LABORATORY BLOOD (1st Edion, Revised 2014 Unit Tabung Jabatan Hospital EXT :

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
LABORATORY
BLOOD
(1st Edition, Revised 2014
Unit Tabung
Jabatan
Hospital
EXT :

2
3
INTRODUCTION
The purpose of having a laboratory manual for transfusion service is to improve
the overall quality of the blood transfusion service in this hospital.
In this laboratory manual, topics such as consent for transfusion, procedures for re-
questing blood transfusion, sample taking and labeling, proper storage and transportation
of blood products, Clinical guidelines in blood transfusion and blood transfusion reaction
will be discussed.
This laboratory manual is for use within Hospital Batu Pahat only. This manual is
mainly based on guidelines from National Blood Center (PDN) and The Clinical Use of
Blood Products by WHO. It is intended to promote better and safer transfusion practice in
this hospital.
4
TABLE OF CONTENTS
CONTENTS
PAGE NO
INTRODUCTION
3
TABLE OF CONTENTS
4 – 5
CONSENT FOR TRANSFUSION
6
MSBOS
6
GSH
6
BLOOD TAKING AND LABELING
6
FILLING REQUEST FORM
7
BLOOD REQUEST IN NEWBORN / CHILDREN
7
COLLECTING BLOOD / BLOOD COMPONENTS
7
ADMINISTRATION OF BLOOD / BLOOD COMPONENTS
8
PRETRANSFUSION MEDICATION
8
PATIENT MONITORING DURING TRANSFUSION
8
NIGHT TIME TRANSFUSION
8
USAGE OF BLOOD WARMER
9
DRUGS / FLUID ADMINISTRATION DURING TRANSFUSION
9
BLOOD TRANSFUSION REACTION
9 – 10
TRANSFUISON OF BLOOD PRODUCTS FROM CLOSED FAMILY MEMBERS / RELATIVE
11
5
GUIDELINES IN CLINICAL USE OF BLOOD / BLOOD PRODUCTS
RED BLOOD CELL TRANSFUSION ---------------------------------------------------------------------------- TRANSFUSION IN ANEMIA ---------------------------------------------------------------------------------------- TRANSFUSION TRIGGERS ------------------------------------------------------------------------------------------ GUIDELINES IN NEONATAL EXCHANGE TRANSFUSION ----------------------------------------------- SELECTION OF NON RED CELL PRODUCTS --------------------------------------------------------------- GUIDELINE IN PLATELETS TRANSFUSION ----------------------------------------------------------------- GUIDELINE IN FFP TRANSFUSION -------------------------------------------------------------------------- GUIDELINES IN CRYOPRECIPITATE TRANSFUSION ------------------------------------------------------ GUIDELINE IN MANAGEMENT OF DISSEMINATED INTRAVASCULAR COAGULATION ----------
12 – 13
14
14
15 - 16
16
17 - 18
19
20
21
CT RATIO
WHAT IS CT RATIO ? --------------------------------------------------------------------------------------------------
CT RATIO OF HOSPITAL BATU PAHAT -----------------------------------------------------------------------
22 - 23
24
APPENDIX
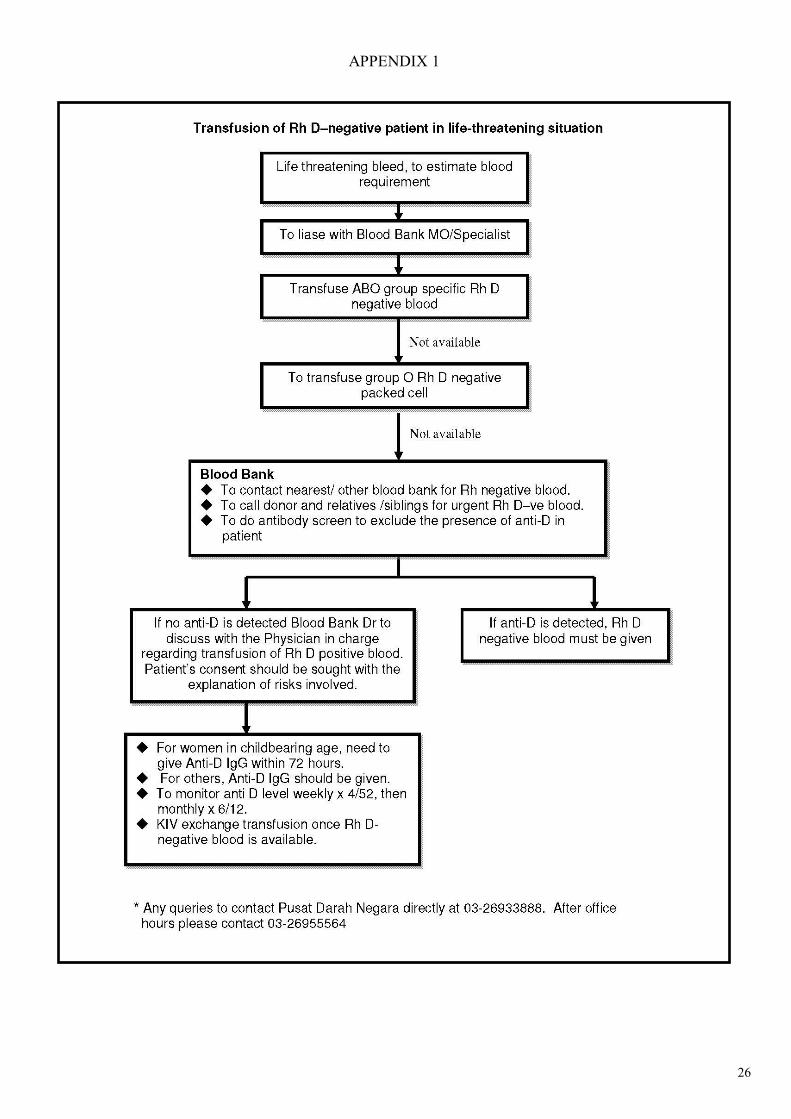
1. TRANSFUSION OF RH D NEGATIVE PATIENT IN LIFE THREATENING SITUATION ----------------
2. MSBOS OF HOSPITAL BATU PAHAT ----------------------------------------------------------------------------
3. CONSENT FORM -------------------------------------------------------------------------------------------------------
4. CHECK LIST FOR TAKING BLOOD FOR GXM ---------------------------------------------------------------
5. BLOOD REQUEST FORM ---------------------------------------------------------------------------------------------
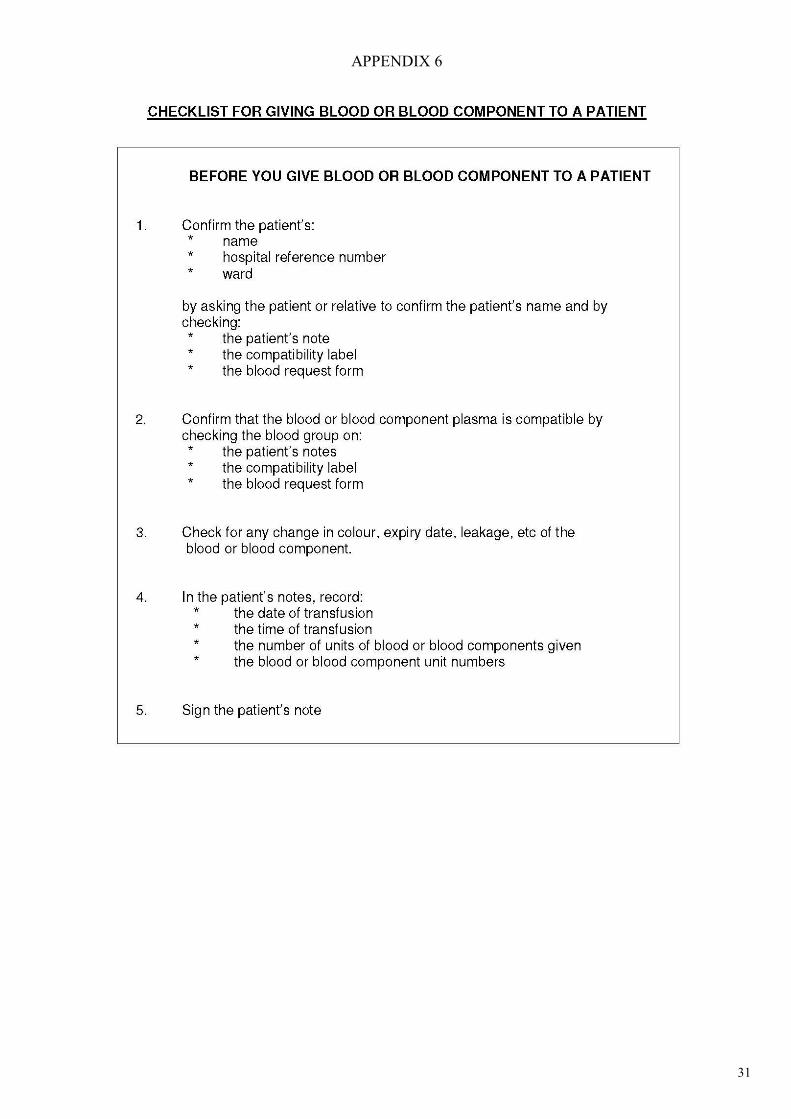
6. CHECK LIST FOR GIVING BLOOD OR BLOOD COMPONENT TO A PATIENT ------------------------
7. SUMMARY OF BLOOD REQUEST TILL BLOOD ISSUING ---------------------------------------------------
8. COLLECTION OF BLOOD / BLOOD PRODUCTS ---------------------------------------------------------------
9. STORAGE OF BLOOD PRODUCT PRIOR TO TRANSFUSION -----------------------------------------------
10. TIME LIMITS FOR TRANSFUSION ----------------------------------------------------------------------------------
11. HOW TO USE BLOOD STICKER -------------------------------------------------------------------------------------
12. BLOOD TRANSFUSION REACTION REPORT FORM ----------------------------------------------------------
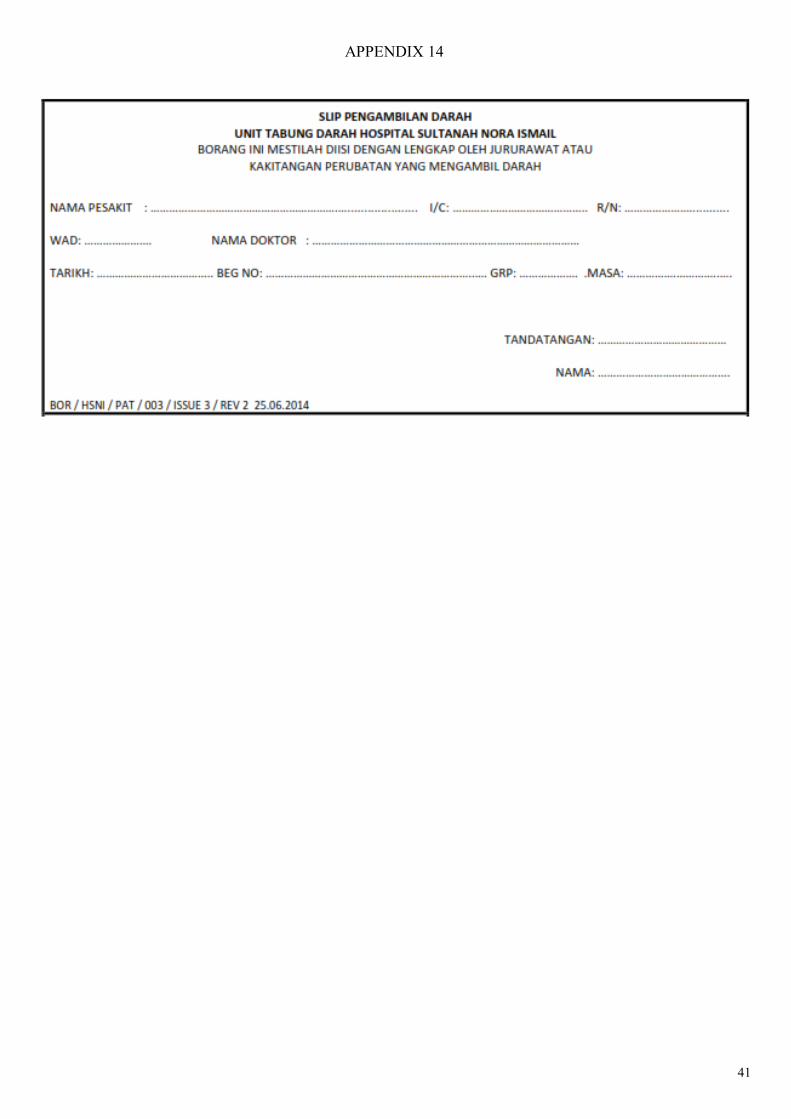
13. S L I P P E N G A M BI L A N D A RA H -----------------------------------------------------------------------------
14. BORANG PEMULANGAN DARAH / KOMPONEN DARAH ----------------------------------------------------
26
27
28
29
30
31
32 - 34
35
36
37
38
39 – 40
41
42
REFERENCES
43
6
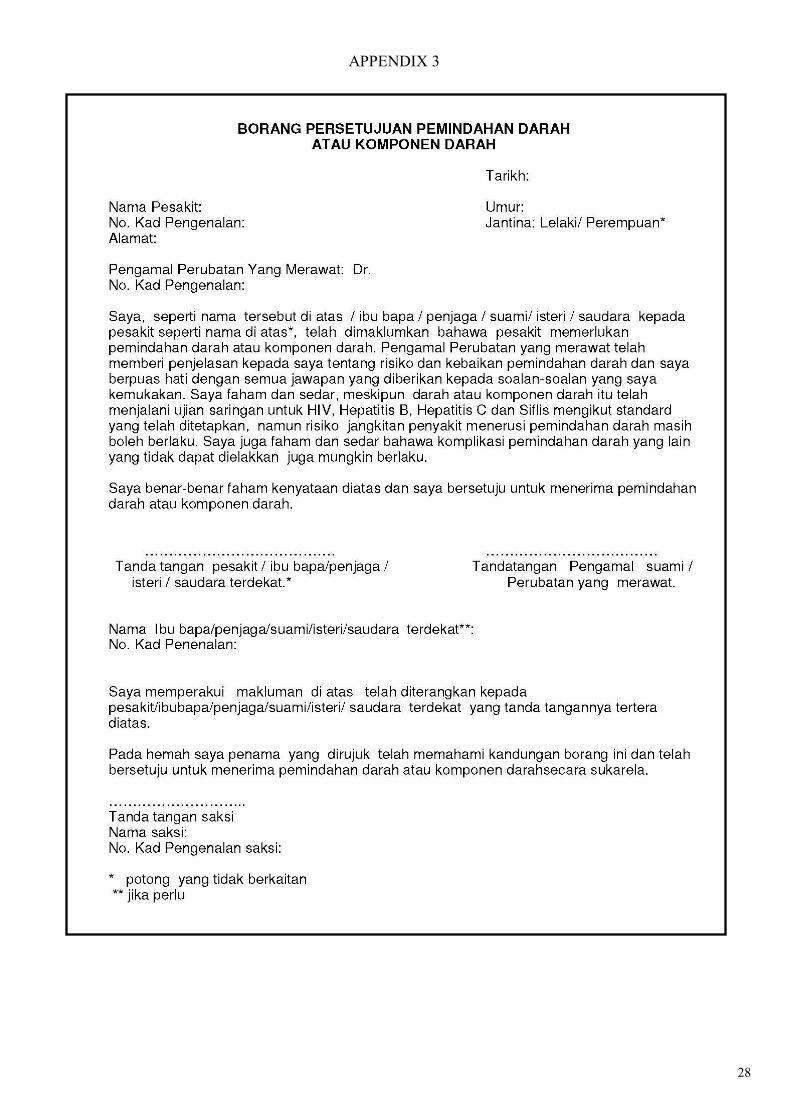
CONSENT FOR TRANSFUSION—Refer to APPENDIX 3 (Page 28)
The patient must give informed consent for transfusion. The clinician in charge of the patient has a responsi-
bility to explain the benefits, risk and alternative to transfusion therapy and ensure that the patient comprehends the
issues discussed. Other than in emergency, the patient should be given opportunity to ask questions, and his/her
informed decision be documented. If the patient is unable to give consent, a responsible family member must
be asked to do so. If no family member is available or in emergency when the need for transfusion leaves no time
for consent, it is prudent to note this in the patient’s medical note. The informed consent for blood transfusion is valid from the time the patient is admission till the time of dis-
charge. If the patient requires multiple transfusions during the same admission, no additions inform consent is required.
