Confidential: For Review Only International multicentre prospective study comparing risk- scoring systems for patients presenting with upper gastrointestinal bleeding Journal: BMJ Manuscript ID BMJ.2016.033358 Article Type: Research BMJ Journal: BMJ Date Submitted by the Author: 07-May-2016 Complete List of Authors: Stanley, Adrian; Glasgow Royal Infirmary, GI Unit Laine, Loren; Yale University School of Medicine, Digestive Diseases Dalton, Harry; Royal Cornwall Hospital, Gastroenterology Ngu, Jing; Singapore General Hospital Schultz, Michael; University of Otago Dunedin School of Medicine Abazi, Rozeta; Odense University Hospital, Department of Gastroenterology and Hepatology Zakko, Liam; Yale University School of Medicine, Digestive Diseases Thornton, Susan; Glasgow Royal Infirmary, GI Unit Wilkinson, Kelly; Royal Cornwall Hospital, Gastroenterology Khor, Cristopher; Singapore General Hospital Murray, Iain; Royal Cornwall Hospital, Gastroenterology Laursen, Stig; Odense University Hospital, Department of Gastroenterology and Hepatology Dunne, Philip; Glasgow Royal Infirmary, GI Unit Fleming, Jude; Glasgow Royal Infirmary, GI Unit Holloway, Amelia; Royal Cornwall Hospital, Gastroenterology Froud, Oliver; Royal Cornwall Hospital, Gastroenterology Sutton, J; Royal Cornwall Hospital, Gastroenterology Michell, Nick; Royal Cornwall Hospital, Gastroenterology Pinchin, Emily; Royal Cornwall Hospital, Gastroenterology Ong, Hock; Singapore General Hospital Chin, Yung; Singapore General Hospital Koay, Doreen; Singapore General Hospital Steiner, Tracey; Dunedin Hospital Keywords: Upper Gastrointestinal bleeding, risk score, Glasgow Blatchford score, Rockall score, AIMS65, PNED https://mc.manuscriptcentral.com/bmj BMJ

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Confidential: For Review O
nly
International multicentre prospective study comparing risk-
scoring systems for patients presenting with upper gastrointestinal bleeding
Journal: BMJ
Manuscript ID BMJ.2016.033358
Article Type: Research
BMJ Journal: BMJ
Date Submitted by the Author: 07-May-2016
Complete List of Authors: Stanley, Adrian; Glasgow Royal Infirmary, GI Unit Laine, Loren; Yale University School of Medicine, Digestive Diseases Dalton, Harry; Royal Cornwall Hospital, Gastroenterology Ngu, Jing; Singapore General Hospital Schultz, Michael; University of Otago Dunedin School of Medicine Abazi, Rozeta; Odense University Hospital, Department of Gastroenterology and Hepatology Zakko, Liam; Yale University School of Medicine, Digestive Diseases Thornton, Susan; Glasgow Royal Infirmary, GI Unit Wilkinson, Kelly; Royal Cornwall Hospital, Gastroenterology Khor, Cristopher; Singapore General Hospital Murray, Iain; Royal Cornwall Hospital, Gastroenterology
Laursen, Stig; Odense University Hospital, Department of Gastroenterology and Hepatology Dunne, Philip; Glasgow Royal Infirmary, GI Unit Fleming, Jude; Glasgow Royal Infirmary, GI Unit Holloway, Amelia; Royal Cornwall Hospital, Gastroenterology Froud, Oliver; Royal Cornwall Hospital, Gastroenterology Sutton, J; Royal Cornwall Hospital, Gastroenterology Michell, Nick; Royal Cornwall Hospital, Gastroenterology Pinchin, Emily; Royal Cornwall Hospital, Gastroenterology Ong, Hock; Singapore General Hospital Chin, Yung; Singapore General Hospital Koay, Doreen; Singapore General Hospital
Steiner, Tracey; Dunedin Hospital
Keywords: Upper Gastrointestinal bleeding, risk score, Glasgow Blatchford score, Rockall score, AIMS65, PNED
https://mc.manuscriptcentral.com/bmj
BMJ

Confidential: For Review O
nly
Page 1 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyInternational multicentre prospective study comparing risk-scoring
systems for patients presenting with upper gastrointestinal bleeding
A J Stanley (Consultant Gastroenterologist)1, L Laine (Professor of Medicine)2, H R
Dalton (Consultant Gastroenterologist)3, J H Ngu (Consultant
Gastroenterologist)4, M Schultz (Associate Professor of Gastroenterology)5,7, R
Abazi (Consultant Gastroenterologist)6, L Zakko (Fellow in Gastroenterology)2, S
Thornton (Research nurse)1, K Wilkinson (Medical student)3, CJL Khor
(Consultant Gastroenterologist)4, IA Murray (Consultant Gastroenterologist)3, SB
Laursen (Postdoctoral researcher in Gastroenterology)6
on behalf of the International GI bleeding consortium (listed below*)
1. Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK
2. Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA
Connecticut Healthcare System, West Haven, Connecticut, USA
3. Gastrointestinal Unit, Royal Cornwall Hospital, Cornwall, UK
4. Department of Gastroenterology & Hepatology, Singapore General Hospital,
Singapore
5. Department of Medicine, Dunedin School of Medicine, University of Otago,
Dunedin, New Zealand
6. Department of Medical Gastroenterology, Odense University Hospital, Odense,
Denmark
7. Gastroenterology Unit, Southern District Health Board, Dunedin Hospital,
Dunedin, New Zealand
Page 2 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
2
*International GI bleeding consortium:
P Dunne1, J Fleming1, A Holloway3, O Froud3, J Sutton3, N Michell3, E Pinchin3, HS
Ong4, YK Chin4, DS Koay4, T Steiner7,
Correspondence to:
Dr Adrian J Stanley,
Consultant Gastroenterologist
Glasgow Royal Infirmary,
Castle St, Glasgow, UK,
G4 OSF
Ph: +44 141 211 4073
Email: [email protected] and [email protected]
Page 3 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
3
Abstract
Objectives: To compare the predictive accuracy and clinical utility of five risk
scoring systems in the assessment of patients presenting with upper
gastrointestinal bleeding (UGIB).
Design & setting: Consecutive patients with UGIB presenting to six large
hospitals in Europe, North America, Asia and Oceania over 12 months were
included. Prospective data were collected to calculate and compare the pre-
endoscopy scores: admission Rockall score (ARS), AIMS65 and Glasgow
Blatchford score (GBS); and the post-endoscopy scores: full Rockall score (FRS)
and PNED.
Participants & main outcome measures: 3012 patients were included. The scores
were compared in their ability to predict pre-defined clinical endpoints:
combined need for intervention or death, endoscopic therapy, mortality,
rebleeding, and length of hospital stay. Optimum score thresholds to identify
low- and high-risk patients were determined.
Results: GBS was best (AUROC=0·89) at predicting intervention or death
compared with PNED (0·71), AIMS65 (0·70), FRS (0·69) or ARS (0·69) (all
P<0·0001). GBS≤1 was the optimum threshold to predict survival without
intervention (sensitivity=98·6%, specificity=34·6%). GBS was better at
predicting endoscopic therapy (AUROC=0·75) than AIMS65 (0·63) and ARS
(0·61) (both P<0·0001). GBS≥7 was the optimum threshold to predict
endoscopic therapy (sensitivity=80%, specificity=57%). PNED (AUROC=0·79)
Page 4 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
4
and AIMS65 (0·78) were best at predicting mortality, with PNED superior to ARS
(0·76), FRS (0·72) (both P<0·05), and GBS (0·69; p<0·0001). Score thresholds of
PNED ≥4, AIMS65 ≥2, ARS ≥4, and FRS ≥5 were optimal at predicting death with
sensitivities 65·8-78·6% and specificities 65·0-65·3%. No score was helpful at
predicting rebleeding or length of stay.
Conclusions: GBS has high accuracy at predicting need for hospital-based
intervention or death. GBS≤1 appears the optimum threshold for directing
patients to outpatient management. AUROCs of scores for the other end-points
are <0·80, therefore their clinical utility for these outcomes appears limited.
Trial registration: The study was registered with ISRCTN (reference no.
16235737)
Funding: Data collection in Glasgow, Singapore and Dunedin was funded by a
Health Board endowment, Hospital Research and guthealthnetwork grant
respectively. The funders had no input to the study design, data collection or
interpretation, writing of report or submission for publication
Page 5 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
5
What is already known on this subject?
Several pre- and post-endoscopy risk scores have been reported to predict a
variety of endpoints in patients presenting with upper GI bleeding. Directing
patient care to outpatient management, or urgent endoscopy and higher-level
care, using low and high scores respectively on presentation has been suggested.
However the accuracy and generalizability, and the optimum thresholds of
scores to predict low and high-risk patients which may help direct care remain
unclear.
What this study adds
This international study suggests that the GBS is accurate (AUROC=0.89) in
predicting need for intervention or death at all centres, with GBS≤1 the optimal
threshold for directing low-risk patients to outpatient management with
sensitivity 98·6%, specificity 34·6%, PPV 96.6% and NPV 56.0%. All scores have
low predictive accuracy for other specific outcomes including endoscopic
therapy and mortality, therefore their clinical utility to direct management of
high-risk patients appears limited.
Widespread use of GBS in Emergency Departments of many countries may allow
a large minority of patients with upper GI bleeding to be safely managed as
outpatients.
