. 1 BIOPROGRESSIVE THERAPY PRESENTED BY : Presented by: Dr. Lavesh Pandey ▪Management umbrella ▪Principles of the Bioprogressive therapy ▪Visual treatment objective or V.T.O BIOPROGRESSIVE THERAPY Developed by : Dr Robert Murray Ricketts ▪ It takes advantage of biological progressions including growth, development and function and directs them in a fashion that normalizes function and enhances aesthetic effect. ▪It accepts as its mission the treatment of the total face rather than narrower objective of the teeth or occlusion. Management umbrella Management of the total practice ultimately determines the degree of efficiency and effectiveness with which the orthodontist solves individual patient problems. Knowlegde of theory + skilled application of technique + administrative efficiency = Success Technical systems cannot function efficiently and have longevity unless they operate under a total management system or umbrella. The management system should increase all of the following at same time : A .Quality B .Quantity C . Effectiveness Management umbrella ➢ PLANNING ➢ ORGANIZING ➢ LEADING ➢ CONTROLLING

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

.
1
BIOPROGRESSIVE THERAPY
PRESENTED BY :
Presented by: Dr. Lavesh Pandey
▪Management umbrella
▪Principles of the Bioprogressive therapy
▪Visual treatment objective or V.T.O
BIOPROGRESSIVE THERAPY
Developed by : Dr Robert Murray Ricketts
▪ It takes advantage of biological progressions including growth,
development and function and directs them in a fashion that
normalizes function and enhances aesthetic effect.
▪It accepts as its mission the treatment of the total face rather than
narrower objective of the teeth or occlusion.
Management umbrella
Management of the total practice ultimately determines the degree of
efficiency and effectiveness with which the orthodontist solves
individual patient problems.
Knowlegde of theory + skilled application of technique +
administrative efficiency = Success
Technical systems cannot function efficiently and have longevity
unless they operate under a total management system or umbrella.
The management system should increase all of the following at same
time :
A .Quality
B .Quantity
C . Effectiveness
Management umbrella
➢ PLANNING
➢ ORGANIZING
➢ LEADING
➢ CONTROLLING

.
2
PLANNING
1.Forecast - Normal growth
2.Deveolp Objectives - Indiviual treatment objective
3.Program - Sequence of mechanics to achieve
objectives
4.Scheduling - Average time for mechanics to function
5.Budget - Fee for case
PRINCIPLES OF THE BIOPROGRESSIVE THERAPY
Ten principles have been developed in an attempt to communicate
an understanding of the mechanical procedures that bio progressive
therapy may use in developing a treatment plan , including appliance
selection and application , specific to each individual patient.
1.The use of systems approach to diagnosis and treatment by application
of the visual treatment objective in planning treatment , evaluating
anchorage and monitoring results.
In 2 year 70% of change is because of treatment and 30 % of change
are due to growth
V.T.O
Allows orthodontist to visualize the changes that should occur .
and to prescribe the necessary treatment to cause it to happen.
Helps in understanding the interrelationship of various changing parts
and the influence that one area has upon another.

.
3
Five areas of superimposition and analysis have been selected to
evaluate the changes that have forecast to visualize the difference
between the expected growth and proposed treatment alterations.
Seven areas of evaluation are used to determine the major moves
needed to accomplish the forecast objective and to design treatment
with a priority sequence for quality results and maximum efficiency
2. Torque control throughout treatment
Most of techniques allow more freedom of movement of tooth by
using round wires .
Bio.prog therapy suggest that movement of teeth can be
more efficient and various treatment procedures more effectively
carried through when control of direction of root movement
available.
Four situation where torque control of root is necessary
• Keep roots in vascular trabecular bone during initial stages
• Place roots in dense cortical bone for anchorage
• Torque to remodel cortical bone for U/L incisor retraction
• Torque to position teeth in final occlusion
3.Muscular and cortical bone anchorage
Anchorage here is considered in terms of stabilizing the
molars and positioning teeth against movement during various stages
of orthodontic treatment.
• Upper arch –Masseter and Temporalis
Facial Type
According to lower facial height angle
cortical bone anchorage
cortical bone is more dense and laminated with very limited
blood supply therefore the physiological process is delayed and
tooth movement is slow .
• U/L molar anchorage increased by Expansion
•Tooth movement can be enhanced by understanding the position of
cortical bone .
4. Movement of all teeth in any direction with proper application of
pressure.
•Rate of tooth movement is dependent on blood supply that sustains
the physiological action that takes place within bone
•Brain lee ,suggested that the most efficient force for tooth movement
is based upon the size of the root surface of the tooth to be moved
which he called as enface root surface or the portion of root that is in
the direction of tooth movement .
• He expressed this value as 200 gm/sq.cm of root surface area
Bio prog therapy suggest as 100gm/sq.cm

.
4
•Density of bone is also an influencing factor movement through
cortical bone require even less forces.
.016 x .016 chrome alloy archwires ,with designs ,that allow more
wire through spanning arches , sectional arches , or multiple loops
have been found to apply light continuous forces
5.Orthopedic alteration
Orthopedic forces changes the relationship of the basic supporting
for jaw structure contrasted to tooth movement in localized area .
It also affects areas associated with supporting structures like
condyles of mandible and palatal plates of maxilla Ex ; Headgear ,
RME
• Headgear according to facial type
6. Treat the overbite before the overjet correction
Most malocclusion , have a deep incisor bite relationship as in
. class II div 1 and div 2
For stability in function and retention it is vital to correct deep
bite so as to get proper overjet ,overbite and inter incisal relationship
Methods of Deep bite correction – A. Extrusion of posterior teeth
(unstable)
B. Intrusion of anterior teeth
Extrusion of Posterior teeth – 1 Vertical growth pattern
(increases anterior facial height)
2 Horizontal
(resist molar extrusion)
•Bio .prog therapy considers incisor intrusion as treatment of choice
• If deep bite is not corrected before overjet correction ?
Interference during retraction leads to limited occlusion and causes
extrusion of posteriors
• Spanning arch - Utility arch
It stabilizes the buccal occlusion and apply light continous force for
incisor intrusion
7. Sectional arch therapy
In continuous arch the force and leveraging action to move
malposed teeth comes primarily from the adjacent tooth along
the arch and , because of the short span between their brackets ,
very heavy forces of a short duration are usually applied.
In sectional arch treatment the arches are broken into sections or
segments in order that the application of force in direction and
amount will be of more benefit in efficient movements of the
teeth.
Four benefits of sectional arch treatment
1 It allows lighter continuous forces to be directed to the
individual teeth.
utility intrusion arch , class II elastic , cuspid retraction
2 More effective root control in the basic tooth movement
For intrusion – Roots of lower incisor ,
Root of cuspid need separate torque

.
5
3. Supplements maxillary orthopedic alteration.
4 Reduces the binding and friction of the brackets along arch wire
8. Concept of overtreatment
It is necessary for the clinician not only to appreciate the changes to
bring the teeth into properly aligned functional occlusion , but to
anticipate changes that follow when all the appliances are removed
and post treatment adjustments begin to occur.
Bio prog therapy suggest four areas where the concept of
overtreatment may help :
1 To overcome the muscular forces against the tooth surfaces
• Narrow upper arches,
• Anterior open bite ,
• Upper anterior protrusion due to lip sucking.
2 Root movements needed for stability:
Deep bite ,Paralleling of roots
adjacent to extraction sites , Severe rotations
3 To overcome orthopedic rebound as heavy forces are eliminated ,
the basic supportive structures may rebound.
4 To allow settling in retention over treatment of the individual teeth
within the arches allows them to settle into a functioning occlusion.
9. Unlocking the malocclusion in a progressive sequence of
treatment in order to establish or restore more normal function
1 To describe the malocclusion and visualize the position of the teeth
in terms of what functional influences have been responsible for their
present form .
2 To describe the facial type and skeletal structure .
3 To describe the present abnormal functional influences upon dental
arches , or the lack of abnormal development by default
Ex: Upper arch expansion , Incisor protrusion correction,
TMJ problems
10. Efficiency in treatment with quality results, utilizing a concept of
prefabrication of appliances .
Allows the clinician to direct his energies in details of appliance
application, diagnosis and treatment planning.
VISUAL TREATMENT OBJECTIVE
(V.T .O)

.
6
V.T.O
“Blue print for building a house”
▪ Its a visual plan to forecast the normal growth of the patient , so as
to establish the individual objectives for that patient .
▪Helps orthodontist to take advantage of growth .
▪ Valuable for orthodontist in self improvement.

.
1
BURSTONE ANALYSIS
CEPHALOMETRICS FOR ORTHOGNATHIC SURGERY
[COGS ANALYSIS]
GIVEN BY CHARLES.J.BURSTONE
AT UNIVERSITY OF CONNECTICUT
Presented by: Dr. Lavesh Pandey
2
• Sample:
– From child research council of the university of
colorado school of medicine.
• Size: 30. ‘14 M’ and ‘16 F’
• Characteristic: longitudinal
• Race: cacausian
• Age: 5 – 20.
3
Burstone Analysis
Hard tissue Analysis Soft tissue Analysis
4
Characteristics of COGS
• The chosen landmarks and measurements can be altered by various surgical procedures.
• The comprehensive appraisal includes all of the facial bones and cranial base reference.
• Rectilinear measurements can be readily transferred to a study cast for mock surgery.
• Critical facial skeletal components are examined.
• Standard and statistics are available for variation in age and sex from 5 -20 on the basis of developmental age.
• COGS appraisal describes dental, skeletal and soft tissue variations.
5
LANDMARKS USED IN COGS
• SELLA (S)
• NASION (N)
• ARTICULARE (Ar)
• PTERYGO MAXILLARY FISSURE (Ptm)
• SUBSPINALE (Pt A)
• POGONION (Pog)
• SUPRAMENTALE (B)
• ANTERIOR NASAL SPINE (ANS)
• POSTERIOR NASAL SPINE (PNS)
• MENTON (Me)
• GNATHION (Gn)
• GONION (Go)
PLANES
.
2
7
Horizontal Plane:
• The base line for comparison for most the data in COGS analysis.
• Is a constructed plane called ‘Horizontal Plane’ which is a surrogate FH plane, constructed by drawing a line 7º from SN plane.
• Most measurements are made for projections either parallel or perpendicular to HP.
8
• Mandibular Plane: constructed from menton to gonion.
• Nasal Floor: plane constructed from ANS to PNS.
• Occlusal Plane: is a line drawn from te
buccal groove of the permanent first molar through a point 1mm with in the incisal edge of the central incisor in each arch.
Hard Tissue Analysis
10
Cranial Base:
• Ar- N:
– Skeletal base line for
corelating other
measurements.
– Relatively stable
anatomic plane.
– Can be changed by
cranial surgery or auto-
rotation of mandible.
11
• Ar-Ptm:
– Determines horizontal
distance between
maxilla and mandible
posteriorly.
– More the distance
between Ar-Ptm, more
the mandible lies
posterior to maxilla.
– Male- 37.1 ± 2.8mm
– Female- 32.8± 1.9mm
12
• Ptm-N:
– Determines the
horizontal end of
maxilla.
– Its less in cases of mid
facial deficiency, Class
III andCleft Palate.
– Male- 52.8 ± 4.1mm
– Female- 50. ± 3mm
.
3
13
Horizontal Skeletal Profile:
• N-A-Pg:
– Angle of convexity.
– Drawback: does not
indicate the jaw
involved.
– +ve –convex profile,
clockwise angle.
– -ve – concave profile,
counterclockwise
angle.
– Male: 3.9º ± 6.4º
– Female: 2.6º ± 5.1º
14
• N-A:
– Horizontal distance
from Pt A to
perpendicular from HP
through N.
– Describes whether
anterior part of maxilla
is protrusive / retrusive
– Male:0.0 ± 3.7mm
– Female: - 2 ± 3.7mm
15
N-B:
The horizontal distance of Pt B to the line perpendicular to HP through N gives N-B measurement.
Gives horizontal position of the apical base of mandible in relation to N in AP direction.
+ve value when Pt B and –ve value when Pt B is behind the perpendicular line.
Male: -5.3±6.7
Female: -6.9±4.316
• N-Pg:
• Indicates the prominence of the chin.
• Used in planning of genial augmentation or genial reduction.
• Male: -4.3±8.5mm
• Female: -6.5±5.1mm
17
Vertical (skeletal and dental)
• Vertical Skeletal:
– Anterior component
– Posterior component
• Vertical Dental:
– Anterior component
– Posterior component
18
Vertical skeletal
Anterior component
• N-ANS:– Represents middle
1/3rd facial height.
– Male:54.7±3.2mm
– Female:50.0±2.4mm
• ANS-Gn:– Represents lower 1/3rd
facial height.
– Male:68.6±3.8mm
– Female: 61.3±3.3mm
Posterior component:
• PNS-N:– Represents posterior
maxillary height.
– males:53.9±1.7mm
– Female:50.6±2.2mm
• MP-HP:– Represents posterior
facial divergence with anterior facial height.
– Males:23.0º±5.9º
– Females:24.2º±5.0º
.
4
19 20
Vertical dental:
ANTERIOR COMPONENT
• Upper CI- NF: Represents anterior maxillary dental height.
– Male: 30.5 ± 2.1mm
– Females: 27.5 ± 1.5mm
• Lower CI-MF: represents total vertical dimension of anterior mandible.
– Male: 45.0 ± 2.1mm
– Female: 40.8 ± 1.8mm
POSTERIOR COMPONENT
• Upper 1st molar-NF: Represents posterior maxillary dental vertical height.
– Males:26.2±2mm
– Female:23.0±1.3mm
• Lower 1st molar-MP: Represents Posterior vertical mandibular dental height.
– Males: 35.8±2.6mm
– Females:32.1±1.9mm
21
Maxilla and mandible:
Maxilla:
• PNS-ANS:– Gives the effective
length of maxilla.
– This distance with the ANS-N and PNS-N measurements gives a quantitative description of the maxilla in the skull complex
– Males:57.7±2.5mm
– Females:52.6±3.5mm
Mandible:
• Ar-Go (linear): – Gives quantitative
length of mandibular ramus.
– Males:52.0±4.2mm
– Females:46.8±2.5mm
• Go-Pg (linear):– Linear measurement of
mandibular body.
– Males:83.7±4.5mm
– Females:74.3±5.8mm
22
23
• Ar-Go-Gn: (gonial angle)– Represents relation
between mandibular
ramus and body.
– Males:119.1º ±5.1º
– Females:122.0º±6.9º
• B-Pg:
– Describes mandibular
chin prominence with
respect to mandibular
denture base.
– Males:8.9±1.7mm
– Females:7.2±1.9mm
24
Dental:
• Occlusal plane angle:
– Angle formed between OP plane and HP. If the teeth
overlap anteriorly to produce an overbite,the OP can be
drawn as a single line.
– If an anterior openbite is pesent then,Op passes through
a point 1 mm within the incisal edge the two Op must be
drawn and measured seperately for the angle with HP.
– Each OP is assessed as to its steepness or flatness
– Vertical facial and dental height must be assessed to
determine which OP should be corrected.
.
5
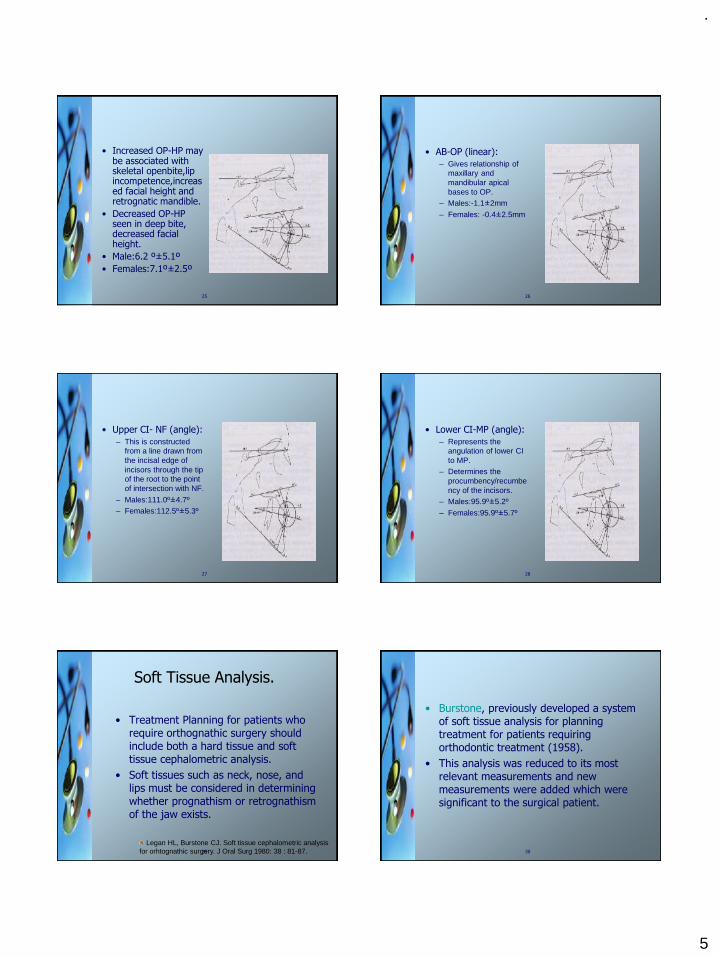
25
• Increased OP-HP may be associated with skeletal openbite,lip incompetence,increased facial height and retrognatic mandible.
• Decreased OP-HP seen in deep bite, decreased facial height.
• Male:6.2 º±5.1º
• Females:7.1º±2.5º
26
• AB-OP (linear):
– Gives relationship of
maxillary and
mandibular apical
bases to OP.
– Males:-1.1±2mm
– Females: -0.4±2.5mm
27
• Upper CI- NF (angle):
– This is constructed
from a line drawn from
the incisal edge of
incisors through the tip
of the root to the point
of intersection with NF.
– Males:111.0º±4.7º
– Females:112.5º±5.3º
28
• Lower CI-MP (angle):
– Represents the
angulation of lower CI
to MP.
– Determines the
procumbency/recumbe
ncy of the incisors.
– Males:95.9º±5.2º
– Females:95.9º±5.7º
29
Soft Tissue Analysis.
• Treatment Planning for patients who require orthognathic surgery should include both a hard tissue and soft tissue cephalometric analysis.
• Soft tissues such as neck, nose, and lips must be considered in determining whether prognathism or retrognathism of the jaw exists.
Legan HL, Burstone CJ. Soft tissue cephalometric analysis
for orhtognathic surgery. J Oral Surg 1980: 38 : 81-87. 30
• Burstone, previously developed a system of soft tissue analysis for planning treatment for patients requiring orthodontic treatment (1958).
• This analysis was reduced to its most relevant measurements and new measurements were added which were significant to the surgical patient.