MSBOS(Maximum Surgical Blood Order Schedule)—Refer to APPENDIX 2 (Page 27)
MSBOS is a table of elective surgical procedures which list the number of units of blood routinely requested
and cross matched for them preoperatively.
The schedule is base on retrospective analysis of actual blood usage associated with the individual surgi-cal procedure.
Please see attachment of MSBOS of Hospital Batu Pahat.
GSH (Group, Screen & Hold)
GSH is for cases that are unlikely to be transfused during surgery, however when antibody screen is positive, compatible blood must be made available.
After GSH the sample will keep for 72hours, if blood is requires within 72hours, will proceed for further cross matching.
A GSH should be used in conjunction with a Maximum Surgical Blood Order Schedule (MSBOS).
BLOOD TAKING AND LABELING—Refer to APPENDIX 4 (Page29)
The process of taking and labeling blood samples must be done in one process at the bedside, one patient only at any time. The doctor performing this must ensure:
1. The patient is correctly identified. The doctor taking the blood sample must read the wristband, if available,
and whenever possible, ask the patient to state his/her full name. This information must be checked against the
case notes.
2. Unconscious patient MUST be identified by the information given on the identity band, such as the
wristband.
3. An emergency casualty who cannot be reliable identified must be given and identity band with a unique num-ber. This number must be used to identify this patient until full and correct personal details are available
4. The person who takes the blood and the person who labeled the blood sample must be same person.
5. The sample must be labeled clearly and accurately at patient’s bedside immediately after blood taking. Use only hand written label and never use preprinted label for labeling sample. The label should include the patient’s full name, hospital registration number or Identity card number.
6. Never label samples from 2 or more patients at the same time.
7
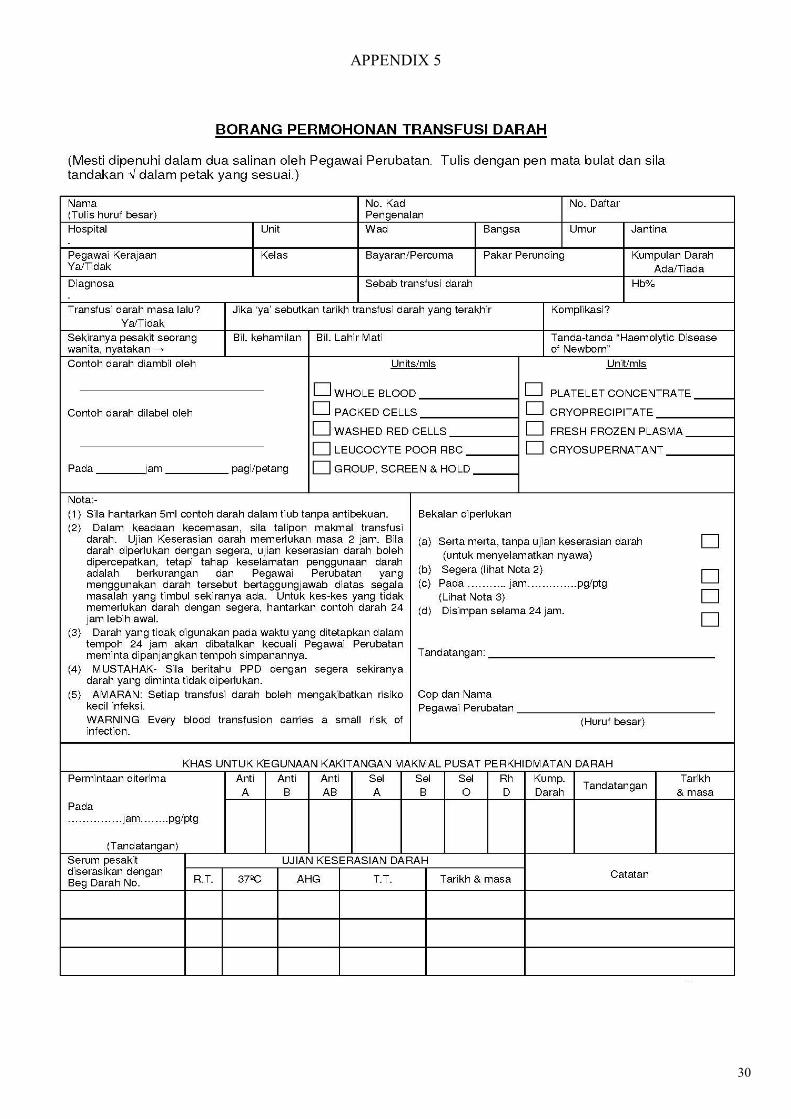
FILLING BLOOD REQUST FORM—Refer to APPENDIX (Page 30)
Prescribing blood and blood products is the responsibility of the doctor managing the patient. However, the doctor is encouraged to consult the doctor in-charge of the Blood Bank on the products to be given, the quantity, the duration of infusion, the precautions to be taken and any other related matters
1. The request form should be completely filled and contain relevant patient information(Full name, IC,
Sex, Reason for transfusion, blood group if known, previous transfusion reaction and etc). No preprinted
label is allowed. Please make sure your hand writing is clearly written and not confusing.
2. The hospital registration number (R/N) should be used on the request form for patients who, at the time
of admission, cannot be reliably identified. This R/N must be ‘unique’ and any investigations for this
patient must be identified using this number. When the patient’s full and correct details are available the
ward personnel should accurately communicate this information to the Blood Bank.
3. The quantity and the approximate time when the blood and blood component would be required must be
stated. Requests for blood to be made available “as soon as possible / STAT” should be avoided as this
would not assist the blood bank personnel in determining priorities.
4. he request form should be signed by the requesting doctor and his/her name should be stamped or written
clearly in block letters.
BLOOD REQUEST IN NEWBORN / CHILDREN
1. For infant less than 4 month of age, blood sample must be accompanied by mother’s blood sample.
2. For baby /child using parent’s IC, please filled up the detail of the infant as shown below:
Nama : B/O Kamariah Bt Othman / Name of the child (Father/Mother’s name)
Kad Pengenalan : 840223-01-5029M2
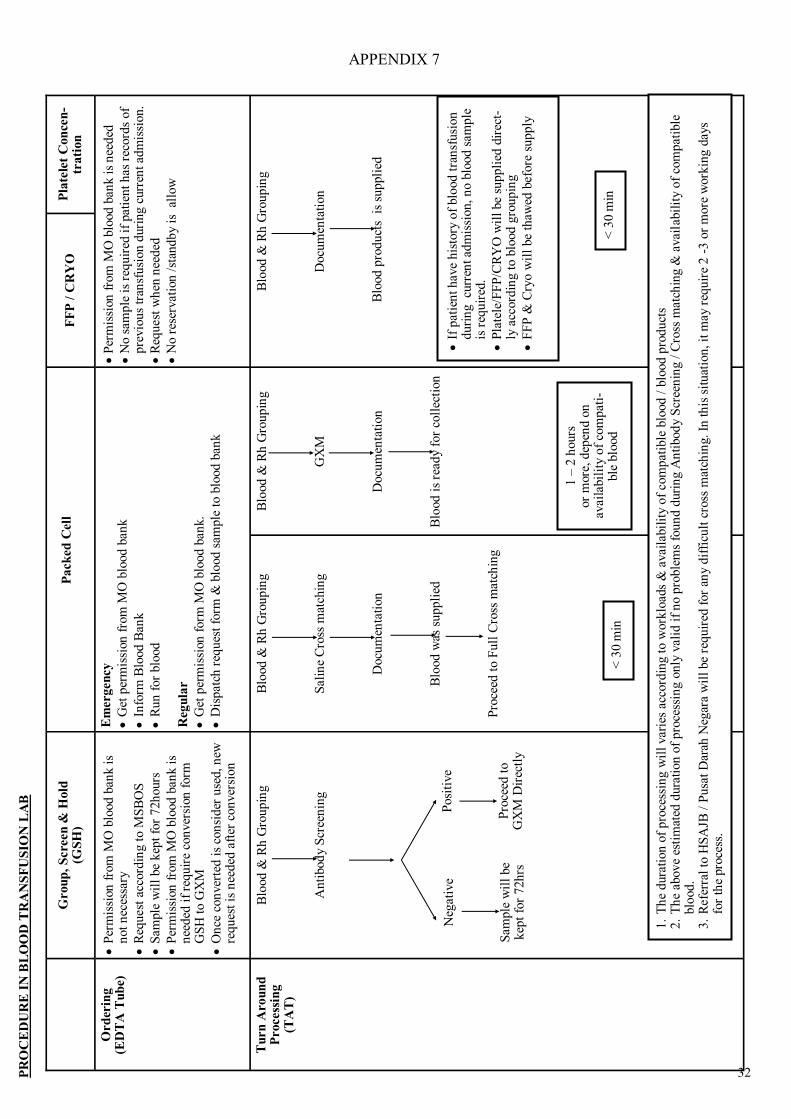
COLLECTING BLOOD / BLOOD COMPONENTS—Refer to APPENDIX 7, 8 & 9 (Page 32 – 36)
The person collecting the blood must bring documentary proof of the patient’s identity. At the time of collection, both blood bank personnel and the person collecting the blood must check that these details match those of the blood unit to be collected. Date and time of issues & collection, name of blood bank personnel & per-son collecting must be recorded.
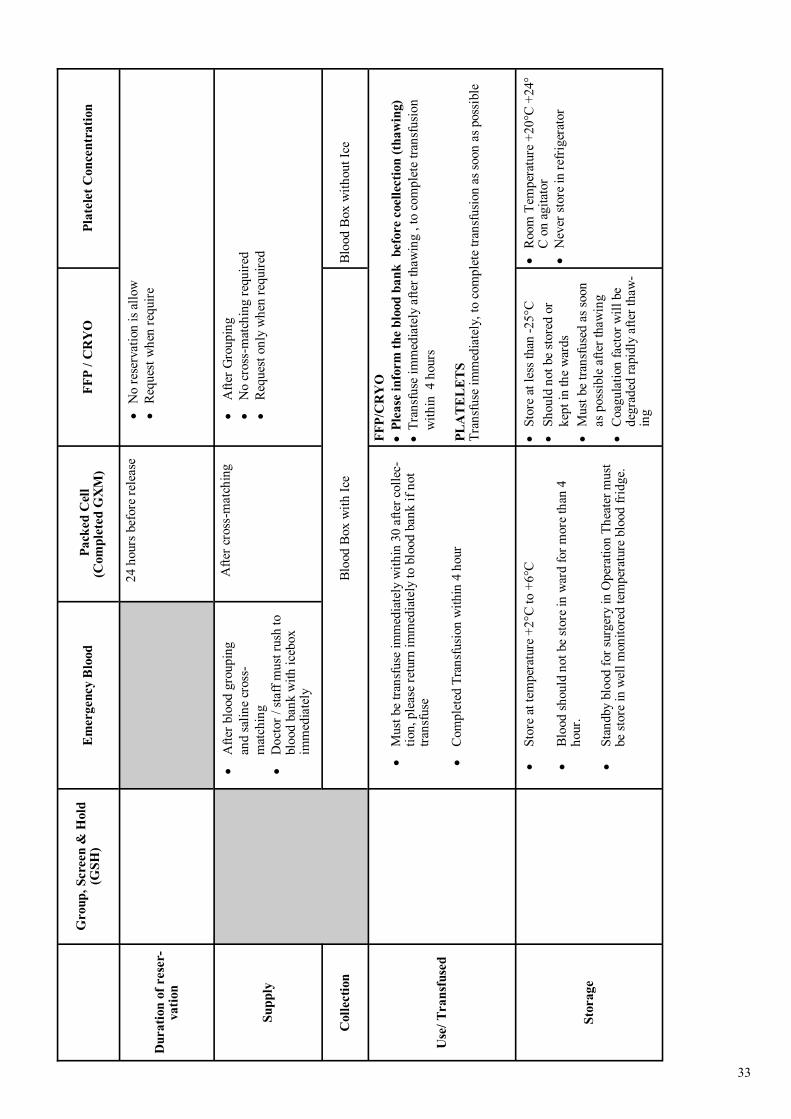
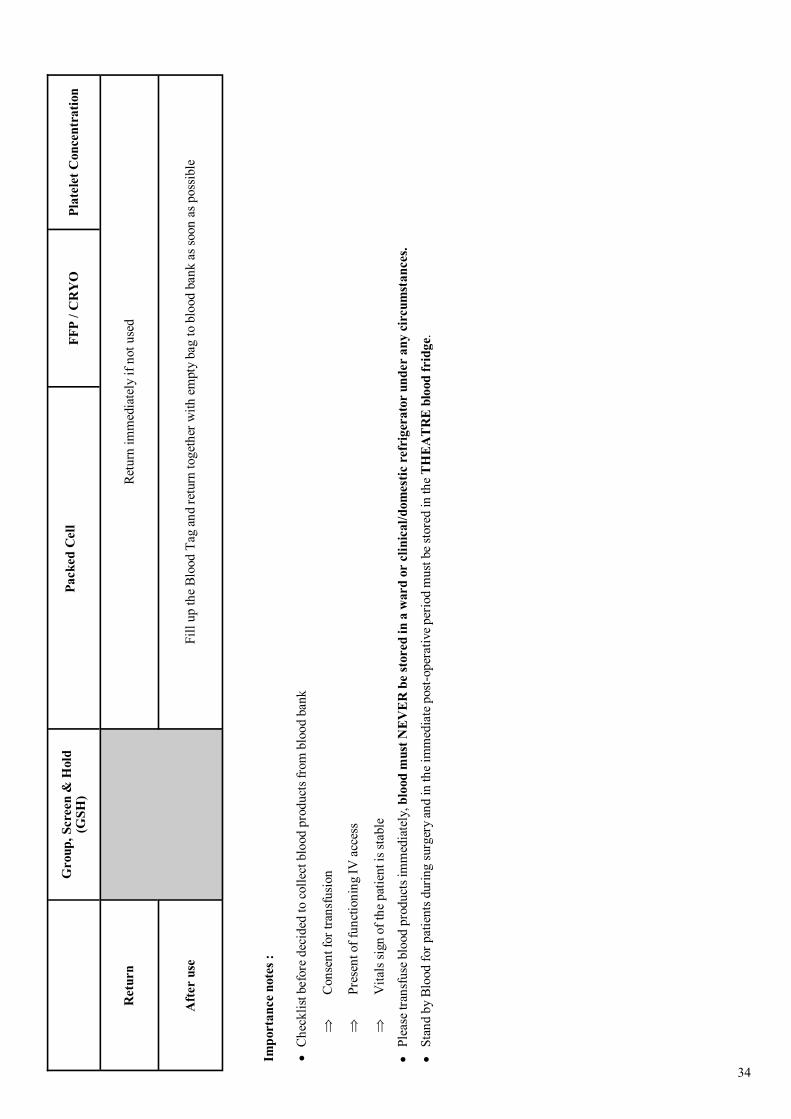
STORAGE AND TRANSPORT OF BLOOD / BLOOD COMPONENTS —Refer to APPENDIX 8 & 9 (Page 35-37)
M1 — 1st child M2 — 2nd child M3 — 3rd child Note:
Please write down the child’ date of birth /
8
Notes: First 50ml of each unit should be transfused slowly as it serves as an in vivo compatibility testing.
