BLOOD SUBSTITUTES IN THERAPY Dr Shahid A Saache Dept. of Pharmacology, BJ GMC, Pune

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
BLOOD SUBSTITUTES IN THERAPY
Dr Shahid A SaacheDept. of Pharmacology,
BJ GMC, Pune
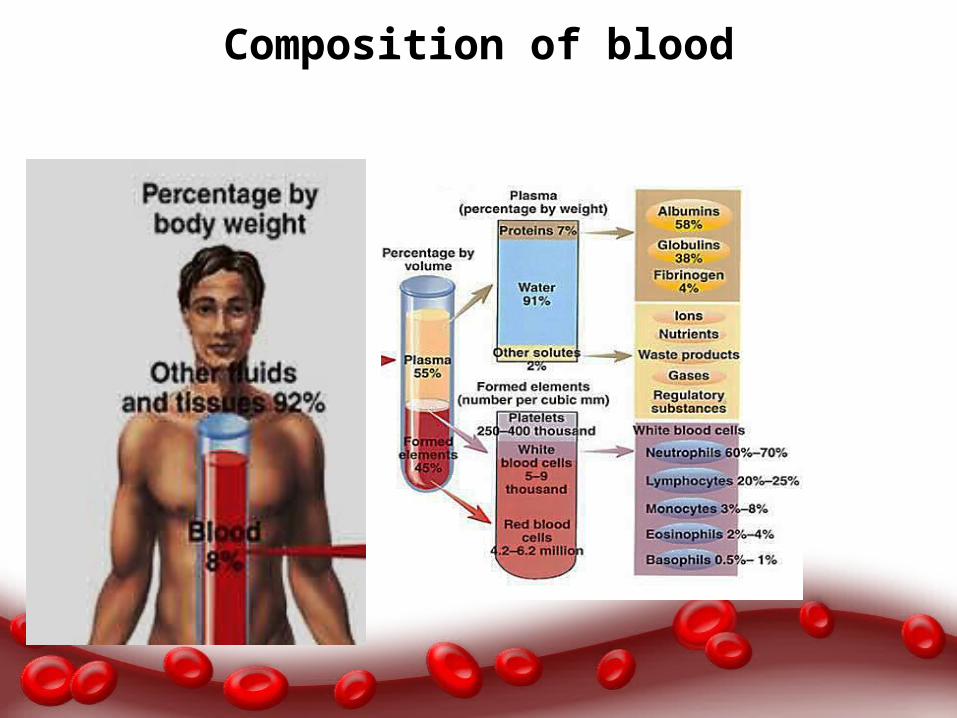
Composition of blood

Major functions of blood
RespirationNutrition ExcretionCoagulationMaintenance of normal acid base balance in the bodyRegulation of body temperature by the distribution of body heat
Regulation of water balance through the effects of blood on the exchange of water between the circulating fluid and the tissue fluidDefence against infectionTransport of hormones and regulation of metabolismTransport of metabolites

A blood substitute is a substance used to mimic and fulfil some functions of biological blood.
It aims to provide an alternative to blood transfusion, which is transferring blood or blood-based products from one person into another.
The Challenge!
The Challenge
• 38,000The number of blood donations needed by India every day!
• 4 CroreNo. of units- every year our nation requires out of which only a meagre 40 Lakh units of blood are available
• 1 million New people are diagnosed with cancer each year• 4
% people in the eligible population of India donates blood
Need for blood substituteShortage: A very important limitation especially during disasters, wars, emergencies, when it is needed most. Short shelf life: This leads to a large amount of wastage of blood. Rare blood groups: This can be a problem, especially in under populated areas or in a situation where there is a large demand for blood. Immunological incompatibility. Disease transmission: HIV, HBV, HCV to name some of the most common pathogens.
Historical aspects
1667 - Jean-Baptiste Denys performed the 1st documented blood transfusion on a 15 yrs. anemic boy with sheep blood.pt. survived, but subsequent transfusions with sheep blood failed1900’s – WWII and Vietnam war ignited the search for blood substitutes - hemoglobin solutions and synthetic O2 carriers1980’s – the search for alternative blood substitutes further fueled by the discovery of HIV and Hep C being transmitted through transfusions
Ideal blood substitute
Oxygen carrying capacity, equalling or surpassing that of biological bloodVolume expansionUniversal compatibility: elimination of cross matchingPathogen free: elimination of blood contained infectionsMinimal side effectsSurvivability over a wider range of storage temperaturesLong shelf lifeCost efficient
Types of blood substitute:
Can serve as – Plasma volume expanders or – Replicate the oxygen carrying function of natural blood
1. Plasma Expanders: These are compounds, which are either entirely synthetic or processed from natural proteins that serve as infusion solutions which expand intravascular volume.2. RBC Substitutes: Modified Haemoglobins - these are essentially human haemoglobins extracted from outdated blood. Perflurocarbons - Synthetic organic compounds that can take over perfusion
Plasma Expanders:
Crystalloids: normal saline, dextrose and ringer lactate.Can serve as volume substitutes and maintain plasma osmolarity.
Colloid: plasma expanders encompass a wide range of substances.These compounds hold water and actually expand volume over the amount infused.
Gelatin: These are modified gelatin polymers, which were among the earliest used colloid expanders, but are now being phased out due to an inherent risk of anaphylaxis.
Dextran: This is a newer generation of colloid expander which uniquely not only expands plasma volume, but also serves to decrease blood viscosity, thereby improving perfusion.
Hydroxyethyl Starch (HES): This is a polymerized form of plant starch which is structurally similar to glycogen and is therefore the safest of the plasma expanders.
Albumins and Purified Protein Derivatives: These are prepared by fractionating albumin and other proteins from pooled human blood and then sterilizing and processing the albumin so that it is iso-osmolar with plasma. These carry the greatest risk of anaphylaxis.
Uses of plasma expanders
Both crystalloids and colloids have a specific role in overall management of hypovolemia & are life saving products for acute emergency situations requiring resuscitation. They are usually used prior to blood transfusion, because no processing or testing of the patient is required for transfusion of expanders and hence can be infused immediately.
Future directions:
Dextrans are currently enjoying a large share of research focus due to potential applications, related to their ability to coat blood cells and prevent thrombus formation. This makes them particularly useful in vascular surgery, such as intravascular stent placement or surgery for DVT.Also, coating of erythrocytes causes mutual repulsion between erythrocytes, and this improves microcirculation. This property has led to investigations of a potential role for dextrans in plastic surgery to improve perfusion and thereby hasten healing of skin grafts.
