Blood transfusion: When to transfuse and risks involved Yung Lyou | June 2014 Department of Internal Medicine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Blood transfusion:When to transfuse and risks involvedYung Lyou | June 2014Department of Internal Medicine
‹#›
Case
A 67 y/o male w/ h/o CAD s/p CABG, CKD stage III, HTN, HLD, DM is admitted for community acquired pneumonia. After 3x days of inpatient treatment with IV antibiotics he is ready to be discharged home with oral antibiotics.
His hemoglobin at admission was 8.2 and on admission his anemia was found to be due to CKD. On the day of discharge he is able to climb 2 flights of stairs without dyspnea or CP. On the day of discharge his Hgb is 7.6. His vital signs are temp (36.5 C), HR is 70, BP 120/80, RR 20, 95% on RA.
‹#›
Which of the following is the best approach in treating his anemia?
A) Transfuse 2 units PRBCB) Transfuse to goal Hg >10C) Recheck Hg/HctD) Discharge patent and have PCP follow-up CBC
‹#›
Which of the following is the best approach in treating his anemia?
A) Transfuse 2 units PRBCB) Transfuse to goal Hg >10C) Recheck Hg/HctD) Discharge patient and have PCP follow-up CBC
We will go over this question again at the end of this lecture.

‹#›
Objectives
• Know when pRBC blood transfusion is indicated
• Know when pRBC blood transfusion is not indicated
• Know some of the basic risks of blood transfusion
‹#›
Goals of blood transfusion
• Increase oxygen delivery to tissues
• Relieve symptomatic anemia
‹#›
Basics principles
• Decision should not be based on only hemoglobin value. Think of the whole clinical picture
-Remember the patient is more than just a number
• 1 unit of pRBC will usually increase Hgb by 1
• American Association of Blood Banks (AABB) guidelines should be used in guiding decision when to transfuse
‹#›
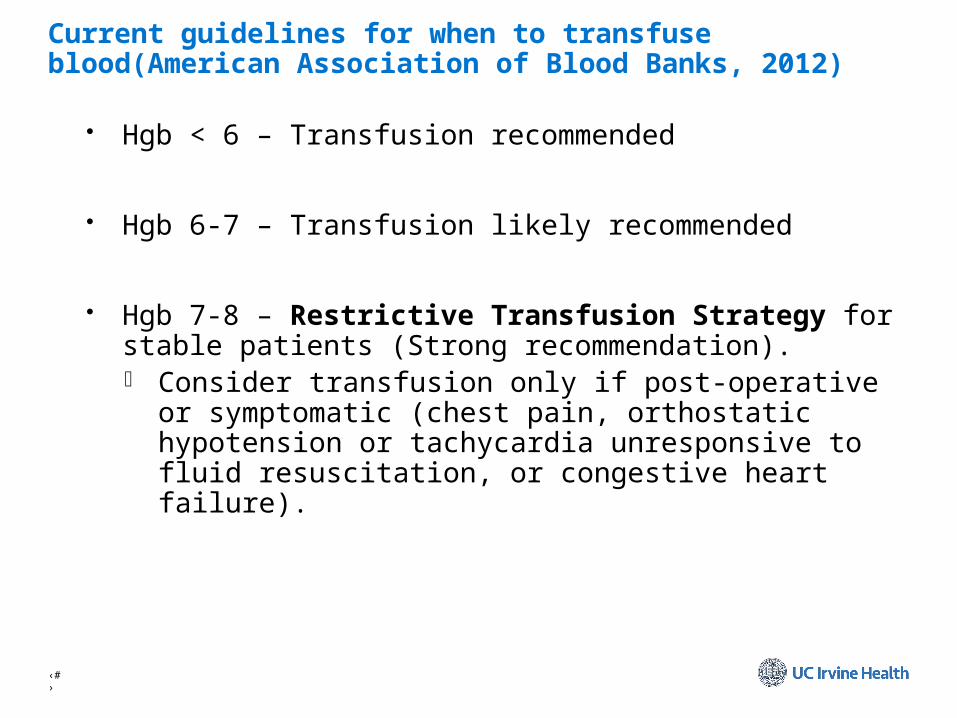
Current guidelines for when to transfuse blood(American Association of Blood Banks, 2012)
• Hgb < 6 – Transfusion recommended
• Hgb 6-7 – Transfusion likely recommended
• Hgb 7-8 – Restrictive Transfusion Strategy for stable patients (Strong recommendation). Consider transfusion only if post-operative or symptomatic (chest
pain, orthostatic hypotension or tachycardia unresponsive to fluid resuscitation, or congestive heart failure).

