Respiratory Tract Infections Associate Professor Raymond Lin Head, Clinical Microbiology BLT18/2008

Blt19 14 Jan 09 A Prof Raymond Lin Respiratory Tract Infections
Jul 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Respiratory Tract Infections
Associate Professor Raymond Lin
Head, Clinical Microbiology
BLT18/2008


The upper and lower respiratory tract is a continuum, along with organisms may track
Defence mechanisms Anatomical e.g. cilia Surface defences at epithelium:
lysozymes, IgA, phagocytes Colonization resistance

Types of pathogens Infect healthy persons Infect those with poor defence
“opportunistic” Use respiratory route to spread to rest of
body

Normal oropharyngeal flora viridans streptococci, Neisseria spp.,
Moraxella catarrhalis, diphtheroids, anaerobes
S. pneumoniae, Haemophilus influenzae, Haemophilus spp.
“colonization resistance” Flora gets replaced with disease, antibiotics,
devices, hospital stay May track to lower respiratory tract
“aspiration”


Pathogens Common respiratory viruses “URTI”
Rhinovirus, influenza, parainfluenza, adenovirus, respiratory syncytial virus (RSV)
Enterovirus, hu coronaviruses, hu metapneumovirus

Pharyngitis (“sore throat”) Group A
streptococcus (S. pyogenes)
Viruses

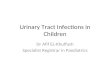
Upper respiratory cavity infections
Acute bacterial sinusitis Acute suppurative otitis media Common bacteria
Streptococcus pneumoniae Haemophilus influenzae Moraxella catarrhalis
Eustachian tube in infants – wider & horizontal


Otitis externa External ear infected
Pseudomonas aeruginosa Aspergillus niger

Otitis externa

sinusitis

“CROUP”laryngo-tracheo-bronchitis
hoarse voice, barking cough severe cases - airway obstruction
Laryngitis
Parainfluenza viruses

Bronchitis
Bronchiolitis
Bronchiectasis
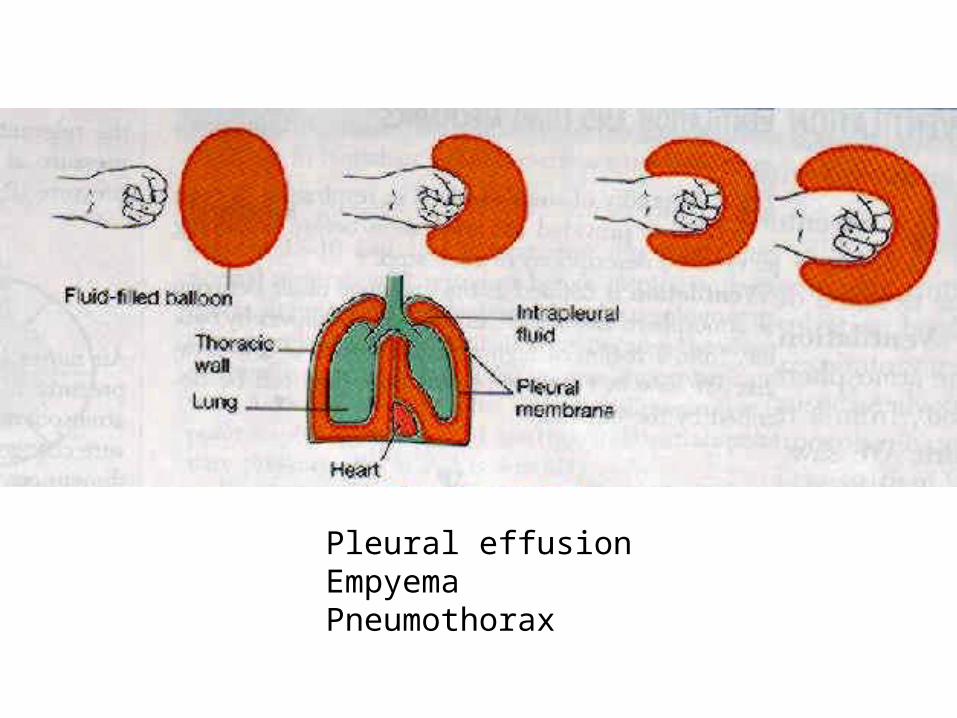
Pleural effusionEmpyemaPneumothorax

Pneumonia Pathogen varies with age, underlying disease Hospital vs. community-acquired Hospital
Immunocompromised ICU - ventilator Antibiotics Multi-resistant bacteria
MRSA, Acinetobacter baumannii

Pneumonia - pathogens Streptococcus pneumoniae
(“pneumococcus”) Haemophilus influenzae Mycoplasma pneumoniae Chlamydia pneumoniae Viruses: adenovirus, influenza
Viruses more important in children.

