BMJ Open is committed to open peer review. As part of this commitment we make the peer review history of every article we publish publicly available. When an article is published we post the peer reviewers’ comments and the authors’ responses online. We also post the versions of the paper that were used during peer review. These are the versions that the peer review comments apply to. The versions of the paper that follow are the versions that were submitted during the peer review process. They are not the versions of record or the final published versions. They should not be cited or distributed as the published version of this manuscript. BMJ Open is an open access journal and the full, final, typeset and author-corrected version of record of the manuscript is available on our site with no access controls, subscription charges or pay-per-view fees (http://bmjopen.bmj.com ). If you have any questions on BMJ Open’s open peer review process please email [email protected] on January 30, 2022 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2018-023592 on 10 September 2018. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
BMJ Open is committed to open peer review. As part of this commitment we make the peer review history of every article we publish publicly available. When an article is published we post the peer reviewers’ comments and the authors’ responses online. We also post the versions of the paper that were used during peer review. These are the versions that the peer review comments apply to. The versions of the paper that follow are the versions that were submitted during the peer review process. They are not the versions of record or the final published versions. They should not be cited or distributed as the published version of this manuscript. BMJ Open is an open access journal and the full, final, typeset and author-corrected version of record of the manuscript is available on our site with no access controls, subscription charges or pay-per-view fees (http://bmjopen.bmj.com). If you have any questions on BMJ Open’s open peer review process please email
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from

For peer review only
Epidemiology of respiratory bacterial infections in people with lower respiratory tract infections in Africa: The
BARIAFRICA systematic review and meta-analysis protocol
Journal: BMJ Open
Manuscript ID bmjopen-2018-023592
Article Type: Protocol
Date Submitted by the Author: 13-Apr-2018
Complete List of Authors: Tchatchouang, Serges; Centre Pasteur of Cameroon, Department of Virology; Faculty of Sciences, University of Yaoundé I, Department of Biochemistry Bigna, Jean Joel; Centre Pasteur of Cameroon, Department of Epidemiology and Public Health Nzouankeu, Ariane; Centre Pasteur of Cameroon, Department of Bacteriology Penlap, Véronique; Faculty of Sciences, University of Yaoundé I, Department of Biochemistry Fonkoua, Marie-Christine; Centre Pasteur of Cameroon, Department of Bacteriology Ndangang, Marie; Rouen University Hospital, Department of Medical Information and Informatics Kenmoe, Sebastien; Centre Pasteur of Cameroon, Department of Virology Njouom, Richard; Centre Pasteur of Cameroon, Department of Virology
Keywords: Epidemiology < INFECTIOUS DISEASES, Respiratory infections < THORACIC MEDICINE, Epidemiology < THORACIC MEDICINE, Epidemiology < TROPICAL MEDICINE
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on January 30, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-023592 on 10 S
eptember 2018. D
ownloaded from
For peer review only
1
Epidemiology of respiratory bacterial infections in people with lower
respiratory tract infections in Africa: The BARIAFRICA systematic review
and meta-analysis protocol
Serges Tchatchouang1, 2
, Jean Joel Bigna3, 4
, Ariane Nzouankeu5, Véronique Penlap
2,
Marie-Christine Fonkoua5, Marie S. Ndangang
6, Sébastien Kenmoe
1, Richard Njouom
1*
1. Department of Virology, Centre Pasteur of Cameroon, Member of the International
Network of Pasteur Institutes, P.O. Box 1274, Yaoundé, Cameroon
2. Department of Biochemistry, Faculty of Sciences, University of Yaoundé I, Yaoundé,
Cameroon
3. Department of Epidemiology and Public Health, Centre Pasteur of Cameroon, Member of
the International Network of Pasteur Institutes, P.O. Box 1274, Yaoundé, Cameroon
4. School of Public Health, Faculty of Medicine, University of Paris Sud XI, 63 Rue Gabriel
Péri, 94270, Le Kremlin-Bicêtre, France
5. Department of Bacteriology, Centre Pasteur of Cameroon, Member of the International
Network of Pasteur Institutes, P.O. Box 1274, Yaoundé, Cameroon
6. Department of Medical Information and Informatics, Rouen University Hospital, Rouen,
France
Email addresses: ST ([email protected]), JJB ([email protected]), AN
([email protected]), VP ([email protected]), M-CF (fonkoua@pasteur-
yaounde.org), MSN ([email protected]), SK ([email protected]), RN
* Corresponding author: Department of Virology, Centre Pasteur of Cameroon, Member of
the International Network of Pasteur Institutes, 451 Street 2005, P.O. Box 1274, Yaoundé II,
Yaoundé, Cameroon. E-mail: [email protected]
Page 1 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
2
Abstract
Introduction
The burden of lower respiratory tract infections (LRTIs) is a substantial public health concern.
However, epidemiology of LRTIs and its main bacterial aetiologies are poorly characterized,
particularly in Africa continent. Providing accurate data can help for designing cost-effective
interventions to curb the burden of respiratory infections in Africa. Therefore, the aim of this
systematic review and meta-analysis, will be to determine the prevalence of respiratory
Bacterial Aetiologies in people with low Respiratory tract Infections in Africa
(BARIAFRICA) and associated factors.
Methods and analysis
We will search PubMed, EMBASE, Web of Science, Africa Journal Online, and Global Index
Medicus to identify cross-sectional studies that reported the prevalence of respiratory bacterial
infections in people with LRTIs in Africa from January 1, 2000 to March 31st, 2018 without
any linguistic restrictions. Diagnosis of respiratory bacterial infections should be based on
polymerase chain reaction and/or culture. Study selection, data extraction, and
methodological quality assessment will be conducted independently by two investigators. The
heterogeneity will be evaluated using the χ² test on Cochrane’s Q statistic. Prevalence will be
pooled using a random-effect meta-analysis model. Subgroup and meta-regression analyses
will be used to identify sources of heterogeneity of prevalence estimates. This study will be
reported according to the Preferred Reporting Items for Systematic reviews and Meta-
Analyses guidelines.
Ethics and dissemination
Page 2 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
3
Since this study will be based on published data, it does not require ethical approval. This
systematic review and meta-analysis is intended to serve as a basis for determining the burden
of LRTIs, for identifying data gaps and guide future investigations in Africa. The final report
will be published in peer reviewed journals, presented in conferences and submitted to
relevant health policy makers.
Review registration number
PROSPERO, CRD42018092359.
Keywords
Epidemiology; bacteria; lower respiratory tract infections; Africa
Page 3 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
4
Strengths and limitations of this study
- To the best of our knowledge, this work will be the first systematic review and meta-
analysis reporting the prevalence of respiratory bacterial infection in people with lower
respiratory tract infections in Africa.
- This study will inform and guide policy and practice in decision-making and guide
researchers in future investigations in the field of respiratory bacterial infections.
- At least two review authors will independently assess the study selection, data extraction,
and methodological quality evaluation of included studies.
- The study will be limited by the broad spectrum definition of cases of lower respiratory
tract infection according to the authors of included articles.
Page 4 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
5
Introduction
Respiratory tract infections are common conditions among humans, with a high burden in
term of public health.1 Depending on their location, diseases can be divided into upper and
lower respiratory tract infections (LRTIs).2 LRTIs include bronchitis, bronchiolitis and
pneumonia 3, are heavy burden and also cause significant economic losses in underdeveloped
countries and especially those in sub-Saharan Africa.4, 5
A systematic analysis in 2015 found
that LRTIs caused 2.74 million deaths and 103 million disability-adjusted life-years (DALYs)
worldwide, making them the fifth leading cause of death overall and the second-leading cause
of DALYs.6 Apart from Asia, the burden of these infections is supported by sub-Saharan
Africa where highest mortalities are among children under 5. For instance, 546.8 and 511.3
deaths per 100 000 were reported in Somalia and Chad respectively meanwhile the lowest
reported mortalities were in Finland in Western Europe with 0.65 deaths per 100 000.6
Several bacteria have been identified as aetiology in the case LRTI including Streptococcus
pneumoniae (pneumococcus), Haemophilus influenzae, Klebsiella pneumoniae,
Staphylococcus aureus, Acinetobacter species, Streptococcus viridans, Pseudomonas
aeruginosa, Escherichia coli, and Proteus species.6, 7
The epidemiology of LTRIs in Africa
can be specific based on its socio-demographical, environmental, and ecological
specificities. A systematic review performed between 2000 and 2015 showed the prevalence
of respiratory pathogens in children under 5 living in Sub-Saharan African countries.8 Apart
from the fact that the systematic review focused only on children, it did not take in account
data from entire Africa, did not perform a meta-analysis, and quality assessment of the
included articles. To the best of our knowledge there is no previous review which assessed
respiratory bacterial aetiologies in people with LRTIs in Africa. We present here a protocol
for a systematic review and meta-analysis to summarise data on the prevalence of respiratory
Bacterial Aetiologies in people with low Respiratory tract Infections in Africa
Page 5 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
6
(BARIAFRICA), with the aim of providing accurate data for designing cost-effective
interventions to curb the burden of respiratory infections in Africa and guide future research.