Problems
Anaplylaxis: This remains the chief drawback with plasma expanders. It is particularly prevalent with gelatins and albumins while HES and Dextrans have a very low reported incidence. Disease transmission: The incidence of transmission of disease is negligible when compared with blood, but cases have been reported. Nephrotoxicity: It is reported especially with dextrans. Volume overload and electrolyte imbalance: Can be prevented by careful titration of transfused amount and monitoring.
Chemicals……..
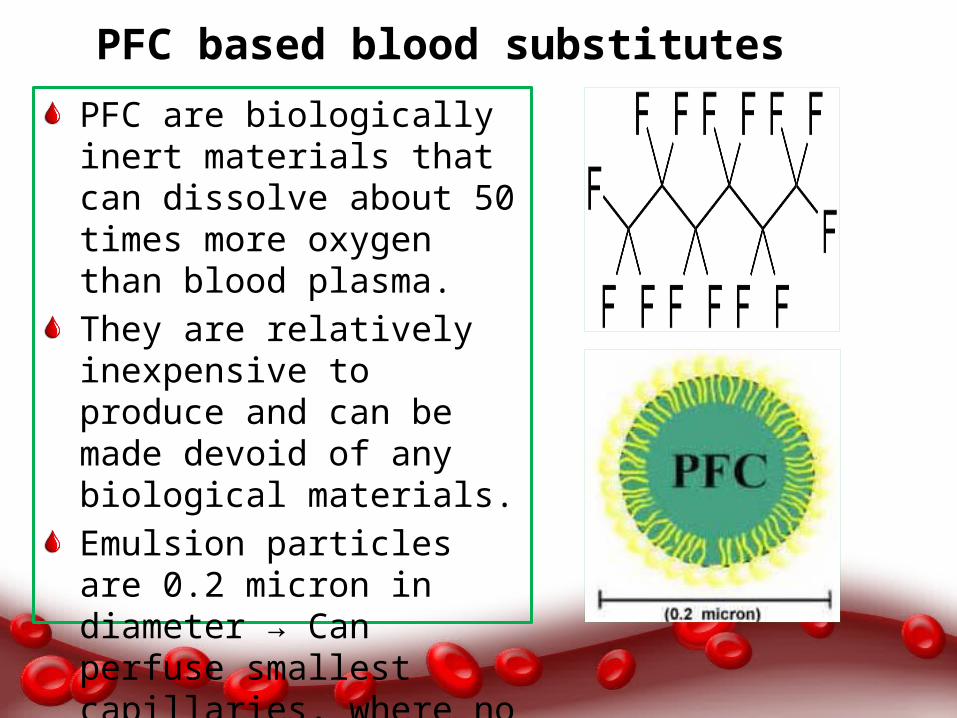
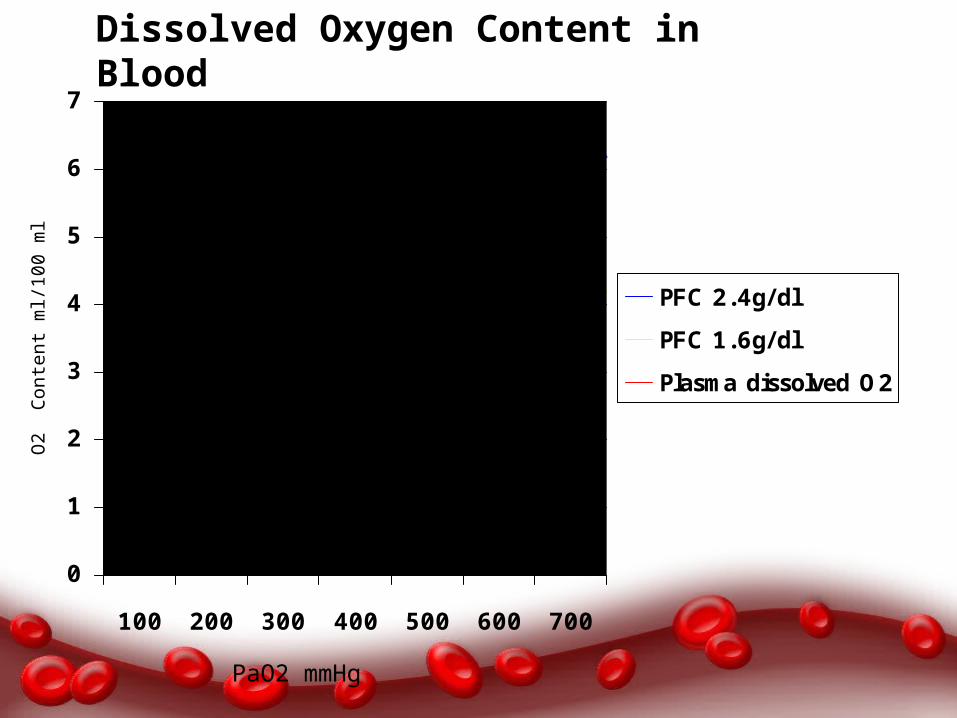
PFC based blood substitutesFC)PFC are biologically inert materials that can dissolve about 50 times more oxygen than blood plasma.They are relatively inexpensive to produce and can be made devoid of any biological materials.Emulsion particles are 0.2 micron in diameter → Can perfuse smallest capillaries, where no RBC flow.
Not soluble in water, which means to get them to work they must be combined with emulsions.Now a day’s most of the PFBOCs are mixtures of perfluorocarbons with emulsifying agentThey have the ability to carry much less oxygen than haemoglobin based products.This means that significantly more PFC must be used.One product of this type has been approved for use by FDA, but it has not been commercially successful because the amount needed to provide a benefit is too high.
0
1
2
3
4
5
6
7
100 200 300 400 500 600 700
PFC 2.4g/dlPFC 1.6g/dlPlasma dissolved O2
PaO2 mmHg
O2
Con
tent
ml/1
00 m
lDissolved Oxygen Content in Blood
Advantages of PFC emulsions
Do not react with oxygen. Inexpensive Allow easy transportation of the oxygen to the body.They allow increased solubility of oxygen in plasma. minimize the effects of factors like pH and temperature in blood circulation.
Disadvantages of perfluorocarbons (PFC) emulsions
Often causes flu-like symptoms.Unable to remain mixed as aqueous solutions – thus, they must be prepared as emulsions for use in patients.A decrease in blood platelet count.PFC products cannot be used by the human body, and must be discarded.
