ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2018 Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1435 Birth asphyxia Fetal scalp blood sampling and risk factors for hypoxic ischemic encephalopathy LENA LILJESTRÖM ISSN 1651-6206 ISBN 978-91-513-0250-8 urn:nbn:se:uu:diva-340782

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1435
Birth asphyxia
Fetal scalp blood sampling and risk factors forhypoxic ischemic encephalopathy
LENA LILJESTRÖM
ISSN 1651-6206ISBN 978-91-513-0250-8urn:nbn:se:uu:diva-340782

Dissertation presented at Uppsala University to be publicly examined in Rosénsalen, Ing95/96, Akademiska sjukhuset, Uppsala, Thursday, 26 April 2018 at 13:15 for the degree ofDoctor of Philosophy (Faculty of Medicine). The examination will be conducted in Swedish.Faculty examiner: Associate professor Andreas Herbst (Department of Obstetrics andGynecology, Lunds University).
AbstractLiljeström, L. 2018. Birth asphyxia. Fetal scalp blood sampling and risk factors for hypoxicischemic encephalopathy. Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1435. 81 pp. Uppsala: Acta Universitatis Upsaliensis.ISBN 978-91-513-0250-8.
Preventing birth asphyxia is a major challenge in delivery care. The aims of this thesis wereto evaluate fetal scalp blood sampling (FBS) and explore risk factors for moderate to severeneonatal hypoxic ischemic encephalopathy (HIE).
In a study of 241 deliveries monitored by FBS, a discrepancy between pH and lactate (oneabnormal and one normal value) was common (55%) in combined FBS. We found that thefrequency of operative deliveries for fetal distress (ODFD) was lower when both pH and lactatewere analysed in FBS compared with analysis of only pH or lactate, without affecting neonataloutcome. (Study I)
In a questionnaire study, women (n = 51) monitored by FBS generally tolerated the test well.Women without epidural, with higher body mass index (BMI), and with less cervical dilatationhad higher pain ratings compared with their counterparts. The obstetricians that performed thetest generally experienced the test as easy to perform, but more complicated with high maternalBMI, less cervical dilatation, and higher station of the fetal head. (Study II)
In a national cohort of 692 428 live births ≥ 36 weeks, risk factors for moderate to severe HIEwere identified. We found a linear association between increasing maternal BMI and decreasingmaternal height and risk of HIE. Compared with non-short (≥156 cm) and normal weight(BMI<25 kg/m2) women, short and overweight women had a threefold risk of HIE. (Study III)
Obstetric emergencies occurred in 29% of HIE cases, more commonly in parous (37%)than in nulliparous (21%) women. Among nulliparous women, shoulder dystocia was mostcommon, with the strongest association to HIE. In parous women without previous caesarean,shoulder dystocia was most common, but placental abruption had the strongest association toHIE. Among parous women with previous caesarean, uterine rupture was the most prevalent,with the strongest association to HIE. (Study IV)
Conclusions: Combined FBS might decrease the frequency of ODFD. FBS is well tolerated inwomen and generally uncomplicated for the obstetrician to perform. Women with short statureand overweight have increased risk of having an infant with HIE. Obstetric emergencies arecommon underlying causes of HIE, especially in parous women.
Keywords: asphyxia, fetal scalp blood sampling, hypoxic ischemic encephalopathy, obstetricemergencies, operative deliveries for fetal distress, overweight, short stature
Lena Liljeström, Department of Women's and Children's Health, Akademiska sjukhuset,Uppsala University, SE-75185 Uppsala, Sweden.
© Lena Liljeström 2018
ISSN 1651-6206ISBN 978-91-513-0250-8urn:nbn:se:uu:diva-340782 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-340782)

To my family

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I. Liljeström L, Wikström AK, Hanson U, Åkerud H, Jonsson
M. (2011) Evaluation of the discrepancy between pH and lac-tate in combined foetal scalp blood sampling. Acta obstetricia et gynecologica Scandinavica, Oct 2011;90(10):1088-1093.
II. Liljeström L, Wikström AK, Skalkidou A, Åkerud H, Jonsson
M. (2014) Experience of foetal scalp blood sampling during labour. Acta obstetricia et gynecologica Scandinavica, Jan 2014;93(1):113-117.
III. Liljeström L, Ågren J, Wikström AK, Jonsson M. (2018) An-tepartum risk factors for moderate to severe neonatal hypoxic ischemic encephalopathy: a Swedish national cohort study. Acta obstetricia et gynecologica Scandinavica. Accepted.
IV. Liljeström L, Wikström AK, Jonsson M. (2018) Obstetric emergencies as antecedents to neonatal hypoxic ischemic en-cephalopathy, does parity matter? Manuscript.
Reprints were made with permission from the respective publishers.


Contents
Introduction ................................................................................................... 11 Management of pregnancy and labour in Sweden ................................... 12 Intrapartum fetal surveillance ................................................................... 13
Cardiotocography ................................................................................ 13 Fetal response to hypoxia—acid-base physiology ............................... 14 Fetal scalp blood sampling .................................................................. 15
Perinatal asphyxia .................................................................................... 20 Neonatal outcome measures ................................................................ 21 Hypoxic ischemic encephalopathy ...................................................... 22
Aims .............................................................................................................. 26
Materials and Methods .................................................................................. 27 Study populations and designs ................................................................. 27
Studies I and II ..................................................................................... 27 Studies III and IV ................................................................................ 28
Methods .................................................................................................... 28 Study I .................................................................................................. 28 Study II ................................................................................................ 29 Studies III and IV ................................................................................ 31
Statistics ................................................................................................... 32 Study I .................................................................................................. 32 Study II ................................................................................................ 32 Studies III and IV ................................................................................ 33
Ethical considerations .............................................................................. 34
Results ........................................................................................................... 35 Study I ...................................................................................................... 35 Study II ..................................................................................................... 38 Studies III and IV ..................................................................................... 41
Study III ............................................................................................... 44 Study IV ............................................................................................... 47
Discussion ..................................................................................................... 52 Clinical implications ................................................................................ 52
Study I .................................................................................................. 52 Study II ................................................................................................ 53 Studies III and IV ................................................................................ 54
Methodological considerations................................................................. 60 Studies I and II ..................................................................................... 60 Studies III and IV ................................................................................ 62
Conclusions ................................................................................................... 64
Future perspectives ....................................................................................... 65
Summary in Swedish - Sammanfattning på svenska .................................... 67
Acknowledgements ....................................................................................... 70
References ..................................................................................................... 72
List of abbreviations
AS Apgar score AOR Adjusted odds ratio BD Base deficit BE Base excess BMI Body mass index CO2 Carbon dioxide CI Confidence interval CS Caesarean section CTG Cardiotocography CP Cerebral palsy FBS Fetal scalp blood sampling TH Therapeutic hypothermia HIE Hypoxic ischemic encephalopathy HCO3 Bicarbonate H+ Hydrogen ions ICD International Classification of Diseases IQR Interquartile range LSD Least significant difference MBR Swedish Medical Birth Register NICU Neonatal intensive care unit O2 Oxygen ODFD Operative delivery for fetal distress OR Odds ratio SD Standard deviation SNQ Swedish Neonatal Quality Register SPSS Statistical Package for Social Science UA Umbilical artery VE Vacuum extraction WHO World Health Organization

Preface
For midwives and obstetricians working in delivery wards, fetal surveillance is a substantial part of the daily workload. Every obstetrician knows what it means to follow and to have the responsibility for an abnormal cardiotocogra-phy, and when non-reassuring fetal scalp blood sampling is performed to en-sure fetal well-being. Our task is to continuously perform timely interventions for those fetuses and women in need, with the knowledge that an intervention performed too late or not at all may endanger the infant’s life and health. At the same time, an overly liberal attitude to interventions can lead to iatrogenic morbidity of mother and child. When an obstetric emergency occurs, my col-leges and I work in teams with good timing, clear communication, profes-sional behaviour, and, in most instances, our effort results in positive out-comes for mother and child.
Many of us have experienced the unpleasant feeling of delivering a baby who is flaccid and blue, but who, after some time, suddenly starts screaming and regains its colours. Many thoughts pass through our minds at such a mo-ment, and we are grateful that everything went well. Some of us may experi-ence an even worse scenario, when the baby doesn’t regain a vigorous state, and in those cases we will not know the outcome. In these situations, we wish we could go back in time, and we wonder if we could have done something to prevent the adverse outcome. Knowledge of clinical recommendations and risk factors is important to enable preventive strategies to decrease neonatal risk and to avoid adverse outcomes. Uppsala, February, 2018 Lena Liljeström

11
Introduction
In Sweden, the birth rate has increased steadily during the 2000s, with approx-imately 120 000 births per year in 2016.1 Physicians and midwives in labour units in Sweden are well educated, and hospitals are modern and well equipped. Neonatal deaths during the first 28 days of life have decreased in Sweden from 7.9 per 1000 in 1973 to 1.5 per 1000 births in 2016.1 Nevertheless, a number of infants are still born with severe asphyxia in Sweden every year.2 Population-based studies from Sweden report that intrapartal asphyxia is likely the cause of cerebral palsy (CP) in 28-45% of term infants,3,4 and neonatal deaths due to intrapartal asphyxia are estimated at 0.3–0.5 per 1000 births.5,6 Severe asphyxia may cause lifelong impairment or death, and therefore birth asphyxia needs to be prevented.5,7-9
Cardiotocography (CTG) was introduced in the 1960s with the aim of im-proving intrapartum fetal surveillance and thereby neonatal outcomes.10 The CTG is the main method for intrapartum monitoring and has high sensitivity, but poor specificity, for adverse outcome.10,11 This means that a normal CTG usually indicates reassuring fetal status, while a non-reassuring CTG does not necessarily equate with fetal distress.
As a complement to CTG, to identify fetuses that are truly compromised in labour, fetal scalp blood sampling (FBS) for pH estimation was introduced shortly after the introduction of CTG in the 1960s.12 Methods for measurement of fetal scalp lactate were introduced in the 1970s, aiming to provide further information on fetal acid-base status during labour.13,14
The Apgar score and umbilical arterial (UA) blood gas analysis are two im-portant tools used to evaluate the condition of the neonate immediately after birth.15,16
Hypoxic ischemic encephalopathy (HIE) describes the clinical manifestation of disordered brain function that is caused by severe peripartum asphyxia.9,17 Knowledge of risk factors for HIE is of great importance in preventive strate-gies, and thereby in decreasing neonatal mortality and life-long morbidity.

12
Management of pregnancy and labour in Sweden In Sweden, prenatal care and delivery care are free of charge, and pregnant women’s participation in the standardised prenatal care programme starting in early pregnancy is almost 100%. Ninety-seven percent of all pregnant women have a routine ultrasound examination at 16 to 18 postmenstrual weeks to de-termine gestational age.18
Normal deliveries are independently managed by midwives; when a delivery is defined as abnormal or complicated, responsibility for the patient is trans-ferred to the obstetrician. Obstetricians, or residents in obstetrics and gynaecol-ogy, are available day and night in delivery units, although the availability of neonatologists and/or paediatricians varies across units and regions of Swe-den.19
According to Swedish standards, an admission test with CTG for at least 20 minutes is routinely performed when the woman enters the delivery ward. Thereafter, low-risk pregnancies in labour are monitored with intermittent CTG repeated every 2–3 hours, with auscultation of fetal heart rate in between. If complications arises during labour, such as abnormal CTG, maternal fever, or need for oxytocin use, a transition to continuous CTG is routine.19 High-risk pregnancies (e.g., preeclampsia, hypertension, suspicion of fetal growth re-striction) are continuously monitored with CTG during labour. All labour units employing CTG monitoring have access to FBS facilities.20
Today, epidural analgesia (EDA) and inhalation of nitrous oxide are the most commonly used methods for pain relief during delivery in Sweden. During vag-inal deliveries, inhalation of nitrous oxide was used in 81% of all deliveries, and EDA was used in in 53% of nulliparous and 22% of parous women in 2016.1 During the 2000s, the use of transvaginal pudendal nerve block remained rela-tively constant, at a level of 3–4%. Paracervical anaesthesia has lost its popu-larity and was used in less than 1% of all deliveries during the last decade.1
There has been a rise in the caesarean section rate during the last three dec-ades, from 5% of all deliveries in the 1970s to a basically unchanged proportion of 17% in the last few years, whereof, in 2016, 8.7% were elective and 7.6% were emergency caesarean sections.1 The proportion of vaginal instrumental deliveries has decreased, with approximately 7% women delivered by vacuum extraction or forceps in 2016.1
After delivery, routine UA blood gas sampling is recommended in all deliv-eries, although some units perform only selective sampling among nonvigorous infants.19,21 The argument for routine sampling is to give an opportunity to ob-jectively measure the degree of hypoxia and to evaluate quality of intrapartum care.22

13
Intrapartum fetal surveillance The aim of fetal surveillance during labour is to prevent and diagnose hypoxia to timely deliver the fetus before the onset of severe hypoxia, which could lead to neonatal and long-term impairment, such as HIE, CP, or fetal death. Until the 1960s, auscultation of the fetal heart rate with Pinard’s stethoscope and inspec-tion of amniotic fluid were the only ways to assess fetal well-being during la-bour. Since then, improved antenatal and intrapartum fetal surveillance have contributed to the decreased rate of fetal deaths in labour and of hypoxia-related intrapartum fetal deaths.23
Cardiotocography (CTG), FBS for pH and/or lactate, fetal pulse oximetry, and fetal electrocardiography have been proposed as monitoring tools in labour. In clinical practice, CTG is generally used, although access to this technology varies across the world. FBS and fetal electrocardiography are used to a lesser extent, and fetal pulse oximetry not at all.10,20,24-26
Cardiotocography Modern intrapartum fetal surveillance is often based on fetal heart rate moni-toring by CTG. Cardiotocography records the changes in the fetal heart rate and their temporal relationship to uterine contractions. External monitoring of the fetal heart is achieved with a fetal stethoscope or by an ultrasound transducer placed on the mother’s abdomen over the region of the fetal heart. Once the amniotic membranes have ruptured, it is also possible to monitor the fetal heart rate with an electrode attached to the fetal scalp. The CTG can be classified as normal/reassuring, abnormal/non-reassuring, or pathological. The classification is based on the fetal heart rate, its variability, and presence of accelerations or decelerations and uterine contractions.10,27
A normal CTG pattern is a reassurance of a well oxygenated fetus and de-mands no specific action. However, a non-reassuring/abnormal CTG pattern occurs in up to 50% of all recordings in labour, and requires clinical actions, such as change in maternal position, improved maternal hydration, decrease or stop of oxytocin infusion, evaluation with FBS, or delivery interventions, alt-hough only a small proportion of these fetuses are at risk of hypoxia.11,24,27
One benefit of CTG is the high sensitivity for detecting fetal hypoxia during labour.10 The method also gives insight into the mechanism causing hypoxia, allowing more specific action. The simultaneous monitoring of uterine contrac-tions provides information about the strain the fetus is exposed to.28
Shortcomings with the CTG is its low specificity for the outcomes used as markers of exposure to hypoxia during labour: metabolic acidosis (UA pH < 7.00 and base deficit [BD] >12 mmol/L), HIE, and neurological impairment.10 Further, there is marked inter- and intra-observer variation in CTG interpreta-tions by midwifes and obstetricians.29,30 The high rate of false positive record-

14
ings may result in inappropriately increased and potentially unnecessary opera-tive interventions due to suspicion of non-reassuring fetal status.10,31 In a sys-tematic review of randomized trials published in 2017, intrapartum surveillance with continuous CTG decreased the rates of neonatal seizures, but not of CP, in comparison with intermittent auscultation. In the same study, continuous CTG surveillance was shown to increase the rates of caesarean and instrumental de-liveries.10 The high rate of false positive CTG recordings means that adjuvant tests are needed to identify babies that are truly compromised and need to be delivered.10,24 In clinical practice, FBS with assessment of pH or lactate is such a test.20
Fetal response to hypoxia—acid-base physiology The fetus depends on the mother for placental exchange of oxygen (O2) and carbon dioxide (CO2). This exchange, in turn, relies on adequate maternal blood gas concentrations, uterine blood supply, placental transfer, and fetal gas transport.
During contractions, placental blood flow and gas exchange decrease tem-porarily. Any factor that affects placental blood flow and gas exchange impacts fetal blood gases, resulting in an accumulation of CO2 (hypercapnia) and short-age of O2 (hypoxemia). The former state causes a respiratory acidosis, and the latter a metabolic acidosis.32 If the oxygen supply is restricted, the normal fetus has several compensatory mechanisms to maintain its intracellular energy pro-duction. The fetal circulatory system can respond with increased heart rate to increase cardiac output,33 and the blood flow can be redirected to vital organs such as the heart, brain, and adrenals.34
The healthy fetus is able to adjust to short episodes of hypoxemia and to maintain an aerobic metabolism in which glucose (or glycogen) is metabolized to pyruvate and oxidized to water and CO2.32 In a sustained severe hypoxic sit-uation, despite the compensatory mechanisms, adequate oxygen supply to the tissues is not maintained, and much less efficient anaerobic metabolism ensues. In anaerobic metabolism, glucose and glycogen are metabolized to pyruvate and lactate. The accumulation of pyruvate and lactate results in an increase in hy-drogen ions [H+]. A stable concentration of free [H+] in tissues is of utmost im-portance for cellular function, and all organisms have buffering systems to maintain concentration within physiologic ranges. Free [H+] ions are buffered with haemoglobin in the blood, as well as protein and bicarbonate in the tissues. When these buffers are saturated, free [H+] ions increase, and there is a decrease in pH with metabolic acidosis.32 Generally, situations that create a metabolic acidosis also cause a respiratory acidosis (mixed acidosis).32,35
The degree of metabolic acidosis is given as an estimate of the base deficit (BD) in the extracellular space, base excess (BE), or increase of lactate. When BE is negative, that is, there is a lack of buffer base due to metabolic acidosis, it is more convenient to use the term base deficit (BD).32

15
Animal studies have shown that lactate increases quickly during hypoxia but falls relatively slowly.36 The pH value decreases more slowly in the same situ-ation but recovers quicker than lactate due to the buffering capacity of [H+] in tissue and blood.37 If anaerobe metabolism continues too long, the pH will de-crease to levels that result in in cellular death, tissue damage, organ system fail-ure, and, ultimately, fetal death.32
Fetal scalp blood sampling In 1962, Bretscher and Saling introduced a technique for blood sampling of the fetal scalp.38,39 Collection in glass capillary tubes of a small blood sample from the scalp for determination of pH values has since been regarded the gold stand-ard adjuvant test to identify hypoxia during labour.38 Lactate has been studied in fetal blood samples since the 1970s, and the sampling technique is the same as for pH.13,14
Most guidelines on fetal surveillance during labour recommend that delivery units employing CTG monitoring should have access to FBS facilities.24,40,41 The current recommendation is based on evidence suggesting that the use of FBS, as a complement to CTG, reduces the frequency of operative delivery, without increasing the proportion of neonates born with acidemia.10,11,31,42-44
A national survey sent to all delivery units in Sweden in 2008 showed that 61% of delivery units measured lactate alone, 28% used lactate and pH (com-bined test), and 11% measured only pH when analysing FBS.20 Of those units using only pH or both methods, only 61% (11/18) analysed a full acid-base bal-ance.20 The current policies at the different delivery units are unknown.
However, the role of FBS in intrapartum fetal surveillance has been ques-tioned, and its use and maintenance varies widely internationally. The propor-tion of obstetric units using FBS was 88% in The Netherlands in 2010 and 36% in Ireland in 2004.45-48 In Germany, FBS is performed in 26% of deliveries with abnormal CTG traces, and its use was less than 2% of corresponding deliveries in the USA.42,45,49 In countries where the method is uniformly implemented, FBS is performed in 7–25% of deliveries.20,25,26,50-54
There are several possible reasons why FBS is not more widely used. The analysis of FBS requires trained personnel, appropriate equipment, and labora-tory resources. Opponents of FBS question whether the scalp capillary bed is representative of the fetal circulation, because the self-regulated redistribution of oxygenated blood from peripheral to central organs which causes peripheral ischemia. By its nature, FBS can only give intermittent information about fetal acid-base status, and with a persistently abnormal CTG, it must be repeated. A study evaluating repeated FBS during labour reported that infants born after ≥ 3 FBS tests during delivery had no increase in neonatal complications compared with infants born after 1–2 FBS during labour. However, the frequency of cae-sarean section was doubled when the CTG abnormalities lead to ≥ 3 compared with 1–2 FBS tests. Furthermore, it was also pointed out that, in the group with

16
repetitive FBS tests during labour, the majority delivered vaginally (58%), and a third of those spontaneously.55
In the literature, FBS is often claimed to be uncomfortable, painful, and even intrusive for the woman in labour,56,57 difficult to perform, and time-consuming for the obstetrician.50-52,58 Despite the reported discomfort and difficulties, there are no studies that have evaluated how the women and obstetricians involved subjectively experience the FBS procedure.
In descriptive studies dealing with attitudes to fetal heart rate monitoring, most women have a positive view of fetal surveillance during labour and feel reassurance.59-61 Women expect that intrapartum fetal monitoring is a part of hospital routine, and they are confident that the monitoring is there to help and is an important source of information.59,62 Most women do not experience the monitoring procedure as uncomfortable.63 However, women do not consider fe-tal monitoring to be more important than the support and reassurance received from midwives.61
pH Saling et al. conducted the first studies investigating the normal range of pH in fetal blood. Through FBS during labour of 306 fetuses who were “very vigorous at birth”, they set a mean value for fetal scalp pH during the first stage of labour between 7.333 and 7.338. They noticed that pH values were quite stable during the first stage of labour, but pH decreased during late second stage. The lower limit of the normal range during labour was set as the mean minus 2 standard deviations (SDs), with the result between 7.227 and 7.196. Based on these em-pirical data, Saling suggested a pH value > 7.25 to be normal, 7.20-7.25 pre-acidotic, and < 7.20 acidotic. Repeated FBS within 20–30 minutes was recom-mended with preacidosis, and a pH value < 7.20 was suggested as a cut-off for intervention (i.e., delivery).38 These cut-offs are still used in clinical practice.24 The means and normal ranges for fetal scalp pH have been confirmed in other studies.64
One of the limitations of pH sampling is the sampling failure rate of 11–20% due to the relatively large amount of blood (30–50 µL) required for the anal-yses.50,52,65 Unless a full blood gas is achieved, analyses of pH do not discrimi-nate between respiratory and metabolic acidemia, the latter being associated with neonatal morbidity and brain damage.66-68
Temporary changes in maternal or fetal pCO2 may lead to scalp pH values that are falsely normal (i.e., maternal hyperventilation) or falsely abnormal (i.e., umbilical cord compression).69 Further, elevation of the pH value by contami-nation of alkaline amniotic fluid or air may mask a hypoxic fetus.70,71 In addi-tion, sampling at the site of caput succedaneum or contamination of meconium that contains bile acids may reduce the pH value.72,73

