1-15| Page International Standard Serial Number (ISSN): 2347-4785 Full Text Available On www.ijpbsrd.com IJPBSRD, Vol.2 Issue 5: July 2014 INTERNATIONAL JOURNAL OF PHARMACEUTICAL AND BIOLOGICAL SCIENCES RESEARCH AND DEVLOPMENT IMPACT FACTOR 0.512*** ICV 3.00*** Pharmaceutical Sciences RESEARCH ARTICLE……!!! BLOOD PRESSURE CONTROL AND ITS CONTRIBUTING FACTOR AMONG AMBULATORY HYPERTENSIVE PATIENTS IN ADAMA HOSPITAL MEDICAL COLLEGE, EAST SHOA, ADAMA, ETHIOPIA Gete Chemeda Lichisa 1* , Gobezie Temesgen Tegegne 1 ,Belayneh Kefale Gelaw 1 , Amsalu Degu Defersha 1 , Minyahil Alebachew 1 , Woldu, Jimma Likisa Linjesa 1 1 Department of Pharmacy, College of Medicine and Health Science, Ambo University, Ambo, Ethiopia. KEYWORDS: Hypertension, Systolic Blood Pressure, Diastolic Blood Pressure. For Correspondence: Gete Chemeda Lichisa * Address: Department of Pharmacy, College of Medicine and Health Science, Ambo University, Ambo, Ethiopia. E- mail: [email protected] ABSTRACT Background: Hypertension is a common medical condition worldwide. It is an important public health challenge because of the associated morbidity, mortality, and the cost to the society. BP was poorly controlled in hypertensive patients and hypertensive patients with diabetes. Objective: to asses extent of blood pressure control and to determine factors that affect blood pressure control among attendants of outpatient departments at Adama hospital medical college in east Ethiopia. Methods: A hospital-based retrospective cross- sectional study was conducted on 160 participants aged 17 years or older from March 2014 to April 2014. Simple random sampling was used. Results: The mean age of the participants was 52.4+ 11.4 years. The average mean of BP in 12 months was 140.58/80.92mmHg; the overall control rate was 43.6%. most of the patients had uncontrolled BP. There was mean BP difference among eight months. Age, sex, area, diagnosis, presence of co morbidity and number of drug had no effect on blood pressure control. Conclusions: The average mean SBP and DBP obtained in 12 month were above the goal of BP needed. Greater than half of the participants had uncontrolled BP in data collection time (April 2014. Age, sex, area, diagnosis, presence of co morbidity and number of drug were not associated with BP control.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
IJPBSRD, Vol.2 Issue 5: July 2014
INTERNATIONAL JOURNAL OF PHARMACEUTICAL AND BIOLOGICAL SCIENCES RESEARCH AND DEVLOPMENT
IMPACT FACTOR 0.512***
ICV 3.00*** Pharmaceutical Sciences RESEARCH ARTICLE……!!!
BLOOD PRESSURE CONTROL AND ITS CONTRIBUTING FACTOR
AMONG AMBULATORY HYPERTENSIVE PATIENTS IN ADAMA
HOSPITAL MEDICAL COLLEGE, EAST SHOA, ADAMA, ETHIOPIA
Gete Chemeda Lichisa1*
, Gobezie Temesgen Tegegne1 ,Belayneh Kefale Gelaw
1 ,Amsalu Degu
Defersha1, Minyahil Alebachew
1, Woldu, Jimma Likisa Linjesa
1
1Department of Pharmacy, College of Medicine and Health Science, Ambo University, Ambo,
Ethiopia.
KEYWORDS:
Hypertension, Systolic
Blood Pressure, Diastolic
Blood Pressure.
For Correspondence:
Gete Chemeda Lichisa *
Address:
Department of Pharmacy,
College of Medicine and
Health Science, Ambo
University, Ambo,
Ethiopia.
E- mail:
ABSTRACT
Background: Hypertension is a common medical condition
worldwide. It is an important public health challenge because of the
associated morbidity, mortality, and the cost to the society. BP was
poorly controlled in hypertensive patients and hypertensive patients
with diabetes. Objective: to asses extent of blood pressure control and
to determine factors that affect blood pressure control among
attendants of outpatient departments at Adama hospital medical college
in east Ethiopia. Methods: A hospital-based retrospective cross-
sectional study was conducted on 160 participants aged 17 years or
older from March 2014 to April 2014. Simple random sampling was
used. Results: The mean age of the participants was 52.4+11.4 years.
The average mean of BP in 12 months was 140.58/80.92mmHg; the
overall control rate was 43.6%. most of the patients had uncontrolled
BP. There was mean BP difference among eight months. Age, sex,
area, diagnosis, presence of co morbidity and number of drug had no
effect on blood pressure control. Conclusions: The average mean SBP
and DBP obtained in 12 month were above the goal of BP needed.
Greater than half of the participants had uncontrolled BP in data
collection time (April 2014. Age, sex, area, diagnosis, presence of co
morbidity and number of drug were not associated with BP control.
