Bioterrorism Agents: Smallpox, Bioterrorism Agents: Smallpox, Botulism, and Tularemia Botulism, and Tularemia Jeff Kuper, Pharm.D., BCPS Jeff Kuper, Pharm.D., BCPS Clinical Associate Professor Clinical Associate Professor Ernest Mario School of Ernest Mario School of Pharmacy Pharmacy Rutgers, The State University Rutgers, The State University of New Jersey of New Jersey

Bioterrorism Agents: Smallpox, Botulism, and Tularemia Jeff Kuper, Pharm.D., BCPS Clinical Associate Professor Ernest Mario School of Pharmacy Rutgers,
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Bioterrorism Agents: Bioterrorism Agents: Smallpox, Botulism, and Smallpox, Botulism, and TularemiaTularemia
Jeff Kuper, Pharm.D., BCPSJeff Kuper, Pharm.D., BCPSClinical Associate ProfessorClinical Associate ProfessorErnest Mario School of PharmacyErnest Mario School of PharmacyRutgers, The State University of Rutgers, The State University of New JerseyNew Jersey

OutlineOutline
DiseasesDiseases SmallpoxSmallpox BotulismBotulism TularemiaTularemia
TopicsTopics HistoryHistory EpidemiologyEpidemiology ManifestationsManifestations DiagnosisDiagnosis Prevention and Prevention and
treatmenttreatment

SmallpoxSmallpoxVariola VirusVariola Virus

SmallpoxSmallpoxHistoryHistory
1754-67: British distribute blankets used by 1754-67: British distribute blankets used by smallpox patients to Native Americans during smallpox patients to Native Americans during the French and Indian Warsthe French and Indian Wars
1796: Edward Jenner demonstrates that 1796: Edward Jenner demonstrates that deliberate infection with cowpox protects deliberate infection with cowpox protects people from smallpox, introducing the people from smallpox, introducing the practice of “vaccination”practice of “vaccination”
1967-77: WHO campaign to eradicate 1967-77: WHO campaign to eradicate smallpoxsmallpox
1980: WHO recommends transfer of all 1980: WHO recommends transfer of all remaining variola virus to two reference labsremaining variola virus to two reference labs

SmallpoxSmallpoxEpidemiologyEpidemiology
Person-to-person transmissionPerson-to-person transmission– Aerosol dropletsAerosol droplets– Direct contact with lesions or contaminated Direct contact with lesions or contaminated
clothing, bedding, etc.clothing, bedding, etc. Transmission usually slower than Transmission usually slower than
chickenpoxchickenpox– Not contagious until rash appearsNot contagious until rash appears
Incubation period is typically 12-14 Incubation period is typically 12-14 daysdays

SmallpoxSmallpoxVariola MajorVariola Major
Initial presentation: high fever, prostration, Initial presentation: high fever, prostration, headache, backache, headache, backache, ± abdominal pain± abdominal pain
Maculopapular rash begins on the face and Maculopapular rash begins on the face and arms, spreading to the trunk and legsarms, spreading to the trunk and legs vesicles vesicles pustules pustules scabs over 7-10 days scabs over 7-10 days
Lesions in one area appear at same stageLesions in one area appear at same stage May leave residual scarringMay leave residual scarring
Complications: toxemia, encephalitisComplications: toxemia, encephalitis Mortality rate > 30% in the unvaccinatedMortality rate > 30% in the unvaccinated

Henderson DA. Henderson DA. JAMA JAMA 1999; 281:21271999; 281:2127

SmallpoxSmallpoxOther Clinical ManifestationsOther Clinical Manifestations
Hemorrhagic smallpoxHemorrhagic smallpox Malignant smallpoxMalignant smallpox Variola minorVariola minor In partially immune patients, the rash In partially immune patients, the rash
may be milder and more atypical and may be milder and more atypical and evolve more quicklyevolve more quickly