Page 6 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
6
Introduction
Upper gastrointestinal bleeding (UGIB) is a common cause of admission to
hospital worldwide, with a UK incidence of 103-172 per 100 000 adults per year
and mortality of 8-14%.1-3 Many risk assessment scores have been developed to
predict clinically relevant outcomes, including mortality, need for hospital-based
intervention, rebleeding, and length of hospital stay.4-9 Several of these including
the Rockall score and recently described Progetto Nazionale Emorragia Digestive
(PNED) score require endoscopy before calculation.4,5 The Rockall score has
been widely reported and it has been suggested that PNED is superior to the
Rockall score, although it has not been externally validated.5 Other endoscopy-
based scores have been described, but are not appropriate for unselected
patients with UGIB, have not been externally validated, or have been shown to be
inferior to the scores above.10 However requiring endoscopy to calculate a score
may delay risk assessment in some healthcare settings, as there can be
significant delays in performing endoscopy out-of-hours or on weekends.11
There has been much recent interest in pre-endoscopic risk scores for UGIB,
which can be calculated shortly after presentation to hospital. The most widely
studied pre-endoscopic scores are the abbreviated “admission” Rockall score
(ARS), the Glasgow-Blatchford score (GBS) and the recently described AIMS65
score.7,8 These use clinical, haemodynamic and (for the latter two) readily
available laboratory parameters. It has been suggested that these scores can be
used to identify very low risk patients who could be managed as outpatients.12-18
Studies have also suggested these scores could identify higher risk patients who
Page 7 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
7
may require urgent endoscopy or management in high dependency or intensive
care units.19-20
Several studies have compared scores in their ability to predict various
outcomes.12,21-23 Although GBS appears useful in identifying very low-risk patient
in the UK, many studies have been small and single centre and no international
study has compared all the commonly used scores. The aim of this prospective
international study was to compare five endoscopic and pre-endoscopic risk
assessment scores in their ability to predict clinically relevant endpoints. In
addition, we assessed the clinical utility of these scores, by determining optimal
thresholds for identifying very low risk patients who could be managed as
outpatients, and higher risk patients who may require specific management
strategies aimed at improving outcome.
Page 8 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
8
Methods
The study was undertaken in Yale-New Haven Hospital (USA), Glasgow Royal
Infirmary (Scotland UK), Royal Cornwall Hospital Truro (England UK), Odense
University Hospital (Denmark), Singapore General Hospital (Singapore) and
Dunedin Hospital (New Zealand). Ethical approval was obtained from West of
Scotland Ethics committee (reference 14/WS/0012; project number: 145837)
and each centre obtained approval from their local research committee or
review board. Due to the observational, non-interventional nature of the study,
the ethical committee (and local committees and boards) agreed that individual
patient consent was not required. The sponsor was NHS Greater Glasgow and
Clyde Health Board, Scotland, UK.
The predetermined clinical endpoints were:
1. combined outcome of need for hospital-based intervention (red blood cell
transfusion, endoscopic therapy, interventional radiology or surgery) or death; 2.
endoscopic therapy; 3. 30-day mortality; 4. rebleeding within 7 days; 5. length of
hospital stay.
Patient management
Patients were included in the study if they presented to the hospital with
evidence of UGIB defined by haematemesis, coffee-ground vomiting, or melaena.
Patients who developed UGIB while already an inpatient for another reason were
not included.
Page 9 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
9
All patients presenting to each hospital with UGIB were initially assessed in the
emergency department or acute assessment unit. Two centres (Glasgow and
Odense) had a policy of non-admission for those with GBS≤1 and one centre
(Truro) for those with GBS≤2 and age <70years, unless required for other
reasons. Out-patient endoscopy was arranged in all three centres. Proton pump
inhibitors (PPIs) were not routinely given to all admitted patients prior to
endoscopy. Following endoscopy, the policy in all centres was to administer high
dose PPIs by intravenous bolus followed by infusion to patients with high-risk
ulcer stigmata who required endoscopic therapy and to other selected patients
depending on clinical judgement.15-18 For patients with suspected variceal
bleeding, the policy in all centres was to give intravenous vasopressors and
antibiotics prior to endoscopy.16,24
The endoscopic practice in all centres for patients with high-risk stigmata of non-
variceal bleeding was to administer injection therapy, thermal contact and/or
clips, but not adrenaline alone.15-18 Band ligation or injection of tissue glue +/-
transjugular intrahepatic portosystemic stent-shunt was performed in cases of
oesophageal or gastric variceal bleeding respectively.16,24 In line with recent
evidence and guidelines, the policy was to administer red cell transfusion at a
haemoglobin threshold of 7-8g/dL, or as guided by the clinician in severe
haemorrhage.24,25
Data collection
At each centre, data on consecutive, unselected patients presenting to the
hospital with UGIB were collected over a twelve-month period between March
Page 10 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
10
2014 and March 2015. Data were collected at each site by a dedicated research
nurse, doctor, or medical student. The data collected included patient
characteristics and haemodynamic and laboratory parameters at presentation
necessary to calculate the full Rockall (FRS), ARS, GBS, AIMS65 and PNED scores
(see supplementary Table 1). Endoscopic findings were recorded.
Interventions including blood transfusion, endoscopic therapy, interventional
radiology and surgery were recorded, as was rebleeding within 7 days as
previously defined (see supplementary Table 2),26 30-day mortality and length of
hospital stay. The collected data are shown in supplementary Table 3.
Patient involvement
There was no direct patient involvement in the development, design or conduct
of the study.
Statistical analysis
We compared each scores’ ability to predict the predetermined outcomes using
calculation of area under the receiver operator characteristics curves (AUROCs)
and 95% confidence intervals (CIs). AUROCs were compared using chi-square
tests. The optimal score thresholds to predict very low risk patients potentially
suitable for outpatient management were identified based on a sensitivity of
≥95%. For the other outcomes, optimal thresholds were identified using the
Youden index.27 In addition, the performance of the scores was assessed by
calculation of sensitivity, specificity, positive predictive values (PPV), negative
predictive values (NPV), and proportion classified as low- or high-risk patients.
Page 11 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
11
We calculated rates of transfusion, endoscopic therapy, and mortality for those
classified as low-risk. Pearsons chi-square test and Fischer’s exact test were used
to compare proportions. The Mann-Whitney U test and the Kruskal-Wallis
equality-of-populations rank test were used to compare medians.
We aimed for an adequate sample size to compare all the outcomes described
above. Existing data indicated that highest power was needed for comparative
analyses on mortality. Therefore assuming mortality AUROC of 0·86 for
AIMS658,20 and 0·78 for FRS10,21 with an alpha of 5%, power of 90%, rank
correlation of 0·5 and mortality of 5%,13 the required sample size was 2814
patients. A two-tailed significance level of 5% was used. Data analysis was
undertaken using STATA 11·0 (StataCorp, College Station, Texas, USA).
Data and publication
Only the local principal investigator and dedicated nurse, junior doctor or
medical student had access to the identifiable data from their centre, with the
anonymised data sent to SBL and AJS for central analysis. Data was collected by
RA, LZ, ST, KW, CJLK, SBL, PN, JF, AH, AF, JS, NM, EP, HSO, YKC, DSK and TS.
The paper was written by AJS and SBL with input from all co-authors who
approved the final manuscript. AJS is the study guarantor. Our report follows
STROBE guidelines.
Page 12 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
12
Results
Patient characteristics and baseline scores:
A total of 3012 patients were included in the study with 2868 (95·2%) followed
up for 30 days. Median age was 65 years and 58% were male. Patient
characteristics, endoscopic findings, interventions and outcome are shown in
Table 1. A total of 1348 (45%) patients needed hospital-based intervention or
died within 30 days. Endoscopic therapy was performed in 574 (19%), 37
(1·2%) required interventional radiological therapy or surgery and 144 (5%)
rebled within 7 days. Median length of stay was 3 days (95% CI: 0-16), and 30-
day mortality 6·9%. Overall mean GBS was 6·6 (95% CI: 0-14), mean AIMS65
was 1 (0-3), mean ARS 2·7 (0-5), mean FRS 3·9 (1-7) and mean PNED 3·0 (0-8).
These data by centre are shown in supplementary Table 4.
Page 13 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
13
Comparison of scores ability to predict outcomes:
Intervention or mortality
GBS had the highest discriminative ability (AUROC 0·89) at predicting need for
intervention or death when compared to PNED (AUROC 0·71; p<0·0001),
AIMS65 (AUROC 0·70; p<0·0001), FRS (AUROC 0·69; p<0·0001) and ARS
(AUROC 0·69; p<0·0001) (Table 2 and Fig. 1). GBS performed consistently well in
all centres with AUROCs ranging between 0·85-0·91 (supplementary Table 5).
However, performance of AIMS65 and FRS varied by centre, with AUROCs
ranging from 0·54-0·75 and 0·57-0·79 respectively. AUROCs for ARS among
centres were 0·59-0·72, and for PNED 0·70-0·76 (supplementary Table 5)
The ability of the three pre-endoscopic scores to predict very low risk patients
who did not require intervention and survived at optimal cut-offs is shown in
Table 3. GBS≤1 had a sensitivity of 98·6%, specificity 34·6%, PPV 96.6% and
NPV 56.0% for this combined end-point. Intervention or death was recorded in
3·4% of the 564 patients with GBS≤1, compared with 14% of the 436 patients
with ARS=0 and 25% of the 865 patients with AIMS65=0. The most common
intervention seen in those with GBS≤1 was blood transfusion, with endoscopic
therapy performed in 1·4%, and overall mortality 0·4%. Compared with GBS ≤1,
patients with AIMS65=0 and ARS=0 had higher rates of both endoscopic
intervention and transfusion (p<0·001; Table 3). The proportion of low risk
patients defined by GBS≤1 varied by site, from 9% in Dunedin to 31% in
Glasgow.