Major blood transfusion reaction will develop within seconds after the transfusion started.
ADMINISTRATION OF BLOOD / BLOOD COMPONENTS
—Refer to APPENDIX 6, 7, 10 (Page 32 – 37)
Each unit of blood component supplied from the Blood Bank should be accompanied by a compatibility label. This should carry the following information.
1. At the time of transfusion the information on the compatibility label accompanying the blood component must be checked carefully against the patient’s identification details on the blood request from and patient’s case notes, including the patient’s wristband.
2. Blood should not be transfused if any of the details; especially the name and identification card number of
the patient does not match exactly with that given on the accompanying compatibility label or the blood
request form.
3. Blood should not be transfused if there is deviation from the usual condition. Blood should be checked
macroscopically for any alteration in color of the blood, presence of clot, leakage, etc. The blood bank
should be informed immediately for appropriate measures to be taken and the blood must be returned to the
blood bank. PRETRANSFUSION MEDICATIONS
Prophylactic medication to prevent transfusion reaction is still controversial.
Premedication such as antipyretic, antihistamine or corticosteroid can be administer (oral/IV route) 30-60minutes before transfusion for individual with history allergic or urticarial reactions to transfu-sions in the past.
PATIENT MONITORING DURING TRANSFUSION The patient’s vital signs, including temperature, pulse rate and blood pressure should be recorded during:
Before starting the transfusion (As a baseline)
As soon as the transfusion is started
15 minutes after starting transfusion
At least every hour of transfusion
On completion of transfusion
4 hour after completion of transfusion
TIME LIMITS FOR INFUSION OF BLOOD COMPONENTS—Refer to APPENDIX 10 (Page 37)
NIGHT TIME TRANSFUSION
Where the clinical condition permits, then transfusion at night must be avoided whenever possible, except for emergency cases as:
There is difficulty in visually detecting reactions.
Lower staffing levels make it difficult to carry out the observations in a timely fashion.
Risk of Blood Transfusion Reaction might be happen unnoticed If Transfusion must occur at night,
The light above the patient must remain on while the patient is being transfused.
It should be ensured that sufficient number of staff is available to monitor the patient.
Major Transfusion Reaction is life threatening, qualified Medical personal must be available imme-diately in this situation.
9
USAGE OF BLOOD WARMER
There is no evidence that warming blood is beneficial to patient when infusion is slow (1unit over 2 hour). Blood warmers are used to minimize the incidence of cardiac arrest and arrhythmias associated with mas-sive transfusion of cold blood components. Use of blood warmers should be limited to patients receiving multiple, rapid transfusion at rates of >50ml/kg/hr in adults and 15ml/kg/hr in children, and infants undergoing ex-change transfusion. Blood warmer to be used must have a visible thermometer and audible warning service. How-ever keeping the patient warm is probably more important than warming the infused blood.
DRUGS / FLUIDS ADMINSTRATION DURING TRANSFUSION
Red cell concentrates may be diluted with sodium chloride 0.9% to improve the flow rate. This is most simply achieved by using a Y pattern blood administration set. No solutions should be added to any blood compo-nent. This may contain additives such as calcium which can cause citrated blood to clot. Dextrose solution can ly-ses red cells.
Medicines should never be added directly to any blood components, if there is an adverse reaction during
transfusion, it may be impossible to determine whether this is due to the blood, to the added drug or to an interaction of the two.
If an intravenous fluid other than normal saline, or a colloid, has to be given at the same time as blood com-
ponents, it should preferably be given through a separate IV line to avoid any risk of these problems. In a
situation when the transfusion line is the only venous access available and a medication has to be given, the trans-
fusion must be stopped and the tubing should be flush with 0.9% normal saline before and after injecting the medi-
cation to prevent direct mixing of the blood and medication. The transfusion can then be resumed.
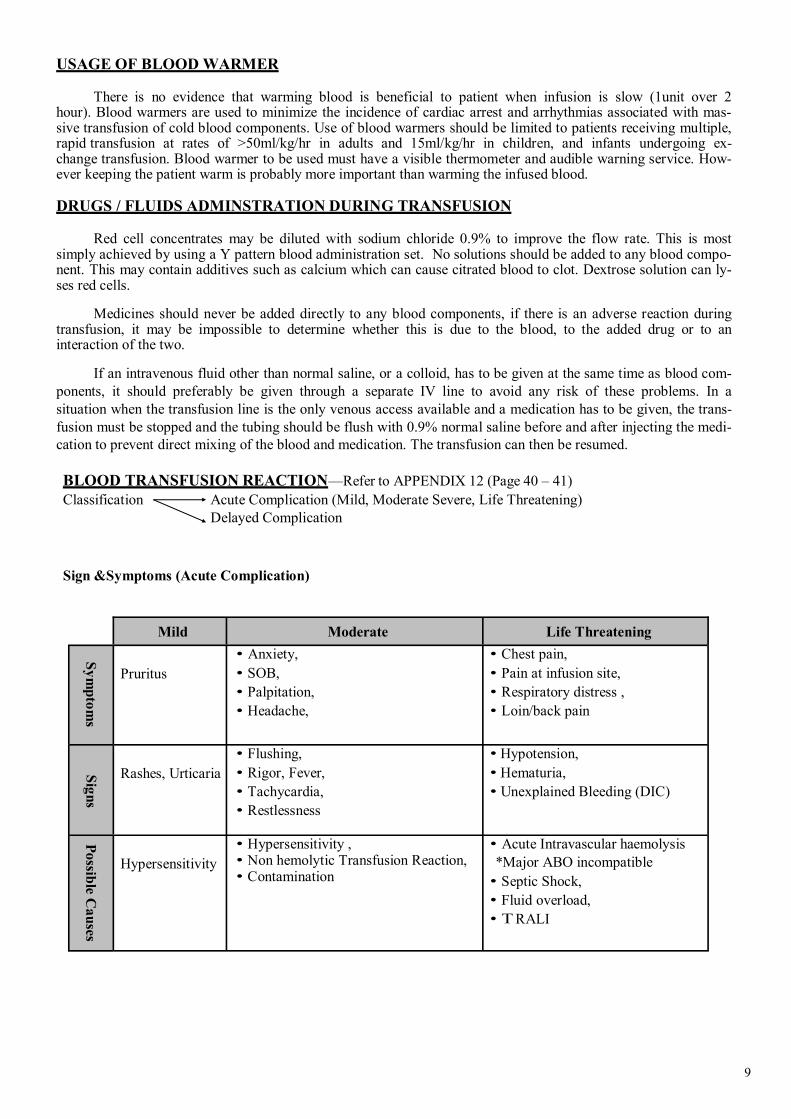
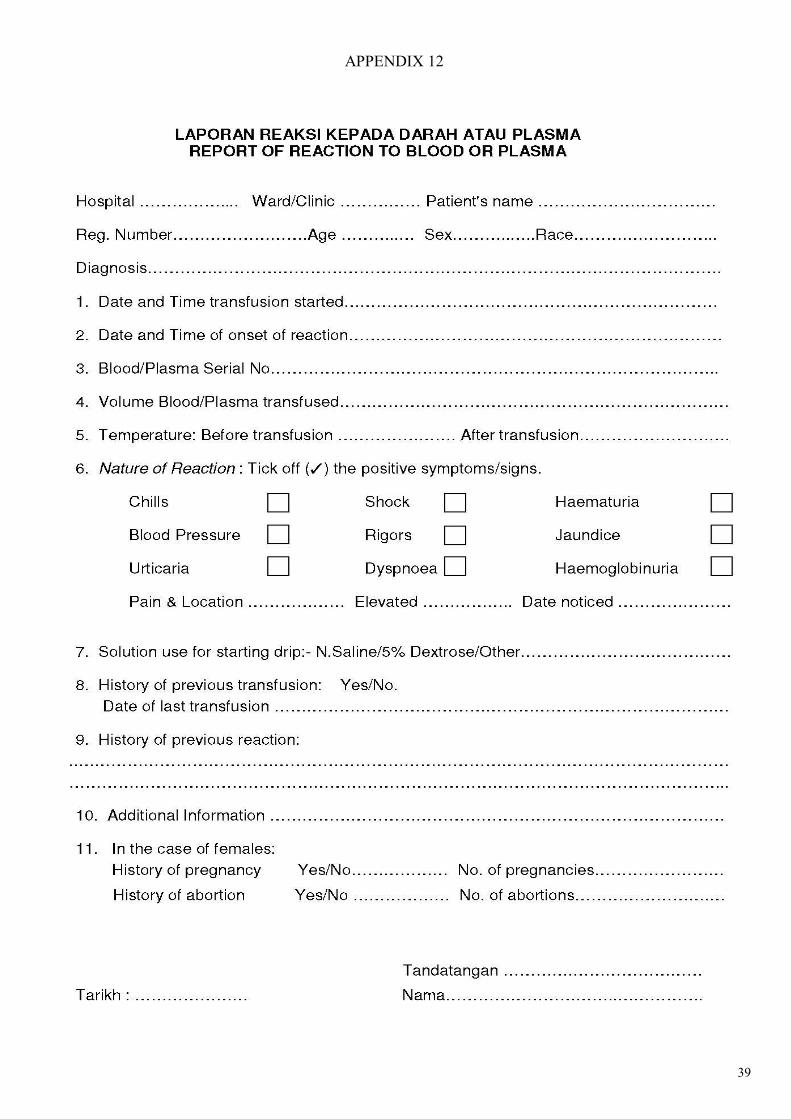
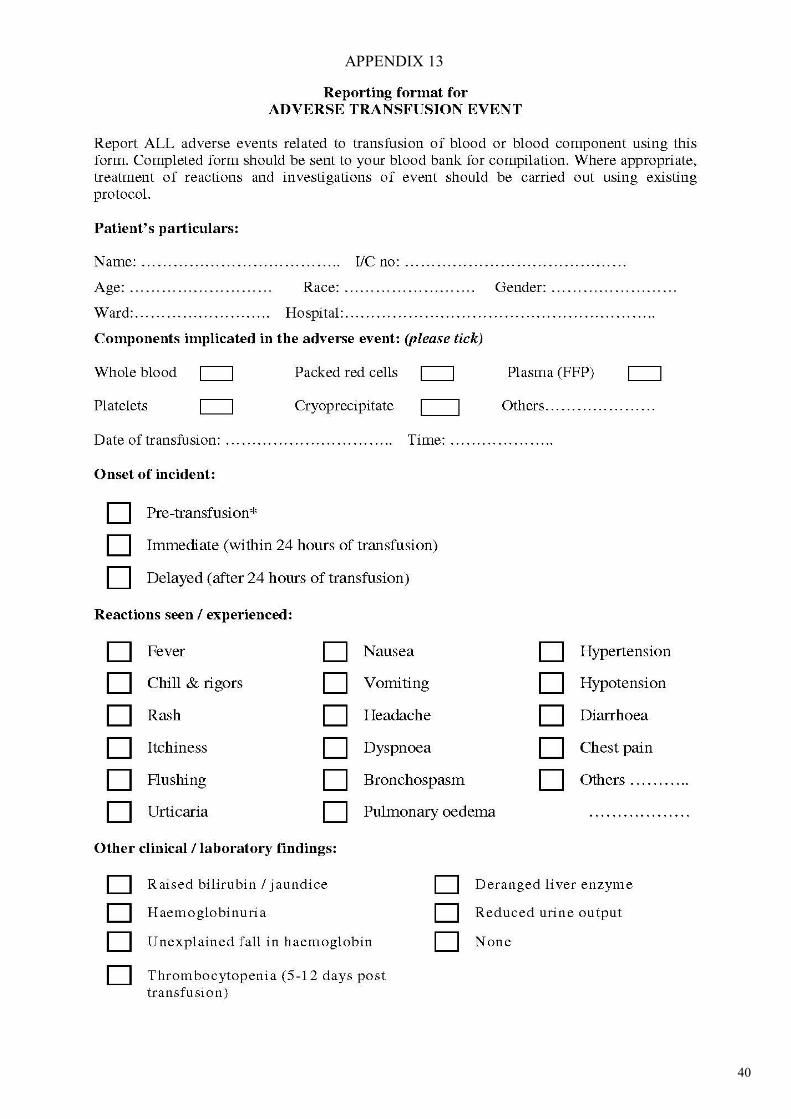
BLOOD TRANSFUSION REACTION—Refer to APPENDIX 12 (Page 40 – 41)
Classification Acute Complication (Mild, Moderate Severe, Life Threatening)
Delayed Complication
Sign &Symptoms (Acute Complication)
Mild Moderate Life Threatening
Sy
mp
tom
s
Pruritus
Anxiety,
SOB,
Palpitation,
Headache,
Chest pain,
Pain at infusion site,
Respiratory distress ,
Loin/back pain S
ign
s
Rashes, Urticaria
Flushing,
Rigor, Fever,
Tachycardia,
Restlessness
Hypotension,
Hematuria,
Unexplained Bleeding (DIC)
Po
ssible C
au
ses
Hypersensitivity
Hypersensitivity , Non hemolytic Transfusion Reaction, Contamination
Acute Intravascular haemolysis
*Major ABO incompatible
Septic Shock,
Fluid overload,
RALI
10
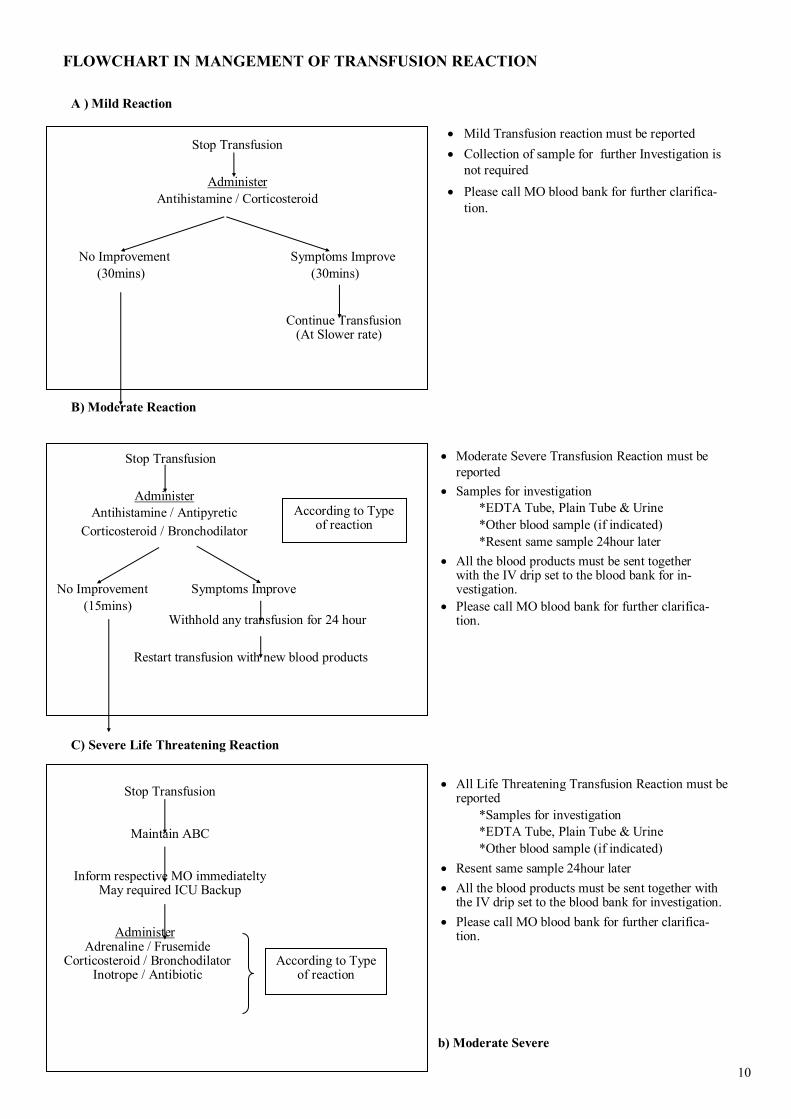
FLOWCHART IN MANGEMENT OF TRANSFUSION REACTION
A ) Mild Reaction
B) Moderate Reaction
C) Severe Life Threatening Reaction
b) Moderate Severe
Stop Transfusion
Administer
Antihistamine / Corticosteroid
No Improvement Symptoms Improve
(30mins) (30mins)
Continue Transfusion
(At Slower rate)
Stop Transfusion
Maintain ABC
Inform respective MO immediatelty May required ICU Backup
Administer Adrenaline / Frusemide
Corticosteroid / Bronchodilator Inotrope / Antibiotic
According to Type of reaction
Mild Transfusion reaction must be reported
Collection of sample for further Investigation is
not required
Please call MO blood bank for further clarifica-
tion.