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
INTRODUCTION:
Hypertension was defined as a persistent systolic blood pressure reading (SBP) of 140mmHg or
greater and or a diastolic blood pressure reading (DBP) of 90mmHg or greater and or taking of
antihypertensive medication.(1)
The exact causes of high blood pressure are not known, but several factors and conditions may
play a role in its development, including Smoking, Being overweight or obese, Lack of physical
activity, Too much salt in the diet, Too much alcohol consumption (more than 1 to 2 drinks per
day), Stress, Older age, Genetics, Family history of high blood pressure, Chronic kidney disease
and Adrenal and thyroid disorders(2). According to the Eighth Joint National Committee on the
management and the goal of hypertension there was strong evidence to support treating
hypertensive persons aged 60 years or older to a BP goal of less than 150/90mmHg and
hypertensive persons 30 through 59 years of age to a diastolic goal of less than 90mmHg;
however, there was insufficient evidence in hypertensive persons younger than 60 years for a
systolic goal, or in those younger than 30 years for a diastolic goal, so the panel recommends a
BP of less than 140/90mmHg for those groups based on expert opinion. The same thresholds and
goals are recommended for hypertensive adults with diabetes or no diabetic chronic kidney
disease (CKD) as for the general hypertensive population younger than 60 years (3). They are
many factors that cause uncontrolled hypertension. These factors include modified and non
modified factors. Non modified factors are age, gender, ethnicity and family history .modifiable
factors include compliance, access to health care, and life style.(1)
The World health organization (WHO) has estimated that about 62% of cerebro-vascular and
49% of ischemic heart disease burden, World Wide, are attributable to suboptimal blood pressure
levels. High blood pressure was estimated to cause 7.1million death annually, accounting for
13% of all deaths globally.(4)
The prevention and control of hypertension has not received due attention by many developing
Countries. However, awareness about treatment and control of hypertension was extremely
low among developing nations including Ethiopia .In these countries health care resources are
over whelmed by other priorities including HIV/AIDS, tuberculosis and malaria (5)
Statement of the problem
Hypertension was a serious public health problem worldwide. It is the leading cause of death in
the world and it’s the commonest cause for outpatient visits to physicians(6). Therefore,
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
hypertension was an important public health problem accounting for about 6% of deaths world
wide .As much as 1 billion people have hypertension world wide and 7.1 million deaths a year
may be attributable to hypertension (7)
In Africa, 15% of the population has hypertension. Although there was shortage of extensive
data, 6% of the Ethiopian population has been estimated to have HTN. Approximately 30% of
adults in Addis Ababa have hypertension above 140/90mmHg or reported use of anti-
hypertensive medication. This indicates an urgent need for strategies and programmers to
prevent and control high blood pressure, and promote healthy lifestyle behaviors primarily
among the urban populations of Ethiopia(8).
Hypertension was a risk factor for all clinical manifestations of atherosclerosis since it was a risk
factor for atherosclerosis itself. It was an independent predisposing factor for heart
failure, coronary artery disease stroke, renal disease, and peripheral arterial disease. It was the
most important risk factor for cardiovascular morbidity and mortality.
With regard to the two main cardiovascular consequences of hypertension – coronary heart
disease and stroke the British Heart Foundation Health Promotion Research Group has calculated
the economic burden for the UK at 1999 prices. The total costs (direct healthcare, informal care
and lost productivity) are equivalent to about £7.06 billion for coronary heart disease and £5.77
billion for stroke. Taking into account the WHO estimates of the contribution raised blood
pressure (115/75mmHg or above) makes to coronary heart disease (49%) and stroke (62%), the
total cost burden of raised blood pressure for these two diseases alone amounts to over £7 billion
at 1999 prices, to say nothing of the additional costs incurred by other health consequences such
as heart failure and renal disease.
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
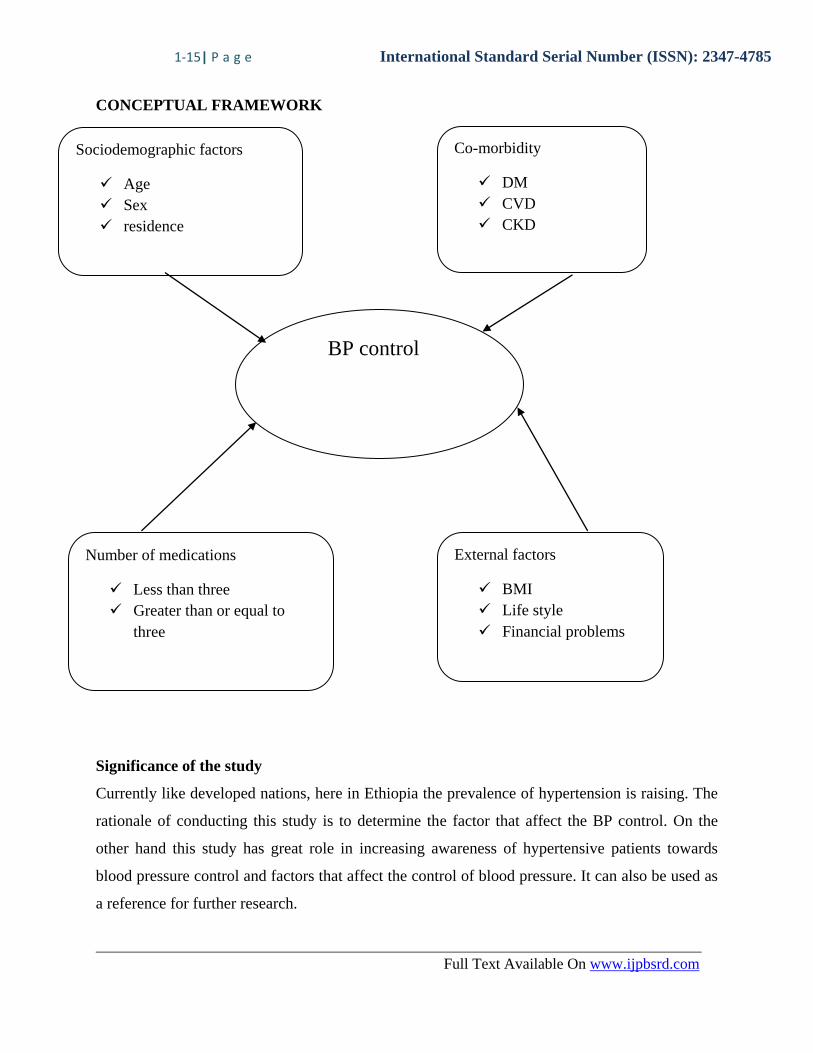
CONCEPTUAL FRAMEWORK
Significance of study
Significance of the study
Currently like developed nations, here in Ethiopia the prevalence of hypertension is raising. The
rationale of conducting this study is to determine the factor that affect the BP control. On the
other hand this study has great role in increasing awareness of hypertensive patients towards
blood pressure control and factors that affect the control of blood pressure. It can also be used as
a reference for further research.
