnel, hospitals, pharmacies, govt. officials
and Patients strongly disagree about the opinion that the unethical drug
promotion practices cannot be stopped now. Majority of respondents’
agreed upon that these unethical practices could still be stopped.
Above qualitative analysis shows that these unethical practices could be stopped, but
there is a big question how? Who will take the responsibility to stop these practices?
The pharmaceutical companies? These are busy in making huge profits from these
practices. The doctors’ community? They are getting unmatched and enormous
benefits from the pharmaceutical companies. Government officials are taking
bribery in order to support all these unethical practices. Actually, everybody is
involved in that unethical practice; therefore, everybody should realize their moral
responsibility and take their own part in order to stop these unethical practices from
the society. Otherwise, hundreds of thousands laws and regulations could not be
stopped these unethical practices.
5.2 RECOMMENDATIONS
The focus groups discussions and survey findings suggest that strong legislation
must be developed, implemented and enforced by the government. However, the

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-93-
regulations and legislation actually works when they are supported by the norms and
values of the society.
In this particular case, these unethical practices are considered as the norms of the
pharmaceutical industry and the doctors community; therefore, it could only be
addressed by educating both the segments for realizing their social responsibilities
with the focus on the patients’ well being.
Furthermore, there must be strong check and monitoring by the Ministry of Health
and other monitoring agencies both on pharmaceutical industry and the doctors.
It is also strongly recommended that there should be strong legislation by the
healthcare authorities and government agencies to stop or at least minimize these
unethical pharmaceutical marketing practices both by the doctor community and the
pharmaceutical industry.
There must be strong enforcement of existing rules and regulations by the relevant
government departments and autonomous bodies whom responsible to implement
and ensure these rules and regulations both on pharmaceutical industry and the
doctors’ community.
It is also recommended to the doctors’ community that this is also their prime and
ethical responsibility to avoid getting unethical benefits from pharmaceutical
companies while they are prescribing their products.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-94-
The pharmaceutical industry should also restrict itself up to ethical marketing offers
and discourage healthcare professionals if they would ask any thing, which is
unethical according to the ethical pharmaceutical practices guidelines.
Most importantly every stakeholder should realize their responsibility and take their
own part in order to stop these unethical pharmaceutical practices from the society.
Pharmaceutical companies should abide the prevailing laws and regulations for
marketing their drugs to the doctors and draw a thick line between ethical and non-
ethical pharmaceutical marketing practices and do not cross that line at any cost.
Doctors’ community should also realize their moral and ethical responsibility and do
not demand for unethical benefits from the pharmaceutical companies and restrict
themselves within the ethical limits. Doctors’ community is known as the most
sophisticated and literate group of people of the society; therefore, they have a more
responsibility to behave seriously in order to stop these unethical practices. They
should discourage pharmaceutical companies if they offer some unethical benefits
because if they accept then they would also be expected to be unethical some point.
They should care their patients and their well-being and do not put economical
burdens on their shoulders at the expense of their own benefits.
Government should increase check and balance on their agencies and employees and
reprimand those officials who are involved in bribery and corruption. If government
will keep on checking and giving punishments then eventually prevailing laws and

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-95-
regulations will be started to work and quantum of these unethical practices will be
diminishing and one day these unethical practices will completely be eradicated
from the society.
5.3 SUGGESTED AREAS OF FURTHER RESEARCH
• Since the under taken study was a case study of Karachi City only, therefore,
it could not be concluded that the result of the study if which would be
conducted on country-wide would be the same as, therefore, further research
can be conducted on Pan-Pakistan basis for more representative sample.
• Another dimension is to segregate the specialties and then could be
conducted the study in order to analyze whether the results of different
specialties are same or different.
• Since in this study only promotional or the marketing aspect of
pharmaceutical industry is been covered, other areas of pharmaceutical
industry like medical, production and procurement could also be covered.
• In this study few variables have been incorporated whereas, in further
research more variables can be incorporated in order to have more clear and
accurate results.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-96-
APPENDIX - I
Annexure – A
Pharmaceutical Drug Promotion in Pakistan: Issues in Ethical and Non-Ethical Practices
QUESTIONNAIRE
Unethical pharmaceutical marketing PRACTICES: It means to promote the product by ignoring the ethical values and principles of PHARMACEUTICAL marketing & SALES:
Q1. Gender � Male � Female Q2. Age? (in years) � Less than 30 � 30-40 � 40-50 � More than 50 Q3. Professional Experience? (in years) � Less than 5 � 5-10 � 10-15 � More than 15 Q4. Respondent? � General
Practitioner � Govt. Official � Consultant � Patient or
Attendant
� Pharmacy � MO or RMO � Hospital � Pharmaceutical Personnel
Q6. Education? � Primary � Secondary � Metric � Intermediate � Graduate � Post Graduate � Ph.D. � Others Q7. Income? (in Thousands) � Less than 5 � 6 to 10 � 11 to 15 � 16 to 20 � 21 to 25 � 26 to 50 � 51 to 100 � More than 100 Q8. Affiliated Institute or Organization?* � Govt. Office (F/P) � Govt. Hospital � Private Hospital � GP
(Urban/Rural) � Pharma. (MNC) � Pharma.
(Local) � Pharmacy (W.
Sale) � Pharmacy
(Retail) � Private Service � Govt.
Employee � Self Employed � Any Other ___

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-97-
Annexure – B
Please Rate the following questions on the scale of 5 to 1 (5 being high and 1 being low) as described follows: Strongly Agree = 5 Agree = 4 Do not Know = 3 Disagree = 2 Strongly Disagree = 1 Q9. Unethical drug promotion practice is common in Pakistan 5 4 3 2 1 Q10. Unethical drug practices are higher in Rural areas: 5 4 3 2 1
Q11. Unethical drug practices are equally higher in Urban areas: 5 4 3 2 1
Q12. The unethical drug practices was initiated by: (a) Pharmaceutical Companies 5 4 3 2 1 (b) Doctors 5 4 3 2 1 (c) Hospitals 5 4 3 2 1 (d) Pharmacies 5 4 3 2 1 Q13. Who are the responsible for the continuation of unethical drug practices? (a) Pharmaceutical Companies 5 4 3 2 1 (b) Doctors 5 4 3 2 1 (c) Hospitals 5 4 3 2 1 (d) Pharmacies 5 4 3 2 1 Q14. Tools which are being used in unethical drug promotion: (a) Monetary Rewards 5 4 3 2 1 (b) Local Visits 5 4 3 2 1 (c) Foreign Visits 5 4 3 2 1 (d) Precious Personalized Gifts 5 4 3 2 1 (e) Chamber’s Decoration 5 4 3 2 1 (f) Home Decoration 5 4 3 2 1 (g) Specify if any Other ___________________________________ 5 4 3 2 1

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-98-
Q15. Do you support to promote the drugs to Non-Qualified Doctors? (a) Pharmaceutical Companies 5 4 3 2 1 (b) Doctors 5 4 3 2 1 (c) Hospitals 5 4 3 2 1 (d) Pharmacies 5 4 3 2 1 (e) Govt. Official 5 4 3 2 1 (f) Patients or Attendants’ 5 4 3 2 1 Q16. Should it be any strong legislation by the government to stop this malpractice? (a) Pharmaceutical Companies Personnel 5 4 3 2 1 (b) Doctors 5 4 3 2 1 (c) Hospital's Influencer 5 4 3 2 1 (d) Pharmacy's Spokesperson 5 4 3 2 1 (e) Govt. Official 5 4 3 2 1 (f) Patients or Attendants’ 5 4 3 2 1 Q17. Is it difficult to stop unethical promotion practices in Pakistan? (a) Pharmaceutical Companies Personnel 5 4 3 2 1 (b) Doctors 5 4 3 2 1 (c) Hospital's Influencer 5 4 3 2 1 (d) Pharmacy's Spokesperson 5 4 3 2 1 (e) Govt. Official 5 4 3 2 1 (f) Patients or Attendants’ 5 4 3 2 1
Abbreviations: F = Federal P = Provincial Pharma = Pharmaceutical Company MNC = Multinational Local = National Pharmaceutical Company W. Sale = Whole Sale Pharmacies GP = General Practitioner MO = Medical Officer RMO = Resident Medical Officer Consultant = Post Graduate in any Specialty
Thank you very much for your valuable time and Cooperation

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-99-
APPENDIX - II
CROSS-TABULATION
i. AGE
TABLE
Age (Years) Respondents’ < 30 81
30-40 76 40-50 78 > 50 65
TOTAL 300
TABLE
Cross-tabulation Respondents’ 81 76 78 65 300 Total
Age Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E 0.83 -0.17 -0.17 -0.17 -0.17 -0.17 0.00
(O - E)² / E 4.17 0.17 0.17 0.17 0.17 0.17 5.00
% of chi sq 13.9% 0.6% 0.6% 0.6% 0.6% 0.6% 16.7%
% of row 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100.0%
% of column 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 16.7%
% of total 16.7% 0.0% 0.0% 0.0% 0.0% 0.0% 16.7%
< 30 Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 0.83 -0.17 -0.17 -0.17 -0.17 0.00
(O - E)² / E 0.17 4.17 0.17 0.17 0.17 0.17 5.00
% of chi sq 0.6% 13.9% 0.6% 0.6% 0.6% 0.6% 16.7%
% of row 0.0% 100.0% 0.0% 0.0% 0.0% 0.0% 100.0%
% of column 0.0% 100.0% 0.0% 0.0% 0.0% 0.0% 16.7%
% of total 0.0% 16.7% 0.0% 0.0% 0.0% 0.0% 16.7%
30-40 Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 -0.17 0.83 -0.17 -0.17 -0.17 0.00
(O - E)² / E 0.17 0.17 4.17 0.17 0.17 0.17 5.00
% of chi sq 0.6% 0.6% 13.9% 0.6% 0.6% 0.6% 16.7%
% of row 0.0% 0.0% 100.0% 0.0% 0.0% 0.0% 100.0%
% of column 0.0% 0.0% 100.0% 0.0% 0.0% 0.0% 16.7%
% of total 0.0% 0.0% 16.7% 0.0% 0.0% 0.0% 16.7%
40-50 Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 -0.17 -0.17 0.83 -0.17 -0.17 0.00
(O - E)² / E 0.17 0.17 0.17 4.17 0.17 0.17 5.00
% of chi sq 0.6% 0.6% 0.6% 13.9% 0.6% 0.6% 16.7%
% of row 0.0% 0.0% 0.0% 100.0% 0.0% 0.0% 100.0%
% of column 0.0% 0.0% 0.0% 100.0% 0.0% 0.0% 16.7%

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-100-
% of total 0.0% 0.0% 0.0% 16.7% 0.0% 0.0% 16.7%
> 50 Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 -0.17 -0.17 -0.17 0.83 -0.17 0.00
(O - E)² / E 0.17 0.17 0.17 0.17 4.17 0.17 5.00
% of chi sq 0.6% 0.6% 0.6% 0.6% 13.9% 0.6% 16.7%
% of row 0.0% 0.0% 0.0% 0.0% 100.0% 0.0% 100.0%
% of column 0.0% 0.0% 0.0% 0.0% 100.0% 0.0% 16.7%
% of total 0.0% 0.0% 0.0% 0.0% 16.7% 0.0% 16.7%
TOTAL Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 -0.17 -0.17 -0.17 -0.17 0.83 0.00
(O - E)² / E 0.17 0.17 0.17 0.17 0.17 4.17 5.00
% of chi sq 0.6% 0.6% 0.6% 0.6% 0.6% 13.9% 16.7%
% of row 0.0% 0.0% 0.0% 0.0% 0.0% 100.0% 100.0%
% of column 0.0% 0.0% 0.0% 0.0% 0.0% 100.0% 16.7%
% of total 0.0% 0.0% 0.0% 0.0% 0.0% 16.7% 16.7%
Total Observed 1 1 1 1 1 1 6
Expected 1.00 1.00 1.00 1.00 1.00 1.00 6.00
O - E 0.00 0.00 0.00 0.00 0.00 0.00 0.00
(O - E)² / E 5.00 5.00 5.00 5.00 5.00 5.00 30.00
% of chi sq 16.7% 16.7% 16.7% 16.7% 16.7% 16.7% 100.0%
% of row 16.7% 16.7% 16.7% 16.7% 16.7% 16.7% 100.0%
% of column 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
% of total 16.7% 16.7% 16.7% 16.7% 16.7% 16.7% 100.0% 30.00 chi-square 25 df .2243 p-value 2.236 Phi coefficient .913 Coefficient of Contingency 1.000 Cramér's V Fisher Exact Probability can only be calculated for a 2 x 2 table.
ii. EXPERIENCE
TABLE
Experience (Years) Respondents’ < 5 47
5—10 57 10—15 67
> 15 129 TOTAL 300
TABLE
Cross-tabulation
Respondents’ 47 57 67 129 300 Total

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-101-
Experience Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E 0.83 -0.17 -0.17 -0.17 -0.17 -0.17 0.00
(O - E)² / E 4.17 0.17 0.17 0.17 0.17 0.17 5.00
% of chi sq 13.9% 0.6% 0.6% 0.6% 0.6% 0.6% 16.7%
% of row 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100.0%
% of column 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 16.7%
% of total 16.7% 0.0% 0.0% 0.0% 0.0% 0.0% 16.7%
< 5 Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 0.83 -0.17 -0.17 -0.17 -0.17 0.00
(O - E)² / E 0.17 4.17 0.17 0.17 0.17 0.17 5.00
% of chi sq 0.6% 13.9% 0.6% 0.6% 0.6% 0.6% 16.7%
% of row 0.0% 100.0% 0.0% 0.0% 0.0% 0.0% 100.0%
% of column 0.0% 100.0% 0.0% 0.0% 0.0% 0.0% 16.7%
% of total 0.0% 16.7% 0.0% 0.0% 0.0% 0.0% 16.7%
5—10 Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 -0.17 0.83 -0.17 -0.17 -0.17 0.00
(O - E)² / E 0.17 0.17 4.17 0.17 0.17 0.17 5.00
% of chi sq 0.6% 0.6% 13.9% 0.6% 0.6% 0.6% 16.7%
% of row 0.0% 0.0% 100.0% 0.0% 0.0% 0.0% 100.0%
% of column 0.0% 0.0% 100.0% 0.0% 0.0% 0.0% 16.7%
% of total 0.0% 0.0% 16.7% 0.0% 0.0% 0.0% 16.7%
10—15 Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 -0.17 -0.17 0.83 -0.17 -0.17 0.00
(O - E)² / E 0.17 0.17 0.17 4.17 0.17 0.17 5.00
% of chi sq 0.6% 0.6% 0.6% 13.9% 0.6% 0.6% 16.7%
% of row 0.0% 0.0% 0.0% 100.0% 0.0% 0.0% 100.0%
% of column 0.0% 0.0% 0.0% 100.0% 0.0% 0.0% 16.7%
% of total 0.0% 0.0% 0.0% 16.7% 0.0% 0.0% 16.7%
> 15 Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 -0.17 -0.17 -0.17 0.83 -0.17 0.00
(O - E)² / E 0.17 0.17 0.17 0.17 4.17 0.17 5.00
% of chi sq 0.6% 0.6% 0.6% 0.6% 13.9% 0.6% 16.7%
% of row 0.0% 0.0% 0.0% 0.0% 100.0% 0.0% 100.0%
% of column 0.0% 0.0% 0.0% 0.0% 100.0% 0.0% 16.7%
% of total 0.0% 0.0% 0.0% 0.0% 16.7% 0.0% 16.7%
TOTAL Observed 1 1
Expected 0.17 0.17 0.17 0.17 0.17 0.17 1.00
O - E -0.17 -0.17 -0.17 -0.17 -0.17 0.83 0.00
(O - E)² / E 0.17 0.17 0.17 0.17 0.17 4.17 5.00
% of chi sq 0.6% 0.6% 0.6% 0.6% 0.6% 13.9% 16.7%
% of row 0.0% 0.0% 0.0% 0.0% 0.0% 100.0% 100.0%
% of column 0.0% 0.0% 0.0% 0.0% 0.0% 100.0% 16.7%
% of total 0.0% 0.0% 0.0% 0.0% 0.0% 16.7% 16.7%
Total Observed 1 1 1 1 1 1 6
Expected 1.00 1.00 1.00 1.00 1.00 1.00 6.00
O - E 0.00 0.00 0.00 0.00 0.00 0.00 0.00
(O - E)² / E 5.00 5.00 5.00 5.00 5.00 5.00 30.00

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-102-
% of chi sq 16.7% 16.7% 16.7% 16.7% 16.7% 16.7% 100.0%
% of row 16.7% 16.7% 16.7% 16.7% 16.7% 16.7% 100.0%
% of column 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
% of total 16.7% 16.7% 16.7% 16.7% 16.7% 16.7% 100.0%
30.00 chi-square
25 df
.2243 p-value
2.236 Phi coefficient
.913 Coefficient of Contingency
1.000 Cramér's V
Fisher Exact Probability can only be calculated for a 2 x 2 table
iii. INCOME
TABLE
Income (in thousands)
Income (Thousands) Respondents’
< 5 8 6—10 12
11—15 21 16—20 44 21—25 59 26—50 49
51—100 51 > 100 56
TOTAL 300
TABLE Cross-tabulation
Respondents’ 8 12 21 44 59 49 51 56 300 Total Income (Thousands) Observed 1 1
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E 0.90 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 0.00
(O - E)² / E 8.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 9.00
% of chi sq 9.0% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 10.0%
% of row 100% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100%
% of column 100% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0%