17
Lactate Kruger et al. retrospectively examined the predictive values of 326 simultane-ous FBS estimations of lactate and pH for Apgar scores, UA pH, and BD, as well as neonatal encephalopathy. Cut-off values for intervention were 4.8 mmol/L for lactate, corresponding to the 75th percentile, and 7.20 mmol/L for pH, corresponding to the 25th percentile.52 These results have been confirmed by Allen et al., who reported that fetal scalp lactate levels ≥ 4.2 mmol/L offered the best sensitivity and specificity for predicting adverse neonatal outcomes.51 Mancho et al. reported an optimal cut-off value for lactate of 4.8 mmol/L for intrapartum acidosis; this value has 100% sensitivity and 63% specificity for detection of UA pH ≤ 7.0 and BD ≥ 12 mmol/L, and it has 100% sensitivity and 64% specificity for UA pH ≤ 7.10 and BD ≥ 12 mmol/L.74
In the 1990s, a new electrochemical test strip device, originally developed for athletes was introduced into clinical practice for measuring lactate in fetal scalp blood (Lactate Pro™ Arkray, Kyoto, Japan). This device required only 5 µL of blood for analysis in 60 seconds, which led to a high success rate in ob-taining adequate samples for analysis.50,75 The Lactate Pro™ was the lactate meter used for intrapartum FBS during the study period. The suggested cut-offs were used: lactate value < 4.2 mmol/L was considered normal, 4.2–4.8 mmol/L as preacidosis, and > 4.8 mmol/L as acidosis.52 Normal lactate values in fetal scalp blood allowed labour to continue. In cases with preacidosis, a repeated FBS test was recommended within 20–30 minute intervals if abnormal CTG patterns persisted, and clinical action needed to be considered. An acidotic re-sult required intervention.52,70
An updated version, Lactate Pro 2TM, has now been launched, which needs only 0.5 µL of blood for analysis and obtains a result in 15 seconds. Comparison of different lactate meters shows good correlation between lactate values, but differences in absolute values. Therefore, the lactate cut-off values for interven-tion must be adapted for the lactate meter in use, and for the Lactate Pro 2TM other cut-off values for clinical management have been recommended.76
There is a risk for false positive test results with fetal scalp lactate values, owing to contamination with amniotic fluid if containing high levels of lactic or bile acids during sampling,71 maternal catecholamine secretion, administration of beta-mimetics (such as terbutaline or salbutamol), and maternal hyperglycae-mia caused by increased pyruvate production.69,70 In the active second stage of labour, Nordstrom et al. showed that lactate concentrations increase by about 1 mmol/L in fetuses and 2 mmol/L in mothers every 30 minutes.77 In a study by Wiberg et al. assessing lactate values during the second stage of labour in cases with reassuring CTG and 5-minute Apgar score ≥ 9, the reference interval for fetal scalp lactate during the second stage was 1.1–5.2 mmol/L (using Lactate Pro™). Further, nulliparity, use of epidural or oxytocin, and the duration of pushing time were associated with increased lactate concentration. The same

18
study found no correlation between advancing gestational age or birthweight and fetal scalp lactate values.78
In previous studies that aimed to establish the lactate cut-off level for inter-vention during labour, the first stage of labour has been referred to.51,79 Nordström et al. suggested that FBS for lactate measurement should only be used in the first stage of labour, because of the physiological increase in fetal lactate during the second stage.77 A long second stage and a longer pushing phase increase lactate values at birth, which might imply a different recom-mended cut-off value for intervention in the second stage.77,78 Yet, in clinical practice, cut-off values recommended for further evaluation or intervention in the first stage are often extrapolated to the second stage.
Theoretically, it has been speculated if the growth restricted fetus could in-crease their lactate concentrations due to reduced glycogen deposits. Holzmann et al. demonstrated that growth-restricted fetuses could respond to hypoxia ad-equately and to the same extent as appropriately grown fetuses in terms of lac-tate production, and that FBS with lactate analysis was therefore a reliable sur-veillance method for growth-restricted fetuses in labour.80 No studies evaluating lactate values obtained at the site of caput succedaneum have been published.
Lactate, pH or both? In randomized controlled trials, where pH has been compared with lactate in FBS, no differences in short-term neonatal outcome (metabolic acidosis, neo-natal encephalopathy, low Apgar scores, admission to the neonatal care unit) or mode of delivery have been reported.11,50,81 However, in the Cochrane review by East et al., it was pointed out that these studies are underpowered to asses differences in these outcomes with low prevalences.11
Holzmann et al. performed a secondary analysis of the data from the ran-domized trial by Itzel et al., and significant, although weak, correlations were reported between both fetal scalp lactate and fetal scalp pH versus UA pH (r = - 0.21 and r = 0.40, respectively, p < 0.05). Further, among 85 fetal scalp lactate measurements > 6.6 mmol/L, only 14 (16.5%) had cord pH levels < 7.10. Holzmann et al. found no differences in outcomes between the two groups, ex-cept for a more rapid delivery in the pH group.82
In the retrospective observational study by Heinis et al., scalp pH ≤ 7.20 had a sensitivity of 41% and a specificity of 86% for metabolic acidosis (pH < 7.05 and BD ≥ 12 mmol/L), and lactate values of ≥ 6.6 mmol/L indicated metabolic acidosis with a sensitivity of 71% and a specificity of 87%, and suggested that scalp lactate provides more accurate information on fetal acid-base status at birth than does pH and/or BD. Nonetheless, 29% of children who were acidotic at birth (pH < 7.05 and BD < -12) were not identified using a lactate limit of 6.6 mmol/L in the fetal scalp blood sample.54
In the retrospective study by Kruger et al. where both fetal scalp blood lactate and pH were analysed, fetal scalp blood lactate was superior to pH in predicting

19
moderate to severe HIE, with a sensitivity of 67% and a specificity of 93% for lactate, versus 49% and 77%, respectively, for pH.52
In a prospective cohort study by Ramanah et al., a scalp lactate cut-off value of 5 mmol/L had the same predictive value as scalp pH < 7.20 to predict neona-tal acidosis.83
Lactate is a final product of anaerobic metabolism and reflects hypoxia and metabolic acidosis in the tissues, and it is therefore thought to be an earlier marker than pH in identifying fetuses at risk.36,37,84 Because lactate analysis is faster and more likely to be successful due to the smaller amount of blood re-quired, lactate is considered an attractive alternative to pH analysis.11,65,81
In the randomized controlled trial by Itzel et al., the lactate group, compared with the pH group, had a significantly higher proportion of operative delivery for fetal distress (ODFD) when the test had an abnormal (preacidosis or acido-sis) value taken within 60 minutes before delivery, but there was no difference in neonatal outcome.81
In a prospective study of 677 deliveries with non-reassuring CTG, both pH and lactate were measured in the same fetal scalp blood sample, either during the first or the second stage of labour. Results showed that the sensitivity and specificity with which a high scalp lactate value (≥ 4.8) predicted a low scalp pH value (< 7.20) was low (0.63 and 0.85, respectively). Additionally, in the same study, clinical decisions were based on pH, and monitoring non-reassuring deliveries with scalp lactate instead of pH would have resulted in more (155 instead of 56) instrumental deliveries, without a decrease in the number of in-fants with severe metabolic acidosis (UA pH < 7.0 and BE < -12).53
Some studies suggest that combined measurement of FBS pH and lactate should not be recommended because it is no better in predicting abnormal neo-natal outcome than either method alone.52,85 Concern has also been raised about the possibility of an increased rate of abnormal tests with combined compared with single testing, resulting in an increased rate of operative interventions.20,81 However, several factors other than hypoxia might have an effect on both FBS lactate and pH values, potentially misleading the obstetrician to perform an un-necessary intervention. Operative delivery (i.e., caesarean section or vacuum extraction) based on results from tests such as FBS is an important outcome to evaluate, because such interventions have immediate and considerable long-term effects on mothers and neonates, as well as resource implications.86
It is not yet known whether lactate analysis could be carried out as a serial monitoring procedure in conjunction with other acid-base parameters to provide more information regarding trends during labour. In response to hypoxia, lactate has been seen to increase earlier than the drop in pH, owing to the buffer capac-ity in blood and tissue, and is regarded as an earlier marker of hypoxia.37 Lactate is slowly cleared from fetal circulation; a high lactate concentration can there-fore be measured some time after transient fetal hypoxia, whereas the pH value will probably be normalized more quickly.36 Importantly, if lactate values con-tinue to rise upon repeated sampling, the ability of the fetus to compensate for
20
acidosis could gradually become depleted, with the impending risk of an acido-sis that develops quickly.70
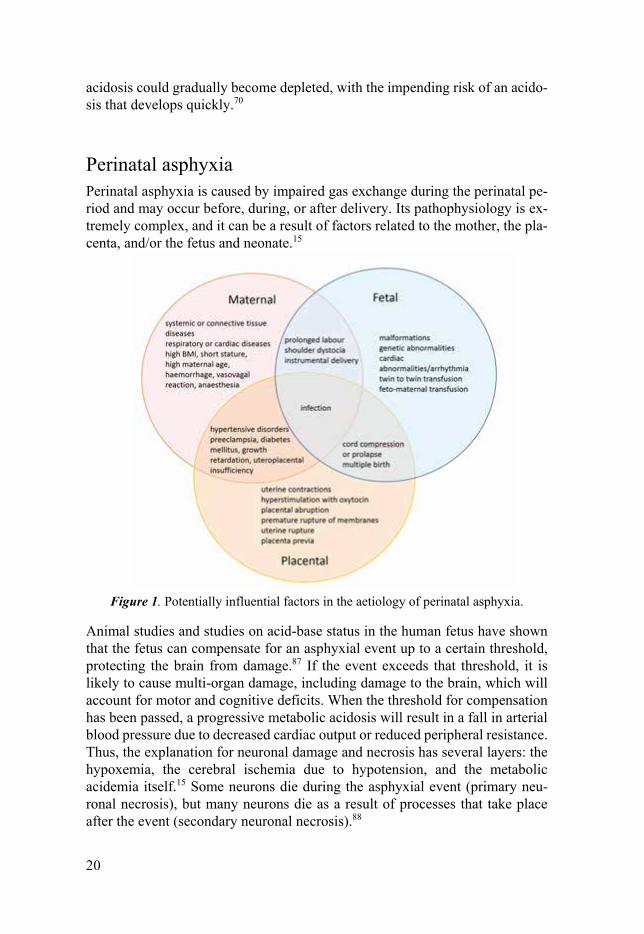
Perinatal asphyxia Perinatal asphyxia is caused by impaired gas exchange during the perinatal pe-riod and may occur before, during, or after delivery. Its pathophysiology is ex-tremely complex, and it can be a result of factors related to the mother, the pla-centa, and/or the fetus and neonate.15
Figure 1. Potentially influential factors in the aetiology of perinatal asphyxia.
Animal studies and studies on acid-base status in the human fetus have shown that the fetus can compensate for an asphyxial event up to a certain threshold, protecting the brain from damage.87 If the event exceeds that threshold, it is likely to cause multi-organ damage, including damage to the brain, which will account for motor and cognitive deficits. When the threshold for compensation has been passed, a progressive metabolic acidosis will result in a fall in arterial blood pressure due to decreased cardiac output or reduced peripheral resistance. Thus, the explanation for neuronal damage and necrosis has several layers: the hypoxemia, the cerebral ischemia due to hypotension, and the metabolic acidemia itself.15 Some neurons die during the asphyxial event (primary neu-ronal necrosis), but many neurons die as a result of processes that take place after the event (secondary neuronal necrosis).88

21
The term birth asphyxia is defined as metabolic acidosis measured at birth, with UA pH < 7.00 and BD ≥ 12 mmol/L, which is associated with neonatal morbid-ity.15,67,89 However, the definition of metabolic acidosis varies among studies, and studies evaluating the quality of obstetric management often use a definition of pH < 7.05 and/or BD ≥ 12.89,90 Thus, a diagnosis of birth asphyxia requires a blood gas for acid-base assessment.15 With the criteria UA pH < 7.00 and BD ≥ 12 mmol/L, birth asphyxia occurs in 3–4 per 1000 deliveries.67,89,91 In Sweden, the incidence of birth asphyxia is estimated to be 1.8–5.4 per 1000 live born infants, and neonatal deaths due to intrapartal asphyxia are estimated at 0.3–0.5 per 1000 term births, or approximately 1 in 2000 deliveries.5,6
Neonates born with severe asphyxia are at risk of suffering from HIE, a syn-drome of central nervous system symptomatology presenting in term and near-term infants.8,9 Neonatal deaths and infants with CP due to intrapartum asphyxia are recruited from the group of neonates born with metabolic acidosis, which also suffers from moderate to severe HIE.92
Although neonatal seizures, other neurologic morbidities, and death are sig-nificantly more common in neonates born with metabolic acidosis, the majority (77%) have an Apgar score ≥ 7 at 5 minutes, and blood gases are corrected quickly after delivery.90,93 Further, nearly two-thirds of neonates born with met-abolic acidosis do not need resuscitative efforts or admission to a neonatal in-tensive care unit (NICU), and they have no apparent neurologic sequele.89,90,93
Neonatal outcome measures In Sweden, the neonatal mortality rate is 1.5 per 1000 live births, the frequency of CP is approximately 1–2 per 1000 live births, and the estimated incidence of neonatal encephalopathy (all grades) is 1.8. per 1000 live births.1,5,94
Since neonatal encephalopathy, CP, and perinatal death are rare outcomes, intermediate measures that occur more often are commonly used, although these measures have lower sensitivity, specificity, and predictive value for serious adverse outcomes.11,17,89 Examples of such measures are different degrees of UA acidemia or metabolic acidosis, low Apgar scores (< 7 or 4 at 5 minutes), NICU admissions, and neonatal seizures.
Low Apgar scores do not indicate the cause of the poor condition and may be associated with many different factors, of which intrapartum hypoxia is one.16,17,95 In a Swedish study of 183 term infants, the majority of Apgar scores < 4 at 5 minutes, and at least half of scores < 7 at 5 minutes could be attributed to birth asphyxia in the absence of malformations.16
Neonatal seizures frequently signal an underlying brain disorder such as in-tracranial haemorrhage, infarction, infection, hypoglycaemia, cerebral malfor-mations, or metabolic disturbances, of which hypoxic-ischemic injury is the most common cause.96
However, Apgar scores, NICU admission, and presence of seizures are per se poor predictors of subsequent neurological morbidity or death.97

22
Hypoxic ischemic encephalopathy Neonatal encephalopathy (NE) is a broadly clinically defined syndrome of dis-turbed neurologic function presenting in term and near-term infants.9,98 The ae-tiology of NE is varied and covers ante-, intra-, and postpartum events, such as infection, inflammation, fetal genetic or metabolic conditions, and birth as-phyxia.9,99-101 In cases with NE, seizures occur in 40–60%, and NE is the single most common underlying cause of CP.102
Hypoxic ischemic encephalopathy is a subgroup of NE and refers to neonatal encephalopathy caused by severe peripartum asphyxia.8,9,17 The incidence of HIE varies across countries and studies depending on the definition of HIE and on study populations.9,89 In population-based studies, the incidence ranges from 1.3 to 1.7 per 1000 live births.9,103
Based on severity of clinical findings, HIE is classified as mild, moderate, or severe, according to classification of Levene, Sarnat and Sarnat (Table 1).104,105
Table 1. Hypoxic ischemic encephalopathy (HIE). Classification modified from Sarnat and Sarnat (1976).
Symptoms Mild HIE Moderate HIE Severe HIE Level of consciousness Hyperalert Lethargic Stuporous Muscle tone Normal Mild hypotonia Flaccid Complex reflexes Suck Normal/weak Weak/absent Absent Moro Strong Weak/incomplete Absent Seizures Absent Common Frequent/difficult
to control
This classification of HIE has been found to be valuable in long-term prognosis, far better than many other variables (e.g., Apgar and acid-base values). The out-come for infants with mild HIE is consistently positive, whereas moderate and severe HIE are associated with serious consequences, including death, cerebral palsy, epilepsy, and cognitive disability. The most severe cases usually die or survive with major handicap.7,17,106 Among cases with HIE in the Swedish pop-ulation, approximately 50% are classified as mild, and 50% as moderate or se-vere.103
HIE is a minor contributor to CP, whereas antenatal causes are more com-mon.3,89 Nevertheless, population-based studies from Sweden report that birth asphyxia is likely the cause of CP in 28–45% of term infants.3,4
Risk factors for HIE Because pathophysiology and aetiology differ between NE and HIE, it is essen-tial that these conditions are studied separately, since prevention strategies may be completely different. There are several known risk factors for NE, 9,17,99-101

23
whereas risk factors for the HIE subgroup are poorly studied. Since HIE is con-sidered more preventable, knowledge of risk factors for this subgroup could re-duce neonatal mortality and life-long morbidity.107
Despite differences in diagnostic criteria and study populations, antepartum and intrapartum risk factors for HIE have been described in previous studies.9,99-
101,103,108-110 Previous population-based studies suggest that antepartum events are the main factors contributing to HIE.9,100 However, these studies have used a broad definition of encephalopathy; and have included infants with genetic, congenital, and developmental abnormalities; and have provided no infor-mation on acid-base status. With no objective evidence on birth asphyxia, as described above, a diagnosis of HIE may not be justified.100,101 Recent hospital-based and case-control studies that used stricter definitions of HIE have stated that intrapartum events are the main contributing factors in the causal pathway of HIE.107-110
A number of antepartum risk factors for NE/HIE have been demonstrated, such as maternal age, maternal obesity, unemployment, lack of private health insurance, a family history of seizures, thyroid disease, infertility treatment, par-ity, history of a previous caesarean, diabetes mellitus, preeclampsia, and intra-uterine growth retardation.99,100,103,108-110
Maternal overweight and obesity is a risk factor for adverse pregnancy and neonatal outcomes. Hypertensive disorders, including preeclampsia, gesta-tional diabetes, preterm delivery, malformations, macrosomia, and stillbirth are all outcomes associated with overweight or obesity.111-119 Labour complications associated with high maternal body mass index (BMI) include post-term deliv-eries, prolonged labour, and shoulder dystocia.118,120,121
An increased risk of birth asphyxia–related complications is reported in in-fants born to women who are overweight compared with those who have normal weight.122-125 A BMI ≥ 40 was associated with an increased risk of HIE in a recent study by Nelson et al.108
Short mothers have higher incidence of cephalopelvic disproportion, labour dystocia, caesarean sections, and adverse neonatal outcomes, including low Ap-gar scores and asphyxia.125-130 In a case control study from Scandinavia, short stature (< 156 cm) was associated with intrauterine asphyxia and Apgar score < 8 at 5 minutes, particularly in vaginally born infants.127 In a population-based study of 159 210 births, maternal height < 155 cm was associated with Apgar < 7 at 1, but not at 5, minutes.131 In a Swedish study, the risk of severe asphyxia was more than doubled among infants born to short mothers (≤ 159 cm) com-pared with infants born to tall mothers (≥ 170 cm).126 Data are conflicting in the few studies on encephalopathy that have addressed the impact of maternal height.99,100
Intrapartum factors associated with HIE include premature rupture of mem-branes, meconium-stained amniotic fluid, oligohydramnios, maternal pyrexia, chorioamnionitis, induced labour, length of labour, a non-cephalic fetal presen-
24
tation, multiple birth, mode of delivery, gestational age, large head circumfer-ence, and birthweight.101,103,108-110,132 However, obstetric emergencies, including placental abruption, eclampsia, umbilical cord prolapse, uterine rupture, and shoulder dystocia, are the most prominent intrapartum risk factors for HIE.103,108,109
The aetiology of these feared events is considered multifactorial. Several risk markers for placental abruption have been reported, with smoking, hypertensive disorders, and history of previous abruption being the strongest factors.133 Mul-tiple risk factors have been documented for eclampsia, including family history, nulliparity, egg donation, diabetes, and obesity.134 Additionally, risk factors for cord prolapse include multiparty, nonvertex presentation, multiple birth, prem-aturity, and polyhydramnios.135 Uterine rupture is associated with maternal age ≥ 35 years, height ≤ 160 cm, a previous caesarean, induction of labour, mal-presentation, second-stage dystocia, use of epidural analgesia, and macro-somia.136-138 Factors predisposing for shoulder dystocia include macrosomia, maternal diabetes mellitus, post-term pregnancy, maternal obesity, labour ar-rest, and assisted operative delivery.139-141
Despite reports of predisposing factors for these obstetric emergencies, they are unpredictable, and they are associated with significantly increased risk of low Apgar score at 1 and 5 minutes, severe birth asphyxia, HIE, CP, and peri-natal mortality.93,103,108,109,136,142,143
Therapeutic hypothermia In Sweden, induced hypothermia treatment has been available for infants diag-nosed with moderate to severe HIE in the last decade.8 This therapy is proven to be neuroprotective and to reduce infant morbidity and mortality in HIE cases.8 Treatment is given by induced reduction of body temperature to 33.5–34.5 °C for 72 hours, and treatment should be started within 6 hours after birth.
Strict criteria are used to exclude other causes of neonatal encephalopathy, apart from birth asphyxia, that not will benefit from hypothermia treatment. The indication for therapeutic hypothermia is based on standardized clinical diag-nostic criteria; thus, it serves well as a surrogate variable for moderate to severe HIE.