SmallpoxSmallpoxDiagnosisDiagnosis
Clinical diagnosis in the setting of a Clinical diagnosis in the setting of a known outbreakknown outbreak
Lab diagnosis requires biolevel 4 Lab diagnosis requires biolevel 4 facilityfacility– Sample vesicular fluid or scabSample vesicular fluid or scab– Characteristic appearance under an Characteristic appearance under an
electron microscopeelectron microscope– Culture and/or PCR for confirmationCulture and/or PCR for confirmation

SmallpoxSmallpoxChickenpox vs. SmallpoxChickenpox vs. Smallpox
ChickenpoxChickenpox SmallpoxSmallpox
ProdromeProdrome none or mildnone or mild pronouncedpronounced
Lesion typesLesion types superficial, different superficial, different stagesstages
deep-seated, same deep-seated, same stagestage
Lesion Lesion distributiondistribution
mostly on trunk, mostly on trunk, face; palms/soles face; palms/soles uncommonuncommon
mostly on face, mostly on face, extremities; extremities; palms/soles palms/soles commoncommon
Lesion Lesion evolutionevolution
rapidrapid slowslow
Systemic Systemic symptomssymptoms
minimalminimal toxic, moribundtoxic, moribund
From http://www.bt.cdc.gov/agent/smallpox/diagnosisFrom http://www.bt.cdc.gov/agent/smallpox/diagnosis

SmallpoxSmallpoxManagementManagement
Post-exposure vaccination: ring Post-exposure vaccination: ring vaccinationvaccination– For all contacts and emergency/essential For all contacts and emergency/essential
workersworkers– Vaccination within 4 days of exposure may Vaccination within 4 days of exposure may
prevent or reduce the severity of illnessprevent or reduce the severity of illness Isolation of persons with feverIsolation of persons with fever ? Cidofovir? Cidofovir

SmallpoxSmallpoxVaccineVaccine
Consists of live vaccinia virus (cowpox)Consists of live vaccinia virus (cowpox) DryvaxDryvax®® is the only FDA-licensed is the only FDA-licensed
vaccinevaccine– Other vaccines held in reserve by CDCOther vaccines held in reserve by CDC

SmallpoxSmallpoxVaccination MethodVaccination Method
Multiple-puncture technique using Multiple-puncture technique using bifurcated needlebifurcated needle– Needle prongs are calibrated to hold the Needle prongs are calibrated to hold the
correct dose when dipped into vaccine vialcorrect dose when dipped into vaccine vial Hold needle perpendicular to skin and Hold needle perpendicular to skin and
make rapid, vigorous puncturesmake rapid, vigorous punctures– Should see trace bloodShould see trace blood– 2-3 punctures for primary vaccination2-3 punctures for primary vaccination

SmallpoxSmallpoxVaccine “Take”Vaccine “Take”
From http://www.bt.cdc.gov/agent/smallpox/From http://www.bt.cdc.gov/agent/smallpox/

SmallpoxSmallpoxVaccine “Take”Vaccine “Take”
From http://www.bt.cdc.gov/agent/smallpox/From http://www.bt.cdc.gov/agent/smallpox/
TakeTake Non-TakeNon-Take

SmallpoxSmallpoxVaccine Site CareVaccine Site Care
Cover with gauze and semipermeable Cover with gauze and semipermeable dressing to decrease risk of transmission of dressing to decrease risk of transmission of vaccinia virusvaccinia virus– Vaccinia is shed from time lesion appears until Vaccinia is shed from time lesion appears until
scab falls offscab falls off Rate of transmission during the ’60s was 2-6 cases Rate of transmission during the ’60s was 2-6 cases
per 100,000 first-time vaccineesper 100,000 first-time vaccinees No evidence of respiratory transmissionNo evidence of respiratory transmission
– Routine infection control proceduresRoutine infection control procedures– Avoid direct contact with the vaccination siteAvoid direct contact with the vaccination site
Healthcare workers do NOT need to be Healthcare workers do NOT need to be furloughed from workfurloughed from work
SmallpoxSmallpoxRelative Vaccine Relative Vaccine ContraindicationsContraindications Atopic dermatitis or eczema (active or Atopic dermatitis or eczema (active or
history)*history)* Other active exfoliative skin Other active exfoliative skin
conditions*conditions* Immunosuppressive conditions*Immunosuppressive conditions*
– Steroid doses Steroid doses ≥ 2 mg/kg or 20 mg/day of ≥ 2 mg/kg or 20 mg/day of prednisone for > 2 weeks within past weekprednisone for > 2 weeks within past week
– Other immunosuppressive meds within Other immunosuppressive meds within past 3 weekspast 3 weeks
* Also contraindicated for household contacts* Also contraindicated for household contacts