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-103-
% of total 10.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% < 5 Observed 1 1
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E -0.10 0.90 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 0.00
(O - E)² / E 0.10 8.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 9.00
% of chi sq 0.1% 9.0% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 10.0%
% of row 0.0% 100% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100%
% of column 0.0% 100% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0%
% of total 0.0% 10.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% 6—10 Observed 1 1
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E -0.10 -0.10 0.90 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 0.00
(O - E)² / E 0.10 0.10 8.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 9.00
% of chi sq 0.1% 0.1% 9.0% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 10.0%
% of row 0.0% 0.0% 100% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100%
% of column 0.0% 0.0% 100% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0%
% of total 0.0% 0.0% 10.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% 11—15 Observed 1 1
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E -0.10 -0.10 -0.10 0.90 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 0.00
(O - E)² / E 0.10 0.10 0.10 8.10 0.10 0.10 0.10 0.10 0.10 0.10 9.00
% of chi sq 0.1% 0.1% 0.1% 9.0% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 10.0%
% of row 0.0% 0.0% 0.0% 100% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100%
% of column 0.0% 0.0% 0.0% 100% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0%
% of total 0.0% 0.0% 0.0% 10.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% 16—20 Observed 1 1
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E -0.10 -0.10 -0.10 -0.10 0.90 -0.10 -0.10 -0.10 -0.10 -0.10 0.00
(O - E)² / E 0.10 0.10 0.10 0.10 8.10 0.10 0.10 0.10 0.10 0.10 9.00
% of chi sq 0.1% 0.1% 0.1% 0.1% 9.0% 0.1% 0.1% 0.1% 0.1% 0.1% 10.0%
% of row 0.0% 0.0% 0.0% 0.0% 100% 0.0% 0.0% 0.0% 0.0% 0.0% 100%
% of column 0.0% 0.0% 0.0% 0.0% 100% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0%
% of total 0.0% 0.0% 0.0% 0.0% 10.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% 21—25 Observed 1 1
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E -0.10 -0.10 -0.10 -0.10 -0.10 0.90 -0.10 -0.10 -0.10 -0.10 0.00
(O - E)² / E 0.10 0.10 0.10 0.10 0.10 8.10 0.10 0.10 0.10 0.10 9.00
% of chi sq 0.1% 0.1% 0.1% 0.1% 0.1% 9.0% 0.1% 0.1% 0.1% 0.1% 10.0%
% of row 0.0% 0.0% 0.0% 0.0% 0.0% 100% 0.0% 0.0% 0.0% 0.0% 100%
% of column 0.0% 0.0% 0.0% 0.0% 0.0% 100% 0.0% 0.0% 0.0% 0.0% 10.0%
% of total 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% 0.0% 0.0% 0.0% 0.0% 10.0% 26—50 Observed 1 1
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 0.90 -0.10 -0.10 -0.10 0.00
(O - E)² / E 0.10 0.10 0.10 0.10 0.10 0.10 8.10 0.10 0.10 0.10 9.00
% of chi sq 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 9.0% 0.1% 0.1% 0.1% 10.0%
% of row 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100% 0.0% 0.0% 0.0% 100%
% of column 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100% 0.0% 0.0% 0.0% 10.0%
% of total 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% 0.0% 0.0% 0.0% 10.0% 51—100 Observed 1 1

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-104-
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 0.90 -0.10 -0.10 0.00
(O - E)² / E 0.10 0.10 0.10 0.10 0.10 0.10 0.10 8.10 0.10 0.10 9.00
% of chi sq 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 9.0% 0.1% 0.1% 10.0%
% of row 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100% 0.0% 0.0% 100%
% of column 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100.0% 0.0% 0.0% 10.0%
% of total 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% 0.0% 0.0% 10.0% > 100 Observed 1 1
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 0.90 -0.10 0.00
(O - E)² / E 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 8.10 0.10 9.00
% of chi sq 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 9.0% 0.1% 10.0%
% of row 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100% 0.0% 100%
% of column 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100% 0.0% 10.0%
% of total 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% 0.0% 10.0% TOTAL Observed 1 1
Expected 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 1.00
O - E -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 -0.10 0.90 0.00
(O - E)² / E 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 0.10 8.10 9.00
% of chi sq 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 0.1% 9.0% 10.0%
% of row 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100% 100%
% of column 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100% 10.0%
% of total 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 10.0% 10.0% Total Observed 1 1 1 1 1 1 1 1 1 1 10
Expected 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 10.00
O - E 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
(O - E)² / E 9.00 9.00 9.00 9.00 9.00 9.00 9.00 9.00 9.00 9.00 90.00
% of chi sq 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 100.0%
% of row 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 100.0%
% of column 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
% of total 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 10.0% 100.0%
90.00 chi-square 81 Df .2313 p-value 3.000 Phi coefficient .949 Coefficient of Contingency 1.000 Cramér's V Fisher Exact Probability can only be calculated for a 2 x 2 table

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-105-
APPENDIX – III
CODE OF ETHICS FOR PHARMACEUTICAL MARKETING
Governing pharmaceutical marketing and relations with pharmaceutical
professionals and healthcare professionals as well as relations between the
pharmaceutical industry and patient organisations applicable to companies engaged
in pharmaceutical marketing in Lithuania
Approved by IFPA and VGA (2012 revision)
Approved at the general meeting of VGA members on 31 May 2012
Approved at the general meeting of IFPA members on 7 June 2012
INTRODUCTION
The Code for Pharmaceutical Marketing has been adopted at the will and upon
common agreement of IFPA and VGA – associations of companies engaged in
pharmaceutical marketing in Lithuania. It seeks to ensure that member
pharmaceutical companies engage in an ethical promotion, restraining from deceitful
practices and potential conflicts of interest with healthcare professionals, whilst
complying with applicable laws and regulations. Thus the Code seeks to enable an
environment where the general public may be sure that the choices regarding their
medicinal products are made based on the merit of each product and the patients’
clinical needs. This Code does not aim at restraining the promotion of medicinal

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-106-
products in such a way as to hinder free competition or limit interaction with
healthcare professionals.
Lithuanian Association of Innovative Pharmaceutical Industry (hereinafter referred
to as IFPA) is the association of companies engaged in the development and/or
marketing of medicines in Lithuania. IFPA is member of the institution representing
the pharmaceutical industry in Europe, the European Federation of Pharmaceutical
Industries and Associations (EFPIA).
The Pharmaceutical Manufacturers’ Association (hereinafter referred to as VGA) is
the association of companies which develop, produce and/or are engaged in the
marketing of medicines and their representatives in Lithuania.
Both associations (IFPA and VGA) contribute to EFPIA mission – to promote
pharmaceutical research and development and the best conditions in Europe for
companies to bring to patients new medicines that improve human health and the
quality of life around the world.
Members of IFPA and VGA are aware of the importance of providing accurate, fair
and objective information about medicinal products enabling people to make
informed decisions about the use of specific medicinal products. Building upon this
goal, IFPA and VGA approved the Code of Ethics for Pharmaceutical Marketing,
which governs pharmaceutical marketing and relations with pharmaceutical
professionals and healthcare professionals as well as relations between the

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-107-
pharmaceutical industry and patient organisations (hereinafter referred to as Code).
The Code has been developed according to the Code of Ethics adopted in Lithuania
in 2004 in compliance with the provisions of the EFPIA code and general ethical
principles as amended on 24 June 2010 and on 14 June 2011. It also reflects the
requirements of the EU Council Directive 2001/83/EC, as amended, (hereinafter
referred to as Directive) concerning the use of medicinal products for human use.
The Code is consistent with the general provisions of the Directive, which
acknowledge voluntary control over promotion of medicinal products implemented
through organisations/institutions, which represent the pharmaceutical industry
sector by providing the opportunity to apply to such organisations when complaints
occur. In addition, the Code incorporates the principles set out in the Law on
Pharmaceutics of the Republic of Lithuania (Official Gazette, 2006 No. 78-3056),
the Law on Advertising of the Republic of Lithuania (Official Gazette, 2000, No.
64-1937, 2002, No. 123-5508) and the Law on Provision of Information to the
Public of the Republic of Lithuania (Official Gazette 1996, No. 71-1706, 2000, No.
75-2272, 2006, No. 82-3254).
SCOPE OF THE CODE OF ETHICS FOR PHARMACEUTICAL
MARKETING
This code for pharmaceutical marketing (hereinafter referred to as Code) covers the
marketing of medicines (both prescription-only and over-the-counter) and
relationships between healthcare professionals and pharmaceutical companies as
well as relationships between the pharmaceutical industry and patient organisations.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-108-
The Code applies to companies engaged in pharmaceutical marketing in Lithuania
and to their representatives (hereinafter referred to as companies).
Companies shall be liable for their obligations under the Code even when they
contract other parties (e.g. companies providing sales services, consultants, market
research companies, advertising agencies) to design, implement and conduct the
activities covered by the Code on their behalf. Furthermore, companies must take
reasonable steps to ensure that any other parties that they commission to design or
implement the activities covered by the Code but which do not act on behalf of the
company (e.g. joint ventures, licensees) comply with the Code.
The Code covers all methods of promotion, including but not limited to oral and
written promotion activities, co-operation, advertising in specialised journals for
healthcare professionals and direct mail advertising, the activities of medical sales
representatives (defined in section 17.1), advertising over the Internet and other
electronic media using audio and video systems, e.g. films, video recordings, data
storage services and the like, as well as the supply of free drug samples, distribution
of gifts and hospitality events.
The Code also applies to relations between companies and healthcare professionals
to govern, including but not limited to, relations emerging from research and
contracts (including clinical trial studies, non-interventional studies and advice, as
well as consultations). Furthermore, this Code governs relations between companies
and patient organisations, which are subject to the requirements set out in Annex C

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-109-
hereto – “The Code of Ethics on the Relations between the Pharmaceutical Industry
and Patient Organisations “
The Code does not aim to restrain or govern provision of non-promotional medicinal,
scientific or factual information.
The Code does not apply to:
- the labelling on medicinal products and accompanying package leaflets
which are subject to Title V of the Directive;
- Correspondence, possibly accompanied by non-promotional material,
required to answer to a specific question on a specific medicinal product;
- factual, informative announcement and reference material relating, for
example, to pack changes, adverse reaction warnings, trade catalogues and
price lists, provided they include no product characteristics;
- non-promotional information regarding human health and diseases;
- non-promotional, general information about companies (such as information
directed to investors or to current/prospective employees), including
financial data, descriptions of research and development programs, and
discussion of regulatory developments affecting the company and its
products.
Attached to the Code are: Annex A − “Implementation and Procedure Rules”, which
is binding upon and obligates members of the association and other committed
companies as well as those with specific guidelines in place to implement the Code

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-110-
to examine complaints and administrate sanctions which may be applied to
pharmaceutical companies; Annex B − “Guidelines for Internet Websites Available
to Healthcare Professionals, Patients and the Public in the EU”, which provide
guidance for pharmaceutical companies with respect to the content of their websites
containing information on medicinal products, and Annex C − “Code of Ethics on
the Relations between the Pharmaceutical Industry and Patient Organisations”.
APPLICABILITY OF THE CODE
The Code sets out the key ethical standards, which are considered binding upon the
companies. IFPA and VGA must comply and ensure their members’ compliance
with the Code and legislative provisions. IFPA and VGA must have specific
procedures in place to ensure compliance with all the codes referred to above by
both their member companies and other companies.
Provisions of the Code must be followed both in spirit and by letter. For example,
companies should follow consistent standards while interacting with healthcare
professionals, in particular as far as gifts and hospitality are concerned. IFPA and
VGA also encourage, on a needs basis, to adhere to the Code of Pharmaceutical
Marketing Practices of the International Federation of Pharmaceutical
Manufacturers and Associations (IFPMA).
The Code for Pharmaceutical Marketing, its content, structure and order may be
revised only upon common agreement between RFA and VGA associations. The

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-111-
Ethics Committee may recommend revisions of the Code, its content, structure and
order based on its experience. The Code shall be reviewed and revised at the
initiative of the Ethics Committee, IFPA and VGA, also following revisions of the
effective Lithuanian laws and regulations (where in conflict with provisions of the
Code) or in the EFPIA Code.
To avoid ambiguities, the term “company” for the purposes of this Code means any
legal entity that organises or sponsors promotion or, within the limits of the Code,
maintains relationships with healthcare professionals or patient organisations in
Lithuania whether such entity be a parent company (e.g. the headquarters, principal
office or controlling company of commercial enterprise), subsidiary company or any
other form of enterprise or organisation.
To ensure proper compliance with the provisions of the Code, IFPA and VGA must
inter alia introduce appropriate procedures for the lodging and examination of
complaints as well as a procedure for imposing sanctions for violations of the Code.
Furthermore, the relevant local subsidiary of the company must be notified in
advance of all international events organised abroad (as provided in Section 9.2 of
the Code) or must be consulted locally.
TERMS EMPLOYED
Participation in an international conference is understood as arrival of the
healthcare professional to the venue of the conference not earlier than one day
before the conference starts and departure not later than one day after the event,

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-112-
registration and payment of the fee, participation in scientific meetings and
acquisition of a participant’s certificate.
Extravagant venues means venues, which are lavish and deluxe, and the visiting of
which could be prejudicial to the image of healthcare professionals/patient
organisations or of the pharmaceutical industry.
Medical Sales Representative means a person appointed by a pharmaceutical or any
other company engaged in the marketing of medicinal products in Lithuania for the
promotion of medicinal products, provision of relevant, precise and evidence-based
information about medicinal products and medical aids and about innovations of the
medical and the pharmaceutical industries, including personnel retained by way of
contract with third parties, any other company representatives who call on healthcare
professionals, pharmacies, hospitals or other healthcare facilities aiming to provide
relevant, precise and evidence-based information about medicinal products and
medical aids and about innovations of the medical and the pharmaceutical industries
and to promote medicinal products. The qualification and competence of the
Medical Sales Representative to carry out the above-listed functions falls within the
responsibility of the company they represent.
Company means pharmaceutical or any other company engaged in pharmaceutical
marketing in Lithuania.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-113-
Entertainment venues means places for leisure and entertainment which advertise
their entertainment facilities on promotional leaflets, also publicly in the press or on
the Internet and which are intended primarily for recreation and/or entertainment, i.e.
entertaining activities rather than professional/business meetings.
Promotion for the purposes of this Code is consistent with the definition provided in
the Law on Pharmaceutics.
Healthcare professionals for the purposes of this Code means general practitioners,
including other members of the medical, dental, pharmacy or nursing profession or
any other persons who in the course of their professional activities may prescribe,
purchase, supply or administer any medicinal products.
Medicinal product for the purposes of the Code shall bear the meaning defined in
Article 1 of the Directive: (a) any substance or combination of substances presented
for treating or preventing disease in human beings; or (b) any substance or
combination of substances which may be administered to human beings with a view
to making a medical diagnosis or to restoring, correcting or modifying physiological
functions in human beings.
Provisions of the Code of Ethics for Pharmaceutical Marketing
Article 1. Marketing Authorisation

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-114-
1.1. A medicinal product must not be promoted prior to the grant of the marketing
authorisation, which permits its sale, or placing on the market, also when promotion
of medicinal products does not meet the approved indications for medicinal products.
1.2. Promotion of a medicine must be consistent with the particulars listed in its
summary of product characteristics.
Article 2. Information that should be Made Available
2.1. Subject to relevant Lithuanian laws and regulations, all promotional materials
must include the following basic information clearly and legibly:
a) essential information consistent with the summary of product characteristics,
indicating the date on which such essential information was generated (if the text
was not revised) or last revised;
b) the classification of the medicinal product placed on the market (prescription-only
or over-the-counter medicinal product);
c) when appropriate, the selling price or indicative price of the various presentations
and the conditions for reimbursement by social security bodies.
2.2. Requirements for the information provided in the advertisement of medicinal
products are set out in Lithuanian laws and regulations governing promotion of
medicinal products.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-115-
2.3. Subject to relevant Lithuanian laws and regulations, where an advertisement is
intended only as a reminder, the requirements of Section 2.1 above need not be
complied with, provided that the advertisement includes no more than the name of
the medicinal product or its international non-proprietary name, if any, or the
trademark.
Article 3. Promotion and Its Substantiation
3.1. Promotion must be accurate, balanced, fair, objective and sufficiently complete
to enable the recipient to form his or her own opinion of the therapeutic value of the
medicinal product concerned. It should be based on an up-to-date evaluation of all
relevant evidence and reflect that evidence clearly. It must not mislead by distortion,
exaggeration, undue emphasis, omission or in any other way.
3.2. Promotion must be capable of substantiation, which must be promptly provided
in response to reasonable requests from pharmaceutical professionals or healthcare
professionals. In particular, promotional claims about side effects must reflect
available evidence or must be capable of substantiation by clinical experience.
Substantiation need not be provided, however, in relation to the validity of elements
approved in the marketing authorisation.
3.3. Promotion must encourage the rational use of medicinal products by presenting
them objectively and without exaggerating their properties. Claims must not imply