BP control
Co-morbidity
DM
CVD
CKD
Sociodemographic factors
Age
Sex
residence
Number of medications
Less than three
Greater than or equal to
three
External factors
BMI
Life style
Financial problems
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
Objectives
General objective
To assess extent of blood pressure control and factors affecting it in Adama General
Hospital.
Specific objectives
To evaluate the extent of blood pressure control in 12 months
To assess factors that affect BP control
Methods
The Study Area and Period
The study was conducted in Adama Hospital Medical College. The hospital is located in Central
Ethiopia, Oromia regional state, in Adama town 99 km from Addis Ababa on Ethio-Djibuti main
road. It was established in 1942 by Italian Missionaries. The hospital was named as
Hailemariam Mammo memorial hospital little bit after establishment but its name was changed
to Adama Referral Hospital in mean time and now it renamed as Adama Hospital Medical
College by Oromia regional state health bureau after it enrolled students in different programs
like accelerated medicine, emergency surgery and some specialties in 2012. Currently the college
hospital has catchment population of about 5 million serving as referral hospital for all nearby
hospitals and the adjacent regions. It has capacity of 200 beds for inpatient with five disciplines
(Surgery, Internal medicine, pediatrics, Gynecology/Obstetrics and ophthalmology) with four
pharmacies (OPD, ward, emergency and ART pharmacy) and serves about 850 patients per day
at OPD during working hours and on average 52 patients per day after working time in private
wing clinic. The hospital has about 465 workers of which 257 were health professionals and the
remaining are administrative workers and teachers. The hospital is now working in collaboration
with Adama General Hospital and Medical College (AGHMC). The study was undertaken from
01 March – 01 June, 2014.
Study design
- A retrospective cross sectional study was conducted.
Population
Source of population
All ambulatory hypertension patients in Adama medical college hospital.
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
Study population
The study populations were patients with hypertension, who were using antihypertensive
treatment and attending at Adama medical college hospital for the last one year.
The inclusion criteria
Patients who were on one follow up for the last one year.
Exclusion criteria
1) Patients who have no complete information
2) Patients less than 17 years of age.
Sample size and sampling techniques
Sample size was calculated from the source population using sample size determination formula
and a convenience sample was drawn from patient who fulfill the criteria
n= Z2 P (1-P)
D2
Where:
n- Sample size
Z- Confidence level = 95% (1.96)
P- Anticipated proportion = 50% (0.5) to allow maximum sample size
D- Margin of errors = 5% (0.05)
There was no study done on factors affecting blood pressure control in Adama Hospital Medical
College in the past. We use proportional (p) 50%, So the sample size will be:
n = (1.96)2 (0.5) (1-0.5)
(0.05)2
n= 384
There were 251 patients who fulfill inclusion criteria.
N =215
Therefore the corrected sample size was calculated as:
Nf= n/ (1+n/N)
Nf= 384/ (1+384/251) = 152 cards
Allowance of 5% =0.05x152 = 8
Therefore total sample size = 160 patients
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
From patients record card who are attending at hypertension clinics in Adama referral medical
collage who met the inclusion criteria, were eligible for inclusion in the sampling list for the
study. Simple random sampling procedure was employed to select the study participants.
Study variables
Dependent variable
Blood pressure control
Independent variables
Age
Sex
Resident area
Assessment
Number of drug
Presence of co morbidity
Data collection tools and techniques
Data were collected from the patient record card on check list.
Data quality management
A pretest was done by the student on 5 patient cards 2 week prior to actual data collection. The
collected was cheeked daily for consistency and accuracy.
Data analysis
The data were cleaned, edited, and entered into a computer to be analyzed using SPSS version
20.0. Logistic regression was used to analyze the associations between different variables, and
other descriptive statistics were used where necessary. Repeated measure ANOVAs and post hoc
analysis were performed to analyze the BP difference among 12 months.
Ethical consideration
Prior to data collection, official letter was obtained from department of pharmacy in order to get
permission from the medical director and research office. The name of the patient was not
mentioned and the entire secret was kept for patient confidentiality.