SmallpoxSmallpoxRelative Vaccine Relative Vaccine ContraindicationsContraindications Pregnancy*Pregnancy* BreastfeedingBreastfeeding Infants < 1 year oldInfants < 1 year old Allergy to vaccine componentAllergy to vaccine component
– Including neomycin, tetracycline, Including neomycin, tetracycline, polymyxin B, streptomycin, glycerin, and polymyxin B, streptomycin, glycerin, and phenolphenol
?? Cardiac disease?? Cardiac disease
* Also contraindicated for household contacts* Also contraindicated for household contacts

SmallpoxSmallpoxExpected Vaccine ReactionsExpected Vaccine Reactions
0 20 40 60 80
Fatigue
Headache
Myalgias
Nausea
Chills
Fever
Vacc. Site Pain
Regional LAD
% Incidence
SE Frey et al. SE Frey et al. NEJM NEJM 2002; 346:1265-742002; 346:1265-74

SmallpoxSmallpoxVaccine ComplicationsVaccine Complications
Satellite lesionsSatellite lesions
Nonspecific rashesNonspecific rashes

SmallpoxSmallpoxVaccine ComplicationsVaccine Complications
Cases per million Cases per million vaccineesvaccinees
Non-life threateningNon-life threatening
Inadvertent inoculationInadvertent inoculation 25-52925-529
Generalized vacciniaGeneralized vaccinia 23-24223-242
Erythema multiformeErythema multiforme 165165
Life-threateningLife-threatening
EncephalitisEncephalitis 3-123-12
Progressive vacciniaProgressive vaccinia 1-21-2
Eczema vaccinatumEczema vaccinatum 10-3910-39
DeathDeath 1-21-2
MMWR MMWR 2003; 52(RR-4):92003; 52(RR-4):9

SmallpoxSmallpoxErythema MultiformeErythema Multiforme

SmallpoxSmallpoxInadvertent InoculationInadvertent Inoculation
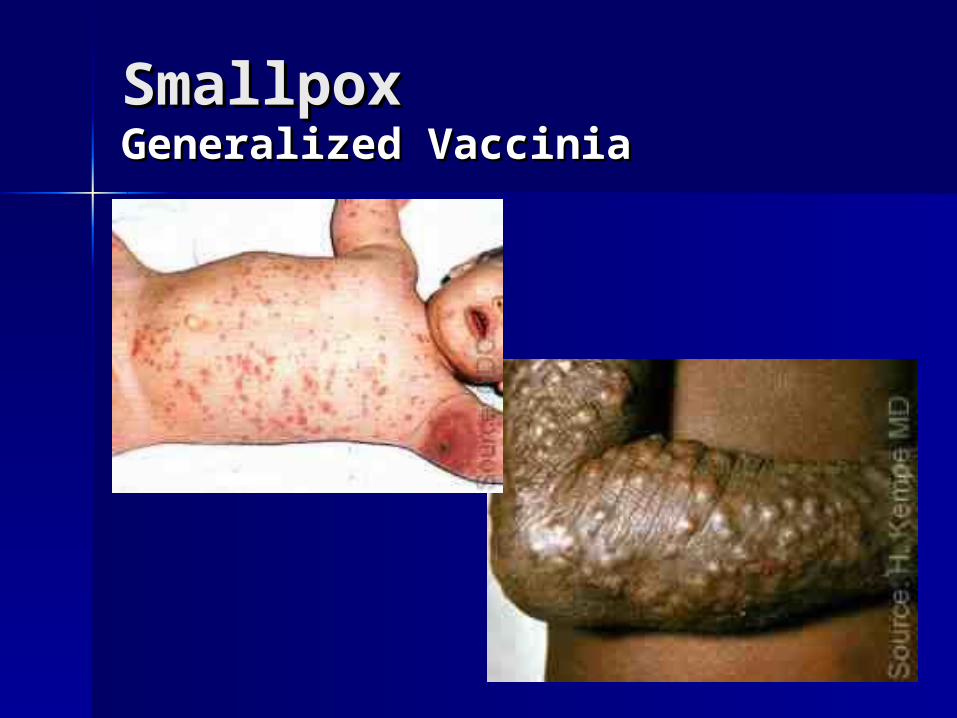
SmallpoxSmallpoxGeneralized VacciniaGeneralized Vaccinia