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-116-
that a medicinal product, or an active ingredient, has some special merit, quality or
property unless this can be substantiated.
3.4. When promotion refers to publish studies, clear references should be given.
3.5. Any comparison made between different medicinal products must stem from
relevant and comparable aspects of the products based on published scientific
evidence. Comparative advertising must not be misleading or disparaging.
3.6. All artwork, including graphs, illustrations, photographs and tables taken from
published studies included in promotional material should:
a) clearly indicate the source(s) of the artwork;
b) be faithfully reproduced; except where adaptation or modification is required in
order to comply with any Applicable Code(s), in which case it must be clearly stated
that the artwork has been adapted and/or modified.
Particular care must be taken to ensure that artwork included in promotion does not
mislead about the nature of a medicine (for example whether it is appropriate for use
in children) or mislead about a claim or comparison (for example by using
incomplete or statistically irrelevant information or unusual scales).
3.7. The words “safe” must never be used to describe a medicinal product without
proper substantiation.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-117-
3.8. The word “new” must not be used to describe any product or presentation which
has been generally available or any therapeutic indication which has been generally
promoted, for more than one year.
3.9. It must not be stated that a product has no side effects, toxic hazards or risks of
addiction or dependency.
Article 4. Use of Quotations in Promotion
4. 1. Quotations from medical and scientific literature or from personal
communications must be faithfully reproduced (except where adaptation or
modification is required in order to comply with any Applicable Code(s), in which
case it must be clearly stated that the quotation has been adapted and/or modified)
and the precise sources identified.
Article 5. Acceptability of Promotion
5.1. Companies must comply with high ethical standards at all times. Promotion
must: a) never be such as to bring discredit upon, or reduce confidence in, the
pharmaceutical industry; b) always be of a nature which recognizes the special
nature of medicines and the professional standing of the recipient(s); c) never cause
offence to the competitors.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-118-
Article 6. Distribution of Promotion
6.1. Promotion should only be directed at those persons whose need for, or interest
in, the particular information can reasonably be assumed.
6.2. Promotional mailing lists must be kept up-to-date. Requests by healthcare
professionals to be removed from promotional mailing lists must be complied with.
6.3. Subject to the relevant Lithuanian laws and regulations, the use of fax, e-mail,
automated calling systems, text messages and other electronic data communication
for promotion of prescription-only medicinal products is allowed only upon
obtaining prior consent of the healthcare professional.
Article 7. Transparency of Promotion
7.1. Promotion must not be disguised.
7.2. Clinical assessments, post-marketing surveillance and experience programmes,
post-authorisation studies (including those that are retrospective in nature) must not
be disguised promotion. They must be conducted with a primarily scientific or
educational purpose.
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-119-
7.3. When a pharmaceutical company pays for, or otherwise secures or arranges the
publication of promotional material in journals, such material must not resemble
independent editorial matter.
7.4. Materials supported by the company referring to its medicinal products and their
use, no matter if they are or not of promotional nature must clearly indicate that the
company sponsored the materials.
Article 8. Limitations Regarding the Advice on Personal Medical Matters
8.1. In the case of requests from individual members of the general public for advice
on personal medical matters, the enquirer should be advised to consult a healthcare
professional.
Article 9. Events and Hospitality
9.1. All promotional, scientific or professional meetings, congresses, conferences,
symposia, and other similar events (including but not limited to advisory board
meetings, visits to production sites or research laboratories, planning meetings,
education (courses) or investigator meetings for clinical or non-interventional
studies), hereinafter referred to as events, organised on behalf of or sponsored by the
company must be held in an appropriate venue that is conducive to the main purpose
of the event and may only offer hospitality when such hospitality is appropriate and
otherwise complies with the provisions of any Applicable Codes. The term

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-120-
“appropriate” is understood as compliant with the provisions of Sections 9.5 and 9.6
of this Code and not in conflict with the relevant Lithuanian laws and regulations.
9.2. No company may organise or sponsor an event that takes place in another
country, unless provided in Section 13.2 of this Code.
9.3. Promotional material which is displayed or provided as hand-out materials at
international events may, unless prohibited or otherwise regulated by local laws and
regulations, refer to medicinal products (or their use) which are not registered in the
country where the event takes place, or which are registered under different
conditions, so long as: (i) any promotional material (excluding promotional aids) is
accompanied by a suitable statement indicating countries where the product is
registered and making clear that the product is not registered or used locally, and (ii)
any such promotional material which refers to the prescribing information
(indications, warnings, etc.) authorised in a country or countries where the medicinal
product is registered must be accompanied by an explanatory statement indicating
that registration conditions differ internationally.
9.4. The provision of hospitality is limited to the healthcare professionals attending
the event who are true (registered) participants of the event (where registration is
required). It may not extend to the persons accompanying the healthcare
professionals attending the event.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-121-
9.5. All forms of hospitality offered to healthcare professionals shall be reasonable
in level and strictly limited to the main purpose of the event. Hospitality costs
should not exceed those allocated to the scientific part of the event. At promotional
events of medicinal products hospitality must be strictly limited to the main purpose
of the event and must not extend beyond participating healthcare professionals
and/or pharmaceutical professionals. Payment of travel, accommodation and other
costs for those professionals is prohibited. The term of promotional events is
understood as defined in the relevant Lithuanian laws and regulations. At
professional/scientific events hospitality must be secondary to the main purpose of
the event. The cost reimbursement of healthcare professionals attending such events
shall be limited to travel, accommodation, catering and/or registration fee.
9.6. Hospitality must not extend to sponsorship or organising of any entertainment
(e.g. sporting or leisure) events. Companies should avoid venues known as
“entertainment venues” or which are “extravagant”. “Entertainment venues” are
understood as places for leisure and entertainment which advertise their
entertainment facilities on promotional leaflets, also publicly in the press or on the
Internet and which are intended primarily for recreation and/or entertainment, i.e.
entertaining activities rather than professional/business meetings. “Extravagant
venues” are understood as places, which are lavish and deluxe, and the visiting of
which could be prejudicial to the image of pharmaceutical professionals, healthcare
professionals, patient organisations or of the pharmaceutical industry.
© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-122-
9.7. Companies should follow the guideline relating to the term “appropriate” in the
meaning used in Article 9 hereof or subject to the provisions of any of the
Applicable Codes.
Article 10. Gifts
10.1. Companies are prohibited to supply, offer or promise to healthcare
professionals gifts, any kind of pecuniary advantage or benefit in kind as an
inducement to prescribe, recommend, supply, sell or buy a medicinal product.
10.2. Subject to Section 10.1 above, when medicinal products are being promoted to
healthcare professionals, objects intended for reminder advertising may be supplied,
offered or promised to such persons only if they are inexpensive and relevant to the
practice of medicine or pharmacy. The term “inexpensive” means that the item cost
the company not more than 35 litas, including VAT, the attached logo and other
extra costs. Section 10.2. does not govern giving of medical literature to healthcare
professionals.
10.3. Except where they carry all the information stipulated in Section 2.1 above,
objects intended for reminder advertising may bear no more than the name and logo
of the company and the name of the medicinal product, or its international non-
proprietary name, if any, or the trademark.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-123-
10.4. Gifts for the personal benefit of pharmaceutical professionals or healthcare
professionals (such as tickets to cultural events or of other entertainment media) are
prohibited.
10.5. Companies should follow the guideline relating to the term “inexpensive” in
the meaning used in Article 10 hereof as indicated in the provisions of any of the
Applicable Codes or related instruments.
Article 11. Sponsorship and Charity for Healthcare or Research Purposes
11.1. The provision of sponsorship and charity to institutions, organisations or
associations that are comprised of pharmaceutical professionals or healthcare
professionals and/or that provide healthcare or conduct behavioural research (that
are not otherwise covered in the Code on the Relations between the Pharmaceutical
Industry and Patient Organisations) is only allowed if: (i) they are made for the
purpose of supporting healthcare or research; (ii) they are documented and kept on
record by the company; (iii) they do not constitute an inducement to recommend,
prescribe, buy, supply, acquire or administer any medicinal product. Sponsorship
and charity to individual healthcare professionals based on this section are not
allowed. Companies’ sponsorship of healthcare professionals attending international
events is governed in Article 13 of the Code. Companies are encouraged to publicize
information about provided sponsorships and charity as defined in this Section 11.1.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-124-
Article 12. Fees for Services
12.1. Contracts between companies and institutions, organisations or associations of
pharmaceutical professionals or healthcare professionals under which such
institutions, organisations or associations provide any type of services on behalf of
companies (or any other type of funding by the company not otherwise covered by
Article 11 or the Code) are only allowed is such services (or other funding): (i) are
made for the purpose of supporting healthcare or research; (ii) do not constitute an
inducement to recommend, prescribe, buy, supply, acquire or administer any
medicinal product.
Article 13. Sponsorship of Healthcare Professionals
13.1. Companies must comply with criteria governing the selection and sponsorship
of healthcare professionals to attend trainings or events as provided in the provisions
of any Applicable Codes or related instruments. Funding must not be offered to
compensate merely for the time spent by healthcare professionals in attending events.
In the case of international events funded by the company, where attended by the
healthcare professional and if any kind of funding is provided to that particular
healthcare professional under the provisions of this Section 13.1, such funding shall
be subject to the procedure of the jurisdiction where the said healthcare professional
is engaged in his/her practice otherwise than the jurisdiction of the location of the
event. For the avoidance of doubt, Section 13.1 of this article is not intended to

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-125-
prohibit the extension of hospitality to healthcare professionals in accordance with
Article 9 hereof.
13.2. A company may sponsor participation of healthcare professionals in
international scientific events arranged by Global, European, North American,
Scandinavian and Baltic professional organisations of healthcare professionals and
scientific institutions.
13.3. When deciding whether or not to sponsor participation of healthcare
professionals in international scientific events in Europe, it is recommended to check
the preliminary evaluation of the corresponding event in the EFPIA database at
www.efpia-e4ethics.eu. It should be noted that the said EFPIA review shall in no
instance be interpreted as an evaluation of the event’s scientific content or
qualification of lecturers. Each company shall decide independently whether or not
to sponsor participation of healthcare professionals in international professional
events, but the decision should take account of the relevant rules and references of
the Code of Ethics.
13.4. The company must report such sponsorship of healthcare professionals to the
Pharmaceutical Marketing Ethics Committee within 30 calendar days following the
end of events, indicating:
a) name, venue and time of event;
b) speciality and number of sponsored pharmaceutical professionals or
healthcare professionals;

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-126-
c) full names of sponsored pharmaceutical professionals or healthcare
professionals.
Information about the sponsorship of association members will be announced
publicly on the website of the Pharmaceutical Marketing Ethics Committee. The
term “sponsorship” includes sponsorship through healthcare facilities,
pharmaceutical or medical trade unions, specialty societies, company subsidiaries
operating in other countries, etc.
Article 14. The Use of Consultants
14.1. Healthcare professionals may be used as consultants and advisors, whether in
groups or individually, for services such as speaking at and chairing meetings,
involvement in scientific/medical studies, clinical trials or training services,
participation at advisory board meetings, and participation in market research where
such participation involves remuneration and/or travel. The arrangements, which
cover these genuine consultancy or other services, must, to the extent relevant to the
particular arrangement, fulfil all the following criteria:
a. A written contract or agreement must be agreed in advance which specifies the
nature of the services to be provided and, subject to condition (g) below, the basis
for payment of those services.
b. A legitimate need for the services must be clearly identified in advance of
requesting the services and entering into arrangements with the prospective
consultants.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-127-
c. The criteria for selecting consultant must be directly related to the identified needs
and the persons responsible for the selecting of consultants must have the expertise
necessary to evaluate whether the particular healthcare professionals meet those
criteria.
d. The number of pharmaceutical professionals or healthcare professionals retained
must not be greater than the number reasonably necessary to achieve the identified
need.
e. The contracting company must maintain records concerning and make appropriate
use of, the services provided by consultants.
f. The hiring of the healthcare professional to provide the relevant service must not
be an inducement to recommend, prescribe, buy, supply, acquire or administer any
medicinal products.
g. The compensation for the services must be reasonable and reflect the fair market
value of the services provided. In this regard, token consultancy arrangements must
not be used to justify compensating healthcare professionals.
14.2. In their written contracts with consultants, companies are strongly encouraged
to include provisions regarding the obligation of the consultant to declare that he/she
is a consultant to the company whenever he/she writes or speaks in public about a
matter that is the subject of the agreement or any other issue relating to that

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-128-
company. Similarly, companies that employ, on a part-time basis, healthcare
professionals that are still practising their profession are strongly encouraged to
ensure that such persons are obliged to declare their employment arrangement with
the company whenever they write or speak in public about a matter that is the
subject of the employment or any other issue relating to that company. The
provision of Section 14.2 of this article also apply to general information of non-
promotional nature about companies which does not fall under the scope of the Code.
14.3. Limited market research, such as one-off telephone interviews or
mail/email/Internet questionnaires is excluded from the scope of this Article 14,
provided that the healthcare professional is not consulted in a recurring manner
(either with respect to the frequency of the calls to the same healthcare professional
generally or of calls relating to the same research) and the compensation for such
consultations is minimum (i.e. does not exceed the level of what a doctor would earn
doing his/her primary job within the time scale he/she spent doing market research).
14.4. If a healthcare professional attends an international event in a consultant or
advisory capacity the relevant provisions of Article 9 and the declaration procedure
in Section 13.2 apply.
Article 15. Non-interventional Studies of Marketed Medicines
15.1. A non-interventional study of a marketed medicine is a study where the
medicine is prescribed in the usual manner in accordance with the terms of its
marketing authorisation. The assignment of the patient to a particular therapeutic

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-129-
strategy is not decided by a study protocol but falls within current practice and the
prescription of the medicine is clearly separated from the decision to include the
patient in the study. No additional diagnostic or monitoring procedures are applied
to the patients and epidemiological methods are used for the analysis of collected
data.
15.2. Non-interventional studies that are prospective in nature and involve the
collection of patient data on behalf of a healthcare professional or a group of
healthcare professionals for a scientific purpose must comply with all the following
criteria:
a. The study is conducted for scientific purposes.
b. (i) There must be a written protocol and (ii) written contract between the
healthcare professionals and/or the institutes at which the study will take place, on
the one part, and the pharmaceutical company sponsoring the study, on the other
part, which specify the nature of the services to be provided and, subject to section
(c) below, the basis for the payment for those services.
c. Any remuneration must be reasonable and reflect the fair market value of the
work.
d. The study protocol must be submitted to the ethics committee for review as
prescribed by Lithuanian laws and regulations.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-130-
e. Applicable Lithuanian laws and regulations on the protection of personal data
(including collection and use of personal data) must be complied with.
f. The study must not constitute an inducement to recommend, prescribe, buy,
supply, acquire or administer a medicinal product.
g. The company’s scientific service must approve the study protocol and must
supervise the conduct of the study as described in Section 17. 2 (a).
h. The study results must be analysed by the contracting company or any other entity
acting on its behalf and summaries must be made available within a reasonable
period of time to the company's scientific service (as described in Section 17.2 (a)),
which service shall maintain records of such reports. The company must send the
summary reports to the ethics committee which reviewed the study protocol (where
requested by the committee or required by law) and to the healthcare professionals
who participated in the study, and make them available to industry self-regulation
bodies and/or committees responsible to the supervision of Applicable Codes, at
their request. If the study results are important for the assessment of benefit-risk, the
summary report should be immediately forwarded to the State Medicines Control
Agency.
i. Medical sales representatives may only be involved in an administrative capacity
and such involvement must be under the supervision of the company’s scientific

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-131-
service which will also ensure that the representatives are adequately trained. Such
involvement must not be linked to the promotion of any medicine or product for
medical use.
In Lithuania, non-interventional studies involving compensated medicines are
allowed only if this does not contravene applicable Lithuanian laws and regulations.
15.3. Companies are encouraged to follow the same principle in applying Section
15.2 to all other types of studies that are subject to Section 15.1, including
epidemiological studies and registries and other studies of retrospective nature.
Whatever is the case, Section 12.1 applies to such studies.
Article 16. Samples
16.1. When promoting medicinal products to healthcare professionals qualified to
prescribe medicinal products, promoters of medicines may use samples of medicinal
products which are not intended for sale. A sample of the medicinal product not
intended for sale must correspond to the smallest package of the medicinal product
of the same title, form and strength and the package must bear the sign “Free
medical sample – not for resale”. Leaving of samples of medicinal products not
intended for sale with healthcare professionals, distributing them to pharmaceutical
professionals and to the general public and using them for healthcare purposes are
prohibited.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-132-
16.2. Companies must have adequate systems of control and accountability for
samples of medicinal products not intended for sale handled by their representatives.
Article 17. Staff of the Pharmaceutical Company
17.1. Medical Sales Representatives must ensure that the frequency, timing and
duration of visits aiming to meet just one or two pharmaceutical professionals or
healthcare professionals and to pharmacies, hospitals or other healthcare facilities,
together with the method of presentation used by Medical Sales Representatives, do
not cause inconvenience to healthcare professionals or patients.
Each company shall ensure that its representatives, including personnel retained by
way of contract with third parties, and any other company staff who call on
healthcare professionals, pharmacies, hospitals or other healthcare facilities in
connection with the promotion of medicinal products (hereinafter referred to as
“Medical Sales Representatives”) are familiar with the relevant requirements of
Applicable Codes and with the provisions of all relevant Lithuanian laws and
regulations, and are adequately trained and have sufficient scientific knowledge to
be able to provide precise and complete information about the medicinal products
they promote.
a) Medical Sales Representatives must comply with the requirements of all
Applicable Codes, and all relevant laws and regulations. Heads of companies are
responsible for ensuring their compliance.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-133-
b) Medical Sales Representatives must approach their duties responsibly and
ethically.
c) During each visit, having regard to the provisions of applicable laws and
regulations, Medical Sales Representatives must hand to visited persons, or have
available for them, a summary of the product characteristics for each medicinal
product they represent.
d) Medical Sales Representatives must transmit to the medical department of their
companies forthwith any information they receive in relation to the use of their
company's medicinal products, particularly reports of side effects.
e) Medical Sales Representatives must ensure that the frequency, timing and
duration of visits to healthcare professionals, pharmacies, hospitals or other
healthcare facilities, together with the manner in which they are made, comply with
the procedure laid down by law.
f) Medical Sales Representatives must not use any inducements or subterfuge to gain
a call. In an interview, or when seeking an appointment for an interview, Medical
Sales Representatives must, from the outset, take reasonable steps to ensure that they
do not mislead a healthcare professional they are addressing as to their identity or
that of the company they represent.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-134-
g) The provisions of Section 15.2(i) also apply to the activities of Medical Sales
Representatives.
17.2. All members of the company’s staff, and any personnel retained by way of
contract with third parties, who are concerned with the preparation or approval of
promotional material or activities must be fully conversant with the requirements of
all Applicable Codes and relevant laws and regulations.
a) Each company must establish a scientific service in charge of information about
the company’s medicines and products for medical use, as well as of approval and
supervision of non-interventional studies. Companies may decide by themselves
about the best way to organise these services according to Section 17.2 (i.e. whether
a single service will be responsible for both duties or whether two services will be
established with clearly defined responsibilities), taking into account their resources
and structure. This department must include at least one doctor or, where appropriate,
a pharmacist who will be responsible for approving any promotional material before
release. Such person must certify that he/she has examined the final form of the
promotional material and that in his/her belief it is in accordance with the
requirements of all Applicable Codes and advertising laws and regulations, is
consistent with the summary of product characteristics and is fair, equal and truthful
representation of the proofs about the medicinal product. Furthermore, the scientific
service must include a doctor or pharmacist in charge of the supervision of any non-
interventional studies (including supervision of any responsibility in connection with
such studies, particularly where such responsibility is undertaken by Medical Sales