Result
Socio –demographic characteristics
A total of 160 patients were involved. The mean age was 52.4 + 11.4 years, with a range from 30
to 77 Years. 64 (40%) of them were men while 146 (91.3%) of them were from urban. Greater
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
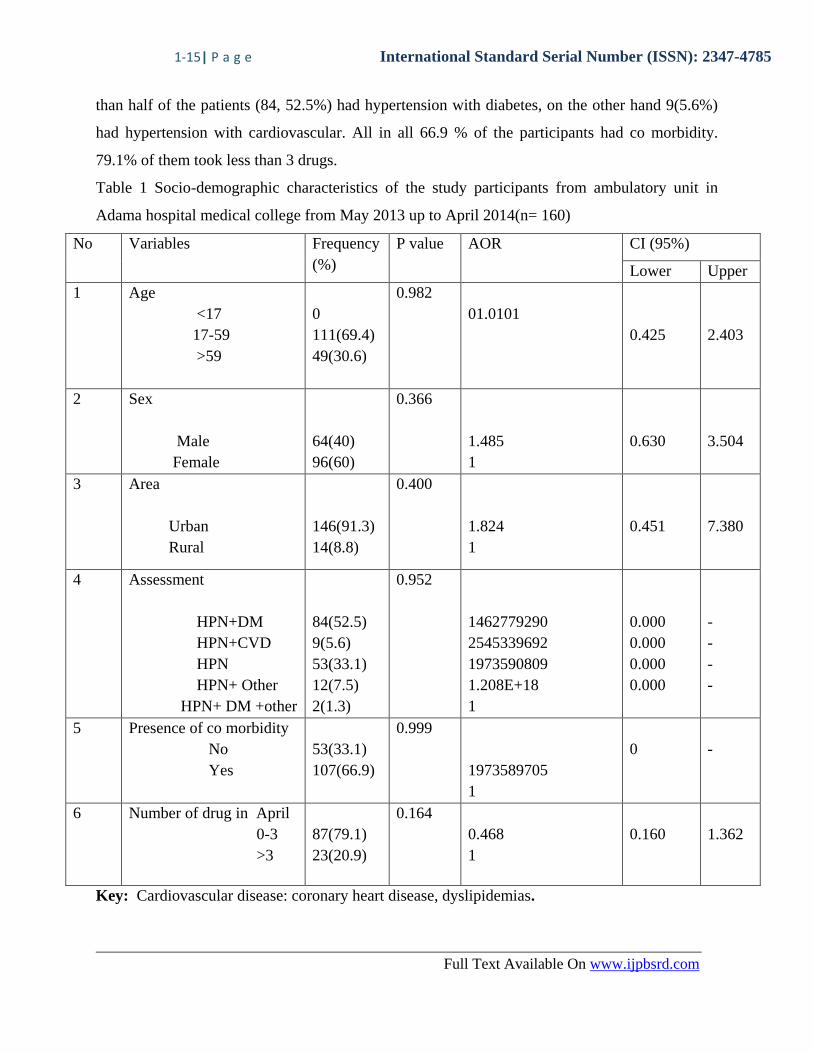
than half of the patients (84, 52.5%) had hypertension with diabetes, on the other hand 9(5.6%)
had hypertension with cardiovascular. All in all 66.9 % of the participants had co morbidity.
79.1% of them took less than 3 drugs.
Table 1 Socio-demographic characteristics of the study participants from ambulatory unit in
Adama hospital medical college from May 2013 up to April 2014(n= 160)
No Variables Frequency
(%)
P value AOR CI (95%)
Lower Upper
1 Age
<17
17-59
>59
0
111(69.4)
49(30.6)
0.982
01.0101
0.425
2.403
2 Sex
Male
Female
64(40)
96(60)
0.366
1.485
1
0.630
3.504
3 Area
Urban
Rural
146(91.3)
14(8.8)
0.400
1.824
1
0.451
7.380
4 Assessment
HPN+DM
HPN+CVD
HPN
HPN+ Other
HPN+ DM +other
84(52.5)
9(5.6)
53(33.1)
12(7.5)
2(1.3)
0.952
1462779290
2545339692
1973590809
1.208E+18
1
0.000
0.000
0.000
0.000
-
-
-
-
5 Presence of co morbidity
No
Yes
53(33.1)
107(66.9)
0.999
1973589705
1
0
-
6 Number of drug in April
0-3
>3
87(79.1)
23(20.9)
0.164
0.468
1
0.160
1.362
Key: Cardiovascular disease: coronary heart disease, dyslipidemias.
