BLOOD BONE MARROW SPLEEN PARASITES By- Dr. Armaan Singh

Bloodbonemarrowspleenparasites
Aug 09, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

BLOOD BONE MARROW
SPLEEN PARASITES
By- Dr. Armaan Singh
BLOOD BONE MARROW
SPLEEN PARASITES
By- Dr. Armaan Singh

BLOOD NEMATODABLOOD NEMATODA Order:Order: Filariata Filariata

BRUGIA MALAYI / BRUGIA MALAYI / WUCHERERIA BANCROFTI WUCHERERIA BANCROFTI

Brugia malayi /Wuchereria bancrofti: B.malayi is transmitted by mosquitoes of the genus Mansonia, Anopheles and Aedes.W.bancrofti is transmitted by mosquitoes of the genus Culex, Anopheles and Aedes. Close-up of mosquitoes on human skin.
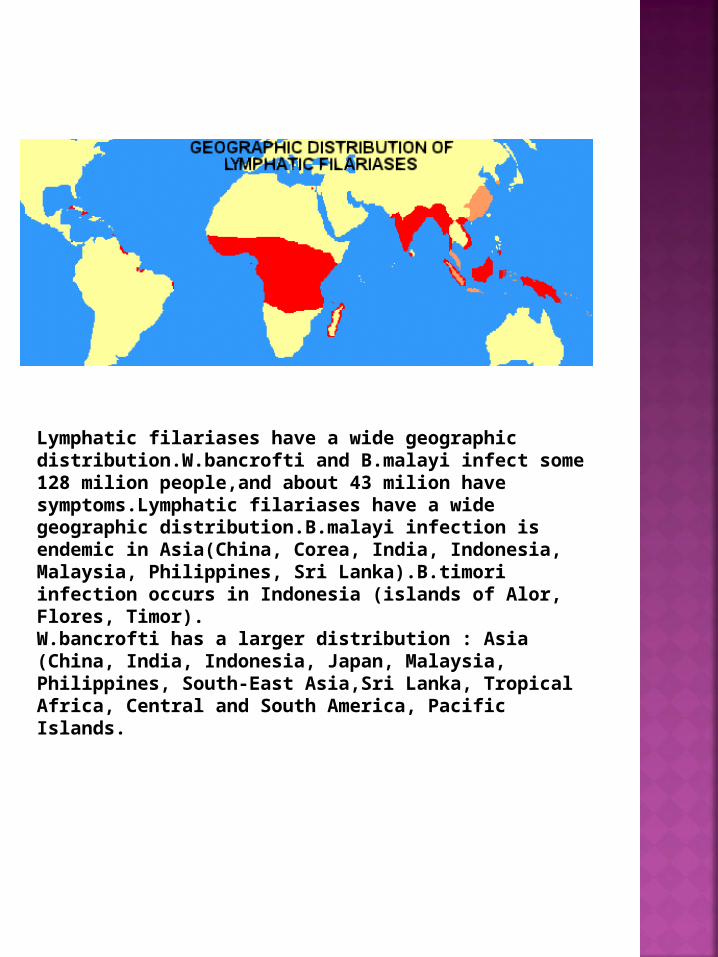
Lymphatic filariases have a wide geographic distribution.W.bancrofti and B.malayi infect some 128 milion people,and about 43 milion have symptoms.Lymphatic filariases have a wide geographic distribution.B.malayi infection is endemic in Asia(China, Corea, India, Indonesia, Malaysia, Philippines, Sri Lanka).B.timori infection occurs in Indonesia (islands of Alor, Flores, Timor). W.bancrofti has a larger distribution : Asia (China, India, Indonesia, Japan, Malaysia, Philippines, South-East Asia,Sri Lanka, Tropical Africa, Central and South America, Pacific Islands.

Brugia malayi:Brugia malayi: microfilariae measure 270 by 8 microfilariae measure 270 by 8 µm, have a sheathµm, have a sheath and a tail with terminal and a tail with terminal constriction,elongated nuclei and absence of constriction,elongated nuclei and absence of nuclei in the cephalic space.They have nocturnal nuclei in the cephalic space.They have nocturnal periodicity.(Wet mount preparation).periodicity.(Wet mount preparation).

Brugia malayi: The microfilariae are sheathed and can be distinguished from W.bancrofti for size (275-320x7,5-10), location of nuclei and tail nuclei.(Fresh examination, particular of the caudal space).

Brugia malayi: detail of the cephalic space. Microfilariae are usually nocturnally periodic but sub-periodic strains of B.malayi and W.bancrofti are observed.(wet mount, detail of the cephalic space of B.malayi microfilaria).

Brugia malayi: identification of microfilariae in stained smear is possible by observation of the stained sheath (W.bancrofti sheath does not stain).

Microfilaria of Microfilaria of Wuchereria bancrofti Wuchereria bancrofti (Giemsa stain, x 400) (Giemsa stain, x 400)

Brugia malayi: the tail is tapered and present a constriction.The last two nuclei are divided by the constriction. The sheath stains pink. (Caudal space of B.malayi, Giemsa stain).

Brugia malayi:Brugia malayi: the cephalic space is longer than the cephalic space is longer than broad(in broad(in W.bancroftiW.bancrofti is as long as broad). is as long as broad). (Detail of the cephalic space of (Detail of the cephalic space of B.malayiB.malayi microfilaria, microfilaria, Giemsa stain). Giemsa stain).

Lymphatic filariasis: adults of B.malayi and W.bancrofti live in the lymphatic vessels and lymphnodes where they cause dilatation, inflammatory infiltrates and, at last, blockage of the lymphatic circulation.Adenolymphangitis, orchitis, epididimitis associated with fever are the commonest manifestation of the acute stage of the infection;eosinophilia is frequent at this stage. Lymphoedema particularly of the legs and scrotum,
hydrocoeles and chyluria are the result of the progression of the disease;genital manifestations are frequent in W.bancrofti infections while they are rare during B.malayi infections. -Lymphatic filariasis: elephantiasis of scrotum.-Tanzanian with elephantiasis due to W.bancrofti.-Another Tanzanian patient with elephantiasis due to W.bancrofti.-Early hydrocoel in a Tanzanian man with W.bancrofti infection

Lymphatic filariasis: elephantiasis is the last consequence of the swelling of limbs and scrotum. Diethylcarbamazine (DEC), ivermectine and albendazole used alone or in combination are the drugs of choice.-Elephantiasis of the limbs. -Thai patient with elephantiasis of leg due to W.bancrofti or Brugia malayi. -Second Thai patient with elephantiasis due to lymphatic filariasis.

LOA LOA LOA LOA

Loa loa: the infection is endemic in West and Central Africa,especially in Angola, Cameroun, Congo, Eq. Guinea, Gabon, Nigeria, RCA, Zaire.

Loa loa: after injection larvae develop into adults in 6 months and may live for 17 years in the organism.Microfilariae measure 275 by 5-6 µm and are present in blood without periodicity. Count is mandatory before therapy.

Loa loa:Loa loa: microfilariae measure with the sheath microfilariae measure with the sheath 240-300 by 5-6 µm.The sheath doesn't stain with 240-300 by 5-6 µm.The sheath doesn't stain with Giemsa. The nuclei extendGiemsa. The nuclei extend from the small cephalic from the small cephalic space to the tip of the tail.(Giemsa stain).space to the tip of the tail.(Giemsa stain).

Loa loa: the sheath does not stain and appears as a virtual space around the larva. (Giemsa stain).

Loa loa:Loa loa: the nuclei form a continuous row to the the nuclei form a continuous row to the tip of tail.The unstained sheath is well visible. tip of tail.The unstained sheath is well visible. (Detail of the caudal space, Giemsa stain).(Detail of the caudal space, Giemsa stain).

Loa loa: large nuclei extend from the little cephalic space. (Detail of the cephalic space, Giemsa stain).