Pneumonia Environment
E.g. legionella E.g. melioidosis

Cooling tower - a possible source of Legionella infection

Pets, animals e.g. Q fever Psittacosis hantavirus pulmonary syndrome “zoonosis”

Pneumonia – immunocompromised patients
Examples: transplant patients, neutropenic, ICU Unusual organisms not affecting normal
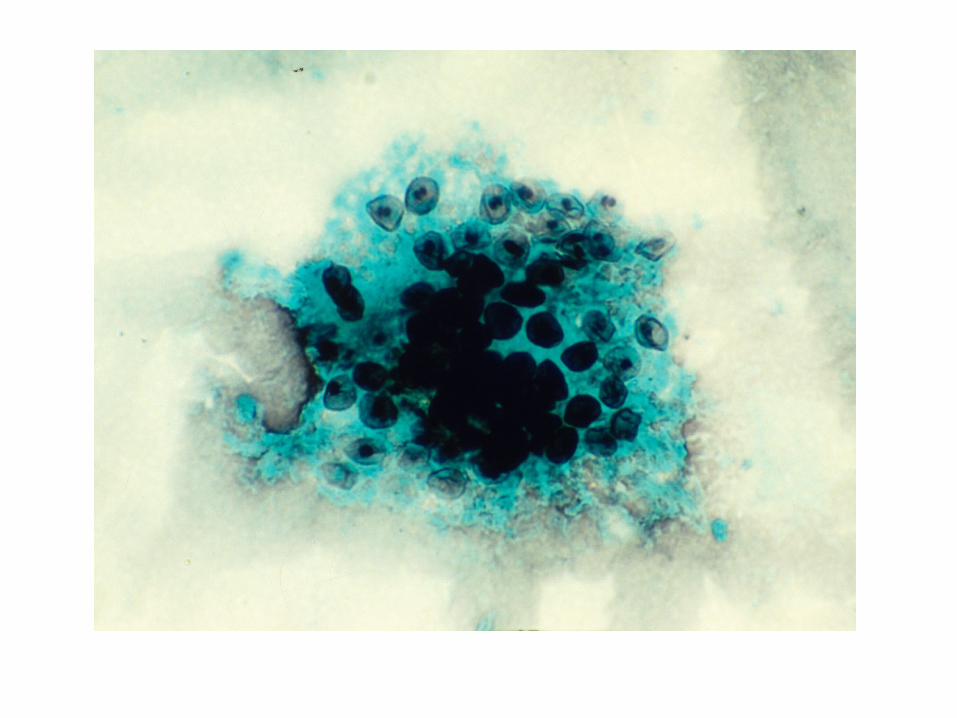
adults E.g. Pneumocystis jiroveci (P. carinii),
cytomegalovirus, aspergillus

Hospital pathogens

Laboratory approaches Sputum culture and gram stain Respiratory virus culture/ IF/ PCR Blood culture Serology
E.g. mycoplasma, legionella

Investigations Sputum culture
Easy to collect and do May be contaminated with oropharyngeal
flora – check epithelial cells on Gram stain Some bacteria are non-cultivable

Investigations Blood culture
More definite proof of causative organism Not sensitive Some bacteria don’t grow in usual media e.g.
Mycoplasma pneumoniae Serology
Host response; good if specific enough Delayed result; cross-reactivity; background
positives E.g. legionella, mycoplasma

Investigations Viruses
Antigen detection e.g. IF – rapid Virus isolation – slow – can find new
viruses PCR – many agents to look for Serology – not usually useful – need paired
titre