Moderate Severe Transfusion Reaction must be
reported
Samples for investigation
*EDTA Tube, Plain Tube & Urine
*Other blood sample (if indicated)
*Resent same sample 24hour later
All the blood products must be sent together with the IV drip set to the blood bank for in-vestigation.
Please call MO blood bank for further clarifica-tion.
All Life Threatening Transfusion Reaction must be reported
*Samples for investigation
*EDTA Tube, Plain Tube & Urine
*Other blood sample (if indicated)
Resent same sample 24hour later
All the blood products must be sent together with the IV drip set to the blood bank for investigation.
Please call MO blood bank for further clarifica-tion.
Stop Transfusion
Administer
Antihistamine / Antipyretic
Corticosteroid / Bronchodilator
No Improvement Symptoms Improve
(15mins) Withhold any transfusion for 24 hour
Restart transfusion with new blood products
According to Type of reaction
11
TRANSFUSION OF BLOOD PRODUCT FROM CLOSED FAMILY MEMBERS / RELATIVE
Blood transfusion within closed family / relative is not advisable.
There is risk of develop of delayed type of blood transfusion complication(Graft versus host disease)
Graft versus host disease occurs in situations.
Blood donor is homozygous and the recipient is heterozygous for an HLAhalotype (usually relative blood)
Immunodeficient patients
This type of delayed type of transfusion complication is cause by donor T Lymphocytes prolifera-
tion and attacking recipient’s tissues.
Prevention of Graft versus host disease in blood transfusion :
Avoid Transfusion of blood products from closed family members / relatives.
Gamma irradiation of blood products before transfusion (Facility not available in Hospital Batu
12
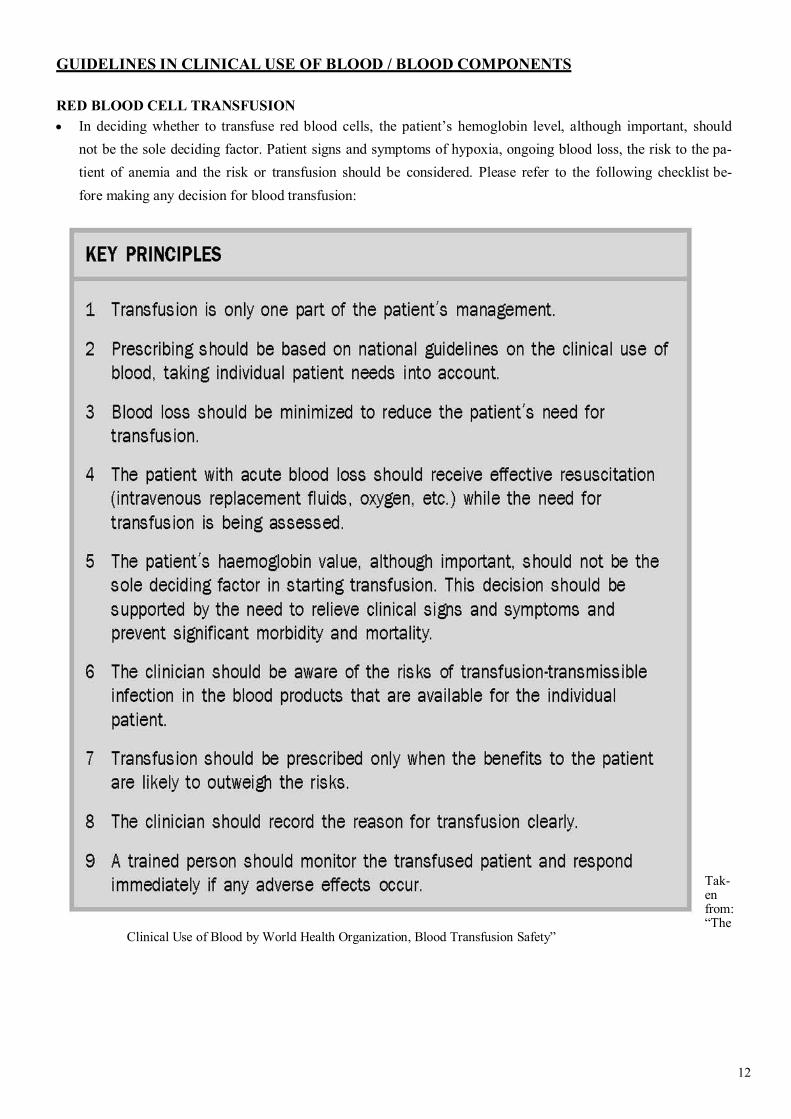
GUIDELINES IN CLINICAL USE OF BLOOD / BLOOD COMPONENTS
RED BLOOD CELL TRANSFUSION
In deciding whether to transfuse red blood cells, the patient’s hemoglobin level, although important, should
not be the sole deciding factor. Patient signs and symptoms of hypoxia, ongoing blood loss, the risk to the pa-
tient of anemia and the risk or transfusion should be considered. Please refer to the following checklist be-
fore making any decision for blood transfusion:
Tak-en from: “The
Clinical Use of Blood by World Health Organization, Blood Transfusion Safety”
13
Taken from: “The Clinical Use of Blood by World Health Organization, Blood Transfusion Safety”
14
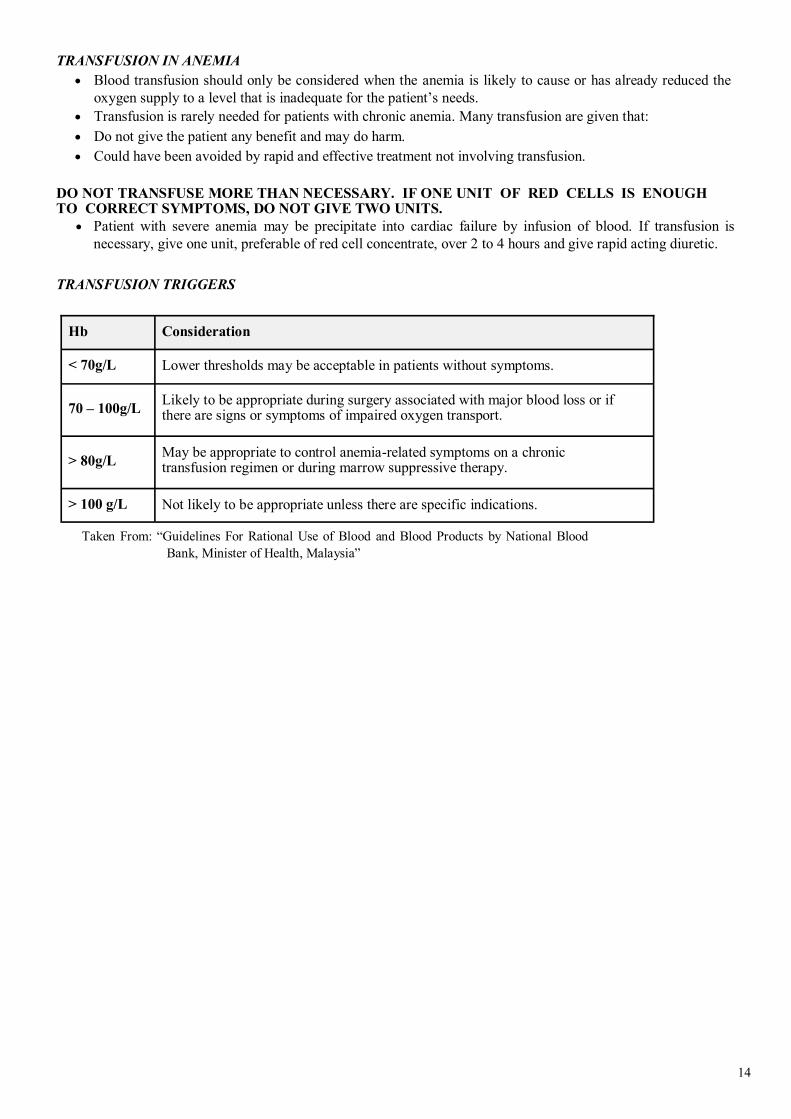
TRANSFUSION IN ANEMIA
Blood transfusion should only be considered when the anemia is likely to cause or has already reduced the
oxygen supply to a level that is inadequate for the patient’s needs.
Transfusion is rarely needed for patients with chronic anemia. Many transfusion are given that:
Do not give the patient any benefit and may do harm.
Could have been avoided by rapid and effective treatment not involving transfusion.
DO NOT TRANSFUSE MORE THAN NECESSARY. IF ONE UNIT OF RED CELLS IS ENOUGH TO CORRECT SYMPTOMS, DO NOT GIVE TWO UNITS.
Patient with severe anemia may be precipitate into cardiac failure by infusion of blood. If transfusion is
necessary, give one unit, preferable of red cell concentrate, over 2 to 4 hours and give rapid acting diuretic.
TRANSFUSION TRIGGERS
Taken From: “Guidelines For Rational Use of Blood and Blood Products by National Blood
Bank, Minister of Health, Malaysia”
Hb
Consideration
< 70g/L
Lower thresholds may be acceptable in patients without symptoms.
70 – 100g/L
Likely to be appropriate during surgery associated with major blood loss or if there are signs or symptoms of impaired oxygen transport.
> 80g/L
May be appropriate to control anemia-related symptoms on a chronic transfusion regimen or during marrow suppressive therapy.
> 100 g/L
Not likely to be appropriate unless there are specific indications.