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
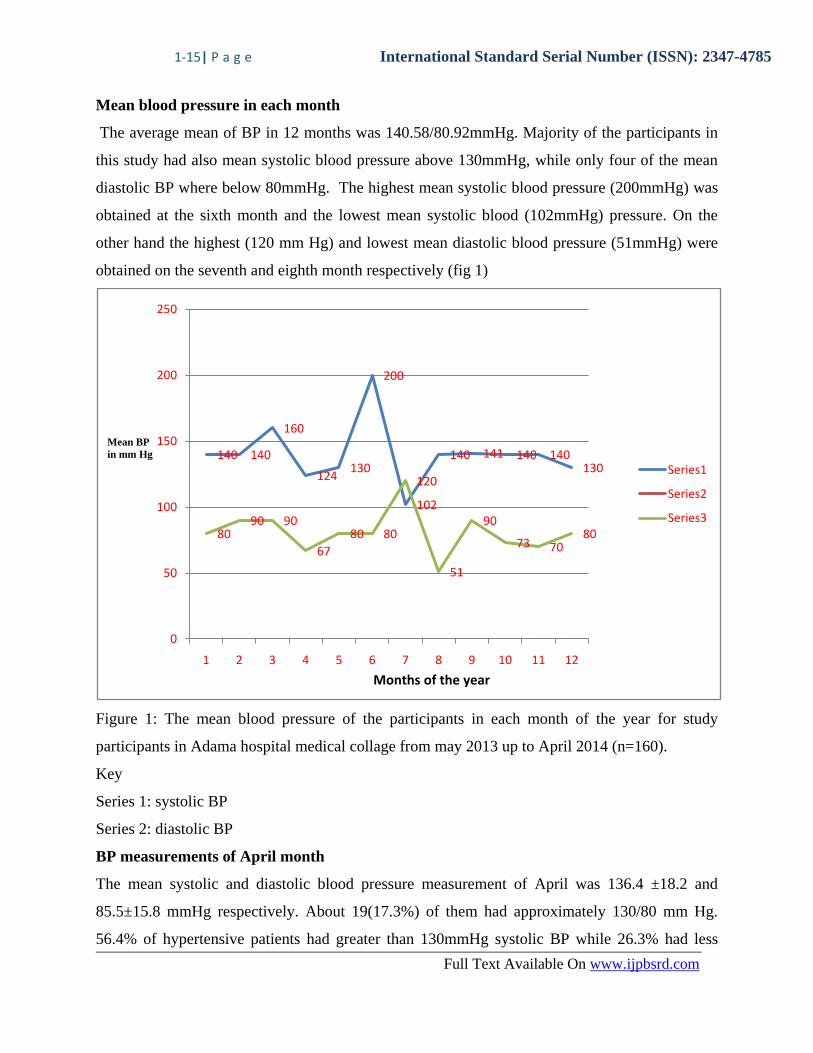
Mean blood pressure in each month
The average mean of BP in 12 months was 140.58/80.92mmHg. Majority of the participants in
this study had also mean systolic blood pressure above 130mmHg, while only four of the mean
diastolic BP where below 80mmHg. The highest mean systolic blood pressure (200mmHg) was
obtained at the sixth month and the lowest mean systolic blood (102mmHg) pressure. On the
other hand the highest (120 mm Hg) and lowest mean diastolic blood pressure (51mmHg) were
obtained on the seventh and eighth month respectively (fig 1)
Figure 1: The mean blood pressure of the participants in each month of the year for study
participants in Adama hospital medical collage from may 2013 up to April 2014 (n=160).
Key
Series 1: systolic BP
Series 2: diastolic BP
BP measurements of April month
The mean systolic and diastolic blood pressure measurement of April was 136.4 ±18.2 and
85.5±15.8 mmHg respectively. About 19(17.3%) of them had approximately 130/80 mm Hg.
56.4% of hypertensive patients had greater than 130mmHg systolic BP while 26.3% had less
140 140
160
124130
200
102
140 141 140 140130
8090 90
67
80 80
120
51
90
73 7080
0
50
100
150
200
250
1 2 3 4 5 6 7 8 9 10 11 12
Series1
Series2
Series3
Months of the year
Mean BP
in mm Hg
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
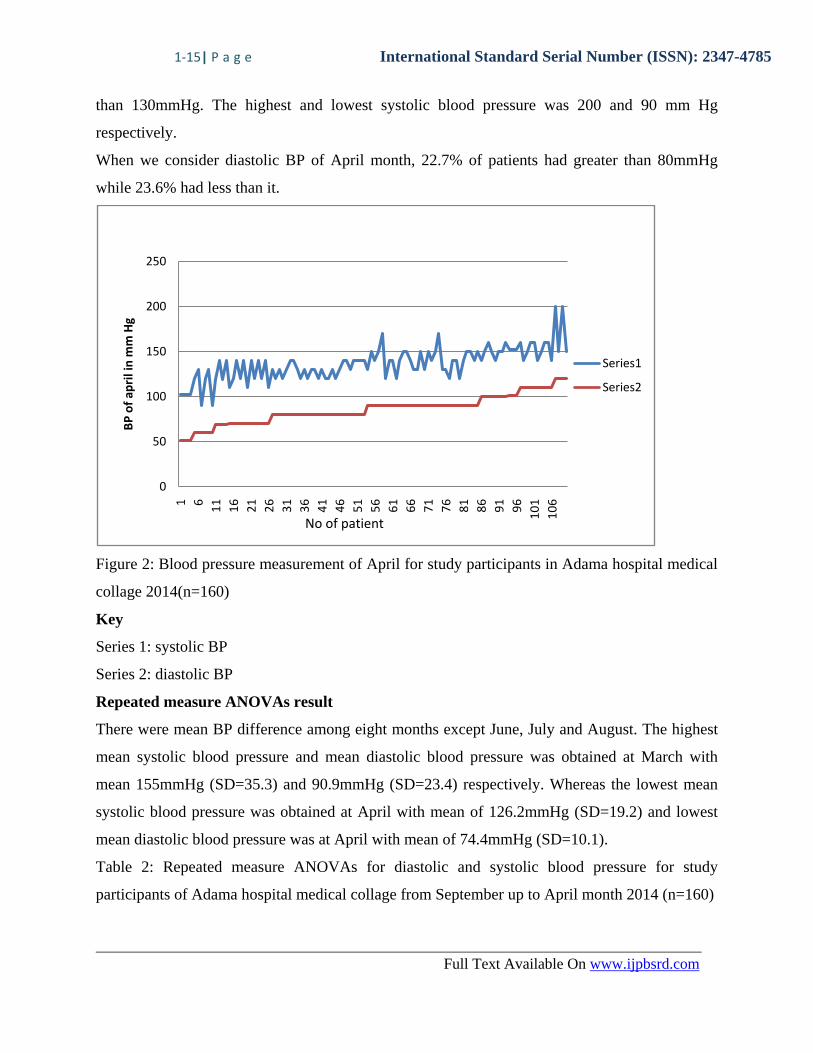
than 130mmHg. The highest and lowest systolic blood pressure was 200 and 90 mm Hg
respectively.