25
Infants with gestational age at or beyond 36 weeks fulfilling at least one of the A criteria and one of the B criteria are qualified for therapeutic hypothermia.144
At least one of following A-criteria; asphyxia based on: Apgar score ≤ 5 at 10 minutes, assisted ventilation initiated at birth and continued for at least 10
minutes, pH ≤ 7.0 in umbilical artery blood or any postnatal blood sample
within 1 hour of age or base exess ≥ 16 in umbilical artery blood or any postnatal blood sam-
ple within 1 hour of age.
And B-criteria; seizures or signs of moderate to severe neonatal encephalopathy based on:
affected level of consciousness (lethargy, stupor, or coma), affected tone (hypotonic, flaccid), or affected primitive reflexes (weak to absent suck or moro).
During the years 2011 to 2015, 0.68 per 1000 live born infants received thera-peutic hypothermia in Sweden.145
26
Aims
The general aim of this thesis was to study birth asphyxia, with an emphasis on evaluating combined FBS pH and lactate analysis and the experience of the pro-cedure, and on identifying risk factors for moderate to severe neonatal HIE.
The specific aims of the separate studies were:
I The primary aim was to evaluate the rate of discrepancy between pH
and lactate values in combined tests of fetal scalp blood sampling. The
secondary aim was to evaluate differences in obstetric management in
response to combined tests (pH and lactate) and single tests (pH or lac-
tate).
II To assess women’s experience of pain during the FBS procedure and
the obstetricians’ experience of how difficult the test was to perform.
III To identify antepartum risk factors for neonatal HIE, with a focus on
maternal BMI and height.
IV To investigate the risk of neonatal HIE by obstetric emergencies, and to
explore the distribution of obstetric emergencies by parity in cases of
HIE.
27
Materials and Methods
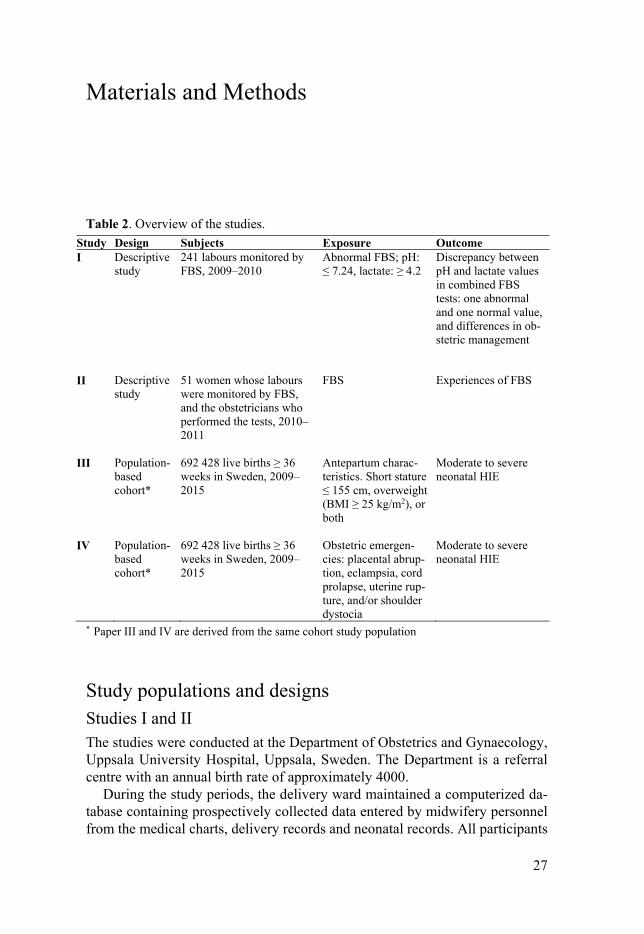
Table 2. Overview of the studies. Study Design Subjects Exposure Outcome I Descriptive
study 241 labours monitored by FBS, 2009–2010
Abnormal FBS; pH: ≤ 7.24, lactate: ≥ 4.2
Discrepancy between pH and lactate values in combined FBS tests: one abnormal and one normal value, and differences in ob-stetric management
II Descriptive study
51 women whose labours were monitored by FBS, and the obstetricians who performed the tests, 2010–2011
FBS Experiences of FBS
III Population-based cohort*
692 428 live births ≥ 36 weeks in Sweden, 2009–2015
Antepartum charac-teristics. Short stature ≤ 155 cm, overweight (BMI ≥ 25 kg/m2), or both
Moderate to severe neonatal HIE
IV Population-based cohort*
692 428 live births ≥ 36 weeks in Sweden, 2009–2015
Obstetric emergen-cies: placental abrup-tion, eclampsia, cord prolapse, uterine rup-ture, and/or shoulder dystocia
Moderate to severe neonatal HIE
* Paper III and IV are derived from the same cohort study population
Study populations and designs Studies I and II The studies were conducted at the Department of Obstetrics and Gynaecology, Uppsala University Hospital, Uppsala, Sweden. The Department is a referral centre with an annual birth rate of approximately 4000.
During the study periods, the delivery ward maintained a computerized da-tabase containing prospectively collected data entered by midwifery personnel from the medical charts, delivery records and neonatal records. All participants

28
were women who underwent FBS during labour. Information about pregnancy, labour, delivery, and the neonate were collected from medical records.
Study I This study included all live-born, singleton pregnancies ≥ 34 weeks of gesta-tional age, monitored by FBS during labour from May, 2009, to April, 2010 (n = 241). During the study period, the assistant nurses registered all FBS to ensure that no samples were missed.
Study II Between May, 2010, and March, 2011, women whose labour was monitored by FBS and the obstetricians who performed the FBS tests were asked to partici-pate in the study (n = 51). The women included were Swedish speaking, had singleton pregnancies, a gestational length of 34 weeks or more, and were ex-posed to FBS during labour.
Studies III and IV A population-based cohort of 692 428 live-born infants at gestational weeks 36 or beyond in Sweden between January, 2009, and December, 2015. By using the individual’s national identification number, allocated to every individual at birth, we linked data from the Swedish Medical Birth Register (MBR) and the Swedish Neonatal Quality Register (SNQ).146
Because the southern health care region did not start to register data in the SNQ until 1 January, 2011, all births in this region (n = 34 302) were excluded for the years 2009–2010. Infants with congenital malformations, chromosome abnormalities, and births before 36 weeks of gestation were excluded.
Methods Study I Fetal scalp blood samples from 241 labours were analysed. According to the departmental guidelines, the following pH and lactate values indicated abnor-mality: pH: < 7.20 acidosis; 7.20–7.24 preacidosis; and > 7.24 normal. Lactate (mmol/L): > 4.8 acidosis; 4.2–4.8 preacidosis; and < 4.2 normal.
Lactate was analysed with an electrochemical single-use strip method (Lactate Pro™, Arkray, Kyoto, Japan). The equipment consists of a small battery-charged meter and disposable strips. This method requires 5 µL of whole blood, and the results can be read on a display after 60 seconds. The pH and acid bal-
29
ance were analysed with an acid-base meter (ABL 800 Flex Radiometer, Co-penhagen, Denmark). This method requires 35 µL of blood for a capillary pH determination, and the device is readily available at the delivery ward. Quality controls are performed daily, and the meters are regularly checked in accord-ance with the manufacturer’s recommendations.
In cases of discrepancy, the clinical situation was evaluated and required continuous surveillance and re-evaluation with repeated FBS.
During the study period, the success rate of UA blood samples was 88%. Metabolic acidosis was defined as UA pH < 7.05 and BD ≥ 12 mmol/L.
Exposures
The FBS results were stratified according to whether the test was normal or abnormal (pre-acidosis or acidosis) and according to whether a combined (pH and lactate) or single analysis (pH or lactate) was performed. If several FBS tests were performed on the same fetus, only the last was used in the statistical analysis.
Outcomes
The main outcome variable was the rate of discrepancy between pH and lactate values in the combined tests. Discrepancy in the combined tests (pH and lactate) was defined as one test having a normal value whereas the other was abnormal (preacidosis or acidosis).
Differences in the frequency of operative delivery for fetal distress (ODFD) and the time intervals from FBS to delivery were calculated when combined or single tests were compared. The mean UA pH upon delivery and the frequency of UA pH < 7.15 was compared between the FBS test groups.
Study II Women who underwent FBS testing and the obstetricians performing the test were asked to complete questionnaires regarding their experiences of FBS.
The women answered the questionnaire within 48 hours after delivery, for their experience of the first FBS, regardless of the number of tests performed. Obstetricians answered the questionnaire anonymously immediately after sam-pling. If more than one test was performed on the same woman, obstetricians completed just one questionnaire, after the first test.
The questionnaires consisted of questions to be answered on a 10-point scale (1 = do not agree at all, 10 = totally agree).
To assess whether the study sample was representative of the total population exposed to FBS during the study period, obstetric variables from a local data-base containing prospectively collected data on all deliveries were retrieved for

30
comparison. These variables were parity, gestational length, and use of epidural anaesthesia.
Exposures The women were asked to complete a questionnaire regarding their experiences of:
1. pain during the sampling procedure,
2. information received about the test,
3. understanding of why the test was performed,
4. anxiety due to the sampling procedure,
5. reassurance due to the test being performed,
6. duration of the test procedure, and
7. overall satisfaction that the test was performed.
The obstetricians performing the FBS tests were asked to complete a question-naire regarding their experiences of:
1. difficulty in performing the test,
2. duration of the test procedure, and
3. patient cooperation during the testing procedure.
Obstetricians who completed the questionnaire were asked to state cervical di-latation and station of the fetal head in relation to the spine (above or below) at the time of sampling. The actual duration of the test procedure was not meas-ured, and the recorded variables reflected the women’s and obstetricians’ sub-jective experience of the time spent. Maternal BMI was categorized according to the World Health Organization’s (WHO’s) definition of normal (< 25 kg/m2) or overweight (≥ 25 kg/m2).113 Gestational length and cervical dilatation were dichotomized into less than, equal to, or above the mean for the study popula-tion.
Outcomes The main outcome variables were the women’s and obstetricians’ experiences of the FBS, as assessed by the questionnaires.
31
Studies III and IV Data sources The Swedish MBR was founded in 1973 and provides information about ma-ternal demographics, reproductive history, and complications during preg-nancy, delivery, and the neonatal period. The register, maintained by the Centre for Epidemiology (EpC) at the Swedish National Board of Health and Welfare, is well validated and covers more than 98% of all births in Sweden.147,148 It is compulsory for every health care provider to report to the register, and the in-formation available is collected from medical records from prenatal care, deliv-ery, and neonatal care. The quality of data is considered to be high.147
Information on maternal characteristics, such as weight, height, and smoking habits, medical history, and obstetric history is collected with an interview dur-ing the first antenatal visit, which usually takes place at the end of the first tri-mester. Information on the mother, as wells as on the pregnancy, delivery, and neonatal period, is prospectively recorded on standardized forms that are for-warded to the registry after the mother and infant are discharged from the hos-pital.148 After delivery, the responsible doctor records each woman’s diseases and complications during pregnancy and delivery, according to the Swedish version of the International Classification of Diseases (ICD), and the diagnostic codes (ICD codes) are forwarded to the MBR.
The SNQ started in 2001, has gradually grown, and all 37 Swedish neonatal units have been included since 1 January, 2011. The register holds prospectively collected perinatal data, including therapeutic hypothermia on all new-born in-fants admitted to one of the neonatal units in Sweden.145
Exposures for studies III and IV All exposure variables were obtained from the MBR. Information on maternal, pregnancy, labour, and neonatal data were retrieved from standardised check-boxes and diagnosis according to ICD-10 codes.
Onset of delivery was defined as prelabour caesarean, spontaneous labour, or induced labour. Mode of delivery was defined as prelabour caesarean, emer-gency caesarean, operative vaginal, or spontaneous vaginal. Hypertensive disorders included women with chronic (O10, I10-15) and gesta-tional (O13, O16) hypertension, preeclampsia (O11, O14), and/or eclampsia (O15). Diabetes mellitus encompassed women with pre- (O240-O243) or ges-tational (O244) diabetes mellitus.
Specific exposures for Study III: Maternal height was categorized into 155 cm or less, 156–160 cm, 161–172 cm, or 172 cm or more. Short maternal stature was defined as 155 cm or less, and non-short was defined as 156 cm or more.
Maternal weight measured in early pregnancy, and self-reported height was used to calculate BMI (kg/m2), which was then categorized according to the

32
WHO’s classification: underweight (BMI < 18.5); normal weight (BMI 18.5–24.9), overweight (BMI 25.0–29.9), or obese (obesity class I: BMI 30–34.9, class II: BMI 35.0–39.9, and class III: BMI ≥ 40, respectively). Normal weight was defined as BMI less than 25 kg/m2 and overweight as BMI 25 kg/m2 or more.
Further, women were categorized as only short, only overweight, or both short and overweight, using non-short and normal weight as references.
Specific exposures for Study IV: The main exposures were obstetric emergen-cies and included women with placental abruption (O45), eclampsia (O15), um-bilical cord prolapse (O690), uterine rupture (O710, O711), and/or shoulder dystocia (O660), identified by diagnostic ICD-10 codes.
Outcome The outcome in studies III and IV was moderate to severe neonatal HIE, whereof therapeutic hypothermia served as a surrogate variable.144
The SNQ register provided information on all infants who received hypother-mia treatment during the study period, retrieved from checkboxes in NICU rec-ords.
Statistics For statistical analysis of data, the IBM Statistical Package for Social Sciences for Windows versions 20.0–24.0 was used (SPSS, Inc., Chicago, IL, USA). A p value < 0.05 was considered to indicate a statistically significant difference.
Study I Data are presented as number of observations (n) and means with standard de-viation (SD). The chi squared test was used to compare group distributions (di-chotomous variables). The t test (compare means between groups) or the Mann-Whitney U test (nonparametric comparisons of categorical and continuous var-iables) was used to compare continuous variables. One-way analysis of variance (ANOVA) with Fisher’s least significant difference (LSD) post-hoc test was used to compare multiple means.
Study II Data are presented as means with SD or medians with interquartile range (IQR). The Mann-Whitney U test was used to compare continuous variables. Spear-man’s correlation (r) was used to analyse correlations between continuous var-iables.

33
Studies III and IV Data are presented as numbers of observations (n), frequencies (%), means with SD, and rates per 1000 live births. Logistic regression was used to assess the associations between ante- and intrapartum covariates and moderate to severe neonatal HIE, presented as crude and adjusted odds ratios (ORs and AORs) with 95% confidence intervals (CIs). We did not adjust for mode of delivery, reason-ing that operative deliveries could represent actions due to suspicion of fetal distress, leading to confounding by indication. No imputation for missing data was performed.
Study III The risk of HIE by maternal, pregnancy, and infant characteristics was esti-mated with crude OR. Thereafter, the OR was adjusted for covariates potentially associated with the outcome HIE in the present and/or previous reports;99-
101,103,108,110,126 these included maternal characteristics (parity, maternal age, height, BMI, cohabitation, country of birth, smoking in early pregnancy, thyroid disease, infertility treatment, hypertensive disorders, diabetes mellitus during pregnancy) and labour and infant characteristics (onset of delivery, gestational age, fetal presentation, infant birthweight, sex, year, and region of birth).
We also calculated the effect on odds for HIE per cm decrease in height and per unit increase in BMI, using BMI and height as continuous variables in the model and adjusting for the other categorical variables.
The risk of HIE by maternal habitus (categorized into only short, only over-weight, and both short and overweight, with non-short and normal weight as reference) was adjusted for the same covariates (except for BMI and height), in two successive models: maternal characteristics (Model 1) and labour and infant characteristics (Model 2).
The risk of HIE by maternal habitus was thereafter stratified by mode of de-livery and adjusted for all variables in Models 1 and 2.
We also stratified by parity, using the same covariates for adjustments. Parity was categorized into nulliparous and parous. Parous women were further sub-grouped into those with or without a previous caesarean delivery.
Study IV The risk of HIE by any obstetric emergency was presented as ORs, with deliv-eries without any obstetric emergency used as reference.
The risk of HIE by each obstetric emergency was presented as ORs and AORs, and deliveries without the corresponding obstetric emergency were used as reference. Covariates for adjustments were calculated with the use of Di-rected Acyclic Graphs (DAG) for each obstetric emergency (accessible on the DAGitty website by the URL presented in the list below), and the confounders included for adjustments for each emergency are presented as follows:

34
Placental abruption: parity, maternal age, cohabitation, country of birth, smoking in early pregnancy, hypertensive disorders, and multiple birth (dagitty.net/mYx3xR_).
Eclampsia: parity, maternal age, height, early pregnancy BMI, cohabita-tion, country of birth, smoking in early pregnancy, chronic hypertension, diabetes mellitus, gestational age, infant birthweight, and multiple birth (dagitty.net/mNO7JKW).
Cord prolapse: parity, induction of labour, gestational age, fetal presenta-tion, premature rupture of membranes, and multiple birth (dagitty.net/mnTf2h4).
Uterine rupture: parity, previous caesarean section, maternal age, height, early pregnancy BMI, induction of labour, gestational age, labour dystocia, fetal presentation, and infant birthweight (dagitty.net/mjVZWS_).
Shoulder dystocia: parity, maternal height, early pregnancy BMI, diabetes mellitus, gestational age, labour dystocia, fetal presentation, and infant birthweight (dagitty.net/mzOaKkY).
The analyses regarding the risk of HIE by cord prolapse and uterine rupture were restricted to labours with a vaginal onset, whereas the risk of HIE by shoul-der dystocia was restricted to vaginal deliveries.
Risks were estimated separately in nulliparous, and parous women with or with-out a previous caesarean.
Ethical considerations All studies were conducted following approved ethical guidelines in compliance with the Helsinki Declaration. In studies I and II, oral and written information was given, and informed written consent was obtained from all included partic-ipants. All clinical data were anonymously saved and coded prior to analysis. In studies III and IV, applications for register linkages were sent to the relevant Swedish authorities, and researchers did not at any time have direct access to personal identity numbers. Therefore, informed consent by each person in-volved was not needed. Each study was approved by the Regional Ethics com-mittee at the Medical Faculty, Uppsala University, Sweden (2010/003, 2011/236, 2015/156).

35
Results
Study I During the 12-month study period, there were 4215 infants born at the depart-ment. The caesarean section rate was 18%, and the vacuum extraction rate 7%. In all births, the mean UA pH was 7.26 ± 0.07, the frequency of UA pH < 7.15 was 6%, and 0.1% had metabolic acidosis. Of the attempted vaginal deliveries, 241 of 3685 (7%) were monitored by FBS, forming the study population.
Table 3. Obstetric outcome variables of the study population.
n = 241 % Gestational age (weeks ± days) a 40 ± 2 - Induction of labour 66 27 Oxytocin use 201 83 Post-term pregnancy (≥ 42 weeks) 35 15 Labour dystocia 148 64 Meconium stained amniotic fluid 98 41 Scalp sampling, 1st stage 147 61 Scalp sampling, 2nd stage 94 39 Combined sample (pH and lactate) 153 63 Single sample, pH 12 5 Single sample, lactate 76 32 Operative delivery b 151 63 ODFD c 88 37 Umbilical artery pH a 7.21 ± 0.08 -
a Values are given as n (%) or Mean ± SD b Caesarean section or vacuum extraction c Operative delivery for fetal distress
There were 177 (73%) nulliparous women in the study population, and UA sam-pling was documented in 186 of 241 (77%). The type of test performed (com-bined or single) did not differ between the different stages of labour.
Among the entire study group with abnormal tests, lactate was more fre-quently abnormal than were pH values. The lactate value accounted for 63% of the abnormal tests in the first stage of labour, and pH for 37%. In the second stage, lactate accounted for 79% of the abnormalities and pH for 21%.
In the combined tests, the lactate values were more often abnormal than were the pH values: 51 of 153 (33%) versus 39 of 153 (25%), respectively, (p < 0.001).

36
The proportion of ODFD did not differ between the combined and single tests, 54 of 153 (35%) versus 34 of 88 (39%), when the entire study group was considered.
Figure 2 displays the distribution of test results. Within the combined tests with any abnormality, the rate of discrepancy (i.e., pH was normal when lactate was abnormal or vice versa) was 55%.
Among the combined tests with abnormality, the lactate value was more of-ten abnormal (86%) than was the pH value (64%), p < 0.05. Among the com-bined tests, 62 of 153 (40%) had at least one abnormal value, and 20 of 88 (23%) of the single tests were abnormal (p = 0.005).
The frequency of ODFD was significantly lower after a combined test than after a single test: 41 of 62 (66%) versus 19 of 20 (95%), respectively (p < 0.05).
ODFD was performed in 23 of 28 cases (82%) where both pH and lactate were abnormal and in 18 of 34 cases (53%) where there was one abnormal value (p = 0.03). There was a difference in the frequency of ODFD between the com-bined tests with one abnormality and a single abnormal test: 18 of 34 (53%) versus 19 of 20 (95%), respectively (p = 0.002).
Figure 2. The distribution of test results in the study group. Rates of operative deliver-ies for fetal distress (ODFD) in relation to sample type in patients with abnormal tests
and rate of discrepancy within combined tests.