Page 14 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
14
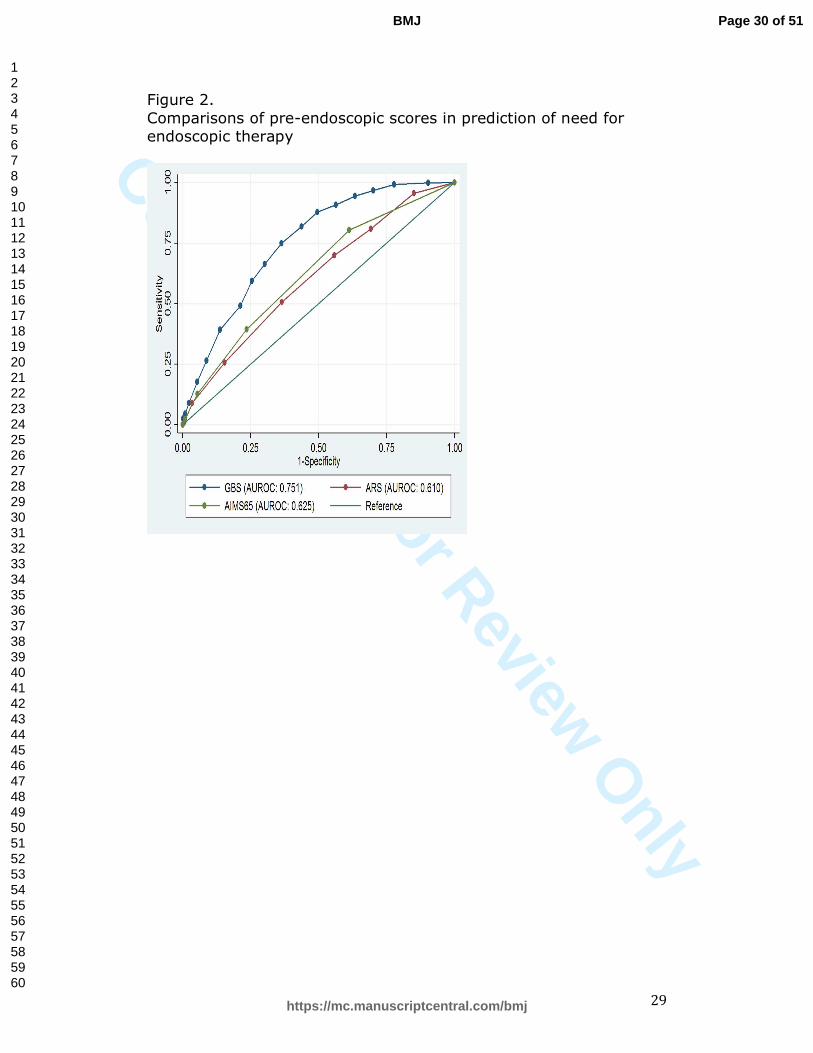
Endoscopic therapy
In predicting need for endoscopic therapy, GBS (AUROC 0·75) performed better
than the other pre-endoscopic scores: AIMS65 (AUROC 0·63; p<0·0001) and ARS
(AUROC 0·61; p<0·0001; see Fig. 2). The GBS performed equally well in
predicting this endpoint in all centres (Supplementary Table 5). A threshold of
GBS ≥7 was best at predicting endoscopic therapy with sensitivity of 80·4%,
specificity of 57·4%, PPV of 31·3% and NPV of 92·4% (Table 4).
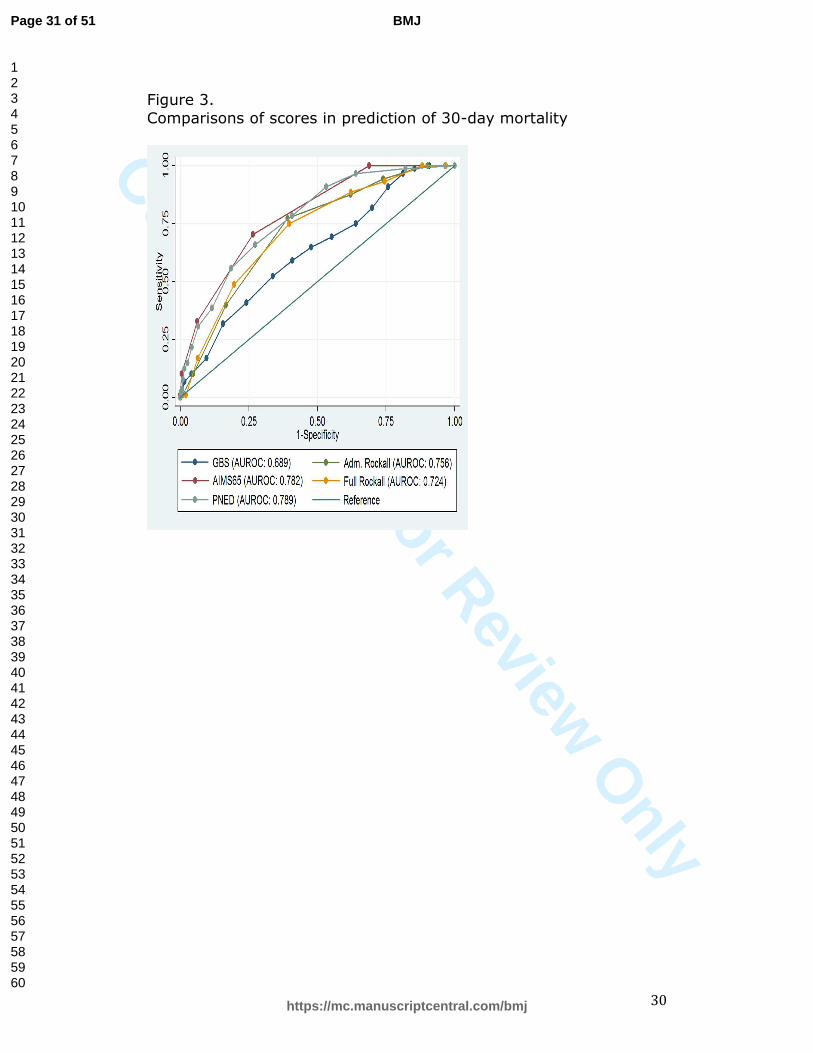
Mortality
PNED (AUROC 0·79) and AIMS65 (AUROC 0·78) had similar discriminative
abilities for predicting 30-day mortality (Table 2 and Figure 3). PNED was better
at predicting mortality than ARS (AUROC 0·76; p=0·03), FRS (AUROC 0·72;
p=0·03) and GBS (AUROC 0·69; p<0·0001). AIMS65 was better at predicting
mortality than GBS (p<0·0001), but the difference in AUROC compared with ARS
and FRS was not statistically significant. PNED ≥4, AIMS65 ≥2, ARS ≥4, FRS ≥5
and GBS ≥5 were the best score thresholds at predicting 30-day mortality. The
predictive ability of all five scores to identify high risk patients are shown in
Table 5.
Rebleeding and length of stay
PNED, which includes rebleeding in the score, was best (AUROC 0·85) at
predicting rebleeding, compared with GBS (AUROC 0·70; p<0·0001), FRS
(AUROC 0·63; p<0·0001), AIMS65 (AUROC 0·62; p<0·0001), and ARS (AUROC
0·62; p<0·0001). The GBS was better at predicting rebleeding compared with
AIMS65 (p=0·0003) and ARS (p=0·0002), but not FRS. All risk scores had
Page 15 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
15
relatively poor discriminative abilities for predicting length of stay >3 days, with
PNED AUROC=0·70, GBS and ARS AUROCs=0·69, FRS AUROC=0·65 and AIMS65
AUROC=0·64.
Missing values:
There were missing values for GBS (n=80), AIMS65 (n=511), Admission Rockall
score (n=43), Full Rockall score (n=1000), PNED (n=178), comorbidity (n=1),
systolic blood pressure (n=41), pulse (n=38), haemoglobin (n=28), findings at
endoscopy (n=2), true low-risk status (n=28), total units of blood transfused
(n=23), performance of endoscopic therapy (n=20), performance of surgery or
embolisation (n=5), rebleeding (n=51), and mortality (n=1).
Page 16 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
16
Discussion
This international multicentre study shows that following UGIB, GBS is a very
accurate risk score at all sites for predicting need for clinical intervention or
death. Although AIMS65 and PNED are the best scores for predicting mortality
and GBS best for predicting endoscopic therapy, accuracy and clinical utility is
relatively low for these endpoints.
Strengths of our study include its international multicentre design and large
number of consecutive patients studied. By assessing the five pre- and post-
endoscopy scores which appeared most promising for clinical use, we could
investigate the optimum way to risk assess patients with UGIB, both very early
after presentation to potentially direct to outpatient management, and also after
endoscopic diagnosis and therapy. Weaknesses of our study include the fact that
we excluded patients who were already inpatients when they developed UGIB.
These patients are already known to be at high risk of poor outcome. In addition,
31% of patients did not undergo endoscopy. In three centres, there was a
guideline to not admit patients with either GBS≤1 or ≤2 and age <70 years, and
many did not attend for outpatient endoscopy. In addition, some clinicians
decided an endoscopy was not required following an apparent trivial bleed, or
was deemed inappropriate for some very ill patients with multiple
comorbidities. Interestingly the UK national UGIB audit reported that 26% of
patients notified to gastroenterologists did not have an inpatient endoscopy.11
We do not believe this had a major effect on our study findings, as 95% patients
were followed up for 30 days after presentation.
Page 17 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
17
Published guidelines suggest outpatient management for patients with GBS of
zero.15-18 However some authors have suggested this low-risk threshold could be
extended to ≤1 or ≤2.13,14 We identified GBS ≤1 as the optimum score threshold
to identify patients who would not require intervention or die with sensitivity of
98·6%. There was a consistent high accuracy of this threshold across
international sites, which comprised 19% of all patients in our study, compared
with the 8·6% patients who had GBS of zero. Of the patients with GBS≤1, all
cause mortality was only 0·4%. This compares favourably with accepted low risk
thresholds of commonly used scores for other medical conditions including
CURB65 for chest infection and the Pulmonary Embolism Severity Index.28,29
Other studies have reported more accurate prediction of death, rebleeding or
length of stay using these scores, but our study has the advantages of a
multicentre design and large numbers and suggests these outcomes are not well
predicted by the studied scores.