SmallpoxSmallpoxEczema VaccinatumEczema Vaccinatum

SmallpoxSmallpoxProgressive VacciniaProgressive Vaccinia

SmallpoxSmallpoxEncephalitis/EncephalomyelitisEncephalitis/Encephalomyelitis
Diagnosis of exclusionDiagnosis of exclusion Encephalitis in infants < 2yoEncephalitis in infants < 2yo
– Onset 6-10 days post-vaccinationOnset 6-10 days post-vaccination– Encephalomyelitis in older personsEncephalomyelitis in older persons
Onset 11-15 days post-vaccinationOnset 11-15 days post-vaccination
Mortality 25%, neurological sequelae Mortality 25%, neurological sequelae 25%25%
Management: supportive, symptomaticManagement: supportive, symptomatic

SmallpoxSmallpoxFetal VacciniaFetal Vaccinia

SmallpoxSmallpoxVaccinia ManagementVaccinia Management
Vaccinia immune globulin (VIG)Vaccinia immune globulin (VIG)– IndicationsIndications
Eczema vaccinatumEczema vaccinatum Progressive vacciniaProgressive vaccinia Generalized vaccinia (severe or Generalized vaccinia (severe or
immunocompromised)immunocompromised) Inadvertent inoculation (severe or Inadvertent inoculation (severe or
ocular other than keratitis)ocular other than keratitis)
– Dose: 100-500 mg/kg x 1Dose: 100-500 mg/kg x 1

SmallpoxSmallpoxVaccinia ManagementVaccinia Management
Topical trifluridine for ocular infectionTopical trifluridine for ocular infection Cidofovir (VistideCidofovir (Vistide®®))
– In vitro activity against orthopoxvirusesIn vitro activity against orthopoxviruses– Nephrotoxic—administer with Nephrotoxic—administer with
probenecid and hydrationprobenecid and hydration– Will be released by CDC as IND if:Will be released by CDC as IND if:
Patient fails VIG treatment Patient fails VIG treatment OROR Patient is near death Patient is near death OROR VIG supplies have been exhaustedVIG supplies have been exhausted

BotulismBotulismClostridium botulinum Clostridium botulinum toxintoxin
From “Todar’s Online Textbook of Bacteriology”From “Todar’s Online Textbook of Bacteriology”

BotulismBotulismHistoryHistory
1812: link recognized between sausage 1812: link recognized between sausage ((botulusbotulus in Latin) and paralytic illness in in Latin) and paralytic illness in GermanyGermany
1897: 1897: C. botulinum C. botulinum and associated toxin first and associated toxin first identifiedidentified
1930s: Japanese army feeds botulinum toxin 1930s: Japanese army feeds botulinum toxin to Chinese POWsto Chinese POWs
1990-95: Aum Shinrikyo cult disperses 1990-95: Aum Shinrikyo cult disperses aerosolized botulinum toxin at multiple sites in aerosolized botulinum toxin at multiple sites in Japan, but no illnesses resultJapan, but no illnesses result
1990s: Iraq produces 19,000 L of toxin, half of 1990s: Iraq produces 19,000 L of toxin, half of which is loaded into weaponswhich is loaded into weapons