.
6
31
• The means and standard deviations were derived from a population of 40 white adults(20 men and 20 women) between the ages of 20 and 30.
• All were orthodontically untreated patients with class I occlusions and had a vertical facial proportions that were determined to be within normal limits. (N-ANS / ANS-Me was
between 0.75 and 0.85)
32
Mesurement Landmarks Mean S.D
Facial Form
•Facial Convexity angle
G-Sn-Pg’ 12 4
•Maxillary Prognathism
G-Sn (HP) 6 3
•Mandibular Prognathism
G-Pg’ (HP) 0 4
•Vertical Height ratio G-Sn/Sn-Me’
(HP)
1 ---
•Lower face - Throat angle
Sn-Gn’-C 100 7
•Lower Vertical Height-Depth Ratio
Sn-Gn’/C-Gn’ 1.2 ---
Soft tissue analysis- Adult Standards
33
Mesurement Landmarks Mean S.D
Lip Position and Form
•Nasolabial Angle Cm-Sn-Ls 102 8
•Upper lip protrusion Ls to (Sn-Pg’) 3 1
•Lower lip protrusion Li to (Sn-Pg’) 2 1
•Mentolabial Sulcus Si to (Li-Pg’) 4 2
•Vertical lip-Chin Ratio
Sn-Stms/Stmi-Me’ 0.5 ---
•Maxillary incisor Exposure &
•Interlabial Gap
Stms – 1
&
Stms-Stmi
2
2
2
2
Soft tissue analysis- Adult Standards
34
Facial Form
• Facial Convexity Angle
( G-Sn-Pg’)
• Describes overall horizontal soft tissue profile of the patient.
• G – Sn – Pg’.
• 12+4
• A clockwise angle is positive (+) and a counterclockwise angle is negative (-).
35
• As the positive angle increases, the profile becomes more convex, suggesting a class II skeletal and dental relationship and vice-versa.
• However, the angle of facial convexity is not specific as to the location of the deformity.
36
• Maxillary and Mandibular Prognathism
• A line perpendicular to the horizontal plane (HP) is dropped from glabella and the relationship of the maxilla and the mandible are related to it.
• It helps to determine whether the problem is in maxilla or mandible.

.
7
37
• Maxillary Prognathism (G-Sn II HP)
• The distance from the line perpendicular to HP to Subnasale is measured.
• Describes the amount of maxillary excess or deficiency in the anteroposterior
dimension.
38
• A negative number suggestive of maxillary retrusion, whereas a large positive number connotes maxillary procumbency.
• Mean – 6+3mm.
39
• Mandibular Prognathism (G-Pg’ II HP)
• The position of pogonion is also measured parallel to HP from the perpendicular line dropped from glabella.
• This measurement gives an indication of mandibular prognathism or retrognathism.
• Mean – 0+4mm.
40
• Vertical Height Ratio
(G-Sn/Sn-Me I HP)
• In the vertical dimension, the anterior facial proportionality is assesed by taking the ratio of middle-third facial height to lower-third facial height measured perpendicular to HP.
• The ratio must be approximately 1:1
41
• A ratio of less than one would connote a disproportionately larger lower third of the face.
• A vertical maxillary excess, vertical macrogenia, or a combination of these deformities can be assesed.
42
• Lower Face-Throat Angle (Sn-Gn’-C)
• It is formed by the intersection of the lines Sn-Gn’ and Gn’-C.
• An application of this angle is critical in planning treatment to correct anteroposterior facial dysplasias.
• Mean- 100+7

.
8
43
• An obtuse angle should warn the clinician not to use those procedures which will reduce the chin prominence.
• Class III patients who have short, heavy throats and an obtuse lower face-throat angles should not have mandibular set backs.
44
• Alternatives such as maxillary advancement, a mandibular subapical surgery, mandibular setback with advancement genioplasty.
• Compromised tooth position can also be attempted.
45
• Lower Vertical Height-Depth Ratio
• Sn-Gn’/C-Gn’
• Is useful in determining the feasibility of reducing or increasing the prominence of chin.
• Mean-1:2
46
• The ratio of the distances subnasale to gnathion and cervical point to gnathion is normally a little larger than 1.
• In other words, if this ratio becomes much larger than 1, the patient has a relatively short neck, and the anterior projection of the chin should not be reduced.
47
Lip Position and Form
• Nasolabial Angle(Cm-Sn-Ls)
• Is an important measurement in assessing anteroposterior maxillary dysplasias.
• Although the angle takes into account the inclination of the nose, it is useful in evaluating the position of the upper lip.
48
• Mean- 102 ±8
• An acute nasolabial angle will often allow us to surgically retract the maxilla or retract the maxillary incisors, or both.
• An obtuse angle suggests a degree of maxillary hypoplasia and calls for a maxillary advancement or orthodontic proclination of maxillary incisors.

.
9
49
• Anteroposterior Lip Position
• Is evaluated by drawing a line from subnalsale to soft tissue pogonion.
• The amount of lip protrusion or retrusion is measured as a perpendicular linear distance from this line to the most prominent point of both lips.
50
• Upper Lip Protrusion {Ls to (Sn-Pg’)}
• Mean - 3+1mm
• Lower Lip Protrusion {Li to (Sn-Pg’)}
• Mean – 2+1mm
• Retracting or protracting the incisors surgically or orthodontically or advancing or reducing the prominence of chin, or both, can achieve concordant lip position.
51
• Mento-Labial Sulcus { Sl to (Li-pg’)}
• Measured from the depth of sulcus perpendicular to the Li-Pg’ line.
• A sulcus of 4mm is average in providing a pleasing lower lip to chin contour.
• Mean – 4+2mm
52
• Factors that can affect the lower lip inclination and deepen the mentolabial sulcus.
• Flared lower incisors.
• Extruded upper incisors.
• Flaccid lower lip tone.
• Abnormal morphology of the lip.
53
• To Reduce a deep Mentolabial Sulcus.
• Upright the lower incisors.
• Intrude the maxillary incisors.
• Cheiloplasty to retract the lower lip.
• Bony Chin. ( Can affect the depth of sulcus)
• Advancement Genioplasty will deepen and Reduction Genioplasty will aid in reducing excessive sulcular depth.
54
• Vertical Lip-Chin ratio.
• Sn-Stms/Stmi-Me’ (HP)
• The lower third of the face (Sn-Me’) can be divided into thirds; the length of the upper lip, or Sn-Stms should be approximately one third the total.
.
10
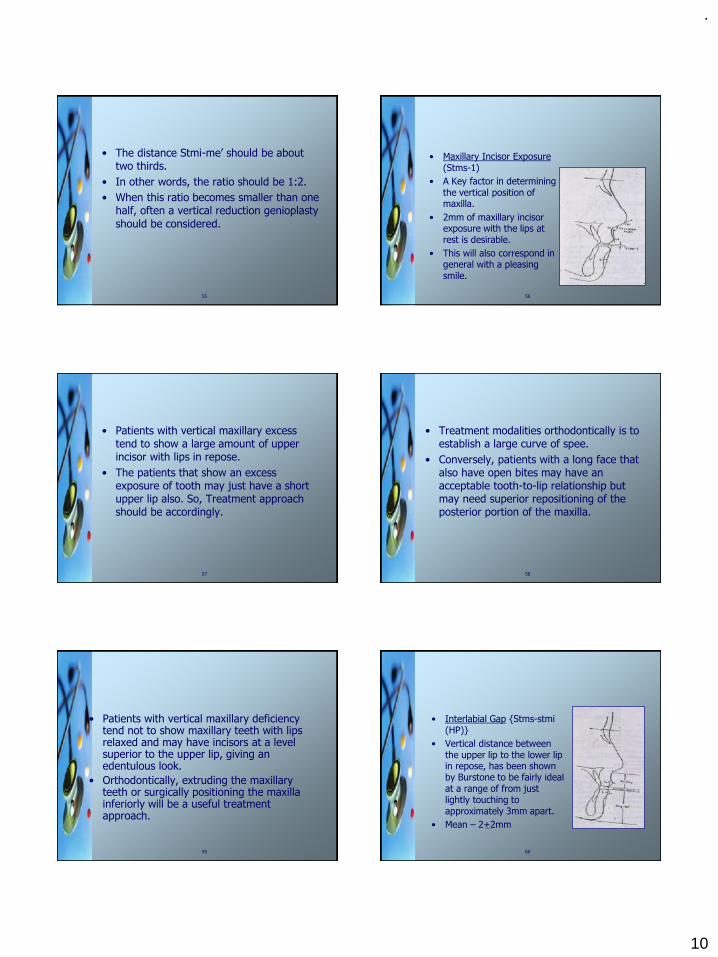
55
• The distance Stmi-me’ should be about two thirds.
• In other words, the ratio should be 1:2.
• When this ratio becomes smaller than one half, often a vertical reduction genioplasty
should be considered.
56
• Maxillary Incisor Exposure(Stms-1)
• A Key factor in determining the vertical position of maxilla.
• 2mm of maxillary incisor exposure with the lips at rest is desirable.
• This will also correspond in general with a pleasing smile.
57
• Patients with vertical maxillary excess tend to show a large amount of upper incisor with lips in repose.
• The patients that show an excess exposure of tooth may just have a short upper lip also. So, Treatment approach should be accordingly.
58
• Treatment modalities orthodontically is to establish a large curve of spee.
• Conversely, patients with a long face that also have open bites may have an acceptable tooth-to-lip relationship but may need superior repositioning of the posterior portion of the maxilla.
59
• Patients with vertical maxillary deficiency tend not to show maxillary teeth with lips relaxed and may have incisors at a level superior to the upper lip, giving an edentulous look.
• Orthodontically, extruding the maxillary teeth or surgically positioning the maxilla inferiorly will be a useful treatment approach.
60
• Interlabial Gap {Stms-stmi (HP)}
• Vertical distance between the upper lip to the lower lip in repose, has been shown by Burstone to be fairly ideal at a range of from just lightly touching to approximately 3mm apart.
• Mean – 2+2mm