‹#›
When NOT to transfuse blood
• Hgb 8 – 10 – TRANSFUSION GENERALLY NOT INDICATED -Exceptions to consider transfusing
ACS w/ active ischemia symptomatic anemia active bleeding critical ill septic shock with ScVO2<70 (although this is now considered
controversial)
• Hgb >10 – TRANSFUSION NOT INDICATED

‹#›
Risks of Blood Transfusion
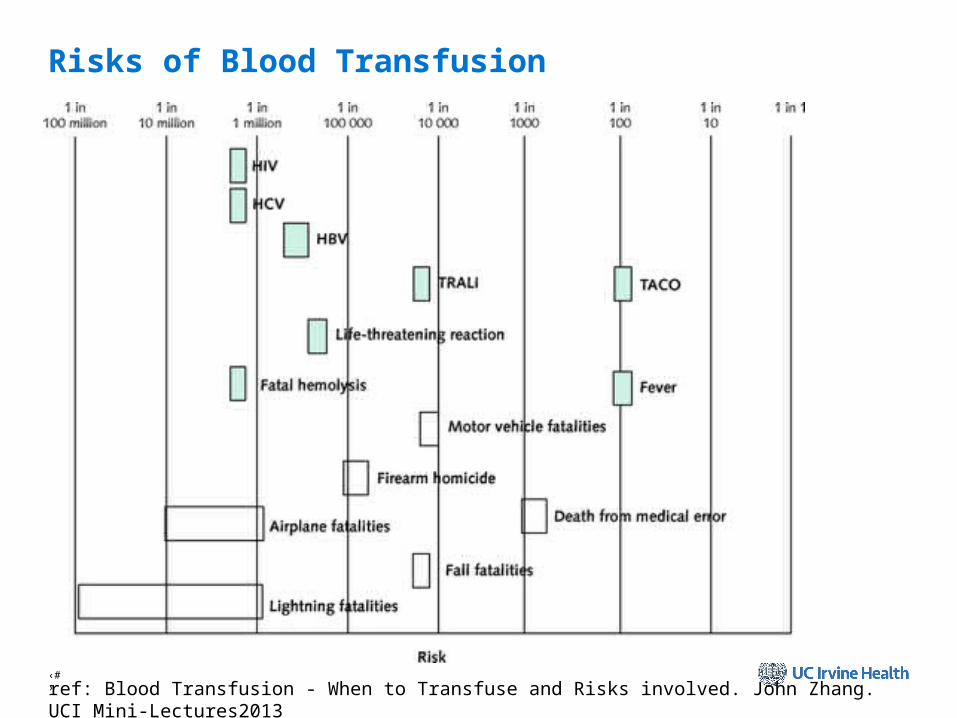
• Transfusion-transmitted pathogens (HIV, HBV, HCV, CMV, bacteria, parasites)
• Allergic and Immunologic Reactions
• Transfusion Associated Circulatory Overload (TACO)
• Transfusion Related Acute Lung Injury (TRALI)
• Electrolyte abnormalities, hyperkalemia, citrate toxicity (metabolic alkalosis or ionized hypocalcemia)
‹#›
Risks of Blood Transfusion
ref: Blood Transfusion - When to Transfuse and Risks involved. John Zhang. UCI Mini-Lectures2013
‹#›
Case
A 67 y/o male w/ h/o CAD s/p CABG, CKD stage III, HTN, HLD, DM is admitted for community acquired pneumonia. After 3x days of inpatient treatment with IV antibiotics he is ready to be discharged home with oral antibiotics.
His hemoglobin at admission was 8.2 and on admission his anemia was found to be due to CKD. On the day of discharge he is able to climb 2 flights of stairs without dyspnea or CP. On the day of discharge his Hgb is 7.6. His vital signs are temp (36.5 C), HR is 70, BP 120/80, RR 20, 95% on RA.
‹#›
Which of the following is the best approach in treating his anemia?
A) Transfuse 2 units PRBCB) Transfuse to goal Hg >10C) Recheck Hg/HctD) Discharge patent and have PCP follow-up CBC
‹#›
Which of the following is the best approach in treating his anemia?
A) Transfuse 2 units PRBCB) Transfuse to goal Hg >10C) Recheck Hg/HctD) Discharge patient and have PCP follow-up CBC

‹#›
Explanation
Answer: D - discharge patient and have PCP follow up CBC
The patient currently has asymptomatic anemia with a decrease in Hgb. This was most likely cause by repeat blood draws during his hospitalization. He has CAD but no chest pain or clinical signs of ACS.
Since he is asymptomatic with no chest pain, dyspnea on exertion, or fatigue blood transfusion is not indicated in this patient at this time according to current AABB.
‹#›
Summary
Evaluate patient’s complete clinical status before ordering transfusion.
Generally avoid transfusion for Hgb above 7 in stable patients without active cardiovascular disease or active bleeding.
Fever and TACO are the most common complications occurring about 1 in 100 transfusions.
‹#›
References
• “RedBlood Cell Transfusion: A Clinical Practice Guideline from the AABB” Ann Intern Med. 2012;157:49-58
• Carson et al. “Mortality and morbidity in patients with very low postoperative Hb levels who decline blood transfusion.” Transfusion 2002
• Blood Transfusion - When to Transfuse and Risks involved. John Zhang. UCI Mini-Lectures2013
• Wang JK, Klein HG. Red blood cell transfusion in the treatment and management of anaemia: the search for the elusive transfusion trigger. Vox Sang. 2010 Jan;98(1):2-11.
• www.uptodate.com
Related Documents