Loa loa:Loa loa: the presence of the unstainded sheath is the presence of the unstainded sheath is clearly visibleclearly visible as a space around the larva. as a space around the larva. (Detail of cephalic space with a polymorphonuclear (Detail of cephalic space with a polymorphonuclear cell, Giemsa stain). cell, Giemsa stain).

Loa loa: microfilaria. Thick film, Mayer's haematoxylin (400 X).
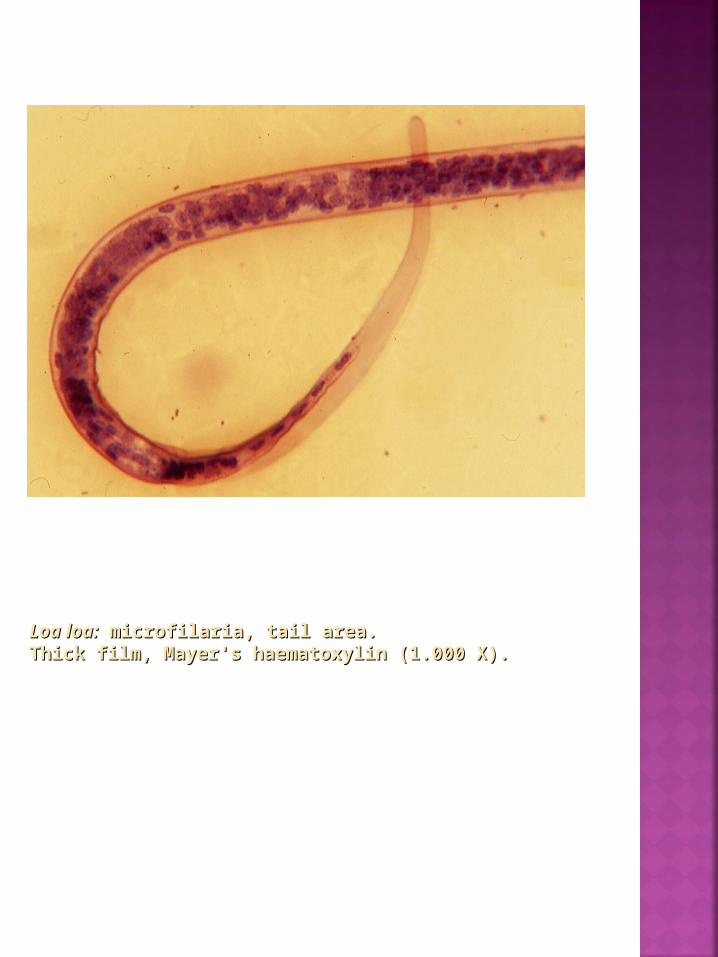
Loa loa:Loa loa: microfilaria, tail area. microfilaria, tail area. Thick film, Mayer's haematoxylin (1.000 X).Thick film, Mayer's haematoxylin (1.000 X).

Loa loa: microfilariae can be demonstrated in blood with fluorochromes (Acridine orange stain).

Loa loa: although direct diagnosis by observation of microfilariae in blood is the reference method, indirect diagnostic tests such as IF may allow diagnosis when direct observation is negative, especially in subjects who are not resident in endemic areas. The frequent cross-reaction with other nematode infections limits the usefulness of serology in these patients. Immunodiagnosis by indirect immunofluorescence.
Antigen: frozen sections of Dirofilaria immitis.

MANSONELLA OZZARDIMANSONELLA OZZARDIMANSONELLA PERSTANS MANSONELLA PERSTANS
M. ozzardi is endemic in Central and South America. The adults live in subcutaneous tissues. Unsheathed microfilariae (200x4-5 µm) released in blood without periodicity,have a small cephalic space, a long and slender tail without nuclei to the end.

M. perstans is endemic in Africa and South America. The adult lives in body cavities. Unsheathed microfilariae (200x4-5 µm) released in blood without periodicity have a small cephalic space and nuclei to the end of tail.

Mansonella perstans: microfilaria. Thick film, (400 X).

BLOOD SPOROZOEABLOOD SPOROZOEA
Order: Eucoccidiida Plasmodium falciparum Plasmodium malariae Plasmodium ovale Plasmodium vivax Toxoplasma gondii

PLASMODIUM FALCIPARUM PLASMODIUM FALCIPARUM

Plasmodium sp.: geographic distribution.

Plasmodium sp.: the genus Anopheles includes more than 400 species of mosquitoes.Many may act as vectors of human diseases such as malaria,filariasis and some arbovirus. Eggs present a pair of lateral floats and are laid singly on the water surface,while larvae lay in a horizontal position under the water surface.

Plasmodium sp.: the resting position of the adult is characteristic with the proboscid, head and abdomen in a straight line at an angle of about 45° with the surface on which they rest.Only about 60 species can transmit malaria and they greatly differ in their efficiency as vectors according to man biting behaviour, survival, fertility, adaptation to different breeding place.The most efficient vectors belong to the A.gambiae complex,widely distributed in tropical Africa, where also important is A.funestus.In Asia important vectors are A.culicifaciens, A.dirus, A.sinensis and A.miminus; in the Pacific area A.farauti and A.maculatus play a predominant role in malaria transmission. The main vector in South America in A.albimanus.

P.falciparum: species identification is possible on the basis of the appearance of parasites of each of the four malaria species.Shape and size of asexual parasites and of macro- and microgametocytes, developmental stages in peripheral blood, modifications of infected erythrocytes,presence of dots or clefts on the red blood cells are the main differential characteristics.

Malaria diagnosis relies on observation of parasites in Giemsa-stained thin or thick smears (G-TS). Alternative techniques for identification of malaria parasites are based on fluorochromes such as Acridine Orange (AO), DAPI-PI or BCP. With these dyes malaria parasites are easily recognized under UV light, reducing the time spent reading the slides.Another method, based on fluorochromes, the quantitative buffy coat (QBC) (Becton-Dickinson) analysis wich uses AO staining of centrifuged parasites in a capillary tube containing a float, has been shown to be rapid and accurate.

P.falciparum:P.falciparum: gametocytes of gametocytes of P.falciparumP.falciparum. . QBC technique (60X).QBC technique (60X).
Recently different immunochromatographic tests such as the ParaSight F(Becton Dickinson) and the Malaquick (ICT) wich capture and detect the histidine rich protein 2 (HRP-2) antigen,and the OPTIMAL wich detects Plasmodium lactate dehydrogenase(pLDH) have been developed and distributed. The tests are highly sensitive and specific and are now able to distinguish P.falciparum infections from non-falciparum infections. P.falciparum trophozoites, thin smear, Giemsa stain.

Malaria diagnosis:whereas thin film gives more informations on parasite morphology and permits an easier morphologic differentiation,G-TS is more sensitive allowing a concentration of plasmodia (10-15 folds) and it is the standard reference diagnostic test.

Malaria diagnosis: G-TS needs careful stain (2% Giemsa) and experience in examining slides;reasonable sensitivity is reached by observing at least 500-1.000 White Blood Cells (WBC).Quantification of baseline parasitemia is necessary for monitoring the response to therapy. Parasites must be counted in parallel with leucocyte and parasitemia expressed as parasites/µl.
N. of parasites counted x N. of WBC/µl
N. of WBC counted
= N. of parasites/µl
P.falciparum trophozoites, thick smear, Giemsa stain.

P. falciparum: trophozoites are small rings with single or double small chromatin dots, and regular cytoplasm; multiple infection and high parasitemia (>5%) are common. Dots or cleft (Maurer's) can be observed on the infected RBCs. P.falciparum trophozoites, thin smear, Giemsa stain.

P. falciparum: sometimes trophozoites appear at the edge of the red blood cell (applique form) left.Erythrocytes maintain regular shape and size. P.falciparum trophozoites, thin smear, Giemsa stain.

P. falciparum: late trophozoites and schizonts usually are not observed in peripheral blood unless in severe infections. Cerebral malaria: late trophozoites with a coarse granule of pigment in peripheral blood. P.falciparum, thin smear, Giemsa stain.