15
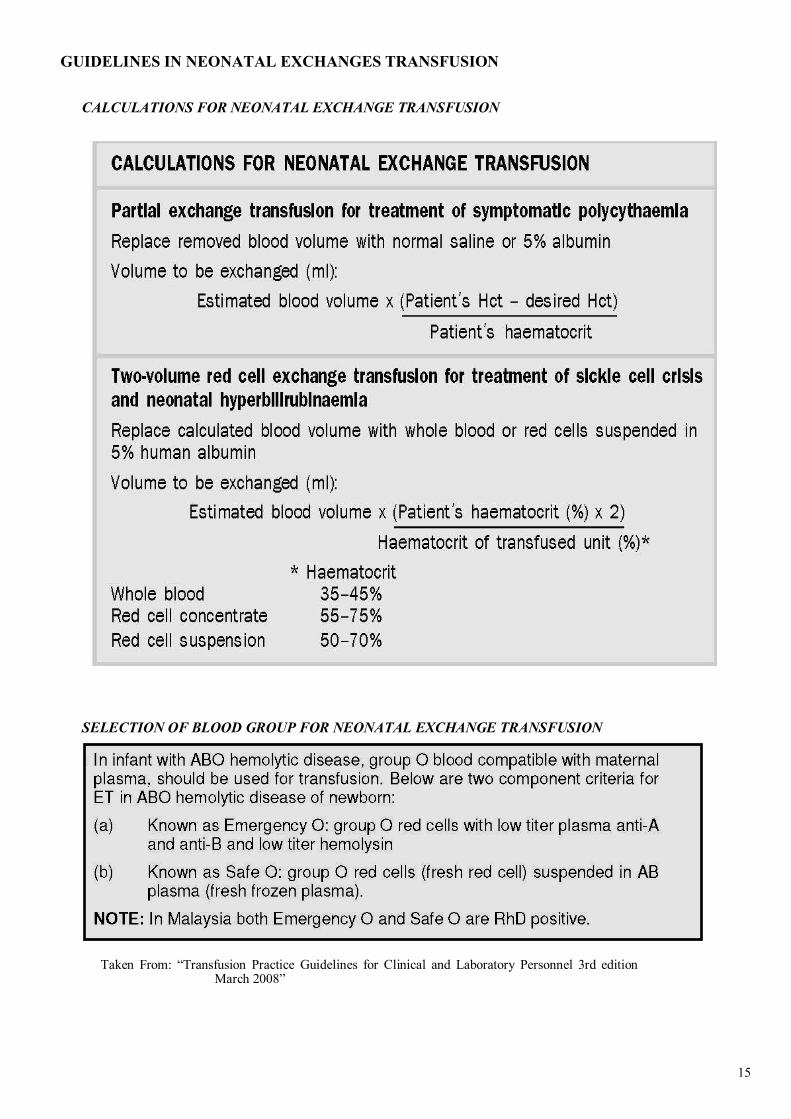
GUIDELINES IN NEONATAL EXCHANGES TRANSFUSION
CALCULATIONS FOR NEONATAL EXCHANGE TRANSFUSION
SELECTION OF BLOOD GROUP FOR NEONATAL EXCHANGE TRANSFUSION
Taken From: “Transfusion Practice Guidelines for Clinical and Laboratory Personnel 3rd edition March 2008”

16
PROCEDURE
Taken from “ The Clinical Use of Blood by World Health Oraganization, Blood Transfusion

17
NON RED CELL PRODUCTS
SELECTION OF NON RED CELL PRODUCTS
Recommended ABO group for plasma products (FFP, Cryoprecipitate)
Platelet Concentrates in order preference should be:
Patient’s own ABO group
ABO antigen compatible (but plasma incompatible)
ABO antigen incompatible GUIDELINES IN PLATELETS TRANSFUSION
1 unit random platelet will increases platelet count up to 5-10 x 109
Cut off values of platelet count for platelet transfusion :
Taken From: “Guidelines For Rational Use of Blood and Blood Products by National Blood Bank, Minis-
ter of Health, Malaysia”
Clinical Indication Cut off values of platelet count
Hematological Malignancies <20x109
PROCEDURE
Bone marrow Aspiration <20x109, providing adequate surface pressure is applied
Lumbar Puncture, Epidural, OGDS, Indwelling lines, Biopsy, Laparotomy
<50x109
Brain & Eye operation <100x109
MASSIVE TRANSFUSION
Acute Bleeding <50x109
Multiple Trauma / CNS Injury <100x109
DISSEMINATED INTRASCULAR COAGULATION
Acute DIVC <50x109
DIVC with absence of bleeding Platelet transfusion should not be given
IMMUNE THROMBOCYTOPENIA
Autoimmune
Thrombocytopenia Only for life – threatening bleeding form GIT/GUT/CNS and other con-
ditions with severe thrombocytopenia (<10x109 )
Neonatal Autoimmune Thrombocytopenia (NAITP)
Transfuse compatible platelet ASAP, ideally HPA-1a neg, HPA-5b neg. Platelet prepared from mother should be irradiated and washed
Post Transfusion Purpura Platelet transfusion usually ineffective, maybe used in acute phase e.g opera-
tion
PLATELET TRANSFUSION IN DENGUE FEVER – Please refer to latest CPG in Management of Dengue
PLATELET FUNCTION DISORDERS
Platelet only indicated if other measures fail to control bleeding
18
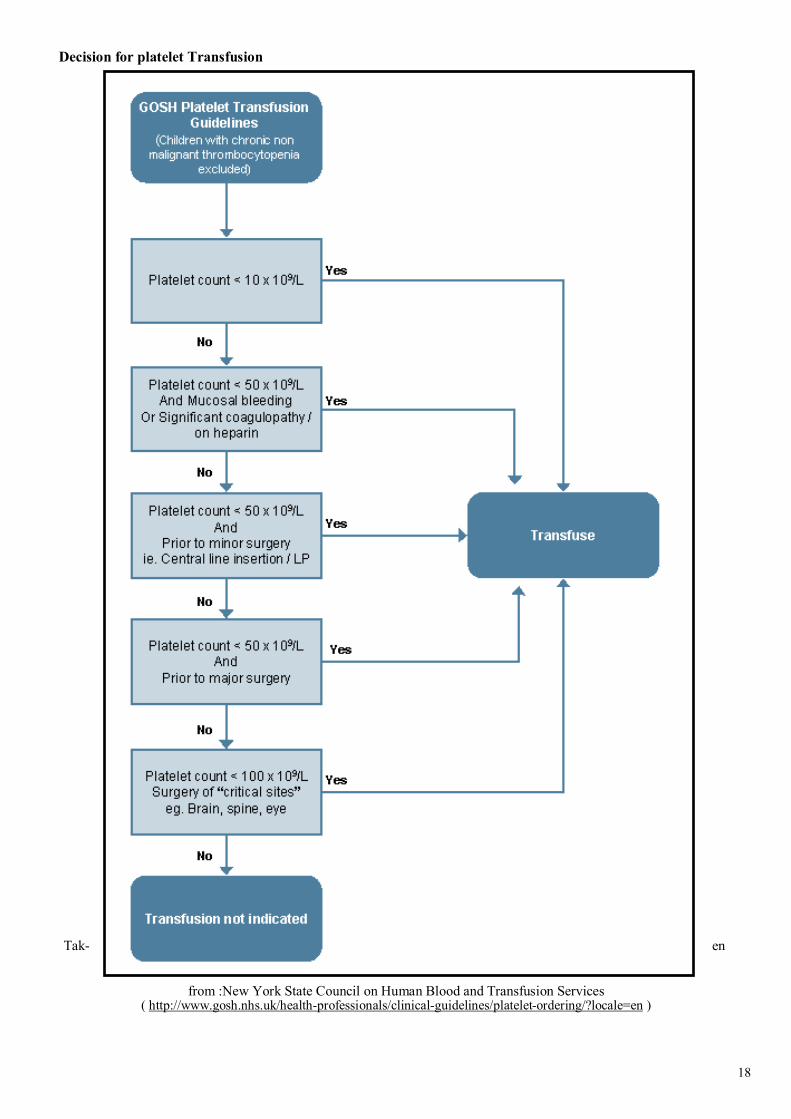
Decision for platelet Transfusion
Tak- en
from :New York State Council on Human Blood and Transfusion Services ( http://www.gosh.nhs.uk/health-professionals/clinical-guidelines/platelet-ordering/?locale=en )
19
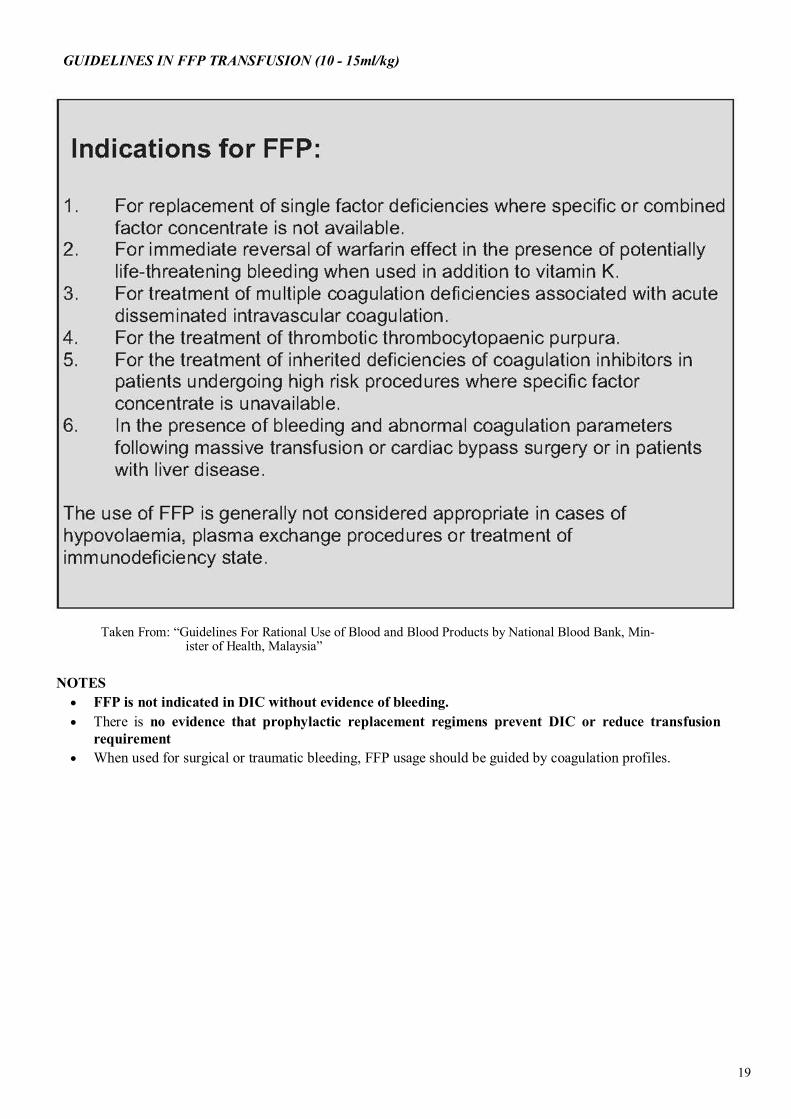
GUIDELINES IN FFP TRANSFUSION (10 - 15ml/kg)
Taken From: “Guidelines For Rational Use of Blood and Blood Products by National Blood Bank, Min-
ister of Health, Malaysia”
NOTES
FFP is not indicated in DIC without evidence of bleeding.
There is no evidence that prophylactic replacement regimens prevent DIC or reduce transfusion
requirement
When used for surgical or traumatic bleeding, FFP usage should be guided by coagulation profiles.

20
GUIDELINES OF CRYOPRECIPITATE TRANSFUSION (5-10ML/kg)
Indicated if the plasma fibrinogen is < 1g/L
Taken From: “Guidelines For Rational Use of Blood and Blood Products by National Blood Bank, Minister of Health,
Malaysia”
21
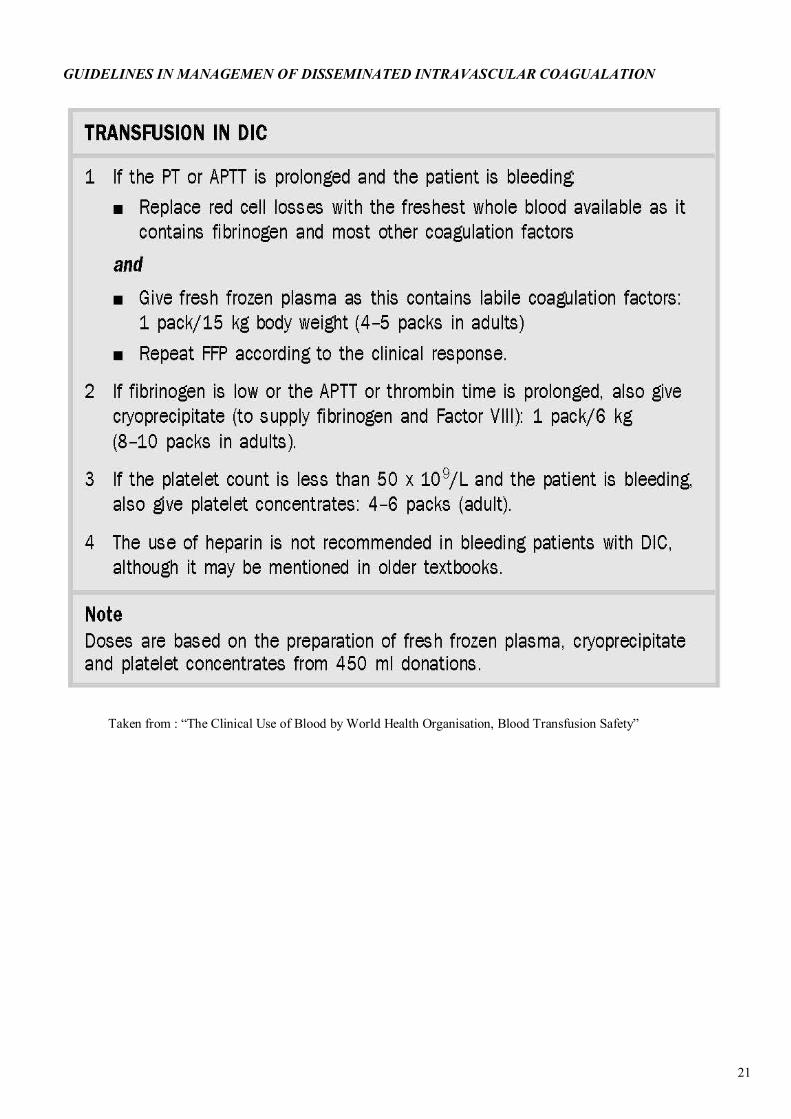
GUIDELINES IN MANAGEMEN OF DISSEMINATED INTRAVASCULAR COAGUALATION
Taken from : “The Clinical Use of Blood by World Health Organisation, Blood Transfusion Safety”

22
WHAT IS CT RATIO ?