Hemoglobin-based products
PFCs absorb oxygen passively, patients must breathe at a linear rate to ensure oxygenation of tissues.The problem with Fluosal-DA was that they dissolve less oxygen than pure liquids.

Examples of PFC based productsOxygent Currently approved for Phase II Trials in US and Europe,
developed to ↓ need for donor blood during surgery. Done well overall in most clinical trials, but recently, a cardiac surgery study found participants to be slightly more likely to suffer if treated with Oxygent rather than by standard care.
Oxycyte Currently approved for Phase II-b Trials in the US. Targeted as an oxygen therapeutic, with successful small scale open label human trials treating traumatic brain injury.
PHER-O2 In research
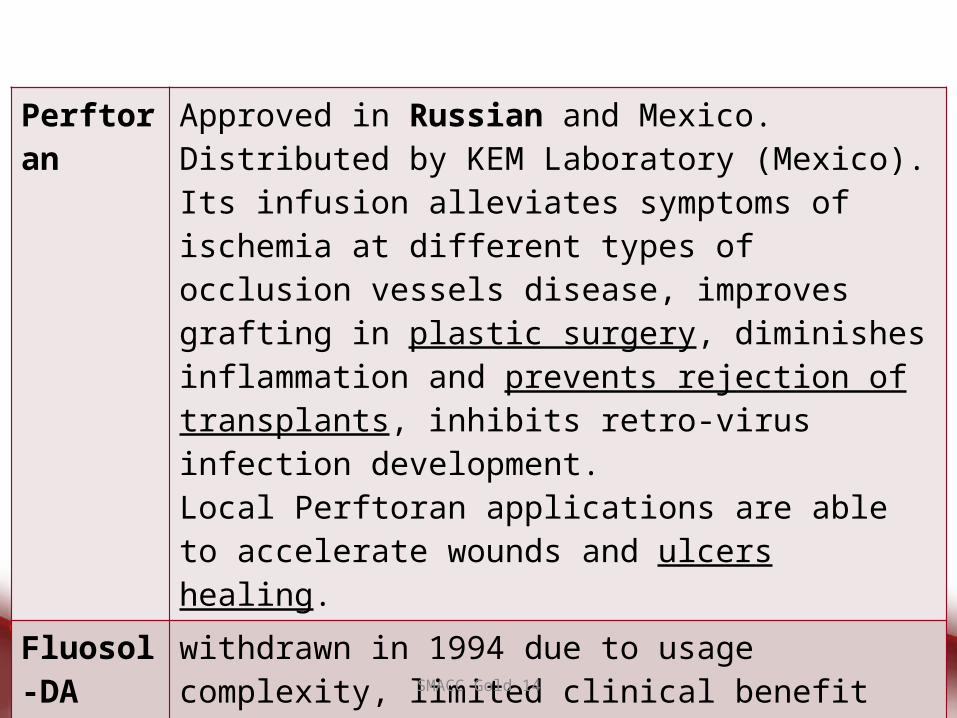
Perftoran Approved in Russian and Mexico. Distributed by KEM Laboratory (Mexico). Its infusion alleviates symptoms of ischemia at different types of occlusion vessels disease, improves grafting in plastic surgery, diminishes inflammation and prevents rejection of transplants, inhibits retro-virus infection development. Local Perftoran applications are able to accelerate wounds and ulcers healing.