The median length of hospital admission for a patient presenting with UGIB in
the UK is 4-5 days,3,12 and a recent study showed the mean in-hospital cost to be
£2458 per patient.30 Use of an accurate score within Emergency Departments or
Acute Assessment units, to identify very low risk patients with UGIB not
requiring admission has clear benefits. Interestingly, the proportion of very low-
risk patients defined by GBS≤1 varied by site. The differences are probably due
to different models of healthcare provision, including extent of primary care
services. At the other end of the spectrum of severity of UGIB, early identification
of high-risk patients who may benefit from urgent endoscopy or higher-level
care could help guide management. An observational study suggested that
Page 18 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
18
patients with GBS>12 have decreased mortality if endoscopy is undertaken <13
hours after presentation.19 Our data suggest that GBS≥7 and AIMS65 have the
highest combination of sensitivity and specificity for predicting endoscopic
therapy or 30-day mortality respectively, but the PPV for both is very low.
Therefore the clinical utility of these scores to direct care in high-risk patients
seems very limited.
In conclusion, GBS is accurate at predicting need for clinical intervention or
death in patients with UGIB in all countries studied. GBS≤1 is the optimum score
threshold for identifying very low risk patients suitable for outpatient
management. GBS≥7 is best at predicting need for endoscopic therapy and
PNED≥4 and AIMS65≥2 best at predicting mortality, although accuracy in
predicting these end-points is relatively low. No score appears accurate at
predicting rebleeding or length of stay. This information can help direct
management of very low risk patients with UGIB, but further studies using these,
or new scores, are required to clarify their role in directing management of
higher risk patients.
Page 19 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
19
References
1. Rockall TA, Logan RFA, Devlin HB, Northfield TC. Incidence of and mortality from
acute upper gastrointestinal haemorrhage in the UK. BMJ 1995; 311: 222-26.
2. Blatchford O, Davidson LA, Murray WR., Blatchford M, Pell J. Acute upper
gastrointestinal haemorrhage in west of Scotland: case ascertainment study. BMJ
1997; 315: 510-14.
3. Hearnshaw, SA, Logan RFA, Lowe D, Travis SP, Murphy MF, Palmer KR. Acute
upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and
outcomes in the 2007 UK audit. Gut 2011;60:1327-1335.
4. Rockall TA, Logan RFA, Devlin HB, Northfield TC. Risk assessment after acute
upper gastrointestinal haemorrhage. Gut 1996;38:316-321 (PMID:8675081)
5. Marmo R, Koch M, Cipoletta L, et al. For the Italian registry on upper
gastrointestinal bleeding. Predicting mortality in non-variceal upper
gastrointestinal bleeders: validation of the Italian PNED score and prospective
comparison with the Rockall score. Am J Gastroenterol 2010;105:1284-91
(PMID: 20051943)
6. Saeed ZA, Winchester CB, Carolyn B, Michaeletz PA, Woods KL, Graham DY. A
scoring system to predict rebleeding after endoscopic therapy of non-variceal
upper gastrointestinal hemorrhage. Am J Gastroenterol 1993;88:1842-9 (PMID:
8237930)
7. Blatchford O, Murray WR, Blatchford M. A risk score to predict need for
treatment for upper gastrointestinal haemorrhage. Lancet 2000;356:1318-21
(PMID 11073-21)
8. Saltzman JR, Tabak YP, Hyett BH, Sun X, Travis AC, Johannes RS. A simple risk
score accurately predicts in hospital mortality, length of stay and cost in acute
upper GI bleeding. Gastrointest Endosc. 2011;74:1215-24.
Page 20 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
20
9. Das A, Ben-Menachem T, Farooq FT,et al. Artificial neural network as a
predictive instrument in patients with acute non-variceal upper gastrointestinal
hemorrhage. Gastroenterol 2008;134:65-74 (PMID: 18061180)
10. Laursen SB, Hansen JM, De Muckadell OBS. The Glasgow Blatchford score is the
most accurate assessment of patients with upper gastrointestinal hemorrhage.
Clin Gastroenterol Hepatol 2012:10:1130-1135
11. Hearnshaw SA, Logan RFA, Lowe D, Travis SPL, Murphy MF, Palmer KR. Use of
endoscopy for management of acute upper gastrointestinal bleeding in the UK:
results of a nationwide audit. Gut 2010;59:1022-1029.
12. Stanley AJ, Ashley D, Dalton HR, et al. Outpatient management of patients with
low-risk upper-gastrointestinal haemorrhage: multicentre validation and
prospective evaluation. Lancet 2009;373:42-47.
13. Laursen SB, Dalton HR, Murray IA, et al. Performance of new thresholds of the
Glasgow Blatchford score in managing patients with upper gastrointestinal
bleeding. Clin Gastroenterol Hepatol 2015;13:115-121.
14. McLaughlin C, Vine L, Chapman L, et al. The management of low-risk primary
upper gastrointestinal haemorrhage in the community: a 5-year observational
study. Eur J Gastroenterol Hepatol 2012;24:288-293.
15. Barkun AN, Bardou M, Kuipers EJ, et al. International consensus
recommendations on the management of patients with nonvariceal upper
gastrointestinal bleeding. Ann Intern Med. 2010;152:101-113.
16. National Institute for Health and Clinical Excellence 2012 Acute Upper
Gastrointestinal Bleeding: management. Clinical Guideline 141. London: NICE.
17. Gralnek IM, Dumoncaeu JM, Kuipers, Lanas A, et al. Non-variceal upper
gastrointestinal haemorrhage: ESGE Guidelines. Endoscopy 2015:47:1-46
18. Laine L, Jensen DM. Management of patients with ulcer bleeding, ACG Practice
guidelines. Am J Gastroenterol 2012;107:345-60
Page 21 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
21
19. Lim, LG, Ho KY, Chan YH, et al. Urgent endoscopy is associated with lower
mortality in high-risk but not low-risk nonvariceal upper gastrointestinal
bleeding. Endoscopy 2011;43:300-306.
20. Hyett BH, Abougergi MS, Charpentier JP, et al. The AIMS65 score compared with
the Glasgow-Blatchford score in predicting outcomes in upper GI
bleeding. Gastrointest Endosc 2013;77:551-557.
21. Stanley AJ, Dalton HR, Blatchford O, et al. Multicentre comparison of the Glasgow
Blatchford and Rockall scores in the prediction of clinical end-points after upper
gastrointestinal haemorrhage. Aliment Pharmacol Therapeut 2011;34:470-475.
22. Pang SH, Ching YJL, Lau JYW, Sung JJY, Graham DY, Chan FKL. Comparing the
Blatchford and pre-endoscopic Rockall score in predicting the need for
endoscopic therapy in patients with upper GI hemorrhage. Gastrointest
Endosc 2010;71:1134-1140.
23. Yaka E, Yilmaz S, Ozgur DN, Pekdemir M. Comparison of the Glasgow-Blatchford
and AIMS65 Scoring Systems for Risk Stratification in Upper Gastrointestinal
Bleeding in the Emergency Department. Acad Emerg Medicine 2015;22:22-30.
24. De Franchis R. Revising consensus on portal hypertension; Report of the Baveno
V consensus workshop on methodology of diagnosis and therapy of portal
hypertension. J Hepatol 2010; 53: 762-768
25. Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper
gastrointestinal bleeding. N Engl J Med 2013;368:11-21
26. Laine L, Spiegel B, Rostom A, et al. Methodology for randomized trials of patients
with nonvariceal upper gastrointestinal bleeding: recommendations from an
international consensus conference. Am J Gastroenterol 2010;105;540-50.
27. Youden WJ. Index for rating diagnostic tests. Cancer 1950;3:32-5
Page 22 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
22
28. Lim W, van der Eeren MM, Laing Boersma W, et al. Defining community acquired
pneumonia severity on presentation to hospital: an international derivation and
validation study. Thorax 2003;58:377-382
29. Aujesky D, Roy PM, Vershuren F et al. Outpatient versus inpatient treatment for
patients with acute pulmonary embolism: an international, open-label,
randomised, non-inferiority trial. Lancet 2011;178:41-48
30. Campbell HE, Stokes EA, Bargo D, et al. Costs and quality of life associated with
acute upper gastrointestinal bleeding in the UK: cohort analysis of patients in a
cluster randomised trial. BMJ open 2015;5.4:e007230.