.
11
61
biblography:
• Cephalometrics for orthognathic surgery.
– Charles J Burstone, DDS,MS; Randal B.
James, DDS; H Legan, DDS; G A Murphy,
DDS; Louis A. Norton DMD, Farmington, Conn.
– Journal of Oral Surgery, Vol 36, Aug 1978.
• Soft tissue cephalometric analysis for
orhtognathic surgery.
– Legan HL, Burstone CJ. J Oral Surg 1980: 38
: 81-87.
Thank you…

.
1
Good morning1
DEVELOPMENT OF
dentition and
OCCLUSION2
Presented by: Dr. Lavesh Pandey
CONTENTS
➢ Introduction
➢Prenatal Dental Development
➢The mouth of neonate – Pre-dentate period
➢Eruption of teeth
➢The Primary teeth and occlusion
▪ Development of teeth
▪ Development of occlusion
➢The mixed Dentition period
▪ First transitional period
▪ Inter-transitional period
▪ Second transitional period
➢Permanent teeth and occlusion
➢Assessment of dental age3
CONTENTS
➢Dentitional and occlusal development in Young Adult
➢Andrew’s six keys of occlusion
➢Occlusion and mandibular movements
➢Factors affecting occlusal development
➢Role of genetics in occlusal development
➢Clinical implications
▪ Normal versus ideal occlusion
▪ Occlusal adaptive mechanisms
➢Conclusion
➢References4
What is “occlusion” ?
Mosby’s dental dictionary (Zwemer;1998) defines occlusion as
”a static morphological tooth contact relationship”
Acc. to Ash and Ramfjord , occlusion may be defined as ”the
contact relationship of the teeth in function or para
function”.
Acc. to Angle, occlusion is “the normal relation of the
occlusal inclined planes of the teeth when the jaws are
closed”.
5
➢ The term occlusion , however, refers not only to contact
at an occlusal interface but also to “ all those factors
concerned with the development and stability of the
masticatory system and with the use of the teeth in oral motor behaviour ”
➢ In most instances , malocclusion and dentofacial
deformity are not caused by some pathological process ,
but by moderate distortions of normal development.
➢ Therefore , knowledge of the process of occlusal
development is necessary for the practice of
orthodontics.
6

.
2
DEVELOPMENT OF DENTITION
➢Humans are having two sets of teeth
Deciduous dentition Permanent dentition7
PRENATAL DENTAL
DEVELOPMENT
8
Prenatal Dental DevelopmentInitiation Of Odontogenesis
• First sign of tooth development - third embryonic week – thickening of epithelial lining
• At sixth week - Epithelial thickenings coalesce -dental lamina
Dental lamina9
Prenatal Dental DevelopmentInitiation Of Odontogenesis
Bud stage Cap stage Bell stage Advanced
bell stage
Initiation Proliferation Histo-differentiation Morpho-differentiation
10
Prenatal Dental Development
➢ Sequential pattern▪ CI-LI-C-M1-M2
▪ Postnatal variations – 25 %
➢Spatial pattern▪ The prenatal dental arch progressively changes shape
▪ 6-8 week- Flat antero-posteriorly
▪ 4th month - Elongation of Ant. Segment - Catenary curve
➢Spacing ▪ Inter-dental spacing is relatively constant during this period.
11
Prenatal Dental Development➢Tooth Fields
▪ Interdental spaces are shared by
neighbouring tooth fields.
▪ Tooth germ together with the space
mesial and distal to it within the dental
arch is called tooth field
▪ Greatest level of occupancy of a tooth
field by a tooth germ is about 80 % for
the first deciduous molar and lateral
incisor.
▪ More occupancy of the field by the
lateral incisor leads to its concomitant
rotation and displacement.
#Van der linden FPGM et al .Tooth size and position before birth . J Dent
Res 1972;51:71-74 12

.
3
Mouth of the neonate
Predentate period
13
Predentate Period
Gum pads➢Cover the alveolar process at birth
➢Pink, firm, covered by dense fibrous periosteum
➢Segmented to indicate sites of developing teeth
➢Transverse groove divides into ten parts
➢Dental groove demarcates the labio-buccal and the lingual portions
➢Lateral sulcus between the canine and the first molar is used to estimate the inter-arch width
14
Predentate Period
➢Size of the gum pads at birth may be determined by (Leighton) :
▪ State of maturity of infant at birth
▪ Size at birth as expressed by birth weight
▪ Size of developing primary teeth
▪ Purely genetic factors
➢ Maxillary arch▪ Horse shoe shaped
▪ Complete overjet labially and bucally
➢ Mandibular arch ▪ Lies posterior to the maxillary arch when the gum pads
contact
15
Predentate Period
➢Neonatal jaw relations
▪ No precise ‘Bite’ or jaw relation
▪ Ant. open bite incidence
➢Dental Arch Width
▪ pre-eruptive:
• significant increase between
6 weeks and 1 year
16
Predentate Period Precociously erupted primary teeth
➢Natal teeth
➢Neonatal teeth
➢ Pre-erupted teeth
➢ Etiology
▪ Superficial position of tooth germ
▪ Febrile incidents, hormonal stimulation, heredity
• Increased rate of eruption
▪Osteoclastic activity
➢ Associated with syndromes
• Chondro-ectodermal dysplasia
17
Predentate Period Self correcting anomalies
➢Retrognathic mandible
▪ Differential and forward growth
➢ Anterior open bite
▪ Eruption of primary incisors
➢ Infantile swallowing pattern
▪ Introduction of solid food in diet
18

.
4
CALCIFICATION
▪ Stages of tooth development given by Nolla
▪ He arbitrarily divided the tooth development in 10 stages
▪ Development of a tooth is compared with drawings
▪ Stage 2 – initial calcification
▪ Stage 6 – beginning of eruptive movements
▪ Girls are more advanced in
calcification of permanent teeth than
boys
# Nolla CM.The development of the permanent teeth. J Dent Child 1960; 27 :254-26619
ERUPTION OF TEETH
20
ERUPTION OF TEETH
➢ It is a developmental process that moves a tooth from it’s crypt position
through the alveolar process into the oral cavity and to occlusion with it’s
antagonist
➢ Physiologic tooth movements leading to tooth eruption can be divided into 3
phases
1. Pre - eruptive phase
2. Eruptive phase
3. Post - eruptive phase 21
➢ERUPTIVE PHASE
Begins with the root formation and the tooth moves from its position
within the jaw bones to its functional position in occlusion. The principal
direction of movement is occlusal.
➢PRE - ERUPTIVE PHASE
Consists of the movements of the developing tooth germs within the
alveolar process before root formation. During this phase, the growing teeth
move in various directions to maintain their position in the expanding jaws.
➢POST - ERUPTIVE PHASE
Consists of tooth movements which
▪Maintain the position of the erupted teeth while the jaws continue to
grow
▪Compensate for occlusal and proximal wear22
Theories of tooth eruption
➢Root elongation theory
▪ Suggests that proliferating root impinges on a fixed base, the
cushion-hammock ligament, thus converting an apically
directed force into occlusal movement.
▪ Evidence against - A series of experiments where rootless
teeth have erupted into functional occlusion.
➢Pulp constriction theory
▪ Suggests that a propulsive force is generated by extrusion of
pulp through three mechanisms : firstly growth of dentin,
secondly interstitial pulp growth and thirdly, hydraulic effects
within the vasculature
▪ Evidence against - The work of Merzberg and Schour, who
removed the pulp of rodent incisors and found that the
eruption rates were unaffected. 23
Theories of tooth eruption➢Hydrostatic pressure theory
▪ Teeth move in their sockets in synchrony with arterial
pulse, thus local volume changes may produce limited
tooth movement.
▪ Evidence against - Surgical excision of a growing root
and associated tissue eliminates the periapical
vasculature without stopping eruption.
➢ Bone remodeling theory
▪ Suggests that selective deposition and resorption of bone
brings about eruption of tooth.
• Evidence supporting - In experiments where tooth germ is
removed but the follicle is left in position, the eruptive
pathway still forms in bone thus proving the dental follicle
and not bone as the major determinant in tooth eruption.
24
.
5
Theories of tooth eruption
➢Periodontal ligament traction theory▪ The periodontal membrane plays an important role in the
tooth eruption. Two causative agents with in the
periodontal ligament which can generate eruptive force.
• Collagen contraction
• Fibroblast traction
▪ Evidence supporting – Changes are induced in the
shape and orientation of PDL fibroblasts by a transition
from impeded to unimpeded eruption.
25
FACTORS AFFECTING
ERUPTION
➢Factors regulating and affecting eruption
▪ Heredity
▪ Socioeconomic status
▪ Racial differences
▪ Nutritional influence
▪ Mechanical disturbance
▪ Localised pathosis
26
Deciduous dentition
27
Deciduous dentition
➢Begins at around 6 months of age with the
eruption of lower central incisors.
➢Completed after all the 2nd molars have attained
occlusion i.e. usually around 2.5 years of age.
➢ Little changes take place in the deciduous
dentition between 2.5 to 5 years of age.
28
Deciduous dentitionDevelopment Of Primary teeth
➢Calcification▪ Central incisor- 14 week
▪ 1st molar- 15 1/2 weeks
▪ Lateral incisor- 16 week
▪ Canine- 17 week
▪ 2nd molar- 18 week
➢Genetic control ▪ Morphology, rate and sequence of growth, pattern
of calcification, mineral content of teeth
29
Deciduous dentition:Development of Primary teeth
➢ Eruption
➢Sexual differences▪ Males - early eruption till 15 month
▪ Females - surpass after 15 months
30

.
6
Deciduous dentitionDevelopment of Primary teeth
➢Developmental anomalies▪ less frequent
▪ fewer than 1% incidence of congenitally missing teeth.
➢Primary tooth resorption▪ Important contribution to permanent tooth eruption
▪ Due to pressure from the erupting permanent successor
though it may occur even its absence
▪ Hastened by inflammation and occlusal trauma
▪ Delayed by splinting and absence of permanent successor
31
➢Ankylosis▪ Primary teeth more likely to be involved as compared to permanent
▪ Teeth fused to alveolar bone and their eruption prevented
▪ Particularly molars
▪ Lower teeth twice as upper
▪ Often bilaterally
▪ Trauma or excessive pressure said to be the cause
▪ Osseous bridging and fusion of bone occuring during rest periods of resorption of dentin
▪ Posterior open bite due to involved tooth being “submerged ”.
32
Deciduous dentition: Development of occlusion
➢Neuromuscular considerations
▪ Sequential inter-dentation begins in the front as the
incisors erupt
▪ Teeth guided into occlusal position by muscular
functional matrix during very active growth of the facial
skeleton.
▪ Low cusp ht. and ease of wear of occlusal surfaces
also contribute to this adaptability
▪ Muscle behaviour is adaptive to skeletal morphology
▪ Acc . to a study by Leighton ,abnormal sucking habits
either largely cause the skeletal differences or
contribute to them.33
Deciduous dentition: Development of occlusion
➢Arch form▪ In maxilla
• Ovoid in shape
• Role of tongue
• Increased intercanine width by 6 mm between 3-13 yrs
• Increased Intermolar width of 2 mm between 3-5 yr34
Deciduous dentition: Development of occlusion
➢Arch form▪ In mandible
▪Ovoid shape
▪ Increased intercaninewidth by 3.7 mm between3-13 yrs
▪ Increased Intermolarwidth of 1.5 mm between3-5 yr
35
Deciduous dentition: Development of occlusion
➢Arch length and
circumference
▪ Small amount of decrease
• mesial migration of second
primary molars during eruption
• proximal caries
36
.
7
Deciduous dentition: Development of occlusion
Spacing➢Usually generalised inter-dental spacing
➢According to Baume▪ Closed dentition
▪ Spaced dentition
• Generalized- Physiologic Pressure from the
tongue (Barber)
• Localized – Primate spaces (anthropoid/
simian spaces)
• Primate spaces• 87% of maxillary arches between lateral incisor
and canine
• 78% of mandibular arches between canines
and first primary molars37
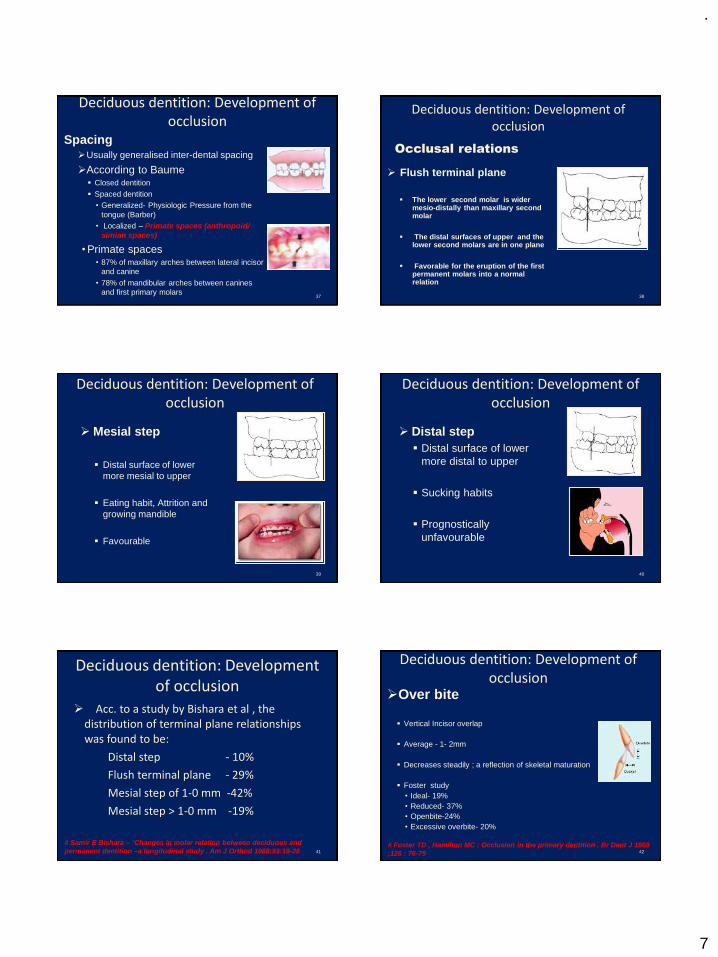
Deciduous dentition: Development of occlusion
➢ Flush terminal plane
▪ The lower second molar is wider mesio-distally than maxillary second molar
▪ The distal surfaces of upper and the lower second molars are in one plane
▪ Favorable for the eruption of the first permanent molars into a normal relation
Occlusal relations
38
Deciduous dentition: Development of occlusion
➢ Mesial step
▪ Distal surface of lower
more mesial to upper
▪ Eating habit, Attrition and
growing mandible
▪ Favourable
39
Deciduous dentition: Development of occlusion
➢ Distal step
▪ Distal surface of lower
more distal to upper
▪ Sucking habits
▪ Prognostically
unfavourable
40
Deciduous dentition: Development of occlusion
➢ Acc. to a study by Bishara et al , the distribution of terminal plane relationships was found to be:
Distal step - 10%
Flush terminal plane - 29%
Mesial step of 1-0 mm -42%
Mesial step > 1-0 mm -19%
# Samir E Bishara – ‘Changes in molar relation between deciduous and
permanent dentition –a longitudinal study . Am J Orthod 1988;93:19-28 41
Deciduous dentition: Development of occlusion
➢Over bite
▪ Vertical Incisor overlap
▪ Average - 1- 2mm
▪ Decreases steadily ; a reflection of skeletal maturation
▪ Foster study
• Ideal- 19%
• Reduced- 37%
• Openbite-24%
• Excessive overbite- 20%
# Foster TD , Hamilton MC : Occlusion in the primary dentition . Br Dent J 1969
;126 : 76-79 42