Fluosol-DA
withdrawn in 1994 due to usage complexity, limited clinical benefit and complications
SMACC Gold 14

Carriers……..
O2
Hemoglobin Based Oxygen Carriers
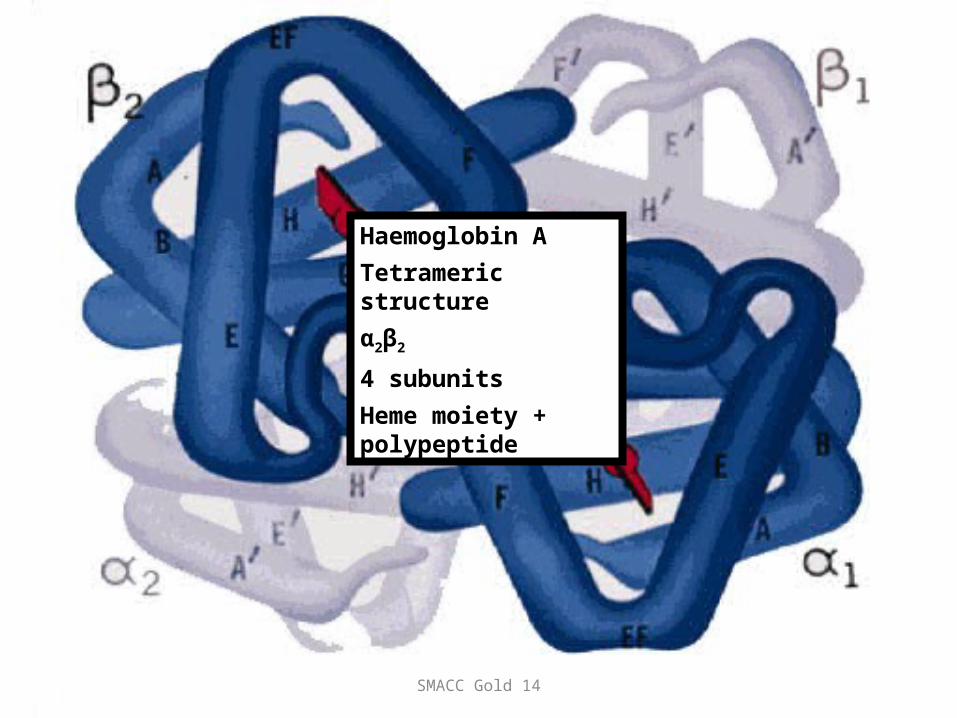
Haemoglobin ATetrameric structure α2β2
4 subunitsHeme moiety + polypeptide
SMACC Gold 14
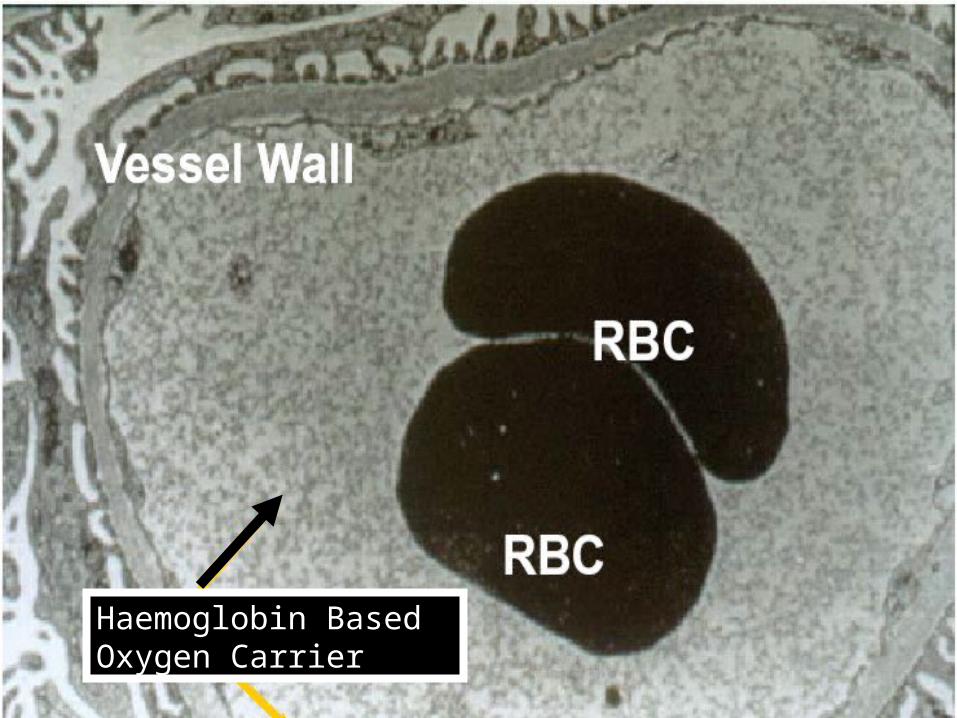
Haemoglobin Based Oxygen Carrier
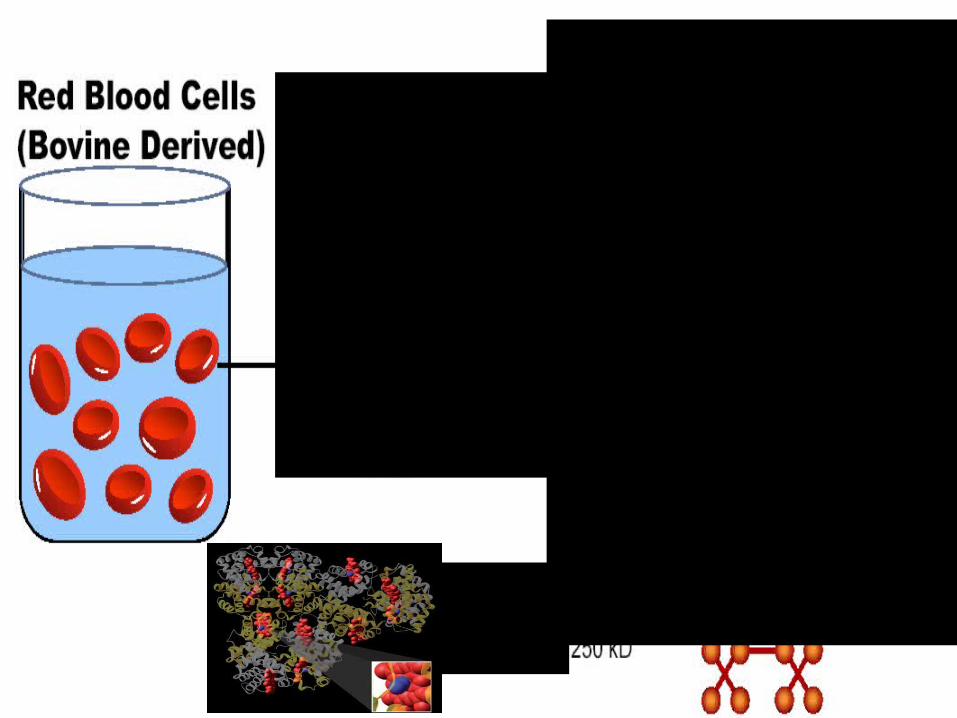
Sources of Haemoglobin
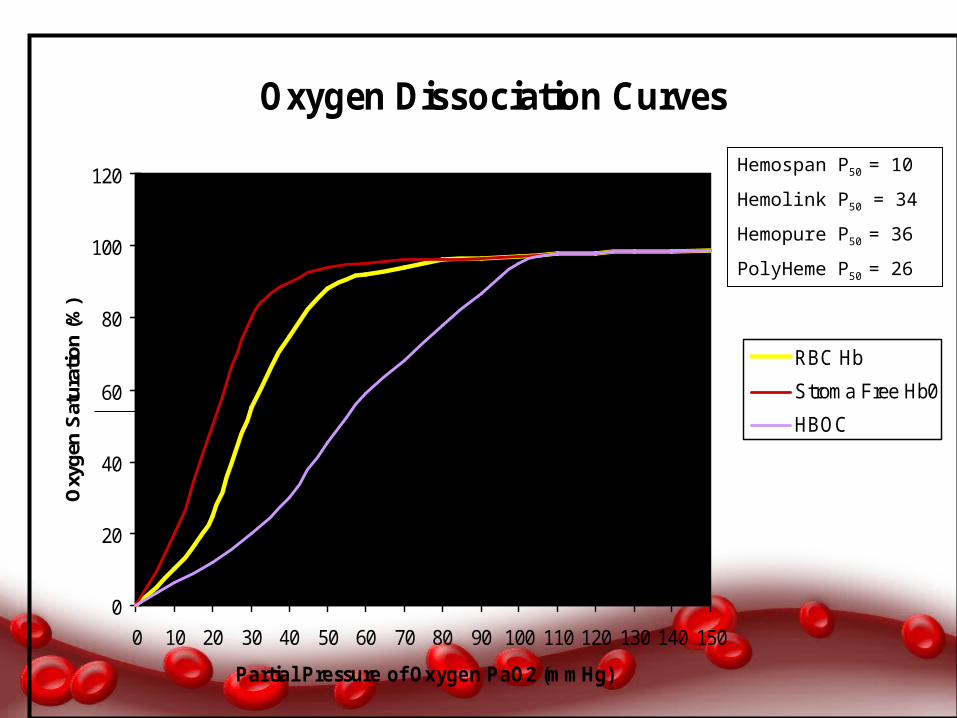
Oxygen Dissociation Curves
0
20
40
60
80
100
120
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150
Partial Pressure of Oxygen PaO2 (mmHg)
Oxy
gen
Satu
ratio
n (%
)
RBC Hb
Stroma Free Hb0
HBOC
Hemospan P50 = 10
Hemolink P50 = 34
Hemopure P50 = 36
PolyHeme P50 = 26
Advantages of HBOCBOCS)-
Available in much larger quantities.Can be stored for long durations.Can be administered rapidly without typing or cross matching blood types.Can be sterilized via pasteurization.