CT RATIO
23
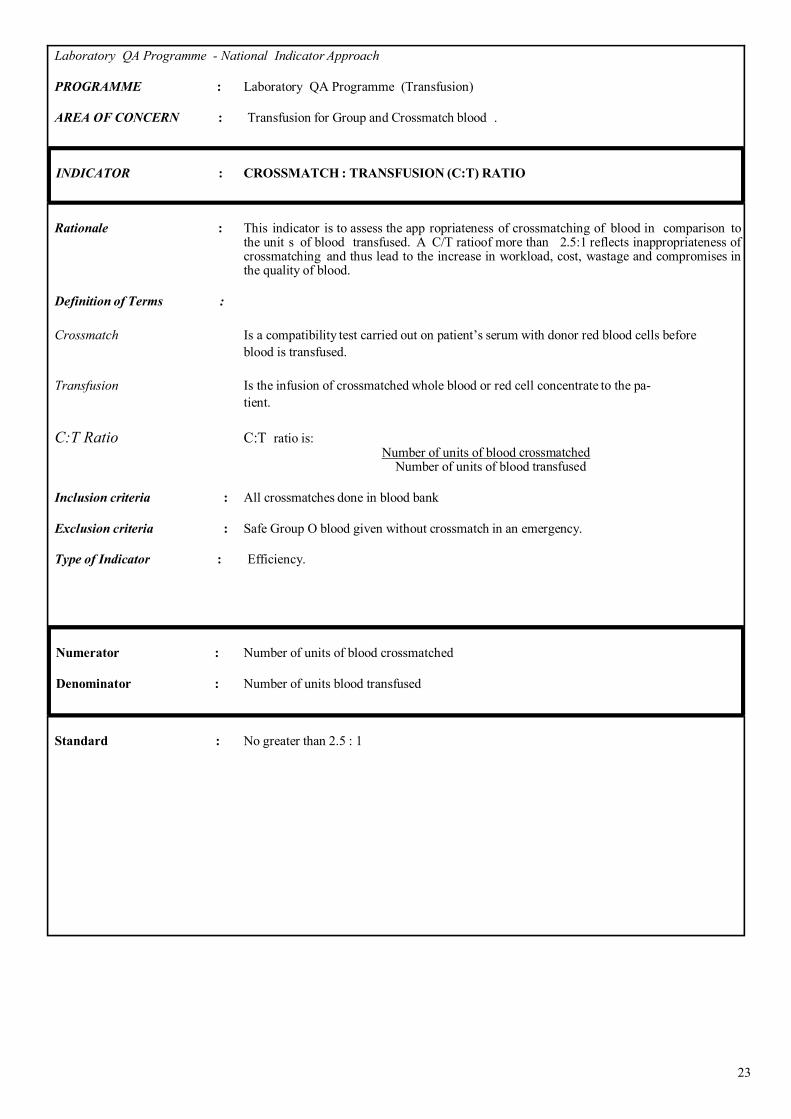
Laboratory QA Programme - National Indicator Approach
PROGRAMME : Laboratory QA Programme (Transfusion)
AREA OF CONCERN : Transfusion for Group and Crossmatch blood .
INDICATOR : CROSSMATCH : TRANSFUSION (C:T) RATIO
Rationale : This indicator is to assess the app ropriateness of crossmatching of blood in comparison to
the unit s of blood transfused. A C/T ratioof more than 2.5:1 reflects inappropriateness of crossmatching and thus lead to the increase in workload, cost, wastage and compromises in the quality of blood.
Definition of Terms :
Crossmatch Is a compatibility test carried out on patient’s serum with donor red blood cells before
blood is transfused.
Transfusion Is the infusion of crossmatched whole blood or red cell concentrate to the pa-
tient.
C:T Ratio C:T ratio is: Number of units of blood
Number of units of blood
Inclusion criteria : All crossmatches done in blood bank
Exclusion criteria : Safe Group O blood given without crossmatch in an emergency.
Type of Indicator : Efficiency.
Numerator : Number of units of blood crossmatched
Denominator : Number of units blood transfused
Standard : No greater than 2.5 : 1
24
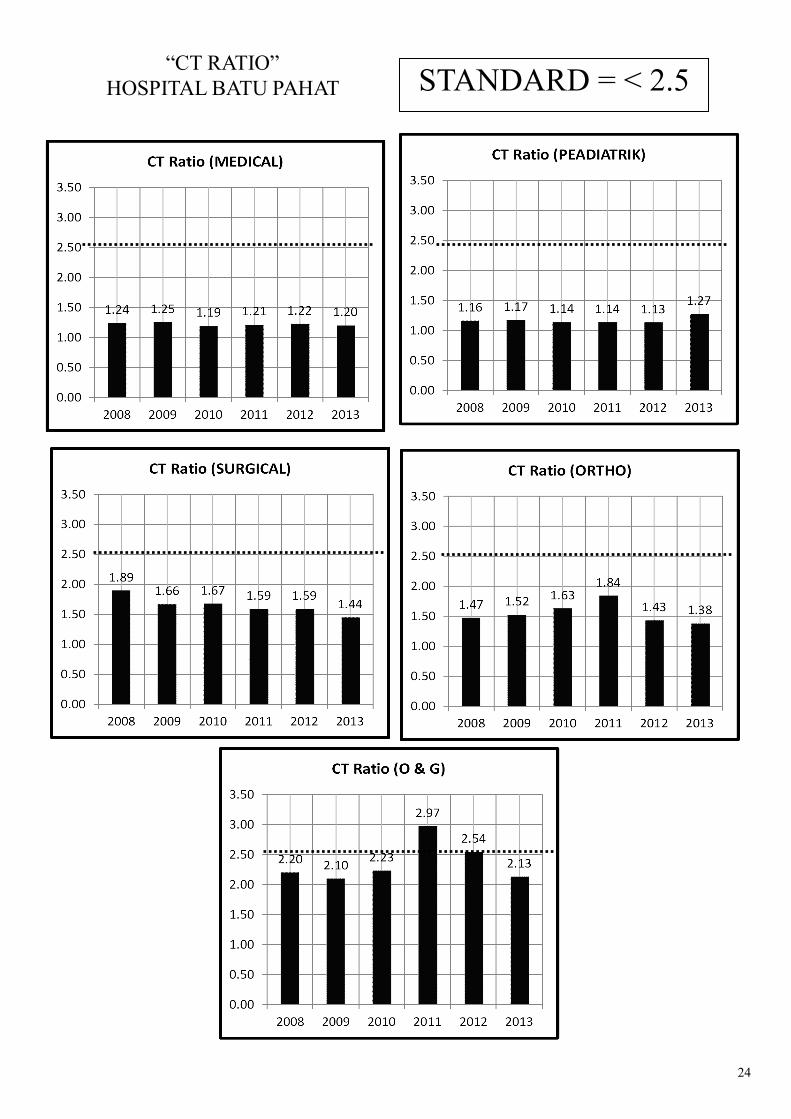
“CT RATIO”
HOSPITAL BATU PAHAT STANDARD = < 2.5
25
APPENDIX
26
APPENDIX 1
27
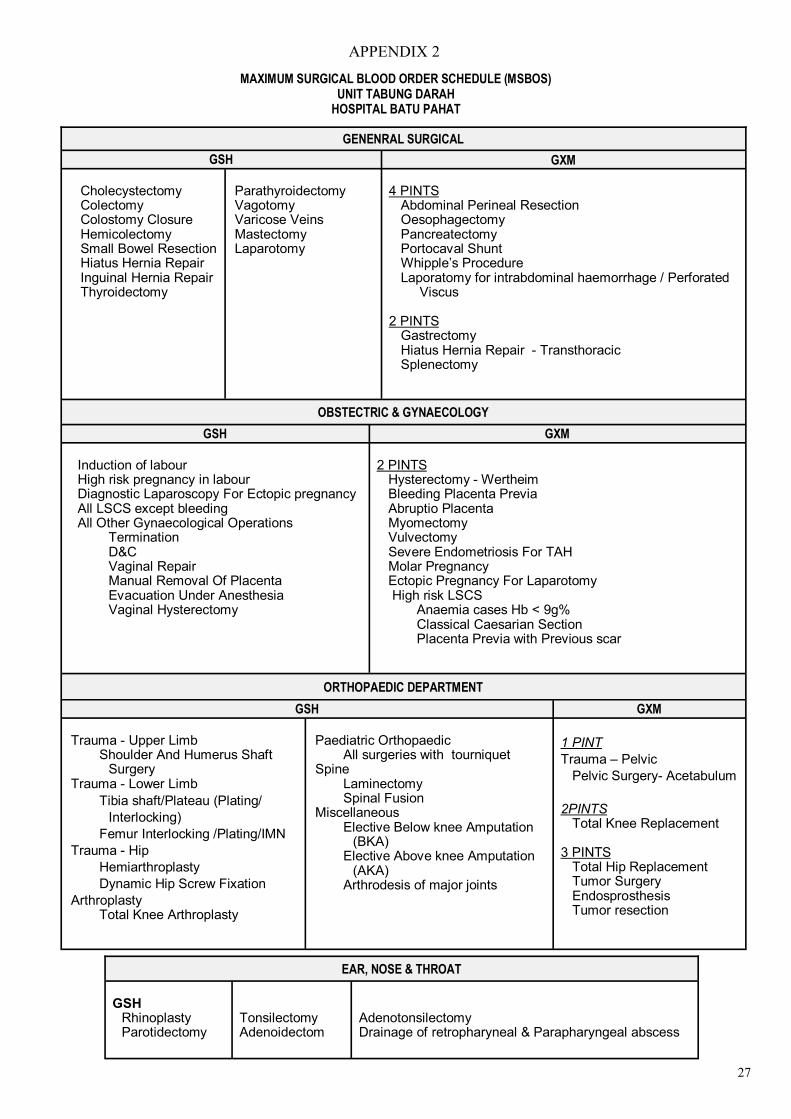
APPENDIX 2
GENENRAL SURGICAL
GSH GXM
Cholecystectomy Colectomy Colostomy Closure Hemicolectomy Small Bowel Resection Hiatus Hernia Repair Inguinal Hernia Repair Thyroidectomy
Parathyroidectomy Vagotomy Varicose Veins Mastectomy Laparotomy
4 PINTS
Abdominal Perineal Resection Oesophagectomy Pancreatectomy Portocaval Shunt Whipple’s Procedure Laporatomy for intrabdominal haemorrhage / Perforated
Viscus 2 PINTS
Gastrectomy Hiatus Hernia Repair - Transthoracic Splenectomy
OBSTECTRIC & GYNAECOLOGY
GSH GXM
Induction of labour High risk pregnancy in labour Diagnostic Laparoscopy For Ectopic pregnancy All LSCS except bleeding All Other Gynaecological Operations
Termination D&C Vaginal Repair Manual Removal Of Placenta Evacuation Under Anesthesia Vaginal Hysterectomy
2 PINTS
Hysterectomy - Wertheim Bleeding Placenta Previa Abruptio Placenta Myomectomy Vulvectomy Severe Endometriosis For TAH Molar Pregnancy Ectopic Pregnancy For Laparotomy High risk LSCS
Anaemia cases Hb < 9g% Classical Caesarian Section Placenta Previa with Previous scar
ORTHOPAEDIC DEPARTMENT
GSH GXM
Trauma - Upper Limb
Shoulder And Humerus Shaft Surgery
Trauma - Lower Limb
Tibia shaft/Plateau (Plating/
Interlocking)
Femur Interlocking /Plating/IMN
Trauma - Hip
Hemiarthroplasty
Dynamic Hip Screw Fixation
Arthroplasty Total Knee Arthroplasty
Paediatric Orthopaedic
All surgeries with tourniquet Spine
Laminectomy Spinal Fusion
Miscellaneous Elective Below knee Amputation
(BKA) Elective Above knee Amputation
(AKA) Arthrodesis of major joints
1 PINT
Trauma – Pelvic
Pelvic Surgery- Acetabulum
2PINTS Total Knee Replacement
3 PINTS
Total Hip Replacement Tumor Surgery Endosprosthesis Tumor resection
EAR, NOSE & THROAT
GSH
Rhinoplasty Parotidectomy
Tonsilectomy Adenoidectom
Adenotonsilectomy Drainage of retropharyneal & Parapharyngeal abscess
MAXIMUM SURGICAL BLOOD ORDER SCHEDULE (MSBOS) UNIT TABUNG DARAH
HOSPITAL BATU PAHAT
28
APPENDIX 3

29
APPENDIX 4
CHECKLIST FOR TAKING BLOOD FOR GROUP AND CRO
Taken From: Transfusion Practice Guidelines For Clinical and Laboratory Personnel, 3rd Edition 2008 by National
Blood Centre, Ministry Of Health Malaysia.
30
APPENDIX 5
31
APPENDIX 6
32
G
rou
p,
Scre
en
& H
old
(G
SH
)
Pa
ck
ed
Cell
FF
P /
CR
YO
P
late
let
Con
cen
-tr
ati
on
Ord
erin
g
(ED
TA
Tu
be)
Per
mis
sion
fro
m M
O b
lood
ban
k i
s n
ot
nec
essa
ry
R
eques
t ac
cord
ing t
o M
SB
OS
S
ample
wil
l be
kep
t fo
r 72h
ours
P
erm
issi
on f
rom
MO
blo
od b
ank i
s n
eed
ed i
f re
qu
ire
con
ver
sion
form
G
SH
to G
XM
O
nce
con
ver
ted i
s co
nsi
der
use
d, n
ew
reques
t is
nee
ded
aft
er c
on
ver
sion
P
erm
issi
on f
rom
MO
blo
od
ban
k i
s n
eed
ed
N
o s
ample
is
requir
ed i
f pat
ient
has
rec
ord
s of
pre
vio
us
tran
sfusi
on d
uri
ng c
urr
ent
adm
issi
on.
R
eques
t w
hen
nee
ded
N
o r
eser
vat
ion
/st
andby
is
allo
w
Em
erg
en
cy
G
et p
erm
issi
on f
rom
MO
blo
od
ban
k
In
form
Blo
od
Ban
k
R
un
for
blo
od
R
eg
ula
r
G
et p
erm
issi
on f
orm
MO
blo
od
ban
k.
D
isp
atch
req
ues
t fo
rm &
blo
od
sam
ple
to b
lood
ban
k
Tu
rn
Aro
un
d
Process
ing
(T
AT
)
Blo
od
& R
h G
rou
pin
g
A
nti
bod
y S
cree
nin
g
Blo
od
& R
h G
rou
pin
g
S
alin
e C
ross
mat
chin
g
D
ocu
men
tati
on
Blo
od
was
su
pp
lied
Pro
ceed
to F
ull
Cro
ss m
atch
ing
Blo
od
& R
h G
rou
pin
g
G
XM
Docu
men
tati
on
Blo
od
is
read
y fo
r co
llec
tion
Blo
od
& R
h G
rou
pin
g
D
ocu
men
tati
on
Blo
od p
roduct
s i
s su
ppli
ed
Posi
tive
P
roce
ed t
o
GX
M D
irec
tly
Neg
ativ
e
Sam
ple
wil
l be
kep
t fo
r 72hrs
1.
Th
e d
ura
tion
of
pro
cess
ing w
ill
var
ies
acco
rdin
g t
o w
ork
load
s &
avai
labil
ity
of
com
pat
ible
blo
od
/ b
lood
pro
du
cts
2.