.
8
Deciduous dentition: Development of occlusion
➢ Overjet▪ Horizontal overlap
▪ Normal :- 0-4 mm in primary dentition
▪ Decreases steadily
▪ Foster study
• ideal – 28%
• excessive – 72%
# Foster TD , Hamilton MC : Occlusion in the primary dentition . Br Dent J
1969 ;126 : 76-79 43
Normal signs of Deciduous
dentition
➢ Spaced anteriors
➢ Primate spaces
➢ Shallow overbite and overjet
➢ Straight terminal plane
➢ Class - I molar and cuspid relationship
➢ Almost vertical inclination of anterior teeth
➢ Ovoid arch form
44
Self correcting anomalies of Deciduous
dentition
➢ Anterior deep bite
▪ Cause - Incisors more upright
▪ Correction
• Forward and downward growth of mandible
• Attrition of incisal edges
• Eruption of permanent molars
45
Self correcting anomalies of Deciduous
dentition
➢ Primate spaces
▪ Early mesial shift
➢ Flush terminal plane
▪ Early mesial shift
▪ Late mesial shift
➢Physiologic spaces
▪ Permanent incisor accommodation
46
MIXED DENTITION PERIOD
47
Mixed dentition
➢Period of both primary and permanent
dentition
➢Those permanent teeth that follow into
place in the arch once held by a primary
teeth are called SUCCESSIONAL TEETH
- Incisors, cuspids and bicuspids)
➢Those teeth that erupt posteriorly to the
primary teeth are termed as
ACCESSIONAL TEETH48

.
9
Mixed dentition
➢Clinical importance
▪ Utilization of arch perimeter
▪ Alignment of permanent incisors.
▪ Space for cuspids and premolars.
▪ Adjustment of the molar occlusion.
▪ Adaptive changes occur in occlusion during the
transition from deciduous dentition to permanent
▪ Orthodontic intervention
49
Eruption of permanent teeth
➢Sequence
➢Maxillary
6-1-2-4-3-5-7 or 6-1-2-4-5-3-7
➢Mandibular
6-1-2-4-3-5-7 or 6-1-2-3-4-5-7
➢This includes 40-50 % of all children
# Lo RT , Moyers Re . Studies in the etiology and prevention of Malocclusion .I .
The sequence of eruption of permanent teeth. Am J Orthod 1953;39:460-750
Mixed dentition
➢ First transitional
period :-
▪ Emergence of first
permanent molars.
▪ Exchange of
deciduous incisors
with permanent
incisors.
▪ Establishment of
occlusion51
Mixed dentition First transitional period
➢1st molar eruption▪ Mandible
• Guided into its occlusal position by distal surface of 2nd primary molar
• Mesial and lingual path of eruption
▪ Maxilla• Forward direction of maxillary growth
• Space created posteriorly
• Distal and buccal path of eruption
52
Mixed dentition First transitional period
➢Factors affecting first molar
eruption
• Congenital absence of tooth itself
• Congenital absence of premolars
• Distal caries of deciduous 2nd molar
• Early loss of deciduous 2nd molar
• Developmental disturbances
53
Mixed dentition First transitional period
➢Molar adjustment
▪ Early mesial shift• Closure of primate spaces and other
inter-dental spaces from the rear
• Controversy - alternative theory
• primate spaces closed by eruption of
incisors without loss of perimeter
▪ Late mesial shift-• Mesial migration of first permanent molar
after loss of second deciduous molar
using leeway space.
5 Yr
7 YrJ Dent Res 1950; 29:331-7
54
.
10
Mixed dentition First transitional period
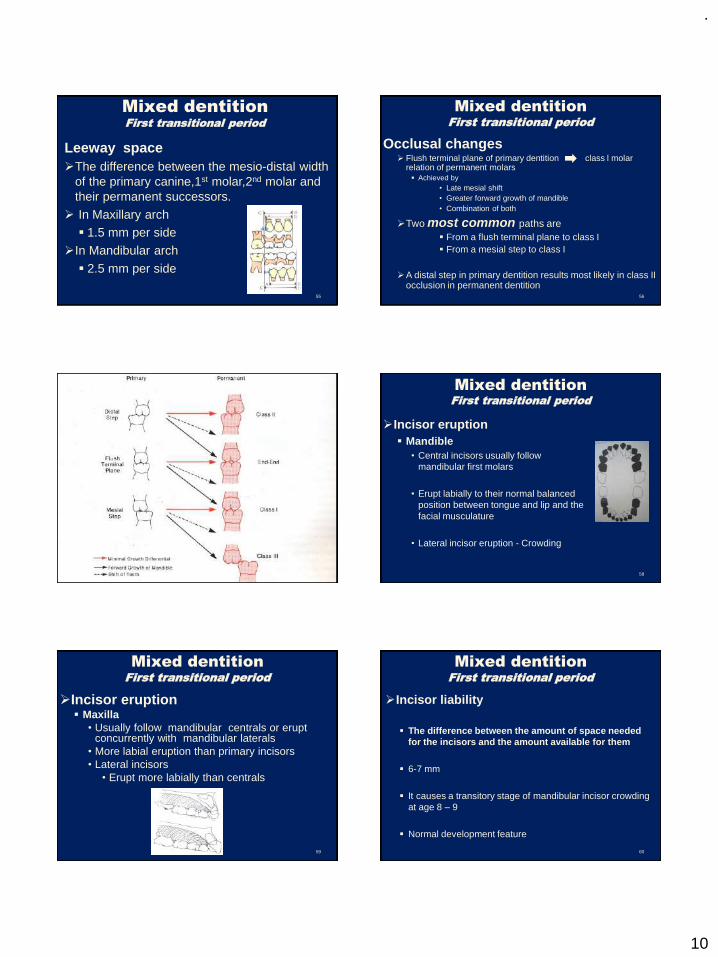
Leeway space
➢The difference between the mesio-distal width
of the primary canine,1st molar,2nd molar and
their permanent successors.
➢ In Maxillary arch
▪ 1.5 mm per side
➢In Mandibular arch
▪ 2.5 mm per side
55
Mixed dentition First transitional period
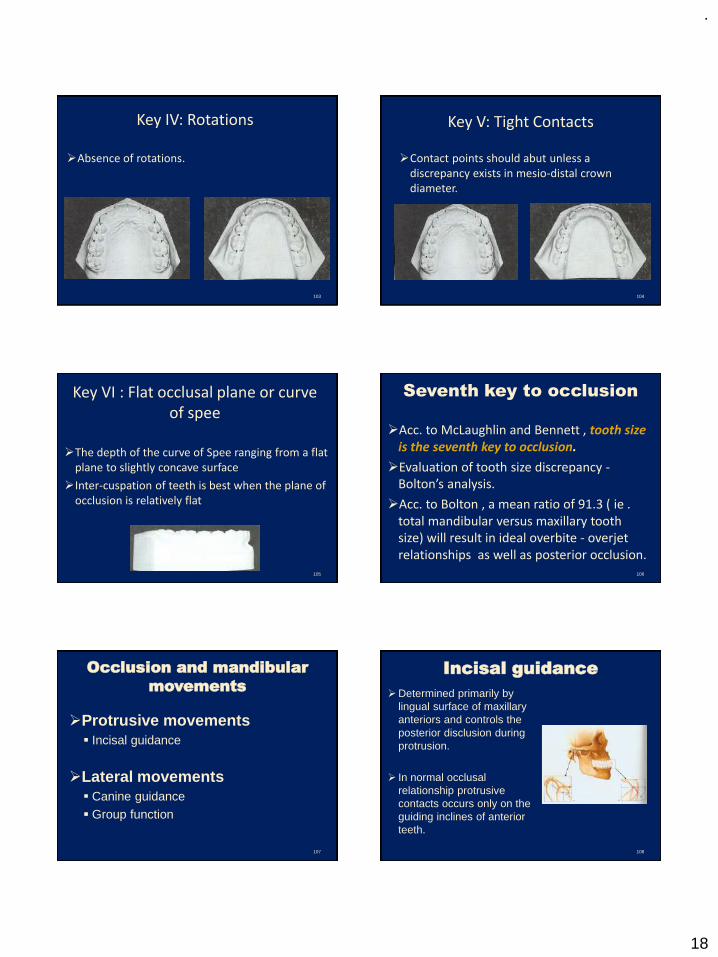
Occlusal changes➢ Flush terminal plane of primary dentition class l molar
relation of permanent molars ▪ Achieved by
• Late mesial shift
• Greater forward growth of mandible
• Combination of both
➢Two most common paths are
▪ From a flush terminal plane to class I
▪ From a mesial step to class I
➢A distal step in primary dentition results most likely in class II occlusion in permanent dentition
56
s
57
Mixed dentition First transitional period
➢Incisor eruption
▪ Mandible
• Central incisors usually follow
mandibular first molars
• Erupt labially to their normal balanced
position between tongue and lip and the
facial musculature
• Lateral incisor eruption - Crowding
58
Mixed dentition First transitional period
➢Incisor eruption▪ Maxilla
• Usually follow mandibular centrals or erupt concurrently with mandibular laterals
• More labial eruption than primary incisors
• Lateral incisors
• Erupt more labially than centrals
59
Mixed dentition First transitional period
➢Incisor liability
▪ The difference between the amount of space needed
for the incisors and the amount available for them
▪ 6-7 mm
▪ It causes a transitory stage of mandibular incisor crowding
at age 8 – 9
▪ Normal development feature
60

.
11
Mixed dentition First transitional period
➢Incisor liability adjustment
▪ Inter-canine arch growth - 3 to 4 mm
( 2 mm average )
▪ Inter-dental (Developmental) spacing -
2 to 3 mm
▪ More anterior position of permanent
incisors as they erupt - 1 to 2 mm
61
Mixed dentition Inter-transitional period
➢Between the 1st and 2nd transitional
period.
➢Stable phase
➢Contains both sets of dentition.
▪ Permanent 1st molars and incisors.
▪ Deciduous canines and deciduous 1st and
2nd molars.
62
Mixed dentition
➢ Second
transitional period
▪ Emergence of
Bicuspids, cuspids,
2nd molars
▪ Establishment of
occlusion
63
Mixed dentition Second transitional period
Mandible➢Most favorable and the most common
eruption sequence
▪ 6-1-2-3-4-5-7
➢ Eruption of cuspids first
▪ Maintenance of arch perimeter
▪ Prevention of lingual tipping of
incisors
64
Mixed dentition Second transitional period
➢ If tooth size-space available ratio is
poor , the cuspid may be stopped in its
eruption by the first molar or the
primary molar may be hastened in its
exfoliation
➢1st Bicuspids▪ Rarely any difficulty
▪ Sometimes show rotation due to
uneven resorption of primary molar
roots
65
Mixed dentition Second transitional period
➢2nd bicuspids▪ Last lower succedaneous teeth to erupt
▪ Extreme variation in calcification and development schedule
▪ Often congenitally missing
▪ Eruption complication
• Mesial migration of 1st molar
• Poor tooth size - space available ratio
• Premature exfoliation of 2nd primary molar
▪ First molar must not be allowed to move mesially untill the second bicuspid has attained its proper position in the arch
66