P.falciparum: micro- and macrogametocytes are easily recognized by their crescentic, cigar- or banana-like shape.Microgametocytes have a diffuse chromatin,while macrogametocytes have thickened chromatin. Microgametocyte, Giemsa thin smear.

P.falciparum: in thick films red blood cells are not visible and leucocytes and parasites appear smaller than in thin smears.Trophozoites have a ring or comma shape, with one or two dots of chromatin.The pigment, when present, is compact.

P.falciparum: trophozoites in Giemsa-stained thick films have a wide range of shapes. Maurer's clefts are not visible.

P.falciparum: micro- and macrogametocytes have an evident malaric pigment,scattered through in the cytoplasm in the microgametocyte. Microgametocyte, Giemsa thick smear.

P.falciparum: staining with fluorochromes is rapid (less than 1 min)and observation of slides can be performed at low magnification (400X) allowing rapid screening of smears even with low parasitemia. P.falciparum (DAPI-PI).

P.falciparum trophozoites. Acridine Orange stain.

P.falciparum: the sensitivity of different isolates of P.falciparum to drugs can be assessed with the WHO "in vitro test". The development to mature schizont in presence of therapeutic levels of the drug demonstrates resistance of the isolate.

P.falciparum: severe P.falciparum infections are clinical forms characterized by potentially fatal manifestations or complications:cerebral malaria, defined by a state of unrousable coma in absence of other causes,is the most common manifestation. Celebral malaria: parasitized RBCs in brain vessels (H&E stain).

P.falciparum: rosetting of infected and uninfected red blood cells and cytoadherence of parasitized erythrocytes to the vascular endothelium,play a crucial role in sequestration of parasites and obstruction of brain vessels. Induction of host cytokines and soluble mediators such as oxygen radicals and NO play an important role in the pathogenesis of the infection.

P.falciparum: the brain appears oedematous, hyperaemic and with pigment deposition; the capillaries, expecially of the white matter, appear dilated and congested and obstructed by parasitized RBCs.

P.falciparum: renal failure may result from sequestration of RBCs and alteration of the renal microcirculation. Glomerulal and interstitial vessels present RBCs adhering to the endothelium.

P.falciparum: renal failure may also result from releasing of compounds secondary to intravascular haemolysis (not haemoglobin itself) that can cause acute tubular necrosis especially in presence of dehydratation and acidosis.

P.falciparum: sequestration and cytoadherence of parasitized RBCs in heart microcirculation is frequent but myocardial dysfunctions and cardiac arrhythmias are uncommon in severe falciparum malaria.

P.falciparum: jaundice and abnormalities of liver function tests are frequent findings in severe falciparum malaria but hepatic failure is rare even in heavily infected individuals.

P.falciparum: histological abnormalities include Kuppfer hyperplasia,mononuclear hyperplasia and sinusoid dilatation;swollen hepatocytes contain haemosiderin.Kuppfer cells contain a lot of malaria pigment.

A fatal case of P.falciparum malaria (liver): malarial pigment within Kupffer cells (H&E X 400)

A fatal case of P.falciparum malaria (liver): note a parasitized erytrocyte (H&E X1000)

P.falciparum: pulmonary, non specific complications, such as atypical pneumonia, lobar pneumonia or bronchopneumonia,frequently occur during malaria infections.Pulmonary oedema is a specific and severe complication of P.falciparum infection: 3-10% This syndrome, wich resembles the Acute Respiratory Distress Syndrome (ARDS),has a relative late onset (wich may be abrupt) in the course of the infection and is often associated with other manifestations of the severe falciparum malaria.Different pathogenic mechanisms have been suggested: -increased capillary membrane permeability[due to microemboli or to Disseminated Intravascular Coagulation (DIC)] -impaired function of the alveolar capillaries; -severe disfunction of the pulmonary microcirculation; -allergic phenomena; -therapeutic fluid overload. The chest radiograph, in severe cases, shows widespread bilateral,confluent intraalveolar and interstitial infiltrates.

PLASMODIUM MALARIAE PLASMODIUM MALARIAE

Plasmodium sp.: geographic distribution.

Plasmodium sp.: the genus Anopheles includes more than 400 species of mosquitoes.Many may act as vectors of human diseases such as malaria, filariasis and some arbovirus. Eggs present a pair of lateral floats and are laid singly on the water surface,while larvae lay in a horizontal position under the water surface.

Plasmodium sp.: the resting position of the adult is characteristic with the proboscid, head and abdomen in a straight line at an angle of about 45° with the surface on which they rest.Only about 60 species can transmit malaria and they greatly differ in their efficiency as vectors according to man biting behaviour, survival, fertility, adaptation to different breeding place.The most efficient vectors belong to the A.gambiae complex,widely distributed in tropical Africa, where also important is A.funestus. In Asia important vectors are A.culicifaciens, A.dirus, A.sinensis and A.miminus;in the Pacific area A.farauti and A.maculatus play a predominant role in malaria transmission. The main vector in South America in A.albimanus.

P.malariae: species identification is possible on the basis of the appearance of parasites of each of the four malaria species.Shape and size of asexual parasites and of macro- and microgametocytes, developmental stages in peripheral blood, modifications of infected erythrocytes,presence of dots or clefts on the red blood cells are the main differential characteristics.

Malaria diagnosis relies mainly on observation of parasites in Giemsa-stained thin or thick smears (G-TS).Alternative techniques for identification of malaria parasites are based on fluorochromes such as Acridine Orange (AO), DAPI-PI or BCP. With these dyes malaria parasites are easily recognized under UV light,reducing the time spent reading the slides.Another method, based on fluorochromes, the quantitative buffy coat (QBC) (Becton-Dickinson) analysis wich uses AO staining of centrifuged parasites in a capillary tube containing a float, has been shown to be rapid and accurate.

P.falciparum: gametocytes of P.falciparum. QBC technique (60X).
Recently different immunochromatographic tests such as the ParaSight F(Becton Dickinson) and the Malaquick (ICT) wich capture and detect the histidine rich protein 2 (HRP-2) antigen, and the OPTIMAL wich detects Plasmodium lactate dehydrogenase (pLDH) have been developed and distributed. The tests are highly sensitive and specific and are now able to distinguish P.falciparum infections from non-falciparum infections. P.malariae trophozoites, thin smear, Giemsa stain.

Malaria diagnosis:whereas thin film gives more informations on parasite morphology and permits an easier morphologic differentiation, G-TS is more sensitive allowing a concentration of plasmodia (10-15 folds)
and it is the standard reference diagnostic test.