BotulismBotulismEpidemiologyEpidemiology
Transmission from exposure of mucous Transmission from exposure of mucous membranes to spores or toxinmembranes to spores or toxin
Outbreaks most often associated with Outbreaks most often associated with home-canned vegetables, fruits, and fishhome-canned vegetables, fruits, and fish
12-72 hr. incubation period12-72 hr. incubation period Clues to intentional releaseClues to intentional release
– Large number of casesLarge number of cases– Unusual toxin typeUnusual toxin type– Simultaneous outbreaks with no common Simultaneous outbreaks with no common
sourcesource

BotulismBotulismClinical ManifestationsClinical Manifestations
Most poisonous substance knownMost poisonous substance known Toxin blocks acetylcholine release, Toxin blocks acetylcholine release,
resulting in flaccid muscle resulting in flaccid muscle paralysisparalysis
Disease formsDisease forms– Wound botulismWound botulism– Infant botulismInfant botulism– Foodborne botulismFoodborne botulism– Inhalational botulismInhalational botulism
man-mademan-made
naturalnatural

BotulismBotulismClinical ManifestationsClinical Manifestations
SymmetricSymmetric, , descendingdescending muscle weakness muscle weakness with prominent cranial nerve palsieswith prominent cranial nerve palsies– Acute onsetAcute onset– 4 D’s: diplopia, dysarthria, dysphonia, 4 D’s: diplopia, dysarthria, dysphonia,
dysphagiadysphagia– May later involve autonomic system (e.g., May later involve autonomic system (e.g.,
bradycardia, hypotension, hypothermia, bradycardia, hypotension, hypothermia, urinary retention)urinary retention)
AfebrileAfebrile No cognitive or sensory defects (other No cognitive or sensory defects (other
than blurred vision)than blurred vision)

BotulismBotulismDiagnosisDiagnosis
Testing only available in specialty Testing only available in specialty labslabs– Mouse bioassay of blood, stool, vomit, Mouse bioassay of blood, stool, vomit,
food for toxin (results in 1-2 days)food for toxin (results in 1-2 days)– Culture of stool (results in 7-10 days)Culture of stool (results in 7-10 days)
ElectromyogramElectromyogram Common misdiagnoses: Guillain-Common misdiagnoses: Guillain-
BarrBarréé syndrome, myasthenia gravis, syndrome, myasthenia gravis, stroke, intoxication, tick paralysisstroke, intoxication, tick paralysis

BotulismBotulismEquine Antitoxin TreatmentEquine Antitoxin Treatment
Give as soon as diagnosis made to Give as soon as diagnosis made to decrease severity and further damagedecrease severity and further damage– Does NOT reverse existing paralysisDoes NOT reverse existing paralysis
Available from CDC via state health Available from CDC via state health depts.depts.
Antibodies against toxins A, B, and EAntibodies against toxins A, B, and E Dose: 1 10-mL vial given by IV infusion Dose: 1 10-mL vial given by IV infusion
+ 2+ 2ndnd vial given IM vial given IM– First skin test and desensitize if necessaryFirst skin test and desensitize if necessary

BotulismBotulismSupportive TreatmentSupportive Treatment
Fluid and nutrition supportFluid and nutrition support Mechanical ventilationMechanical ventilation Antibiotics for secondary infectionsAntibiotics for secondary infections
– Avoid aminoglycosides, tetracyclines, and Avoid aminoglycosides, tetracyclines, and clindamycinclindamycin
? Role for activated charcoal? Role for activated charcoal ? Botulism immune globulin (BIG)? Botulism immune globulin (BIG)

TularemiaTularemiaFrancisella tularensisFrancisella tularensis
From From http://www.denniskunkel.com/http://www.denniskunkel.com/