37
Table 4 shows the mean scalp pH and lactate values, and the UA results. In the combined tests, the mean scalp pH values were significantly lower when there were two abnormal results compared with one abnormal result, whereas the mean scalp lactate values showed significant differences between all groups; single or combined test (p <0.05). There was no difference in mean UA pH or pH < 7.15 between the groups with abnormal test results.
Table 4. Mean scalp pH and lactate values and umbilical artery pH results in relation to sample type.
Values are given as mean ± SD or n (%). pH > 7.24 normal; pH < 7.24 abnormal; lactate < 4.2 normal; lactate > 4.2 abnormal. a p < 0.05 compared with normal samples; b p < 0.05 compared with both pH and lactate abnormal; c p < 0.05 compared with one of pH or lactate abnormal; d p < 0.05 compared with single sample abnormal
In Table 5, the frequency of ODFD and the time intervals from the last FBS to delivery are displayed. When restricted to the samples showing an abnormality, the time interval was longer after combined tests with one abnormal result com-pared with combined tests with two abnormal results: 75 versus 37 minutes (p = 0.045), with a tendency for a longer time interval to delivery with an ab-normal lactate value compared with an abnormal pH value: 70 versus 47 minutes (p = 0.06; not shown in table). Furthermore, there was a tendency to-ward a longer time interval after a combined test with one abnormal test com-pared with after an abnormal single test result: 75 versus 36 minutes (p = 0.051).
Fetal Blood Sample n = 241 Last
scalp pH Last
scalp lactate UA pH
UA pH < 7.15
Normal test 159 7.32 ± 0.04b, c, d 2.56 ± 0.74b, c, d 7.23 ± 0.07 b, d 19 (12)
Combined test: pH and lactate abnormal
28 7.18 ± 0.06a, c 6.57 ± 1.95a, c, d 7.18 ± 0.09a 9 (32)a
Combined test: one of pH or lactate abnormal
34 7.27 ± 0.07a, b, d 4.87 ± 1.78a, b, d 7.21 ± 0.08 5 (15)
Single test: abnormal 20 7.16 ± 0.04a, c 5.71 ± 1.57a, b, c 7.18 ± 0.08a 7 (35 a

38
Table 5. Operative deliveries for fetal distress (ODFD) and time intervals from fetal blood sampling (FBS) to ODFD in relation to sample type.
Fetal Blood Sample n ODFD
n (%) Minutes from FBS to ODFD
Normal test 159 28 (18) 114 ± 89 b, c, d Combined test: pH and lactate abnormal
28 23 (82) 37 ± 25 a, c
Combined test: one of pH or lactate abnormal
34 18 (53) b 75 ± 57 a, b
Single test: abnormal 20 19 (95) c 36 ± 21 a Values are given as mean ± SD or n (%). pH > 7.24 normal; pH < 7.24 abnormal; lactate < 4.2 normal; lactate > 4.2 abnormal. a p < 0.05 compared with normal samples; b p < 0.05 compared with both pH and lactate abnormal; c p < 0.05 compared with one of pH or lactate abnormal; d p < 0.05 compared with single sample abnormal.
In our study population, no infants were born with metabolic acidosis. The fre-quencies of UA pH < 7.15 and Apgar score < 7 at 5 minutes were 40 of 241 (17%) and 8 of 241 (3%), respectively.
Study II During the study period, 3393 infants were born after attempted vaginal deliv-ery, and 266 (8%) were monitored with FBS during labour.
Table 6. Maternal and obstetric characteristics of the study population.
Values are given as n (%) or mean ± SD a In early pregnancy. b Information retrieved from the partogram; duration of labour was calculated from a dilation of 3 cm until delivery. c Caesarean section or vacuum extraction.
Study population (n = 51)
Maternal characteristics Maternal age (years) 30 ± 5 Body mass index (kg/m²) a 26 ± 5 Nulliparous 39 (77)
Obstetric characteristics Gestational length (weeks ± days) 40 ± 2 Induction of labour 18 (35) Epidural anaesthesia at sampling 38 (75) Cervical dilation at sampling (cm) 7 ± 2 Station of fetal head at sampling
Above the spine 37 (73) Below the spine 13 (26) Missing 1 (2)
Total duration of labour (hours) b 9 ± 3 Operative delivery c 29 (57)

39
There were no complete FBS failures. Sampling was mostly performed by the resident obstetrician (71%), otherwise by a specialist (27%). In one question-naire, there is no information about whether the obstetrician was a resident or a specialist in obstetrics and gynaecology. There were no differences between the study population and the total population exposed to FBS with regard to parity, gestational length, or use of epidural analgesia. No woman or obstetrician de-clined to participate in the study.
In Figure 3, the women’s questionnaire results are presented as medians with interquartile ranges. The women’s experience of pain during the sampling pro-cedure had a median of 3.5. The experience of information received about the test and understanding why the test was performed had a median of 10.0. The experience of time taken to perform the test had a median of 3.0, and overall satisfaction that the test had been performed a median of 10.0.
1 2 3 4 5 6 7 8 9 10
Information
Understanding
Pain
Anxiety
Reassurance
Duration of thetest procedure
Overall satisfaction
Figure 3. Women’s experiences of FBS.
In Figure 4, the obstetrician’s questionnaire results are presented as medians with interquartile ranges. The obstetrician’s experience of difficulty in perform-ing the test, time taken for the testing procedure, and patient cooperation during the testing procedure had medians of 3.0, 2.0, and 10.0, respectively.
Figure 4. Obstetrician’s experiences of FBS.

40
Table 7 illustrates the correlations between the women’s and the obstetricians’ experiences of FBS. The women’s experience of pain during the sampling pro-cedure correlated with their experience of longer duration of the test procedure (p < 0.001). The obstetricians’ experience of difficulty in performing the test correlated with the women’s experience of pain (p < 0.05) and with the obste-tricians’ experience of longer duration of the test procedure (p < 0.001).
Table 7. Correlations between women’s and obstetricians’ experiences of fetal scalp blood sampling.
Women’s experience of
pain
Obstetricians’ experience of
difficulty
Spearman rank correlation coefficients
Women’s experience of Pain during the sampling procedure - 0.31* Information received about the test -0.24 -0.02 Understanding why the test was performed -0.10 0.05 Anxiety due to the sampling procedure 0.04 0.02 Reassurance due to the fact that the test was performed -0.04 0.03 Duration of the test procedure 0.50*** 0.20 Overall satisfaction that the test was performed -0.18 0.10 Obstetricians’ experience of Difficulty in performing the test
0.31*
-
Duration of the test procedure 0.32* 0.62*** Patient cooperation during the testing procedure –0.32* –0.13
*p < 0.05, **p < 0.01, ***p < 0.001
Table 8 displays women’s experience of pain during the sampling procedure and the obstetricians’ experience of difficulty in performing the test in relation to maternal and obstetric characteristics. Women with a high BMI experienced more pain compared with those with a low BMI (7.0 vs. 2.0; p = 0.001). Women without epidural analgesia experienced the testing procedure as more painful compared with women with epidural analgesia (7.0 vs. 3.0; p = 0.02). Sampling at a cervical dilation < 7 cm was associated with higher ratings of pain compared with sampling at cervical dilation ≥ 7 cm (7.0 vs. 3.0; p = 0.03). Obstetricians experienced the testing procedure as more difficult when the cervical dilation was < 7 cm compared with ≥ 7 cm (5.0 vs. 1.0; p = 0.002), as well as when the station of the fetal head was above compared to below the ischial spine (3.0 vs. 1.0; p = 0.02).
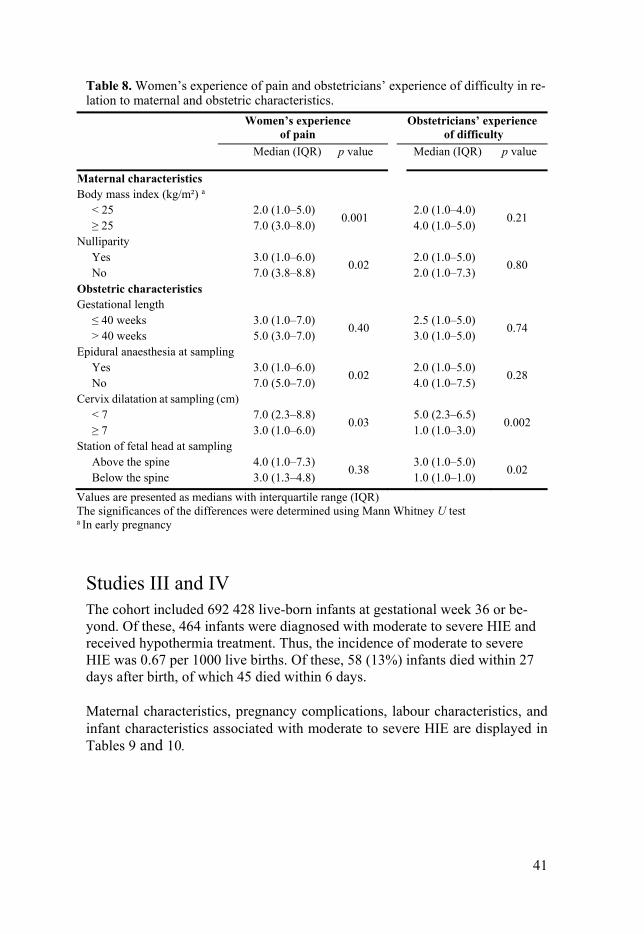
41
Table 8. Women’s experience of pain and obstetricians’ experience of difficulty in re-lation to maternal and obstetric characteristics.
Women’s experience of pain
Obstetricians’ experience of difficulty
Median (IQR) p value Median (IQR) p value
Maternal characteristics Body mass index (kg/m²) a < 25 2.0 (1.0–5.0)
0.001 2.0 (1.0–4.0)
0.21 ≥ 25 7.0 (3.0–8.0) 4.0 (1.0–5.0) Nulliparity Yes 3.0 (1.0–6.0)
0.02 2.0 (1.0–5.0)
0.80 No 7.0 (3.8–8.8) 2.0 (1.0–7.3) Obstetric characteristics Gestational length ≤ 40 weeks 3.0 (1.0–7.0)
0.40 2.5 (1.0–5.0)
0.74 > 40 weeks 5.0 (3.0–7.0) 3.0 (1.0–5.0) Epidural anaesthesia at sampling Yes 3.0 (1.0–6.0)
0.02 2.0 (1.0–5.0)
0.28 No 7.0 (5.0–7.0) 4.0 (1.0–7.5) Cervix dilatation at sampling (cm) < 7 7.0 (2.3–8.8)
0.03 5.0 (2.3–6.5)
0.002 ≥ 7 3.0 (1.0–6.0) 1.0 (1.0–3.0) Station of fetal head at sampling Above the spine 4.0 (1.0–7.3)
0.38 3.0 (1.0–5.0)
0.02 Below the spine 3.0 (1.3–4.8) 1.0 (1.0–1.0)
Values are presented as medians with interquartile range (IQR) The significances of the differences were determined using Mann Whitney U test a In early pregnancy
Studies III and IV The cohort included 692 428 live-born infants at gestational week 36 or be-yond. Of these, 464 infants were diagnosed with moderate to severe HIE and received hypothermia treatment. Thus, the incidence of moderate to severe HIE was 0.67 per 1000 live births. Of these, 58 (13%) infants died within 27 days after birth, of which 45 died within 6 days.
Maternal characteristics, pregnancy complications, labour characteristics, and infant characteristics associated with moderate to severe HIE are displayed in Tables 9 and 10.

42
Table 9. Maternal characteristics and pregnancy complications associated with mod-erate to severe hypoxic ischemic encephalopathy (HIE).
a Adjusted for parity, maternal age, height, early pregnancy BMI, cohabitation, country of birth, smoking in early pregnancy, thyroid disease, infertility treatment, hypertensive disorders, diabe-tes during pregnancy, onset of delivery, gestational age, fetal presentation, infant birthweight, sex, year and region of birth. b At least one previous caesarean section, restricted to parous women. c Chronic hypertension, gestational hypertension, preeclampsia, or eclampsia. d Pregestational or gestational diabetes.
n (%)
Moderate to severe HIE
n (%) Rate /1000
Odds ratio (95% confidence interval)
Crude Adjusted a Total population 692 428 464 0.67 Parity 0 298 345 (43.08) 249 (53.66) 0.83 1.53 (1.28–1.84) 1.87 (1.47–2.39) ≥ 1 394 083 (56.91) 215 (46.34) 0.55 reference reference Previous caesarean b 70 724 (17.95) 81 (37.67) 1.15 2.77 (2.10–3.65) 2.46 (1.68–3.60)
Maternal age (years) ≤ 20 17 636 (2.55) 8 (1.72) 0.45 0.70 (0.35–1.41) 0.59 (0.24–1.45) 21–34 521 565 (75.32) 338 (72.84) 0.65 reference reference ≥ 35 153 224 (22.13) 118 (25.43) 0.77 1.19 (0.96–1.47) 1.30 (0.99–1.71) Missing 3 (0.00) 0 (0) Maternal height (cm)
≤ 155 32 886 (4.75) 37 (7.97) 1.13 1.76 (1.25–2.48) 1.62 (1.05–2.52) 156–160 100 432 (14.5) 100 (21.55) 1.00 1.55 (1.24–1.96) 1.44 (1.08–1.93) 161–172 421 365 (60.85) 270 (58.19) 0.64 reference reference > 172 112 540 (16.25) 44 (9.48) 0.39 0.61 (0.44–0.84) 0.56 (0.38–0.83) Missing 25 205 (3.64) 13 (2.80) 0.52 Early pregnancy BMI (kg/m²)
< 18.5 16 354 (2.36) 5 (1.08) 0.31 0.64 (0.26–1.56) 0.77 (0.28–2.08) 18.5–24.9 382 459 (55.23) 182 (39.22) 0.48 reference reference 25–29.9 169 846 (24.53) 149 (32.11) 0.88 1.84 (1.49–2.29) 1.68 (1.30–2.19) 30–34.9 58 576 (8.46) 69 (14.87) 1.18 2.48 (1.88–3.27) 2.08 (1.47–2.92) 35–39.9 18 353 (2.65) 27 (5.82) 1.47 3.10 (2.07–4.64) 1.74 (0.97–3.11) > 40 6 451 (0.93) 14 (3.02) 2.17 4.57 (2.65–7.87) 2.56 (1.18–5.55) Missing 40 389 (5.83) 18 (3.88) 0.45 Hypertensive disorders c
29 530 (4.26) 43 (9.27) 1.46 2.30 (1.68–3.14) 1.44 (0.94–2.21)
Diabetes d 11 190 (1.62) 13 (2.80) 1.16 1.76 (1.01–3.05) 1.27 (0.64–2.51)
Onset of delivery
Spontaneous 529 314 (76.44) 304 (65.52) 0.57 reference reference Induction 103 059 (14.88) 113 (24.35) 1.10 1.91 (1.54–2.37) 1.31 (0.98–1.77)
Prelabour caesarean
57 843 (8.35) 45 (9.70) 0.78 1.36 (1.00–1.85) 1.03 (0.65–1.63)
Missing 2 207 (0.32) 2 (0.43) 0.91

43
Table 10. Labour and infant characteristics associated with moderate to severe HIE.
a Adjusted for parity, maternal age, height, early pregnancy BMI, cohabitation, country of birth, smoking in early pregnancy, thyroid disease, infertility treatment, hypertensive disorders, diabe-tes during pregnancy, onset of delivery, gestational age, fetal presentation, infant birthweight, sex, year and region of birth. b Fetal-pelvic disproportion. c All other presentations.
Nulliparity, previous caesarean, short stature, high BMI, fetal-pelvic dispropor-tion, multiple birth, gestational age of 36 weeks, late and post-term delivery, occiput posterior position, and birthweight > 4000 grams were all associated with moderate to severe HIE.
n (%)
Moderate to severe HIE
n (%) Rate
/1000
Odds ratio (95% confidence interval)
Crude Adjusted a Labour dystocia 80 007 (11.55) 99 (21.34) 1.24 2.08 (1.66-2.59) 1.32 (0.98-1.78) Disproportion b 51 129 (7.38) 110 (23.71) 2.15 3.90 (3.15-4.84) 4.23 (3.13-5.71) Multiple birth 14 077 (2.03) 16 (3.45) 1.14 1.72 (1.05-2.84) 2.09 (1.11-3.94) Gestational age 36 15 410 (2.23) 22 (4.74) 1.43 2.75 (1.78-4.25) 2.67 (1.56–4.58) 37–40 500 526 (72.29) 260 (56.03) 0.52 reference reference 41 (late term) 128 433 (18.55) 118 (25.43) 0.92 1.77 (1.42-2.20) 1.68 (1.26–2.23) ≥42 (post term) 48 059 (6.94) 64 (13.79) 1.33 2.57 (1.95-3.37) 2.01 (1.38–2.93) Fetal presentation Occiput anterior 612 360 (88.44) 318 (68.53) 0.52 reference reference Occiput posterior 30 814 (4.45) 33 (7.11) 1.07 2.06 (1.44-2.95) 1.80 (1.19-2.73) Breech 20 118 (2.91) 12 (2.59) 0.60 1.15 (0.64-2.04) 1.28 (0.64-2.56) Other c 13 049 (1.88) 31 (6.68) 2.38 4.58 (3.17-6.63) 4.28 (2.79-5.56) Missing 16 017 (2.31) 70 (15.09) 4.37 Birthweight (grams) <3000 83 988 (12.13) 66 (14.22) 0.79 1.61 (1.23-2.12) 1.29 (0.90-1.85) 3000–4000 478 192 (69.06) 233 (50.22) 0.49 reference reference >4000 129 508 (18.70) 118 (25.43) 0.91 1.87 (1.50-2.34) 1.77 (1.35-2.32) Missing 740 (0.11) 47 (10.13) 63.5 Sex Male 353 529 (51.06) 249 (53.66) 0.70 reference reference Female 338 898 (48.94) 215 (46.34) 0.63 0.90 (0.75-1.08) 0.93 (0.74–1.17) Missing 1 (0.0) 0 (0)

44
Study III In the population, 32 886 (5%) women were categorized as short (≤ 155 cm) and 253 226 (37%) as overweight or obese (BMI ≥ 25).
We found a dose-response association between HIE and decreasing maternal height, as well as increasing BMI. The risk of moderate to severe HIE decreased by 4.7% (95% CI 3.0–6.5) per cm of increased maternal height and increased 5.2% (95% CI 3.1–7.4%) per BMI unit (not shown in table).
Compared to the reference, women with short stature (≤ 155 cm) had a 62% increased risk of having an infant with HIE, and women with obesity (BMI ≥ 30) had a twofold risk increase (Table 9).
The odds ratios for HIE by maternal habitus are displayed in Figure 5. Com-pared with non-short women with normal weight, overweight women had an increased risk of HIE (AOR 1.88; 95% CI 1.48–2.40), and that risk was even more pronounced in women who were both short and overweight (AOR 2.83; CI 1.62–4.92). Further, the rate of HIE was highest in short and overweight women (not shown in figure).
Non-short is defined as 156 cm or more, and short as 155 cm or less. Normal weight is defined as a BMI less than 25 kg/m2 and overweight as a BMI 25 kg/m2 or more. Non-short and normal weight were used as references. Model 1 is adjusted for parity, maternal age, cohabitation, country of birth, smoking in early pregnancy, thyroid disease, infertility treatment, hypertensive disorders, and diabetes during preg-nancy. Model 2 is adjusted by the same variables as model 1, and additionally for onset of deliv-ery, gestational age, fetal presentation, infant birthweight, sex, year and region of birth.
Figure 5. Odds ratio for moderate to severe hypoxic ischemic encephalopathy (HIE) by maternal height and BMI.
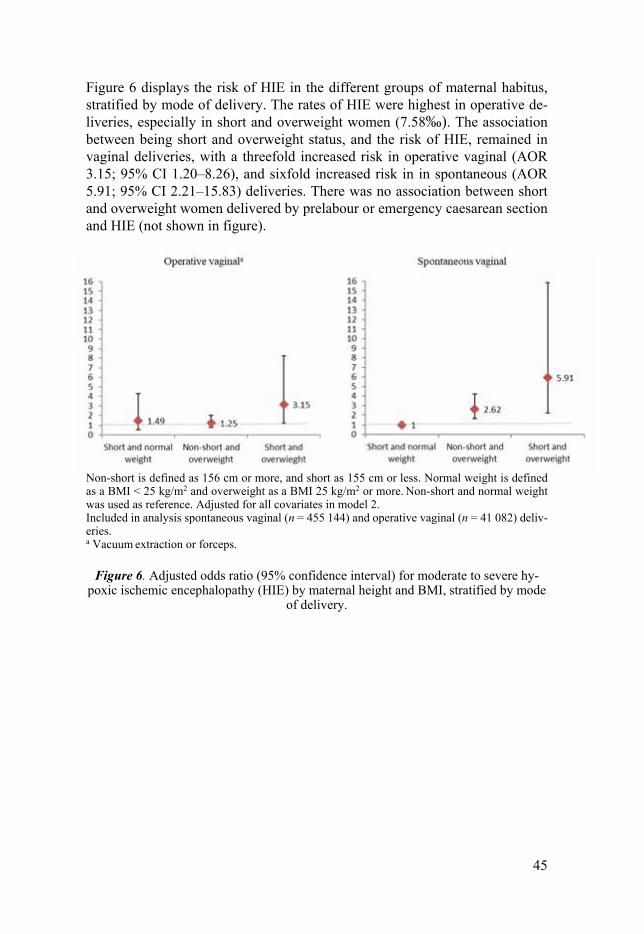
45
Figure 6 displays the risk of HIE in the different groups of maternal habitus, stratified by mode of delivery. The rates of HIE were highest in operative de-liveries, especially in short and overweight women (7.58‰). The association between being short and overweight status, and the risk of HIE, remained in vaginal deliveries, with a threefold increased risk in operative vaginal (AOR 3.15; 95% CI 1.20–8.26), and sixfold increased risk in in spontaneous (AOR 5.91; 95% CI 2.21–15.83) deliveries. There was no association between short and overweight women delivered by prelabour or emergency caesarean section and HIE (not shown in figure).
Non-short is defined as 156 cm or more, and short as 155 cm or less. Normal weight is defined as a BMI < 25 kg/m2 and overweight as a BMI 25 kg/m2 or more. Non-short and normal weight was used as reference. Adjusted for all covariates in model 2. Included in analysis spontaneous vaginal (n = 455 144) and operative vaginal (n = 41 082) deliv-eries. a Vacuum extraction or forceps.
Figure 6. Adjusted odds ratio (95% confidence interval) for moderate to severe hy-poxic ischemic encephalopathy (HIE) by maternal height and BMI, stratified by mode
of delivery.

46
Figure 7 displays the risk of HIE in the different groups of maternal habitus, stratified by parity. The rate was higher in nulliparous women in all categories of maternal habitus (0.64–1.28 ‰), except in short and overweight women, where the rate was higher in parous women (1.84‰). We found an association to HIE in both nulliparous and parous overweight women. Parous women who were both short and overweight had an increased risk of having an infant with HIE (AOR 4.49; 95% CI 2.17–9.27). In the subgroup analysis based on his-tory of previous caesarean, short and overweight parous women without a his-tory of previous caesarean had the highest risk (AOR 4.99; 95% CI 1.96–12.69; not shown in figures).
Non-short is defined as 156 cm or more, and short as 155 cm or less. Normal weight is defined as a BMI < 25 kg/m2, and overweight as a BMI 25 kg/m2 or more. Non-short and normal weight were used as references. Adjusted for all covariates in model 2.
Figure 7. Adjusted odds ratio (95% confidence interval) for moderate to severe hypoxic ischemic encephalopathy (HIE) by maternal height and BMI, stratified by
parity.
Diagnoses of dystocia and fetal-pelvic disproportion were more prevalent among women with short stature (14.9% and 14.5%, respectively), compared with non-short women (11.4% and 7.0%, respectively), p < 0.001 for both. Further, fetal-pelvic disproportion was more frequent among overweight or obese women (8.9%) compared with normal weight women (6.5%), p < 0.001. There was no difference in frequency of diagnosis of dystocia in overweight or obese women (11.3%) compared with normal weight women (11.7%), p = 0.2. Not shown in table.