Disadvantages of HBOCRS (HBOCS)
Short half-lifeDisrupts certain physiological structures, especially the gastrointestinal tract and normal red blood cell haemoglobin.They release free radicals into the bodyAvailability and cost
SMACC Gold 14
Nanobiotechnology
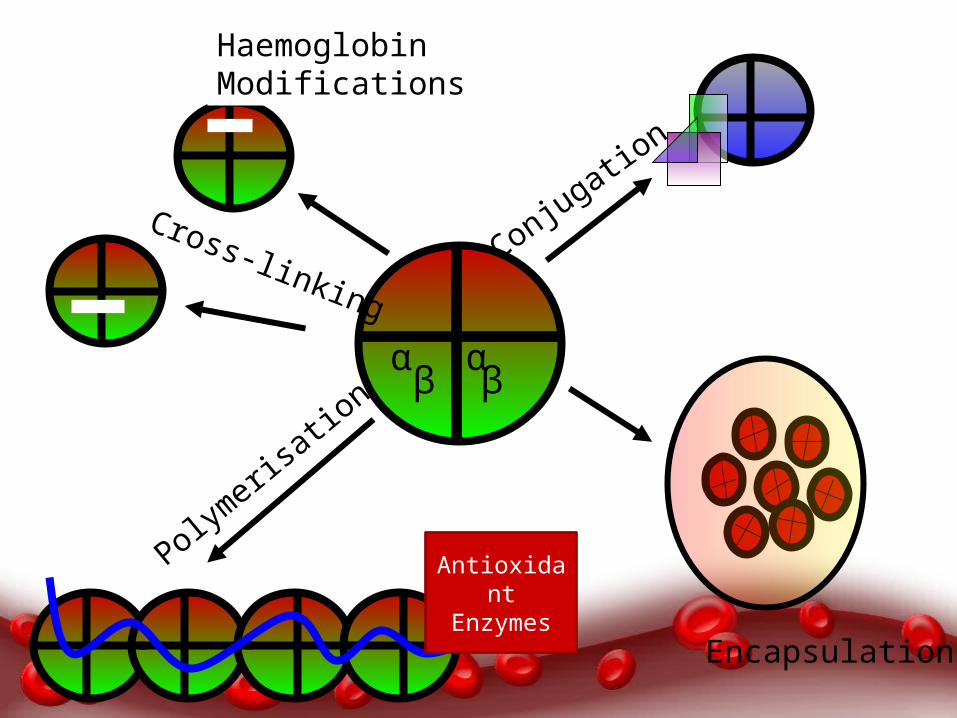
α α
β β
Haemoglobin Modifications
Antioxidant Enzymes
Polymeris
ation
Cross-linking
Conjugation
Encapsulation
SMACC Gold 14
Nanodimension Complete Artificial RBC
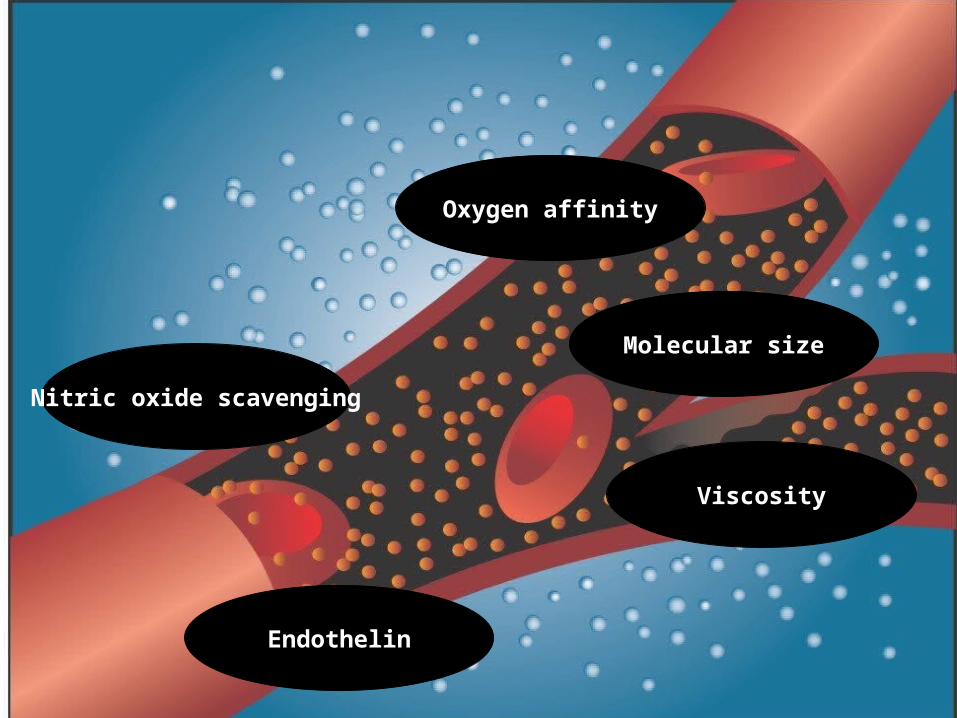
Vasoconstriction
Nitric oxide scavenging
Molecular size
Endothelin
Viscosity
Oxygen affinity

Other Concerns
SMACC Gold 14
Free radical generation
Iron deposition
macrophage function Antigenicity
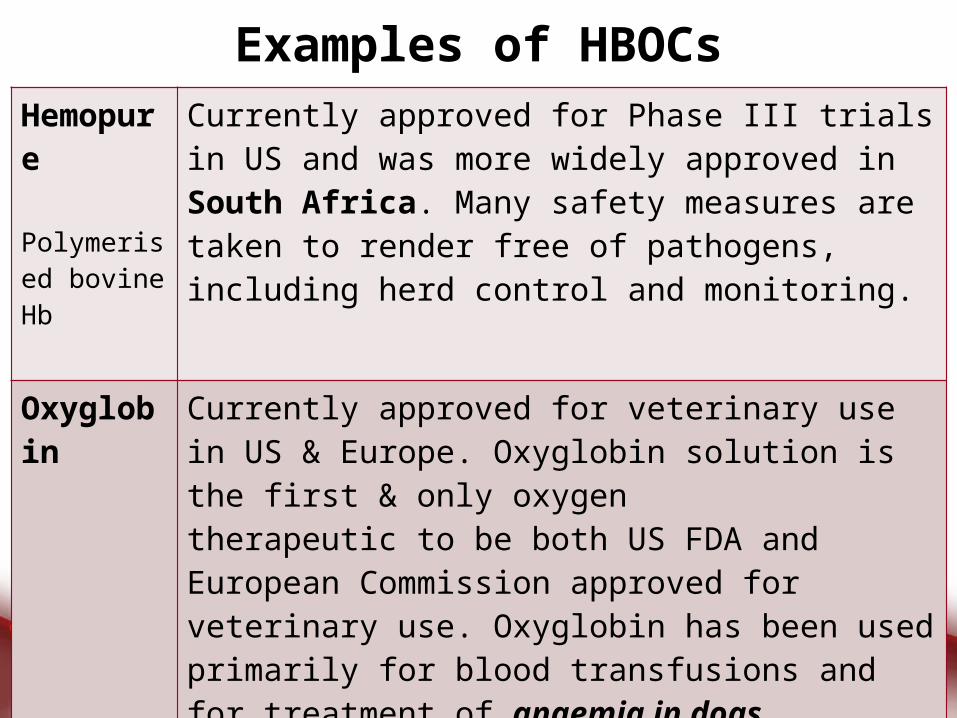
Examples of HBOCsHemopure Polymerised bovine Hb
Currently approved for Phase III trials in US and was more widely approved in South Africa. Many safety measures are taken to render free of pathogens, including herd control and monitoring.