When we consider diastolic BP of April month, 22.7% of patients had greater than 80mmHg
while 23.6% had less than it.
Figure 2: Blood pressure measurement of April for study participants in Adama hospital medical
collage 2014(n=160)
Key
Series 1: systolic BP
Series 2: diastolic BP
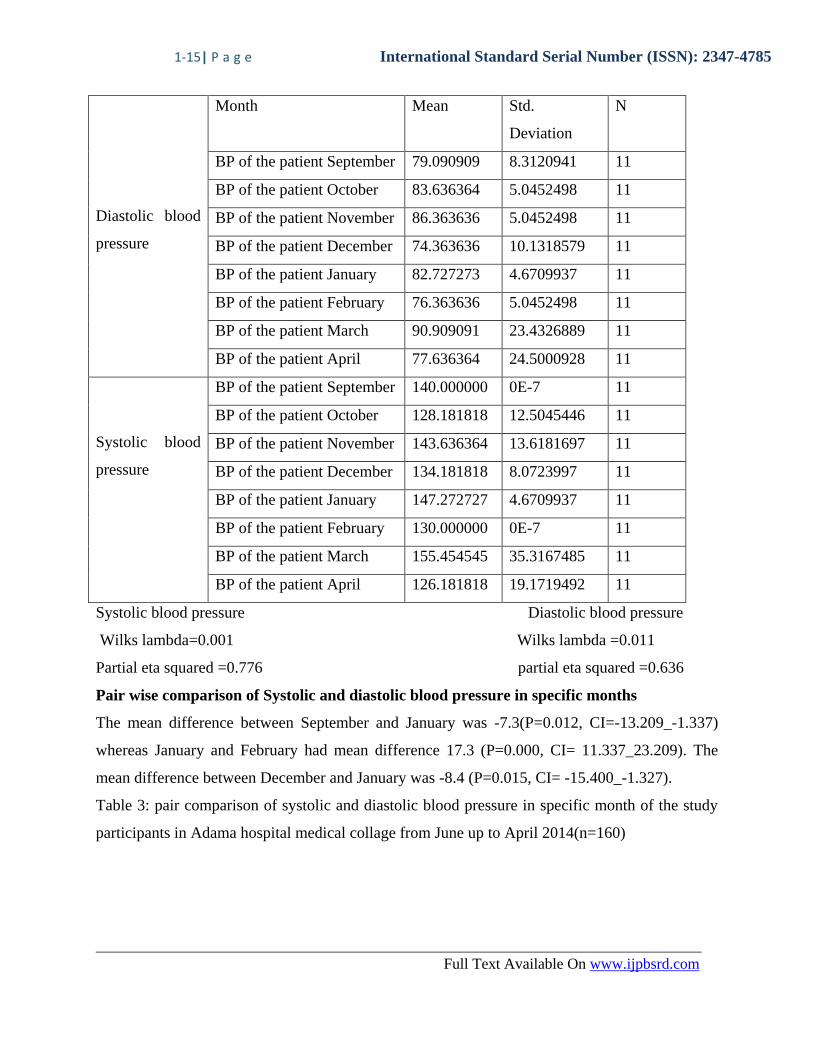
Repeated measure ANOVAs result
There were mean BP difference among eight months except June, July and August. The highest
mean systolic blood pressure and mean diastolic blood pressure was obtained at March with
mean 155mmHg (SD=35.3) and 90.9mmHg (SD=23.4) respectively. Whereas the lowest mean
systolic blood pressure was obtained at April with mean of 126.2mmHg (SD=19.2) and lowest
mean diastolic blood pressure was at April with mean of 74.4mmHg (SD=10.1).
Table 2: Repeated measure ANOVAs for diastolic and systolic blood pressure for study
participants of Adama hospital medical collage from September up to April month 2014 (n=160)
0
50
100
150
200
250
1 6
11
16
21
26
31
36
41
46
51
56
61
66
71
76
81
86
91
96
10
1
10
6
BP
of
apri
l in
mm
Hg
Series1
Series2
No of patient
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
Diastolic blood
pressure
Month Mean Std.