47
Study IV In our population, the prevalence of obstetric emergencies was 0.7%. Any ob-stetric emergency occurred in 133 of 464 (29%) among all HIE cases and was more common in parous women (80 of 215; 37%) compared with nulliparous women (53 of 249; 21%), p < 0.001. In the total population, shoulder dystocia was the most common obstetric emergency, occurring in 55 of 464 (12%) cases, with the highest risk of HIE (AOR 50.3; 95% CI 33.6–75.4; not shown in table).
Figure 8 displays the distribution of obstetric emergencies among HIE cases in the nulliparous and parous women with and without a previous caesarean de-livery.
Figure 8. The distribution of obstetric emergencies by parity among HIE cases.
In Tables 11–13, the risks of HIE by obstetric emergencies stratified by parity are outlined.
Among nulliparous women, shoulder dystocia was the most common obstet-ric emergency in HIE cases, occurring in 31 of 249 (12%) cases, and had the highest risk of HIE (AOR 48.2; 95% CI 28.2–82.6).
Among parous women, any obstetric emergency was more frequent with than without a previous caesarean (39 of 81 [48%] vs. 41 of 134 [31%]). In parous women without a previous caesarean, shoulder dystocia was the most common obstetric emergency among HIE cases (21 of 134 [16%]), but in the adjusted analysis placental abruption had the strongest association to HIE (AOR 73.8; 95% CI 40.8–133.5). In parous women with a previous caesarean delivery, uterine rupture was the most common obstetric emergency among HIE cases (31 of 81 [38%]), with the highest risk of HIE (AOR 45.6; 95% CI 24.5– 84.6).

48
Table 11. Risk of moderate to severe hypoxic ischemic encephalopathy (HIE) by ob-stetric emergencies in nulliparous women, n = 298 345.
Nulliparous
n
HIE (n = 249)
n (%) Odds Ratio
(95% confidence interval) Crude Adjusted
No obstetric emergency 296 716 196 (0.1) reference
Any obstetric emergency a 1 629 53 (3.3) 50.9 (37.4–69.2)
Obstetric emergency by diagnosis
Placental abruption b Yes 584 18 (3.1) 41.0 (25.2–66.6) 34.1 (20.3–57.3)
No 297 761 231 (0.1) reference reference
Eclampsia c Yes 233 1 (0.4) 5.2 (0.7–37.1) 5.1 (0.7–36.8)
No 298 112 248 (0.1) reference reference
Cord prolapse d, ‡ Yes 168 3 (1.8) 22.7 (7.2–71.7) 20.8 (5.6–76.7)
No 280 280 224 (0.1) reference reference
Uterine rupture e, ‡ Yes 20 1 (5.0) 65.3 (8.7–489.5) –
No 280 428 226 (0.1) reference
Shoulder dystocia f, † Yes 611 31 (5.1) 121.2 (80.6–182.1) 48.2 (28.2–82.6)
No 244 953 108 (0.0) reference reference a Placental abruption, eclampsia, cord prolapse, uterine rupture, shoulder dystocia. ‡ Restricted to deliveries with vaginal onset (n = 280 448); † Restricted to vaginal deliveries (n = 245 564). Adjustments were made for b maternal age, cohabitation, country of birth, smoking, hypertensive disorders, and multiple birth; c maternal age, height, BMI, cohabitation, country of birth, smoking, chronic hypertension, diabetes, gestational age, birthweight, and multiple birth; d induction of labour, gestational age, fetal presentation, premature rupture of membranes, and multiple birth; e maternal age, height, BMI, induction of labour, gestational age, dystocia, fetal presentation, and birthweight; and f maternal height, BMI, diabetes, gestational age, dystocia, fetal presentation, and birthweight.

49
Table 12. Risk of moderate to severe hypoxic ischemic encephalopathy (HIE) by ob-stetric emergencies in parous women without a previous caesarean, n = 323 359.
Parous without a previous caesarean
n
HIE (n = 134)
n (%) Odds Ratio
(95% confidence interval) Crude Adjusted
No obstetric emergency 321 466 93 (0.0) reference
Any obstetric emergency a 1 893 41 (2.2) 76.5 (52.8–110.8)
Obstetric emergency by diagnosis
Placental abruption b
Yes 446 14 (3.1) 87.2 (49.7–152.9) 73.8 (40.8–133.5)
No 322 913 120 (0.0) reference reference
Eclampsia c
Yes 43 0 (0) – –
No 323 316 134 (0.0)
Cord prolapse d, ‡
Yes 401 3 (0.8) 20.4 (6.4–64.4) 4.7 (1.4–16.6)
No 310 991 115 (0.0) reference reference
Uterine rupture e, ‡
Yes 51 2 (3.9) 109.5 (26.3–445.6) 21.4 (2.6–174.6)
No 331 341 116 (0.1) reference reference
Shoulder dystocia f, †
Yes 930 21 (2.3) 139.8 (83.6–233.6) 69.6 (34.4–140.8)
No 302 533 50 (0.0) reference reference a Placental abruption, eclampsia, cord prolapse, uterine rupture, shoulder dystocia. ‡ Restricted to deliveries with vaginal onset (n = 311 392); † Restricted to vaginal deliveries (n = 303 463) Adjustments were made for b maternal age, cohabitation, country of birth, smoking, hypertensive disorders, and multiple birth; c maternal age, height, BMI, cohabitation, country of birth, smoking, chronic hypertension, diabetes, gestational age, birthweight, and multiple birth; d induction of labour, gestational age, fetal presentation, premature rupture of membranes, and multiple birth; e maternal age, height, BMI, induction of labour, gestational age, dystocia, fetal presentation, and birthweight; and f maternal height, BMI, diabetes, gestational age, dystocia, fetal presentation, and birthweight.
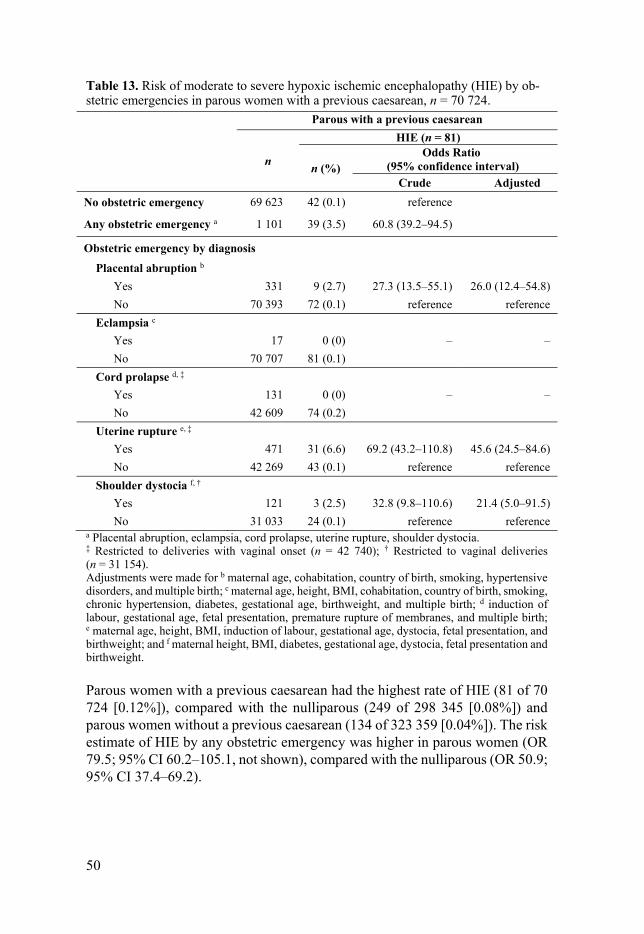
50
Table 13. Risk of moderate to severe hypoxic ischemic encephalopathy (HIE) by ob-stetric emergencies in parous women with a previous caesarean, n = 70 724.
Parous with a previous caesarean
n
HIE (n = 81)
n (%) Odds Ratio
(95% confidence interval)
Crude Adjusted
No obstetric emergency 69 623 42 (0.1) reference
Any obstetric emergency a 1 101 39 (3.5) 60.8 (39.2–94.5)
Obstetric emergency by diagnosis
Placental abruption b
Yes 331 9 (2.7) 27.3 (13.5–55.1) 26.0 (12.4–54.8)
No 70 393 72 (0.1) reference reference
Eclampsia c
Yes 17 0 (0) – –
No 70 707 81 (0.1)
Cord prolapse d, ‡
Yes 131 0 (0) – –
No 42 609 74 (0.2)
Uterine rupture e, ‡
Yes 471 31 (6.6) 69.2 (43.2–110.8) 45.6 (24.5–84.6)
No 42 269 43 (0.1) reference reference
Shoulder dystocia f, †
Yes 121 3 (2.5) 32.8 (9.8–110.6) 21.4 (5.0–91.5)
No 31 033 24 (0.1) reference reference a Placental abruption, eclampsia, cord prolapse, uterine rupture, shoulder dystocia. ‡ Restricted to deliveries with vaginal onset (n = 42 740); † Restricted to vaginal deliveries (n = 31 154). Adjustments were made for b maternal age, cohabitation, country of birth, smoking, hypertensive disorders, and multiple birth; c maternal age, height, BMI, cohabitation, country of birth, smoking, chronic hypertension, diabetes, gestational age, birthweight, and multiple birth; d induction of labour, gestational age, fetal presentation, premature rupture of membranes, and multiple birth; e maternal age, height, BMI, induction of labour, gestational age, dystocia, fetal presentation, and birthweight; and f maternal height, BMI, diabetes, gestational age, dystocia, fetal presentation and birthweight.
Parous women with a previous caesarean had the highest rate of HIE (81 of 70 724 [0.12%]), compared with the nulliparous (249 of 298 345 [0.08%]) and parous women without a previous caesarean (134 of 323 359 [0.04%]). The risk estimate of HIE by any obstetric emergency was higher in parous women (OR 79.5; 95% CI 60.2–105.1, not shown), compared with the nulliparous (OR 50.9; 95% CI 37.4–69.2).

51
In further subanalysis, differences in the maternal and infant characteristics among the different obstetric emergencies were found when they were com-pared with women without the corresponding diagnosis.
In women with placental abruption, maternal age ≥ 35 years (29%), smoking (10%), a previous caesarean (24%), hypertension disorders (9%), gestational age of 36 weeks (15%), and infant birthweight < 3000 grams (33%) were more frequent compared with women without placental abruption, (p < 0.05 for all).
Women with eclampsia were more often nulliparous (80%), short (8%), di-agnosed with diabetes mellitus (4%), induced (44%), delivered at 36 gestational weeks (10%), and had infants with birthweight < 3000 grams (32%), p < 0.001 for all).
Women with cord prolapse were more often parous (76%), overweight (54%), induced (37%), had breech presentation (12%), multiple birth (21%), and infant birthweight < 3000 grams, (p < 0.001 for all).
Of those with a uterine rupture, 87% had a previous caesarean, and the ma-jority were parous women (96%). Women with a uterus rupture were more often ≥ 35 years old (38%), short (8%), overweight (49%), induced (28%), had diag-nosis of dystocia (21%) and fetal-pelvic disproportion (48%), occiput posterior presentation (10%), infant birthweight > 4000 grams (26%), and late term de-livery (37%) compared with women without ruptured uterus, (p < 0.001 for all).
In labours complicated by shoulder dystocia, women were more often parous (63%), short (9%), overweight (50%), induced (22%), more frequently diag-nosed with diabetes mellitus (7%), dystocia (33%), had late term (39%), and vacuum extraction delivery (31%), and infant with birthweight > 4000 grams (75%) compared with women without shoulder dystocia, (p < 0.001 for all). Not shown in table.

52
Discussion
Clinical implications Study I A discrepancy between fetal scalp lactate and pH values was common in the combined test and occurred in 55% of tests with any abnormality (preacido-sis/acidosis). Obstetric management was influenced by the discrepancy, and cli-nicians seemed to act more readily on an abnormal pH value when combined tests had one abnormal test result. Combined sampling resulted in a higher pro-portion of abnormal tests; however, this study could not confirm the concern for an increased rate of operative interventions with the combined test. On the contrary, the ODFD rate was significantly lower compared with the single test.
Consistent with our findings of discrepancy between tests, O’Brian et al., who evaluated mean pH in paired FBS, demonstrated inconsistency in results. However, they reported a higher intervention rate due to the discrepancy. When one test was above the delivery threshold, a repeated sampling resulted in an instrumental vaginal delivery instead of an emergency caesarean section, which they believed would support the argument for serial measurements.149
Rorby et al., measuring lactate and pH in the same FBS (where scalp pH was used for clinical decisions, whereas the lactate value was blinded to the obste-trician), demonstrated that more instrumental deliveries would have been per-formed using scalp lactate instead of pH, and no cases of acidosis would have been missed. Additionally, the frequency of operative delivery due to fetal dis-tress was 82% in cases with both an abnormal scalp pH and lactate measure-ment, compared with 53% when only one of the parameters was abnormal.53
Fetal monitoring during labour is complex and requires knowledge of fetal physiology. Methods used should have reasonable balance between false posi-tive and false negative test results to prevent adverse neonatal outcomes while at the same time avoiding unnecessary operative deliveries. The outcomes of interest are the ability of the test to predict an adverse neonatal outcome, the success rate of the test, and interventions resulting from the test. It is important to record specific interventions such as vacuum delivery and caesarean section, since operative births are associated with immediate and long-term effects for both mother and child and have considerable resource implications.
Fetal scalp sampling should be regarded as a complement to CTG, to dis-criminate which fetuses with non-reassuring CTGs that are at risk of hypoxia.

53
It is important that the clinician consider the full clinical picture, rather than acting on a single finding, and the obstetrician should have knowledge of path-ophysiology, current evidence, and the described pitfalls. Additionally, FBS has an educational value for learning about fetal physiology and might aid in the interpretation of CTG patterns.31
FBS with lactate measurement is common in Sweden, and almost two-thirds of delivery units use lactate as a single test.20 An important clinical issue is to consider whether replacement of pH measurement with lactate measurement could result in an increase in positive tests, with a concomitant increase in in-terventions. The result from our study provides some support for such an unde-sirable effect. To establish a better understanding of the metabolic state of the fetus, we speculate that parallel analyses of both pH and lactate could provide more information on which to base the clinical decision. However, larger pro-spective studies are needed to assess the impact of obstetric management with combined FBS.
Study II We found that FBS was generally well tolerated in women who had epidural analgesia in labour and that obstetricians did not generally experience FBS as difficult to perform. Neither women nor obstetricians experienced FBS as time consuming. However, with higher maternal BMI, less cervical dilation, and higher station of the fetal head, the sampling procedure was experienced as more complicated. Thus, previous assertions and beliefs about the FBS proce-dure that can be found in the literature may be incorrect and misleading. Fur-thermore, women expressed satisfaction that the test was performed.
FBS was well tolerated by most women in our study, which may be explained by the fact that the majority had epidural analgesia during labour. The use of epidural analgesia in labour has increased over the last two decades in Sweden, as well as in other Western countries.1,150 The introduction of a bedside test strip device for measuring lactate in fetal scalp blood has added benefits: it requires less blood and fewer scalp incisions, it is quicker, and it is more likely to be successful.50 Thus, although never previously studied, the assertions of the FBS procedure being associated with discomfort and difficulties may not apply in modern obstetrics.
Compared with women with a normal BMI, overweight and obese women have higher risks of intrapartum complications, and CTG monitoring during la-bour is considered more difficult among these women.151 However, studies evaluating FBS in women with high BMI are lacking. In this study, women with high BMI reported more pain during the FBS procedure than women with nor-mal BMI. The reason may be that it is more difficult to accomplish a vaginal examination and access the fetal head with standard equipment. Obstetricians also experienced FBS to be more difficult in women with high BMI, but the difference was not significant, which might be influenced by our sample size.

54
Less cervical dilation is associated with greater difficulty in obtaining scalp blood.50 This accorded with our findings of associations between less cervical dilation, a higher station of the fetal head, and the obstetricians’ experience of difficulty in performing the test. These results suggest that sampling is expected to be more difficult in the early phase of active labour.
Women who participated in the present study reported that they had received adequate information about the test, and obstetricians perceived that women co-operated during sampling. It is possible that the high scores of overall satisfac-tions with the test were a result of adequate information given before sampling. An important factor related to childbirth satisfaction is a perception of personal control during labour.152-154 Being adequately informed regarding a medical pro-cedure is very important and gives the woman a feeling of control and the op-portunity of being involved in decision-making. This might, in turn, help an individual to experience less anxiety and facilitate coping with pain.152,155-157
The time aspect in a situation with suspected intrapartum fetal hypoxia is important, and investigations with additional methods should not cause a delay in clinical management. In one earlier study, the average time from the decision to perform a FBS to the available result was 18 minutes,58 indicating that scalp sampling can be a time-consuming procedure.
Obstetricians are faced almost daily with clinical dilemmas requiring imme-diate decision-making, as, in the course of minutes, the well-being of mother and fetus might be compromised. In such circumstances, it is of paramount im-portance for clinicians to have as much information as possible about the even-tual time an extra procedure such as FBS would take, and about factors associ-ated with a more complicated procedure, like higher BMI, absence of epidural anaesthesia, less cervical dilation, or fetal head above the spine. When such conditions apply and the obstetrician still decides that there is sufficient time for FBS, it would be appropriate to inform the labouring woman that difficulties might be faced during the sampling and that the procedure might be painful. However, it is important to point out that our study indicated that, even in cases where women experienced pain and anxiety due to the FBS procedure, they still felt reassured and satisfied that the test was performed.
Studies III and IV We found a lower incidence of HIE in our population (0.67 per 1 000 live born infants) compared with prior reports (0.9–1.7 per 1000).9,99,101,103,108,110 The higher incidences in previous reports are probably due to differences in the def-inition of HIE and different study designs and populations.9 In previous reports, the definition of HIE was broader, including cases of NE, infants with seizures only, or all grades of HIE.9,99,101,103,109,110 The prognosis and risk for permanent disabilities differs within grades of HIE.7,106 The incidence of HIE in the present study was lower than in a recent study by Nelson et al., the only study that used the same surrogate variable (hypothermia treatment) for moderate to severe

55
HIE.108 However, the study by Nelson et al. was a hospital-based study, where estimates are generally higher than in population-based studies, possibly due to referral bias.9 In accordance with our results, in a previous study from Sweden, the incidence of moderate to severe HIE was 0.67 per 1000 live births.107
In contrast to some previous studies, we found no associations between ma-ternal thyroid disease, infertility treatment, diabetes mellitus, or history of con-vulsions and HIE.99,100,108,109 Dissimilarities concerning risk factors for HIE may also be attributable to the diagnostic diversity of HIE and/or different study de-signs.9 It is clearly a challenge to correctly distinguish HIE from other entities of neonatal encephalopathy, and from seizures alone. These conditions have of-ten been used interchangeably in previous studies, limiting their generalizabil-ity.9,99,101 Additionally, risk factors are likely to vary across populations and over time because of dissimilar clinical practice and characteristics of pregnant pop-ulations. In our population, covering all Swedish woman, prenatal and delivery care is free of charge. Pregnant women’s participation in the standardised pre-natal care programme starting in early pregnancy is almost 100%, and care and medical charges are subsidized on equal terms, which may positively impact maternal morbidity and neonatal outcomes.
In line with previous studies, we found associations between HIE and nul-liparity, previous caesarean, high BMI, short stature, multiple birth, gestational age of 36 weeks, late and post-term delivery, and occiput posterior position at birth.99,100,103,108,110 Fetal-pelvic disproportion is associated with birth asphyxia and perinatal mortality.158 To the best of our knowledge, there are no prior re-ports that have addressed the impact of disproportion and HIE. We found a more than fourfold increased risk for moderate to severe HIE in infants born to moth-ers with a diagnosis of fetal-pelvic disproportion.
Low birthweight (less than 3th or 9th percentile) has been associated with an increased risk for HIE in previous studies,100,108,109 and was also associated with an increased risk for HIE in the unadjusted analysis of our results. However, after adjustments for potential confounders, this risk was no longer significant, although a birthweight > 4000 g was still significantly associated with HIE. A birthweight > 4500 g is associated with increased risk of asphyxia-related peri-natal mortality and morbidity.159 In a Swedish study of 177 infants, very large birthweight for gestational age had almost a fourfold increased risk of suffering from encephalopathy caused by asphyxia.126
Maternal overweight and obesity are associated with a wide spectrum of pregnancy and neonatal complications. Known neonatal complications include increased risk of low Apgar scores, meconium aspiration, NICU admissions, birth asphyxia, CP, and stillbirth.4,113,117-119,122-125 A BMI ≥ 40 was associated with an increased risk of HIE in the study by Nelson et al.; maternal height, however, was not considered in that study.108 We also found an increased risk for moderate to severe HIE in lower BMI classes.