.
12
Mixed dentition Second transitional period
Maxilla
➢Sequence of eruption
▪ 6-1-2-4-5-3-7 or 6-1-2-4-3-5-7
➢1st bicuspid▪ Minimal difficulty in eruption
▪ Nearly the same size as its predecessor
67
Mixed dentition Second transitional period
Maxilla
➢2nd bicuspid▪ Easy eruption
▪ Larger mesio-distal width
of primary predecessor
permits easy eruption in
its place in the arch
68
Mixed dentition Second transitional period
➢Cuspid
▪ More difficult and tortuous path of eruption than any other tooth
▪ Uses leeway space for acomodation
▪ Favourable sequence
• Cuspid before 2nd molar
▪ In case of short arch length
• labioversion with a decided mesial inclination
69 70
Impacted maxillary cuspids
➢Frequently impacted
➢Females more than males.
➢Reasons :-
▪ High initial position in the crypt
▪ Deviated path of eruption
▪ Lack of guidance from maxillary lateral incisor
▪ Lack of space
▪ Congenital absence of lateral incisor
▪ Presence of supernumerary teeth
Mixed dentition Second transitional period
2nd molars➢Last teeth to erupt before 3rd molar
➢Mandible
▪ If precede 2nd bicuspid, the 1st molar may tip mesially
▪ Erupts typically before maxillary second molar
➢Maxilla
▪ Eruption of maxillary second molar ahead of the mandibular second molar is said to be symtomatic of a developing class ll malocclusion
# Lo RT , Moyers Re : Studies in the etiology and prevention of malocclusion.I.
The sequence of eruption of the permanent dentition . Am J Orthod 1953 39 :
460-467 71
Mixed dentition Self correcting anomalies
➢Ugly Duckling Midline diastema
(Broadbent phenomena)
72

.
13
Mixed dentition
Self correcting anomalies
➢Mandibular anterior crowding
▪ Increased inter-canine width
▪ Tongue pressure
• Labial movement and change in inclination of
incisors
73
Mixed dentition
Self correcting anomalies
➢End on molar relation▪ Late mesial shift
• Leeway space
74
PERMANENT
DENTITION
75
PERMNENT DENTITION
Factors determining the tooth’s position
➢Mesial drift▪ strong inherent tendency of the teeth to
move mesially even before they appear in the oral cavity
➢Anterior component of force ▪ Axial inclination of permanent teeth are
such that some of the forces of chewing produce a mesial resultant through the contact points of the teeth
▪ Result of muscle forces acting through the inter-cuspation of the occlusal surface.
▪ Counteracted by proximal contacts of the
teeth and by the musculature of the lips
and cheeks.76
Permanent dentition
Arch Width➢ Width increase involves alveolar process growth
➢ Maxillary alveolar processes diverge while the
mandibular processes are more parallel
Maxilla➢ Maxillary width increases are much greater and
they can be more easily altered in treatment
➢ Mid-palatal suture can be reopened with RME –
large amount of actual widening
Mandible➢ Widening the basal bony width – deposition on
lateral borders of corpus mandibularis
➢ Little help to clinician to widen the arch
77
Permanent dentitionSafety valve mechanism
➢Mandibular inter-canine arch width completed
▪ Girls – 9 years
▪ Boys – 10 years
➢Maxillary inter-canine arch width completed
▪ Girls – 12 years
▪ Boys – upto 18 years
➢Differences in increase in maxillary dimensions – pubertal growth spurts - in girls form 10 ½ - 12 years and from 12-18 years in boys
➢Maxillary inter-canine arch width increase serves as a
‘safety valve’ for the dominant horizontal basal mandibular growth during growth spurts. 78

.
14
Permanent dentition
Arch Circumference or perimeter➢Maxilla
▪ Typically increases slightly
▪ Angulation of incisors and greater increase in width - Preservation of circumference
➢Mandible▪ Reduction
• Late mesial shift
• Mesial drifting tendency
• Lingual positioning of incisors due to differential mandibulo-maxillary growth
• Original tipped position of incisors and molars
79
Permanent dentition
Overjet and overbite
➢Mixed to permanent dentition
▪ Overbite
• Increases followed by decrease
• Great variability
• Correlated with a number of facial dimensions ( eg . Ramus height )
▪ Overjet
• Reflection of antero-posterior skeletal relationship
• Sensitive to abnormal lip and tongue function
# Fleming HB .An investigation of the vertical overbite during the eruption of the
permanent dentition . Angle Orthod 1961;31:53-62 80
Assessment of dental age
➢Which teeth have erupted ?
➢The amount of resorption of the primary
teeth
➢The amount of development of the
permanent teeth.
81 82
DENTAL AGE - 6
➢Near simultaneous eruption
of permanent mandibular
central incisors, maxillary 1st
molars and mandibular 1st
molars.
83
DENTAL AGE - 7
➢Eruption of maxillary central incisors
followed by mandibular lateral incisors.
➢Root formation of maxillary lateral incisor
advanced.
➢Premolars and canines in stage of crown
completion.
84
DENTAL AGE - 8
➢Eruption of maxillary
lateral incisors
➢Delay of 2-3 years
before any more
permanent teeth erupt.

.
15
85
DENTAL AGE - 9
➢Primary canines,1st and 2nd
deciduous molars present
➢Root development of maxillary canines and all second premolars is just beginning
➢One third of the root of the mandibular canines and all of the first premolars have been completed.
86
DENTAL AGE - 10
➢Completion of one half of the root development
of mandibular canine, mandibular 1st premolar
and maxillary 1st premolar
➢Completion of roots of mandibular incisor teeth
➢Near completion of roots of maxillary laterals.
87
DENTAL AGE - 11
➢Near simultaneous
eruption of mandibular
canine , mandibular 1st
premolar and maxillary 1st
premolar.
Dental age – 12
88
➢Eruption of maxillary
canine, maxillary and
mandibular 2nd premolar.
➢Second permanent molars
in both the arches are
nearing eruption.
89
DENTAL AGE – 13 , 14 , 15
➢Progressive completion of
roots of permanent teeth.
➢ If 3rd molar is present
crown formation is
complete.
Dentitional and occlusal changes in young
adults
➢3rd molar development
▪ Most variable in calcification and eruption
▪ Role of 3rd molar in crowding
▪ Impacted mandibular third molars
• seen more frequently with skeletal class II particularly when mandible is short and acutely angled
90

.
16
Dentitional and occlusal changes in young
adults
➢Dimensional changes
▪ Decrease in arch perimeter during the late adolescent and
young adult period
➢Occlusal changes▪ Decrease in overjet and overbite in 2nd decade
• Forward growth of mandible
▪ Changes in Sagittal relationships
• Mesial drifting tendency
• Inter-proximal wear
• Continuing growth of mandible
▪ 3rd molar eruption
91
Dentitional and occlusal changes in
young adults
➢Resorption of permanent teeth
▪ Idiopathic resorption of one or more teeth – by the
end of the second decade
▪ Frequency increasing with age
▪ Orthodontic treatment - increased severity and
number of resorbed teeth
92
Dentitional and occlusal changes in
young adults
➢Arrangement of teeth in the jaws
▪ Intra arch tooth alignment
• Relationship of teeth with in the dental arch
• Teeth seen in varying degree of inclination
• Lateral view – curve of spee
• Frontal view - curve of wilson
• Proximal view
93
Dentitional and occlusal changes in
young adults▪ Curve of spee
• First described by Von Spee in
1928
• Inclination of teeth in lateral view
• Antero-posterior curvature of the
occlusal plane
• The average value 2.5 – 3 mm
94
Dentitional and occlusal changes in
young adults
▪ Curve of Wilson
• In frontal view • Posterior teeth
• Maxillary arch - Slight buccal inclination
• Mandibular arch - Lingual inclination
• Medio-lateral or transverse curvature of the
occlusal plane
95
Dentitional and occlusal changes in
young adults
▪ In the proximal view
• Maxillary arch
• Anterior teeth - mesially inclined
• Posterior teeth - Distally inclined
• Mandible – oblique backwards
96

.
17
Dentitional and occlusal changes in young
adults
➢Inter arch tooth alignment
• Relationship of teeth in one arch to those in other arch.
• Every tooth occludes with two opposing teeth except mandibularcentral incisors and maxillary third molars ; this one to two relationship leads to distribution of masticatoryload over the entire arch.
• Occlusal contacts occur mainly through two types
• Cusp to fossae relationship
• Cusp to embrasure relationship 97
Andrews six keys to normal occlusion
➢These are a set of six characteristics that
were consistently present in collection of
120 casts of naturally optimal occlusion ,
identified by Dr. Lawrence F Andrews
#Andrew L.F. The six keys to normal occlusion . Am J Orthod.1972 ; 62 : 296-302. 98
Key I : Interarch Relationships
➢ The mesio-buccal cusp of the
permanent maxillary first molar
occludes in the groove between the
mesial and middle buccal cusps of the
permanent mandibular first molar –
originally given by Angle
➢ The distal surface of the disto-buccal
cusp of the upper first permanent first
molar occludes with the mesial surface
of the mesio-buccal cusp of the lower
second molar
99
Key II : Crown Angulation
➢The mesio-distal tip of the
long axis of the crown
➢Measured as the angle
formed between the long
axis of the crown and a line
bearing 90 degrees from the
occlusal plane.
➢The gingival portion of the
long axis of crown is more
distal than the incisal portion
100
Key III : Crown inclination
➢ Labio-lingual or bucco-lingual
inclination
➢ Measured as the angle formed
by a line which bears 90 degrees
to the occlusal plane and a line
that is tangent to the bracket
side
101
Key III : Crown inclination
➢ Most maxillary incisors have a
positive inclination; mandibular
incisors have a slightly
negative inclination
➢ For posterior teeth a
progressively minus inclination
is seen from canine through
the second molars
102
.
18
Key IV: Rotations
➢Absence of rotations.
103
Key V: Tight Contacts
➢Contact points should abut unless a discrepancy exists in mesio-distal crown diameter.
104
Key VI : Flat occlusal plane or curve of spee
➢The depth of the curve of Spee ranging from a flat plane to slightly concave surface
➢Inter-cuspation of teeth is best when the plane of occlusion is relatively flat
105
Seventh key to occlusion
➢Acc. to McLaughlin and Bennett , tooth size is the seventh key to occlusion.
➢Evaluation of tooth size discrepancy -Bolton’s analysis.
➢Acc. to Bolton , a mean ratio of 91.3 ( ie . total mandibular versus maxillary tooth size) will result in ideal overbite - overjetrelationships as well as posterior occlusion.
106
Occlusion and mandibular
movements
➢Protrusive movements
▪ Incisal guidance
➢Lateral movements
▪ Canine guidance
▪ Group function
107
Incisal guidance
➢Determined primarily by
lingual surface of maxillary
anteriors and controls the
posterior disclusion during
protrusion.
➢ In normal occlusal
relationship protrusive
contacts occurs only on the
guiding inclines of anterior
teeth.
108

.
19
Incisal guidance
➢Reasons
▪ Incisors are located far away from TMJ
thus, creating less amount of stresses
on them.
▪ Gliding type of movement is more
adaptive to the incisors due to their
favorable anatomy.
109
Canine guidance
➢When mandible moves laterally contact
occurs only between the canines thus ,
discluding posteriors and incisors.
110
Canine guidance
➢Reasons▪Good crown to root ratio of canines.
▪Hard compact bone surrounding the tooth.
▪Location far away from TMJ receiving less amount of
stresses.
▪Many receptors in PDL of canines.
➢Prevents the breakdown of periodontal fibers of
posteriors and incisors.
➢Cannot be possible in periodontally
compromised canines or missing canines
111
Group function
➢Working side contacts extend posteriorly involving
premolars and mesiobuccal cusp of first molar.
➢Can be achieved when canine guidance is not
possible.
112
Mutually protected occlusion
➢Anterior and posterior teeth function differently
➢The posterior teeth function more effectively in stopping the mandible during closure, whereas anterior teeth function most effectively in guiding the mandible during eccentric movement.
➢Posterior teeth should thus contact slightly more heavily than anterior teeth in centric relation.
➢ This condition is described as mutually protected occlusion.
113
FACTORS AFFECTING OCCLUSAL DEVELOPMENT
➢General factors▪ Heredity
▪ Skeletal factors
▪ Muscle factor
➢Local factors▪ Aberrant
developmental
position of teeth
▪ Supernumerary
teeth
▪ Hypodontia
▪ Oral habits
▪ Localized soft
tissue anomalies114

.
20
Role of genetics in occlusal
development
➢Occlusal characteristics could be inherited in two
major ways
▪ An inherited disproportion between the size of
the teeth and the size of the jaws, which
would produce crowding or spacing
▪ An inherited disproportion between size or
shape of the upper and lower jaws, which
would cause improper occlusal relationships.
➢The more independently these characteristics
are determined, the more likely that disproportions could be inherited.
115
Role of genetics in occlusal
development
➢There is dental anthropological evidence that
population groups that are genetically
homogeneous tend to have normal occlusion.
However, in heterogeneous populations the
incidence of jaw discrepancies and occlusal
disharmonies is significantly greater.
➢The influence of inherited tendencies is
particularly strong for mandibular prognathism.
116
Clinical implications
➢Normal versus ideal occlusion
▪Normal occlusion implies more than a
range of anatomically acceptable values.
▪ It also indicates physiological adaptability
and the absence of recognizable
pathological manifestations.
117
Clinical implications
➢Ideal occlusion is a state in which no
neuromuscular adaptation is needed because no
occlusal interferences are present
• The concept of an ideal occlusion refers both to an
esthetic and physiological ideal
• It is a hypothetical formula which does not and
cannot exist in man
118
Clinical implications
➢Occlusal adaptive mechanisms
119
Conclusion
➢Occlusion , good or bad, is the result of an
intricate and complicated synthesis of
genetic and environmental relationships at
work throughout the early developmental
stages of childhood and young adulthood.
➢Understanding the concepts has thus got
far reaching implications in diagnosis,
treatment planning and prognosis of
malocclusion.120

.
21
References➢ Robert Meyers. Handbook of orthodontics
➢ Samir E. Bishara . Textbook of Orthodontics
➢ William R. Profitt .Contemporary orthodontics: fourth
edition
➢ Wheelers dental anatomy
➢ Woelfel , Scheid .Dental anatomy
➢ A.R. Ten Cate . Oral histology – development, structure
and function
➢ Berkovitz ,Holland and Moxham .Oral anatomy,histology,
embryology
➢ Ramfjord SP. Occlusion
➢ McLaughlin , Bennett and Trevisi – Systemized
orthodontic treatment mechanics
121
References
➢ Andrew L.F. The six keys to normal occlusion . Am J
Orthod. Vol. 62; 1972: 296-302.
➢ Samir E. Bishara .Changes in molar relationship
between deciduous and permanent dentition – a
longitudinal study. Am J Orthod. 1988; 93:19-28.
➢ Lo RT , Moyers Re : Studies in the etiology and
prevention of malocclusion . I. The sequence of eruption
of the permanent dentition . Am J Orthod 1953 39 : 460-
467
➢ Fleming HB .An investigation of the vertical overbite
during the eruption of the permanent dentition . Angle
Orthod 1961;31:53-62
➢ Functional occlusion for orthodontist . JCO 1981;jan 32-
51122
References
➢ Foster TD , Hamilton MC : Occlusion in the primary
dentition . Br Dent J 1969 ;126 : 76-79
➢ Nolla CM.The development of the permanent teeth. J
Dent Child 1960; 27 :254-266
➢ Van der linden FPGM et al .Tooth size and position before
birth . J Dent Res 1972;51:71-74
123
Thank you124