Page 23 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
23
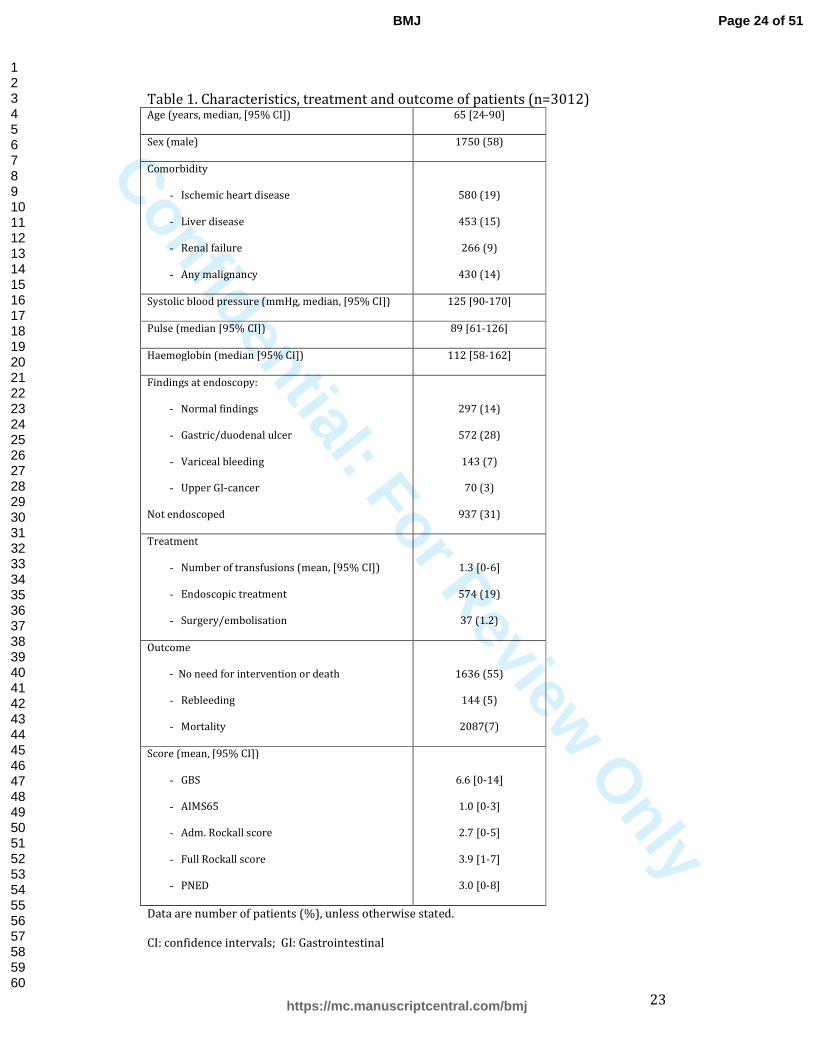
Table 1. Characteristics, treatment and outcome of patients (n=3012) Age (years, median, [95% CI]) 65 [24-90]
Sex (male) 1750 (58)
Comorbidity
- Ischemic heart disease
- Liver disease
- Renal failure
- Any malignancy
580 (19)
453 (15)
266 (9)
430 (14)
Systolic blood pressure (mmHg, median, [95% CI]) 125 [90-170]
Pulse (median [95% CI]) 89 [61-126]
Haemoglobin (median [95% CI]) 112 [58-162]
Findings at endoscopy:
- Normal findings
- Gastric/duodenal ulcer
- Variceal bleeding
- Upper GI-cancer
Not endoscoped
297 (14)
572 (28)
143 (7)
70 (3)
937 (31)
Treatment
- Number of transfusions (mean, [95% CI])
- Endoscopic treatment
- Surgery/embolisation
1.3 [0-6]
574 (19)
37 (1.2)
Outcome
- No need for intervention or death
- Rebleeding
- Mortality
1636 (55)
144 (5)
2087(7)
Score (mean, [95% CI])
- GBS
- AIMS65
- Adm. Rockall score
- Full Rockall score
- PNED
6.6 [0-14]
1.0 [0-3]
2.7 [0-5]
3.9 [1-7]
3.0 [0-8]
Data are number of patients (%), unless otherwise stated.
CI: confidence intervals; GI: Gastrointestinal
Page 24 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
24
Table 2. Discriminative ability of evaluated scoring systems
Outcome AUROC [95% CI]
Intervention or death
- GBS
- AIMS65
- ARS
- FRS
- PNED
0.89 [0.87-0.90]
0.70 [0.68-0.72]
0.69 [0.67-0.71]
0.69 [0.67-0.71]
0.71 [0.70-0.73]
Need for endoscopic therapy
- GBS
- AIMS65
- ARS
0.75 [0.73-0.77]
0.63 [0.60-0.65]
0.61 [0.59-0.64]
Rebleeding
- GBS
- AIMS65
- ARS
- FRS
- PNED
0.70 (0.66-0.74)
0.62 (0.57-0.66)
0.62 (0.57-0.66)
0.63 (0.58-0.68)
0.85 (0.83-0.88)
Mortality
- GBS
- AIMS65
- ARS
- FRS
- PNED
0.69 [0.66-0.72]
0.78 [0.75-0.81]
0.76 [0.73-0.79]
0.72 [0.68-0.77]
0.79 [0.76-0.82]
AUROC: Area under receiver operator characteristics curves; CI: Confidence Interval
Page 25 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only 25
Table 3. Outcomes at optimal thresholds of GBS, AIMS65 and ARS in prediction of need for intervention or death
System Cut-off
Low-risk
n(%)a
Sens.
(%)
Spec.
(%)
PPV
(%)
NPV
(%)
Transfusion
n(%)
Endo-therapy n(%)
Surgery/
Int. radiol
n(%)b
Mortality
n(%)c
GBS ≤1 564 (19.2) 98.6 34.6 96.6 56.0 10 (1.8) 8 (1.4) 2 (0.4) 2 (0.4)
AIMS65 =0 865 (34.6) 81.5 49.9 74.7 59.9 165 (19) 107 (12) 9 (1.0) 6 (0.7)
ARS =0 436 (14.7) 95.6 23.4 86.5 50.9 41 (9.4) 29 (6.7) 0 (0) 1 (0.2)
a Number (%) of classified low-risk patients according to risk-scoring system
b Number (%) of patients needing surgery, or arterial embolisation among patients classified as low-risk
c Number (%) of patients dying during admission among patients classified as low-risk
PPV: Positive predictive value; NPV: Negative predictive value
Page 26 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
26
Table 4. Need for endoscopic therapy at optimal score thresholds of each of the
pre-endoscopic scores: GBS, AIMS65 and ARS
System Cut-off
Number of classified
high-risk patients (%)
Sensitivity
(%)
Specificity
(%)
PPV
(%)
NPV
(%)
GBS ≥7 1456 (50) 80.4 57.4 31.3 92.4
AIMS65 ≥1 1619 (65) 79.7 38.7 25.9 87.6
ARS ≥3 1686 (57) 69.8 45.9 23.5 86.5
PPV: Positive predictive value; NPV: Negative predictive value
Page 27 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
27
Table 5. 30-day mortality at optimal score thresholds of GBS, AIMS65, PNED and
FRS
System
Cut-off
High-risk
n(%)a
Sensitivity
(%)
Specificity
(%)
PPV
(%)
NPV
(%)
AIMS65 ≥2 672 (26.9) 65.8 76.2 18.0 96.6
PNED ≥4 1065 (37.6) 77.3 65.3 14.1 97.5
ARS ≥4 1130 (38.1) 78.6 65.0 14.3 97.6
FRS ≥5 815 (40.5) 74.0 61.7 11.1 97.3
GBS ≥5 1812 (61.8) 88.7 40.2 9.9 97.9
a Number (%) of classified high-risk patients according to risk-scoring system
PPV: Positive predictive value; NPV: Negative predictive value
Page 28 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
28
Figure 1.
Comparisons of scores in prediction of need for any intervention (transfusion, endoscopic therapy, interventional-radiology or surgery) or 30-day mortality
Page 29 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
29
Figure 2.
Comparisons of pre-endoscopic scores in prediction of need for endoscopic therapy
Page 30 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
30
Figure 3.
Comparisons of scores in prediction of 30-day mortality
Page 31 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
31
Supplementary Table 1.
Risk scores evaluated in study.
1 a) Full Rockall score (FRS; ref 4)
1 b) Admission Rockall score (ARS) excludes parameters marked with *
0 1 2 3
Age (yrs) <60 60-79 ≥80 -
Shock No shock
(SBP≥100mmHg
and pulse
<100bpm)
Pulse
>100bpm
SBP
<100mmHg
-
Co-morbidity No major
comorbidity
- Cardiac
failure,
Ischaemic
heart disease,
Any major
comorbidity
Renal failure,
Liver failure,
Metastatic
cancer
Diagnosis * Mallory Weiss
tear, no lesion,
no stigmata
All other
diagnoses
Malignancy of
upper GI tract
-
Major
Stigmata *
None or dark
spot only
- Blood in
upper GI
tract,
adherent clot,
visible or
spurting
vessel
-
SBP: Systolic blood pressure
Page 32 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
32
1 c) Glasgow Blatchford Score (GBS; ref 7)
Admission Criteria Score
Haemoglobin (g/dl)
Male
12 - <13
10 - <12
<10
Female
10 - <12
<10
1
3
6
1
6
Urea (mmol/L)
6.5 - <8
8.0 – 10
10 - <25
≥ 25
2
3
4
6
Systolic Blood pressure (mmHg)
100 – 109
90 -99
<90
1
2
3
Pulse (bpm)
≥ 100 bpm
1
Melaena 1
Syncope 2
Cardiac failure 2
Liver failure 2
Page 33 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
33
1 d) AIMS65 (ref 8)
Admission Criteria Score
Albumin <30g/l
1
*INR >1.5
1
Mental State: +GCS <14
1
Systolic Blood Pressure <90mmHg
1
Age >65yrs
1
*International Normalised Ratio
+Glasgow Coma Scale
Page 34 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
34
1 e) Progetto Nazionale Emorragia Digestive score (PNED; ref 5)
Score: 1 2 3 4
Risk factors: *ASA 3,
Time to
admission <8hrs
Hb ≤7g/dL,
Age ≥80yrs,
Renal failure
Rebleeding,
ASA 4,
Neoplasia,
Liver cirrhosis
Failure of
endoscopic
therapy
*ASA: American Society of Anesthesiologists score
Page 35 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
35
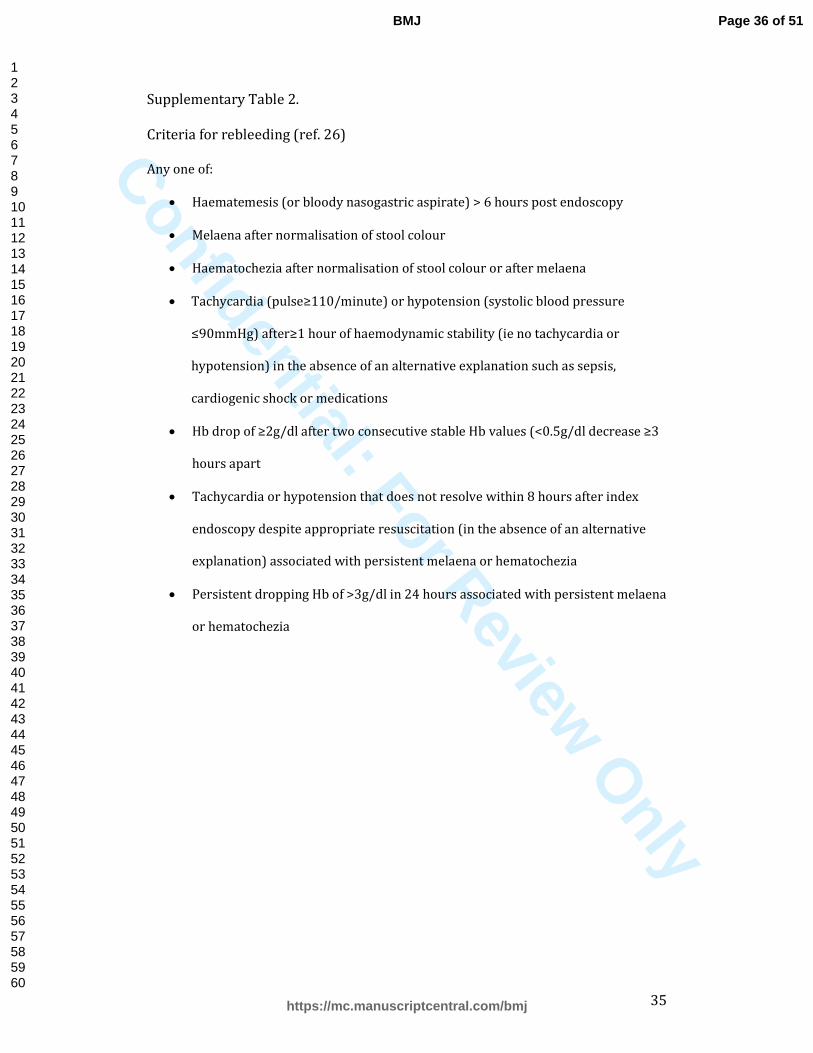
Supplementary Table 2.