56
The mechanisms involved in the adverse neonatal outcomes associated with maternal overweight and obesity are considered multifactorial. Pregnancy com-plications could result from a cascade of events, starting with having an over-weight disorder such as hypertension or diabetes mellitus during pregnancy, or with being postdate, leading to induction of labour. However, after adjusting for these covariates, the associations between maternal overweight and HIE per-sisted and remained statistically significant in our results.
Moreover, increased markers of inflammation, difficulty in estimating fetal weight, intrapartum complications such as inability to adequately monitor the fetus and contractions, and difficult labour with dystocia and fetal-pelvic dis-proportion due to increased maternal pelvic soft tissue are complications that might prevail in overweight women.4,117,121
Another consequence of high maternal BMI is fetal hyperinsulinemia and maternal diabetes mellitus, which in turn are well-known risk factors for mac-rosomia.117,160 In our study, diabetes mellitus was not associated with HIE after adjusting for potentially confounding factors such as BMI and birthweight, pos-sibly reflecting the limited number of cases. There are linear associations be-tween maternal BMI and fetal macrosomia and between maternal BMI and measures of hyperinsulinemia in cord blood,117,160 independent of maternal glu-cose values.161 Results from both experimental and clinical studies strongly sug-gest that fetal hyperinsulinemia is a risk factor for fetal hypoxia.162-164 Thus, it is possible that fetal hyperinsulinemia is of pathophysiological importance for the increased risk of birth asphyxia in pregnancies with maternal overweight.
The effects of maternal overweight on severe neonatal asphyxia may partly be explained by traumatic labour, which often results from macrosomia.4,109 Fe-tal macrosomia, often defined as birth weight > 4000 g, is the most prevalent complication in pregnancies with maternal overweight.113,117,165 Macrosomia was associated with moderate or severe HIE in our population, which contrasts with the findings by Nelson et al., who used the same outcome measure.108 This difference could possibly be due to fewer cases in that study.
Short maternal stature is considered an obstetrical risk that is not within the reach of prevention. In the study by Ellis et al. maternal height < 145 cm was associated with encephalopathy,99 whereas we found an association already at 160 cm or less for the stricter outcome, moderate to severe HIE, after adjusting for covariates. The effect of short stature on infant outcome is considered at-tributable to relation of short stature to fetal-pelvic disproportion, leading to obstructed labour.128-131,166 Obstructed labour is a risk factor for adverse neona-tal outcomes such as infection, low Apgar scores, birth asphyxia, and meconium aspiration.167,168 In our study, a diagnosis of dystocia and fetal-pelvic dispropor-tion were more prevalent in women with short stature (≤ 155 cm) compared with non-short women (≥ 156 cm). In parallel, we found that being tall (> 172 cm) was associated with a considerably reduced risk (44%) of subsequent HIE.

57
The combination short maternal height and fetal macrosomia may lead to pro-tracted labour, owing to the higher prevalence of fetal-pelvic disproportion and labour dystocia in short women, with greater prevalence of interventions and traumatic labour.127-130 We found that the combination of short maternal stature and overweight in-creased by threefold the risk of having an infant with moderate to severe HIE when compared with women with non-short stature and normal weight. The odds ratio of the combined maternal habitus for HIE was higher than that of either short stature or BMI alone, although overlapping confidence intervals be-tween groups indicate some uncertainty. The absence of a significant associa-tion between women with only short stature and having an infant with HIE might be influenced by power. When we stratified for parity, being overweight was associated to HIE in both nulliparous and parous women, whereas the com-bination of being short and overweight had an impact only in parous women, which also could be explained by power.
In the obstetric context, parity is an important variable to consider for out-comes. Regardless of the outcomes studied, nulliparity is usually a risk factor, and HIE is not an exception. However, based on our data, we would argue that parous women, especially those without a history of previous caesarean, might in fact have a risk of giving birth to an infant with HIE. Fetal-pelvic dispropor-tion and labour dystocia, as well as incautious use of oxytocin due to protracted labour, might prevail in such situations. This argument is to some extent sup-ported by the stratified analysis on mode of delivery, where the risk of HIE was pronounced in short and overweight women delivered vaginally. Furthermore, infants born to short and overweight women and delivered by caesarean section had no risk of HIE. Deliveries by emergency caesarean section had a high ab-solute risk; however, maternal habitus was not the risk factor.
Although the number of infants with HIE born to short and overweight moth-ers is low, the severity of moderate to severe HIE warrants meticulous intrapar-tum management for these women. An important task for clinicians is to choose mode of delivery after appropriate risk assessment, given all information avail-able. In general, vaginal delivery is considered safer than both prelabour and emergency caesareans, from both short and long-term perspectives.169,170 Addi-tionally, given the high prevalence of overweight in the pregnant population and the low absolute risk of HIE, primary caesarean is not warranted. However, our results indicate that, in short and overweight women, the level of effort to ac-complish a vaginal delivery needs to be carefully considered with individual risk assessment, in nulliparous as well as in parous women.
We found dose-response relationships between increasing BMI and decreas-ing maternal height and the risk of HIE. Early prevention measures for over-weight in the population could indeed be expected to positively impact neonatal outcomes, particularly in short women.

58
The prevalence of obstetric emergencies in our population (0.7%) is consistent with the results of previous studies.93,136,140 We report a higher proportion of obstetric emergencies in HIE cases (29%) compared with a recent study that used the same definition of HIE (13%),108 and compared with studies where mild HIE was also included (22%).103,109 Prior studies used different definitions of obstetric emergency; some did not include shoulder dystocia as an emer-gency,93,99 or merged different emergencies into a composite, 99,101,109 owing to small numbers of HIE cases and/or emergencies.
None of the previous studies had the opportunity to evaluate how the associ-ations between obstetric emergencies and HIE depended on parity or to take the history of caesarean into account in parous women. In HIE cases, obstetric emergencies were more common in the parous (overall 37%; 48% with and 31% without a previous caesarean) than in the nulliparous (21%) women. Among nulliparous women, shoulder dystocia was the most common obstetric emer-gency and had the strongest association to HIE. In parous women without a previous caesarean, shoulder dystocia was most common, but placental abrup-tion had the strongest association to HIE. Among women with a previous cae-sarean, uterine rupture was the most common obstetric emergency among cases of HIE (38%) and was the strongest predictor of HIE by all emergencies, with a 45 times greater risk in our study.
The relationships between maternal habitus, age, parity, previous caesarean, birthweight, and intrapartum complications such as obstetric emergencies have previously been explored.133,136,138-141 In parallel, several of the expected differ-ences regarding the maternal and infant characteristic among the different ob-stetric emergencies were found in our population.
In our study, women with shoulder dystocia were more often short and over-weight, had higher prevalence of diabetes mellitus, induced labours, dystocia, late term and vacuum extraction delivery, and infant birthweight > 4000 g. The strong association between birthweight and shoulder dystocia is confirmed in our study, where the risk of HIE was considerably reduced after adjustment for birthweight. Regardless of parity, shoulder dystocia was common among HIE cases in our study (12%) and was strongly associated to HIE.
Uterine rupture is considered the strongest risk factor for HIE.93,103,108 In ac-cordance with previous reports, the great majority of women with uterine rup-ture were parous women (96%) and had a history of caesarean delivery (87%).136,138 Further, women with a uterine rupture were more often older, short and overweight, induced, had a diagnosis of dystocia and/or fetal-pelvic dispro-portion, occiput posterior position, late term delivery, and infant birthweight > 4000 g. The reported incidence of uterine rupture in attempted vaginal deliv-ery after caesarean section is 0.4–1.5%,137,138,171,172 with a high incidence (1.3%) reported in a Swedish cohort.137 There is a present policy in Sweden of allowing a trial of labour after one caesarean section, which occurs in approximately 60%

59
of mothers with previous caesarean. Of those who use this option, approxi-mately 16% are induced and 75% have vaginal deliveries.137,138 Although the incidence of uterine rupture is low, obstetric communities should reflect on be-ing in the upper range, and on the finding that uterine rupture was the underlying cause in 38% of HIE cases among parous women with a previous caesarean in our study. It is probable that a significant number of HIE cases could be pre-vented by repeat caesarean section performed before labour in selected cases or timely during a trial of labour.173
In cases with placental abruption, maternal age ≥ 35 years, smoking, hyper-tension disorders, gestational age of 36 weeks, and infant birthweight < 3000 grams was more prevalent. Further, multiparity (three or more deliveries) is a known risk factor for abruption,133 and, accordingly, we report placental abrup-tion to have the strongest association to HIE in parous women without a previ-ous caesarean delivery.
Our results suggest that neonatal HIE is caused by multiple risk factors, where antepartum factors may predispose some women to experience adverse intra-partum events, such as obstetric emergencies or traumatic labours. It is also possible that some antepartum factors may increase fetal susceptibility to peri-natal asphyxia.
Given the dismal consequences of moderate to severe HIE, it is most relevant and important to identify risk factors for HIE in the goal of increasing the un-derstanding of causal pathways and developing preventive strategies. In our population, intrapartum events had the strongest association to HIE, and several risk factors for HIE were found, potentially aiding in risk assessment during labour to reduce adverse intrapartum events.
Obstetric emergencies are common underlying causes of moderate to severe neonatal HIE. The strong association to shoulder dystocia in nulliparous women, and to uterine rupture in women with previous caesarean deliveries, implies an opportunity for prevention of HIE.
However, risk factors for obstetric emergencies are common, while the con-dition they predict is not. Therefore, sensitivity and specificity for HIE will be low or lacking. Still, in the individual woman with cumulative risk factors such as clinical fetal macrosomia, protracted labour in the late first stage, and slow descent in the second stage, where assisted mid-pelvic delivery is considered, a difficult delivery with potentially dangerous complications (shoulder dystocia, uterine rupture) may be indicated, and a caesarean delivery would be more pru-dent, both for nulliparous and parous women.

60
Figure 9. Illustration of contributing risk factors in the development of HIE.
Methodological considerations Studies I and II Studies I and II were descriptive and were conducted at a given time at the De-partment of Obstetrics and Gynaecology, Uppsala University Hospital, in Swe-den. With an annual birth rate of approximately 4000 deliveries, FBS was per-formed in 7–8% of attempted vaginal deliveries. Both the success rate and the experience of performing FBS is probably affected by the routine and training of the staff. At departments where the method is frequently used, such as in the study from Hvidovre Hospital, Copenhagen, where 25% of deliveries were monitored with FBS, the failure rate was less than 1% of the pH measure-ments.53 In study I, the failure rate was not recorded, but the majority of FBS tests were combined (lactate and pH). In study II, there were no complete (lac-tate and pH) FBS failures.
Power calculations were not possible, since no previous data about discrep-ancy of combined FBS or the experience of FBS among patients and obstetri-cians existed.
Study I This study provides a good illustration of the discrepancy in combined FBS and obstetric management based on test results, and the study design can be consid-ered appropriate. However, this study design can only test a hypothesis and can-not prove an association or causation. The major weaknesses of the study are the retrospective design and the relatively small number of samples. To confirm our results, larger studies are needed.
Due to the retrospective design, information on important variables such as presence of caput succedaneum, sampling failures, or contamination of amni-otic fluid during FBS is missing.
Umbilical cord blood gas analysis is considered to be an objective and sen-sitive indicator of fetal oxygenation and acid-base condition of the infant at birth.22 Within our study population, data on UA blood gases were missing in 23% of deliveries. A population-based study from Sweden, including 155 235 infants, reported an increased risk of missing samples when using selective sam-pling with respect to high-risk deliveries, and the risk increased almost sixfold in labours where at least two FBS tests were done during delivery.21 However, analysis of our missing UA data revealed that the rate of Apgar score < 7 at 5

61
minutes, operative interventions, and admission to neonatal care were similar to the rates in the whole study population.
Our study included pregnancies ≥ 34 weeks of gestational age, although only a minority of samples (3%) were obtained between 34 to 36 gestational weeks. Since lactate in umbilical blood rises with advancing gestational length, we could have limited the study population to those with gestational age of 37 weeks or more, although the rate of discrepancy would certainly be un-changed.174
Obstetricians performing the FBS were not recorded, and type of test was therefore not compared among caregivers. The frequency of combined and sin-gle tests was evenly distributed, irrespective of the stage of labour, which indi-cates that there was no preference for the test used in relation to the stage of labour.
Study II This is the first and only study to date that has evaluated the experience of FBS among women and obstetricians performing the test, and the study design should be regarded as a pilot study.
The main limitation of this study was the small number of participants. Nev-ertheless, the sample was representative of the women undergoing FBS proce-dures in our unit.
Initially, we had 118 questionnaires completed by women exposed to sam-pling and 60 questionnaires completed by the obstetricians who performed the tests. Because we wanted to analyse correlations and associations between women’s and obstetricians’ experiences of FBS, we decided to analyse ques-tionnaires that could be paired (i.e., a sampling situation resulting in one ques-tionnaire filled in by the women and one questionnaire filled in by the obstetri-cian who performed the test; n = 51). However, the results of all questionnaires were analysed, and the experience of difficulty and pain, as well as the other variables, had the same medians and almost the same interquartile ranges as presented in our study population of 51 FBS situations.
Another limitation was the use of a questionnaire that has not been validated. We have, on the other hand, used a 10-point scale that at least is validated and applied in clinical practice for pain assessment.175 Larger prospective studies using validated questionnaires would enable multivariate logistic regression analyses.
Recording the actual time spent on the FBS procedure would have been op-timal. It is likely that the duration of sampling can be influenced by optimizing logistics, availability of equipment, and trained personnel. In our study, the ac-tual time required for sampling and analysis was not measured. However, nei-ther women nor obstetricians experienced the testing procedure as time con-suming. At the department where the study was conducted, FBS is performed in 8% of deliveries, and the equipment is readily available at the delivery ward. Test results are available within 1 to 3 minutes after sampling. We also

62
acknowledge that our findings are based on the population at one academic medical centre in Sweden and may therefore not be generalizable.
Among the strengths of the study were that the obstetricians anonymously completed the questionnaires immediately after performing the procedure, and that the women completed the questionnaire within 48 hours after delivery, min-imizing the risk for recall bias. However, the women’s general experience of the delivery, and not just the FBS procedure, could have influenced how the questions were answered.176 Additionally, the total experience of labour and fear of childbirth could have been evaluated. The response frequency was 100%, minimizing selection bias.
Studies III and IV These studies were designed as register-based cohort studies. Epidemiologic studies restrict interpretation of causality and biological actions between expo-sures and outcomes. A disadvantage with cohort studies is that rare outcomes such as HIE are difficult to study, owing to the need of large datasets for anal-ysis, which can bring unreasonable costs and waiting time between exposure and outcome. By using register data, the exposure and outcome are already reg-istered.
Further, the findings in cohort studies may be subject to bias, related to the information used, and the selection of covariates that are associated with the measures of exposures and outcomes (confounders, mediators, and colliders). To improve the accuracy of our estimates, covariates potentially associated with HIE in our and previous studies were adjusted for.
Mode of delivery was not used for adjustments in the regression analyses, because we reasoned that these interventions (i.e., vacuum extraction and cae-sarean section) could have been actions taken because of suspected fetal dis-tress, leading to confounding by indication, and might impact the association between exposure and outcome. However, in study III, the risk of HIE by ma-ternal habitus was stratified by mode of delivery. In Study IV, confounders were calculated with DAG for each obstetric emergency, because they each have dif-ferent associated covariates.
In all studies, multiple testing increases the risk of type 1 error (false posi-tive), where some of the associations might be by chance. By using a large sam-ple size, this error can be minimized. The CI around the estimates reported in study III were narrow, indicating high precision. Additionally, we found a dose-response association between increasing BMI and decreasing maternal height, which is generally considered to strengthen the possibility of causal relation-ships (Hill’s criterion). The CIs were broader in study IV, possibly owing to few observations and missing covariates in the analysis. Strengths include the population-based design with prospectively collected data on exposures and outcomes from healthcare registers, minimizing the risk of

63
selection and information bias. The MBR is well validated and covers more than 98% of all births in Sweden during the study period,147,148 providing high inter-nal validity.
There are no published systematic validations of the SNQ registry. However, the registry has covered all neonatal units in Sweden since 1 January, 2011. All infants treated with hypothermia in Sweden are registered prospectively in standardized forms, and data input is monitored.145 By using hypothermia treat-ment as a surrogate variable, the diagnostic accuracy was improved with stricter definition for the rare outcome, enabling analyses of moderate to severe HIE cases specifically, which we consider the major strength of studies III and IV.
Further, the large sample size and reliable data for exposure and outcome allowed stratification and adjustments for potentially confounding variables, despite the rare outcome.
A limitation of the studies, due to the data collection from registers, is missing information on certain interesting covariates, such as labour duration, active pushing time, and CTG traces. However, data on dystocia and disproportion were retrieved from the ICD-10 codes.
Further, using register data is always associated with a risk of underreporting and errors. For example, ICD codes are occasionally underreported or incor-rect.147,148 Moreover, there is a possibility that the coding of a diagnosis may be more frequent after a complicated delivery or after an adverse neonatal out-come. A sizeable proportion (5.8%) of women were excluded from the analysis due to missing data on BMI. Exclusions due to missing data may lead to selec-tion bias and impact the risk estimates, and no imputation was made for missing data. Additionally, we relied on self-reported height, and overweight women might tend to slightly over-report their height, leading to misclassification bias.177 However, BMI was calculated from measured weight. Considering that we found increased risk for HIE in infants born to overweight women, the true risk would most likely be even greater.
Another weakness is that the external validity might be limited, and the re-sults can only be generalized to facilities with similar socioeconomic and de-mographic characteristics, and to healthcare systems of comparable standard.
A problem resulting from large study populations may be the interpretation of statistical significance at group level to clinical significance at the individual level. The absolute risks of short maternal height, obstetric emergencies, and HIE are low. Although statistically significant, the risk increase in absolute terms may not have a strong impact for the individual, however of great im-portance from a public health perspective, especially when the prevalence of overweight is high in the population.
64
Conclusions
In the combined test, discrepancies between pH and lactate measurements were common and occurred in half of the samples with an abnormality. Obstetric management was influenced by the discrepancy between test re-sults with respect to ODFD rates and the time interval from the last FBS to delivery. (Study I)
FBS was well tolerated in women who had epidural analgesia, but might be associated with pain in women without. Higher maternal BMI and less cer-vical dilatation were associated with higher pain ratings. Obstetricians did not generally experience FBS as difficult to perform. The sampling proce-dure can be more complicated in situations with higher maternal BMI, less cervical dilatation, and higher station of the fetal head. (Study II)
There is a dose-response relationship between increasing BMI and decreas-ing maternal height and the risk of moderate to severe HIE. The combina-tion of maternal short stature and overweight increased the risk of HIE, es-pecially in parous women without a previous caesarean. (Study III)
An obstetric emergency was a common underlying cause of HIE, more commonly in parous than in nulliparous women. Among nulliparous women, shoulder dystocia was the most common event with the strongest association to HIE. In parous women without a previous caesarean, shoul-der dystocia was most common, but placental abruption had the strongest association to HIE. In parous women with a previous caesarean, uterine rupture was the most common event, with the strongest association to HIE. (Study IV)
Although the absolute risk of moderate to severe HIE is small, its severity warrants meticulous intrapartum management, with attention to mode of delivery, in the risk groups identified. The strong association to uterine rup-ture and shoulder dystocia implies an opportunity for prevention of HIE. (Studies III and IV)

65
Future perspectives
Future studies could address the possibility of using the combined FBS test in preference to, or as a complement to, the single test, to avoid unnecessary oper-ative interventions, and could consider subgroup analysis of FBS lactate and pH values by the stage of labour and sampling within a protracted labour in the first and second stages. However, this requires large, randomized studies, and be-cause the neonatal outcome must be secured, a limit cut-off safe for all fetuses must be guaranteed, and different action cut-offs would be difficult to set, mak-ing the test method less feasible in clinical practice. Further, the results may not be of interest in a majority of developed countries, where FBS is not used.
Additionally, we await the findings from the ongoing randomised controlled Flamingo and SCALP trials, which are comparing allocation to CTG alone with CTG and FBS for lactate; addressing rates of caesarean section, longer-term neonatal outcomes, and maternal satisfaction with intrapartum fetal monitoring; and conducting economic analysis.11,178
Larger studies regarding maternal experience of FBS are needed, with eval-uation of the total experience of labour where FBS is performed, and differences in women with and without fear of childbirth could be assessed using validated questionnaires.
The challenge in countries with high standards of obstetric care, where perinatal death rates are low, is to improve neonatal morbidity and mortality further. The use of a computer-generated support system to CTG did not improve neonatal outcomes nor decrease rates of operative deliveries.179,180 Prediction models that provides individual probability of having an adverse neonatal outcome could be developed and used for risk assessment during labour. However, continuous education and training, as well as high competence in delivery units during all hours, are probably just as important. A cohort study from Australia demon-strated that a review of CTG by a consultant obstetrician, prior to the decision to perform FBS, was associated with reductions in FBS performed, UA acido-sis, and ODFD.181
The differences in outcome measures restrict interpretation and comparisons between studies on HIE. Using therapeutic hypothermia as a surrogate variable for moderate to severe neonatal HIE is better than using ICD-codes for HIE and could be the first choice of outcome measure in future studies.

66
By combining national quality registers, epidemiologic studies are feasible in respect to follow-up, power, and costs.
A study evaluating the differences in short- and long-term outcomes among infants with moderate to severe HIE born to women with or without an obstetric emergency during labour is in progress.
Additional knowledge is of importance regarding the effect on pregnancy and labour outcomes among women with maternal overweight and obesity. The underlying mechanisms of known complications in women with high BMI should be explored by preclinical and clinical studies concerning differences in labour outcomes and interventions in these women.
An even more challenging issue for researches and health care providers is to find effective preventive measures to reduce the overall proportion of over-weight and obesity among women of reproductive age, before pregnancy.