Review questions
1. What is the prevalence and distribution of major respiratory bacterial infections among
people with LRTIs living in Africa?
2. What are factors associated with respiratory bacterial infections in people with LRTIs in
Africa?
Method and analysis
Design and registration
This systematic review and meta-analysis protocol will be conducted following Centre for
Reviews and Dissemination guidelines.9 The present BARIAFRICA systematic review and
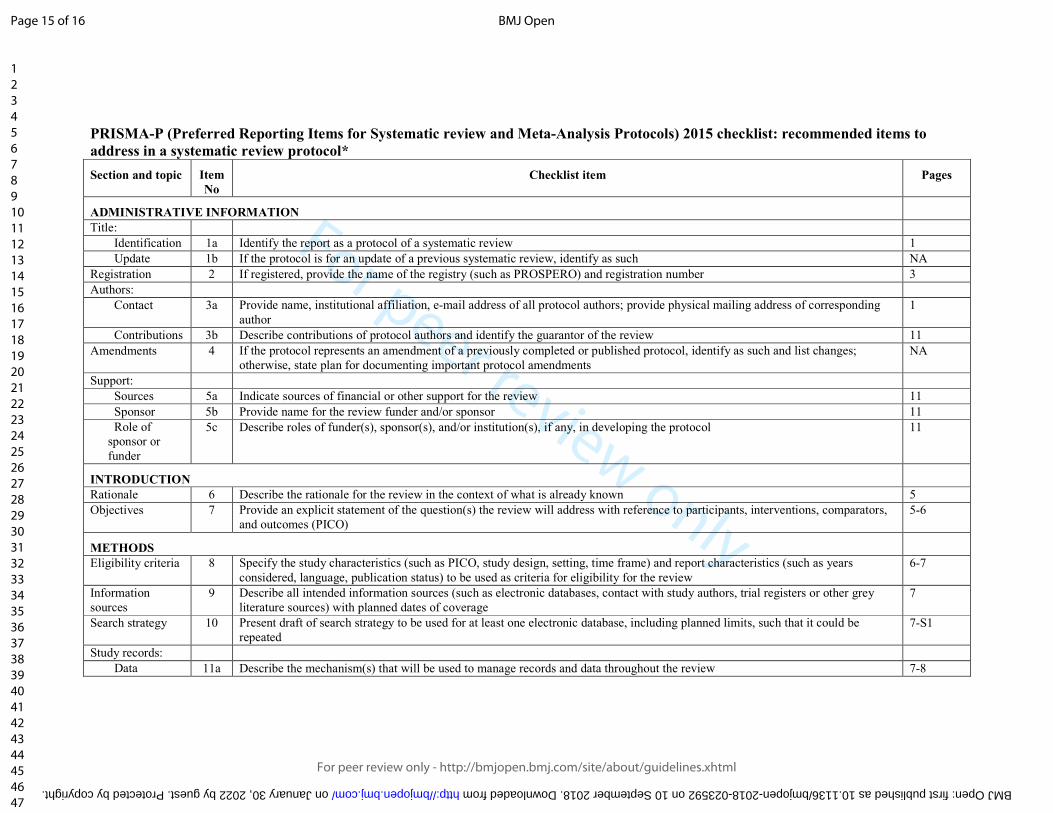
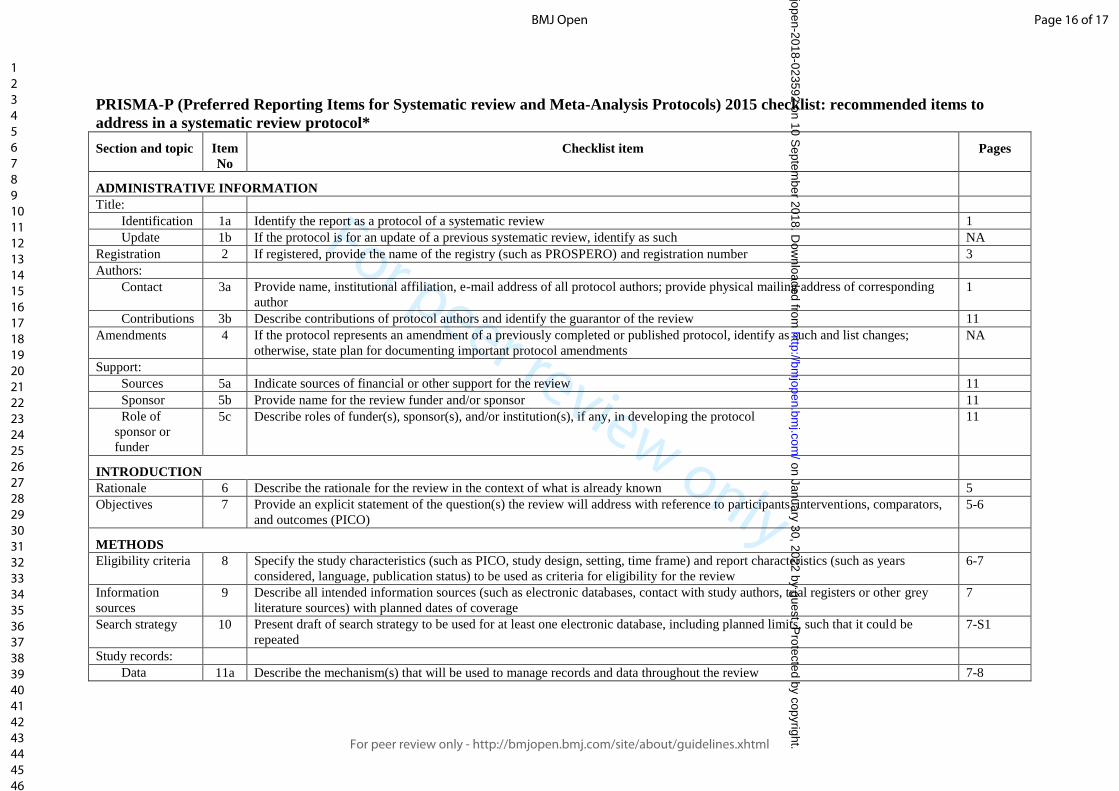
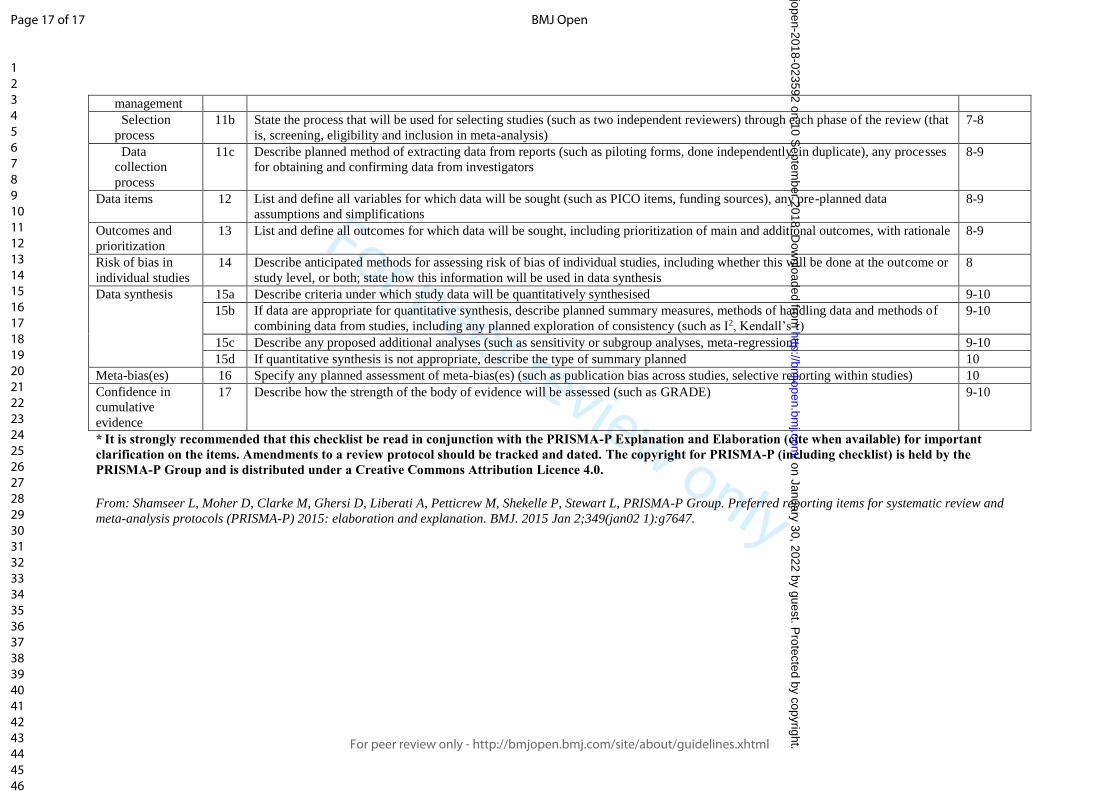
meta-analysis protocol was reported according to Preferred Reporting Items for Systematic
Reviews and Meta-Analysis Protocols (PRISMA-P).10
The study protocol was registered with
PROSPERO, CRD42018092359.