.
1
Hard tissue Analysis
Presented by: Dr. Lavesh Pandey
Contents
Mc Namara Analysis
Quadrilateral Analysis
Bjork Analysis
Jaraback Analysis
PA Ceph Analysis
Mc’Namara’s Analysis
1984, American journal of Orthodontics.
This analysis is derived in parts from the
principles of the cephalometric analysis of
Ricketts (1960; 1972;1981)
Harvold ( 1974)
Woodside (1975)
The construction of Nasion perpendicular & pt. A are
presumed to be original.
Composite normative standards based on 3
cepholometrics sample are provided
1.Lat ceph of the children comprising the
Bolton Standards-
-longitudnally followed up from 6-18yrs
-retraced and digitized by Behrents &
Mcnamara
2. Group of untreated children from Burlington
orthodontic centre
- longitudinally followed up from 6-20 yrs.
3. Ann Arbor sample of 111 young adults
- Good to excellent profile
- Class I occlusion
- Good skeletal balance
average age of females-26yrs 8 mths
average age of males - 30 yrs 9 mths
In an effort to create a clinically useful analysis
the craniofacial skeletal complex is divided
into-
Maxilla to cranial base
Maxilla to mandible
Mandible to cranial base
Dentition
Airway
.
2
Maxilla to cranial base
The position of maxilla relative to cranial base
is evaluated in two ways;
Soft tissue profile
Skeletal relationship of Point A to the N
perpendicular
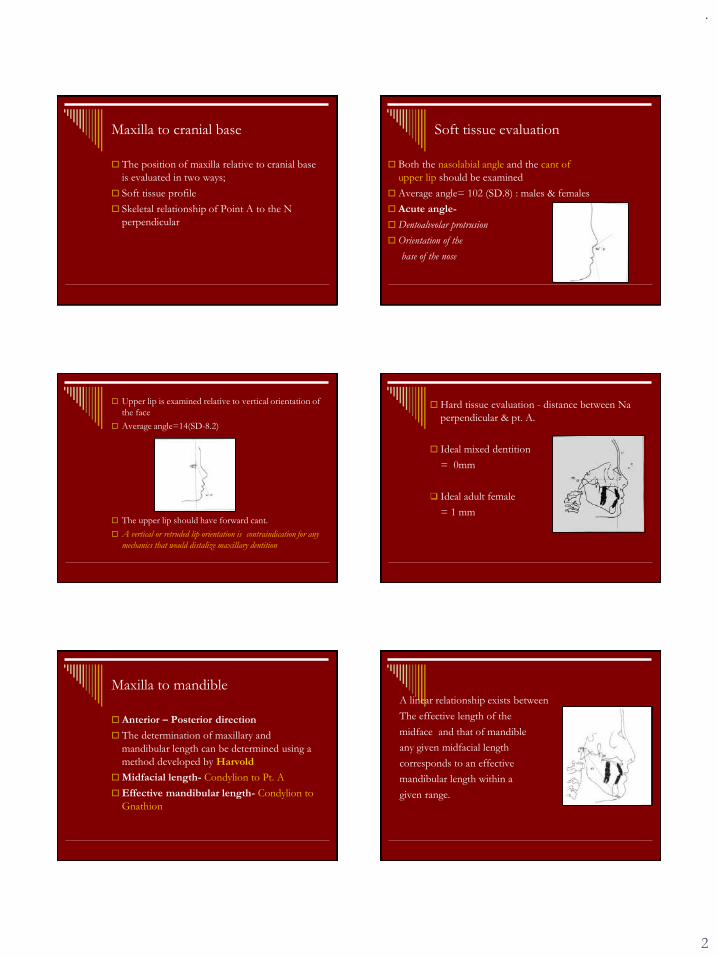
Soft tissue evaluation
Both the nasolabial angle and the cant of
upper lip should be examined
Average angle= 102 (SD.8) : males & females
Acute angle-
Dentoalveolar protrusion
Orientation of the
base of the nose
Upper lip is examined relative to vertical orientation of
the face
Average angle=14(SD-8.2)
The upper lip should have forward cant.
A vertical or retruded lip orientation is contraindication for any
mechanics that would distalize maxillary dentition
Hard tissue evaluation - distance between Na
perpendicular & pt. A.
Ideal mixed dentition
= 0mm
❑ Ideal adult female
= 1 mm
Maxilla to mandible
Anterior – Posterior direction
The determination of maxillary and
mandibular length can be determined using a
method developed by Harvold
Midfacial length- Condylion to Pt. A
Effective mandibular length- Condylion to
Gnathion
A linear relationship exists between
The effective length of the
midface and that of mandible
any given midfacial length
corresponds to an effective
mandibular length within a
given range.

.
3
Maxillo mandibular relationship=
M.L - M.F.
Ideal max. mand differences;
Small= 20 - 30 mm
Medium =25 – 27 mm
Large = 30 – 33 mm
Vertical dimensions
The clinical appearance of the relationship
between the upper and lower jaws is affected
to a great extent by lower facial height
The lower anterior facial height is measured from
ANS to Menton
Increase in LAFH
- downward &
backward position of
chin
❑ Decrease in LAFH
❑ - autorotation of chin in
a forward &upward
direction
An increase or decrease
in LAFH can have
profound effect on the
horizontal relationship
of mandible to maxilla
Other measures of Vertical Dimensions:
Mandibular plane angle
Facial axis of Ricketts.

.
4
Mandible to cranial base
Distance from
pogonion to the Na
perpendicular
Mixed dentition:
-8mm to -6mm
Adult female
-4mm to 0mm
Adult male
-2mm to 4mm
Dentition
Relating the upper incisors to maxilla
A-P position
Ideal distance=
4-6 mm
Advantage over Ricketts
In instances of malrelationships between
maxilla and mandible,serious error may result
if the position of upper incisor is determined
by any measurement that uses the mandible as
reference point.( A-Pog line)
Advantages over Steiner
It is valid only if the maxilla is in a neutral
position A-P relative to cranial base.
Retrusive position of the maxilla relative to
Na- upper incisor appear more flared
Protrusive position- upper incisors appear
more retrusive.
Vertical position:
Incisal edge of upper incisor should lie 2-3mm
below the upper lip at rest.
Upper lip should be at gingival margin while
smiling
Some adjustments may be needed to interpret the meaning of these measurements according to the functional state of the lip musculature and axial inclination of the tooth prior to treatment
Retruded and upright incisors- more gingival tissue is seen.
Following either functional or orthognathic theraapy- a hypotonic lip may become more active, thus changing functional state.

.
5
Relating lower incisors to mandible
A-P position
Ideal distance is 1- 3mm
Vertical position:
Evaluated on the basis of existing LAFH
Excessive curve of spee
intrusion of incisors
or
eruption of molars……????
LAFH excessive or normal
- lower incisors intruded
❑ Inadequate- extrusion or eruption of buccal
segment
Airway Analysis
Upper pharynx-
Post outline of the soft
palate to the closest point on
pharynx
Normal= 15-20mm
<2 – airway impairment
Lower Pharynx
Point of intersection of the post border of
tongue & the inf border of the mandible to the
closest point on post. Pharyngeal wall.
Normal=11-14mm
Smaller than av-
-Little consequences
Greater than av.-
-Possible ant. Positioning
Of tongue
Strengths
Considers changes in midfacial,mandibular, lower ant facial height.
Advantageous over ricketts and steiners on AP positioning of upper incisors to maxilla
It allows interpretation of changes in growth pattern
Linear measurements primarily so that treatment planning for surgery is simplified
Drawbacks
Na perpendicular to Pt. A
Position of N
Position of Pt A
Linear changes are more affected by error in magnification than angular measuremnts
The Quadrilateral
Analysis
-An individualized skeletal assessment
-Developed by- Rocco. J.Di Paolo 1969
.
6
Quadrilateral
The four measures:
Maxillary base length,
Mandibular base length
ALFH & PLFH
Forms the basis for the
quadrilateral analysis of
lower face
The quadrilateral analysis, concerns itself
primarily with the skeletal configurations of
the individual dentofacial complex in both the
horizontal and vertical dimensions, regardless
of dentoalveolar relationship.
It provides an individual skeletal assessment of
each case.
Analysis
Skeletal assessment
Dental assessment
Concepts of lower facial proportionality
In a balanced facial pattern there is a 1:1 proportionality that exists between the maxillary base length and mandibular base length; also the average of ALFH & PLFH equals the denture base.
Skeletal analysis
Two horizontal facial planes are used:
Palatal plane – (ANS- PNS)
Mandibular Plane – (Go- Gn)
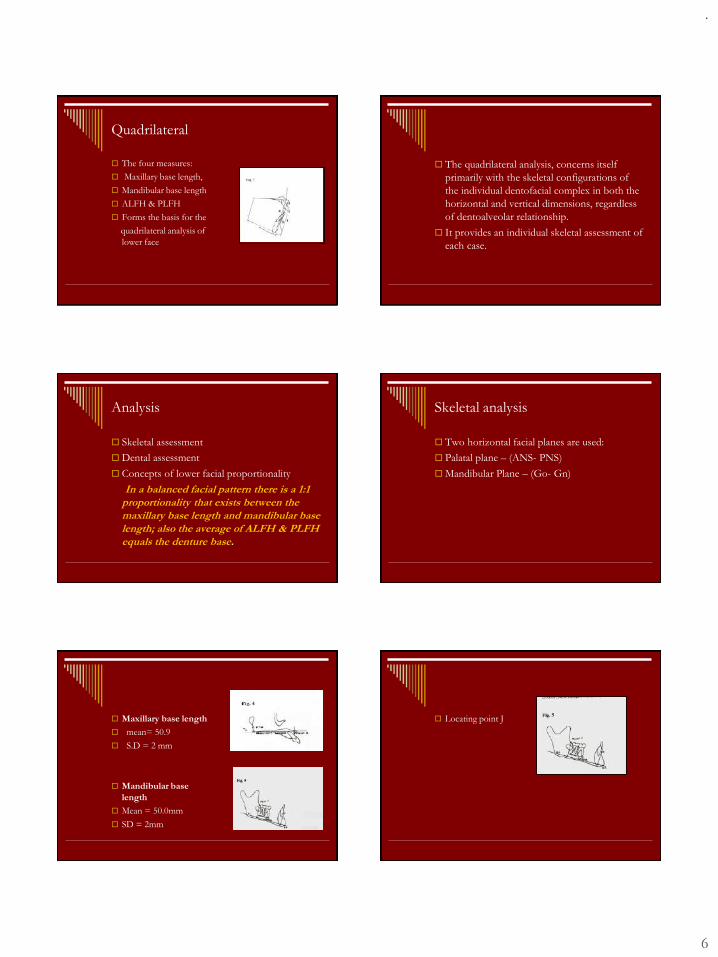
Maxillary base length
mean= 50.9
S.D = 2 mm
Mandibular base
length
Mean = 50.0mm
SD = 2mm
Locating point J
.
7
Anterior lower facial
height
Mean = 60mm
SD – 3.5mm
Posterior lower facial
height
Mean = 39.4mm
SD= 2.2 mm
Anterior upper facial
height
Measured from
projection of Pt.A onto
palatal bone to Nasion
on cranial base
Mean = 49.2mm
SD- 2.3 mm
A proportional relationship exists between
anterior upper facial height and ant lower facial
height.
This proportion is 45:55 and is in agreement
with the original work of Wylie & Johnston.
Angle of facial
convexity
the angle that is formed
by ALFH & ALFH at
the projection of Pt.A
onto the palatal plane.
168-178
SD -3.2
This angle relates the quadrilateral to the
cranial base and upper face.
It is a means of establishing a skeleta profile
assessment.
It focuses on possible areas of skeletal
discrepancies, such as posture of lower facial
complex, cranial base deflections, and denture
base discrepancies.
Dental Assessment
Point A line
Line from Pt. A parallel
to AFH
Measure the distance
between
most ant. Point on
incisors to this line
Average = 5 (SD- 1)
.
8
Point B line
A line from Pt. B
parallel to AFH
Indicates mandibular
incisor position
Av- 2mm
Pogonion line
A line drawn tangent to
pogonion & parallel to
AFH
Indicates chin excessive
/ deficient
Before any dental assessment can be made, a
thorough knowledge of the skeletal pattern of
the patient is essential.
Only then can we relate incisor positioning
with the skeletal pattern that has been
established
Advantages
It informs the clinician of discrepancies
between the sizes of upper and lower jaw.
By using an analysis of vertical proportionality,
we can determine which jaw is normal
It determines the direction & extent of skeletal
dysplasia in millimeter measurement which is
more understandable in surgical orthodontics
than angular measurements.
Bjork Analysis
Sample
Size and age
Group I- 20 twelve years old
Group II- 322 twelve years old
Group III- 281 high school graduates
Race – Scandinavian
Sex- males
It mainly tells about growth pattern .
Takes in account posterior angles
Saddle angle
Articulare angle
Gonial angle
.
9
Saddle Angle- N-S-Ar-
angle between ant
cranial base and post
cranial base
Mean value- 123+ 5
Articular Angle- may be
altered by Orthodontics.
143+6
Bite is opened by extrusion of the post teeth
or distalization- angle increases
Large angel- retrognathic profile
Small angle- prognathic profile
Gonial Angle-
Mean value- 128+ 7
Sum of the posterior angle-
Sum of the three angles, saddle, articulare, and
gonial angle is 396 +6
If it is greater than 396- vertical growth
If it is smaller - horizontalJaraback Analysis
Jarabck 1972