Deviation
N
BP of the patient September 79.090909 8.3120941 11
BP of the patient October 83.636364 5.0452498 11
BP of the patient November 86.363636 5.0452498 11
BP of the patient December 74.363636 10.1318579 11
BP of the patient January 82.727273 4.6709937 11
BP of the patient February 76.363636 5.0452498 11
BP of the patient March 90.909091 23.4326889 11
BP of the patient April 77.636364 24.5000928 11
Systolic blood
pressure
BP of the patient September 140.000000 0E-7 11
BP of the patient October 128.181818 12.5045446 11
BP of the patient November 143.636364 13.6181697 11
BP of the patient December 134.181818 8.0723997 11
BP of the patient January 147.272727 4.6709937 11
BP of the patient February 130.000000 0E-7 11
BP of the patient March 155.454545 35.3167485 11
BP of the patient April 126.181818 19.1719492 11
Systolic blood pressure Diastolic blood pressure
Wilks lambda=0.001 Wilks lambda =0.011
Partial eta squared =0.776 partial eta squared =0.636
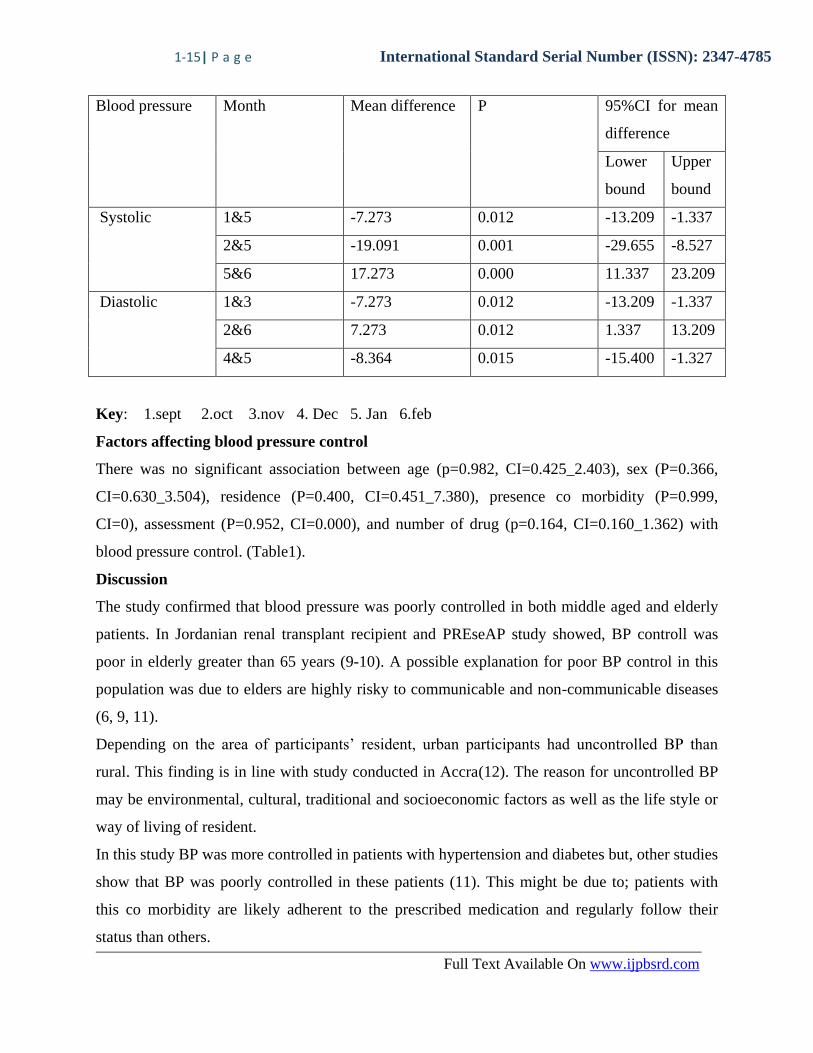
Pair wise comparison of Systolic and diastolic blood pressure in specific months
The mean difference between September and January was -7.3(P=0.012, CI=-13.209_-1.337)
whereas January and February had mean difference 17.3 (P=0.000, CI= 11.337_23.209). The
mean difference between December and January was -8.4 (P=0.015, CI= -15.400_-1.327).
Table 3: pair comparison of systolic and diastolic blood pressure in specific month of the study
participants in Adama hospital medical collage from June up to April 2014(n=160)
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
Blood pressure Month Mean difference P 95%CI for mean
difference
Lower
bound
Upper
bound
Systolic 1&5 -7.273 0.012 -13.209 -1.337
2&5 -19.091 0.001 -29.655 -8.527
5&6 17.273 0.000 11.337 23.209
Diastolic 1&3 -7.273 0.012 -13.209 -1.337
2&6 7.273 0.012 1.337 13.209
4&5 -8.364 0.015 -15.400 -1.327
Key: 1.sept 2.oct 3.nov 4. Dec 5. Jan 6.feb
Factors affecting blood pressure control
There was no significant association between age (p=0.982, CI=0.425_2.403), sex (P=0.366,
CI=0.630_3.504), residence (P=0.400, CI=0.451_7.380), presence co morbidity (P=0.999,
CI=0), assessment (P=0.952, CI=0.000), and number of drug (p=0.164, CI=0.160_1.362) with
blood pressure control. (Table1).
Discussion
The study confirmed that blood pressure was poorly controlled in both middle aged and elderly
patients. In Jordanian renal transplant recipient and PREseAP study showed, BP controll was
poor in elderly greater than 65 years (9-10). A possible explanation for poor BP control in this
population was due to elders are highly risky to communicable and non-communicable diseases
(6, 9, 11).
Depending on the area of participants’ resident, urban participants had uncontrolled BP than
rural. This finding is in line with study conducted in Accra(12). The reason for uncontrolled BP
may be environmental, cultural, traditional and socioeconomic factors as well as the life style or
way of living of resident.