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-135-
Representatives). Such a person must confirm that he/she examined the protocol of
non-interventional studies and that in his/her belief the protocol is consistent with
the requirements of this Code and of other Applicable Codes.
b) Each company must appoint at least one senior employee who shall be
responsible for the supervision of the activities of the company and its subsidiaries
to ensure compliance with the standards of all Applicable Codes.
17.3. Companies engaged in pharmaceutical marketing in Lithuania cannot employ
healthcare professionals who work simultaneously at healthcare facilities.
Article 18. Enforcement
18.1. IFPA and VGA must, within current applicable rules and legislation, enforce
the provisions of this Code. In the event that a breach is established pursuant to the
procedures of the National code, each IFPA, VGA or any other company which has
joined enforcement of the Code shall require from the offending company an
immediate cessation of the offending activity and a signed undertaking by the
company to prevent recurrence.
18.2. The procedure for the examination of violations of this Code and sanctions for
violations of the Code are set out in Annex A hereto.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-136-
Article 19. Awareness and Education
19.1. IFPA and VGA must, within current applicable rules and legislation facilitate
companies’ awareness of and education about the Code, including by providing
guidance to companies in order to prevent breaches of the Code.
Annex A
Pharmaceutical Marketing Ethics Committee
INTRODUCTION
Supervision of the Code of Ethics for Pharmaceutical Marketing, which governs
pharmaceutical marketing and mutual relations with pharmaceutical professionals
and healthcare professionals as well as relations between the pharmaceutical
industry and patient organisations (hereinafter referred to as the Code) is performed
by the Pharmaceutical Marketing Ethics Committee (hereinafter referred to as
Committee). The names of reporting individuals outside the pharmaceutical industry
are kept confidential. In special cases the company specified in the report to the
Committee needs to know the identity of the reporting person to be able to examine
the case adequately. Even in such cases the identity of the reporting person shall be
disclosed only after obtaining his/her consent. The Committee shall submit the
number of processed violation reports to members of IFPA and VGA on a quarterly
basis.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-137-
The Committee shall ensure that industry and non-industry complaints are processed
in the same manner, without regard to who has made the complaint.
STRUCTURE AND RESPONSIBILITY
1. The Pharmaceutical Marketing Ethics Committee is responsible for:
1.1. Organisation of the Committee’s procedures and selection of the required
technical staff, resources and consultants;
1.2. Supervision of the Code, including advice, comments and guidance related to
the application and enhancement of the Code;
1.3. Examination of reported violations of the Code;
1.4. Imposition and enforcement of sanctions for violations of the Code;
1.5. Supervision of the Committee’s website.
2. Structure of the Pharmaceutical Marketing Ethics Committee
2.1. The Committee is accountable to IFPA and VGA. On an annual basis the
Committee shall generate its operational report, which the Chairperson of the

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-138-
Committee shall present separately at the general meetings of IFPA and VGA
members. The Committee’s annual report shall be posted on its website.
2.2. IFPA and VGA each delegate 3 members to the Committee.
2.3. The Committee shall be elected for the period of one year. Within at least one
month before expiration of this term, IFPA and VGA shall approve members of the
Committee for the next term of office. The Committee is composed of 7 members,
including the Chairperson. If a member of the Committee in person or the company
he/she represents violates the CEPM more than once over one year, the Chairperson
of the Committee may, at the Committee’s decision, file a proposal to the
association to replace the Committee member concerned.
2.4. The Committee shall be chaired by an individual outside the pharmaceutical
sector. The Chairperson of the Committee shall be approved by IFPA and VGA
upon common agreement.
2.5. Decisions shall be adopted by majority voting. The votes of the Chairperson (or
in the absence of same, his/her deputy) and three members shall form the quorum.
At least one member must represent VGA or IFPA. In the event of equal distribution
of votes, the vote of the Chairperson (or in the absence of same, his/her deputy) shall
be decisive.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-139-
2.6. The deputy to the Chairperson of the Committee shall be elected by rotation
from Committee members representing IFPA or VGA for the entire term of office of
the Committee.
2.7. The Committee shall have the right to obtain the material required for the
examination of the reported violation of the Code from pharmaceutical companies
suspected of violating the Code. The company may refuse to provide the
information which constitutes its commercial secret.
3. Operating and Funding Procedure of the Pharmaceutical Marketing Ethics
Committee
3.1. The Committee shall hold meetings upon receiving violation reports or
whenever intending to address any other matters in connection with the Code or the
Committee’s area of responsibility. Each Committee member shall have the right of
initiative to convene a Committee meeting. Committee meetings shall be convened
at the decision of the Chairperson of the Committee (or in the absence of same,
his/her deputy).
3.2. At meetings of the Committee minutes shall be taken. The draft minutes shall be
emailed to members of the Committee for information and comments. The minutes
shall be signed by the Chairperson and Secretary of the meeting. The Chairperson of
the Committee shall be responsible for storage of minutes and other materials of the
Committee.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-140-
3.3. The Committee may seek assistance from experts. Advising experts may be
invited to attend Committee meetings without the right to vote.
3.4. To prevent conflicts of interest it is required that prior to examination of the
violation members of the Committee name all interests related to the violation. The
Chairperson (deputy) shall then determine whether such a member can participate in
the examination of the reported violation. Where a member of the Committee is
related to the complainant or to the respondent, he/she shall suspend himself/herself
(the Committee shall decide which parties may attend the meeting) from the
adoption of the relevant decision as long as the Committee examines that particular
violation report.
3.5. While the Committee examines the violation report, both the complainant and
the respondent may be invited to attend or be represented at its meeting. At a
Committee meeting, the company may not be represented by the same individual
who is member of the Committee, even if he/she has suspended himself/herself from
the case.
3.6. Where it is impossible to adequately identify the circumstances of the violation
report between the complainant and the respective company based solely on the
report, the Committee shall have the right to invite directly related persons to attend
the meeting as well as to provide and receive information in oral form.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-141-
3.7. The costs of the Committee shall be covered from the IFPA and VGA budget in
equal contributions which ensure the activities of the Committee. When compiling
the budget, IFPA and VGA must include funds on a separate line according to the
planned cost estimate provided in advance by the Committee.
3.8. The Committee may incur costs in connection with the remuneration of the
Committee member outside the pharmaceutical industry and with the hiring of
experts whose opinions are reasonably required to examine specific reports, but
without exceeding the estimated budget funds. The Committee shall report its
expenditure to IFPA and VGA Boards in the form of a financial statement.
PROCEDURE FOR LODGING AND PROCESSING VIOLATION REPORTS
4. Lodging of Violation Reports
4.1. Reports of potential violations of the Code may be lodged by representatives of
pharmaceutical companies, pharmaceutical or healthcare professionals,
representatives of patient organisations, representatives of legal entities and natural
persons. After receiving information about a potential violation(s) of the Code, the
Committee may initiate ex-officio investigations.
4.2. Violations of this Code (unless the Committee initiates an ex-officio
investigation) shall be reported in writing to the Chairperson of the Committee. The

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-142-
Committee Secretary shall register the received report and notify members of the
Committee thereof.
4.3. A report of a potentially committed violation of the Code must include:
4.3.1. The full name, postal address, email address (if any) and phone number of the
reporting person;
4.3.2. The institution, company or organisation represented by the reporting person;
4.3.3. Information about the violation and available evidence (place, time,
circumstances and persons involved);
4.3.4. The articles and sections of the Code whose provisions were violated under
the circumstances specified in the Report. A violation report lodged by a
pharmaceutical company must be signed by the company’s manager or his/her
authorised person indicating the clauses of the Code which in the company’s belief
have been breached;
4.3.5. The Report shall be accompanied by documentation and other evidence which
substantiate the circumstances named in the Report.
4.4. Reports of potential violations of the Code may be provided in writing, by email
or through the section “Write us” on the Committee’s website.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-143-
4.5. Anonymous reports shall not be processed.
5. Actions upon Receiving a Violation Report
5.1. Suspected violations of the Code must be reported in writing accompanied by
all information about the violation and with the available evidence. Upon receipt of
a report of a potential violation, the Chairperson of the Committee shall within 10
(ten) business days following receipt convene a Committee meeting to review the
received material and to establish whether the report of a violation of the Code falls
within the scope of the Code. The matter may be settled by an email voting by
members of the Committee. If no responses “AGAINST” are received within 5
business days, the Committee shall be deemed to have agreed that the report falls
within the scope of the Code. After deciding that the violation report falls within the
scope of the Code, the Committee shall notify the complainant and respondent
thereof.
5.2. Where the Committee decides that the report of a violation of the Code does not
fall within the scope of the Code, the reporting person shall be notified thereof.
5.3. The Committee shall apply to the manager of the relevant company suspected of
breaching the respective provisions of the Code in writing (the letter must be faxed,
emailed or posted by registered mail to the company’s headquarters) asking to
comment on the material stated in the report and shall establish the term for
providing responses and comments.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-144-
5.4. Upon receipt of the Committee’s appeal regarding a potential violation, the
relevant company shall furnish the Committee with a written response within 5
business days following dispatch of the Committee’s letter by fax or email. Where
the response is posted by registered mail, on the sending date it must also be faxed
or emailed to the Committee. Failing to receive the company’s response within 5
business days following dispatch of the appeal, the Committee shall examine the
violation without waiting for the response.
5.5. In the process of examining the report, the Commission may apply to public
authorities requesting information available to them required to investigate the
circumstances stated in the report or ask those authorities to carry out an
investigation within their purview and to provide the obtained information to the
Committee.
5.6. After the Committee has collected sufficient information about the potential
violation, but not later than within 6 (six) weeks following receipt of the violation
report, a Committee meeting shall be convened to adopt a decision regarding the
violation of the Code. Where the meeting fails to adopt a decision, another meeting
must be arranged within 2 (two) weeks to arrive to the final decision.
5.7. The violation report must be examined in substance and the final decision must
be adopted within not more than 8 (eight) weeks following receipt thereof.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-145-
5.8. The Committee’s decision may be appealed against to a competent court of the
Republic of Lithuania in accordance with the law within 15 (fifteen) calendar days.
The Committee’s decision shall come into effect only following expiry of the
defined appeal term. During the said appeal term implementation of the
Committee’s decision and enforcement of imposed sanctions shall be suspended.
5.9. The Committee and its members undertake to protect any information received
from companies during the examination of the violation as confidential information
and to refrain from using it for any purposes other than its primary purpose.
6. Decisions of the Pharmaceutical Marketing Ethics Committee
6.1. Where the Committee decides that the Code was breached, this shall be
communicated to the complainant and the respondent indicating causes for adopting
such a decision.
6.2. Where the Committee decides that the Code was breached, it may impose on the
relevant company one or more (depending on the severity of the violation) sanctions:
a) a written warning;
b) notifying the company’s principal office;
c) notifying IFPA and VGA members;
d) reporting the violation to EU member associations;
e) proposing to the general meeting of IFPA or VGA members to exclude the
breaching company from the association;

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-146-
f) forwarding the case for further examination by public authorities;
6.3. The Committee shall publish effective decisions on its website:
1) in the case of severe or recurrent violations, indicating the company’s name and
details of the violation;
2) in the case of minor violations, providing details of the violation without
indicating the company’s name.
6.3. Where the Committee finds that no breach occurred, such a decision of the
Committee shall not be announced subject to informing only the complainant and
the respondent companies.
Annex B
Guidelines for Internet Websites Available to Healthcare Professionals,
Patients and the Public in the EU
The Guidelines for Internet Websites Available to Healthcare Professionals, Patients
and the Public in the EU set forth herein are intended as a supplement to the
provisions of the Code for Pharmaceutical Marketing (hereinafter referred to as the
Code).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-147-
Section 1. Transparency Of Website Origin, Content And Purpose
Each website shall clearly identify:
a) the identity and physical and electronic addresses of the sponsor(s) of the
website;
b) the source(s) of all information included on the website, the date of
publication of the source(s) and the identity and credentials (including the
date credentials were received) of all individual/institutional providers of
information included on the website;
c) the procedure followed in selecting the content included on the website;
d) the target audience of the website (e.g. healthcare professionals, patients and
the general public, or a combination thereof); and;
e) the purpose or objective of the website.
Section 2. Content of Websites
a) Information included in the website shall be regularly updated and shall clearly
display, for each page and/or item, as applicable, the most recent date as of which
such information was updated.
b) Examples of the information that may be included in a single website or in
multiple websites are: (1) general information on the company; (2) health education
information; (3) information intended for healthcare professionals (as defined in the

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-148-
Code); (4) non-promotional information intended for patients and the general public
about specific medicinal products marketed by the company.
1) General information on the company
Websites may contain information that would be of interest to investors, the news
media and the general public, including financial data of the company, description of
research and development programmes, discussion of regulatory developments
affecting the company and its products, information for prospective employees, etc.
The content of this information is not regulated by these guidelines or provisions of
the medicines advertising law.
2) Health education information
Websites may contain non-promotional health education information about the
characteristics of diseases; methods of prevention and screening and treatments, as
well as other information intended to promote public health. They may refer to
medicinal products, provided that the discussion is balanced and accurate. Relevant
information may be given about alternative treatments, including, where appropriate,
surgery, diet, behavioural change and other interventions that do not require use of
medicinal products. Websites containing health education information must always
advise persons to consult a healthcare professional for further information.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-149-
3) Information for healthcare professionals
Any information on websites directed to healthcare professionals that constitutes
promotion (as defined in the Code) must comply with the Code and Lithuanian law.
Such information must be clearly identified as information for healthcare
professionals. In addition, access to such information must be technically restricted
for patients and for the general public and shall be made available only subject to
request from a healthcare professional.
4) Non-promotional information for patients and the general public
Subject to any national laws and regulations, websites may include non-promotional
information for patients and the general public on products distributed by the
company (including information on their indications, adverse effects, interactions
with other medicines, proper use, reports of clinical research, etc.), provided that
such information is balanced, accurate and consistent with the approved summary of
product characteristics. For each product that is discussed, the website must contain
full, unedited copies of the applicable summary of product characteristics and
patient leaflet. These documents should be posted in conjunction with other
information about the products or be connected with that discussion by a prominent
link advising the reader to consult them. In addition, the website may provide a link
to the full, unedited copy of any public assessment report issued by the Committee
for Medicinal Products for Human Use or the State Medicines Control Agency.
Brand names should be accompanied by international non-proprietary names. The

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-150-
website may include links to other websites containing reliable information on
medicinal products, including websites maintained by government authorities,
medical research bodies, patient organisations, etc. The website must always advise
persons to consult a healthcare professional for further information.
Section 3. Email Enquiries
A website may invite electronic mail communications from healthcare professionals
and patients or the general public seeking further information regarding the
company’s products or other matters (e.g., feedback regarding the website). The
company concerned may reply to such communications in the same manner as it
would reply to enquiries received by post, telephone or other media. In
communications with patients or members of the general public, discussion of
personal medical matters must be avoided. If personal medical information about the
specific individual’s health problems is revealed, it must be held in confidence and
not published. Where appropriate, replies shall recommend that a healthcare
professional be consulted for further information.
Section 4. Links from Other Websites
Links may be established to a company-sponsored website from websites sponsored
by other persons, but companies should not establish links from websites designed
for the general public to company-sponsored websites that are designed for
healthcare professionals. Based on the same principle, links may be made to