Th
e ab
ove
esti
mat
ed d
ura
tion
of
pro
cess
ing
on
ly v
alid
if
no p
roble
ms
fou
nd
duri
ng A
nti
bod
y S
cree
nin
g /
Cro
ss m
atch
ing &
avai
labil
ity
of
com
pat
ible
blo
od.
3.
Ref
erra
l to
HS
AJB
/ P
usa
t D
arah
Neg
ara
wil
l be
req
uir
ed f
or
any
dif
ficu
lt c
ross
mat
chin
g. In
th
is s
ituat
ion, it
may
req
uir
e 2
-3
or
more
work
ing d
ays
for
the
pro
cess
.
< 3
0 m
in
1 –
2 h
ours
or
mor
e, d
epen
d o
n
avai
labil
ity o
f co
mpati
-ble
blo
od
<
30 m
in
If
pat
ien
t hav
e his
tory
of
blo
od t
ran
sfusi
on
duri
ng
curr
ent
adm
issi
on, n
o b
lood s
ample
is
req
uir
ed.
P
late
le/F
FP
/CR
YO
wil
l be
sup
pli
ed d
irec
t-ly
acc
ord
ing t
o b
lood g
roupin
g
F
FP
& C
ryo w
ill
be
thaw
ed b
efore
supply
APPENDIX 7
PR
OC
ED
UR
E I
N B
LO
OD
TR
AN
SF
US
ION
LA
B
33
G
rou
p,
Scre
en
& H
old
(G
SH
)
Em
erg
en
cy B
lood
Pa
cked
Cel
l (C
om
ple
ted
GX
M)
F
FP
/ C
RY
O
Pla
tele
t C
on
cen
trati
on
Du
ra
tion
of
rese
r-va
tion
24
hours
bef
ore
rel
ease
No r
eser
vat
ion
is
allo
w
R
equ
est
wh
en r
equir
e
Su
pp
ly
Aft
er b
lood
gro
up
ing
and s
alin
e cr
oss
-
mat
chin
g
D
oct
or
/ st
aff
mu
st r
ush
to
blo
od
ban
k w
ith
ice
box
im
med
iate
ly
Aft
er c
ross
-mat
chin
g
A
fter
Gro
upin
g
N
o c
ross
-mat
chin
g r
equir
ed
R
equ
est
on
ly w
hen
req
uir
ed
Coll
ecti
on
B
lood
Box
wit
h I
ce
B
lood
Box
wit
hou
t Ic
e
Use
/ T
ra
nsf
use
d
Mu
st b
e tr
ansf
use
im
med
iate
ly w
ith
in 3
0 a
fter
coll
ec-
tion
, p
leas
e re
turn
im
med
iate
ly t
o b
lood
ban
k i
f n
ot
tran
sfu
se
C
om
ple
ted
Tra
nsf
usi
on
wit
hin
4 h
our
FF
P/C
RY
O
P
lease
in
form
th
e b
lood
ban
k
befo
re
coell
ecti
on
(th
aw
ing)
T
ran
sfuse
im
med
iate
ly a
fter
thaw
ing , t
o c
om
ple
te t
ran
sfusi
on
wit
hin
4
hours
PL
AT
EL
ET
S
Tra
nsf
use
im
med
iate
ly,
to c
om
ple
te t
ran
sfusi
on a
s so
on
as
poss
ible
Sto
ra
ge
Sto
re a
t le
ss t
han
-25°C
S
hou
ld n
ot
be
store
d o
r
kep
t in
th
e w
ards
M
ust
be
tran
sfu
sed a
s so
on
as p
oss
ible
aft
er t
haw
ing
C
oag
ula
tion
fac
tor
wil
l be
deg
rad
ed r
apid
ly a
fter
thaw
-in
g
R
oom
Tem
per
ature
+20°C
+2
4°
C o
n a
git
ator
N
ever
sto
re i
n r
efri
ger
ator
S
tore
at
tem
per
ature
+2
°C t
o +
6°C
B
lood
sh
ou
ld n
ot
be
store
in
war
d f
or
more
th
an 4
h
our.
Sta
ndby
blo
od
for
surg
ery
in O
per
atio
n T
hea
ter
mu
st
be
store
in
wel
l m
onit
ore
d t
emp
erat
ure
blo
od
fri
dge.
34
G
rou
p,
Scre
en
& H
old
(G
SH
)
FF
P /
CR
YO
P
late
let
Con
cen
trati
on
Pa
ck
ed
Cell
Retu
rn
Ret
urn
im
med
iate
ly i
f n
ot
use
d
Aft
er
use
F
ill
up t
he
Blo
od
Tag
an
d r
eturn
tog
eth
er w
ith e
mpty
bag
to b
lood b
ank a
s so
on
as
poss
ible
Imp
orta
nce n
ote
s :
C
hec
kli
st b
efore
dec
ided
to c
oll
ect
blo
od
pro
du
cts
from
blo
od
ban
k
Con
sen
t fo
r tr
ansf
usi
on
Pre
sen
t of
fun
ctio
nin
g I
V a
cces
s
Vit
als
sign
of
the
pat
ient
is s
table
P
leas
e tr
ansf
use
blo
od p
rodu
cts
imm
edia
tely
, b
lood
mu
st N
EV
ER
be
stored
in
a w
ard
or
cli
nic
al/
dom
est
ic r
efr
iger
ato
r u
nd
er a
ny
cir
cu
mst
an
ces.
S
tan
d b
y B
lood f
or
pat
ien
ts d
uri
ng s
urg
ery
and in th
e im
med
iate
post
-op
erat
ive
per
iod
mu
st b
e st
ore
d in th
e T
HE
AT
RE
blo
od
frid
ge.
35
APPENDIX 8
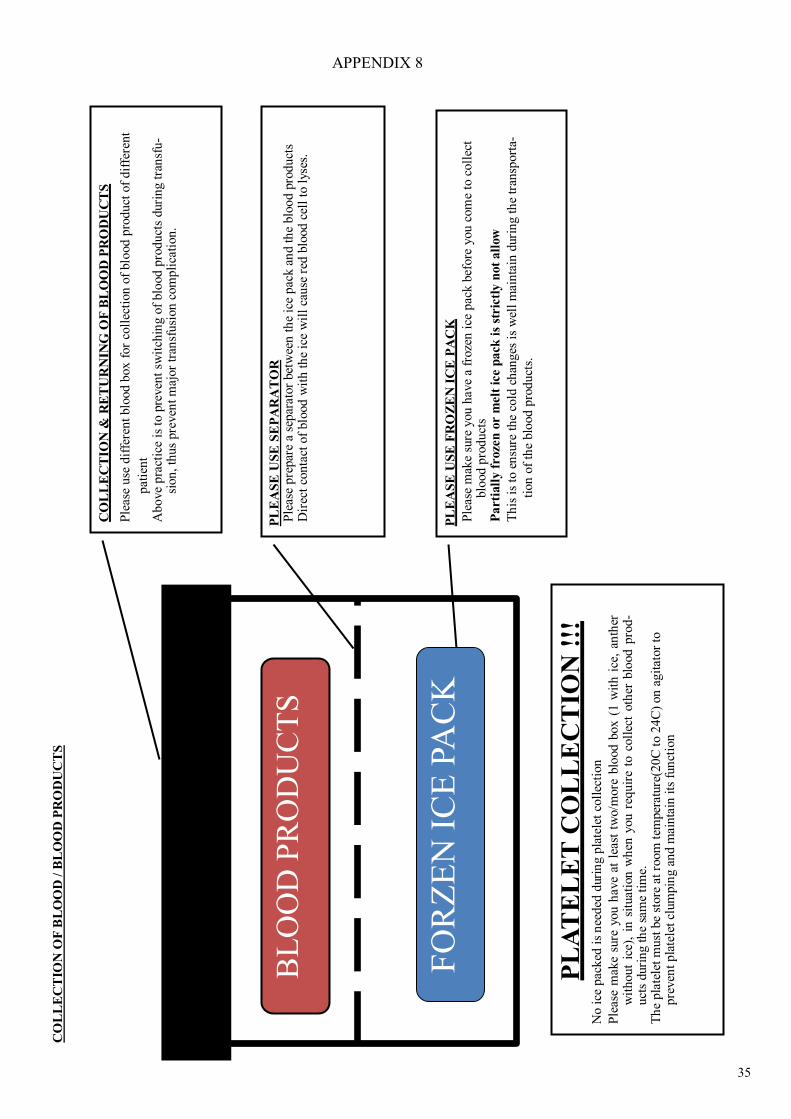
CO
LL
EC
TIO
N &
RE
TU
RN
ING
OF
BL
OO
D P
RO
DU
CT
S
Ple
ase
use
dif
fere
nt
blo
od b
ox f
or
coll
ecti
on
of
blo
od p
roduct
of
dif
fere
nt
pat
ien
t A
bo
ve
pra
ctic
e is
to p
reven
t sw
itch
ing o
f blo
od p
rodu
cts
duri
ng
tra
nsf
u-
sion
, th
us
pre
ven
t m
ajor
tran
sfusi
on c
om
pli
cati
on.
BL
OO
D P
RO
DU
CT
S
PL
EA
SE
US
E S
EP
AR
AT
OR
P
leas
e p
repar
e a
separ
ator
bet
wee
n t
he
ice
pac
k a
nd t
he
blo
od p
roduct
s D
irec
t co
nta
ct o
f blo
od w
ith t
he
ice
wil
l ca
use
red
blo
od c
ell
to l
yses
.
PL
EA
SE
US
E F
RO
ZE
N I
CE
PA
CK
Ple
ase
mak
e su
re y
ou
hav
e a
froze
n i
ce p
ack b
efore
you c
om
e to
coll
ect
blo
od
pro
du
cts
Pa
rti
all
y f
roze
n o
r m
elt
ice p
ack
is
stric
tly n
ot
all
ow
Th
is i
s to
en
sure
the
cold
ch
ang
es i
s w
ell
mai
nta
in d
uri
ng t
he
tran
sport
a-
tion
of
the
blo
od p
roduct
s.
FO
RZ
EN
IC
E P
AC
K
PL
AT
EL
ET
CO
LL
EC
TIO
N !
!!
No i
ce p
ack
ed i
s n
eeded
dur
ing p
late
let
coll
ecti
on
Ple
ase
mak
e su
re y
ou h
ave
at l
east
tw
o/m
ore
blo
od
box
(1
wit
h i
ce,
anth
er
wit
hou
t ic
e),
in s
ituat
ion
wh
en y
ou r
equir
e to
coll
ect
oth
er b
lood
pro
d-
uct
s duri
ng t
he
sam
e ti
me.
T
he
pla
tele
t m
ust
be
store
at
room
tem
per
ature
(20C
to 2
4C
) on
agit
ator
to
pre
ven
t p
late
let
clum
pin
g a
nd m
ainta
in i
ts f
un
ctio
n
CO
LL
EC
TIO
N O
F B
LO
OD
/ B
LO
OD
PR
OD
UC
TS
36
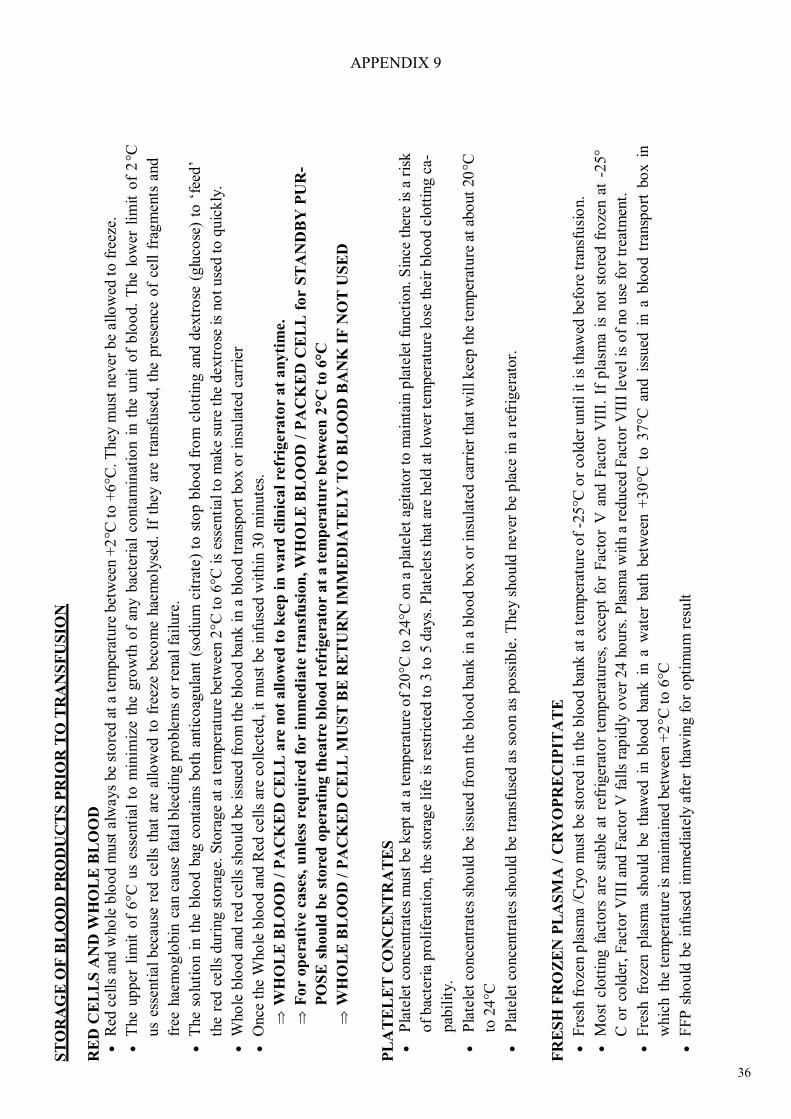
ST
OR
AG
E O
F B
LO
OD
PR
OD
UC
TS
PR
IOR
TO
TR
AN
SF
US
ION
R
ED
CE
LL
S A
ND
WH
OL
E B
LO
OD
Red
cell
s and w
ho
le b
loo
d m
ust
alw
ays
be
sto
red a
t a
tem
per
atu
re b
etw
een +
2°C
to +
6°C
. T
hey m
ust
never
be
all
ow
ed t
o f
reez
e.
T
he
upper
lim
it o
f 6°C
us
esse
nti
al
to m
inim
ize
the
gro
wth
of
any b
acte
rial
conta
min
atio
n i
n t
he
unit
of
blo
od.
The
low
er l
imit
of
°C
us
esse
nti
al
bec
ause
red
cell
s th
at a
re a
llo
wed
to f
reez
e bec
om
e hae
mo
lyse
d.
If t
hey a
re t
ransf
use
d,
the
pre
sence
of
cell
fg
ments
and
free
hae
mo
glo
bin
can c
ause
fat
al ble
ed
ing p
roble
ms
or
renal fa
ilure
.