Malaria diagnosis: G-TS needs careful stain (2% Giemsa) and experience in examining slides; reasonable sensitivity is reached by observing at least 500-1.000 White Blood Cells (WBC). Quantification of baseline parasitemia is necessary for monitoring the response to therapy. Parasites must be counted in parallel with leucocyte and parasitemia expressed as parasites/µl.
N. of parasites counted x N. of WBC/µl
N. of WBC counted
= N. of parasites/µl
trophozoites,thick smear
Schizont,thick smear
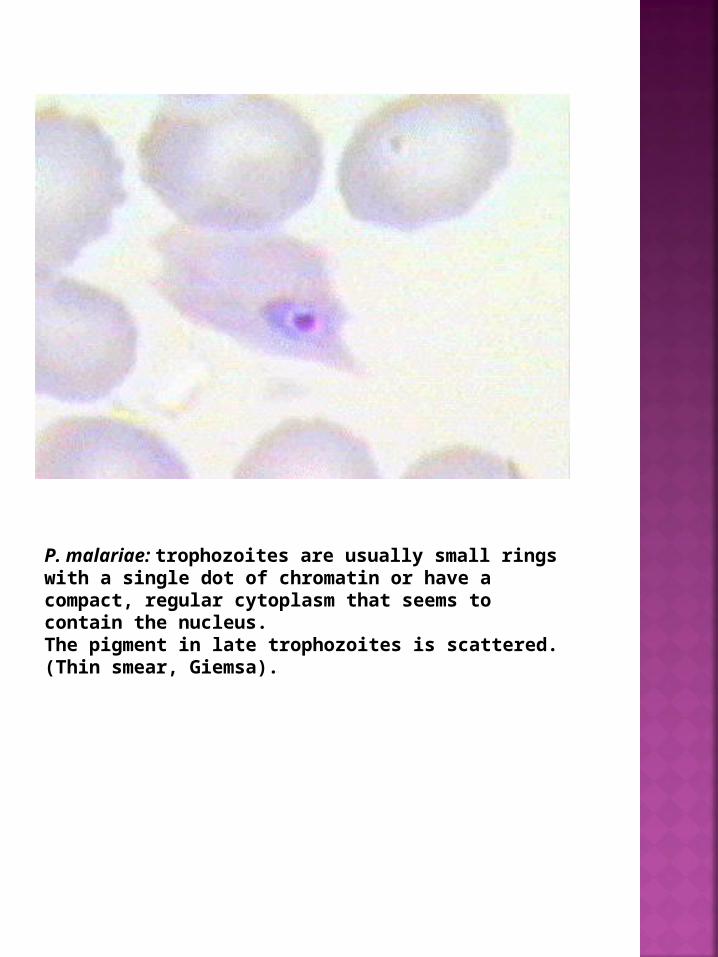
P. malariae: trophozoites are usually small rings with a single dot of chromatin or have a compact, regular cytoplasm that seems to contain the nucleus. The pigment in late trophozoites is scattered. (Thin smear, Giemsa).

P. malariae: trophozoites may assume a band form typical of the species.Red blood cells are not enlarged or rather smaller than normal.Multiple infection is rare. The parasitemia is usually low. No dots or clefts.(Thin smear, Giemsa).

P.malariae: schizonts are small and with a low number of merozoites (<12) arranged in regular forms (rosettes) with a thickened, often central, pigment.The complete erythrocytic cycle takes 72 hours and ends with the releasing of free merozoites (c).(Thin smear, Giemsa).

P. malariae: micro- and macrogametocytes are round, small with chromatin defined; they must be differentiated from late trophozoites.During P.malariae infection all stages of development are present in peripheral blood. (Microgametocyte, Giemsa stain).

PLASMODIUM OVALE PLASMODIUM OVALE

Plasmodium sp.: geographic distribution.

Plasmodium sp.: the genus Anopheles includes more than 400 species of mosquitoes.Many may act as vectors of human diseases such as malaria, filariasis and some arbovirus. Eggs present a pair of lateral floats and are laid singly on the water surface,while larvae lay in a horizontal position under the water surface.

Plasmodium sp.: the resting position of the adult is characteristic with the proboscid, head and abdomen in a straight line at an angle of about 45° with the surface on which they rest.Only about 60 species can transmit malaria and they greatly differ in their efficiency as vectors according to man biting behaviour, survival, fertility, adaptation to different breeding place.The most efficient vectors belong to the A.gambiae complex,widely distributed in tropical Africa, where also important is A.funestus. In Asia important vectors are A.culicifaciens, A.dirus, A.sinensis and A.miminus;in the Pacific area A.farauti and A.maculatus play a predominant role in malaria transmission. The main vector in South America in A.albimanus.

P.ovale: species identification is possible on the basis of the appearance of parasites of each of the four malaria species.Shape and size of asexual parasites and of macro- and microgametocytes, developmental stages in peripheral blood, modifications of infected erythrocytes,presence of dots or clefts on the red blood cells are the main differential characteristics.

Malaria diagnosis relies on observation of parasites in Giemsa-stained thin or thick smears (G-TS).Alternative techniques for identification of malaria parasites are based on fluorochromes such as Acridine Orange (AO), DAPI-PI or BCP. With these dyes malaria parasites are easily recognized under UV light,reducing the time spent reading the slides.Another method, based on fluorochromes, the quantitative buffy coat (QBC)(Becton-Dickinson) analysis wich uses AO staining of centrifuged parasites in a capillary tube containing a float, has been shown to be rapid and accurate.

Recently different immunochromatographic tests such as the ParaSight F (Becton Dickinson) and the Malaquick (ICT) wich capture and detect the histidine rich protein 2 (HRP-2) antigen, and the OPTIMAL wich detects Plasmodium lactate dehydrogenase (pLDH) have been developed and distributed.The tests are highly sensitive and specific and are now able to distinguish P.falciparum infections from non-falciparum infections. P.ovale, thin smear, Giemsa stain.

Malaria diagnosis: whereas thin film gives more informations on parasite morphology and permits an easier morphologic differentiation, G-TS is more sensitive allowing a concentration of plasmodia (10-15 folds)and it is the standard reference diagnostic test.

Malaria diagnosis: G-TS needs careful stain (2% Giemsa) and experience in examining slides; reasonable sensitivity is reached by observing at least 500-1.000 White Blood Cells (WBC). Quantification of baseline parasitemia is necessary for monitoring the response to therapy. Parasites must be counted in parallel with leucocyte and parasitemia expressed as parasites/µl.
N. of parasites counted x N. of WBC/µl
N. of WBC counted
= N. of parasites/µl
P.ovaleP.ovale, thick smear, Giemsa stain., thick smear, Giemsa stain.

Plasmodium ovale: trophozoite
All stages are seen in blood films; prominent Shuffner's dots are present at all stages. Trophozoites appear as rings with, usually, a compact cytoplasm;they do not have ameboid cytoplasm.The parasites are smaller than P.vivax.

P.ovale: red blood cells are enlarged, ovalized and distorted with fimbriae at poles. Schizonts have usually 8-10 merozoites.

P.ovale: micro- and macrogametocytes are sometimes difficult to differentiate from late trophozoites;they are round and occupy almost the entire erythrocyte.Microgametocytes have a more scattered chromatin.

PLASMODIUM VIVAX PLASMODIUM VIVAX

Plasmodium sp.: geographic distribution.

Plasmodium sp.: the genus Anopheles includes more than 400 species of mosquitoes.Many may act as vectors of human diseases such as malaria, filariasis and some arbovirus. Eggs present a pair of lateral floats and are laid singly on the water surface,while larvae lay in a horizontal position under the water surface.

Plasmodium sp.: the resting position of the adult is characteristic with the proboscid, head and abdomen in a straight line at an angle of about 45° with the surface on which they rest.Only about 60 species can transmit malaria and they greatly differ in their efficiency as vectors according to man biting behaviour, survival, fertility, adaptation to different breeding place.The most efficient vectors belong to the A.gambiae complex,widely distributed in tropical Africa, where also important is A.funestus. In Asia important vectors are A.culicifaciens, A.dirus, A.sinensis and A.miminus;in the Pacific area A.farauti and A.maculatus play a predominant role in malaria transmission. The main vector in South America in A.albimanus.

P.vivax: species identification is possible on the basis of the appearance of parasites of each of the four malaria species. Shape and size of asexual parasites and of macro- and microgametocytes, developmental stages in peripheral blood, modifications of infected erythrocytes,presence of dots or clefts on the red blood cells are the main differential characteristics.

Malaria diagnosis relies mainly on observation of parasites in Giemsa-stained thin or thick smears (G-TS).Alternative techniques for identification of malaria parasites are based on fluorochromes such as Acridine Orange (AO), DAPI-PI or BCP. With these dyes malaria parasites are easily recognized under UV light, reducing the time spent reading the slides.Another method, based on fluorochromes, the quantitative buffy coat (QBC) (Becton-Dickinson) analysis wich uses AO staining of centrifuged parasites in a capillary tube containing a float,has been shown to be rapid and accurate.