67
Summary in Swedish - Sammanfattning på svenska
Syftet med fosterövervakning under förlossningen är att förebygga uppkomst av syrebrist (asfyxi), och därmed minska risken för neonatal sjuklighet, neuro-logisk skada eller död.
Cardiotocografi (CTG), som är den grundläggande metoden för fosteröver-vakning under förlossning, introducerades på 1960-talet med stora förhopp-ningar om att reducera sjuklighet och dödlighet på grund av asfyxi. Randomi-serade studier har visat att CTG, jämfört med intermittent övervakning, minskar förekomsten av neonatala kramper men inte för cerebral pares eller neonatal död till följd av syrebrist. Problem med CTG är den subjektiva tolkningen som medför en avsevärd variation mellan olika CTG bedömare, samt metodens låga specificitet för asfyxi. Ett normal CTG är ett betryggande tecken och indikerar ett väl syresatt foster. Dock gäller inte det motsatta, då många friska foster ofta uppvisar avvikande CTG mönster någon gång under förlossningen. CTG har således en hög sensitivitet, men låg specificitet med många falskt positiva test, vilket kan leda till onödiga interventioner jämfört med auskultation.
Som komplement vid avvikande CTG används därför ofta blodprovstagning från fostrets skalp (skalpprov) för analys av pH och laktat. I randomiserande studier, där analys av pH har jämförts med laktat, har inga skillnader i neonatalt utfall (metabol acidos, neonatal encephalopati, låga Apgar poäng, vård på neo-natal avdelning) eller förlossningssätt rapporterats. Huruvida pH eller laktat är bättre är fortfarande obesvarat. Laktat anses vara det bästa alternativet då mindre blodmängd krävs för laktatanalys vilket bidrar till högre frekvens lyck-ade provtagningar än pH. Dessutom anses laktat bättre återspegla syrebrist och surhetsgraden i vävnaderna och betraktas därför som en tidigare markör för svår syrebrist.
Kombinerad analys med pH och laktat rekommenderas inte, då det inte antas kunna förutse neonatala utfall bättre än var metod för sig. Det har även fram-kommit oro över möjligheten till ökad frekvens av onormala provsvar med ett kombinerat test, jämfört med ett enda test, vilket skulle resultera i en ökad fre-kvens av operativa ingrepp. Dessa antaganden har dock inte studerats.
Kvinnornas tillfredställelse med olika övervakningsmetoder under förloss-ningen är viktig då det påverkar upplevelsen av kontroll, och därmed upplevel-sen av förlossningen. I litteraturen beskrivs ofta skalpprovtagning som en be-svärlig, svår och tidskrävande undersökning för både den födande kvinna och

68
provtagande läkare. Trots dessa påståenden finns ingen studie som utvärderat kvinnornas och provtagande läkares subjektiva upplevelse av skalpprovtagning.
Hypoxisk ischemisk encefalopati (HIE) är ett syndrom med hjärnfunktions-påverkan hos nyfödda fullgångna barn orsakat av svår syrebrist under förloss-ningen, och drabbar 0,9–1,7 av 1000 barn i västvärlden. Baserat på allvarlig-hetsgraden av kliniska fynd, klassificeras HIE till mild, måttlig eller svår. För barn med mild HIE är prognosen konsekvent positiv, medans barn med måttlig till svår HIE har stor risk för allvarliga konsekvenser inklusive död, cerebral pares, epilepsi och kognitiv funktionsnedsättning. Även om HIE är ovanligt är konsekvenserna betydande för de familjer som drabbas, varför det är viktigt att identifiera orsakssamband och riskfaktorer för HIE som kan vara vägledande för förebyggande åtgärder.
Stora skillnader i hur asfyxi definierats är ett problem, och studiepopulation-erna har sett olika ut i tidigare studier. Kylbehandling har under det senaste de-cenniet funnits tillgänglig för barn med måttlig till svår HIE, och har visat sig reducera risken för hjärnskada eller död hos dessa barn. Indikationen för kylbe-handling baseras på standardiserade kliniska diagnostiska kriterier och kan där-med användas som surrogat för måttlig till svår HIE.
Delarbete I Syftet med studien var att undersöka om det förelåg diskrepans mellan laktat och pH i kombinerade skalpprov, samt att ta reda på om handläggningen påver-kas av diskrepansen. Mellan maj 2009 och april 2010 monitorerades 241 förlossningar med skalp-prov. Diskrepans vid skalpprovsvar för pH och laktat vid kombinerat test fö-relåg då ett prov var normalt och ett onormalt (onormalt pH: ≤7.24, lak-tat: ≥ 4.2). Handläggningen studerades med avseende andelen operativa för-lossningar p.g.a. hotande fosterasfyxi samt tidsintervallet från sista skalpprov till operativ förlossning pga hotande fosterasfyxi.
Vi fann att det fanns en diskrepans mellan laktat och pH i över häften av provsvaren. Andelen operativa förlossningar på grund av hotande asfyxi var mindre vid kombinerat prov jämfört med singel prov. Tiden från sista skalpprov till operativ förlossning på grund av hotande asfyxi var längre vid kombinerat prov med ett onormalt provsvar, jämfört med två onormala provsvar.
Delarbete II Syftet med studien var att utvärdera de födande kvinnornas och provtagande läkares subjektiva upplevelse av skalpprovtagning.
Mellan maj 2010 och mars 2011, tillfrågades kvinnor som övervakades med skalpprov under förlossningen samt läkare som utförde provtagningen om de ville svara på ett frågeformulär avseende upplevelsen av skalpprovtagningen (n = 51). Frågeformuläret bestod av frågor om som besvarades på en 10-gradig skala (1=stämmer inte alls, 10= stämmer helt). Läkarna uppgav även öppnings-

69
grad av livmodertappen samt station av fosterhuvudet vid provtagningen. Mo-derns body mass index (BMI) kategoriserades enligt World Health Organizat-ions definition av normalvikt (BMI < 25 kg/m2) eller övervikt (BMI ≥ 25 kg/m2).
Vi fann att kvinnor tolererade skalpprovtagningen väl, framförallt kvinnor som hade ryggbedövning. Upplevelse av smärta var vanligare hos kvinnor med högre BMI och vid mindre öppningsgrad av livmodertappen. Läkare tyckte ge-nerellt inte att provtagning innebar några svårigheter men att den var mer kom-plicerad hos kvinnor med högre BMI, mindre öppningsgrad och högre belägen station av fostret.
Delarbete III-IV Syftet med dessa delarbeten var att studera graviditets- samt förlossningsrelate-rade riskfaktorer för måttlig till svår neonatal HIE. I delarbete III studerades graviditetsrelaterade faktorer, med fokus på moderns längd och BMI. I delar-bete IV studerades proportionen av obstetriska katastrofer bland fall av HIE, och förekomsten av dessa beroende av paritet.
Genom länkning av det Medicinska födelseregistret (MFR) till Svenskt Ne-onatalt Kvalitetsregister (SNQ), erhölls en kohort på 692 428 levande födslar ≥ 36 graviditetsveckor för åren 2009–2015. Kylbehandling användes som surro-gat för måttlig till svår neonatal HIE (n = 464). Kvinnor kategoriseras som korta (≤ 155 cm), övervikta (BMI ≥ 25 kg/m2), eller både korta och överviktig, där ej korta och normalviktiga kvinnor användes som referens. Obstetriska katastrofer definierades som moderkaksavlosssning, eklampsi, navelsträngsframfall, uterusruptur och/eller skulderdystoci.
Vi fann att förstföderskor, kvinnor med tidigare kejsarsnitt, kortvuxenhet, övervikt, graviditetslängd, vidöppen bjudning vid förlossning samt barnvikt > 4000 gram var oberoende riskfaktorer för HIE.
Delarbete III visade att det fanns ett dosberoende samband mellan risken för HIE och ökande BMI enhet samt minskade längd per cm hos modern. Kvinnor med kombinationen av kortvuxenhet (≤ 155 cm) och övervikt (BMI > 25 kg/m2), hade tre gånger ökad risk för att få ett barn med måttlig till svår HIE jämfört med ej korta och normalviktiga kvinnor.
Delarbete IV: visade att obstetriska katastrofer var vanligt förekommande (29%) vid måttlig till svår HIE, vanligare hos omföderskor (37%) än hos först-föderskor (21%). Bland förstföderskor var skulderdystoci den vanligaste hän-delsen med det starkaste sambandet till HIE. Bland omföderskor utan tidigare kejsarsnitt var skulderdystoci den vanligaste obstetriska katastrofen, men mo-derkaksavlosssning hade starkaste sambandet till HIE. Bland omföderskor med tidigare kejsarsnitt var uterusruptur den vanligaste obstetriska katastrofen och hade även största risken för HIE.

70
Acknowledgements
I am grateful to many people who in various ways have contributed to this work. In particular, I would like to thank:
All the women who willingly contributed to this research.
Maria Jonsson, my main supervisor, for introducing me to science and sharing your huge knowledge of fetal surveillance, as well as your enthusiasm for the scientific approach. Thank you for generously sharing your kitchen table and scientific knowledge, and for the extra time you spent when I needed you. Dur-ing all those hours of working together, we have also come to discuss clinical aspects, and you have become an inspiring clinical mentor.
Anna-Karin Wikström, my co-supervisor. Never has the word ‘thanks’ seemed so inadequate. My sincerest appreciation for sharing your vast knowledge of epidemiology, statistics, design of manuscripts, tables and fig-ures. A conversation with you will always be longer than planned, my Previa counsellor.
My co-supervisors, Ulf Hansson, Ulf Högberg, Alkistis Skalkidou, Helena Åkerud, and Johan Ågren, for your hard work and valuable competence that made this thesis possible.
Masoumeh Rezapour, head of the Department of Obstetrics and Gynaecology in Uppsala, for providing me with working conditions that enabled me to finish this thesis.
Gudlaug Sverrisdottir and Kristiina Kask, head and former head of the Gy-naecological division, for believing in me and giving me the opportunity to be a part of the team, as well as being flexible and understanding and for giving me time off to complete my thesis.
Marianne Larsson for support and always having your door open.
My colleagues at the Department of Obstetrics and Gynaecology in Uppsala, for great friendship and a supportive atmosphere. You make my job the best!

71
My dear colleagues and friends Johanna and Mariella. We’ve shared all these years, starting from our student years, as residents, and later through thesis anx-iety. Thank you for shared laughs, thoughts, and worries about research, clinical work, and family. Without your encouragement, this would not have been pos-sible.
I’m forever grateful to my parents, Gunilla and Anders Forsberg, for your love and unwavering pride in me that gave me the courage to never give up.
My sister Eva and brother Lars for our close relationship and always standing side by side.
Gudrun and Roland, my dear parents in law, for your admirable wisdom, boundless support and kindness.
My pride Kajsa, Karl, and Olof, for being the amazing people that you are. And for reminding me what matters. I love you!
Behind every successful woman stands a strong man. Without you, Per, this thesis would never have been written. And the editing of tables would certainly be substandard. Thanks for taking full responsibility for our family in my most busy time periods. But most of all for being in my life. The best in life would not have been without you.
The studies were financially supported by The Gillbergska stiftelsen and Upp-sala County Council (ALF project).

72
References
1. Socialstyrelsen. Official Statistics of Sweden. Statistics - Health and Medical care. Pregnancies, Deliveries and Newborn Infant 2016. 2018.
2. Jonsson M, Norden SL, Hanson U. Analysis of malpractice claims with a focus on oxytocin use in labour. Acta Obstet Gynecol Scand. 2007;86(3):315-319.
3. Hagberg B, Hagberg G, Beckung E, Uvebrant P. Changing panorama of cerebral palsy in Sweden. VIII. Prevalence and origin in the birth year period 1991-94. Acta Paediatr. 2001;90(3):271-277.
4. Villamor E, Tedroff K, Peterson M, et al. Association between maternal body mass index in early pregnancy and incidence of cerebral palsy. JAMA. 2017;317(9):925-936.
5. Thornberg E, Thiringer K, Odeback A, Milsom I. Birth asphyxia: incidence, clinical course and outcome in a Swedish population. Acta Paediatr. 1995;84(8):927-932.
6. Milsom I, Ladfors L, Thiringer K, Niklasson A, Odeback A, Thornberg E. In-fluence of maternal, obstetric and fetal risk factors on the prevalence of birth asphyxia at term in a Swedish urban population. Acta Obstet Gynecol Scand. 2002;81(10):909-917.
7. de Vries LS, Jongmans MJ. Long-term outcome after neonatal hypoxic-is-chaemic encephalopathy. Arch Dis Child Fetal Neonatal Ed. 2010;95(3):F220-224.
8. Jacobs SE, Berg M, Hunt R, Tarnow-Mordi WO, Inder TE, Davis PG. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev. 2013(1):CD003311.
9. Kurinczuk JJ, White-Koning M, Badawi N. Epidemiology of neonatal encepha-lopathy and hypoxic-ischaemic encephalopathy. Early Hum Dev. 2010;86(6):329-338.
10. Alfirevic Z, Devane D, Gyte GM, Cuthbert A. Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour. Cochrane Database Syst Rev. 2017;2:CD006066.
11. East CE, Leader LR, Sheehan P, Henshall NE, Colditz PB, Lau R. Intrapartum fetal scalp lactate sampling for fetal assessment in the presence of a non-reassur-ing fetal heart rate trace. Cochrane Database Syst Rev. 2015;5:CD006174.
12. Saling E, Schneider D. Biochemical supervision of the foetus during labour. J Obstet Gynaecol Br Commonw. 1967;74(6):799-811.
13. Low JA, Pancham SR, Worthington D, Boston RW. Acid-base, lactate, and py-ruvate characteristics of the normal obstetric patient and fetus during the intra-partum period. Am J Obstet Gynecol. 1974;120(7):862-867.
14. Smith NC, Quinn MC, Soutter WP, Sharp F. Rapid whole blood lactate meas-urement in the fetus and mother during labour. Early Hum Dev. 1979;3(1):89-95.
15. Low JA. Determining the contribution of asphyxia to brain damage in the neo-nate. J Obstet Gynaecol Res. 2004;30(4):276-286.
73
16. Hogan L, Ingemarsson I, Thorngren-Jerneck K, Herbst A. How often is a low 5-min Apgar score in term newborns due to asphyxia? Eur J Obstet Gynecol Re-prod Biol. 2007;130(2):169-175.
17. Kumar S, Paterson-Brown S. Obstetric aspects of hypoxic ischemic encephalo-pathy. Early Hum Dev. 2010;86(6):339-344.
18. SBU. (Swedish Council on Technology Assessment in Health care) Rutinmässig ultraljudsundersökning under graviditet (Routine Ultarsound Examination in Pregnancy). Report No : 139. 1998.
19. Socialstyrelsen. Handläggning av normal förlossning- State of the Art. Social-styrelsen. 2001; Stockholm. https://www.sfog.se/me-dia/66770/state_of_the_art_pn.pdf.
20. Holzmann M, Nordstrom L. Follow-up national survey (Sweden) of routines for intrapartum fetal surveillance. Acta Obstet Gynecol Scand. 2010;89(5):712-714.
21. Ahlberg M, Elvander C, Johansson S, Cnattingius S, Stephansson O. A policy of routine umbilical cord blood gas analysis decreased missing samples from high-risk births. Acta Paediatr. 2017;106(1):43-48.
22. Neilson JP. Umbilical cord blood gas analysis. BMJ. 2010;340:c1720. 23. Walsh CA, McMenamin MB, Foley ME, Daly SF, Robson MS, Geary MP.
Trends in intrapartum fetal death, 1979-2003. Am J Obstet Gynecol. 2008;198(1):e41-47.
24. National Institute fot Health and Clinical Excellence. Intraparum care cgLNIfHaCE, September. p. 225-292.
25. Liljestrom L, Wikstrom AK, Hanson U, Akerud H, Jonsson M. Evaluation of the discrepancy between pH and lactate in combined fetal scalp blood sampling. Acta Obstet Gynecol Scand. 2011;90(10):1088-1093.
26. Liljestrom L, Wikstrom AK, Skalkidou A, Akerud H, Jonsson M. Experience of fetal scalp blood sampling during labor. Acta Obstet Gynecol Scand. 2014;93(1):113-117.
27. Svensk förening för obstetrik och Gynekologi (SFOG): CTG guidelines. http://www.sfog.se/start/om-sfog/aktuellt/nya-svenska-riktlinjer-for-ctg-tolk-ning-under-forlossning. 2017.
28. Jonsson M, Norden-Lindeberg S, Ostlund I, Hanson U. Acidemia at birth, related to obstetric characteristics and to oxytocin use, during the last two hours of labor. Acta Obstet Gynecol Scand. 2008;87(7):745-750.
29. Devane D, Lalor J. Midwives’ visual interpretation of intrapartum cardioto-cographs: intra- and inter-observer agreement. J Adv Nurs. 2005;52(2):133-141.
30. Chauhan SP, Klauser CK, Woodring TC, Sanderson M, Magann EF, Morrison JC. Intrapartum nonreassuring fetal heart rate tracing and prediction of adverse outcomes: interobserver variability. Am J Obstet Gynecol. 2008;199(6):623 e621-625.
31. Jorgensen JS, Weber T. Fetal scalp blood sampling in labor--a review. Acta Ob-stet Gynecol Scand. 2014;93(6):548-555.
32. Rooth G. Perinatal acid-base balance. Lund: Studentlitteratur. 1988. 33. Nijland R, Jongsma HW, Nijhuis JG, van den Berg PP, Oeseburg B. Arterial
oxygen saturation in relation to metabolic acidosis in fetal lambs. Am J Obstet Gynecol. 1995;172(3):810-819.
34. Li H, Gudmundsson S, Olofsson P. Acute centralization of blood flow in com-promised human fetuses evoked by uterine contractions. Early Hum Dev. 2006;82(11):747-752.
35. Keith R. Green MD F. Antepartum and intrapartum fetal assessment. Scalp blood analysis. Obstetrics and Gynecology Clinics. 1999;26(4):642-656.

74
36. Engidawork E, Chen Y, Dell'Anna E, et al. Effect of perinatal asphyxia on sys-temic and intracerebral pH and glycolysis metabolism in the rat. Exp Neurol. 1997;145(2 Pt 1):390-396.
37. Eguiluz A, Lopez Bernal A, McPherson K, Parrilla JJ, Abad L. The use of intra-partum fetal blood lactate measurements for the early diagnosis of fetal distress. Am J Obstet Gynecol. 1983;147(8):949-954.
38. Bretscher J, Saling E. pH values in the human fetus during labor. Am J Obstet Gynecol. 1967;97(7):906-911.
39. Saling E. [A new method for examination of the child during labor. Introduction, technic and principles]. Archiv fur Gynakologie. 1962;197:108-122.
40. Royal Collage of Obstetricians and Gynecologists. The use of electronic fetal monitoring.The use and interpretation of cardiotocography in intrapartum fetal surveillance. Evidence-based Clinical Guideline Number 8. London. RCOG Press; 2001. .
41. Hill JB, Chauhan SP, Magann EF, Morrison JC, Abuhamad AZ. Intrapartum fetal surveillance: review of three national guidelines. Am J Perinatol. 2012;29(7):539-550.
42. Stein W, Hellmeyer L, Misselwitz B, Schmidt S. Impact of fetal blood sampling on vaginal delivery and neonatal outcome in deliveries complicated by patho-logic fetal heart rate: a population based cohort study. J Perinat Med. 2006;34(6):479-483.
43. Ayromlooi J, Garfinkel R. Impact of fetal scalp blood pH on the incidence of cesarean section performed for fetal distress. Int J Gynaecol Obstet. 1980;17(4):391-392.
44. Reif P, Haas J, Scholl W, Lang U. [Foetal scalp blood sampling: impact on the incidence of Caesarean section and assisted vaginal deliveries for non-reassuring foetal heart rate and its use according to gestational age]. Zeitschrift fur Geburtshilfe und Neonatologie. 2011;215(5):194-198.
45. Mahendru AA, Lees CC. Is intrapartum fetal blood sampling a gold standard diagnostic tool for fetal distress? Eur J Obstet Gynecol Reprod Biol. 2011;156(2):137-139.
46. Devane D, Lalor J, Bonnar J. The use of intrapartum electronic fetal heart rate monitoring: a national survey. Ir Med J. 2007;100(2):360-362.
47. Westerhuis M. Intrapartum fetal monitoring by ST-analysis of the fetal ECG. Thesis for doctoral degree UU, Netherlands. 2010. p.19.
48. Wheble AM, Gillmer MD, Spencer JA, Sykes GS. Changes in fetal monitoring practice in the UK: 1977-1984. Br J Obstet Gynaecol. 1989;96(10):1140-1147.
49. Goodwin TM, Milner-Masterson L, Paul RH. Elimination of fetal scalp blood sampling on a large clinical service. Obstet Gynecol. 1994;83(6):971-974.
50. Westgren M, Kruger K, Ek S, et al. Lactate compared with pH analysis at fetal scalp blood sampling: a prospective randomised study. Br J Obstet Gynaecol. 1998;105(1):29-33.
51. Allen RM, Bowling FG, Oats JJ. Determining the fetal scalp lactate level that indicates the need for intervention in labour. Aust N Z J Obstet Gynaecol. 2004;44(6):549-552.
52. Kruger K, Hallberg B, Blennow M, Kublickas M, Westgren M. Predictive value of fetal scalp blood lactate concentration and pH as markers of neurologic disa-bility. Am J Obstet Gynecol. 1999;181(5 Pt 1):1072-1078.
53. Rorbye C, Perslev A, Nickelsen C. Lactate versus pH levels in fetal scalp blood during labor--using the Lactate Scout System. J Matern Fetal Neonatal Med. 2016;29(8):1200-1204.

75
54. Heinis AM, Spaanderman ME, Gunnewiek JM, Lotgering FK. Scalp blood lac-tate for intra-partum assessment of fetal metabolic acidosis. Acta Obstet Gynecol Scand. 2011;90(10):1107-1114.
55. Holzmann M, Wretler S, Cnattingius S, Nordstrom L. Neonatal outcome and delivery mode in labors with repetitive fetal scalp blood sampling. Eur J Obstet Gynecol Reprod Biol. 2015;184:97-102.
56. Steer PJ. Is fetal blood sampling and pH estimation helpful or harmful? Arch Dis Child. 1987;62(11):1097-1098.
57. Neilson JP. Fetal scalp sampling in labour. BMJ. 2008;336(7656):1257-1258. 58. Tuffnell D, Haw WL, Wilkinson K. How long does a fetal scalp blood sample
take? BJOG. 2006;113(3):332-334. 59. Molfese V, Sunshine P, Bennett A. Reactions of women to intrapartum fetal
monitoring. Obstet Gynecol. 1982;59(6):705-709. 60. Parisaei M, Harrington KF, Erskine KJ. Maternal satisfaction and acceptability
of foetal electrocardiographic (STAN(R)) monitoring system. Arch Gynecol Ob-stet. 2011;283(1):31-35.
61. Killien MG, Shy K. A randomized trial of electronic fetal monitoring in preterm labor: mothers’ views. Birth. 1989;16(1):7-12.
62. Hindley C, Hinsliff SW, Thomson AM. Pregnant women’s views about choice of intrapartum monitoring of the fetal heart rate: a questionnaire survey. Int J Nurs Stud. 2008;45(2):224-231.
63. Crawford A, Hayes D, Johnstone ED, Heazell AEP. Women's experiences of continuous fetal monitoring - a mixed-methods systematic review. Acta Obstet Gynecol Scand. 2017;96(12):1404-1413.
64. Ingemarsson I, Arulkumaran S. Fetal acid-base balance in low-risk patients in labor. Am J Obstet Gynecol. 1986;155(1):66-69.
65. Westgren M, Kublickas M, Kruger K. Role of lactate measurements during la-bor. Obstet Gynecol Surv. 1999;54(1):43-48.
66. Low JA. Intrapartum fetal surveillance. Is it worthwhile? Obstet Gynecol Clin North Am. 1999;26(4):725-739.
67. Goldaber KG, Gilstrap LC, 3rd, Leveno KJ, Dax JS, McIntire DD. Pathologic fetal acidemia. Obstet Gynecol. 1991;78(6):1103-1107.
68. Yoshioka T, Roux JF. Correlation of fetal scalp blood pH, glucose, lactate and pyruvate concentrations with cord blood determinations at time of delivery and cesarean section. J Reprod Med. 1970;5(5):209-214.
69. Nordstrom L, Ingemarsson I, Westgren M. Fetal monitoring with lactate. Baillieres Clin Obstet Gynaecol. 1996;10(2):225-242.
70. Nordstrom L. Fetal scalp and cord blood lactate. Best Pract Res Clin Obstet Gy-naecol. 2004;18(3):467-476.
71. Losch A, Kainz C, Kohlberger P, et al. Influence on fetal blood pH when adding amniotic fluid: an in vitro model. BJOG. 2003;110(5):453-456.
72. Odendaal H. Factors influencing the pH value of foetal scalp blood with special reference to caput succedaneum. S Afr Med J. 1974;48(2):59-62.
73. Carbonne B, Cudeville C, Maillard F, Goffinet F, French Study Group on Fetal Pulse O. Predictive value of pulse oximetry and fetal scalp blood pH in the case of meconium-stained amniotic fluid. Eur J Obstet Gynecol Reprod Biol. 2003;109(1):27-32.
74. Pascual Mancho J, Marti Gamboa S, Redrado Gimenez O, Crespo Esteras R, Rodriguez Solanilla B, Castan Mateo S. Diagnostic accuracy of fetal scalp lac-tate for intrapartum acidosis compared with scalp pH. J Perinat Med. 2017;45(3):315-320.