Criteria to consider studies for this review
Inclusion criteria
1. Types of studies: cross-sectional studies.
2. Types of participants: studies conducted in people with LRTIs residing in Africa.
3. Types of outcomes: studies with polymerase chain reaction and bacterial culture used as
tool for the diagnosis respiratory bacterial infections in respiratory samples.
Page 6 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
7
4. Studies that have been published from January 1, 2000 until March 31st, 2018.
5. Studies published regardless of language of publication.
Exclusion criteria
1. Studies in patients with underlying diseases or conditions like pregnant women.
2. Studies conducted during or after outbreak period.
3. Case reports, letters, conference abstracts, comments, editorials, and case series (< 30
participants).
4. Studies with imported cases of respiratory bacterial infections.
5. In case of duplicates, only the study with the largest sample size will be considered.
6. Studies whose full texts are not available or prevalence data are not complete even after
the request to the authors.
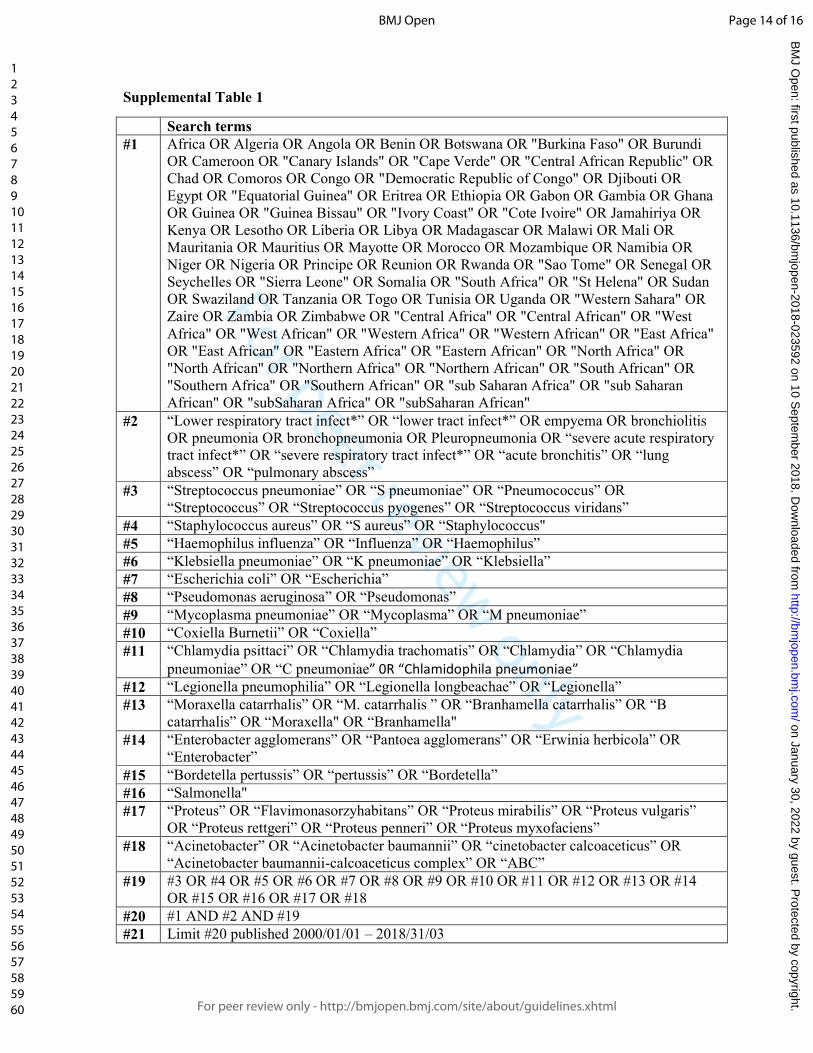
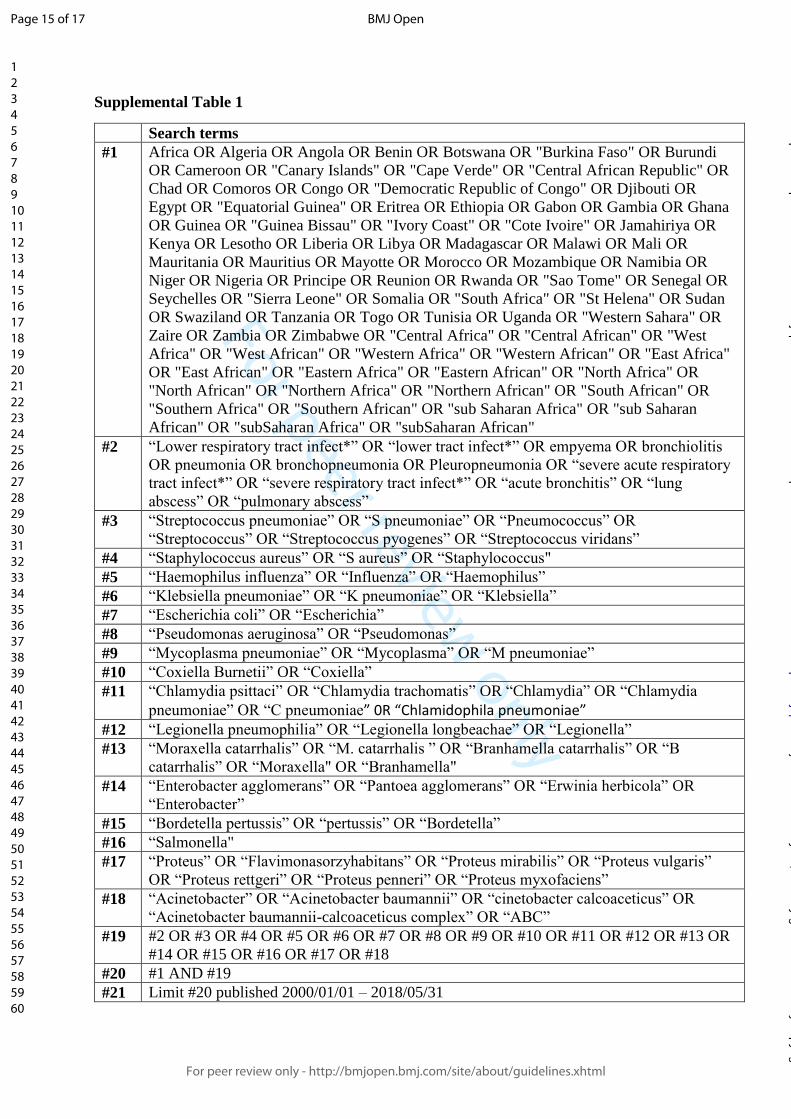
Search strategy for identifying relevant studies
The search strategy including the name of the all African countries and their synonyms will be
applied in electronic databases. The name of the country in the language relevant to that
region will also be applied. Relevant articles will be found by combining the key words in the
field of lower respiratory infections and the names of African sub-regions. The following
databases will be used: PubMed, EMBASE, Web of Science, Africa Journal Online, and
Global Index Medicus. The search strategy in PubMed is presented in the Supplementary
Table 1. The search strategy will be adapted for other databases. The reference list of the
eligible articles and relevant reviews will be manually searched to identify additional studies.
Selection of studies for inclusion in the review
Two review authors using Rayyan application, will independently select records based on the
titles and abstracts. Any disagreement will be solved by consultation and consensus or will
Page 7 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
8
involve a third review author as an arbitrator. Studies in language different of English or
French will be translated using Google Translate and considered for eligibility. Two review
authors will independently evaluate the full text of the selected records. Discrepancies will be
resolved by consensus or by an arbitration of a third review author. The agreement between
the two first review authors will be estimated by Cohen's kappa coefficient.11
Methodological quality and risk of bias assessment
The evaluation of included studies for methodological quality and bias will be done using an
adapted version of the risk of bias tool for prevalence studies developed by Hoy et al.12
Based
on this tool, studies will be rated as low risk, moderate risk and high risk for scores ≤5, 6–8
and >8, respectively. The defined questions will be scored with 0 for no and 1 for yes. The
total score of each article will be calculated by the sum of its points. Discrepancy of
methodological quality assessment among the review authors will be solved by discussion and
consensus or by arbitration of a third review author.