Oxyglobin Currently approved for veterinary use in US & Europe. Oxyglobin solution is the first & only oxygentherapeutic to be both US FDA and European Commission approved for veterinary use. Oxyglobin has been used primarily for blood transfusions and for treatment of anaemia in dogs.
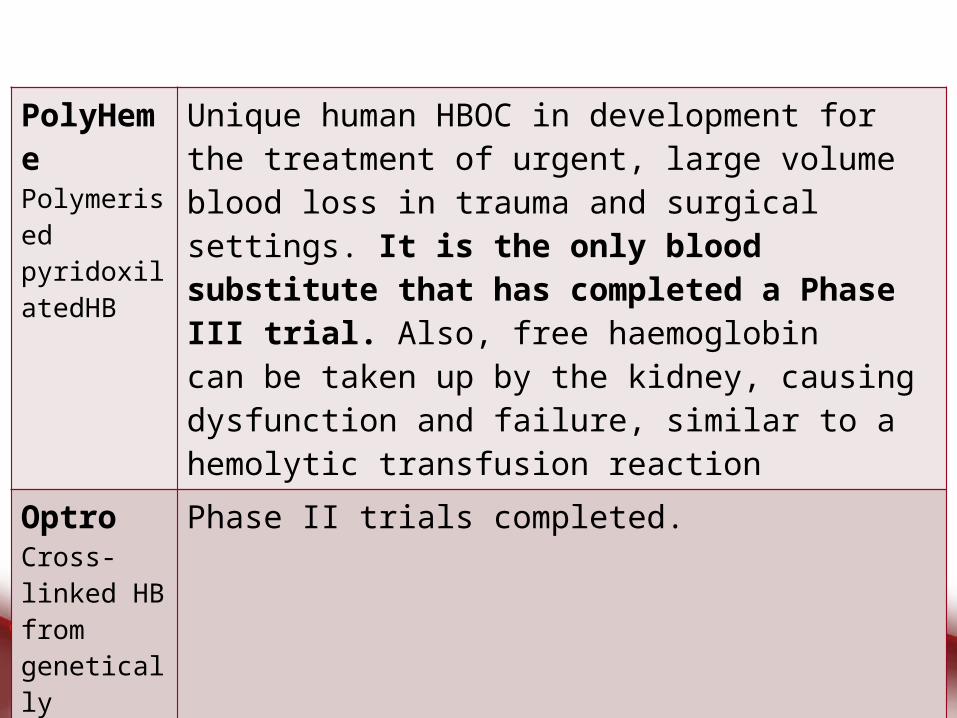
PolyHemePolymerised pyridoxilatedHB
Unique human HBOC in development for the treatment of urgent, large volume blood loss in trauma and surgical settings. It is the only blood substitute that has completed a Phase III trial. Also, free haemoglobincan be taken up by the kidney, causing dysfunction and failure, similar to a hemolytic transfusion reaction
Optro Cross-linked HB from genetically modified E. coli
Phase II trials completed.
HemospanConjugated human Hb
Hemospan is currently in Phase II trials in the US. It is produced in powder form, which can then be mixed into liquid form and transfused immediately, regardless of a patient’s blood type. This technology relies on coupling with polyethylene glycol (PEG) to eliminate the toxicity associated with free haemoglobin.
HemolinkCross-linked human Hb
Phase 3 trials completed. Abandoned due to cardiac toxicity.