T
he
solu
tio
n i
n t
he
blo
od b
ag c
onta
ins
bo
th a
nti
co
agula
nt
(so
diu
m c
itra
te)
to s
top b
loo
d f
rom
clo
ttin
g a
nd d
extr
ose
(glu
cose
) to
‘fe
ed’
the
red c
ell
s duri
ng s
tora
ge.
Sto
rage
at a
tem
per
ature
bet
wee
n 2
°C t
o 6
°C i
s es
senti
al to
mak
e su
re t
he
dextr
ose
is
no
t u
sed t
o q
uic
kly
.
W
ho
le b
loo
d a
nd r
ed c
ells
sho
uld
be
issu
ed f
rom
the
blo
od b
ank
in a
blo
od t
ransp
ort
bo
x o
r in
sula
ted c
arri
er
O
nce
the
Who
le b
loo
d a
nd R
ed c
ell
s ar
e co
llect
ed, it
mu
st b
e in
fuse
d w
ithin
30 m
inute
s.
W
HO
LE
BL
OO
D /
PA
CK
ED
CE
LL
are
not
all
ow
ed t
o k
eep
in
ward
cli
nic
al
refr
igera
tor
at
an
yti
me.
F
or
op
era
tive
case
s, u
nle
ss r
equ
ired
fo
r im
med
iate
tra
nsf
usi
on
, W
HO
LE
BL
OO
D /
PA
CK
ED
CE
LL
fo
r S
TA
ND
BY
PU
R-
PO
SE
sh
ou
ld b
e st
ore
d o
per
ati
ng t
hea
tre
blo
od
ref
rigera
tor
at
a t
emp
era
ture
bet
wee
n 2
°C t
o 6
°C
W
HO
LE
BL
OO
D /
PA
CK
ED
CE
LL
MU
ST
BE
RE
TU
RN
IM
ME
DIA
TE
LY
TO
BL
OO
D B
AN
K I
F N
OT
US
ED
PL
AT
EL
ET
CO
NC
EN
TR
AT
ES
Pla
tele
t co
nce
ntr
ates
must
be
kep
t at
a t
emper
ature
of
20
°C t
o 2
4°C
on a
pla
tele
t ag
itat
or
to m
ain
tain
pla
tele
t fu
nct
ion.
Sin
ce t
her
e is
a r
isk
of
bac
teri
a pro
life
rati
on, th
e st
ora
ge
life
is
rest
rict
ed t
o 3
to 5
days.
Pla
tele
ts t
hat
are
held
at
low
er t
emper
ature
lo
se
heir
blo
od c
lott
ing c
a-
pab
ilit
y.
P
late
let
conce
ntr
ates
sho
uld
be
issu
ed f
rom
the
blo
od b
ank i
n a
blo
od b
ox o
r in
sula
ted c
arri
er t
hat
wil
l keep
the
tem
per
ature
at
abo
ut
20
°C
to 2
4°C
P
late
let
conce
ntr
ates
sho
uld
be
tran
sfuse
d a
s so
on a
s po
ssib
le.
They s
ho
uld
never
be
pla
ce i
n a
refr
igera
tor.
FR
ES
H F
RO
ZE
N P
LA
SM
A /
CR
YO
PR
EC
IPIT
AT
E
F
resh
fro
zen p
lasm
a /C
ryo
must
be
store
d in t
he
blo
od b
ank a
t a
tem
per
ature
of
-25
°C o
r co
lder
unti
l it
is
thaw
ed b
efo
re t
ransf
usi
on.
M
ost
clo
ttin
g f
acto
rs a
re s
table
at
refr
iger
ato
r te
mper
ature
s, e
xce
pt
for
Fac
tor
V a
nd F
acto
r V
III.
If
pla
sma
is n
ot
sto
red f
roze
n a
t -2
5°
C o
r co
lder
, F
acto
r V
III
and
Fac
tor
V f
all
s ra
pid
ly o
ver
24 h
ours
. P
lasm
a w
ith a
red
uce
d F
acto
r V
III
level
is o
f no
use
fo
r tr
eatm
ent.
F
resh
fro
zen p
lasm
a sh
ou
ld b
e th
awed
in b
loo
d b
ank i
n a
wat
er b
ath b
etw
een +
30
°C t
o 3
7°C
and i
ssued
in a
blo
od t
ransp
ort
bo
x i
n
whic
h t
he
tem
per
ature
is
main
tain
ed b
etw
een +
2°C
to
6°C
F
FP
sho
uld
be
infu
sed i
mm
edia
tely
aft
er t
haw
ing f
or
opti
mu
m r
esu
lt
APPENDIX 9
37
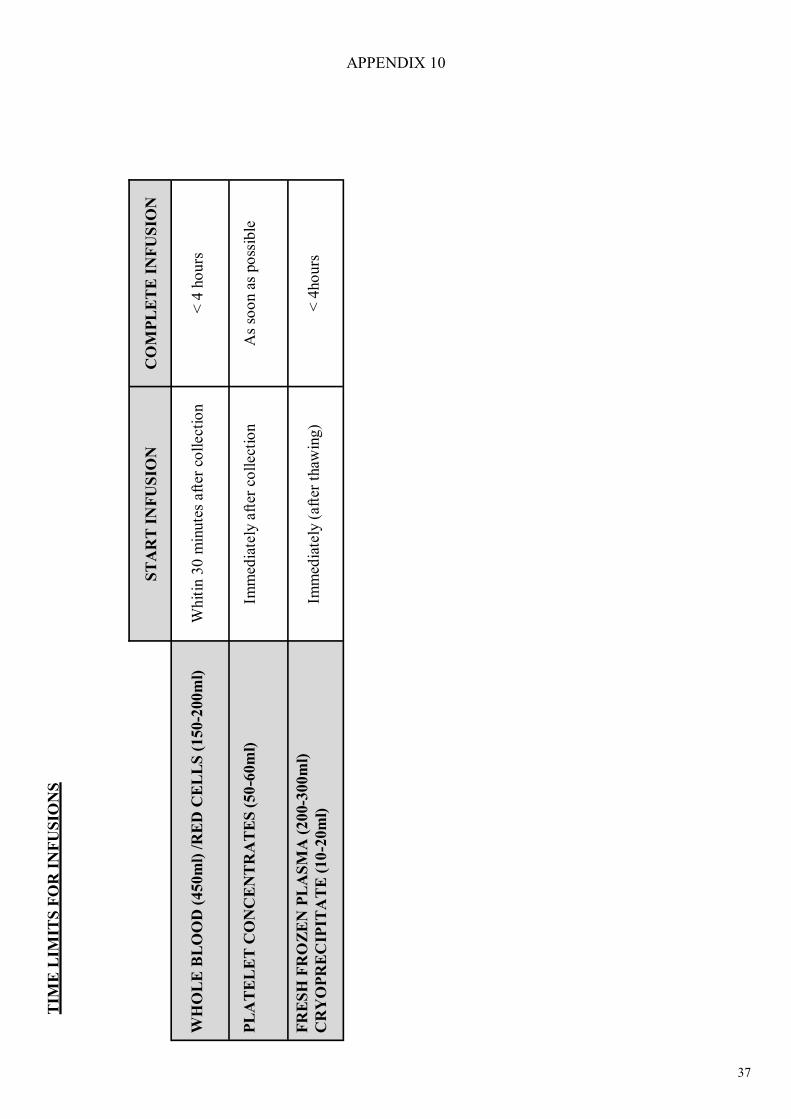
TIM
E L
IMIT
S F
OR
IN
FU
SIO
NS
ST
AR
T I
NF
US
ION
C
OM
PL
ET
E I
NF
US
ION
WH
OL
E B
LO
OD
(450m
l) /
RE
D C
EL
LS
(1
50-2
00m
l)
W
hit
in 3
0 m
inute
s aft
er c
oll
ect
ion
<
4 h
ours
P
LA
TE
LE
T C
ON
CE
NT
RA
TE
S (
50
-60m
l)
Im
med
iate
ly a
fter
co
llect
ion
A
s so
on a
s po
ssib
le
FR
ES
H F
RO
ZE
N P
LA
SM
A (
200-3
00m
l)
CR
YO
PR
EC
IPIT
AT
E (
10
-20m
l)
Im
med
iate
ly (
aft
er t
haw
ing)
<
4ho
urs
APPENDIX 10

38
HO
W T
O U
SE
BL
OO
D S
TIC
KE
R
APPENDIX 11
UP
PE
R S
EC
TIO
N:
Fil
l u
p t
he
deta
ils
of
tran
sfu
sion
com
ple
tely
R
etu
rn
th
e c
ard
togeth
er w
ith
em
pty
blo
od
bags
to
Blo
od
Ban
k a
s so
on
as
poss
ible
L
OW
ER
SE
CT
ION
: F
ill
up
th
e d
eta
ils
of
tran
sfu
sion
com
ple
tely
P
ast
e o
n p
ati
en
t’ f
ile f
or
futu
re r
efe
ren
ce
39
APPENDIX 12
40
APPENDIX 13
41
APPENDIX 14
42
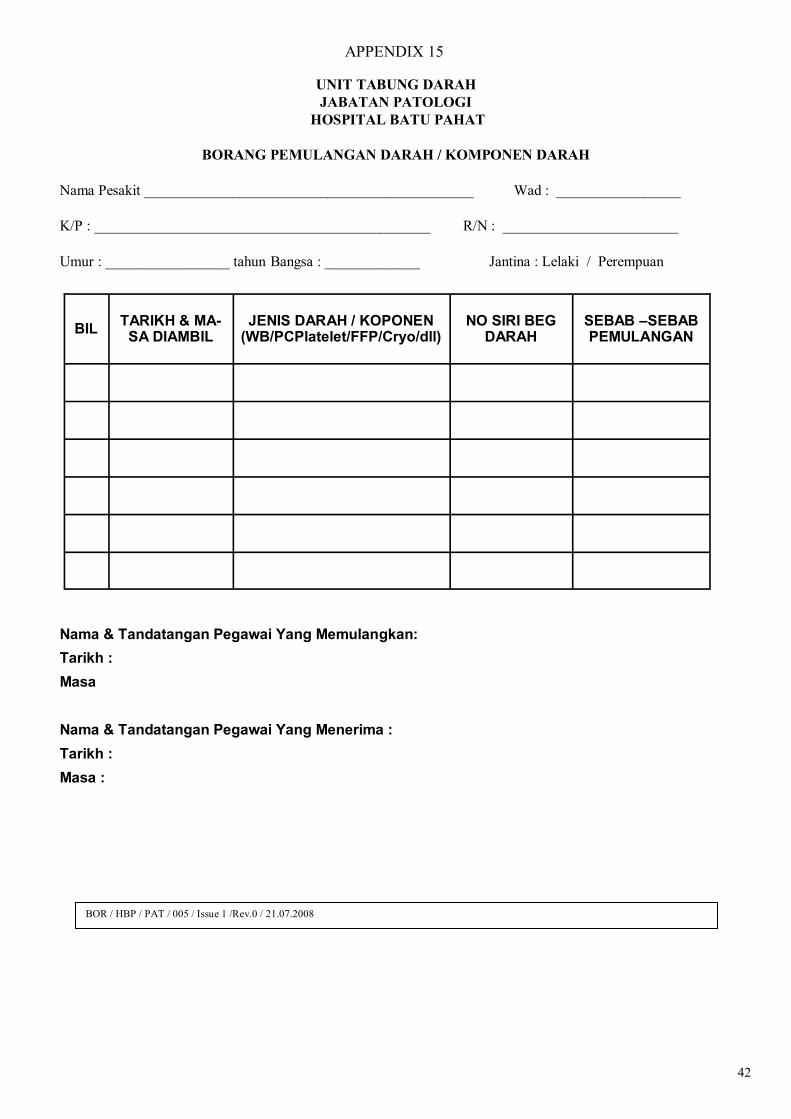
UNIT TABUNG DARAH
JABATAN PATOLOGI
HOSPITAL BATU PAHAT
BORANG PEMULANGAN DARAH / KOMPONEN DARAH
Nama Pesakit _____________________________________________ Wad : _________________
K/P : ______________________________________________ R/N : ________________________
Umur : _________________ tahun Bangsa : _____________ Jantina : Lelaki / Perempuan
Nama & Tandatangan Pegawai Yang Memulangkan:
Tarikh :
Masa
Nama & Tandatangan Pegawai Yang Menerima :
Tarikh :
Masa :
BIL TARIKH & MA-
SA DIAMBIL
JENIS DARAH / KOPONEN
(WB/PCPlatelet/FFP/Cryo/dll)
NO SIRI BEG DARAH
SEBAB –SEBAB PEMULANGAN
BOR / HBP / PAT / 005 / Issue 1 /Rev.0 / 21.07.2008
APPENDIX 15
43
REFERENCES
TRANSFUSION PRACTICE GUILDLINES FOR CLINICAL AND LABORATORY PERSONNEL,
3RD EDITION 2008 (By National Blood Centre, Ministry Of Health Malaysia)
Website: http://www.pdn.gov.my
GUILDLINES FOR THE RATIONAL USE OF BLOOD AND BLOOD PRODUCTS, 2ND EDITION
2007 (By National Blood Centre, Ministry Of Health Malaysia)
Website: http://www.pdn.gov.my
LABORATORY MANUAL (By Unit Transfusion medicine, HSAJB)
Website: http://hsajb.moh.gov.my/modules/xt_conteudo/index.php?&id=196
THE CLINICAL USE OF BLOOD(By World Health Organization, Blood Transfusion Safety)
Website: http://www.who.int/bloodsafety/clinical_use/en/Manual_EN.pdf
TECHNICAL MANUAL(By American Association of Blood Bank) A PHYSICIAN’S GUIDE TO TRANSFUSION OPTIONS (By New York State Council on Human Blood and Transfusion Services, Second Edition 2008) OTHER REFERENCE / WEBSITE
MOH Dengue Management CPG( http://moh.gov.my/v/id )
MOH Management of Thalassemia( http://moh.gov.my/v/ha )
MOH Management of ITP (http://moh.gov.my/v/hae )
http://www.transfusionguidelines.org.uk/docs/pdfs/htm_edition-4_all-pages.pdf
http://www.gosh.nhs.uk/clinical_information/clinical_guidelines?category=Blood%20transfusion
http://www.sld.cu/galerias/pdf/sitios/anestesiologia/practical_guidelines_blood_transfusion.pdf
http://www.nhmrc.gov.au/publications/synopses/cp77syn.htm

44

45
Notes
46
Notes

47
Notes
48
TERIMA KASIH DARI UNIT TABUNG DARAH HBP
Related Documents