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-151-
individual websites, including websites sponsored by the company or other persons.
Links should ordinarily be made to the home page of a website or otherwise
managed so that the reader is aware of the identity of the website.
Section 5. Website Addresses on Packaging
Subject to any applicable national laws and regulations, the addresses of company-
sponsored websites that comply with these guidelines may be included in packaging
of medicinal products.
Section 6. Scientific Review
Companies should ensure that scientific and medical information prepared by them
for inclusion in their websites is reviewed for accuracy and compliance with the
relevant code(s). The scientific service established within the company pursuant to
those provisions of the Applicable Code that adapt the Section 13.2 of the Code may
perform this function, or it may be entrusted to other appropriately qualified
professionals.
Section 7. Privacy
The website must conform to legislation and Applicable Codes of conduct
governing the privacy, security and confidentiality of personal information.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-152-
Annex C
Code of Ethics on the Relations between the Pharmaceutical Industry and
Patient Organisations
INTRODUCTION
The pharmaceutical industry recognises that it has common interests with patient
organisations, which represent and/or support the needs of patients and/or caregivers.
In order to ensure that relationships between the pharmaceutical industry and patient
organisations are ethical and transparent, IFPA and VGA have adopted the Code of
Ethics on the Relations between the Pharmaceutical Industry and Patient
Organisations, which is considered as an integral part of the Code of Ethics for
Pharmaceutical Marketing governing pharmaceutical marketing and relations with
healthcare professionals as well as relations between the pharmaceutical industry
and patient organisations (hereinafter referred to as the Code).
The present Code builds upon the following principles:
1. The independence of patient organisations, in terms of their political
judgement, policies and activities, shall be assured.
2. All partnerships between patient organisations and the pharmaceutical
industry shall be based on mutual respect with the views and decisions of
each partner having equal value.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-153-
3. The pharmaceutical industry shall not request, nor shall patient organisations
undertake, the promotion of a particular prescription-only medicine.
4. The objectives and content of any partnership shall be transparent. Financial
and nonfinancial support provided by the pharmaceutical industry shall
always be clearly acknowledged in a proper way.
5. The pharmaceutical industry welcomes funding of patient organisations from
multiple sources.
Scope
The provisions of this Code shall apply to relations between IFPA and VGA
member companies operating in Lithuania and their affiliates or hired third parties as
well as to other parties acceded to this Code and patient organisations.
Patient organisations are defined as any non-profit organisation (including the
umbrella organisations that integrate patient associations), composed of patients
and/or caregivers, the main activity and objectives of which are expressed in
supporting the needs of patients and/or caregivers.
Application
Pharmaceutical companies must comply with this Code and any laws and
regulations that apply to them; and:

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-154-
(a) In the case of partnerships or other mode of joint activity with a patient
organisation in Lithuania, this Code and Lithuanian laws and regulations
shall apply;
(b) In the case of cross-border partnerships and activities, the industry code of
the country where the patient organisation has its principal headquarters shall
apply. In the event of discrepancies between the codes, more stringent
provisions of a code shall apply.
Activity as referred to above shall mean any interaction between a pharmaceutical
company and a patient organisation, including financial support.
Provisions
Article 1 Non-promotion of prescription-only medicines
Promotion of prescription-only medicinal products to the general public is
prohibited, unless permitted by Lithuanian law.
Article 2 Written agreements
Any financial support, significant indirect support and/or other forms of significant
non-financial support from a pharmaceutical company to a patient organisation shall
be provided basing on written agreement. The agreement must specify the amount of
funding/non-financial support as well as its purpose (e.g. unrestricted grant, specific
meeting or publication, etc.). In addition, a description of significant indirect and
significant non-financial support (e.g. time allocation for a public relations campaign
and the nature of participation) must be provided. When support is provided to a

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-155-
patient organisation in another country, the agreement must specify the codes of
ethics that apply to cooperation relations in the home countries of the
pharmaceutical company and of the patient organisation. Each pharmaceutical
company must have an approval process in place for such agreements.
An example of a written agreement is provided in Annex I.
Article 3 Use of logos and proprietary materials of patient organisations
The public use of patient organisation’s trademark (logos and/or its proprietary
materials) by a pharmaceutical company requires written permission from the
patient organisation. The provision of such permission shall be based on a written
statement of the specific purpose and the way the trademark (logo) and/or the
proprietary materials will be used.
Article 4 Editorial control
Companies must not influence the reference materials made by a patient
organisation they sponsor in a manner favourable to their own commercial interests.
This prohibition does not preclude companies from correcting factual inaccuracies in
materials.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-156-
Article 5 Transparency
a. Each company must make publicly available a list of patient organisations to
which it provides financial support and/or significant indirect/non-financial
support. This should include a description of support that is sufficiently
complete and clear to enable an average reader to gain an understanding of
the meaning of support. The description must include the monetary value of
financial support and of invoiced costs. For significant non-financial support
that cannot be assigned a meaningful monetary value the description must
clearly describe the non-monetary benefit that the patient organisation
receives. This information shall be provided on a national and European
level. In Lithuania information about financial support and/or significant
indirect/non-financial support shall be provided to the Pharmaceutical
Marketing Ethics Committee once per calendar year before February 1 of the
following year.
b. Companies must ensure that their sponsorship is always clearly
acknowledged and apparent from the outset.
c. Each company must make publicly available a list of patient organisations
that it has engaged to provide significant contracted services. This should
include a description of services provided that does not disclose confidential
information but is sufficiently complete to enable the average reader to gain
an understanding of the nature of the arrangement. Each company shall also
make public the total amount paid per patient organisation over the reporting
period in accordance with the procedure and timeframe described above.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-157-
Article 6 Contracted Services
Contracts between companies and patient organisations where under the latter
provide any type of services to companies are only allowed if such services are
provided for the purpose of supporting healthcare or research.
Members of patient organisations may be invited to deliver presentations or to
provide expert or advisory services for a compensation at company-sponsored
events or advisory boards. Arrangements that cover consultancy or other services
must, to the extent relevant to the particular arrangement, meet each of the following
criteria:
a. A written contract or agreement is agreed in advance specifying the nature of
the services to be provided, and, subject to clause (g) below, the basis of
payment for those services;
b. A legitimate need for the services has been clearly identified and
documented in advance of requesting the services and entering into the
agreements;
c. The criteria for selecting services are directly related to the identified need
and persons in charge of selecting the service have the expertise required to
evaluate whether the particular experts and advisors meet those criteria;
d. The scope of the service is not greater than is reasonably necessary to meet
the identified need;

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-158-
e. The contracting company keeps records of and makes appropriate use of the
services;
f. The engaging of patient organisations into paid activities is not an
inducement to recommend a particular medicinal product;
g. The compensation for the services is reasonable and does not exceed the fair
market value of the services provided. In this regard the payment of
compensation to patient organisations may not be justified with symbolic or
formal agreements for consulting and other services;
h. In their written contracts with patient organisations companies are strongly
encouraged to include provisions regarding an obligation of the patient
organisation to declare that they have provided paid services to the company
whenever they write or speak in public about a matter than is the subject of
the agreement or any other issue relating to that company;
i. Each company must make publicly available a list of patient organisations
that it has engaged to provide paid services – please refer to Article 5(c)
above.
Article 7 Single company funding
No company may demand the conditions of being the sole sponsor of the respective
patient organisation or any of its major programmes.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-159-
Article 8 Events and hospitality
All events sponsored or organised by a company must be held in an appropriate
venue that is conductive to the main purpose of the event, avoiding those that are
renowned for their entertainment facilities or are extravagant“. “Entertainment
venues” are understood as places for leisure and entertainment which advertise their
entertainment facilities on promotional leaflets, also publicly in the press or on the
Internet and which are intended primarily for recreation and/or entertainment, i.e.
entertaining activities rather than professional/business meetings. “Extravagant
venues” are understood as places which are lavish and deluxe and the visiting of
which could be prejudicial to the image of patient organisations or of the
pharmaceutical industry.
All forms of hospitality of the pharmaceutical company offered to patient
organisations and their members must be “reasonable” and must not override the
principal purpose of the event whether organised by a patient organisation or a
pharmaceutical company.
Hospitality must be limited to the funding of return travel to the event, catering,
accommodation and registration fees.
Hospitality may only be extended to persons who are invited to and participate in an
event in their right of a participant. In exceptional cases, in case of apparent health

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-160-
needs (e.g. disability), travel, catering and accommodation expenses and the
registration fee of the accompanying person considered a carer can be covered.
All forms of hospitality offered to patient organisations and their representatives
shall be adequate and related to the purpose of the event.
Hospitality shall not include sponsoring or organising entertainment (e.g. sporting or
leisure events).
No company may organise or sponsor an event that takes place outside its country of
incorporation, unless:
a) most of the invitees are from other countries (other than the state of registration of
the company organising the event) and, given the countries of origin of most of
the invitees it makes greater logistical sense to hold the event in another country;
b) given the location of the relevant resource or expertise that is the object or subject
matter of the event, it makes greater strategic/logistical sense to hold the event in
another country.
Article 8 Enforcement and implementation
Ensuring supervision over the Code of Ethics on the Relations between the
Pharmaceutical Industry and Patient Organisations and compliance with the

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-161-
provisions of this Code respectively shall be controlled by the Pharmaceutical
Marketing Violation Committee, as defined in Annex A of the Code. The procedure
for lodging and examining violation reports shall be the same as that of the Code of
Ethics for Pharmaceutical Marketing (Annex A).
Annex I
201.... Declaration of Interest
of member of the Pharmaceutical Marketing Ethics Committee
......................................................................(full name)
1. Have you been engaged in any kind of financial relationships with
pharmaceutical manufacturers other than your represented company (employment
relations, the pharmaceutical manufacturer paid for your participation in a
conference, congress, consultation, symposium, etc., paid you a honorarium for a
presentation, copyright work, letter, advice or studies, you were involved in clinical
trails conducted by the pharmaceutical manufacturer or received gifts the value of
which exceeded 1 MSL and the like) in the past 5 years?
YES
NO
If “YES”, please provide more detailed information specifying the nature of
interest, name of the pharmaceutical manufacturer,
etc. .………………………………………………………...........................................
...............................

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-162-
2. Are there any other circumstances that could affect your objectivity and integrity
of decision-making as member of the Code of Ethics for Pharmaceutical Marketing
Violation Committee?
YES
NO
If “YES”, please provide more detailed information specifying the nature of
interest, name of the pharmaceutical manufacturer,
etc. ………………………………………………………............................................
...............................
3. If your answer to at least one of the questions was “YES”, due to a potential
conflict of interest the Committee may propose that you do not participate in the
consideration of related matters or voting.
I confirm that the above is true and complete information. Should any of the details
provided in this declaration change, I commit to provide changes within 20 days. I
agree that my declaration is communicated to IFPA or VGA members.
----------------------- ----------------------------------------------------------------
(signature and full name of the person who completed the declaration and
completion date)
The declaration is completed once a year before 1 March of the current year
and is provided to the Chairperson of the Committee.
----------------------------------------------------------------------------------------
(signature and full name of the person who accepted the declaration and date)

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-163-
Annex II
Template of a written agreement between the pharmaceutical industry and
patient organisations
Any financial support, significant indirect support and/or other forms of significant
non-financial support from a pharmaceutical company to a patient organisation shall
be provided basing on written agreement.
Below please find the key elements of a written agreement. The agreement must
directly indicate its subject, i.e. what the parties agree about, consistent with the
requirements of the Code of Ethics on the Relations between the Pharmaceutical
Industry and Patient Organisations.
• Name of activity
• Name of partnering organisations (pharmaceutical company, patient
organisation and, where applicable, third parties that will be brought in to
help , as agreed between both the pharmaceutical company and the patient
organisation)
• Type of activity (e.g. whether agreement relates to unrestricted grant,
specific event, publication, etc.)
• Objectives
• Envisaged role of the pharmaceutical company and the patient organisation
• Time-frame

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-164-
• Amount of funding
• Description of significant indirect/non-financial support (e.g. the donation of
public relations agency, free courses)
• Country codes valid in the home countries of the pharmaceutical company
and of the patient organisation that apply to cross-border cooperation
relations between patient organisations and pharmaceutical companies.
All parties must be well aware that support must be clearly indicated and known
from the onset.
Applicable Code(s) of ethics:
Contracting parties:
Contract date:

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-165-
APPENDIX - IV
THE NEW PHRMA CODE ON INTERACTIONS WITH HEALTHCARE
PROFESSIONALS
(Effective January 1, 2009)
The recently released PhRMA Code scheduled to take effect January 1, 2009
is an extension and amplification of the Code that became effective July 1, 2007.
The Codes are remarkably similar, and focus on perceived abuses of pharmaceutical
industry interactions with healthcare professionals (HCPs).
In both cases, there is a clear distinction between legitimate pharmaceutical
promotion and possible inappropriate interactions with HCPs. Traditional product
promotion is not addressed in either of the Codes, but gifts from pharmaceutical
manufacturers, their representatives, and other manufacturer interactions with HCPs
are covered in detail.
Both the 2002 Code and the 2009 Code can be seen as influenced by the
anti-kickback statutes issued by the OIG. The new Code is designed to eliminate
inappropriate inducements to HCPs to prescribe specific products. In general,
outright gifts lacking medical relevancy may be correctly viewed as improper
inducements. On the other hand, advertising placed in traditional medical
advertising media (medical publications, prescription forms, patient record services,
etc.) is designed to persuade through education.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-166-
Items that are obviously intended for the personal benefit of HCPs “…such
as floral arrangements, artwork, music CDs, or tickets to a sporting event…” are
deemed unacceptable in both the 2002 and 2009 Codes. (See Item 7.c in the 2002
Code and Item 10 in the 2009 Code.)
The major difference between the Codes that occurs with regard to
promotional items (i.e., gifts) comes in the change from the previous Code where
“Items of minimal value may be offered by a company if they are primarily
associated with the HCP’s practice (pens, notepads, and similar ‘reminder’ items
bearing a corporate or brand logo).” (These items have been routinely referred to as
“medically relevant.”)
The new Code places a more restrictive boundary in this area, relegating
items of “medical relevance” that provide neither professional nor patient education
to the level of unacceptability. The new Code requires that brand presentations (via
personal and/or non-personal media) have an HCP or patient education component.
Both Codes refer specifically to interactions between pharmaceutical
companies and HCPs in terms of what may be “offered” or “given” to HCPs by
pharmaceutical representatives. Personal and/or non-personal media must have a
HCP or patient education component. Both Codes seek to eliminate any appearance
of impropriety in the interaction between pharmaceutical representatives and
physicians (and their staffs). Replacing “medically relevant” with “items of an

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-167-
educational nature” is one way to circumscribe the types of materials individual
pharmaceutical companies may appropriately provide to physicians.
It is useful to note the first paragraph from Item #10 of the new Code
(emphasis added): “Providing items for HCPs’ use that do not advance disease or
treatment education—even if they are practice-related items of minimal value (such
as pens, note pads, mugs and similar “reminder” items with company or product
logos)—may foster implications that company interactions with HCPs are not based
on informing them about medical and scientific issues. Such non-educations items
should not be offered to HCPs or members of their staff, even if they are
accompanied by patient or physician educational materials.”
The 2009 Code expands the definition of inappropriate “gifts to physicians” as it
was initially outlined in the 2002 Code.
A distinction may also be made between gifts to physicians and the inclusion
of traditional product promotion in services to which they may subscribe. This
includes prescription forms, patient record services, and similar services physicians
request to receive (and expect to receive) regardless of support from any given
company or brand. Medical publications and third-party services provided to
physicians are not initiated by any particular company or brand, and constitute usual
and customary promotion activity.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-168-
Health Care Ethics
ETHICAL DECISION MAKING IN HEALTH CARE
Medical ethics, more commonly referred to today as biomedical ethics, is not a new
area of inquiry. The first code of ethics for medicine was credited to Hippocrates in
the 5th century B.C. In many ways, his code is timeless. For example, his direction
that no physician should “give a deadly drug to anybody if asked for it, nor . . . make
a suggestion to this effect” (Edelstein, 1967, p. 6) provides one moral perspective on
the contemporary issue of assisted suicide. What has changed over the past decade
or so is the attention given to biomedical ethics in the professional and scientific
literature and by health professions schools. In pharmacy, for example, surveys were
conducted in 1963 and again in 1980 to determine the state of ethics instruction in
schools of pharmacy. The 1963 survey found that only 8 of 65 schools that
responded required a formal, separate course in ethics; 19 schools offered no
required or elective course that included ethics as an explicit part. In the 1980 study,
the numbers were still worse: only 2 of 52 schools required an ethics course, and 32
schools did not offer one (Smith and Smith, 1981).
Today, most pharmacy, nursing, and medical schools require some instruction in
biomedical ethics. Haddad and colleagues, reporting on a 1991 survey of ethics
instruction at pharmacy schools, said, “While the quantity of ethics instruction has
not increased, there are encouraging signs that the quality and depth of ethics
education is improving” (Haddad et al., 1993, p. 35S). No one factor is responsible

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-169-
for the heightened attention given to the study of ethics in health care. Several
factors, however, are certainly important contributors. First is the explosion of
biotechnology. Medical professionals now have available to them an arsenal of
weapons to fight disease. The ability to sustain life, deal with premature birth, and
treat conditions that heretofore were thought to be untreatable has generated new
ethical dilemmas. When we were unable to sustain the life of a person in a persistent
vegetative state, then the question of whether or not to “pull the plug” did not arise.
Likewise, when no treatment existed for dealing with prematurity, cancer, or
cardiovascular disease, the ethical questions associated with those treatments did not
need to be answered. The second factor is the rapidly rising cost of health care in the
United States. The United States spends a greater proportion of its gross domestic
product on health care than any other nation, yet leaves many of its citizens without
adequate access to care, as in the case of Leo and his family. As Howard Hiatt (1975)
has described, we have only limited resources to spend on health care; how much we
spend, and how we allocate it within health care, is a vital question we must answer
as a society. These financial concerns give rise to questions of limiting access,
rationing, and denial of care.
Biotechnology and costs are not the only factors that have led to this increased
emphasis on ethics instruction and research, but they are clearly major contributors.
Whatever the reason, ethical considerations play a very significant role in health
care delivery as we begin the new millennium. This chapter discusses health care
ethics from a practical perspective by introducing ethical “tools” that health care
professionals can use in their daily practice. These tools include ethical theories and