.
10
Sample
Origin – some of the measurements were
taken from B’jork cephalometric analysis
Size- not specified
Race- not specified
Sex- not specified
Age- not specified.
This analysis is mainly concerned with growth
pattern.
For this purpose two measurements are taken
into consideration
Facial height
Gonial angle
Facial height
It is an appraisal of face
in vertical dimension
Determination of AFH
& PFH and use the
result to arrive at a
figure which suggests
direction of growth
AFH
Linear measurement
from Na- Me.
PFH
Linear measurements
from S- Go
Ratio is-
Posterior facial height x 100
Anterior facial height
Mean value= 62-65%
Higher percentage- great PFH & horizontal
growth
Small percentage – short PFH & vertical growth
Gonial Angle
Angle formed by intersection of a line tangent
to post border of ramus and mandibular plane
(Go-Me)
Large angle- posterior rotation of the mandible
Small angle- anterior rotation of the mandible
Determines degree of inclination of ramus to
mandibular plane & growth pattern
.
11
For accurate analysis,
gonial angle is divided
into UGA & LGA by a
line drawn from Na to
Go.
UGA-
Mean 52- 55
LGA
Mean 70-75
Large UGA- horizontal growth pattern
large LGA- vertical growth pattern
The gonial angle has marked influence on
direction of growth, profile changeand the
position of the lower incisors
The magnitude is determined by the relation
between AFH & length of ramus
Increase in AFH- angle is obtuse
Decrease in AFH- acute angle
Posterioanterior
Cephalometry
In cases of dentoalveolar &facial asymmetries
Dental & skeletal crossbite
Functional mandibular displacement.
Methods of Analysis
Ricketts Analysis
Grummons Analysis
Grayson analysis
Hewitt Analysis
RICKETT’S FRONTAL ANALYSIS
Nasal width: importance of attaining normal respiration in the
orthodontic patient.
Used in combination with the palatal plane in clinical diagnosis,
The nasal cavity can be altered with extraoral traction.
Measured from N.C.-N.C.( widest points in nasal capsule)
Increases 0.5mm per yr
.
12
Mandibular width:Basal mandibular width is described by points just below the
trihedral eminence, called Ag (antegonial tubercle).
Stable area undistorted by muscle attachments
Maxillary width:
About a 10mm distance from J point to the fronto-lateral facial line is
desirable.
Symmetry:Symmetry is evaluated by relating point
A and pogonion to the midsagittal
plane,.
A midline plane is dropped through the
top of the nasal septum or crista galli,
perpendicular to the line through the
centers of the zygomatic arches,
asymmetries can be located within the
maxilla or in mandible or in
combination. Thus this information assists
in the diagnosis of unilateral conditions and
severe midline deviations.
Symmetry:Symmetry is evaluated by relating point
A and pogonion to the midsagittal
plane,.
A midline plane is dropped through the
top of the nasal septum or crista galli,
perpendicular to the line through the
centers of the zygomatic arches,
asymmetries can be located within the
maxilla or in mandible or in
combination. Thus this information assists
in the diagnosis of unilateral conditions and
severe midline deviations.
Denture relations in the frontal
Molar width:
In the denture pattern a primary
interest is the lower molar width
relative to the skeleton. In this
molars are evaluated related to
basal bone near its position. The
lower molar measurement
changes with age.
Intermolar width:
It is measured from buccal
surface of the first permanent
molars transversely.
Intercuspid width:
The width between the tips of
the lower cuspids is assessed.
These teeth also changes
relationship during the time of
eruption, requiring the
appraisal of age effects in any
evaluation.

.
13
Denture symmetry:
Similar to basal midlines, the denture
midline is assessed from points
between the upper and lower central
incisor roots. And central sagittal
plane should falls on all these
midlines.
.
Upper to lower molar relation:
Width differences
between upper and
lower molars are useful
in identifying actual and
potential crossbites.
The measurements is
made at most
prominent buccal
contour of each tooth.
The average value is
1mm.
Grummons analysis
Duane. C. Grummons
Martin A. Kappeyne Van De Coppello (1987 jco)
Comparative and quantitative PA ceph analysis: not
related to normative data
2 forms of this analysis: Comprehensive
Summary
The information gathered can be correlated with lat ceph
data to complete a three dimensional facial assessment.
Construction of horizontal planes
Medial aspect of ZF suture
Centers of ZA
Medial aspect of jugal process
Parallel to Z plane
through menton
Construction of mid sagital
reference line
Cg through ANS to chin area
perpendicular to Z plane
Key reference line-
closely follows the visual plane
subnasale & the mid points
between the eyes
MSR- centre of cervical vertebrae
–possible head rotation
In cases of anatomic variations in
upper & middle facial region……
Location of Cg???...
- midpoint of the Z plane through ANS
Upper facial asymmetries???
- midpoint of Z through
mid point of Fr-Fr line

.
14
What may appear as asymmetry on film may
be quite different from patient’s actual
asymmetry if the head to tip or rotate to
conform to the cephalostat…
Extend Z plane and compare the distance
between Z& cranial borders.
To ensure correct head tilt when taking the
radiograph, check the patient from the side to
see FP is close to horizontal.
Mandibular morphology
Left & Right triangles are formed- Co-Ag-Me
Split by ANS-Me line
Linear values
Angles
Anatomy can be measured
Quite sensitive to head
rotation
Volumetric Comparison
2 volumes (polygon) are calculated from the area defined
by Co-Ag- Me &the intersection with a perpendicular
from Co-MSR
Superimposition done
by computer
Maxillo mandibular comparison of
asymmetry
Perpendiculars to MSR from J & Ag
Connecting lines from Cg- J& Ag
Linear asymmetries
Vertical offset & linear distance is measured from MSR-
Co,NC,J,Ag,Me
Maxillo-mandibular relation
Buccal cusps of upper 1st molars along the
perpendiculars
Ag plane, MSR, & ANS-Me
Are drawn to depict the dental
Compensations for any skeletal
Asymmetries.

.
15
Frontal vertical proportions
Upper facial ratio-
Cg-ANS/Cg-Me
❑ Lower facial ratio
ANS-Me/Cg-Me
❑Maxillary ratio
ANS-A1/ANS-Me
❑ Total maxillary ratio
ANS-A1/Cg-Me
Mandibular ratio
B1-Me/ ANS- Me
Total mandibular ratio
B1-Me/Cg-Me
Maxillo mandibular ratio
ANS-A1/B1-Me
Advantages
It provides a practical,
functional method of
determining the
locations and amount of
facial asymmetry
It includes volumetric
comparison
Limitations
Head rotation and
improper construction
of MSR can reduce the
effectiveness of this
analyses.
The measurements are
subjected to distortion
from projection
technique.
Grayson AnalysisBarry Grayson; Fred Bookstein 1983
Landmarks are identified in different frontal planes at
selected depth of the craniofacial complex and
subsequent skeletal midlines are constructed
The analysis enables visualization of midlines and
midpoints in third (sagital dimension)
The midlines and midpoint may be combined and warped
midsagiatl plane can be outcome of this analysis
The analysis is performed on 3 different
acetate tracing papers using the same PA ceph
Separate acetate tracings are made on the same
radiograph, corresponding to structures of the lateral
view

.
16
Tracing 1. A. Orbital rims B. pyriform aperture
C. Maxillary & Mandibular incisors. D. Inferior
border of symphysis
In this 1st drawing, the
anatomy of the most
superficial aspect of the
craniofacial complex, as
indicated by plane A, is
presented.
Tracing 2. A. Greater and lesser wing of
sphenoid. B. lat cross section of the zygomatic
arch. C, coronoid process . D. Maxillary and
Mandibular first molars. E body of the
mandible F mental foramina
These structures are
located on or near the
deeper coronal plane
B
Tracing 3 A. Superior surface of the petrous
portion of the temporal bone B. Mandibular
condyles with outer border of ramus C.
mastoid process, corresponding to plane C
Midline construction for all the 3 planes
The result is a segmented construction of
these midlines, whose angles express the
degree of asymmetry of the structures in this
specific plane.
If the 3tracings are sperimposed, the
phenomenon of warping within craniofacial
skeleton can be observed.
In most asymmetric patients, the craniofacial
asymmetry will appear less severe in the most
post and in the deep lying cranial structures.
.
17
Advantages
3 dimensional multiplane cephalometric
analysis integrating information from both the
PA and basilar cephalometric radiographs.
The study of structures in various coronal and
transeverse planes makes it possible to
measure and record the three dimensional
relationship of anatomic structures to one
another.
Hewitt Analysis
It is performed by dividing the craniofacial
complex in constructed triangles, the so called
triangulation of face.
The different angles, triangles and component
areas can be compared for both the left and
right side.
Cranial base
Lat. Maxillary region
Upper max region
Middle max region
Lower max region
Dental region
Mandibular region
.
1
1
Loops in Orthodontics
Presented by: Dr. Lavesh Pandey
Contents
⚫ Introduction
⚫ Hiistory
⚫ Types of loops
⚫ T-loop
⚫ K-loop.
⚫ M-loop
⚫ Omega loop
⚫ Vertical loop
⚫ K -sir loop
⚫ Opus loop
⚫ Rickets loop
⚫ Box loop
⚫ Bull loop.
⚫ Tear drop
⚫ Triangular loop.
⚫ L-loop.
⚫ Balista loop.
⚫ Rectangular loop.
⚫ L-loop
⚫ Most of the time ,due to anatomic limitations in the oral cavity, it is
not usually possible to devise an intraoral mechanism to deliver a
force whose line of action passes through a tooth's center of
resistance. Equivalent force systems, comprised of forces and
moments, are instead applied to brackets bonded to the tooth's
crown to achieve translatory movement.
⚫ Two approaches can be used to apply the force systems
necessary to trigger the biologic phenomena that result in space-
closing movement of individual teeth or groups of teeth (“en
masse”).
⚫ 1.Sliding mechanics
2. Loop mechanics – a) Segmental and b) Continues.
Introduction.
⚫ Force: is defined as an act upon a body that
changes or tends to change the state of rest or
the motion of that body.
⚫ The correct unit to express forces are
Newtons (N). However, in orthodontics forces
have been commonly expressed in grams.
4
1gm = 0.00981 N (or) 1N = 101.937gm
Basics of the biomechanics.
5
⚫ A force is a “vector”.
⚫ Vector quantities are characterized by having both magnitude &
direction.
⚫ The magnitude of vector represents its size.
⚫ Direction is described by the vector’s line of action, sense & point of
origin (point of application).
⚫ In order to indicate all of these features, force vectors are
represented as arrows. The length of the arrow is proportional to
the magnitude of the force.
Basics of the biomechanics.
6
Line of action
Sense/DirectionOrigin or
point of application
The point of application of a force is indicated by the origin of the arrow.
This is simply the point of contact between the body being moved and
the applied force.
Direction is indicated by the body of the arrow itself and the arrowhead.
Without the head of the arrow, the body alone indicates the line of
action. The sense is determined by which end we put the arrowhead on.
Basics of the biomechanics.