In this study BP was more controlled in patients with hypertension and diabetes but, other studies
show that BP was poorly controlled in these patients (11). This might be due to; patients with
this co morbidity are likely adherent to the prescribed medication and regularly follow their
status than others.
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
The study also found that participants who had taken greater than 3 drugs (73.9%) had poor BP
control than who took less than 3 (51.7%) drugs. This may be due to non adherence to the drug
and financial problems.
From the result of pair wise comparison it is conclude that the systolic BP of January was greater
than February and diastolic BP of December is less than January by 17.3mmHg and 8.34mmHg
respectively. The reason for this difference was that the non adherence of participants to refill,
BP measurement, and different type and dose of medication in each month, life style difference,
and environmental difference.
It was found that SBP is controlled better than DBP. This might be due to higher prevalence of
isolated systolic hypertension and other reasons.
Finally, the BP of three months (June, July and august) were elevated. This is because of the
temperature during this month were cold (summer) so, this climate change can constrict blood
vessels.
The study in Bedele and Jordanian renal transplant Blood pressure found, BP was more
controlled by females than males unlike this study (6, 9, 11).
The effect of age, sex, diagnosis, number of co morbidity and drugs not shows significant
association with blood pressure control.
Conclusion
The average mean SBP and DBP obtained in 12 month were above the goal of BP needed.
Greater than half of the participants had uncontrolled BP in data collection time (April 2014).The
highest mean systolic and diastolic blood pressure were obtained at March. Whereas from pair
wise comparison the highest mean difference of systolic and diastolic was obtained between
January and February, and October and February respectively, as well as the lowest was obtained
between October and January and December and January respectively. Age, sex, area, diagnosis,
presence of co morbidity and number of drug were not associated with BP control.
Recommendation
Policy makers: to make this chronic illness as part of the public health agenda
Ministry of health: to give health education and other measures by providing an emphasis on
the prevention, early detection, and treatment of hypertension. Funding agency or the
government should had to provide their aid for the hospital to have hypertension clinic
separately to avoid crowding and the health care providers should had to provide their great
1-15| P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
efforts to help the patients as well as to increase the intensity of already started treatment and to
pay special attention to patients diagnosed with co morbidity. Furthermore, researchers and
health care providers should work to uncover the burden of hypertension overall.
Acknowledgement
We are very grateful to our college staff members for unreserved guidance and constructive
suggestions and comments from the stage of proposal development to this end. We would like to
thank Ambo University for supporting the budget which required for this research. Finally our
deepest gratitude goes to Adama Hospital Medical College staff workers who help and allow us
in conducting this research.
Abbreviation and acronyms
AA=Addis Ababa
BMI=Body mass index
P=Blood pressure
CKD=Chronic kidney disease
DBP=Diastolic blood pressure
HIV/AIDS=Human immune virus/acquired immune deficiency syndrome
HTN=Hypertension
SBP=systolic blood pressure
UK=United Kingdom
WHO=World health organization.
1-22 | P a g e International Standard Serial Number (ISSN): 2347-4785
Full Text Available On www.ijpbsrd.com
REFERENCES:
1. ELHADI IE. Identification of factors affecting blood pressure control in patients admitted
with hypertension in penang general hospitaL. 2007.
2. Center HHBPH. Causes of High Blood Pressure. 2012.
3. Paul A. James MSO, MD. et'al. 2014 Evidence-Based Guideline for the Management of High
Blood Pressure in Adults. jama2013.
4. Joho AA. Factors affecting treatment compliance among hypertension patients in three
district hospitals - DAR ES SALAAM. 2012.
5. Awoke A, Awoke T, Alemu S, Megabiaw B. Prevalence and associated factors of
hypertension among adults in Gondar, Northwest Ethiopia: a community based cross-
sectional study. BMC Cardiovasc Disord. 2012;12:113.
6. Feyie Bonsa1 EKG, Kifle Woldemichael Hajito. prevalence of hypertension and associated
factors in bedele town, southwest Ethiopia. 2014.
7. E, Gudina1 sK, Michael1 Y, S, Assegid2 a. Prevalence of hypertension and its risk factors in
southwest Ethiopia: a hospital-based cross-sectional survey. 2013.
8. Habtamu Abera Hareri1 MA. Assessments of Adherence to Hypertension Medications and
Associated Factors among Patients Attending Tikur Anbessa Specialized Hospital Renal
Unit. 2012.
9. NBA-MY, HQGAKWA, Al-Ulemat AWM. Management of hypertension and factors
affecting its control in Jordanian renal transplant recipients. 2012.
10. Domingo Orozco-Beltrán aCB, b Irene Moral,b Núria Soriano,b María A. del Valle,c, Ana I.
Rodríguez dJMP, e and Ana Pastor,f on behalf of the PREseAP study research group. Factors
Affecting the Control of Blood Pressure and Lipid Levels in Patients With Cardiovascular
Disease:The PREseAP Study. 2008.
11. M Thoenes HRN, M Volper, BV khan,W kirch. Antihypertensive drug thearapy and
pressure control in men and women :an inernational perispective. Human hypertension 2009.
12. Ghana phfi. Prevalence, awareness, treatment and control of hypertension in urban poor
communities in Accra. 2012.
Related Documents