Recently different immunochromatographic tests such as the ParaSight F(Becton Dickinson) and the Malaquick (ICT) wich capture and detect the histidine rich protein 2 (HRP-2) antigen, and the OPTIMAL wich detects Plasmodium lactate dehydrogenase (pLDH)have been developed and distributed.The tests are highly sensitive and specific and are now able to distinguish P.falciparum infections from non-falciparum infections. P.vivax trophozoites, GT-s.

Malaria diagnosis: whereas thin film gives more informations on parasite morphology and permits an easier morphologic differentiation,G-TS is more sensitive allowing a concentration of plasmodia(10-15 folds) and it is the standard reference diagnostic test.

Malaria diagnosis: G-TS needs careful stain (2% Giemsa) and experience in examining slides;reasonable sensitivity is reached by observing at least 500-1.000 White Blood Cells (WBC). Quantification of baseline parasitemia is necessary for monitoring the response to therapy.Parasites must be counted in parallel with leucocyte and parasitemia expressed as parasites/µl.
N. of parasites counted x N. of WBC/µl
N. of WBC counted
= N. of parasites/µl
P. vivax P. vivax trophozoites, thick smear, Giemsa stain.trophozoites, thick smear, Giemsa stain.

P.vivax: young trophozoites are small with single (rarely double) chromatin,with a loop of thin cytoplasm.The red blood cell is sligthly enlarged and a few Shuffner's dots are present. Parasitemia range form 0.5 to 2%, multiple infection is rare.

P.vivax: the trophozoites increases in size and the cytoplasm becomes ameboid with rapid movements ("vivax").The red blood cell enlarges and prominet Shuffner's dots are present.(Thin smear, Giemsa).

P.vivax: in more advanced stage of development trophozoites occupy most of the RBC, and have a large vacuole and fine rods of pigment.The nucleus increases in size.

P.vivax: late trophozoites have a more dense cytoplasm, and a large vacuole.

P.vivax: in young schizonts the nucleus divides and the vacuole disappears; the cytoplasm is dense.

P.vivax: in about 48hours schizogony is completed.Mature schizont may contain 12-24 merozoites. In thick smears schizonts look smaller than in thin smears and the Schuffner's dots are not always visible.

P.vivax: gametocytes are round or oval without vacuole; most of the RBC is occupied by the parasite. Macrogametocytes have a compact chromatin mass while microgametocytes have a more diffuse nucleus stained pink.

P.vivax: staining with fluorochromes is rapid (less than 1 min) and observation of slides can be performed at low magnification (400X) allowing rapid screening of smears even with low parasitemia.P. vivax (DAPI-PI).
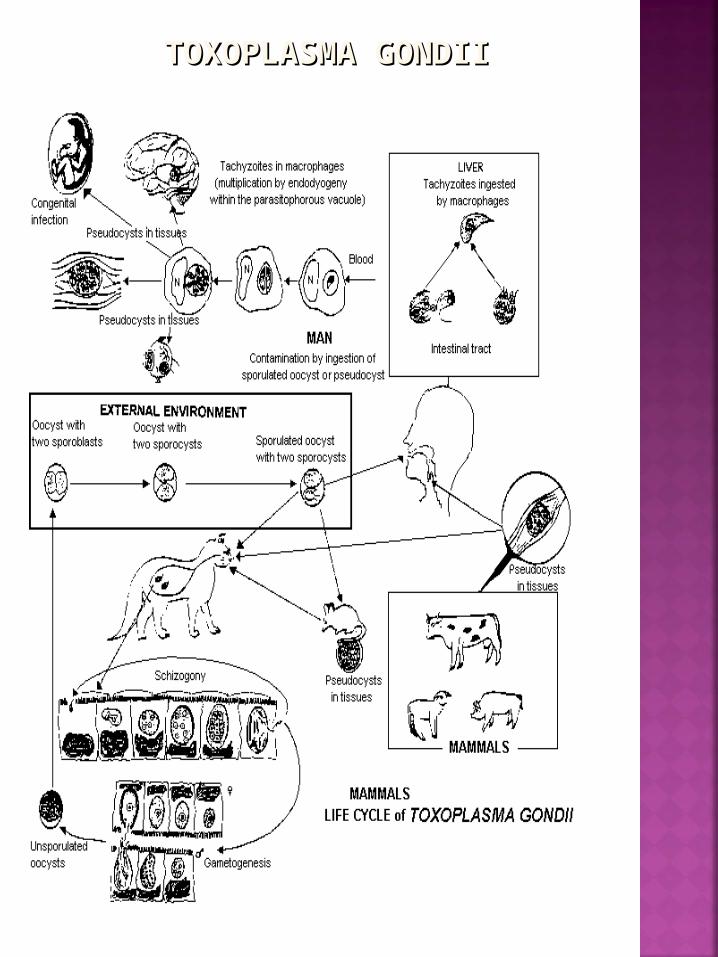
TOXOPLASMA GONDIITOXOPLASMA GONDII

T. gondii: T.gondii encephalitis (TE) is the most common cerebral opportunistic infection in patients with AIDS. The typical lesion is an ipodense focal area with ring contrast-enhancement and edema. (CT scan of a toxoplasmic encephalitis).

T. gondii: tissue cysts, 100-300 µm, may contain up to 3.000 bradyzoites.The wall of mature pseudocysts is believed to represent a combination of host and parasitic components.

T. gondii: diagnosis of TE is usually presumptive, based on clinical and radiologic findings and on the response to treatment; cerebral biopsy sometimes allows identification of pseudocysts in tissue sections. (H&E stain).

T. gondii: toxoplasmic pseudocyst within an inflammatory tissue reaction. (H&E stain).

T. gondii: the pseudocysts of T.gondii can be observed in tissue sections with monoclonal antibodies.

T. gondii: direct detection of T.gondii in clinical specimens is rare;parasites can be isolated from blood, CSF, amniotic fluid,tissue biopsies on cell lines (THP-1 or MRC-5). In clinical specimens the presence of parasites can also be demonstrated by PCR analysis.

T. gondii: intracellular trophozoites of T.gondii in a cell culture. The trophozoites proliferate within the vacuole developing a pseudocyst. (Trophozoites in a THP-1 cell, Giemsa stain).

T. gondii: in cell cultures T.gondii proliferates to form a pseudocyst of 8-20 parasites. (Trophozoites in a THP-1 cell, Giemsa stain).

T. gondii: lysis of a THP-1 cell with release of tachizoites in culture. (Trophozoites in a THP-1 cell, Giemsa stain).

T. gondii: microscopical features of tachizoites of Toxoplasma gondii and peritoneal macrophages of mouse in peritoneal exudate. (SEM)

T. gondii: microscopical features of tachizoites of Toxoplasma gondii and peritoneal macrophages of mouse in peritoneal exudate. (SEM)

T. gondii: the anterior pole of an endozoid in tangential projection.Several subpellicular fibrils and their insertion on the anterior polar ring are visible.