Criteria for rebleeding (ref. 26)
Any one of:
• Haematemesis (or bloody nasogastric aspirate) > 6 hours post endoscopy
• Melaena after normalisation of stool colour
• Haematochezia after normalisation of stool colour or after melaena
• Tachycardia (pulse≥110/minute) or hypotension (systolic blood pressure
≤90mmHg) after≥1 hour of haemodynamic stability (ie no tachycardia or
hypotension) in the absence of an alternative explanation such as sepsis,
cardiogenic shock or medications
• Hb drop of ≥2g/dl after two consecutive stable Hb values (<0.5g/dl decrease ≥3
hours apart
• Tachycardia or hypotension that does not resolve within 8 hours after index
endoscopy despite appropriate resuscitation (in the absence of an alternative
explanation) associated with persistent melaena or hematochezia
• Persistent dropping Hb of >3g/dl in 24 hours associated with persistent melaena
or hematochezia
Page 36 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
36
Supplementary Table 3
Registered data
Characteristics of patients - Age - Sex
Comorbidity - ASA-score - Ischaemic heart disease - Cardiac failure - Renal failure - Liver disease - Liver cirrhosis - Liver failure - Any malignancy - Disseminated malignancy - Any major comorbidity - Previous surgery for peptic ulcer
Medication use - NSAIDs - Aspirin - ADP-receptor inhibitors - Anticoagulants
Symptoms - Coffee ground vomiting - Haematemesis - Melaena - Haematochezia - Syncope - Altered mental status
Blood tests - Haemoglobin - Urea - Creatinine - INR - Albumin
Circulatory status at hospital admission - Systolic blood pressure - Pulse
Endoscopy - Time from admission to performance of endoscopy - Findings at endoscopy - Performance of endoscopic therapy - Bleeding uncontrolled by endoscopic therapy - Performance of endoscopic therapy impossible
Other treatment - Number of received blood transfusions - Performance of surgery or interventional radiological intervention
Rebleeding - Development of rebleeding
Page 37 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
37
- Treatment of rebleeding Mortality
- Bleeding-related mortality - Non-bleeding-related mortality
Other data (related to hospitalisation and follow-up) - Time from development of symptoms to hospital admission - Admission overnight/weekend - Length of ICU admission - Patient discharged without performance of endoscopy - Endoscopy performed on an outpatient basis - Time of follow-up
ADP-receptor inhibitors : Adenosine diphosphate receptor inhibitors
ASA: American Society of Anesthesiologists
ICU: Intensive care unit
INR: International normalised ratio
NSAIDs: Nonsteroidal anti-inflammatory drugs
Page 38 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only 38
Supplementary Table 4.
Characteristics, treatment and outcome of patients by centre
Site Yale Glasgow Truro Odense Singapore Dunedin Overall
n 799 600 542 539 433 99 3012
Age (years, median, [95% CI]) 63 [24-90] 55 [22-87] 69 [24-91] 72 [31-93] 66 [27-87] 71 [22-88] 65 [24-90]
Sex (male) 432 (54) 371 (62) 314 (58) 301 (56) 274 (63) 58 (59) 1750 (58)
Comorbidity
- Ischemic heart disease
- Liver disease
- Renal failure
- Any malignancy
181 (23)
151 (19)
56 (7)
157 (20)
95 (16)
127 (21)
77 (13)
75 (13)
85 (16)
60 (11)
40 (7)
75 (14)
117 (22)
51 (9)
25 (5)
47 (9)
81 (19)
48 (11)
62 (14)
61 (14)
21 (21)
16 (16)
6 (6)
15 (15)
580 (19)
453 (15)
266 (9)
430 (14)
Systolic blood pressure (mmHg) median, [95% CI]) 125 [92-170] 127 [92-163] 129 [90-173] 125 [86-169] 120 [83-164] 127 [90-171] 125 [90-170]
Pulse (median [95% CI]) 87 [60-125] 92 [62-133] 90 [63-126] 90 [62-124] 91 [62-125] 86 [56-115] 89 [61-126]
Haemoglobin (median [95% CI]) 107 [60-161] 128 [66-168] 124 [64-167] 102 [52-153] 101 [54-156] 97 [54-146] 112 [58-162]
Findings at endoscopy
- Normal findings
- Erosive diseasea
- Mallory-Weiss tear
47 (10)
92 (20)
14 (3)
45 (13)
91 (27)
19 (6)
62 (16)
177 (45)
8 (2)
91 (18)
133 (27)
13 (3)
38 (12)
83 (26)
6 (2)
14 (23)
7 (11)
3 (5)
297 (14)
583 (28)
63 (3)
Page 39 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
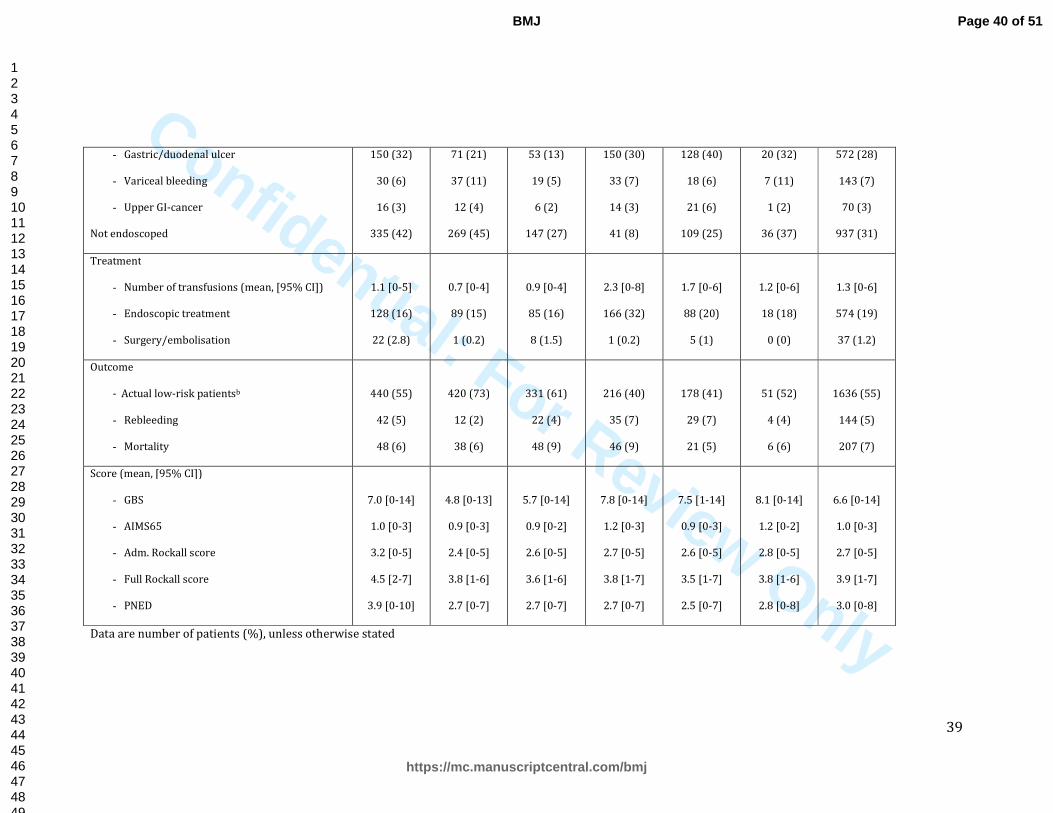
Confidential: For Review Only 39
- Gastric/duodenal ulcer
- Variceal bleeding
- Upper GI-cancer
Not endoscoped
150 (32)
30 (6)
16 (3)
335 (42)
71 (21)
37 (11)
12 (4)
269 (45)
53 (13)
19 (5)
6 (2)
147 (27)
150 (30)
33 (7)
14 (3)
41 (8)
128 (40)
18 (6)
21 (6)