TularemiaTularemiaEpidemiologyEpidemiology
MMWR MMWR 2002; 51:1832002; 51:183

TularemiaTularemiaEpidemiologyEpidemiology
Routes of human transmissionRoutes of human transmission– Bites by infected insectsBites by infected insects– Handling infectious animalsHandling infectious animals– Contact with infected food, water, soilContact with infected food, water, soil– Aerosol inhalationAerosol inhalation– NOT contagious from person to personNOT contagious from person to person
Clues to intentional releaseClues to intentional release– Abrupt onset of large numbers of people with Abrupt onset of large numbers of people with
febrile, mild respiratory illness, many of whom febrile, mild respiratory illness, many of whom progress to life-threatening pneumonitis progress to life-threatening pneumonitis ± sepsis± sepsis
– Young, healthy people affectedYoung, healthy people affected– Multiple cases in urban settingMultiple cases in urban setting

TularemiaTularemiaClinical ManifestationsClinical Manifestations
Ulceroglandular, glandular, oculoglandular Ulceroglandular, glandular, oculoglandular diseasedisease
Oropharyngeal tularemiaOropharyngeal tularemia Pneumonic tularemiaPneumonic tularemia Typhoidal tularemiaTyphoidal tularemia Septic tularemiaSeptic tularemia

TularemiaTularemiaDiagnosisDiagnosis
Routine Gram staining and culturing Routine Gram staining and culturing will miss tularemiawill miss tularemia
Direct microscopic examination of Direct microscopic examination of infected fluids or tissuesinfected fluids or tissues
Confirmed by special culture mediaConfirmed by special culture media– Results may take 10 daysResults may take 10 days– Special safety precautions necessarySpecial safety precautions necessary
Other tests available at reference Other tests available at reference labslabs

TularemiaTularemiaTreatmentTreatment
Preferred: streptomycin 1 Gm IM Preferred: streptomycin 1 Gm IM q12h q12h OROR gentamicin 5 mg/kg gentamicin 5 mg/kg IV/IM q24hIV/IM q24h
Alternatives:Alternatives:– Doxycycline 100 mg IV/PO q12hDoxycycline 100 mg IV/PO q12h– Ciprofloxacin 400 mg IV q12h Ciprofloxacin 400 mg IV q12h OROR
500 mg PO q12h 500 mg PO q12h– Chloramphenicol 15 mg/kg IV q6hChloramphenicol 15 mg/kg IV q6h

TularemiaTularemiaTreatmentTreatment
Duration of therapy: Duration of therapy: – Aminoglycoside or quinolone: 10 daysAminoglycoside or quinolone: 10 days– Doxycycline or chloramphenicol: 14-21 daysDoxycycline or chloramphenicol: 14-21 days– Mass casualty setting (Rx entirely PO): 14 Mass casualty setting (Rx entirely PO): 14
daysdays Pediatrics: Pediatrics:
– Same agents as for adultsSame agents as for adults– Strepto., gent., doxy., cipro. dosing as for Strepto., gent., doxy., cipro. dosing as for
plagueplague– Chloramphenicol 15 mg/kg q6hChloramphenicol 15 mg/kg q6h

TularemiaTularemiaProphylaxisProphylaxis
Live, attenuated vaccine is not currently Live, attenuated vaccine is not currently availableavailable– Previously available to lab workers, others at high Previously available to lab workers, others at high
riskrisk– Would NOT be useful as post-exposure prophylaxisWould NOT be useful as post-exposure prophylaxis
Post-exposure antibioticsPost-exposure antibiotics– Recommended for persons known to have had Recommended for persons known to have had
high-risk exposures and who are identified during high-risk exposures and who are identified during incubation periodincubation period
Oral doxycycline or ciprofloxacin x 14 daysOral doxycycline or ciprofloxacin x 14 days
– If exposure is unclear, start treatment for persons If exposure is unclear, start treatment for persons who develop fever or flu-like illness within 14 dayswho develop fever or flu-like illness within 14 days
Related Documents