T. gondii:T. gondii: transmision electron microscopic picture. transmision electron microscopic picture. Longitudinal section of an endozoid.Longitudinal section of an endozoid.
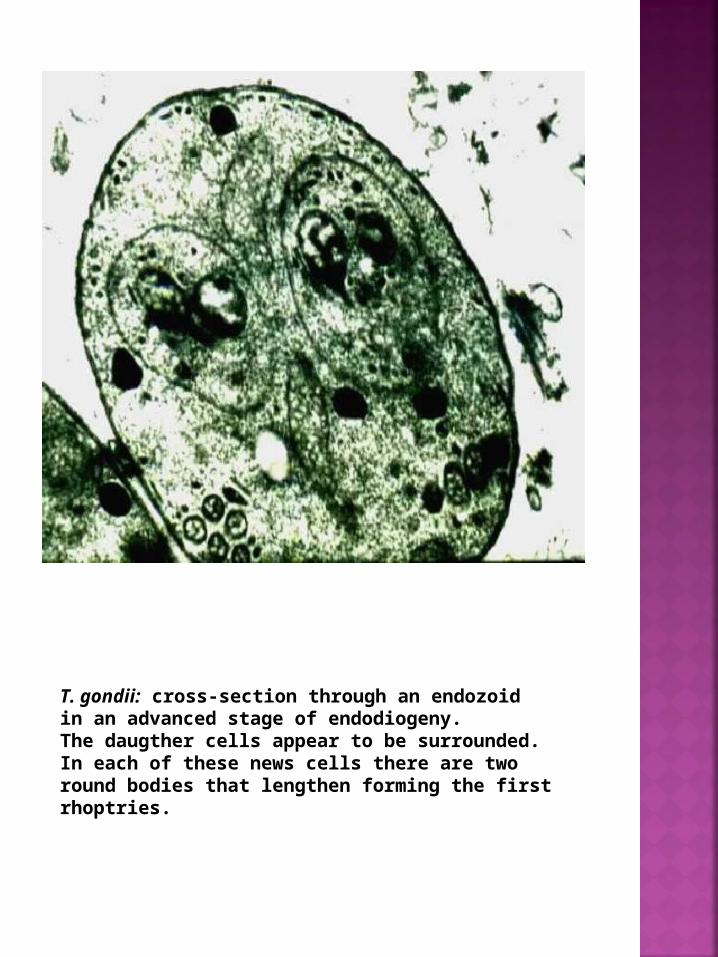
T. gondii: cross-section through an endozoid in an advanced stage of endodiogeny. The daugther cells appear to be surrounded. In each of these news cells there are two round bodies that lengthen forming the first rhoptries.

SPOROZOEASPOROZOEA Order :Order :PiroplasmidaPiroplasmida

BABESIA CANISBABESIA CANIS
Babesia spp: babesiosis is a zoonosis that affects several animals:B.canis (dogs), B.equi (horses), B.bovis (cattle), B.microti (rodents).Some Babesia spp. are not host specific and can be transmitted to humans:B. microti and B.bovis/divergens.The infection is transmitted by the bite of ticks of the Family Ixodidae of the genera Dermatocentor, Ixodes and Rhipicephalus.The main vector of B.microti is I.dammini, while vector of B.microti is I.ricinus B.canis, Giemsa stain.

Babesia spp.: intraerythrocytic organisms in blood smears

Babesia spp.: after inoculation by the vector, the trophozoites enter the bloodstream and multiply inside the erythrocytes by budding, releasing two to fours daughter parasites and causing hemolytic anemia. Ticks become infected by ingesting blood of parasitized mammals. Motile "vermicules" develop and multiply in the tick's gut and then migrate through the body (salivary glands and ovaries).In some species transovarial transmission (B.bovis and B.caballi)or transtadial passage, from larva to nimph (B.microti) occur.Vermicules of Babesia spp. (B.caballi ?) obtained from crushed Rhipicephalus turanicus eggs. Tick collected from horses in a military farm in Turkey where the prevalence of equine babesiosis is high.

Babesia spp.: by transovarial transmission "vermicules" can infect tick eggs; they multiply in the yolk and in intestinal tissues of the larva; pyriform bodies are then observed in the salivary glands of the haematophage larvae and nimphs.Vermicules of Babesia spp. (B.caballi ?) obtained from crushed Rhipicephalus turanicus eggs. Tick collected from horses in a military farm in Turkey where the prevalence of equine babesiosis is high.

B.canis: diagnosis depends on the observation of the intraerythrocytic organisms in blood smears.Pear shaped microorganisms (2-5 µm) and tetrads are the diagnostic shape of the parasite. (Giemsa stain).

B.canis: intraerythrocytic parasites can be confused with P.falciparum or P.malariae trophozoites. Ring and band forms are sometimes observed. (Giemsa stain).
B.equi: trophozoites of B.equi can mimic P.falciparum young ring trophozoites.

ZOOMASTIGOPHOREA ZOOMASTIGOPHOREA Order:Order: KinetoplastidaKinetoplastida

TRYPANOSOMA CRUZITRYPANOSOMA CRUZI (Chagas' disease)(Chagas' disease)
T. cruzi: american trypanosomiasis was first described by Carlos Chagas in Brasil in 1909. The infection, Chagas' disease, is caused by the haemoflagellate Trypanosoma cruzi. tc1: T.cruzi in blood sample, Giemsa.

T. cruzi: the disease is a public health threat in most Latin American countries,although cases due to blood derivatives or blood transfusion has been reported in non-endemic regions. According to WHO the overall prevalence of human T.cruzi infection is estimated in 18 million cases and 100 million people are living at risk. tc2: T. cruzi: geographical distribution.

T. cruzi: the vectors are reduvidae bugs which are haematophagus and the most important are Triatoma infestans(Argentina, Chile, Brazil, Bolivia, Paraguay, Uruguay, Peru),T. sordida (Argentina, Bolivia, Brazil, Paraguay),Rhodnius prolixus (Colombia, Venezuela, Mexico, Central America),T. dimidiata (Ecuador, Mexico, Central America),and Panstrogylus megistus (northeast Brazil).

T. cruzi: the transmission by the vector is faecal. T.cruzi infective metacyclic trypomastigotes are shed in the faeces of the bug and are inoculated into the human host by scratching infected faeces into skin abrasions usually caused by the bug in the process of feeding (blood-sucking). T.cruzi metacyclic trypomastigote: scanning electron microscopy showing T.cruzi trypomastigotes recovered from an infected Triatoma spp. in Pedro Carbo, Ecuador.

T. cruzi: infective metacyclic trypomastigotes are shed in the faeces of the bug and inoculated into the vertebrate host not only by skin lesions but also through the mucosa of the mouth and,in humans, through the conjunctiva of the eyes.

T. cruzi: trypomastigotes can infect most of the vertebrate cells,polymorphonuclear leucocytes and macrophages are probably among the first vertebrate host cells with which T.cruzi interacts in vivo. tc7a: In vitro T.cruzi infection of macrophages showing the presence of amastigotes: Wright-Giemsa stain, showing replicating T.cruzi amastigotes within host cell.

T. cruzi: this invasive step is crucial for the life cycle of the parasite since it has to become intracellular to multiply. tc7b: In vitro T.cruzi infection of macrophages showing the presence of amastigotes: immunofluorescence assay showing T.cruzi amastigotes after treatment with anti-T.cruzi polyclonal mouse sera.

T. cruzi: trypomastigotes in the host cell transform into amastigotes,which multiply intracellularly by binary division inducing inflammatory and immunological responses in vivo, and destroy cells in vitro. Amastigotes are then released into the blood stream as trypomastigotes.The latter are nondividing forms which are able to infect a wide range of new host cells but muscle and glia seem most often parasitized,or they have to be ingested by another reduviid bug in order to continue the parasite life cycle in the invertebrate host. tc8: Trypomastigotes reach the myocardial cells and after penetration they multiply as amastigotes with formation of a pseudocyst.

T. cruzi: in the Reduvidae bug the bloodstream derived trypomastigote forms pass along the digestive tract through irreversible morphological transformations in sequence;each developmental stage occurs in a specific portion of the insect's gut. Thus, in the stomach, most blood trypomastigotes change into epimastigotes and rounded forms (sphaeromastigotes). tc9: T.cruzi epimastigote. Immunofluorescence studies using antibodies to a T.cruzi protein named Tc52(immunosuppressive factor which also express a thiol-transferase activity)and confocal microscopy. An intense labeling located at the posterior end of an epimastigote indicate that Tc52 is targeted to the reservosomes(These organelles are small vesicles inside multivesicular structures being formed predominantly at the posterior end of epimastigotes).

T. cruzi: epimastigotes divide actively in the vector's intestine and reach the rectum where a final differentiation results in the infective metacyclic trypomastigotes which are eliminated in the bug's faeces.tc10: T.cruzi epimastigote. Epimastigote reacting with a monoclonal antibody against T.cruzi.