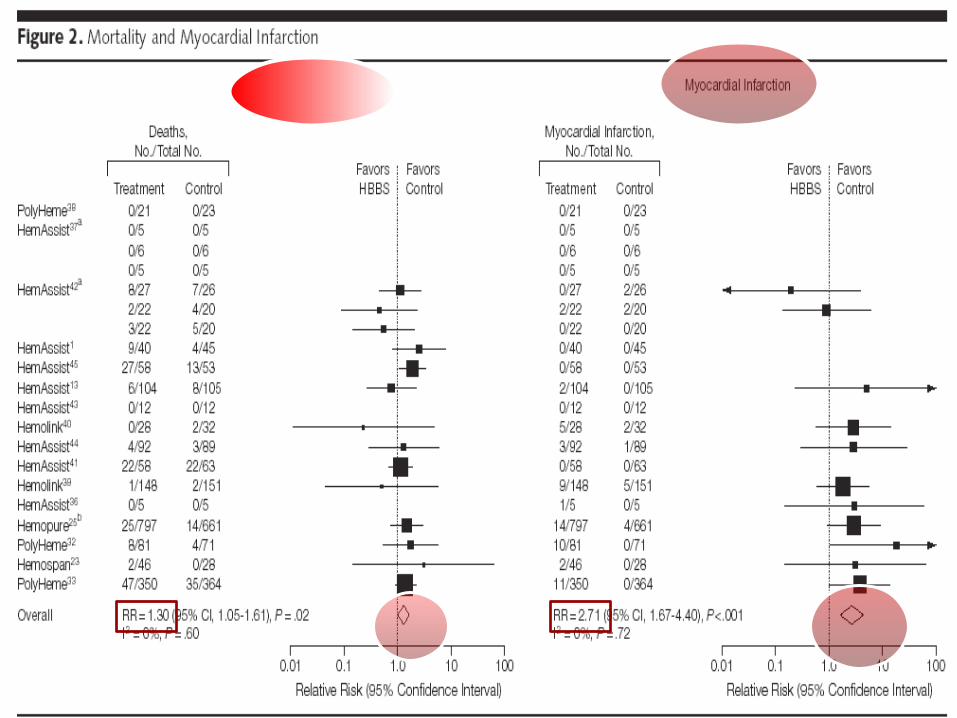
Safety of HBOCs1980 – 200870 trials 16 trials 5 products n =3711

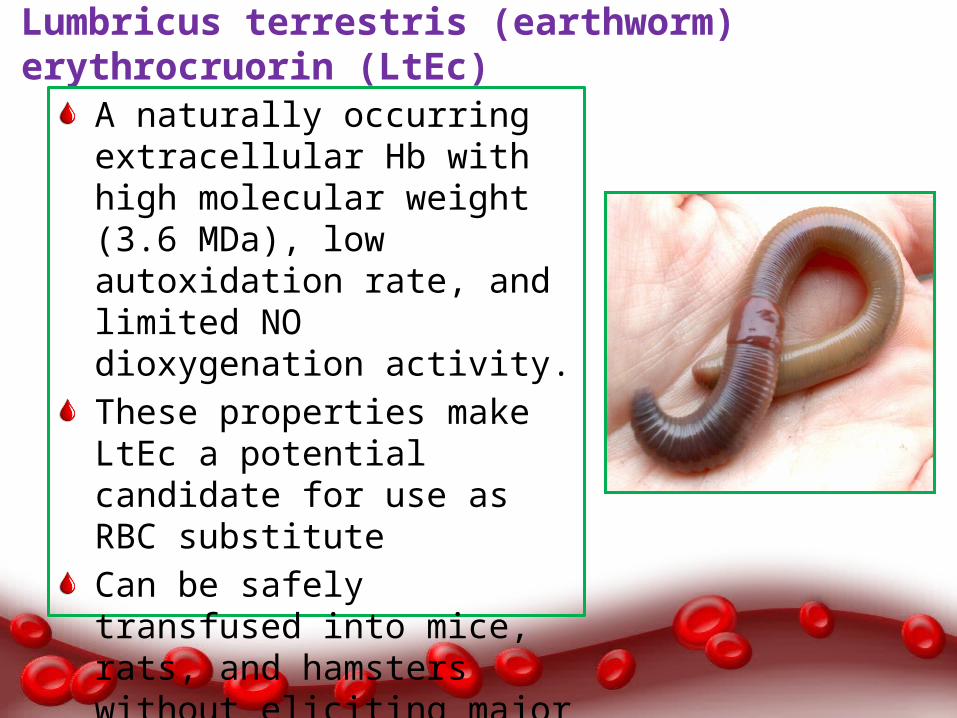
Lumbricus terrestris (earthworm) erythrocruorin (LtEc)
A naturally occurring extracellular Hb with high molecular weight (3.6 MDa), low autoxidation rate, and limited NO dioxygenation activity.These properties make LtEc a potential candidate for use as RBC substituteCan be safely transfused into mice, rats, and hamsters without eliciting major side effects.
Polyhemoglobin-Fibrinogen (polyHb-Fg)
A novel blood substitute that is an oxygen carrier with platelet-like activity.Formed by crosslinking fibrinogen to hemoglobin to form polyhemoglobin-fibrinogen (polyHb-Fg).In the in vitro experiments, PolyHb-Fg showed similar clotting times as whole blood, whereas polyHb showed significantly higher clotting times.
Hemopure, as with any oxygen carrying therapeutic, carries a risk of being used improperly as a performance enhancement in sports.on July 20, 2007, Michael Rasmussen was accused by mountain bike racer Whitney Richards of attempted Hemopure smuggling for potential later use in a doping program.
Platelet substitutes
Infusible platelet membranes
Red cells with surface-bound fibrinogen
Liposome-based agents
Thrombosphere
Blood products grown from stem cellsRBCs may be grown either from embryonic stem cells or hematopoietic progenitor cells.in 2008, Lu et al reported success using embryonic stem cells to grow mature erythrocytes on a large scale.However, the cells produced show a phenotype more consistent with fetal or embryonic erythrocytes than adult blood cells.Further research will be required to increase yields, eliminate potentially tumorigenic nucleated cells, and determine the half-life and immunogenicity of erythrocytes grown from stem cells.
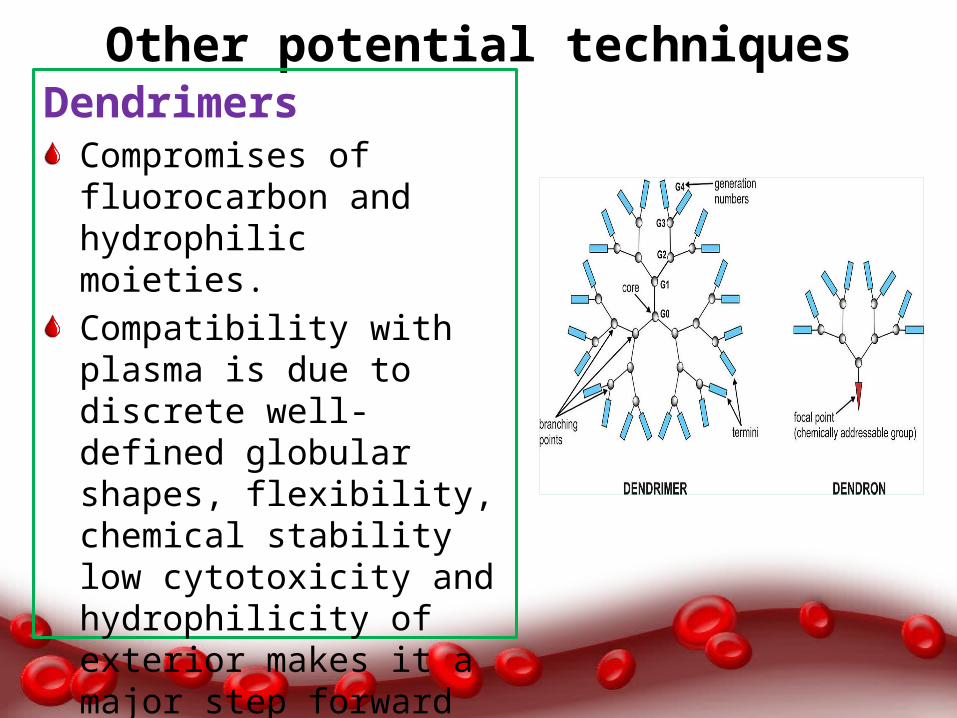
Other potential techniquesDendrimers
Compromises of fluorocarbon and hydrophilic moieties.Compatibility with plasma is due to discrete well defined ‐globular shapes, flexibility, chemical stability low cytotoxicity and hydrophilicity of exterior makes it a major step forward in the field of blood substitutes e.g. Poly amidoamino dendrimers (PAMAM).