Data extraction and management
Study characteristics such as name of the first author, year of publication, the study
population, number of bacteria searched, age range, study design, diagnostic criteria and
outcomes measured, location, country in which the study was conducted, criteria for sample
selection and sample size, city, latitude, longitude, altitude, clinical presentation, number of
patients tested, number of patients infected with bacteria, diagnostic technique used, and male
proportion will be recorded. Prevalence will be calculated using primary data on the number
of patients tested and the number of cases for each pathogen searched. Prevalence by country
will be calculated for multinational studies. Where cases and sample for estimating prevalence
will not be available, we will contact the corresponding author of the study to request the
missing information. The countries will be grouped in regions according to the United
Page 8 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
9
Nations Statistics Division. Lower respiratory infections will be classified as bronchitis,
bronchiolitis and pneumonia. Data extraction will be done independently by two review
authors. Disagreements between the two review authors will be solved by discussion or will
involve if necessary a third review author for arbitration.
Data synthesis
Data will be analysed using the ‘meta’ and ‘metafor’ packages of the statistical software R
(version 3.4.4, The R Foundation for statistical computing, Vienna, Austria). Unadjusted
prevalence will be recalculated based on the information of crude numerators and
denominators provided by individual studies. Prevalence will be reported with theirs 95%
confidence and prediction intervals. To keep the effect of studies with extremely small or
extremely large prevalence estimates on the overall estimate to a minimum, the variance of
the study-specific prevalence will be stabilized with the Freeman-Tukey double arcsine
transformation before pooling the data with the random-effects meta-analysis model.13
Egger’s test will serve for detecting the presence of publication bias.14
A p-value < 0.10 on
Egger test will be considered indicative of statistically significant publication bias.
Heterogeneity will be evaluated by the χ² test on Cochrane’s Q statistic 15
, which will be
quantified by H and I² values. The I² statistic estimates the percentage of total variation across
studies due to true between-study differences rather than chance. In general, I² values greater
than 60-70% indicate the presence of substantial heterogeneity.16
Subgroup analyses will be performed for the following subgroups: children versus adults and
UNSD African Regions. Univariable and multivariable meta-regression analyses will be used
to test for an effect of study and participants’ characteristics (year of publication, seasonality,
number of screened bacteria, age groups, population, UNSD of regions, absolute latitude
[distance to equator], latitude, longitude, and altitude). To be included in multivariable meta-
Page 9 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
10
regression analysis, a p value < 0.25 in univariable analysis will be required. For categorical
variables, the global p value will be considered for the inclusion in multivariable models. We
will apply a manual backward selection procedure to identify factors independently associated
with the variation of overall prevalence. We successively from the model the less significantly
associated variables. A p value < 0.05 will be considered statistically significant. Following
crude overall prevalence, we will conduct two sensitivity analyses to assess the robustness of
our findings. The first one will include only studies with low risk of bias and the second only
studies reporting data of a full year(s) period (complete season(s)). If it is not possible to
conduct meta-analysis, data will be synthetized using narrative approach.
Potential amendments
We do not plan to make any changes to this protocol. However, if substantial changes occur
during the revision, they will be reported in the published results.
Patient and Public Involvement
Patients and public were not involved in the conception and design of this protocol.
Ethics and dissemination
This work relies on published data and therefore does not require an ethical approval. The
findings will be published in a scientific peer-reviewed journal. They will be also submitted to
conferences and to relevant public health actors.
Conclusions
Page 10 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
11
Taking in account the burden of LRTIs in Africans, the findings from this systematic review
and meta-analysis will be useful for health stakeholders to provide information that can lead
to efficient strategies for controlling the burden of LRTIs in Africa. Different definitions of
LRTIs and inclusion criteria would lead to substantial heterogeneity during meta-analysis.
Authors’ contributions
ST, JJB, SK and RN conceived the protocol and with AN, MSN, VP, and M-CF designed the
protocol. ST, JJB and SK drafted the manuscript. ST, JJB, SK, MSN, AN, VP, M-CF, and RN
revised successive drafts of the manuscript. All authors approved the final version of the
manuscript.
Funding statement
This work received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors
Competing interests statement
The authors declare no competing interest.
References
1. Khan S, Priti S, Ankit S. Bacteria Etiological Agents Causing Lower Respiratory Tract
Infections and Their Resistance Patterns. Iranian biomedical journal 2015; 19(4): 240-6.
2. Neumark T. Treatment of Respiratory Tract Infections in Primary Care with special
emphasis on Acute Otitis Media [Medical Dissertations]. Sweden Linköping University;
2010.
Page 11 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
12
3. Kocsis B, Szabo D. New treatment options for lower respiratory tract infections.
Expert opinion on pharmacotherapy 2017; 18(13): 1345-55.
4. Organization WH. Estimating the burden of respiratory diseases. Practical Approach
to Lung Health: Manual on Initiating PAL Implementation. Geneva; 2008: 138.
5. Bates M, Mudenda V, Mwaba P, Zumla A. Deaths due to respiratory tract infections in
Africa: a review of autopsy studies. Current opinion in pulmonary medicine 2013; 19(3): 229-
37.
6. Collaborators GL. Estimates of the global, regional, and national morbidity, mortality,
and aetiologies of lower respiratory tract infections in 195 countries: a systematic analysis for
the Global Burden of Disease Study 2015. The Lancet Infectious diseases 2017; 17(11): 1133-
61.
7. Uzoamaka M, Ngozi O, Johnbull OS, Martin O. Bacterial Etiology of Lower
Respiratory Tract Infections and Their Antimicrobial Susceptibility. Am J Med Sci 2017;
354(5): 471.
8. Armel Moumouni Sanou, Assana Cissé, Tieba Millogo, et al. Systematic Review of
Articles on Etiologies of Acute Respiratory Infections in Children Aged Less Than Five Years
in Sub-Saharan Africa, 2000-2015. EC Microbiology 2016; 3.6: 556-71.
9. Dissemination CfRa. CRD’s guidance for undertaking reviews in healthcare: centers
for reviews and dissemination; 2009.
10. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review
and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic reviews 2015; 4: 1.
11. Viera AJ, Garrett JM. Understanding interobserver agreement: the kappa statistic.
Family medicine 2005; 37(5): 360-3.
12. Hoy D, Brooks P, Woolf A, et al. Assessing risk of bias in prevalence studies:
modification of an existing tool and evidence of interrater agreement. Journal of clinical
epidemiology 2012; 65(9): 934-9.
13. Barendregt JJ, Doi SA, Lee YY, Norman RE, Vos T. Meta-analysis of prevalence.
Journal of epidemiology and community health 2013; 67(11): 974-8.
14. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a
simple, graphical test. BMJ (Clinical research ed) 1997; 315(7109): 629-34.
15. Cochran WG. The Combination of Estimates from Different Experiments. Biometrics
1954; 10(1): 101-29.
16. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Statistics in
medicine 2002; 21(11): 1539-58.