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-170-
principles, moral rules, and codes of ethics. Special emphasis is given to the ethical
aspects of pharmacy practice.
“MACRO” VERSUS “MICRO” ETHICAL SITUATIONS
Ethical situations in health care can be divided into two broad categories: “macro”
and “micro.” Macro situations involve issues that are not specific to a given health
care practitioner (such as the pharmacist); these situations involve issues that must
be addressed by all health care practitioners and society in general (such as abortion,
assisted suicide, genomics, rationing of and access to health care, organ
transplantation, and in vitro fertilization). Micro situations are those that may
confront individual practitioners in the course of their daily practice. In the case of
pharmacists, they include the use of placebos, patient confidentiality (for example,
revealing information about a patient’s medications to members of his or her family),
informed consent (such as what and how much information about a medication
should be disclosed to a patient), and as illustrated in Leo’s situation, providing
necessary medications to those who are uninsured and unable to pay.
Sometimes, macro issues are manifested in micro situations. This is especially true
with socially controversial issues like abortion and assisted suicide. For example, a
pharmacist may receive a prescription for a drug that is known to be intended for use
in an assisted suicide. The pharmacist must deal not only with the legal issues
involved but also with his or her ethical responsibility as a health care professional.
A further complication in this and similar situations is what—if any—influence the

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-171-
pharmacist’s (or other health care professional’s) personal beliefs should have on his
or her course of action.
COMPETENCE, TRUSTWORTHINESS, AND CARING
Any discussion of health care ethics must begin by describing the basic moral
responsibilities health care practitioners have toward their patients. Berger (1993)
has attempted to describe the characteristics that a pharmacist should possess. First,
pharmacists must be competent. They must possess a knowledge base that at least
minimally allows them to carry out their functions as reliable therapeutic experts.
However, competency is more than simply having an adequate base of knowledge.
Skills that allow the pharmacist to appropriately time and organize patient
counseling information, or that include the patient as a partner in his or her own care,
are of equal importance in evaluating a pharmacist’s competence.
Second, pharmacists must be trustworthy. Patients must know that they can
confidentially seek the advice and assistance of their pharmacist and that their
wishes will be carried out. As Berger notes, “Being seen as trustworthy by the
patient is connected to the ethical covenant made between the pharmacist and the
patient. Once the pharmacist and patient identify what each is responsible for, trust
becomes a measure of the patient’s perception of how well and how consistently the
pharmacist upholds his or her end of the covenant” (Berger, 1993, p. 2401).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-172-
Third, pharmacists must care for and about their patients. The American Pharmacists
(formerly Pharmaceutical) Association (APhA) code of ethics (1995) directs, “A
pharmacist places concern for the wellbeing of the patient at the center of
professional practice.” Unfortunately, pharmacists do not always effectively
communicate that they care about their patients’ welfare. All too often, patients
perceive just the opposite. Busy practitioners who fail to spend adequate time
interacting with their patients do little to alter this perception. Conversely,
pharmacists who do spend time with their patients and attempt to understand
patients’ concerns are much more likely to be viewed as caring. As Berger points
out, “Probably nothing is more powerful in communicating caring than
understanding, and thus legitimizing, the concerns of the patient” (Berger, 1993, p.
2401).
These characteristics of pharmacists described by Berger also hold true for all health
professionals. Physicians, nurses, physical therapists, and others should—within the
moral and professional parameters of their own profession—strive to be competent,
trustworthy, and caring (McCarthy, 1996c).
THE HEALTH PROFESSIONAL–PATIENT RELATIONSHIP: CONSUMERISM
VERSUS PATERNALISM
Not long ago, when patients were instructed by their physician or pharmacist to have
an operation, go for a laboratory test, or take a medication, they did so without
question. Medical paternalism—the belief that the health care professional knew

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-173-
best—was accepted as standard practice by most health care professionals and their
patients. The medical rights of patients were not as widely recognized as other rights
(such as suffrage or due process).
Today, patients have become true consumers of medical care. Patients wish—and
have a right—to be informed and to be asked for their consent. To do otherwise
would be both unprofessional and unethical—not to mention the potential legal
ramifications. Patients expect a certain level of service. As with sellers of other
goods and services, health professionals who fail to meet the demands of health care
consumers may lose customers or experience legal problems (McCarthy, 1996c).
MORAL RIGHTS VERSUS LEGAL RIGHTS TO HEALTH CARE
It is important in any discussion of health care ethics to be clear about what is meant
by the term rights. In contemporary U.S. society, one frequently refers to the legal
rights of individuals. These are rights that are guaranteed fundamentally in the U.S.
Constitution (such as the right of free speech and the right of assembly) or are
provided by laws and regulations promulgated at the federal, state, or local level. We
sometimes confuse what is really a legal duty (such as providing free elementary
and secondary school education) with our moral obligation to do something (such as
our responsibility to ensure that the next generation of Americans is provided with
an adequate education).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-174-
Moral rights may be reinforced by laws, but their basis lies not in the law, but in
ethical principles. Such rights might include the right to live without fear of harm
and the right to food and adequate shelter. More recently, Americans have grappled
with the question of health care as a moral right. Do Leo and his children, for
example, have a moral right to adequate health care? As one might expect, moral
rights and legal rights may be in conflict. There is disagreement over whether issues
like abortion involve moral rights or legal rights. The question of the right to die has
been played out in the media across the country. Dr. Jack Kevorkian and his so-
called suicide machine have forced this society to deal with a moral question in legal
terms.
PATIENTS’ RIGHTS
When patients seek the care of health care providers, what rights do they have?
What can they reasonably expect from health care providers? Patients can expect
that clinicians will employ their knowledge and experience in caring for them. As
autonomous individuals, patients can expect that health care providers will respond
to their wishes about their treatment.
At first glance, the American health care system seems fundamentally based upon
ensuring the rights of patients. Patients generally choose their own physician,
pharmacy, and hospital. Patients are allowed to choose from multiple options for
treatment when they exist (such as surgery versus drug therapy). Patients must give
their approval, through the process of informed consent, prior to the initiation of

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-175-
care. All of the preceding presupposes that treatment is available and that the patient
has the economic wherewithal to pay for that treatment. For patients who are
uninsured or lack the ability to pay (like Leo), the right to choose the nature of their
health care is meaningless. As Mappes and Zembaty argue, the United Nations (UN)
Declaration of Human Rights may state “that all persons have a right to medical
treatment” (1991, p. 36), but “A citizen of the United States . . . cannot walk into a
hospital, demand and receive treatment simply on the basis of the claim that the UN
Declaration proclaims his or her right to such care” (1991, p. 37). Patients also have
a right to treatment that is both safe and effective within given parameters. The
fundamental question that must be posed prior to considering any medical or
surgical treatment for a patient is, “Is the treatment safe and effective?” Such a legal
standard for drugs has been in effect since the early part of last century (Musto,
1987). Not only must a drug be shown to be effective—that is, able to produce the
effect for which it was administered—but it must do so with a certain degree of
safety.
HEALTH CARE PRACTITIONERS’ DUTY TO THEIR PATIENTS
What is the responsibility of health care practitioners? As Mappes and Zembaty
point out, “The [Hippocratic] oath requires physicians to act so as to ‘benefit’ the
sick and ‘keep them from harm’” (1991, p. 45). Some might argue that health care
providers have a Hippocratic responsibility to their patients and that this
responsibility focuses solely on what is best for the patient, irrespective of the
consequences to others.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-176-
This view is supported by the Code of Ethics of the APhA, which states, “A
pharmacist promotes the good of every patient in a caring, compassionate, and
confidential manner” (APhA, 1995, p. 2131). The code suggests that pharmacists
have a moral obligation to do whatever they deem necessary in the interest of their
patients. But the code goes on to state, “A pharmacist serves individual, community
and societal needs.” Therefore, how far does a pharmacist’s or another health care
professional’s duty to his or her patients go? Is it the health care professional’s
moral obligation to care for patients without exception?
LEGAL RESPONSIBILITY VERSUS MORAL OBLIGATION
Rem Edwards provides an example of a radical interpretation of the Hippocratic
Oath when he asserts that medical professionals have an obligation to do whatever is
necessary to relieve the pain and suffering of their patients (Edwards, 1984).
Edwards’ contention, although seemingly laudatory, has serious flaws when applied
to medical practitioners. All health care professionals practice under the constraints
of law, which may limit their doing “whatever is necessary.”
As a result, the patient’s rights and the practitioner’s responsibilities may sometimes
be in conflict not on ethical grounds but on legal ones. To direct that health care
professionals should assume an individualistic approach and take an illegal, yet
ethical, action for their patients despite the legal consequences is asking them to
unrealistically subjugate their own interests to those of their patients.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-177-
ETHICAL RESPONSIBILITY IN PHARMACY: PHARMACEUTICAL CARE
In their landmark paper, the members of the Commission to Implement Change in
Pharmaceutical Education stated their belief “that the mission of pharmacy practice
is to render pharmaceutical care. Pharmaceutical care focuses pharmacists’ attitudes,
behaviors, commitments, concerns, ethics, functions, knowledge, responsibilities
and skills on the provision of drug therapy with the goal of achieving definite
outcomes toward the improvement of a patient’s quality of life” (Commission to
Implement Change in Pharmaceutical Education, 1993, p. 376).
Pharmaceutical care, therefore, changes the focus of pharmacy practice and
broadens the professional responsibility of pharmacy practitioners. In traditional
pharmacy practice, both the legal and ethical obligations of pharmacists centered
around ensuring that the proper medication as ordered by the prescriber was
delivered to the patient. Physicians, and not pharmacists, were the health care
professionals who held ultimate responsibility for monitoring the patient’s progress
and ensuring that the desired outcome was achieved. Pharmaceutical care directs
that this responsibility is to be a shared obligation between the prescriber and the
pharmacist (McCarthy, 1996c; for further reading, see Chapter 3).
VEATCH’S FRAMEWORK FOR ETHICAL ANALYSIS

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-178-
Robert Veatch (1989) has suggested a framework for ethical analysis that health care
professionals can use to determine the ethical course of action to follow in a given
situation. His four-step approach involves ensuring adequate knowledge of all the
pertinent facts involved in a given situation (step 1), and the application of moral
rules (step 2), ethical principles (step 3), and ethical theories (step 4). When faced
with a situation involving ethical decision making, health care practitioners should
begin with step 1 and continue along Veatch’s continuum, through steps 2, 3, and 4,
if needed, until a decision is made
Veatch contends that ethical situations can sometimes be solved without the
application of moral rules, ethical principles, or ethical theories. Sometimes an
ethical dilemma can be solved by simply ensuring that all the facts are known about
a case (step 1). For example, a question of whether to break patient confidentiality
might be moot if it is determined that the patient has agreed to allow the health
professional to divulge such information.
If step 1 does not provide an answer, step 2 involves the application of moral rules.
The rules of confidentiality and/or consent (informed consent) may offer some
guidance. If a dilemma still exists, ethical principles may be employed (step 3).
These include autonomy, beneficence, no maleficence, veracity, fidelity, and justice.
Sometimes there may be a conflict among two or more moral rules or ethical
principles. In such cases, one should determine whether one rule or principle or
combination of rules or principles has precedence in the given situation; if not, an
ethical theory should be employed. According to Veatch, ethical theories (step 4) are
the ultimate arbiter of ethical dilemmas (see Exhibit 7–1).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-179-
ETHICAL THEORIES
A number of ethical theories have been described. The two most prominent types in
the modern period are teleological (consequentialist) theories and deontological
(nonconsequentialist) theories. There are other approaches to ethics that have
applicability to the biomedical field, such as virtue-based and feminist theories.
However, most contemporary biomedical texts focus on teleological and
deontological theories.
Teleological theories, such as utilitarianism, state that the rightness or wrongness of
an action depends on the consequences produced. According to Beauchamp and
Childress: “Consequentialism is the moral theory that actions are right or wrong
according to their consequences rather than any intrinsic features they may have,
such as truthfulness or fidelity” (1989, p. 25). Utilitarianism, as a consequentialist
theory, directs that the most appropriate course of action is that which will produce
the “greatest good for the greatest number” when the consequences of all
alternatives in a given situation are weighed.
Conversely, deontological theories, such as Kantian ethical theory, argue that the
rightness or wrongness of an action is independent of the consequences produced.
According to Beauchamp and Childress, “Deontologists maintain that the concepts
of obligation and right are independent of the concept of good and the right actions
are not determined exclusively by the production of good consequences” (1989, p.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-180-
26). Deontologists maintain that factors other than consequences, such as integrity
and truth telling, should be included when determining the ethical acceptability of a
given action (Beauchamp and Childress, 1989).
For example, consider the question of whether a health care professional ought to
tell an elderly patient she is terminally ill despite pleas from her children that she not
be told. A utilitarian would consider the consequences of the available options (tell
or not tell), while the Kantian would consider factors including the health care
professional’s obligation to be truthful with the patient.
A more detailed discussion of ethical theories is beyond the scope of this chapter,
especially given that ethical principles and moral rules are more likely to be the
“tools” used by health care practitioners on a daily basis as they face ethical
situations.
ETHICAL PRINCIPLES AND MORAL RULES
Medical practitioners have an ethical obligation to care for their patients. Ethical
principles and moral rules provide guidance for practitioners about what this
obligation entails. When faced with an ethical dilemma, health care professionals
should first consider whether or not moral rules are applicable and helpful in
determining an acceptable course of action (step 2). If not, they should move to the
level of ethical principles (step 3) for guidance.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-181-
Autonomy
The principle of autonomy states that an individual’s liberty of choice, action, and
thought is not to be interfered with. As Beauchamp and Childress have noted,
“Autonomy has . . . been used to refer to a set of diverse notions including self-
governance, liberty rights, privacy, individual choice, liberty to follow one’s will,
causing one’s own behavior, and being one’s own person” (1989, pp. 67–68). In
health care, we think of autonomy as the right of individuals to make decisions
about what will happen to their bodies (for example, whether or not to have surgery),
what choice will be made among competing options (such as surgery versus medical
management), and what they choose to take or not take into their bodies (for
example, compliance versus noncompliance with prescribed medications). We also
allude to questions of autonomy when we refer to choice among health care
providers (such as physicians, hospitals, and pharmacies) and the choice to refuse
medical treatment (such as decisions about the right to die and assisted suicide)
(McCarthy, 1996b).
There are two ethically justifiable exceptions to the principle of autonomy: weak
paternalism and the harm principle. The concept of medical paternalism is in direct
conflict with the principle of patient autonomy. Medical paternalism suggests that
physicians and other health care professionals—because of their education and
training—know what is best for their patients. As a result, health care professionals
believe they are justified in overriding a patient’s autonomy. Medical paternalism
dominated Western medical practice until the last several decades, when the primacy

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-182-
of patients’ rights and the concept of medical consumerism became recognized.
Nevertheless, a form of medical paternalism, “weak paternalism,” has remained
generally ac-accepted as a justifiable exception to the principle of autonomy. Weak
paternalism allows an individual’s autonomy to be violated if that individual is not
or does not appear to be autonomous, or if minimal intervention is necessary to
determine whether the patient is autonomous. It might be argued that given the stress
caused by his current situation, Leo is not an autonomous individual and is thus
unable to make a rational decision whether to enter a clinical trial or end his life.
Some have argued that weak paternalism is not paternalism. If a person cannot make
an autonomous decision because he or she lacks the capacity to do so, then how can
that individual’s autonomy be overidden? Strong paternalism—the violation of
another’s autonomy because they are making the wrong decision or a decision that
will cause harm to themselves—is not considered an ethically justifiable reason to
override a patient’s autonomy. Consequently, to override Leo’s decision to end his
life based on strong paternalism would be unethical.
Under the harm principle, one is justified in overriding another’s autonomy if, in the
exercise of that autonomy, harm may come to others. In Leo’s situation, one could
argue that he should be prevented from ending his life (i.e., his autonomy should be
overridden) because of the emotional harm such an act would inflict upon his
children.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-183-
Informed Consent
The principle of autonomy is a vital component of informed consent. For example,
when one provides informed consent to an individual contemplating participation in
a clinical research trial, one respects that individual’s right to make an autonomous
decision. The rule of informed consent directs that patients must be fully informed
about the benefits and risks of participating in a clinical trial, taking a medication, or
electing to have surgery; this disclosure is followed by their autonomous consent.
For legal and ethical reasons, informed consent is always obtained through a written
form in situations such as clinical research and surgery. In the case of clinical
research, these documents are usually drafted by the investigator or research sponsor
(e.g., pharmaceutical manufacturer) and subsequently approved by the institutional
review board (IRB) at the institution where the research will take place.
Informed consent is also obtained informally in some instances. For example,
whenever a pharmacist counsels a patient and dispenses a medication to a patient, a
type of informal informed consent is occurring. The patient is informed about the
benefits and risks of the drug and then decides whether or not to take it.
Informed consent is composed of five elements: disclosure, understanding,
voluntariness, competence, and consent (McCarthy, 1996b). Disclosure directs that
all the pertinent information necessary for an informed decision be made available to
the patient. Understanding requires that the patient fully understand what he or she is
consenting to, including any benefits or hazards. Voluntariness instructs that patients