Sputum specimen composed of saliva and purulent material




Organisms that can be missed in a sputumOrganisms that can be missed in a sputum
BALBAL- - Legionella Legionella
- - Pneumocystis jiroveciPneumocystis jiroveci
Respiratory Tract SpecimensRespiratory Tract Specimens





Mycobacteria
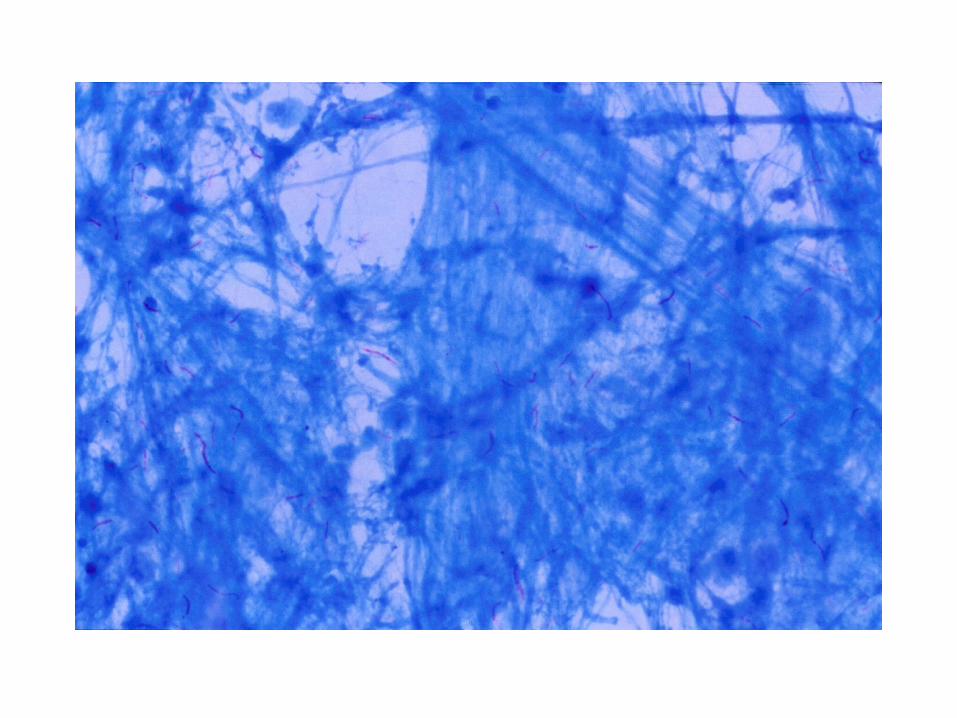
TB bacillusMycobacterium tuberculosis
Non-TB bacillimany speciesM leprae, M avium, M kansasi etc

TB bacillusMycobacterium tuberculosis
Acid fast bacilli (AFB)when stained with ZN technique
Normal habitatinfected humansinfected cattle
Pathogenicityabout 10 million people affected3 million deaths
Spreaddroplets > lungs > lymph / blood > kidney, bone, joints

Mycobacterium tuberculosis Primary infection Latent infection – no symptoms Dormancy – remains in lymph nodes for
many years Reactivation disease – when elderly or
immunocompromised

Tuberculosis - diagnosis Clinical symptoms: cough, night sweats,
loss of weight CXR Lab tests

Tests for tuberculosis Sputum or BAL or gastric aspirate
Acid-fast smear (“AFB” smear) Molecular detection e.g. MTD, PCR Culture e.g. L-J media, broth (MGIT, BacTAlert)
Immunity or exposure Mantoux test Interferon gamma tests
Quantiferon TBSpot (ELISPOT)


Bordetella pertussis (“whooping cough”)
Affects mainly children, milder symptoms in adults
Vaccine preventable (part of childhood DPT immunization)
Clinical features: coughing fits and vomiting, inspiratory “whoop”, pneumonia
Occasional cases in children; epidemics when immunization low

pertussis Laboratory workup
Direct IF Culture : Bordet-Gengou media PCR : most sensitive test now Serology : IgA, IgM – not so reliable – not
used in Singapore
Summary Be able to
List the main pathogens for each site e.g. pneumonia, sinusitis, otitis media, URTI
Outline the diagnostic approaches with examples; limitations of each
TB: know some basic concepts
Related Documents