T. cruzi: some researchers have postulated that sphaeromastigotes may change either into short epimastigotes,dividing forms in the intestine, or into long epimastigotes which are nondividing forms but are able to reach the rectum where they transform into the final metacyclic trypomastigote form.In any case, this hypothesis remains controversial.tc10b: T.cruzi epimastigote. Scanning electron microscopyshowing T.cruzi epimastigote.

T. cruzi: there are three phases of the infection. The acute phase usually passes unnoticed but there may be an inflamed swelling or chagoma at the site of entry of the trypanosomes. Romanas'sign is when this swelling involves the eyelids but it occurs only in about 1-2% of the cases.In the acute phase, mortality is less than 5% and death may result from acute heart failure or meningoencephalitis in children less than two years old.Romana’s sign, clinical manifestation tipically observed in the acute phase of some Chagas’ disease patients.

T. cruzi: general symptoms in acute Chagas' diseasemay also include fever, hepatosplenomegaly, adenopathies and myocarditis.Electrocardiographic changes involve sinus tachycardia, prolongation of the P-R interval, primary T-wave changes and low QRS voltage.Chest X-ray can reveal cardiomegaly of different degrees. The intermediate phase is clinically asymptomatic and is detected by the presence of specific antibodies.No parasites are found in bloostream smears but xenodiagnosis could be positive in some cases. Acute Chagas myocarditis (Haematoxylin and Eosin X 160)tc12: Posteroanterior chest radiograph showing enlarged heart due to T.cruzi infection.tc12a: Acute Chagas' disease myocarditis (Haematoxylin and Eosin X160)

T.cruzi parasitize mainly the cardiac muscle but any cell type may be parasitized (smooth muscle cells, hystiocytes): cardiac muscle with amastigotes, H&E stain.
T. cruzi:T. cruzi: the chronic phase of Chagas'disease the chronic phase of Chagas'disease develops 10 - 20 years after infection and affects develops 10 - 20 years after infection and affects internal organs such as the heart,oesophagus and internal organs such as the heart,oesophagus and colon as well as the peripheral nervous system. colon as well as the peripheral nervous system. The lesions of Chagas’ disease are incurable and in The lesions of Chagas’ disease are incurable and in severe casessevere cases patients may die as result of heart patients may die as result of heart failure.failure.

Chagas' disease megacardia (slide from the late Prof.Koberle, Brazil)

Apical aneurysm in Chagas' disease (slide from the late Prof.Koberle, Brazil)

T. cruzi: on the other side, megacolon is associated with abnormal constipation (weeks).Faecal impaction and sigmoid volvulus are side-effects of megacolon.Neurological changes in chronic Chagas' disease include changes at the level of the central, peripheral or autonomic nervous system.
Chagasic megacolon with enlargement of the sigmoid;patient from Morona Santiago province, southeastern Ecuador

X-ray showing megaoesophagus in Chagas' disease
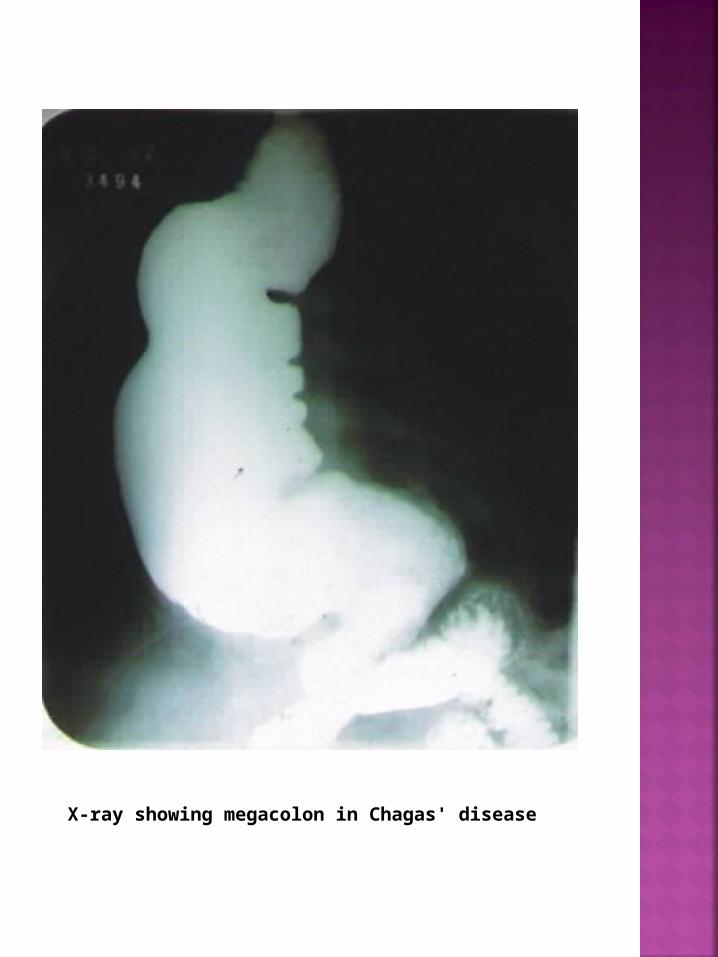
X-ray showing megacolon in Chagas' disease

T. cruzi: can be observed in the peripheral blood only in the acute case of the disease.Its presence is the best definition of the acute phase as all other signs are variable. -Wright-Giemsa staining of T.cruzi trypomastigote in peripheral blood smear from an acute infected patient.-T.cruzi in mouse blood (Giemsa stain)

T. cruzi: trypomastigotes have a prominent subterminal kinetoplast that often distort the membrane of the cell,an elongated nucleus and an undulating membrane. -T.cruzi trypomastigote: blood stream trypomastigotes are 15-20 µm in length and appear with a typical C or S-shaped form.

T. cruzi: multiplication only occurs in the amastigote phase, which grows in a variety of tissue cells especially muscle. -In vitro infected fibroblast showing a large number of intracellular amastigotes.

T. cruzi: laboratory diagnostic tests based on serology (IFA, ELISA) and Polymerase Chain Reaction (PCR) specific for T.cruzi, have been developed. -T.cruzi trypomastigotes reacting with monoclonal Ab.

T. cruzi: serological cross-reactions can occur with infections such as leprosy, leishmaniasis, treponematoses, malaria and multiple myeloma.Trypanosoma rangeli is also an important cause of false-positive testing, especially in areas where T.cruzi coexists with T.rangeli. -In vitro T.cruzi infection of macrophages showing the presence of amastigotes: confocal microscopy showing T.cruzi amastigotes after treatment with anti-Tc24 mouse sera.

T. cruzi: two drugs are in common use. Nifurtimox (Lampit, production was discontinued in 1991)and Benznidazole (Rochagan). The latter which is now the drug of choice, is given in an oral dose of 6 mg/kg body weight for 30 or 60 days.Both drugs produce anorexia, weight loss, headache and dizziness,gastric irritation, and sometimes peripheral neuritis.Experimental drugs are under evaluation.Treatment of patients in the intermediate or chronic phase is controversial. Congenital Chagas'disease and transfusion-associated acute disease require Rochagan therapy.Transfusion infection can be prevented by donor screening or,by mixing the blood with gentian violet (0,25 gr./L for 24 hours) to kill T.cruzi.Vector control programmes involving insecticide spraying with modern pyretroids and new tools for delivery in endemic areas is being carried out in some Latin American countries. tc20: TEM microphotograph of T.cruzi epimastigote.

ZOOMASTIGOPHOREA ZOOMASTIGOPHOREA Order:Order: Kinetoplastida Kinetoplastida

TRYPANOSOMA TRYPANOSOMA BRUCEI RHODESIENSE /BRUCEI RHODESIENSE /
T.B. GAMBIENSE T.B. GAMBIENSE

Sleeping sickness occurs in Africa between the 15° North and the 20° South. The T.b.rhodesiense form is found in East and Central-East Africa whereas the T.b.gambiense infection occurs in Central and West Africa.