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-184-
must choose to enroll in a research endeavor or be compliant with a medication free
from coercion. (It might be argued that Leo would not be making a voluntary
decision to enroll in the clinical trial given his financial circumstances.) Competence
requires that patients be autonomous individuals, who functionally have the ability
to make decisions for themselves. Consent is the final legal and moral criterion that
must be met in order to ensure that informed consent has been obtained. It provides
the patient with a point of decision.
Confidentiality
The rule of confidentiality, much like informed consent, is an application of the
principle of autonomy. When a health care professional keeps information private
from others, unless given permission to do so by the patient, the professional
respects the individual’s autonomous decision. Medical confidentiality need not be
expressed explicitly by the patient. All medical information, by nature, is generally
considered to be confidential unless released with the patient’s approval.
The terms confidentiality and privacy are often used interchangeably, yet, in
actuality, they are not the same. Confidentiality is the act, by a health care
professional, of keeping information private from others, unless given the
permission to reveal such information by the patient. In contrast, privacy is the act of
keeping information from others who do not have our consent, or even the right, to
access such information. A violation of confidentiality occurs when a health care
professional inappropriately discloses patient information, either purposefully or
accidentally, to others after being given access to such information. A violation of

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-185-
privacy occurs when an individual (e.g., a computer hacker) gains inappropriate
access to private information. Given this distinction, the primary focus of
biomedical ethicists is on confidentiality.
In health care, it is sometimes unclear which members of the health care team
should have access to confidential medical records without express consent of the
patient. Should a pharmacist or physical therapist caring for a patient have the same
access to medical records afforded the patient’s physician or hospital nurse?
Generally, these individuals do have access to such records, absent specific
instructions from the patient or patient’s family that they should not.
Another difficult ethical situation involves a patient who explicitly expresses a
desire not to have information divulged to a member of the health care team. For
example, a patient may divulge to a pharmacist his or her decision to alter a
prescribed therapeutic regimen but request that the pharmacist not disclose this
information to the physician.
Confidentiality has the same two ethically justifiable exceptions as does the
principle of autonomy: the harm principle and weak paternalism. As with autonomy,
a health care professional may be ethically justified in violating a patient’s
confidentiality if, by keeping information private, harm may come to others (harm
principle) or if the patient lacks autonomy (weak paternalism).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-186-
Confidentiality is an example of an ethical precept that has found its way into our
legal system. The Health Insurance Portability and Accountability Act (HIPAA) of
1996, though primarily focused on the portability of employer-based health
insurance, codified health care professionals’ responsibility to maintain patient
confidentiality. The provision of this law relating to the security and privacy of
health information was only fully effective in early 2003 (Giacalone and Cacciatore,
2003). Consequently, the impact of the HIPAA on health care delivery in the United
States is still to be determined. Nevertheless, it is already clear that HIPAA will
dramatically change the way health care professionals handle patient-sensitive
information. The concern is whether HIPPA, while protecting patient confidentiality,
may result in new ethical problems involving limiting access to patient information
that may impair a health care professional’s ability to care for their patient.
Beneficence/Nonmaleficence
Beneficence and nonmaleficence are ethical principles that, in a sense, are
complementary. To act in a beneficent manner indicates that one will act to “do
good” for another. Nonmaleficence refers to “avoiding harm” or “taking due care.”
Beauchamp and Childress compare these related principles:
The word nonmaleficence is sometimes used more broadly to include the prevention
of harm and the removal of harmful conditions. However, because prevention and
removal require positive acts to assist others, we include them under beneficence

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-187-
along with the provision of benefit. Nonmaleficence is restricted . . . to the
noninfliction of harm. (1989, p. 194)
A practical example of the difference between beneficence and nonmaleficence
might be as follows: While driving down the street one day, you notice an elderly
woman crossing the street. Stopping your car to allow her to cross safely is an
example of practicing nonmaleficence, while getting out of your car to assist her
across the street exemplifies beneficence. Similarly, in health care, a pharmacist who
refuses to fill a prescription because of a drug interaction is practicing
nonmaleficence. The same pharmacist contacting the prescriber for an alternative
medication is demonstrating beneficence.
Fidelity
The principle of fidelity requires that health care professionals act in such a way as
to demonstrate loyalty to their patients. A type of bond or promise is established
between the practitioner and the patient. This professional relationship places on the
health professional the burden of acting in the patient’s best interest. Health care
professionals have a fidelity obligation to all their patients, regardless of the length
of the professional relationship. In community pharmacy, for example, practitioners
have the same obligation to show fidelity to an occasional patient as they do to a
“regular” customer (McCarthy, 1996c).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-188-
Ethicists sometimes describe two types of fidelity obligations: contractual and
covenantal. Contractual fidelity is that which occurs as the result of an agreement—
a contract—between two parties. It refers to the obligations that might exist between,
for example, a building contractor and a client or an employer and an employee.
Covenantal fidelity, on the other hand, implies a much deeper or spiritual
commitment such as that which exists between a husband and wife or a member of
the clergy and his congregation. Contractual and covenantal fidelity lie on opposites
end of a continuum. Fidelity obligations may be contractual or covenantal in nature
or may lie some where between the two on the continuum. Where the relationship
between pharmacist and patient falls along the continuum is a point of much
discourse. This is important from a practical perspective when one considers the
level of obligation health care professionals have to their patients. How far should
medical practitioners go to ensure that their patient’s needs and desires are met? In
Leo’s case, what level of fidelity do his physician and other health care professional
have?
Veracity is the ethical principle that instructs practitioners to be honest in their
dealings with patients. There may be times when the violation of veracity is ethically
justifiable (for example, the use of placebos to benefit a patient), but the violation of
this principle for non-patient-centered reasons would appear to be unethical. In a
professional relationship based upon professional fidelity, patients have a right to
expect that health care professionals will be forthright in dealing with them
(McCarthy, 1996c).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-189-
Distributive Justice
Distributive justice refers to the equal distribution of the benefits and burdens of
society among all of society’s members. We often think of distributive justice in
terms of our health care delivery system. This principle is frequently used as a
justification for providing health care as a right to all Americans.
Health professionals do not always provide care with equal fervor to all patients.
Justice instructs health care providers to demonstrate an equivalent amount of care
toward all their patients. Unfortunately, issues such as the patient’s socioeconomic
status often affect the level and intensity of care provided by health care
professionals. Medicaid patients are sometimes provided a much lower quality of
care than cash paying customers or patients who have a “Cadillac” drug benefit plan.
All too often, the care provided by a health care professional is viewed in terms of
the personal reward for the professional—that is, the level of reimbursement that the
care is likely to reap. Justice demands that the health care professional focus on the
patient and his or her medical needs, not on the financial impact on the health care
professional.
As the United States examines the possibility of significantly reforming its health
care system, equal access to quality care for those like Leo and his family must be
the cornerstone of any reform effort (McCarthy, 1996c).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-190-
ETHICAL CODES
Ethical principles that apply to medical practice and research—such as autonomy,
beneficence, and justice—have long served as the basis for a system or code of
ethical conduct. Western medical ethics is primarily based on the Hippocratic code
established by the Greek philosopher Hippocrates in the 5th century B.C. Medicine
(American Medical Association) and pharmacy (Philadelphia College of Pharmacy)
developed codes of conduct for their practitioners in 1847 (American Medical
Association, 2000) and 1848, respectively. As Montagne notes, “The guiding
principles of these codes were a respect for human life and service to humanity”
(1992, p. 303).
The Holocaust during World War II, and the subsequent Nuremberg trials, prompted
the first major development of a code dealing specifically with experimentation on
human subjects. After Nuremberg, several other codes of medical ethics were
established. In 1949, the World Medical Association drafted the Geneva Convention
Code of Medical Ethics, a contemporary version of the Hippocratic Oath. In the
1960s, the same organization established an ethical code on clinical research. The
Declaration of Helsinki was adopted in 1964 (and revised in 1975); this was based
upon the Nuremberg principles (Montagne, 1992). In 1972, the American Hospital
Association issued a “Statement on a Patient’s Bill of Rights.” In 1977, the
Declaration of Hawaii provided ethical guidelines for clinical research in psychiatry
(Montagne, 1992). Nurses are guided by the “Code of Ethics for Nurses,” most
recently revised by the American Nurses Association in 2001. Physicians follow the
“Principles of Medical Ethics,” revised by the American Medical Association in

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-191-
2001. In 1992, the National Association of Boards of Pharmacy issued a revised
“Pharmacy Patient’s Bill of Rights” (Buerki and Vottero, 2002).
These codes provide health care professionals with standards to guide their practice.
However, ethical principles and codes cannot provide health care professionals with
answers to every moral question that may arise in the course of their practice.
Ethical questions in health care involve decision making that is usually situation-
specific. The purpose of such principles and codes is not to provide practitioners
with right and wrong answers but to offer them a framework to use when faced with
ethical questions. As Montagne points out, “The formulation of an oath or ethical
code does not remove the moral choices and the need to carefully consider each
individual situation and the alternative actions or decisions that can be made” (1992,
p. 304).
APhA Code of Ethics
The code of ethics of the American Pharmacists (formerly Pharmaceutical)
Association (APhA) is the only one that specifically guides the practice of pharmacy.
A careful examination of the evolution of the code since its inception in 1852 shows
both a greater degree of responsibility to the patient expected of the pharmacist and
a greater respect for the autonomy of patients.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-192-
The first APhA code reflected the wide acceptance of medical paternalism or the
attitude that the “physician knows best.” In Article 5 of the 1852 code, for example,
is the following:
As physicians are liable to commit errors in writing their prescriptions . . . the
apothecary should always, when he deems an error has been made, consult the
physician before proceeding. . . . It is his duty, when possible to accomplish the
interview without compromising the reputation of the physician. . . . When
apothecaries commit errors . . . the physician . . . should feel bound to screen them
from undue censure, unless the result of a culpable negligence (APhA, 1865, p. 25).
Amazingly, the 1852 code suggests that errors by physicians or pharmacists, unless
made negligently, need not—in fact should not—be revealed to patients.
The 1952 code clearly outlined the duties of a pharmacist, which were quite in
conflict with what is accepted practice today. The preamble begins: “The primary
obligation of pharmacy is the service it can render to the public in safeguarding the
preparation, compounding, and dispensing of drugs and the storage and handling of
drugs and medical supplies” (APhA, 1952, p. 721).
The pharmacist refuses to prescribe or diagnose; he refers those needing such
service to a properly licensed practitioner. . . . The pharmacist does not discuss the
therapeutic effects or composition of a prescription with a patient. When such
questions are asked, he suggests that the qualified practitioner is the proper person
with whom such matters should be discussed (APhA, 1952, p. 722).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-193-
By the 1969 revision, the code was significantly shorter, enabling it to be placed on
a placard suitable for display in pharmacies. The 1981 code was gender neutral; “he”
was replaced by “a pharmacist.”
The 1994 code, much less prescriptive than earlier versions, speaks to the
“covenantal relationship between the patient and the pharmacist” and the obligation
of pharmacists to promote “the good of every patient in a caring . . . manner” (APhA,
1995, p. 2131). The elements of pharmaceutical care appear throughout and are
consistent with the new mission of pharmacy (see Exhibit 7–2; see Chapter 3).
ETHICAL ISSUES IN HEALTH CARE
Law and Ethics
Many of the laws, regulations, and other rules that govern our daily life are an
outgrowth of our morality and ethics. Laws that prohibit homicide, robbery, and
similar offenses are simply a codification of the values we share as members of
society. Unfortunately, laws and regulations cannot be promulgated to cover every
eventuality, nuance, condition, or situation. They are created in such a way as to
provide legal guidelines for the “usual” or “most common” situation. What should
be done, then, when the legal course of action is inconsistent with the ethical course
of action (for example, when a person commits homicide in self-defense)?

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-194-
Conflicts of this kind occur routinely in medicine. For example, what should a
pharmacist do when a patient’s prescription for heart medicine has been depleted, no
refills remain, and the prescriber is unavailable? Clearly, most pharmacists would do
the ethical thing and provide the patient with a few doses to hold the patient over
until a new prescription can be obtained, even though this course of action is illegal.
To follow the example a bit further, what if the medication is a controlled substance
used for pain control in a terminally ill patient? A pharmacist might be more
reluctant to dispense a few doses, even though the patient might be in just as much
need, due to potential legal ramifications from drug enforcement authorities.
Rationing
As the cost of providing health care services continues to grow, some have
suggested and even attempted to implement a system that would ration the
availability of health care (for example, the Oregon Plan). American health care
policy makers have tried to avoid this approach because it contradicts a long-
standing implicit belief that all that can be done for each patient ought to be done.
Medical insurance providers, both publicly and privately funded, have attempted to
support this traditional ideal. But the lack of cost containment has resulted in rising
insurance rates, thereby driving individuals out of the health insurance system and
threatening the viability of governmental programs.
The consequence of this policy is seen in increasing numbers of individuals who are
unable to afford health insurance. Fewer people have access to health care and

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-195-
others have decreased choices of where they can receive health care (such as
municipal hospitals, free clinics). As McDermott points out:
Approximately 15% of our people [Americans] have no health insurance coverage at
any one time, and at least 57 million nonelderly Americans lack health insurance for
some part of the year. This does not even include the underinsured and those on
Medicaid whose coverage cannot begin to provide them with access that is
consistent with good health care (1994, p. 782).
As a result, the United States may not in theory ration health care, but in practice it
certainly does. As Light argues in reference to the arbitrary way private insurance
companies often make coverage decisions:
Surely, criteria for rationing should be developed openly and with fairness to all. So
far, the American health care system has relied on myriad private companies to
make not only these decisions but also related ones on the use of resources, using
hundreds of proprietary systems with different forms and different, unsubstantiated
methods (1994, p. 498).
For at least the present, most American health care planners have determined that
rationing of care, in any manner, is not a viable alternative for dealing with our
current crisis. At the same time, however, there is a shared determination by the
government and the public at large that reform is essential and that whatever
changes are made must ensure universal access to health care while controlling costs

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-196-
and reducing fraud (you will recall the discussion of distributive justice and equal
access to health care earlier in this chapter). As Friedman notes, “High health care
costs breed medical indigence; if one is to be fixed, so must the other” (1993, p.
2438).
Assisted Suicide
Although medical euthanasia (“mercy killing”) has long been an ethical issue, it has
only been in recent years that the question of assisted suicide has been examined.
The activities of Dr. Jack Kevorkian (frequently referred to as “Dr. Death” for his
activities assisting terminally and chronically ill patients to end their life) have
spurred a great deal of public and professional discussion of this issue. Several states
have considered the legality of assisted suicide. Some have rejected it (Washington),
while others have accepted it within strict guidelines (Oregon). In 1997, the U.S.
Supreme Court ruled that assisted suicide is nota constitutionally granted right,
while upholding state laws in New York and Washington banning the practice.
However, the Court left to individual states the option of legalizing assisted suicide.
From an ethical perspective, the key issue remains whether assisted suicide violates
the Hippocratic responsibilities of health care practitioners to “do no harm.” Those
who advocate its availability to patients suggest that allowing a patient to continue
to experience unrelenting pain is to do harm. They suggest that patients have the
right to make an autonomous decision to end their life; opponents worry that legal
assisted suicide would be abused (such as might be the case with Leo).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-197-
Human Drug Experimentation
As discussed earlier, a number of ethical codes have been established by the medical
community since 1945. Several of these codes deal with research on human subjects,
including the testing of drugs. Two important ethical aspects of human drug
experimentation are the role of the institutional review board (IRB) and the use of
placebos.
The IRB is the body responsible for overseeing all clinical research conducted
within a given institution. Traditionally, most clinical drug research was conducted
in hospital settings. However, with the shift in the locus of health care delivery from
the inpatient to the ambulatory setting, IRBs are now found in managed care
organizations and other ambulatory facilities. The IRB has two primary
responsibilities. The first is to ensure the integrity and scientific rigor of the
proposed research study. The IRB evaluates risks versus benefits to study
participants. If the risks outweigh benefits, the IRB would likely reject the proposal.
The board acts as somewhat of a “subject advocate” to ensure that the patient-
subject’s rights and welfare are protected (Gallelli, Hiranaka, and Grimes, 1986, p.
487). The IRB’s second major responsibility is to evaluate and approve informed
consent forms used in conjunction with the research? Such forms should be drafted
in a manner consistent with the elements of informed consent discussed previously.
IRBs vary in their size and representation. Their membership may include
physicians, nurses, other allied health professionals (including pharmacists),

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-198-
institutional administrators, attorneys, clergy, medical ethicists, and community
members (McCarthy, 1996b).
Placebos have generally had two roles in medicine: (1) in clinical drug research, and
(2) as a means of decreasing the dose of or weaning a patient off a drug to which a
patient has become dependent. The use of placebos has long been an integral
component of clinical drug research. Whether the drug being tested is a new drug
compound or an existing drug under study for a new indication, placebos have
served as a point of comparison for determining therapeutic efficacy. Although the
use of placebos in some instances has been shown to provide therapeutic usefulness
(such as for pain control), placebos—by definition—are agents devoid of
pharmacologic activity. Patient-subjects who receive placebos as a component of
their participation in a clinical drug study can generally not hope to derive any
benefit (beneficence) from these substances. This raises the question of whether the
use of placebos in drug research, despite the obvious scientific advantages, is ethical.
This question is further complicated by the expectation that placebos will be
employed in clinical research. A Food and Drug Administration regulator has stated:
“It is desirable to include some placebo controlled studies unless it is considered
unethical to do so” (Freedman, 1990, p. 2). This suggests that the use of placebos is
ethical in certain instances but unethical in others (McCarthy, 1996b). In a meeting
in the fall of 2000, representatives of the World Medical Association approved a
change in the 1964 Declaration of Helsinki stating “that the use of placebos in
medical experiments is unethical when treatments are available for the diseases that

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-199-
are under study” (McMillen, 2000). Though this action does not have legal force in
the United States, it does carry considerable ethical weight worldwide.
The use of placebos to address genuine or perceived dependence is even more
ethically problematic. The belief that the health care practitioner knows best and,
therefore, is justified in practicing medical paternalism has been a long-standing
component of the “medical authority” model of practice. Under this model, the
patient’s perceptions and desires are subjugated to the judgment of the health care
professional. This type of thinking would be used, for example, as justification for a
practitioner to shift a patient judged to be drug dependent to a placebo without the
patient’s knowledge. Today, such use of placebos with-out patient knowledge and
consent might be judged to be un-ethical—a direct violation of patient autonomy
and informed consent.
Drug Formularies
A drug formulary is a list of drugs that are approved for use either within an
institution (such as a hospital) or for reimbursement by a third-party payer. Its
purpose is to eliminate therapeutic duplication and provide patients with the best
drug at the lowest cost (see Chapter 22). In their early days, formularies were used
by hospitals to control drug inventories and provide prescribers with a list of “drugs
of choice” for various conditions. However, a drug’s absence from the formulary
was not usually a great barrier to a prescriber’s obtaining it for a patient. The

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-200-
prescriber could make a special request to a member of the hospital’s pharmacy and
therapeutics committee and, usually, the drug would be obtained.
When managed care organizations and pharmacy benefit management companies
began to employ formularies, circumventing them became much more difficult. This
restrictive nature of formularies has led to a number of important ethical questions.
For example, does the use of generics or therapeutic substitution violate the
autonomy of the patient or prescriber? Is the use of such substitution a violation of
informed consent? Does the use of formularies violate the ethical principles of
beneficence (“do good”) and nonmaleficence (“avoid harm”) (McCarthy, 1996a)?
However, one could argue that the use of formularies and the resultant constraint on
drug costs helps to ensure affordable access to quality health care for more people
(distributive justice).