Page 12 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
13
Page 13 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
Supplemental Table 1
Search terms
#1 Africa OR Algeria OR Angola OR Benin OR Botswana OR "Burkina Faso" OR Burundi
OR Cameroon OR "Canary Islands" OR "Cape Verde" OR "Central African Republic" OR
Chad OR Comoros OR Congo OR "Democratic Republic of Congo" OR Djibouti OR
Egypt OR "Equatorial Guinea" OR Eritrea OR Ethiopia OR Gabon OR Gambia OR Ghana
OR Guinea OR "Guinea Bissau" OR "Ivory Coast" OR "Cote Ivoire" OR Jamahiriya OR
Kenya OR Lesotho OR Liberia OR Libya OR Madagascar OR Malawi OR Mali OR
Mauritania OR Mauritius OR Mayotte OR Morocco OR Mozambique OR Namibia OR
Niger OR Nigeria OR Principe OR Reunion OR Rwanda OR "Sao Tome" OR Senegal OR
Seychelles OR "Sierra Leone" OR Somalia OR "South Africa" OR "St Helena" OR Sudan
OR Swaziland OR Tanzania OR Togo OR Tunisia OR Uganda OR "Western Sahara" OR
Zaire OR Zambia OR Zimbabwe OR "Central Africa" OR "Central African" OR "West
Africa" OR "West African" OR "Western Africa" OR "Western African" OR "East Africa"
OR "East African" OR "Eastern Africa" OR "Eastern African" OR "North Africa" OR
"North African" OR "Northern Africa" OR "Northern African" OR "South African" OR
"Southern Africa" OR "Southern African" OR "sub Saharan Africa" OR "sub Saharan
African" OR "subSaharan Africa" OR "subSaharan African"
#2 “Lower respiratory tract infect*” OR “lower tract infect*” OR empyema OR bronchiolitis
OR pneumonia OR bronchopneumonia OR Pleuropneumonia OR “severe acute respiratory
tract infect*” OR “severe respiratory tract infect*” OR “acute bronchitis” OR “lung
abscess” OR “pulmonary abscess”
#3 “Streptococcus pneumoniae” OR “S pneumoniae” OR “Pneumococcus” OR
“Streptococcus” OR “Streptococcus pyogenes” OR “Streptococcus viridans”
#4 “Staphylococcus aureus” OR “S aureus” OR “Staphylococcus"
#5 “Haemophilus influenza” OR “Influenza” OR “Haemophilus”
#6 “Klebsiella pneumoniae” OR “K pneumoniae” OR “Klebsiella”
#7 “Escherichia coli” OR “Escherichia”
#8 “Pseudomonas aeruginosa” OR “Pseudomonas”
#9 “Mycoplasma pneumoniae” OR “Mycoplasma” OR “M pneumoniae”
#10 “Coxiella Burnetii” OR “Coxiella”
#11 “Chlamydia psittaci” OR “Chlamydia trachomatis” OR “Chlamydia” OR “Chlamydia
pneumoniae” OR “C pneumoniae” 0R “Chlamidophila pneumoniae”
#12 “Legionella pneumophilia” OR “Legionella longbeachae” OR “Legionella”
#13 “Moraxella catarrhalis” OR “M. catarrhalis ” OR “Branhamella catarrhalis” OR “B
catarrhalis” OR “Moraxella" OR “Branhamella"
#14 “Enterobacter agglomerans” OR “Pantoea agglomerans” OR “Erwinia herbicola” OR
“Enterobacter”
#15 “Bordetella pertussis” OR “pertussis” OR “Bordetella”
#16 “Salmonella"
#17 “Proteus” OR “Flavimonasorzyhabitans” OR “Proteus mirabilis” OR “Proteus vulgaris”
OR “Proteus rettgeri” OR “Proteus penneri” OR “Proteus myxofaciens”
#18 “Acinetobacter” OR “Acinetobacter baumannii” OR “cinetobacter calcoaceticus” OR
“Acinetobacter baumannii-calcoaceticus complex” OR “ABC”
#19 #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14
OR #15 OR #16 OR #17 OR #18
#20 #1 AND #2 AND #19
#21 Limit #20 published 2000/01/01 – 2018/31/03
Page 14 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
PRISMA-P (Preferred Reporting Items for Systematic review and Meta-Analysis Protocols) 2015 checklist: recommended items to
address in a systematic review protocol*
Section and topic Item
No
Checklist item Pages
ADMINISTRATIVE INFORMATION
Title:
Identification 1a Identify the report as a protocol of a systematic review 1
Update 1b If the protocol is for an update of a previous systematic review, identify as such NA
Registration 2 If registered, provide the name of the registry (such as PROSPERO) and registration number 3
Authors:
Contact 3a Provide name, institutional affiliation, e-mail address of all protocol authors; provide physical mailing address of corresponding
author
1
Contributions 3b Describe contributions of protocol authors and identify the guarantor of the review 11
Amendments 4 If the protocol represents an amendment of a previously completed or published protocol, identify as such and list changes;
otherwise, state plan for documenting important protocol amendments
NA
Support:
Sources 5a Indicate sources of financial or other support for the review 11
Sponsor 5b Provide name for the review funder and/or sponsor 11
Role of
sponsor or
funder
5c Describe roles of funder(s), sponsor(s), and/or institution(s), if any, in developing the protocol 11
INTRODUCTION
Rationale 6 Describe the rationale for the review in the context of what is already known 5
Objectives 7 Provide an explicit statement of the question(s) the review will address with reference to participants, interventions, comparators,
and outcomes (PICO)
5-6
METHODS
Eligibility criteria 8 Specify the study characteristics (such as PICO, study design, setting, time frame) and report characteristics (such as years
considered, language, publication status) to be used as criteria for eligibility for the review
6-7
Information
sources
9 Describe all intended information sources (such as electronic databases, contact with study authors, trial registers or other grey
literature sources) with planned dates of coverage
7
Search strategy 10 Present draft of search strategy to be used for at least one electronic database, including planned limits, such that it could be
repeated
7-S1
Study records:
Data 11a Describe the mechanism(s) that will be used to manage records and data throughout the review 7-8
Page 15 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2018-023592 on 10 September 2018. Downloaded from

For peer review only
management
Selection
process
11b State the process that will be used for selecting studies (such as two independent reviewers) through each phase of the review (that
is, screening, eligibility and inclusion in meta-analysis)
7-8
Data
collection
process
11c Describe planned method of extracting data from reports (such as piloting forms, done independently, in duplicate), any processes
for obtaining and confirming data from investigators
8-9
Data items 12 List and define all variables for which data will be sought (such as PICO items, funding sources), any pre-planned data
assumptions and simplifications
8-9
Outcomes and
prioritization
13 List and define all outcomes for which data will be sought, including prioritization of main and additional outcomes, with rationale 8-9
Risk of bias in
individual studies
14 Describe anticipated methods for assessing risk of bias of individual studies, including whether this will be done at the outcome or
study level, or both; state how this information will be used in data synthesis
8
Data synthesis 15a Describe criteria under which study data will be quantitatively synthesised 9-10
15b If data are appropriate for quantitative synthesis, describe planned summary measures, methods of handling data and methods of
combining data from studies, including any planned exploration of consistency (such as I2, Kendall’s τ)
9-10
15c Describe any proposed additional analyses (such as sensitivity or subgroup analyses, meta-regression) 9-10
15d If quantitative synthesis is not appropriate, describe the type of summary planned 10
Meta-bias(es) 16 Specify any planned assessment of meta-bias(es) (such as publication bias across studies, selective reporting within studies) 10
Confidence in
cumulative
evidence
17 Describe how the strength of the body of evidence will be assessed (such as GRADE) 9-10
* It is strongly recommended that this checklist be read in conjunction with the PRISMA-P Explanation and Elaboration (cite when available) for important
clarification on the items. Amendments to a review protocol should be tracked and dated. The copyright for PRISMA-P (including checklist) is held by the
PRISMA-P Group and is distributed under a Creative Commons Attribution Licence 4.0.
From: Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart L, PRISMA-P Group. Preferred reporting items for systematic review and
meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015 Jan 2;349(jan02 1):g7647.
Page 16 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2018-023592 on 10 September 2018. Downloaded from

For peer review only
Prevalence of respiratory bacterial infections in people with
lower respiratory tract infections in Africa: The BARIAFRICA
systematic review and meta-analysis protocol
Journal: BMJ Open
Manuscript ID bmjopen-2018-023592.R1
Article Type: Protocol
Date Submitted by the Author: 08-Jun-2018
Complete List of Authors: Tchatchouang, Serges; Centre Pasteur of Cameroon, Department of Virology; Faculty of Sciences, University of Yaoundé I, Department of Biochemistry Bigna, Jean Joel; Centre Pasteur of Cameroon, Department of Epidemiology and Public Health Nzouankeu, Ariane; Centre Pasteur of Cameroon, Department of Bacteriology Fonkoua, Marie-Christine; Centre Pasteur of Cameroon, Department of Bacteriology Nansseu, Jobert Richie; Mother and Child Centre, Chantal Biya Foundation, Sickle cell unit Ndangang, Marie; Rouen University Hospital, Department of Medical Information and Informatics Kenmoe, Sebastien; Centre Pasteur of Cameroon, Department of Virology Penlap, Véronique; Faculty of Sciences, University of Yaoundé I, Department of Biochemistry Njouom, Richard; Centre Pasteur of Cameroon, Department of Virology
<b>Primary Subject Heading</b>:
Infectious diseases
Secondary Subject Heading: Epidemiology, Global health, Public health, Respiratory medicine
Keywords: Epidemiology < INFECTIOUS DISEASES, Respiratory infections < THORACIC MEDICINE, Epidemiology < THORACIC MEDICINE, Epidemiology < TROPICAL MEDICINE
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on January 30, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-023592 on 10 S
eptember 2018. D
ownloaded from
For peer review only
1
Prevalence of respiratory bacterial infections in people with lower
respiratory tract infections in Africa: The BARIAFRICA systematic review
and meta-analysis protocol
Serges Tchatchouang1, 2, 3
, Jean Joel Bigna4, Ariane Nzouankeu
1, Marie-Christine Fonkoua
1,
Jobert Richie Nansseu5, Marie S. Ndangang
5, Sébastien Kenmoe
2, Véronique B. Penlap
3,
Richard Njouom2*
1. Department of Bacteriology, Centre Pasteur of Cameroon, Member of the International
Network of Pasteur Institutes, P.O. Box 1274, Yaoundé, Cameroon
2. Department of Virology, Centre Pasteur of Cameroon, Member of the International
Network of Pasteur Institutes, P.O. Box 1274, Yaoundé, Cameroon
3. Department of Biochemistry, Faculty of Sciences, University of Yaoundé I, Yaoundé,
Cameroon
4. Department of Epidemiology and Public Health, Centre Pasteur of Cameroon, Member of
the International Network of Pasteur Institutes, P.O. Box 1274, Yaoundé, Cameroon
5. Department of Public Health, Faculty of Medicine and Biomedical Sciences, University of
Yaoundé I, Yaoundé, Cameroon
6. Department of Medical Information and Informatics, Rouen University Hospital, Rouen,
France
Email addresses: ST ([email protected]), JJB ([email protected]), AN
([email protected]), VP ([email protected]), M-CF (fonkoua@pasteur-
yaounde.org), MSN ([email protected]), SK ([email protected]), RN
* Corresponding author: Department of Virology, Centre Pasteur of Cameroon, Member of
the International Network of Pasteur Institutes, 451 Street 2005, P.O. Box 1274, Yaoundé II,
Yaoundé, Cameroon. E-mail: [email protected]
Page 1 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
2
Abstract
Introduction
The burden of lower respiratory tract infections (LRTIs) is a substantial public health concern.