109 (25)
20 (32)
7 (11)
1 (2)
36 (37)
572 (28)
143 (7)
70 (3)
937 (31)
Treatment
- Number of transfusions (mean, [95% CI])
- Endoscopic treatment
- Surgery/embolisation
1.1 [0-5]
128 (16)
22 (2.8)
0.7 [0-4]
89 (15)
1 (0.2)
0.9 [0-4]
85 (16)
8 (1.5)
2.3 [0-8]
166 (32)
1 (0.2)
1.7 [0-6]
88 (20)
5 (1)
1.2 [0-6]
18 (18)
0 (0)
1.3 [0-6]
574 (19)
37 (1.2)
Outcome
- Actual low-risk patientsb
- Rebleeding
- Mortality
440 (55)
42 (5)
48 (6)
420 (73)
12 (2)
38 (6)
331 (61)
22 (4)
48 (9)
216 (40)
35 (7)
46 (9)
178 (41)
29 (7)
21 (5)
51 (52)
4 (4)
6 (6)
1636 (55)
144 (5)
207 (7)
Score (mean, [95% CI])
- GBS
- AIMS65
- Adm. Rockall score
- Full Rockall score
- PNED
7.0 [0-14]
1.0 [0-3]
3.2 [0-5]
4.5 [2-7]
3.9 [0-10]
4.8 [0-13]
0.9 [0-3]
2.4 [0-5]
3.8 [1-6]
2.7 [0-7]
5.7 [0-14]
0.9 [0-2]
2.6 [0-5]
3.6 [1-6]
2.7 [0-7]
7.8 [0-14]
1.2 [0-3]
2.7 [0-5]
3.8 [1-7]
2.7 [0-7]
7.5 [1-14]
0.9 [0-3]
2.6 [0-5]
3.5 [1-7]
2.5 [0-7]
8.1 [0-14]
1.2 [0-2]
2.8 [0-5]
3.8 [1-6]
2.8 [0-8]
6.6 [0-14]
1.0 [0-3]
2.7 [0-5]
3.9 [1-7]
3.0 [0-8]
Data are number of patients (%), unless otherwise stated
Page 40 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review Only 40
aoesophagitis, gastritis or duodenitis
bNumber of patients without need of intervention (transfusion, endoscopic treatment, surgery, or embolization) who survive
CI: Confidence Interval
GI: Gastrointestinal
Page 41 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review Only 41
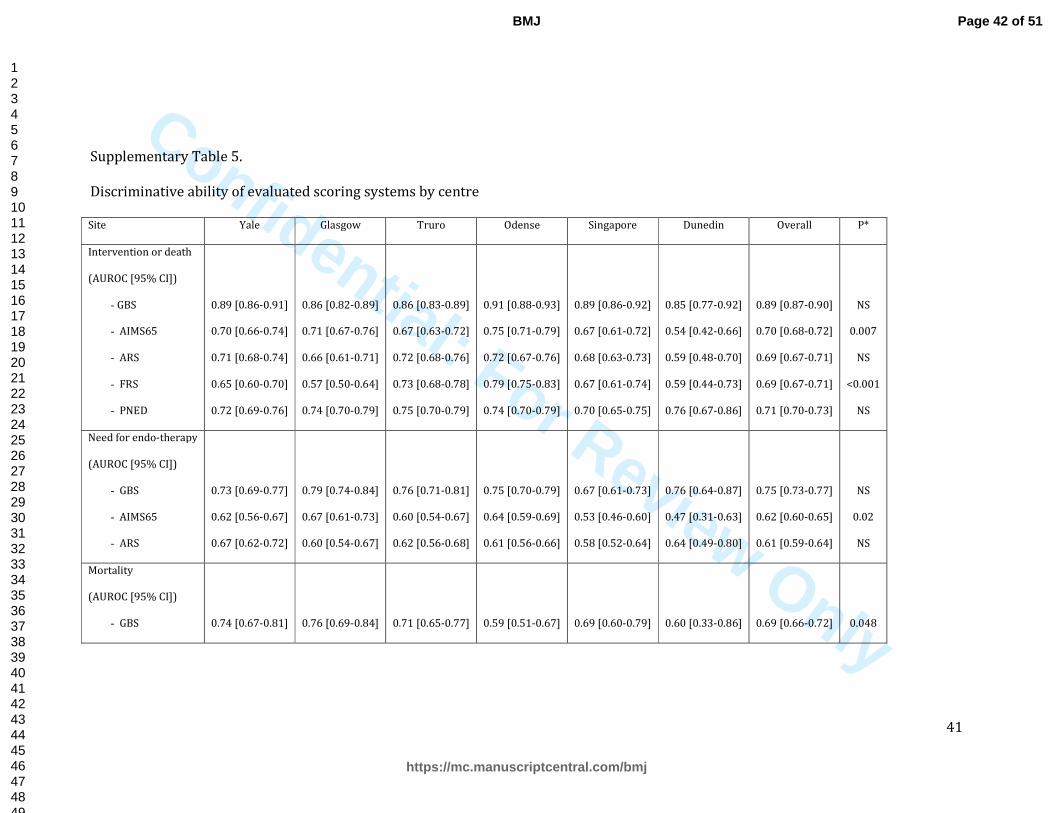
Supplementary Table 5.
Discriminative ability of evaluated scoring systems by centre
Site Yale Glasgow Truro Odense Singapore Dunedin Overall P*
Intervention or death
(AUROC [95% CI])
- GBS
- AIMS65
- ARS
- FRS
- PNED
0.89 [0.86-0.91]
0.70 [0.66-0.74]
0.71 [0.68-0.74]
0.65 [0.60-0.70]
0.72 [0.69-0.76]
0.86 [0.82-0.89]
0.71 [0.67-0.76]
0.66 [0.61-0.71]
0.57 [0.50-0.64]
0.74 [0.70-0.79]
0.86 [0.83-0.89]
0.67 [0.63-0.72]
0.72 [0.68-0.76]
0.73 [0.68-0.78]
0.75 [0.70-0.79]
0.91 [0.88-0.93]
0.75 [0.71-0.79]
0.72 [0.67-0.76]
0.79 [0.75-0.83]
0.74 [0.70-0.79]
0.89 [0.86-0.92]
0.67 [0.61-0.72]
0.68 [0.63-0.73]
0.67 [0.61-0.74]
0.70 [0.65-0.75]
0.85 [0.77-0.92]
0.54 [0.42-0.66]
0.59 [0.48-0.70]
0.59 [0.44-0.73]
0.76 [0.67-0.86]
0.89 [0.87-0.90]
0.70 [0.68-0.72]
0.69 [0.67-0.71]
0.69 [0.67-0.71]
0.71 [0.70-0.73]
NS
0.007
NS
<0.001
NS
Need for endo-therapy
(AUROC [95% CI])
- GBS
- AIMS65
- ARS
0.73 [0.69-0.77]
0.62 [0.56-0.67]
0.67 [0.62-0.72]
0.79 [0.74-0.84]
0.67 [0.61-0.73]
0.60 [0.54-0.67]
0.76 [0.71-0.81]
0.60 [0.54-0.67]
0.62 [0.56-0.68]
0.75 [0.70-0.79]
0.64 [0.59-0.69]
0.61 [0.56-0.66]
0.67 [0.61-0.73]
0.53 [0.46-0.60]
0.58 [0.52-0.64]
0.76 [0.64-0.87]
0.47 [0.31-0.63]
0.64 [0.49-0.80]
0.75 [0.73-0.77]
0.62 [0.60-0.65]
0.61 [0.59-0.64]
NS
0.02
NS
Mortality
(AUROC [95% CI])
- GBS
0.74 [0.67-0.81]
0.76 [0.69-0.84]
0.71 [0.65-0.77]
0.59 [0.51-0.67]
0.69 [0.60-0.79]
0.60 [0.33-0.86]
0.69 [0.66-0.72]
0.048
Page 42 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only 42
- AIMS65
- ARS
- FRS
- PNED
0.79 [0.73-0.85]
0.78 [0.73-0.84]
0.73 [0.62-0.83]
0.82 [0.77-0.87]
0.85 [0.80-0.89]
0.74 [0.67-0.81]
0.66 [0.56-0.75]
0.81 [0.73-0.89]
0.73 [0.66-0.80]
0.79 [0.73-0.85]
0.76 [0.68-0.85]
0.79 [0.73-0.85]
0.75 [0.68-0.82]
0.72 [0.65-0.78]
0.72 [0.64-0.79]
0.77 [0.72-0.83]
0.86 [0.79-0.94]
0.83 [0.77-0.89]
0.84 [0.75-0.94]
0.82 [0.73-0.91]
0.63 [0.38-0.88]
0.62 [0.33-0.90]
0.94 [0.85-1.00]
0.79 [0.56-1.00]
0.78 [0.75-0.81]
0.76 [0.73-0.79]
0.72 [0.68-0.77]
0.79 [0.76-0.82]
0.014
NS
0.003
NS
AUROC: area under the receiver operator characteristics curves; CI: Confidence Interval; * Difference in discriminative performance between centres
Page 43 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
43
Supplemental file:
Study protocol
International multicentre study comparing risk scoring systems for
patients presenting with upper gastrointestinal bleeding.
Study Protocol
1. General information
1.1 Running Title
“International study on scoring systems for upper GI bleeding”
1.2 Study details
Protocol version 1.4
Date: 20.01.14
REC number: 145837/544932/1/939
Sponsor’s protocol (R&D) reference number: GN13GA571
Sponsor: NHS Greater Glasgow & Clyde
Funding: There is no specific funding for this clinically designed and led study.
Each centre will access support from existing local audit/research nurses and/or
a junior doctor to collect data.