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-201-
REFERENCES
A. Catlin et al., “National Health Spending in 2005: The Slowdown
Continues,” Health Affairs 26, no. 1 (2007): 142–153. Aaker, J. L., Williams, P. (1998). Empathy versus pride: The influence of emotional
appeals across cultures. Journal of Consumer Research, 25(3), 241-261. Aday, L. A. (1996). Designing and conducting health surveys (2nd ed.). San
Francisco: Jossey-Bass. Ahmed, R. R., & Jalees, T. (2008). Pharmaceutical Industry in Pakistan: Unethical
Pharmaceutical Marketing Practices. Market Forces-Journal of Management Thoughts, 4(2): 30-39.
American College of Physicians. (1990). Physicians and the pharmaceutical industry.
Annals of Internal Medicine, 112, 392-394. American Medical Association. (1991). Council on Ethical and Judicial Affairs.
Gifts to physicians from the industry. JAMA, 265, 501. American Medical Association. (1995-2002). Council on Ethical and Judicial
Affairs. Ethical guidelines for gifts to physicians from the industry. Retrieved February 13, 2002 from: http://www.ama-assn.org/ama/pub/printcat/5689.html
Avorn, J., Chen, M., & Hartley, R. (1982). Scientific versus commercial sources of
influence on prescribing behaviors of physicians. American Journal of Medicine, 73(1), 4-8.
Bar-On, R., Parker, J. D. (Ed.). (2000). The handbook of emotional intelligence. San
Francisco: Jossey-Bass. Berenson, R. A., & Pollack, A. (2007). Doctors reap millions for anemia drugs. New
York Times. Retrieved February 16, 2010 from http://www.nytimes.com/2007/05/09business/09anemia.html
Bodenheimer, T. (2000). Uneasy alliance: clinical investigators and the
pharmaceutical industry. N England J. Med, 342: 1539-1544. Boseley, S. (2006). Drug firms a danger to health – report. The Guardian, 26th June. Bowman, M. A., & Pearle, D. L. (1988). Changes in drug prescribing patterns
related to commercial company funding of continuing medical education. Journal of Continuing Education Health Professions, 8(1), 13-20.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-202-
Brennan, TA., Rothman, DJ., Blank, L., Blumenthal, D., Chimonas, SC., Cohen, JJ., Goldman, J, Kassirer, JP., Kimball, H., Naughton, J., Smelser, N. (2006). Health industry practices that create conflicts of interest, Journal of the American Medical Association, 295 (4); 429-433.
Campbell, E., Gruen, R., Mountford, J., Miller, L., Cleary, P., & Blumentahl, M.
(2007). A National Survey of Physician –Industry Relationships. N England. J. Med, 356:17.
Chew, L. D., O’Young, T.S., Hazlet, T. K., Bradley, K. A., Maynard, C., & Lessler,
D. S. (2000). A Physician Survey of the Effect of Drug Sample availability on Physicians' Behavior. Journal of General Internal Medicine, 15, 478-483.
Coleman, J., Katz, E., Menzel, H. (1968). Doctors and new drugs. New York: The
Free Press of Glencoe. Coyle, S. L. (2002a). Ethics and Human Rights Committee, American College of
Physicians-American Society of Internal Medicine. Position Paper: Physician-industry relations. Part 1: Individual physicians. Annals of Internal Medicine, 136 (5), 396-402.
Coyle, S. L. (2002b). Ethics and Human Rights Committee, American College of
Physicians-American Society of Internal Medicine. Position Paper: Physician-industry relations. Part 2: Organizational issues. Annals of Internal Medicine, 136 (5), 403-406.
Curcura, P. J. (1999). Stop saying “dinner meetings” it’s peer selling and it’s a
science. Medical Marketing and Media, 34(12), 92-100. Daniella, A., & Michael. A. (2005). Interactions between Pharmaceutical
Representatives and Doctors in Training. J Gen Intern Med, 20(8): 777–786. Fisher, S., Bryant, SG., Kent, TA. (1993). Post marketing surveillance by patient
self-monitoring: trazodone versus fluoxetine. J Clin Psychopharmacology, 13:235-242.
Frederick S., et al. (2005). Medical Students’ Exposure to and Attitudes About Drug
Company Interactions. JAMA, 294(9): 1034-1042. Gibbons, R. V., Landry, F. J., Blouch, D. L., Jones, D. L., Williams, F. K., Lucey, C.
R. et al. (1998). A comparison of physicians' and patients' attitudes toward pharmaceutical industry gifts. J Gen Intern Medicine, 13: 151-154.
Giri, BR., Shankar, PR. (2005). Learning How Drug Companies Promote Medicines
in Nepal. PLoS Med 2(8): e256.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-203-
Gonul, F. F., Carter, F., Petrova, E., & Srinivasan, K. (2001). Promotion of prescription drugs and its impact on physician’s choice behaviors. Journal of Marketing, 65: 79-90.
Greene, J. (1999). Concern raised over increasing role of non-physicians. American
Medical News (December 6). Retrieved January 21, 2002 from: http://www.ama-assn.org
Greene, J. (2000). Drug reps targeting non-physicians. American Medical News
(March 27). Retrieved January 21, 2002 from: http://www.ama-assn.org Harris, G. (2004). As doctors write prescriptions, drug company writes a check. New
York Times, June 27, 2004. Retrieved July 2, 2004 from: http://www.nytimes.com/2004/06/27/business/27DRUG.final.html?ex=1089337894&ei=1&en=c0877fb1c152b62
Haxby, D. G., Rodriguez, G. S., Zenchnich, A. D., Schuff, R. A., Tanigawa, J. S.
(1995). Manufacturers’ distribution of drug samples to a family medicine clinic. American Journal of Health Systems Pharmacology, 52: 496-499.
Healthy Skepticism (2002). About Healthy Skepticism Inc. Retrieved June 21, 2002
from: http://www.healthyskepticism.org/index.htm . Hemminki, E. (1975). Review of literature on the factors affecting drug prescribing.
Soc Sci Med, 9: 111-115. Hodges, B. (1995). Interactions with the pharmaceutical industry: Experiences and
attitudes of psychiatry interns, residents and clerks. Canadian Medical Association Journal, 153, 553-559.
Holmer, A. F. (1999). Direct-to-consumer prescription drug advertising builds
bridges between patients and physicians. JAMA, 281(3): 380-382. Holmes, D.R., Firth, B.G., James, A., Winslow, R., Hodgson, P.K., Gamble G.
(2008). Evolving changes in medical device evaluation. Catheter Cardiovasc Intrv, 72(1): 1-6. https://ironclad.secure-orders.net/nofreelu/pledge.htm
IMS Health. (2002). Free pharmaceutical sample distribution. Retrieved June 24,
2002 from: http://www.ims-global.com/cgi Ingelfinger, F. J. (1972). Advertising: informational but not educational. New
England Journal of Medicine, 286: 1318-1319. Kessenich, C. R., Westbrook, M. H. (1999). Pharmaceutical companies and the
prescriptive practices of nurse practitioners. Journal of the American Academy of Nurse Practitioners, 11 (12): 533-538.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-204-
Lane, R. D. (2000). Levels of emotional awareness. In R. Bar-On & J. D. A. Parker. (Ed.),The handbook of emotional intelligence (pp. 171-191). San Francisco: Jossey-Bass.
Lexchin J. (1995). Deception by design: pharmaceutical promotion in the third
world. Consumers International, Malaysia. Lexchin, J. (1992). Pharmaceutical promotion in the third world. Journal of Drug
Issues, 22(2):417-422. Lidstone, J., and MacLennan, J. (1999). Marketing Planning for the Pharmaceutical.
Industry (2nd ed). Gower Publishing: United Kingdom. Lurie, N., Rich, E. C., & Simpson, D. E. (1990). Pharmaceutical representatives in
academic medical centers: Interaction with faculty and housestaff. Journal of General Internal Medicine, 5: 240-243.
Manning, R. & Keith, A. (2001). The economics of direct-to-consumer advertising
of prescription drugs. In Manning, R. L. & Masia, N. A. (Eds.) Economic Realities in Health Care Policy, 2 (1), 10-15. Retrieved May 13, 2002 from: http://www.Pfizer.com/pfizerinc/policy/Erhealthcare.pdf .
Manning, R. L. & Masia, N. A. (Eds.) (2001). Economic Realities in Health Care
Policy, 2 (1), 10-15. Retrieved May 13, 2002 from: http://www.Pfizer.com/pfizerinc/policy/Erhealthcare.pdf .
Mathieu MP, editor. Parexel’s pharmaceutical R & D statistical sourcebook 1998.
Waltham, Massachusetts: Parexel International Corporation, 1999. Mintzes, B. (1998). Blurring the boundaries: new trends in drug promotion.
Amsterdam: HAI-Europe. Retrieved February 1, 2003 from: http://www.haiweb.org/pubs/blurring/blurring.intro.html .
Mintzes, B., Barer, M. L., Kravitz, R. L., Kazanjian, A., Bassett, K., Lexchin, J. et al.
(2002). Influence of direct to consumer pharmaceutical advertising and patients’ requests on prescribing decisions: two sites cross sectional survey. British Medical Journal, 324, 278-279.
Mixed Reaction to Consumer Advertising. (2003, March). Clinician News, 7(2), 13. Murray, D. (2002, October 11). Gifts what’s all the fuss about? Medical Economics,
79 (9), 119-120. National Institute for Health Care Management. (2001, November). Advertised
prescription drugs are the hottest sellers. Washington, DC: Mahoney, A., Findlay, S. Retrieved February 15, 2003 from: http://nihcm.org/DTC2001PR.html .

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-205-
National Institute for Health Care Management. (2002, May). Prescription drug expenditures in 2001: Another year of escalating costs. Washington, DC: Research and Educational Foundation. Available from: http://www.nihcm.org/spending2001.pdf .
Nishtar, S. (2007). Politics of health systems: WHO's new frontier. LANCET, 15;
370(9591): 935-6. No Free Lunch (2002b). Take the Pledge. Retrieved September 15, 2002 from: No Free Lunch (2002a). About Us. Retrieved September 15, 2002 from:
http://www.nofreelunch.org/aboutus.htm Pakistani pharmaceutical industry. (2010). Information of Medical Statistics, 2nd
Issue, 2: 22-33. Pakistani pharmaceutical industry. (2010). Information of Medical Statistics, 3rd
Issue, 3: 20-31. Parmar, V., & Jalees, T. (2004). Pharmaceutical Industry in Hyderabad, Unethical
Practices in Drug Promotion, Independent Study for MS, Shaheed Zulfiqar Ali Bhutto Institute of Science & Technology, Karachi, May.
Paul A. Komesaroff and Ian H. Kerridge. (2002). Ethical issues concerning the
relationships between medical practitioners and the pharmaceutical industry. Med J. Aust, 176 (3): 118-121
Pearson, L. (2002) Legislative Update. Nurse Practitioner, 27(1): 10-30. Perry, K. (1995). Why patients love physician extenders. Medical Economics,
August 21, 1995, 58-67. Petty, R. E., Cacioppo, J. T. (1985) Processes of social influence: The Elaboration
Likelihood model of persuasion. [Chapter] Kendall, Philip C (Ed). (1985). Advances in cognitive-behavioral research and therapy, Vol. 4. Advances in cognitive-behavioral research and therapy. (pp. 215-274). San Diego, CA, Academic Press, Inc.
Phatak, A. (1998). The pharmaceutical industry and the medical profession. Indian
Journal of Medical Ethics, Oct-Dec, 6 (4): 131-2. PhRMA (2002b). PhRMA Code on Interactions with Healthcare Professionals.
Washington, D.C.: Authors. PhRMA. (2002a). Media Room Press Release, April 19, 2002. PhRMA adopts new
marketing code. Retrieved October 16, 2002 from: http://www.phrma.org/mediaroom/press/releases/19.04.2002.390.cfm .

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-206-
Pinkerton, J., & Bush, H. (2000). Nurse practitioners and physicians: Patients’ perceived health and satisfaction with care. Journal of the American Academy of Nurse Practitioners, 12(6): 211-217.
Poor judgment in spite of high intellect: Neurological evidence for emotional
intelligence. In Bar-On, R., Parker, J. D. (Ed.). (2000). The handbook of emotional intelligence. San Francisco: Jossey-Bass, pp192-214.
Popp, R.L., Harrington. R.A. (2004). Conflict of interest, American Heart Journal,
147(2): 228-237. Pulcini, J., & Vampola, M. A. (2000). NPACE nurse practitioner practice
characteristics, salary, and benefits survey: 1999. Clinical Excellence for Nurse Practitioners, 4(6): 366-372.
Pulliam, L. (1991). Client satisfaction with a nurse-managed clinic. Journal of
Community Health Nursing, 8(2): 97-112. Sandberg, W. S., Carlos, R., Sandberg, E. H., Roizen, M. F. (1997). The effect of
educational gifts from pharmaceutical firms on medical students’ recall of company names and products. Academic Medicine, 72: 916-918.
Sharpe, V.A. (2002). Science, bioethics, and the public trust, Hastings Center
Report, 32(3): 23-26. Sibbald, H. (2004). Legal action against GSK over SSRI data CMAJ, July 6; 171(1):
23.doi: 10.1503/cmaj.1040982. Socolar, D., Sager, A. (2001, October). Pharmaceutical marketing and research
spending: The evidence does not support PhRMA’s claims. Paper presented at American Public Health Association Annual Meeting (session 2018.0), Atlanta, GA.
Steinman, M. A., Shlipak, M. G., & McPhee, S. J. (2001). Of principles and pens:
Attitudes and practices of medical house staff toward pharmaceutical industry promotions. The American Journal of Medicine, 110, 551-557.
Stolberg, S. G., & Gerth, J. (2000, November 16). High tech stealth being used to
sway doctor prescriptions. New York Times. From http://nytimes.com/2000/11/16/science/16PRES.html
T. Brennan et al. (2006). Health industry practices that create conflicts of interest.
JAMA, 295(4): 429-433. Tomlinson, H. (2004). AstraZeneca sued for ulcer drug profits. The Guardian, 24
November.

© GRIN Verlag GmbH All content copyright restricted. Copying and distribution prohibited
http://www.grin.com
-207-
Tutor2u. (2004). Buyer Behavior - Stimulus-Response Model. Retived June 25, 2004 from: http://www.tutor2u.net/business/marketing/buying_stimulus_model.asp.
Wang, T. J., Ausiello, J. C., & Stafford, R. S. (1999). Trends in antihypertensive
drug advertising, 1985-1996. Circulation, 99(15), 2055-2057. Waud, D. R. (1992). Pharmaceutical promotions-a free lunch? New England Journal
of Medicine, 327, 351-353. Wazana, A. (2000). Physicians and the Pharmaceutical Industry: Is a gift ever just a
gift? JAMA, 283(3), 373-80. Wazana, A. (2000). Physicians and the pharmaceutical industry: is a gift ever just a
gift? JAMA, 283(3), 373-80. Westfall, J. M., McCabe, H., & Nicholas, R. A. (1997). Personal use of drug
samples by physicians and office staff. JAMA, 278:141-143. Westfall, J. M., McCabe, H., & Nicholas, R. A. (1998). Reply to Drug samples:
Benefit or bait? JAMA, 279(21), 169-1699. Willimack, D. K., Schuman, H., Pennell, B. E., & Lepkowski, J. M. (1995). Effects
of pre-paid non-monetary incentive on response rates and response quality in a face-to-face survey. Public Opinion Quarterly, 59, 78-92.
Wolf, B. (1998). Drug samples: Benefit or bait? JAMA, 279(21), 1698-1699. Wolfe, S. M. (2002). Direct-to-consumer advertising – Education or emotion
promotion? New England Journal of Medicine, 346(7), 524-526. Zaidi, SH., Niaz, U., Jafary, MH., & Jawaid SA. (1995). Medical Ethics in the
Contemporary Era. (Eds) Pakistan Medical Journalists Association, Karachi, Pakistan.
Ziegler, M. G., Lew, P., & Singer, B. C. (1995). The accuracy of drug information
from pharmaceutical sales representatives. JAMA, 27, 1296-1298.
Related Documents