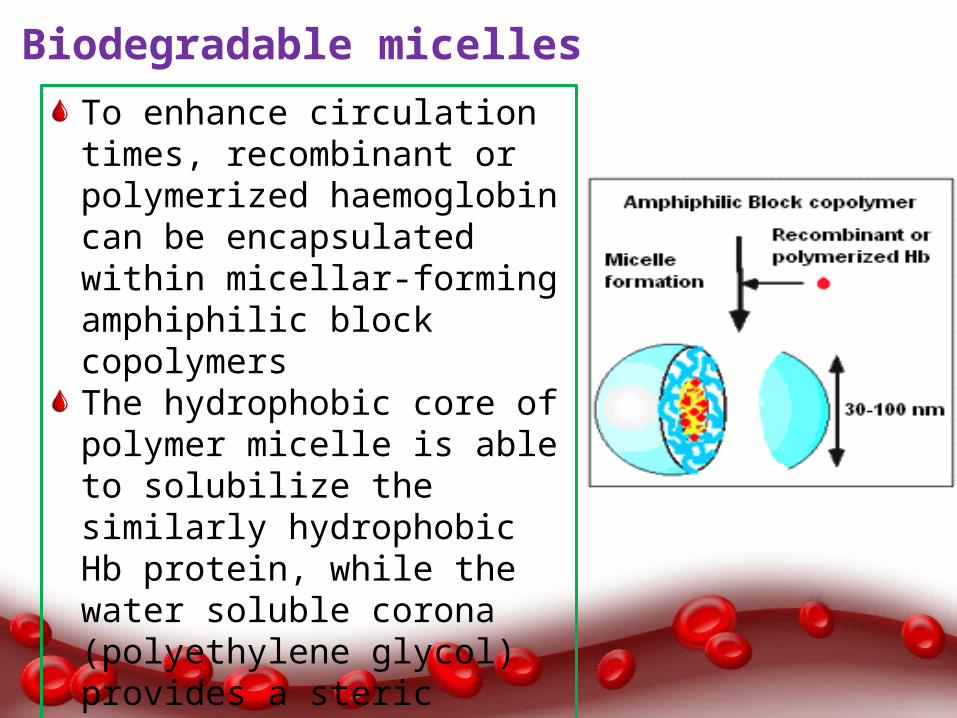
Biodegradable micellesTo enhance circulation times, recombinant or polymerized haemoglobin can be encapsulated within micellar-forming amphiphilic block copolymersThe hydrophobic core of polymer micelle is able to solubilize the similarly hydrophobic Hb protein, while the water soluble corona (polyethylene glycol) provides a steric barrier to protein absorption, and provides protection from clearance by RES.
Placental umbilical cord bloodCord blood collected aseptically from the placenta after the birth of a healthy baby can be used safely as a blood substitute.higher haemoglobin content and growth factors than normal blood from an adult, which has the potential to benefit patients in varying diseases.
RespirocytesAre hypothetical, microscopic, artificial red blood cells that can emulate the function of its organic counterpart with increased efficiency.
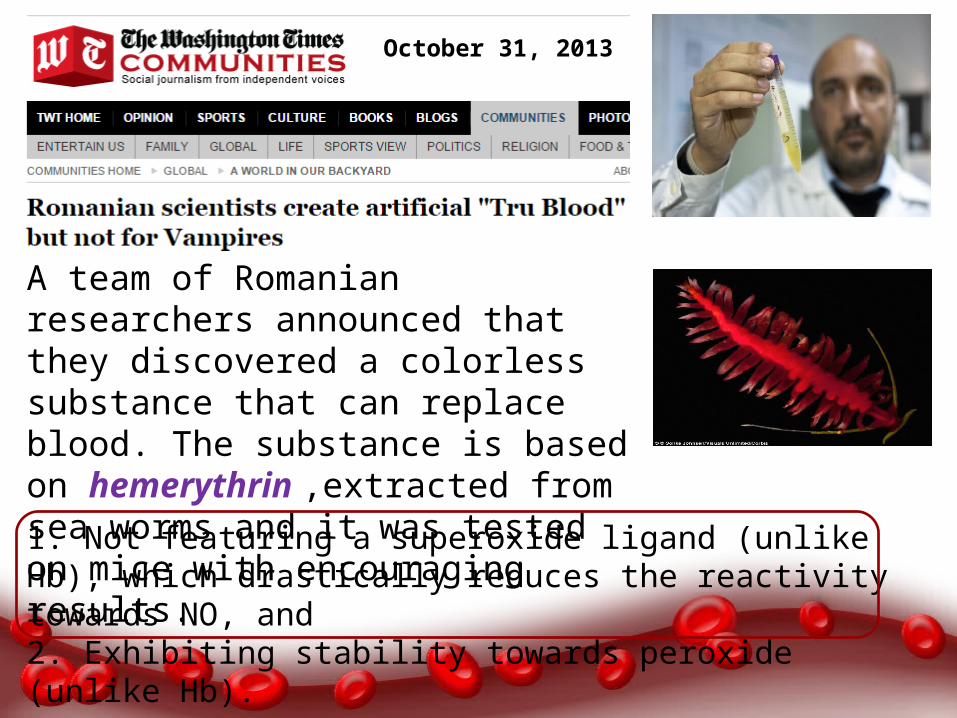
A team of Romanian researchers announced that they discovered a colorless substance that can replace blood. The substance is based on hemerythrin ,extracted from sea worms and it was tested on mice with encouraging results.
October 31, 2013
1. Not featuring a superoxide ligand (unlike Hb), which drastically reduces the reactivity towards NO, and 2. Exhibiting stability towards peroxide (unlike Hb).

The more you sweat in peace, the less you bleed in war.
--Norman Schwarzkopf
THANK YOU
Related Documents