This study will be performed according to the Research Governance Framework
for Health and Community Care (second edition, 2006) and World Medical
Association Declaration of Helsinki Ethical Principles for Medical Research
Involving Human Subjects 1964 (as amended)
Page 44 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
44
1.3 Contacts
1.3.1 Chief Investigator:
Dr Adrian J Stanley MD, Department of Gastroenterology,
Glasgow Royal Infirmary, Glasgow, G4 OSF, UK
Tel: 0141 211 4073
Fax: 0141 211 5131
Email: [email protected]
1.3.2 Sponsor’s representative:
Ms Maureen Travers
NHS Greater Glasgow & Clyde health Board (GG&CHB)
Research and Development Management Office
Tennant Institute,
38 Church St,
Western Infirmary,
Glasgow G11 6NT
Tel: 0141 211 6389
Email: [email protected]
1.4 Investigators
1.4.1 Chief Investigator
AJ Stanley, MD, Department of Gastroenterology, Glasgow Royal Infirmary,
Glasgow, UK
1.4.2 Principle Investigators
1. L Laine, MD, Internal Medicine, Yale School of Medicine, New Haven,
Connecticut, USA
2. SB Laursen, MD, PhD, Department of Medical Gastroenterology, Odense
University Hospital, Odense, Denmark
3. HR Dalton, MD, DPhil, Gastrointestinal Unit, Royal Cornwall Hospital, Truro,
Cornwall, UK
Page 45 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
45
4. IA Murray, MD, Gastrointestinal Unit, Royal Cornwall Hospital, Truro,
Cornwall, UK
5. M Schultz, MD, PhD, Department of Medicine, Dunedin School of Medicine,
University of Otago, Dunedin, New Zealand
6. JH Ngu, MB ChB, PhD, Department of Gastroenterology, Singapore General
Hospital, Singapore
7. CJL Khor, MBBS, Department of Gastroenterology, Singapore General Hospital,
Singapore
8. Rozeta Abazi, MD, Department of Medical Gastroenterology, Odense University
Hospital, Odense, Denmark
1.5 Study start date
March 2014
1.6 Estimated primary completion date
March 2015
2. Background
Several recent international guidelines have recommended the use of early risk
assessment in patients who present with upper gastrointestinal bleeding (UGIB)
(1-3). Several risk scoring tools have been developed for use in this situation.
Many of these incorporate findings from the patient’s endoscopy including the
widely used Rockall score from the UK (4), the American Baylor and Cedars Sinai
scores, the Spanish Almela and Italian PNED scores (5-8). However in many
centres, endoscopy is often delayed unless for emergency reasons. Therefore
several scores have been developed which can be calculated very soon after
presentation, prior to endoscopy, which are particularly useful in helping
identify a cohort of “low risk” patients who may be able to avoid admission and
have out-patient management. These scores can also direct higher risk patients
Page 46 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
46
to appropriate management and interventional strategies. These pre-endoscopy
scores include the “Clinical” Rockall (omitting the endoscopic components of the
full Rockall score), the Glasgow Blatchford (GBS) and Cambridge scores from the
UK, the American AIM65 score and several artificial neural networks (ANNs) (9-
13).
There have been numerous studies comparing various combinations of risk
scores for UGIB although relatively few are multicentre. In addition there are
very limited data on international comparison of risk assessment scores. Current
evidence suggests the scores with the highest accuracy for identifying poor
outcome as defined by mortality, rebleeding or clinical intervention (need for
transfusion, endoscopic, surgical or radiological intervention) are the post-
endoscopic full Rockall score and the pre-endoscopic GBS or AIM65. However
several of the newer scores have not been externally validated or compared with
other risk assessment tools. Therefore the optimum score for use in clinical
practice remains uncertain.
3. Aim
The aim of this study is to compare the clinical utility of the Clinical Rockall, GBS,
AIM65, full Rockall and PNED scores in a prospective, multicentre, international
cohort of patients presenting with UGIB. All collected data will be anonymised,
with patients only identifiable to the local PI or research nurse. The data will also
be analysed to assess whether an improved new score (pre-endoscopy or post-
endoscopy) can improve the prediction of outcome for patients with UGIB.
4. Methods
The study is designed as a non-interventional, prospective, multicentre,
international cohort study. Consecutive patients presenting with UGIB and
fulfilling the criteria for inclusion (see point 4.2) will be included at the
participating centres (see point 4.4).
All centres will collect the same data. Registered data will include patients’
characteristics, blood tests, findings at endoscopy (if undertaken), and
interventions in the form of blood transfusion, endoscopic treatment, surgery, or
Page 47 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
47
radiological intervention (see point 4.6 for details). Persistent bleeding,
rebleeding, in-hospital death and 30-day mortality will be recorded. Data will be
collected by medical doctors, medical students, or research nurses depending on
the site. All data will be anonymised on the database and only identifiable to the
local PI or research nurse.
The study is non-interventional with no randomisation and all patient
management will be as per standard of care for patients with UGIB. The
registered anonymised data will be used to compare the predictive abilities of
the clinical and full Rockall score, GBS, AIM65, and PNED (see point 4.9 for
details). Furthermore, the data will be interrogated to try and develop a new risk
score and compare the performance of this with the existing risk score systems.
4.1 Study population
Consecutive patients presenting with symptoms of UGIB at the participating
centres are included. UGIB is defined as history of haematemesis, coffee-ground
vomit, or melaena. Patients with the combined presence of hematochezia and
circulatory insufficiency will also be included (see 4.2).
4.2 Inclusion criteria
- Patients presenting with haematemesis, coffee-ground vomit, melaena, or:
- Patients presenting with haematochezia and circulatory insufficiency (heart
rate >100bpm and/or systolic blood pressure <100mmHg)
4.3 Exclusion criteria
- Patients presenting with UGIB while already in-patients for another reason
4.4 Participating centres
- Glasgow Royal Infirmary, Glasgow, UK
- Royal Cornwall Hospital, Truro, UK
- Odense University Hospital, Odense, Denmark
- Dunedin Public Hospital, Dunedin, New Zealand
- Yale University Hospital, New Haven, Connecticut, USA
- Singapore General Hospital, Singapore
Page 48 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
48
(Humanitas Hospital, Milan and St Johns Hospital, London Ontario – if can obtain
resource to undertake study)
4.5 Intervention
There are no interventions. Patients will be treated according to the standard of
care for patients presenting with UGIB.
4.6 Registered data
4.6.1 Patient characteristics
Age, sex, comorbidity (ischaemic heart disease, cardiac failure, renal failure, liver
disease, liver cirrhosis, liver failure, COPD, Diabetes, cerebrovascular disease,
any malignancy, disseminated malignancy), altered mental status, previous
peptic ulcer, use of NSAID’s, antiplatelet or anticoagulant medication, American
Society of anesthesiologists (ASA) score and blood tests (serum urea, creatinine,
albumin, haemoglobin and INR)
4.6.2 Presentation
Symptoms (coffee ground vomiting, haematemesis, melaena, haematochezia,
syncope), and time from development of symptoms to presentation to hospital.
4.6.3 Bleeding source and severity of bleeding
Pulse and systolic blood pressure at presentation and findings at upper
endoscopy (and blood tests as above)
4.6.4 Outcomes
Treatment with blood transfusion, performance of endoscopic therapy,
performance of surgical/radiological haemostasis, persistent bleeding,
development of rebleeding, time to development of, and severity of rebleeding
(need for transfusion/repeat endoscopy/surgery/radiological intervention), and
30-day mortality
4.6.5 Other data regarding hospital admission/discharge from the
emergency department
Page 49 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
49
Admission overnight or at weekends, time from presentation to performance of
endoscopy, length of hospitalisation, and discharge from emergency department
without hospitalisation.
4.6.6 Study management & Data handling
Each patient will have a study number. Each centre will collect and add the local
anonymised data to their own local database. Patient data will only be
identifiable to the local research nurse and PI, with the identifiable link being
held as a paper copy in a local locked cabinet. Presentation data will be entered
anonymously onto the local database by the research nurse, with the 30-day
follow-up data added subsequently from electronic records. On completion of the
study, local anonymised data from each centre will be sent to Drs Laursen and
Stanley for final analysis.
4.7 Primary outcome
- Need for hospital based intervention defined as need for blood transfusion,
haemostatic intervention (endoscopic/surgical/radiological haemostasis), or 30-
day mortality
4.8 Secondary outcomes
- Rebleeding
- Length of hospital stay
4.9 Statistical analyses
The predictive abilities of the examined risk scoring systems will be evaluated by
calculation of sensitivity, specificity, positive predictive values (PPV), negative
predictive values (NPV), and receiver operating characteristics (ROC) curves.
Potential geographic variation will be analysed. The outcome among patients
classified as low-risk (not requiring transfusion, haemostatic intervention and
alive at 30-days) will be compared between systems.
A new risk score for identifying patients in need for hospital based intervention
will be developed using regression analysis. The predictive ability of this new
score will be described by sensitivity, specificity, positive predictive values
Page 50 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
50
(PPV), negative predictive values (NPV), and ROC curves. The predictive ability
will be compared to the performance of the clinical and full Rockall score, GBS,
AIM65, and PNED.
5. Funding
There is no specific funding for this study. Each centre will involve existing local
research or audit nurses +/- a junior doctor to collect data.
6. End of study definition
The end of the study will be 30 days after inclusion of the last patient (estimated
March 2015).
7. Publication
The results of the study will be presented at international conferences in
gastroenterology and will be published in an international pear reviewed
journal.
Page 51 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
51
Declaration of competing interests
All authors have completed the Unified Competing Interest form at
www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author)
and declare that (1) no authors have support from any company for the submitted work;
(2) no authors have relationships with any company that might have an interest in the
submitted work (3) no author, their spouses, partners, or children have financial
relationships that may be relevant to the submitted work and (4) no authors have any
non-financial interests that may be relevant to the submitted work.
Transparency Declaration
AJS (study guarantor) affirms that the manuscript is an honest, accurate and transparent
account of the study being reported. No important aspects of the study have been
omitted and no discrepancies identified.
Data sharing statement
Patient level data and/or full dataset available from the corresponding author AJS.
Consent was not obtained but the presented data are anonymised and risk of
identification is low.
Exclusive License
Dr Stanley (as corresponding author) on behalf of all authors grants a worldwide license
to the publishers and its licensees in perpetuity in all forms to publish this contribution.
Page 52 of 51
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Related Documents