However, epidemiology of LRTIs and its bacterial aetiologies are poorly characterized,
particularly in the African continent. Providing accurate data can help design cost-effective
interventions to curb the burden of respiratory infections in Africa. Therefore, the aim of this
systematic review and meta-analysis, will be to determine the prevalence of respiratory
Bacterial Aetiologies in people with low Respiratory tract Infections in Africa
(BARIAFRICA) and associated factors.
Methods and analysis
We will search PubMed, EMBASE, Web of Science, Africa Journal Online, CINAHL, and
Global Index Medicus to identify studies that reported the prevalence (of enough data to
compute this estimate) of respiratory bacterial infections in people with LRTIs in Africa from
January 1, 2000 to March 31st, 2018 without any linguistic restrictions. Study selection, data
extraction, and risk of bias assessment will be conducted independently by two investigators.
The heterogeneity will be evaluated using the χ² test on Cochrane’s Q statistic and quantified
with H and I² statistics. Prevalence will be pooled using a random-effect meta-analysis
model. Subgroup and meta-regression analyses will be used to identify sources of
heterogeneity of prevalence estimates. This study will be reported according to the Preferred
Reporting Items for Systematic reviews and Meta-Analyses guidelines.
Ethics and dissemination
Since this study will be based on published data, it does not require ethical approval. This
systematic review and meta-analysis is intended to serve as a basis for determining the burden
Page 2 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
3
of LRTIs, for identifying data gaps and guide future investigations in Africa. The final report
will be published in peer reviewed journals, presented in conferences and submitted to
relevant health policy makers.
Review registration number
PROSPERO, CRD42018092359.
Keywords
Epidemiology; bacteria; lower respiratory tract infections; Africa
Page 3 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
4
Strengths and limitations of this study
- To the best of our knowledge, this work will be the first systematic review and meta-
analysis reporting the prevalence of respiratory bacterial infection in people with lower
respiratory tract infections in Africa.
- This study will inform and guide policy and practice in decision-making and guide
researchers in future investigations in the field of respiratory bacterial infections.
- Two review authors will independently assess the study selection, data extraction, and risk
of bias in included studies.
- The study will be limited by the broad spectrum definition of cases of lower respiratory
tract infection according to the authors of included articles.
Page 4 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
5
Introduction
Respiratory tract infections are common conditions among humans, with a high burden in
term of public health.1 Depending on their location, diseases can be divided into upper and
lower respiratory tract infections (LRTIs).2 LRTIs including bronchitis, bronchiolitis and
pneumonia3 are heavy burden and also cause significant economic losses in developing
countries and especially those in sub-Saharan Africa.4 5
In sub-Saharan Africa, LRTIs rank at
the third place after HIV/AIDS and malaria in terms of causes of mortality. LTRIs is the first
cause of deaths in 9 African countries.6 A systematic analysis in 2015 found that LRTIs
caused 2.74 million deaths and 103 million disability-adjusted life-years (DALYs) worldwide,
making them the fifth leading cause of death overall and the second-leading cause of
DALYs.7 The burden of these infections is supported by sub-Saharan Africa and Asia where
highest mortality are among children under 5. For instance, 546.8 and 511.3 deaths per
100000 were reported in Somalia and Chad respectively meanwhile the lowest reported
mortality were in Finland in Western Europe with 0.65 deaths per 100000.7 Several bacteria
have been identified as aetiology of LRTIs including Streptococcus pneumoniae
(pneumococcus), Haemophilus influenzae, Klebsiella pneumoniae, Staphylococcus aureus,
Acinetobacter species, Streptococcus viridans, Pseudomonas aeruginosa, Escherichia coli,
and Proteus species.7 8
The epidemiology of LTRIs in Africa can be specific based on its
socio-demographical, environmental, and ecological specificities. A systematic review
performed between 2000 and 2015 showed the prevalence of respiratory pathogens in
children under 5 living in Sub-Saharan African countries.9 Apart from the fact that the
systematic review focused only on children, it did not take in account data from entire Africa,
did not perform any meta-analysis of the included studies. To the best of our knowledge there
is no previous review which assessed respiratory bacterial aetiologies in people with LRTIs in
Africa. We present here a protocol for a systematic review and meta-analysis to summarise
Page 5 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
6
data on the prevalence of respiratory Bacterial Aetiologies in people with low Respiratory
tract Infections in Africa (BARIAFRICA), with the aim to provide accurate data for designing
cost-effective interventions to curb the burden of respiratory infections in Africa and guide
future research.
Review questions
1. What is the prevalence and distribution of respiratory bacterial infections among people
with LRTIs living in Africa?
2. What are sources of heterogeneity of the prevalence of respiratory bacterial infections in
people with LRTIs in Africa?
Method and analysis
Design and registration
This systematic review and meta-analysis protocol will be conducted following Centre for
Reviews and Dissemination guidelines.10
The present BARIAFRICA systematic review and
meta-analysis protocol was reported according to Preferred Reporting Items for Systematic
Reviews and Meta-Analysis Protocols (PRISMA-P).11
The study protocol was registered with
PROSPERO, CRD42018092359.
Criteria to consider studies for this review
Inclusion criteria
Page 6 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
7
1. Types of studies. We will consider cross-sectional studies, case-control studies, baseline
data of cohort studies, surveillance data, as well as control group (without any
intervention) of clinical trials.
2. Types of participants. We will consider studies conducted in people with clinically
diagnosed LRTIs residing in Africa regardless of age group and settings. LRTIs had to be
diagnosed by a physician.
3. Types of outcomes. We will consider studies reporting the prevalence of respiratory
bacterial infections regardless of laboratory diagnostic technique used (or enough data to
compute this estimate). Prevalence will be calculated as number of a respiratory bacterial
infection on number of people with LRTI among which specific bacteria were searched.
4. Studies that have been published from January 1st, 2000 until March 31
st, 2018.
5. Studies published regardless of language of publication.
Exclusion criteria
1. Studies conducted during or after outbreak period.
2. Case reports, letters, conference abstracts, comments, editorials, and case series (< 30
participants).
3. Studies with imported cases of respiratory bacterial infections.
Search strategy for identifying relevant studies
The search strategy including the name of the all African countries and their synonyms will be
applied in electronic databases. The name of the country in the language relevant to that
region will also be applied. Relevant articles will be found by combining the key words in the
field of lower respiratory infections and the names of African sub-regions. The following
databases will be used: Medline through PubMed, EMBASE, Web of Science, CINAHL,
Africa Journal Online, and Global Index Medicus. The search strategy in PubMed is presented
Page 7 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from

For peer review only
8
in the Supplementary Table 1. The search strategy will be adapted for other databases. The
reference list of the eligible articles and relevant reviews will be manually searched to identify
additional studies.
Selection of studies for inclusion in the review
Two review authors using the Rayyan application,12
will independently select records based
on the titles and abstracts. Any disagreement will be solved by discussion and consensus or
will involve a third review author as an arbitrator. Studies in language different of English or
French will be translated using Google Translate and considered for eligibility. Two review
authors will independently evaluate the full text of the selected records. Discrepancies will be
resolved by consensus or by an arbitration of a third review author. The agreement between
the two first review authors will be estimated by Cohen's kappa coefficient.13
Risk of bias assessment
The evaluation of included studies for risk bias will be done using an adapted version of the
risk of bias tool for prevalence studies developed by Hoy et al.14
Based on this tool, studies
will be rated as low risk, moderate risk and high risk for scores ≤5, 6–8 and >8, respectively.