The African trypanosomiasis is transmitted by several species of tse-tse flies (Glossina spp.).
Larva and pupae of Glossina morsitans
Adult Glossina tachinoides in West Africa

T. b. gambiense and rhodesiense: two forms of trypomastigote can be seen in peripheral blood: one is long slender, 30 µm in length,and is capable of multiplying in the host, the other is stumpy, not dividing,18 µm in length.

Trypanosoma brucei gambiense and rhodesiense: trypanosomes appear in the peripheral blood 5 to 21 days after the infecting bite.
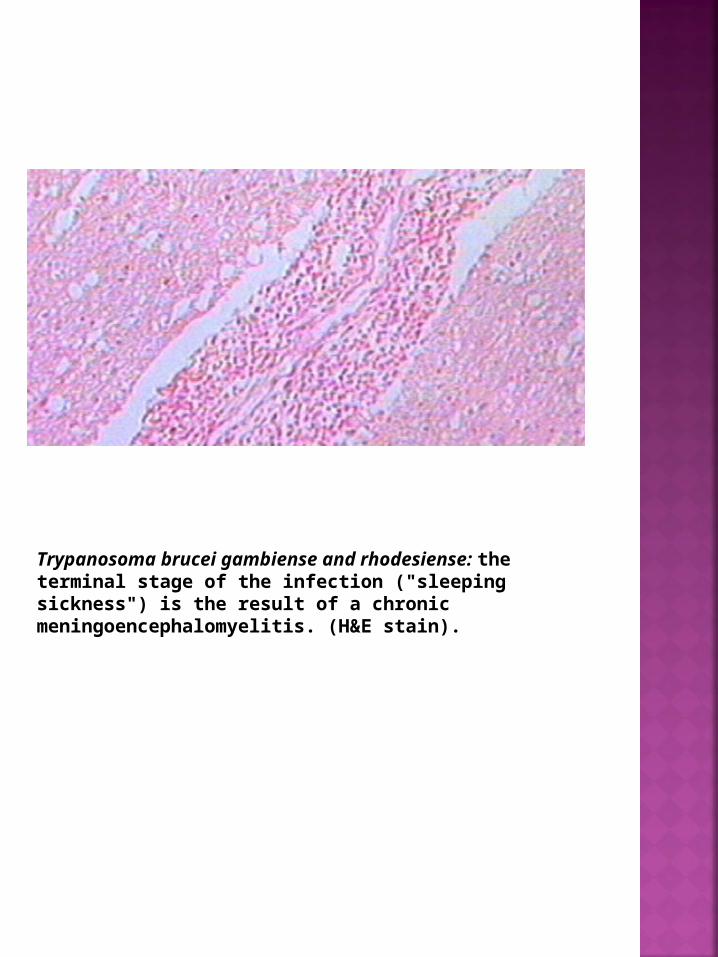
Trypanosoma brucei gambiense and rhodesiense: the terminal stage of the infection ("sleeping sickness") is the result of a chronic meningoencephalomyelitis. (H&E stain).

Trypanosoma brucei gambiense and rhodesiense: the typical pathological lesion of trypanosomiasis is a perivascular round-cell infiltration (perivascular cuffing) due to glial cells, lymphocytes and plasmocytes (Mott cells). (H&E stain).

LEISHMANIA DONOVANI LEISHMANIA DONOVANI

Visceral leishmaniasis has a wide geographic distribution.North-Eastern China, India, Middle-East, Southern Europe (Mediterranean bassin), Northern Africa, Central-East Africa and, in foci, Central and South America(especially Brazil and Honduras).
The infection is transmitted by various species of Phlebotomus, the sand fly.

Leishamnia spp. wich affect humans can be differentiated by geographical distribution, clinical spectrum, immunological features,isoenzymes and Kinetoplast DNA (kDNA) characterization. (Leishmania amastigotes, bone marrow aspirate, Giemsa stain).

Visceral leishmaniasis (Kala-azar) is caused by parasites of the genus Leishmania, subgenus Leishmania, complex donovani (donovani, infantum, chagasi species).Viscerotropic strains of L.infantum and L.tropica have been described. (bone marrow aspirate)

Diagnosis of the infection depends on identification of amastigotes in tissues (bone marrow, spleen, liver, limph nodes) or in blood.Other organs may be affected, expecially in HIV-1 positive patients (intestinal and respiratory tract).Amastigotes can be found inside and outside the reticuloendothelial cells. They measure 2-5 µm, are oval with a large nucleus (in red), a kinetoplast (usually perpendicular, in red to violet) and a pale blue cytoplasm.(Bone marrow aspirate).

Leishamnia sp.: Cultures (on NNN or Tobie media) of blood or tissues samples may permit isolation of the parasite, allowing the subsequent characterisation. When introduced in culture the amastigotes transform into promastigotes in 7-21 days. (Wet mount preparation).
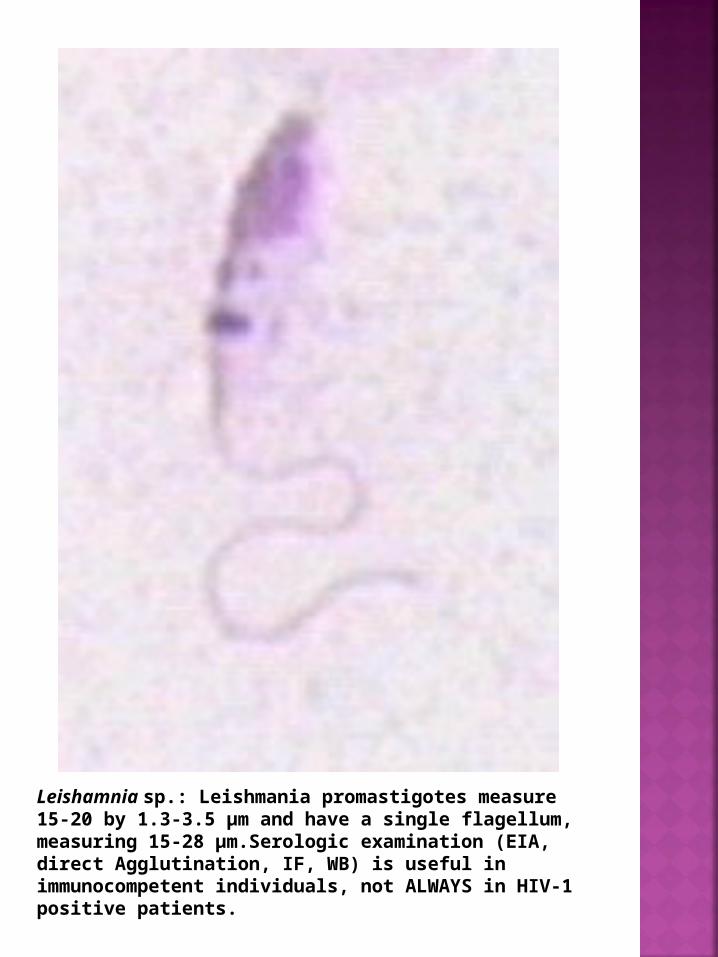
Leishamnia sp.: Leishmania promastigotes measure 15-20 by 1.3-3.5 µm and have a single flagellum, measuring 15-28 µm.Serologic examination (EIA, direct Agglutination, IF, WB) is useful in immunocompetent individuals, not ALWAYS in HIV-1 positive patients.

Visceral leishmaniasis: liver biopsy can demonstrate the Leishmania amastigotes inside the reticuloendothelial cells. The hepatic structure is preserved.

Visceral leishmaniasis: liver biopsy at higher magnification with intracellular amastigotes.

Visceral leishmaniasis: spleen biopsy is a very high sensitive method of diagnosis but it is not widely used because of the risk of hemorrhage. Splenic tissue is rich in amastigotes allowing a rapid and sensitive diagnosis.

Visceral leishmaniasis: spleen biopsy with intracellular amastigotes.