76
75. Nordstrom L, Persson B, Shimojo N, Westgren M. Fetal scalp and umbilical artery blood lactate measured with a new test strip method. Br J Obstet Gynae-col. 1992;99(4):307-309.
76. Birgisdottir BT, Holzmann M, Varli IH, Graner S, Saltvedt S, Nordstrom L. Ref-erence values for Lactate Pro 2 in fetal blood sampling during labor: a cross-sectional study. J Perinat Med. 2017;45(3):321-325.
77. Nordstrom L, Achanna S, Naka K, Arulkumaran S. Fetal and maternal lactate increase during active second stage of labour. BJOG. 2001;108(3):263-268.
78. Wiberg N, Kallen K. Fetal scalp blood lactate during second stage of labor: de-termination of reference values and impact of obstetrical interventions. J Matern Fetal Neonatal Med. 2017;30(5):612-617.
79. Nordstrom L, Ingemarsson I, Persson B, Shimojo N, Westgren M. Lactate in fetal scalp blood and umbilical artery blood measured during normal labor with a test strip method. Acta Obstet Gynecol Scand. 1994;73(3):250-254.
80. Holzmann M, Cnattingius S, Nordstrom L. Lactate production as a response to intrapartum hypoxia in the growth-restricted fetus. BJOG. 2012;119(10):1265-1269.
81. Wiberg-Itzel E, Lipponer C, Norman M, et al. Determination of pH or lactate in fetal scalp blood in management of intrapartum fetal distress: randomised con-trolled multicentre trial. BMJ. 2008;336(7656):1284-1287.
82. Holzmann M, Cnattingius S, Nordstrom L. Outcome of severe intrapartum acidemia diagnosed with fetal scalp blood sampling. J Perinat Med. 2011;39(5):545-548.
83. Ramanah R, Martin A, Riethmuller D, Maillet R, Schaal JP. [Value of fetal scalp lactate sampling during labour: a comparative study with scalp pH]. Gynecol Obstet Fertil. 2005;33(3):107-112.
84. Nordstrom L. Fetal scalp blood measurements during labour-lactate or pH? Clin Biochem. 2011;44(7):456-457.
85. Nordstrom L. Fetal lactate levels during labour and at delivery determined with test strip methods. Thesis for doctoral degree KI, Stockholm, Sweden, 1995. p. 45-46.
86. Althabe F, Belizan JM. Caesarean section: the paradox. Lancet. 2006;368(9546):1472-1473.
87. Low JA. Metabolic acidosis and fetal reserve. Baillieres Clin Obstet Gynaecol. 1996;10(2):211-224.
88. Gluckman PD, Williams CE. When and why do brain cells die? Dev Med Child Neurol. 1992;34(11):1010-1014.
89. Graham EM, Ruis KA, Hartman AL, Northington FJ, Fox HE. A systematic re-view of the role of intrapartum hypoxia-ischemia in the causation of neonatal encephalopathy. Am J Obstet Gynecol. 2008;199(6):587-595.
90. Jonsson M, Norden-Lindeberg S, Ostlund I, Hanson U. Metabolic acidosis at birth and suboptimal care--illustration of the gap between knowledge and clini-cal practice. BJOG. 2009;116(11):1453-1460.
91. Morgan JL, Casey BM, Bloom SL, McIntire DD, Leveno KJ. Metabolic Acidemia in Live Births at 35 Weeks of Gestation or Greater. Obstet Gynecol. 2015;126(2):279-283.
92. Hankins GD, Speer M. Defining the pathogenesis and pathophysiology of neo-natal encephalopathy and cerebral palsy. Obstet Gynecol. 2003;102(3):628-636.
93. Martinez-Biarge M, Madero R, Gonzalez A, Quero J, Garcia-Alix A. Perinatal morbidity and risk of hypoxic-ischemic encephalopathy associated with intra-partum sentinel events. Am J Obstet Gynecol. 2012;206(2):148 e141-147.

77
94. Himmelmann K, Uvebrant P. The panorama of cerebral palsy in Sweden. XI. Changing patterns in the birth-year period 2003-2006. Acta Paediatr. 2014;103(6):618-624.
95. Sykes GS, Molloy PM, Johnson P, et al. Do Apgar scores indicate asphyxia? Lancet. 1982;1(8270):494-496.
96. Loman AM, ter Horst HJ, Lambrechtsen FA, Lunsing RJ. Neonatal seizures: aetiology by means of a standardized work-up. Eur J Paediatr Neurol. 2014;18(3):360-367.
97. MacLennan A. A template for defining a causal relation between acute intrapar-tum events and cerebral palsy: international consensus statement. BMJ. 1999;319(7216):1054-1059.
98. Executive summary: Neonatal encephalopathy and neurologic outcome, second edition. Report of the American College of Obstetricians and Gynecologists' Task Force on Neonatal Encephalopathy. Obstet Gynecol. 2014;123(4):896-901.
99. Ellis M, Manandhar N, Manandhar DS, Costello AM. Risk factors for neonatal encephalopathy in Kathmandu, Nepal, a developing country: unmatched case-control study. BMJ. 2000;320(7244):1229-1236.
100. Badawi N, Kurinczuk JJ, Keogh JM, et al. Antepartum risk factors for newborn encephalopathy: the Western Australian case-control study. BMJ. 1998;317(7172):1549-1553.
101. Badawi N, Kurinczuk JJ, Keogh JM, et al. Intrapartum risk factors for newborn encephalopathy: the Western Australian case-control study. BMJ. 1998;317(7172):1554-1558.
102. Nelson KB, Leviton A. How much of neonatal encephalopathy is due to birth asphyxia? Am J Dis Child. 1991;145(11):1325-1331.
103. Lundgren C, Brudin L, Wanby AS, Blomberg M. Ante- and intrapartum risk factors for neonatal hypoxic ischemic encephalopathy. J Matern Fetal Neonatal Med. 2017:1-7.
104. Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clin-ical and electroencephalographic study. Arch Neurol. 1976;33(10):696-705.
105. Levene MI, Sands C, Grindulis H, Moore JR. Comparison of two methods of predicting outcome in perinatal asphyxia. Lancet. 1986;1(8472):67-69.
106. van Handel M, Swaab H, de Vries LS, Jongmans MJ. Long-term cognitive and behavioral consequences of neonatal encephalopathy following perinatal as-phyxia: a review. Eur J Pediatr. 2007;166(7):645-654.
107. Jonsson M, Agren J, Norden-Lindeberg S, Ohlin A, Hanson U. Neonatal enceph-alopathy and the association to asphyxia in labor. Am J Obstet Gynecol. 2014;211(6):667 e661-668.
108. Nelson DB, Lucke AM, McIntire DD, Sanchez PJ, Leveno KJ, Chalak LF. Ob-stetric antecedents to body-cooling treatment of the newborn infant. Am J Obstet Gynecol. 2014;211(2):155 e151-156.
109. Martinez-Biarge M, Diez-Sebastian J, Wusthoff CJ, Mercuri E, Cowan FM. An-tepartum and intrapartum factors preceding neonatal hypoxic-ischemic enceph-alopathy. Pediatrics. 2013;132(4):e952-959.
110. Locatelli A, Incerti M, Paterlini G, et al. Antepartum and intrapartum risk factors for neonatal encephalopathy at term. Am J Perinatol. 2010;27(8):649-654.
111. Blomberg MI, Kallen B. Maternal obesity and morbid obesity: the risk for birth defects in the offspring. Birth Defects Res A Clin Mol Teratol. 2010;88(1):35-40.
112. Hildebrand E, Kallen B, Josefsson A, Gottvall T, Blomberg M. Maternal obesity and risk of Down syndrome in the offspring. Prenat Diagn. 2014;34(4):310-315.
78
113. Cedergren MI. Maternal morbid obesity and the risk of adverse pregnancy out-come. Obstet Gynecol. 2004;103(2):219-224.
114. Singh J, Huang CC, Driggers RW, et al. The impact of pre-pregnancy body mass index on the risk of gestational diabetes. J Matern Fetal Neonatal Med. 2012;25(1):5-10.
115. Cnattingius S, Villamor E, Johansson S, et al. Maternal obesity and risk of pre-term delivery. JAMA. 2013;309(22):2362-2370.
116. Woolner AM, Bhattacharya S. Obesity and stillbirth. Best Pract Res Clin Obstet Gynaecol. 2015;29(3):415-426.
117. Ovesen P, Rasmussen S, Kesmodel U. Effect of prepregnancy maternal over-weight and obesity on pregnancy outcome. Obstet Gynecol. 2011;118(2 Pt 1):305-312.
118. Usha Kiran TS, Hemmadi S, Bethel J, Evans J. Outcome of pregnancy in a woman with an increased body mass index. BJOG. 2005;112(6):768-772.
119. Scott-Pillai R, Spence D, Cardwell CR, Hunter A, Holmes VA. The impact of body mass index on maternal and neonatal outcomes: a retrospective study in a UK obstetric population, 2004-2011. BJOG. 2013;120(8):932-939.
120. Siega-Riz AM, Siega-Riz AM, Laraia B. The implications of maternal over-weight and obesity on the course of pregnancy and birth outcomes. Matern Child Health J. 2006;10(5 Suppl):S153-156.
121. Carlhall S, Kallen K, Blomberg M. Maternal body mass index and duration of labor. Eur J Obstet Gynecol Reprod Biol. 2013;171(1):49-53.
122. Minsart AF, Buekens P, De Spiegelaere M, Englert Y. Neonatal outcomes in obese mothers: a population-based analysis. BMC Pregnancy Childbirth. 2013;13:36.
123. Zhu T, Tang J, Zhao F, Qu Y, Mu D. Association between maternal obesity and offspring Apgar score or cord pH: a systematic review and meta-analysis. Sci Rep. 2015;5:18386.
124. Persson M, Johansson S, Villamor E, Cnattingius S. Maternal overweight and obesity and risks of severe birth-asphyxia-related complications in term infants: a population-based cohort study in Sweden. PLoS Med. 2014;11(5):e1001648.
125. Johansson S, Villamor E, Altman M, Bonamy AK, Granath F, Cnattingius S. Maternal overweight and obesity in early pregnancy and risk of infant mortality: a population based cohort study in Sweden. BMJ. 2014;349:g6572.
126. Berglund S, Grunewald C, Pettersson H, Cnattingius S. Risk factors for asphyxia associated with substandard care during labor. Acta Obstet Gynecol Scand. 2010;89(1):39-48.
127. Kappel B, Eriksen G, Hansen KB, et al. Short stature in Scandinavian women. An obstetrical risk factor. Acta Obstet Gynecol Scand. 1987;66(2):153-158.
128. Tsu VD. Maternal height and age: risk factors for cephalopelvic disproportion in Zimbabwe. Int J Epidemiol. 1992;21(5):941-946.
129. Sandstrom A, Cnattingius S, Wikstrom AK, Stephansson O. Labour dystocia--risk of recurrence and instrumental delivery in following labour--a population-based cohort study. BJOG. 2012;119(13):1648-1656.
130. Kjaergaard H, Dykes AK, Ottesen B, Olsen J. Risk indicators for dystocia in low-risk nulliparous women: a study on lifestyle and anthropometrical factors. J Obstet Gynaecol. 2010;30(1):25-29.
131. Sheiner E, Levy A, Katz M, Mazor M. Short stature--an independent risk factor for Cesarean delivery. Eur J Obstet Gynecol Reprod Biol. 2005;120(2):175-178.
132. Hayes BC, McGarvey C, Mulvany S, et al. A case-control study of hypoxic-ischemic encephalopathy in newborn infants at >36 weeks gestation. Am J Ob-stet Gynecol. 2013;209(1):29 e21-29 e19.

79
133. Tikkanen M. Placental abruption: epidemiology, risk factors and consequences. Acta Obstet Gynecol Scand. 2011;90(2):140-149.
134. English FA, Kenny LC, McCarthy FP. Risk factors and effective management of preeclampsia. Integr Blood Press Control. 2015;8:7-12.
135. Lin MG. Umbilical cord prolapse. Obstet Gynecol Surv. 2006;61(4):269-277. 136. Ofir K, Sheiner E, Levy A, Katz M, Mazor M. Uterine rupture: risk factors and
pregnancy outcome. Am J Obstet Gynecol. 2003;189(4):1042-1046. 137. Hesselman S, Hogberg U, Ekholm-Selling K, Rassjo EB, Jonsson M. The risk
of uterine rupture is not increased with single- compared with double-layer clo-sure: a Swedish cohort study. BJOG. 2015;122(11):1535-1541.
138. Kaczmarczyk M, Sparen P, Terry P, Cnattingius S. Risk factors for uterine rup-ture and neonatal consequences of uterine rupture: a population-based study of successive pregnancies in Sweden. BJOG. 2007;114(10):1208-1214.
139. Baskett TF. Shoulder dystocia. Best Pract Res Clin Obstet Gynaecol. 2002;16(1):57-68.
140. Sheiner E, Levy A, Hershkovitz R, et al. Determining factors associated with shoulder dystocia: a population-based study. Eur J Obstet Gynecol Reprod Biol. 2006;126(1):11-15.
141. Gherman RB. Shoulder dystocia: prevention and management. Obstet Gynecol Clin North Am. 2005;32(2):297-305, x.
142. Lopez E, de Courtivron B, Saliba E. [Neonatal complications related to shoulder dystocia]. J Gynecol Obstet Biol Reprod (Paris). 2015;44(10):1294-1302.
143. Gherman RB, Chauhan S, Ouzounian JG, Lerner H, Gonik B, Goodwin TM. Shoulder dystocia: the unpreventable obstetric emergency with empiric manage-ment guidelines. Am J Obstet Gynecol. 2006;195(3):657-672.
144. Svenska neonatlföreningen. http://neo.barnlakarforeningen.se/wp-content/uplo-ads/sites/14/2014/03/hypotermi.
145. National Board of Health and Welfare (Socialstyrelsen). www.socialstyrel-sen.se/register/halsodataregister Swedish Medical Birth Register. Swedish Neo-natal Quality Register.
146. Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical re-search. Eur J Epidemiol. 2009;24(11):659-667.
147. Swedish National Board of Health and Welfare (Socialstyrelsen). The Swedish Medical Birth Register. A summary of content and quality. 2003:112-113.
148. Cnattingius S, Ericson A, Gunnarskog J, Kallen B. A quality study of a medical birth registry. Scand J Soc Med. 1990;18(2):143-148.
149. O'Brien YM, Murphy DJ. The reliability of foetal blood sampling as a test of foetal acidosis in labour. Eur J Obstet Gynecol Reprod Biol. 2013;167(2):142-145.
150. Elvander C, Ekeus C, Gemzell-Danielsson K, Cnattingius S. Reason for the in-creasing use of vacuum extraction in Sweden: a population-based study. Acta Obstet Gynecol Scand. 2013;92(10):1175-1182.
151. Ray A, Hildreth A, Esen UI. Morbid obesity and intra-partum care. J Obstet Gynaecol. 2008;28(3):301-304.
152. Bramadat IJ, Driedger M. Satisfaction with childbirth: theories and methods of measurement. Birth. 1993;20(1):22-29.
153. Goodman P, Mackey MC, Tavakoli AS. Factors related to childbirth satisfaction. J Adv Nurs. 2004;46(2):212-219.
154. Christiaens W, Bracke P. Assessment of social psychological determinants of satisfaction with childbirth in a cross-national perspective. BMC Pregnancy Childbirth. 2007;7:26.

80
155. Lavender T, Walkinshaw SA, Walton I. A prospective study of women's views of factors contributing to a positive birth experience. Midwifery. 1999;15(1):40-46.
156. Hodnett ED, Simmons-Tropea DA. The Labour Agentry Scale: psychometric properties of an instrument measuring control during childbirth. Res Nurs Health. 1987;10(5):301-310.
157. DiMatteo MR, Kahn KL, Berry SH. Narratives of birth and the postpartum: anal-ysis of the focus group responses of new mothers. Birth. 1993;20(4):204-211.
158. Benjamin SJ, Daniel AB, Kamath A, Ramkumar V. Anthropometric measure-ments as predictors of cephalopelvic disproportion: Can the diagnostic accuracy be improved? Acta Obstet Gynecol Scand. 2012;91(1):122-127.
159. Zhang X, Decker A, Platt RW, Kramer MS. How big is too big? The perinatal consequences of fetal macrosomia. Am J Obstet Gynecol. 2008;198(5):517 e511-516.
160. Group HSCR. Hyperglycaemia and Adverse Pregnancy Outcome (HAPO) Study: associations with maternal body mass index. BJOG. 2010;117(5):575-584.
161. Sewell MF, Huston-Presley L, Super DM, Catalano P. Increased neonatal fat mass, not lean body mass, is associated with maternal obesity. Am J Obstet Gy-necol. 2006;195(4):1100-1103.
162. Philipps AF, Widness JA, Garcia JF, Raye JR, Schwartz R. Erythropoietin ele-vation in the chronically hyperglycemic fetal lamb. Proc Soc Exp Biol Med. 1982;170(1):42-47.
163. Stonestreet BS, Widness JA, Berard DJ. Circulatory and metabolic effects of hypoxia in the hyperinsulinemic ovine fetus. Pediatr Res. 1995;38(1):67-75.
164. Teramo KA, Widness JA. Increased fetal plasma and amniotic fluid erythropoi-etin concentrations: markers of intrauterine hypoxia. Neonatology. 2009;95(2):105-116.
165. Sebire NJ, Jolly M, Harris JP, et al. Maternal obesity and pregnancy outcome: a study of 287,213 pregnancies in London. Int J Obes Relat Metab Disord. 2001;25(8):1175-1182.
166. McGuinness BJ, Trivedi AN. Maternal height as a risk factor for Caesarean sec-tion due to failure to progress in labour. Aust N Z J Obstet Gynaecol. 1999;39(2):152-154.
167. Allen VM, Baskett TF, O'Connell CM, McKeen D, Allen AC. Maternal and per-inatal outcomes with increasing duration of the second stage of labor. Obstet Gynecol. 2009;113(6):1248-1258.
168. Cheng YW, Hopkins LM, Laros RK, Jr., Caughey AB. Duration of the second stage of labor in multiparous women: maternal and neonatal outcomes. Am J Obstet Gynecol. 2007;196(6):585 e581-586.
169. Solheim KN, Esakoff TF, Little SE, Cheng YW, Sparks TN, Caughey AB. The effect of cesarean delivery rates on the future incidence of placenta previa, pla-centa accreta, and maternal mortality. J Matern Fetal Neonatal Med. 2011;24(11):1341-1346.
170. Ayres-de-Campos D. Obesity and the challenges of caesarean delivery: preven-tion and management of wound complications. Best Pract Res Clin Obstet Gy-naecol. 2015;29(3):406-414.
171. Smith GC, Pell JP, Pasupathy D, Dobbie R. Factors predisposing to perinatal death related to uterine rupture during attempted vaginal birth after caesarean section: retrospective cohort study. BMJ. 2004;329(7462):375.

81
172. Kwee A, Bots ML, Visser GH, Bruinse HW. Obstetric management and outcome of pregnancy in women with a history of caesarean section in the Netherlands. Eur J Obstet Gynecol Reprod Biol. 2007;132(2):171-176.
173. Colmorn LB, Langhoff-Roos J, Jakobsson M, et al. National rates of uterine rup-ture are not associated with rates of previous caesarean delivery: results from the Nordic Obstetric Surveillance Study. Paediatr Perinat Epidemiol. 2017;31(3):176-182.
174. Wiberg N, Kallen K, Herbst A, Aberg A, Olofsson P. Lactate concentration in umbilical cord blood is gestational age-dependent: a population-based study of 17 867 newborns. BJOG. 2008;115(6):704-709.
175. Huskisson EC. Measurement of pain. Lancet. 1974;2(7889):1127-1131. 176. Waldenstrom U. Why do some women change their opinion about childbirth
over time? Birth. 2004;31(2):102-107. 177. Brunner Huber LR. Validity of self-reported height and weight in women of re-
productive age. Matern Child Health J. 2007;11(2):137-144. 178. East CE, Kane SC, Davey MA, Kamlin CO, Brennecke SP, Flamingo Study G.
Protocol for a randomised controlled trial of fetal scalp blood lactate measure-ment to reduce caesarean sections during labour: the Flamingo trial [ACTRN12611000172909]. BMC Pregnancy Childbirth. 2015;15:285.
179. Neilson JP. Fetal electrocardiogram (ECG) for fetal monitoring during labour. Cochrane Database Syst Rev. 2015(12):CD000116.
180. Group IC. Computerised interpretation of fetal heart rate during labour (IN-FANT): a randomised controlled trial. Lancet. 2017;389(10080):1719-1729.
181. Lowe B, Beckmann M. Involving the consultant before fetal blood sampling. Aust N Z J Obstet Gynaecol. 2016;56(4):387-390.

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1435
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-340782
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018
Related Documents