The defined questions will be scored with 0 for no and 1 for yes. The total score of each
article will be calculated by the sum of its points. Discrepancy of risk of bias assessment
among the review authors will be solved by discussion and consensus or by arbitration of a
third review author.
Data extraction and management
Study characteristics such as name of the first author, year of publication, the study
population, number of bacteria searched, age range, study design, setting, diagnostic criteria
and outcomes measured, location, country in which the study was conducted, criteria for
Page 8 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
9
sample selection and sample size, city, latitude, longitude, altitude, clinical presentation,
number of clinical isolates, comorbid conditions/underlying conditions, number of patients
tested, number of patients infected with bacteria, diagnostic technique used, and male
proportion will be recorded. Prevalence by country will be calculated for multinational
studies. Where cases and sample for estimating prevalence will not be available, we will
contact the corresponding author of the study to request the missing information. The
countries will be grouped in regions according to the United Nations Statistics
Division. Lower respiratory infections will be classified as bronchitis, bronchiolitis and
pneumonia. Data extraction will be done independently by two review authors. Disagreements
between the two review authors will be solved by discussion or will involve if necessary a
third review author for arbitration.
Data synthesis
Data will be analysed using the ‘meta’ and ‘metafor’ packages of the statistical software R
(version 3.4.4, The R Foundation for statistical computing, Vienna, Austria). Unadjusted
prevalence will be recalculated based on the information of crude numerators and
denominators provided by individual studies. Prevalence will be reported with theirs 95%
confidence and prediction intervals. To keep the effect of studies with extremely small or
extremely large prevalence estimates on the overall estimate to a minimum, the variance of
the study-specific prevalence will be stabilized with the Freeman-Tukey double arcsine
transformation before pooling the data with the random-effects meta-analysis model.15
Only
studies conducted in populations with close clinical presentation/underlying conditions and
with same laboratory diagnostic technique will be pooled together. If it is not possible to
conduct meta-analysis, data will be synthetized using a narrative approach. Egger’s test will
serve for detecting the presence of publication bias.16
A p-value < 0.10 on Egger test will be
considered indicative of statistically significant publication bias. Heterogeneity will be
Page 9 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
10
evaluated by the χ² test on Cochrane’s Q statistic 17
, which will be quantified by H and I²
values. The I² statistic estimates the percentage of total variation across studies due to true
between-study differences rather than chance. In general, I² values greater than 60-70%
indicate the presence of substantial heterogeneity.18
In the case of substantial heterogeneity, subgroup and meta-regression analyses will be used
to investigate sources of heterogeneity. Subgroup analyses will be performed for the
following subgroups: children versus adults, UNSD African Regions, level of country
income, clinical presentation, setting (primary care, intensive care and emergency units,
inpatients, outpatients) and study period of inclusion. Univariable and multivariable meta-
regression analyses will be used to test for an effect of study and participants’ characteristics
(year of publication, seasonality, setting, clinical presentation, comorbid conditions, number
of screened bacteria, age groups, population, UNSD of regions, absolute latitude [distance to
equator], latitude, longitude, and altitude). To be included in multivariable meta-regression
analysis, a p value < 0.25 in univariable analysis will be required. For categorical variables,
the global p value will be considered for the inclusion in multivariable models. We will apply
a manual forward selection procedure to identify factors independently associated with the
variation of the overall prevalence. We will successively add in the model the more
significantly associated variables. The final model that will be considered is the one with
lowest Bayesian Information Criterion. A p value < 0.05 will be considered statistically
significant. Following crude overall prevalence, we will conduct two sensitivity analyses to
assess the robustness of our findings. The first one will include only studies with low risk of
bias and the second only studies reporting data of a full year(s) period (complete season(s)).
Potential amendments
Page 10 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
11
We do not plan to make any changes to this protocol. However, if substantial changes occur
during the review, they will be reported in the published results.
Patient and Public Involvement
Patients and public were not involved in the conception and design of this protocol.
Ethics and dissemination
This work relies on published data and therefore does not require an ethical approval. The
findings will be published in a scientific peer-reviewed journal. They will be also submitted to
conferences and to relevant public health actors.
Conclusions
Taking in account the burden of LRTIs in Africans, the findings from this systematic review
and meta-analysis will be useful for health stakeholders to provide information that can lead
to efficient strategies for controlling the burden of LRTIs in Africa. As all settings in Africa
are not able to diagnose bacterial aetiologies in people with LRTI, knowledge of major
respiratory bacterial infections can help in this case to orientate the first line treatment.
Different definitions of LRTIs and inclusion criteria would lead to substantial heterogeneity
during meta-analysis.
Authors’ contributions
ST, JJB, SK and RN conceived the protocol and with AN, MSN, VP, and M-CF designed the
protocol. ST, JJB and SK drafted the manuscript. ST, JJB, SK, MSN, AN, VP, M-CF, and RN
Page 11 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
12
revised successive drafts of the manuscript. All authors approved the final version of the
manuscript.
Funding statement
This work received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors
Competing interests statement
The authors declare no competing interest.
References
1. Khan S, Priti S, Ankit S. Bacteria Etiological Agents Causing Lower Respiratory Tract
Infections and Their Resistance Patterns. Iranian biomedical journal 2015;19(4):240-
6. [published Online First: 2015/07/30]
2. Neumark T. Treatment of Respiratory Tract Infections in Primary Care with special
emphasis on Acute Otitis Media [Medical Dissertations]. Linköping University, 2010.
3. Kocsis B, Szabo D. New treatment options for lower respiratory tract infections. Expert
opinion on pharmacotherapy 2017;18(13):1345-55. doi:
10.1080/14656566.2017.1363179 [published Online First: 2017/08/02]
4. WHO. Estimating the burden of respiratory diseases. Practical Approach to Lung Health:
Manual on Initiating PAL Implementation. Geneva 2008:138.
5. Bates M, Mudenda V, Mwaba P, et al. Deaths due to respiratory tract infections in Africa: a
review of autopsy studies. Current opinion in pulmonary medicine 2013;19(3):229-37.
doi: 10.1097/MCP.0b013e32835f4fe4 [published Online First: 2013/02/23]
6. Global, regional, and national age-sex specific all-cause and cause-specific mortality for
240 causes of death, 1990-2013: a systematic analysis for the Global Burden of
Disease Study 2013. Lancet (London, England) 2015;385(9963):117-71. doi:
10.1016/s0140-6736(14)61682-2 [published Online First: 2014/12/23]
Page 12 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
13
7. Global Burden Disease Collaborators. Estimates of the global, regional, and national
morbidity, mortality, and aetiologies of lower respiratory tract infections in 195
countries: a systematic analysis for the Global Burden of Disease Study 2015. The
Lancet Infectious diseases 2017;17(11):1133-61. doi: 10.1016/s1473-3099(17)30396-
1 [published Online First: 2017/08/28]
8. Uzoamaka M, Ngozi O, Johnbull OS, et al. Bacterial Etiology of Lower Respiratory Tract
Infections and Their Antimicrobial Susceptibility. Am J Med Sci 2017;354(5):471. doi:
10.1016/j.amjms.2017.06.025
9. Armel Moumouni Sanou, Assana Cissé, Tieba Millogo, et al. Systematic Review of
Articles on Etiologies of Acute Respiratory Infections in Children Aged Less Than
Five Years in Sub-Saharan Africa, 2000-2015. EC Microbiology 2016;3.6:556-71.
10. CRD’s guidance for undertaking reviews in healthcare: centers for reviews and
dissemination 2009.
11. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review
and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic reviews
2015;4:1. doi: 10.1186/2046-4053-4-1 [published Online First: 2015/01/03]
12. Ouzzani M, Hammady H, Fedorowicz Z, et al. Rayyan-a web and mobile app for
systematic reviews. Systematic reviews 2016;5(1):210. doi: 10.1186/s13643-016-
0384-4 [published Online First: 2016/12/07]
13. Viera AJ, Garrett JM. Understanding interobserver agreement: the kappa statistic. Family
medicine 2005;37(5):360-3. [published Online First: 2005/05/11]
14. Hoy D, Brooks P, Woolf A, et al. Assessing risk of bias in prevalence studies:
modification of an existing tool and evidence of interrater agreement. Journal of
clinical epidemiology 2012;65(9):934-9. doi: 10.1016/j.jclinepi.2011.11.014
[published Online First: 2012/06/30]
15. Barendregt JJ, Doi SA, Lee YY, et al. Meta-analysis of prevalence. Journal of
epidemiology and community health 2013;67(11):974-8. doi: 10.1136/jech-2013-
203104 [published Online First: 2013/08/22]
16. Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple,
graphical test. BMJ (Clinical research ed) 1997;315(7109):629-34. [published Online
First: 1997/10/06]
17. Cochran WG. The Combination of Estimates from Different Experiments. Biometrics
1954;10(1):101-29. doi: 10.2307/3001666
Page 13 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
14
18. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Statistics in
medicine 2002;21(11):1539-58. doi: 10.1002/sim.1186 [published Online First:
2002/07/12]
Page 14 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
Supplemental Table 1
Search terms
#1 Africa OR Algeria OR Angola OR Benin OR Botswana OR "Burkina Faso" OR Burundi
OR Cameroon OR "Canary Islands" OR "Cape Verde" OR "Central African Republic" OR
Chad OR Comoros OR Congo OR "Democratic Republic of Congo" OR Djibouti OR
Egypt OR "Equatorial Guinea" OR Eritrea OR Ethiopia OR Gabon OR Gambia OR Ghana
OR Guinea OR "Guinea Bissau" OR "Ivory Coast" OR "Cote Ivoire" OR Jamahiriya OR
Kenya OR Lesotho OR Liberia OR Libya OR Madagascar OR Malawi OR Mali OR
Mauritania OR Mauritius OR Mayotte OR Morocco OR Mozambique OR Namibia OR
Niger OR Nigeria OR Principe OR Reunion OR Rwanda OR "Sao Tome" OR Senegal OR
Seychelles OR "Sierra Leone" OR Somalia OR "South Africa" OR "St Helena" OR Sudan
OR Swaziland OR Tanzania OR Togo OR Tunisia OR Uganda OR "Western Sahara" OR
Zaire OR Zambia OR Zimbabwe OR "Central Africa" OR "Central African" OR "West
Africa" OR "West African" OR "Western Africa" OR "Western African" OR "East Africa"
OR "East African" OR "Eastern Africa" OR "Eastern African" OR "North Africa" OR
"North African" OR "Northern Africa" OR "Northern African" OR "South African" OR
"Southern Africa" OR "Southern African" OR "sub Saharan Africa" OR "sub Saharan
African" OR "subSaharan Africa" OR "subSaharan African"
#2 “Lower respiratory tract infect*” OR “lower tract infect*” OR empyema OR bronchiolitis
OR pneumonia OR bronchopneumonia OR Pleuropneumonia OR “severe acute respiratory
tract infect*” OR “severe respiratory tract infect*” OR “acute bronchitis” OR “lung
abscess” OR “pulmonary abscess”
#3 “Streptococcus pneumoniae” OR “S pneumoniae” OR “Pneumococcus” OR
“Streptococcus” OR “Streptococcus pyogenes” OR “Streptococcus viridans”
#4 “Staphylococcus aureus” OR “S aureus” OR “Staphylococcus"
#5 “Haemophilus influenza” OR “Influenza” OR “Haemophilus”
#6 “Klebsiella pneumoniae” OR “K pneumoniae” OR “Klebsiella”
#7 “Escherichia coli” OR “Escherichia”
#8 “Pseudomonas aeruginosa” OR “Pseudomonas”
#9 “Mycoplasma pneumoniae” OR “Mycoplasma” OR “M pneumoniae”
#10 “Coxiella Burnetii” OR “Coxiella”
#11 “Chlamydia psittaci” OR “Chlamydia trachomatis” OR “Chlamydia” OR “Chlamydia
pneumoniae” OR “C pneumoniae” 0R “Chlamidophila pneumoniae”
#12 “Legionella pneumophilia” OR “Legionella longbeachae” OR “Legionella”
#13 “Moraxella catarrhalis” OR “M. catarrhalis ” OR “Branhamella catarrhalis” OR “B
catarrhalis” OR “Moraxella" OR “Branhamella"
#14 “Enterobacter agglomerans” OR “Pantoea agglomerans” OR “Erwinia herbicola” OR
“Enterobacter”
#15 “Bordetella pertussis” OR “pertussis” OR “Bordetella”
#16 “Salmonella"
#17 “Proteus” OR “Flavimonasorzyhabitans” OR “Proteus mirabilis” OR “Proteus vulgaris”
OR “Proteus rettgeri” OR “Proteus penneri” OR “Proteus myxofaciens”
#18 “Acinetobacter” OR “Acinetobacter baumannii” OR “cinetobacter calcoaceticus” OR
“Acinetobacter baumannii-calcoaceticus complex” OR “ABC”
#19 #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR
#14 OR #15 OR #16 OR #17 OR #18
#20 #1 AND #19
#21 Limit #20 published 2000/01/01 – 2018/05/31
Page 15 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
PRISMA-P (Preferred Reporting Items for Systematic review and Meta-Analysis Protocols) 2015 checklist: recommended items to
address in a systematic review protocol*
Section and topic Item
No
Checklist item Pages
ADMINISTRATIVE INFORMATION
Title:
Identification 1a Identify the report as a protocol of a systematic review 1
Update 1b If the protocol is for an update of a previous systematic review, identify as such NA
Registration 2 If registered, provide the name of the registry (such as PROSPERO) and registration number 3
Authors:
Contact 3a Provide name, institutional affiliation, e-mail address of all protocol authors; provide physical mailing address of corresponding
author
1
Contributions 3b Describe contributions of protocol authors and identify the guarantor of the review 11
Amendments 4 If the protocol represents an amendment of a previously completed or published protocol, identify as such and list changes;
otherwise, state plan for documenting important protocol amendments
NA
Support:
Sources 5a Indicate sources of financial or other support for the review 11
Sponsor 5b Provide name for the review funder and/or sponsor 11
Role of
sponsor or
funder
5c Describe roles of funder(s), sponsor(s), and/or institution(s), if any, in developing the protocol 11
INTRODUCTION
Rationale 6 Describe the rationale for the review in the context of what is already known 5
Objectives 7 Provide an explicit statement of the question(s) the review will address with reference to participants, interventions, comparators,
and outcomes (PICO)
5-6
METHODS
Eligibility criteria 8 Specify the study characteristics (such as PICO, study design, setting, time frame) and report characteristics (such as years
considered, language, publication status) to be used as criteria for eligibility for the review
6-7
Information
sources
9 Describe all intended information sources (such as electronic databases, contact with study authors, trial registers or other grey
literature sources) with planned dates of coverage
7
Search strategy 10 Present draft of search strategy to be used for at least one electronic database, including planned limits, such that it could be
repeated
7-S1
Study records:
Data 11a Describe the mechanism(s) that will be used to manage records and data throughout the review 7-8
Page 16 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
For peer review only
management
Selection
process
11b State the process that will be used for selecting studies (such as two independent reviewers) through each phase of the review (that
is, screening, eligibility and inclusion in meta-analysis)
7-8
Data
collection
process
11c Describe planned method of extracting data from reports (such as piloting forms, done independently, in duplicate), any processes
for obtaining and confirming data from investigators
8-9
Data items 12 List and define all variables for which data will be sought (such as PICO items, funding sources), any pre-planned data
assumptions and simplifications
8-9
Outcomes and
prioritization
13 List and define all outcomes for which data will be sought, including prioritization of main and additional outcomes, with rationale 8-9
Risk of bias in
individual studies
14 Describe anticipated methods for assessing risk of bias of individual studies, including whether this will be done at the outcome or
study level, or both; state how this information will be used in data synthesis
8
Data synthesis 15a Describe criteria under which study data will be quantitatively synthesised 9-10
15b If data are appropriate for quantitative synthesis, describe planned summary measures, methods of handling data and methods of
combining data from studies, including any planned exploration of consistency (such as I2, Kendall’s τ)
9-10
15c Describe any proposed additional analyses (such as sensitivity or subgroup analyses, meta-regression) 9-10
15d If quantitative synthesis is not appropriate, describe the type of summary planned 10
Meta-bias(es) 16 Specify any planned assessment of meta-bias(es) (such as publication bias across studies, selective reporting within studies) 10
Confidence in
cumulative
evidence
17 Describe how the strength of the body of evidence will be assessed (such as GRADE) 9-10
* It is strongly recommended that this checklist be read in conjunction with the PRISMA-P Explanation and Elaboration (cite when available) for important
clarification on the items. Amendments to a review protocol should be tracked and dated. The copyright for PRISMA-P (including checklist) is held by the
PRISMA-P Group and is distributed under a Creative Commons Attribution Licence 4.0.
From: Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart L, PRISMA-P Group. Preferred reporting items for systematic review and
meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015 Jan 2;349(jan02 1):g7647.
Page 17 of 17
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 30, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2018-023592 on 10 Septem
ber 2018. Dow
nloaded from
Related Documents







![BMJ Paediatrics Open is committed to open peer review. As ... · every neonatal intensive care unit (NICU) [1]. Clinical Trials examining safety and tolerability of paracetamol exposure](https://static.cupdf.com/doc/110x72/5f267247aa582a024f7f168c/bmj-paediatrics-open-is-committed-to-open-peer-review-as-every-neonatal-intensive.jpg)