.
2
7
Points Of Application:
Orthodontic forces are commonly applied at the
crowns of a tooth.
1) centre of mass
2) centre of gravity
3) centre of resistance.
⚫ Centre of a mass: is a single point within it
where all of its mass is concentrated.
8
⚫ A tooth in the oral cavity is not a free body
because its supporting periodontal tissues
restrain it. The analogous centre of mass for an
in vivo tooth is referred to as the “centre of
resistance” of the tooth.
⚫ It can be defined as a point at which resistance
to tooth movement is concentrated.
9
Centre of gravity
Centre of resistance⚫ The centre of resistance of single rooted tooth lies
approximately six-tenth of the distance between the
apex of the tooth and crest of the supporting
alveolar bone. ( PROFFIT )
⚫ It lies at 66% of the root length from apex towards
alveolar crest. ( BURSTONE)
• The centre of resistance of multirooted tooth lies just
above the furcation.
• The centre of resistance of whole dentition lies
between the premolar roots.
⚫ If a force is applied to a free body & the force
does not act through the centre of resistance, it
causes the body to rotate.
⚫ Rotation is the movement of a body where no
two points on the body move the same amount
in same direction.
⚫ Moment: The tendency to rotate is called a
moment.
⚫ Moments can be symbolized by curved arrows.
12
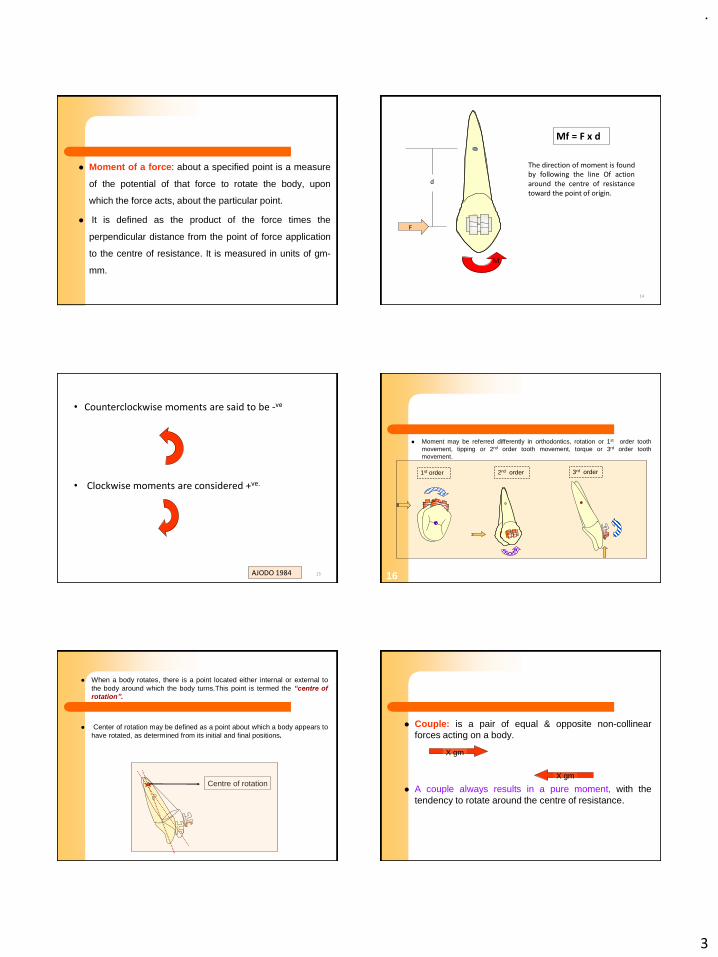
.
3
13
⚫ Moment of a force: about a specified point is a measure
of the potential of that force to rotate the body, upon
which the force acts, about the particular point.
⚫ It is defined as the product of the force times the
perpendicular distance from the point of force application
to the centre of resistance. It is measured in units of gm-
mm.
14
d
Mf = F x d
M
The direction of moment is foundby following the line Of actionaround the centre of resistancetoward the point of origin.
F
15
• Counterclockwise moments are said to be -ve
• Clockwise moments are considered +ve.
AJODO 1984
⚫ Moment may be referred differently in orthodontics, rotation or 1st order tooth
movement, tipping or 2nd order tooth movement, torque or 3rd order tooth
movement.
16
1st order 2nd order 3rd order
17
⚫ When a body rotates, there is a point located either internal or external to
the body around which the body turns.This point is termed the “centre of
rotation”.
⚫ Center of rotation may be defined as a point about which a body appears to
have rotated, as determined from its initial and final positions.
Centre of rotation
18
⚫ Couple: is a pair of equal & opposite non-collinear
forces acting on a body.
⚫ A couple always results in a pure moment, with the
tendency to rotate around the centre of resistance.
X gm
X gm
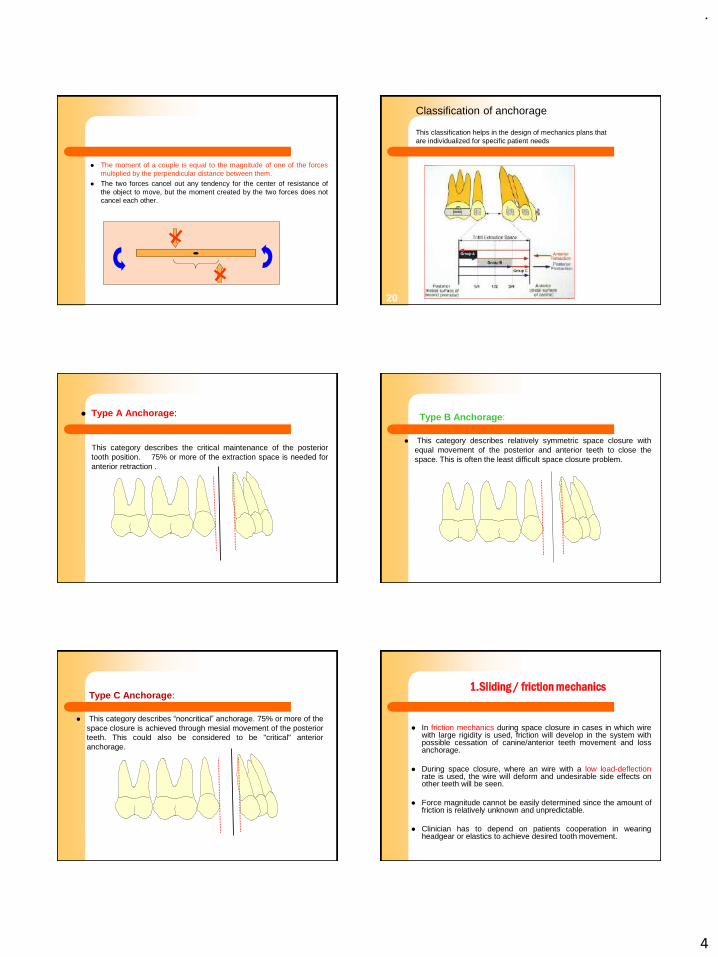
.
4
19
⚫ The moment of a couple is equal to the magnitude of one of the forces
multiplied by the perpendicular distance between them.
⚫ The two forces cancel out any tendency for the center of resistance of
the object to move, but the moment created by the two forces does not
cancel each other.
20
Classification of anchorage
This classification helps in the design of mechanics plans that
are individualized for specific patient needs
21
⚫ Type A Anchorage:
This category describes the critical maintenance of the posterior
tooth position. 75% or more of the extraction space is needed for
anterior retraction .
22
Type B Anchorage:
⚫ This category describes relatively symmetric space closure with
equal movement of the posterior and anterior teeth to close the
space. This is often the least difficult space closure problem.
23
Type C Anchorage:
⚫ This category describes “noncritical” anchorage. 75% or more of the
space closure is achieved through mesial movement of the posterior
teeth. This could also be considered to be "critical" anterior
anchorage.
⚫ In friction mechanics during space closure in cases in which wirewith large rigidity is used, friction will develop in the system withpossible cessation of canine/anterior teeth movement and lossanchorage.
⚫ During space closure, where an wire with a low load-deflectionrate is used, the wire will deform and undesirable side effects onother teeth will be seen.
⚫ Force magnitude cannot be easily determined since the amount offriction is relatively unknown and unpredictable.
⚫ Clinician has to depend on patients cooperation in wearingheadgear or elastics to achieve desired tooth movement.
1.Sliding / friction mechanics

.
5
⚫ Control of the force system that is applied to the teeth is one of themain problems in the field of biomechanics. Straight arch wiresseldom produce forces and moments that are of appropriatedirection and magnitude .For this reason, orthodontic loops havebeen extensively used, either in order to decrease the forcemagnitude or to produce a force system compatible with thedesired tooth movement.
⚫ A major use of loops is the retraction of canines, where a momentto force ratio is essential for the bodily movement. The design of ofthe loop influences the force levels and the moment to forceratio(M/F) in such a way that is difficult to change the one withoutadversely affecting the other.
⚫ Loop:
Loop is a orthodontic spring of various shapes & configurations.
⚫ This approach is friction-free; when activated, the arch wire loops distort from their original configuration; as the tooth (or teeth) moves, the loop gradually returns to its undistorted position, delivering the energy stored at the time of activation.
⚫ Brackets are not sliding along the arch wire during the process. Groups of teeth can therefore be moved with more accurately defined force systems for more precise anchorage control to achieve treatment goals more readily than methods in which friction plays a role.
2.Loop mechanics
⚫ By giving a loop ,that will increase the length of the wire , there bydecreasing the force value and increasing the flexibility.
⚫ To lower the load/deflection rate by addition of more wire.
⚫ Preactivation bends can be placed in loops to obtain higher moment,& to achieve frictionless tooth movement.
⚫ To avoid the inconsistency of the force system delivered by a straightwire. The major reason for putting in a loop is to control the forcesystem to the teeth on either side of the loop.
⚫ To increase the range of activation, to deflect the wire further withoutpermanent deformation.
Why a loop ?
1. It must provide appropriate levels of force and moment-to-force (M/F)
ratios to achieve the tooth displacement desired.
2. It must be able to undergo a reasonable range of activation/deactivation
in which the appliance delivers relatively constant forces and moments.
3. It must be small enough to fit comfortably in the space available for
intraoral treatment.
4. A loop should be “fail safe”- this means that, although a reasonable
range of action is desired from each activation, tooth movement should
stop after a prescribed range of movement even if the patient does not
return for a scheduled appointment.
5. It should be simple.
Ideal properties of a loop:
⚫ Translation of a free body occurs when a net applied force has a
line of action that passes through the body's center of mass. A
constrained body translates when the force's line of action passes
through its center of resistance, a fixed point determined by the
geometry of the body and its constraints.
⚫ It is often desired to move malposed teeth via translation to avoid
localized areas of high stress and strain that can produce
traumatic resorption of tooth roots and investing structures.
Tipping and root movement produce localized high stress areas.
Omega loop.It is fabricated by using .0215X.028 arch
wire
Can be used as a stop and tieback.
Fabrication.
Use a pencil to mark the center of the
wire.
Use tweed loop forming player.
Bend up the distal leg by 20 deg.

.
6
From the cant by slanting towards the ,using the
Beak player 1-1.5mm away from the beak end.
Bend it up the distal leg by 90 deg.
Plier is positioned at the top of the loop.
Bend up the distal leg by 90 deg.
To bend up the distal leg ,hold the plier
Positioned more backward.
Until wire become horizontal,bend the distal leg
Mesial;60 deg,distal ; 90 deg.omega loop must
Be bended at the degree of more powerful slant
Of cant towaards the center.
⚫ The vertical loop has two vertical components and
may be activated in any plane perpendicular to these
components.
⚫ It may be contoured as an open or closed loop.
The Vertical Loop;
⚫ A closed loop will always have a greater range of
activation than an open loop of the same design,
because of the additional wire and because of the
'Bauschinger effect' which states that the range of
activation of loop is always greatest in the direction of
the last bend.
⚫ To activate a open loop the legs of the loop are pulled
apart unbending the loop.
⚫ To activate a closed loop, the legs are brought
together, in the direction of the last bend of the loop.
The Vertical Loop;
Pre- activated vertical loop
⚫ Loop design suggested by Dr. Harry Bull .
⚫ The single open vertical loop is most efficent when used to open
space. In such cases, the arch wire is fixed to the brackets, the
loop is activated by compressing the legs, and as the loop returns
to its original position, the teeth move apart.
⚫ It can be used somewhat less effectively to close space, where a
short range of activity will accomplish the movement. Then it is
activated by opening the legs,.
Vertical loop
⚫ The single open vertical loop may also be used for added labio-
lingual deflection when rotation of a tooth is desired. By contouring
a vertical loop adjacent to the displaced contact of the rotated tooth,
immediate bracket engagement is possible.
⚫ The increased resiliency permits deflection of the loop and allows a
greater duration of activity that will tend to rotate the tooth toward its
desired position.

.
7
Preactivated out-of-plane vertical loop
(a) geometry before installation,
(b) geometry after installation
Dimensions
⚫ The height of a vertical loop is limited by anatomical restrictions. It must
not impinge on the gingival or alveolar tissues. For practical, clinical
consideration, it is rarely possible to use vertical loops longer than 6 or
8mm, thought occasionally 10 mm. loops can be used. Standardizing
loop heights will tend to standardize predicted force potential and allow
the operator predicatable responses on activation.
⚫ The double vertical loop is contoured on either side of a
tooth and has two effective uses. One is to move a labially
or lingually displaced tooth into line through the labiolingual
spring quality inherent in the horizontal section between the
two loops. The other is to rotate a tooth.
⚫ When tied into the bracket of a rotated tooth, the loop on
one side of the tooth will be displaced labially, causing a
reciprocal rotational activity on the brackets.
The Double vertical Loop:
⚫ The double vertical loop has also been used to move a tooth
bodily in a mesial or distal direction. This is accomplished by fixing
or stopping the connecting horizontal section to the brackets, so
that the archwire cannot slide, and then opening one loop and
compressing the other. The contraction and expansion of the
loops will tend to move the tooth bodily in a mesial or distal
direction.
The Double vertical Loop:
TWIN HELICAL LOOP.
⚫ The presecne of two helices provides additional wire, permitting
greater force reduction and longer range of activity.
⚫ It is used to shorten arch length where great range of activity is
desired.
Modifications of the Vertical Loop.
TWIN HELICAL LOOP.
⚫ The design of this loop permits the legs to touch each other, using
minimal space in the interbarcket span.
⚫ The presecne of two helices provides additional wire, permitting
greater force reduction and longer range of activity.
⚫ Because of the position of the helices, this loop is activated by
extension, or drawing the legs apart. This, in turn, follows the
principle of activation the loop in the direction of the contour, in
that extension of the legs continues to wind the two helices.
.
8
T-loop.
⚫ The segmented arch technique, as developed by Burstone,
utilizes T-loop space closure springs for anterior retraction,
symmetric space closure or posterior protraction
⚫ One of the underlying principles of a segmented approach is
to treat the anterior and posterior units as if they were each
one large tooth. Each segment should be prepared for space
closure with the placement of large rectangular wires in the
bracket slots. The left and right buccal segments are
connected with a transpalatal arch or lingual arch, creating a
single large posterior unit.
⚫ The configuration for the basic T-loop spring uses .017x .025"
TMA wire.
General Concepts for Segmented T-Loop Use :
⚫ Understanding an appliance design requires
recognition of the passive form of a spring and
its activation. There are no forces or moments
acting on the spring in this state. The activation
of the spring requires the application of, forces
and moments to engage the spring in the
brackets or tubes. The spring exerts a force
system on the teeth in its active form.
⚫ An essential concept in understanding the use of T-loops for space closure is the neutral position. The neutral position is found by applying the activation moments to the spring without any horizontal forces. In other words, the anterior and posterior extensions of the spring are "twisted" to bring each level to its respective attachment on the occlusal plane. In this position the spring has zero horizontal force
⚫ The horizontal force is produced by pulling the
"T" open from this position. The activation of
the spring is always considered with respect to
the neutral position, and this can be evaluated
only by the application of the activation
moments. When the proper preactivation
bends are placed, the spring is designed such
that the spring forms a "T" in the neutral
position.
⚫ Differential anchorage is obtained by the application of
unequal alpha and beta moments. The higher moment
is applied to the anchorage teeth.
⚫ The differential moments are obtained by applying the
concept of the off-center V-bend. An off-center V-bend
in a wire results in unequal moments. The closer the V-
bend to a tooth or set of teeth, the higher the applied
moment
⚫ The segmented T-loop approximates a "V" shape.
Centering the T-loop equally between the anteror and
posterior tubes produces equal and opposite moments.
Positioning the loop slightly off center relative to the
anterior and posterior tubes generates unequal
moments. The spring is positioned closer to the
anchorage teeth. Clinically, the spring usually needs to
be 1 to 2mm closer to one side than to the other to
obtain a moment differential.

.
9
⚫ Subtle changes in the position of the V-bend can resultin significant changes in the moment magnitudes,especially with small interbracket distances.
⚫ One advantage of the segmented T-loop is the use of alarger interbracket distance, reducing the relative effectof minor errors in spring position.
⚫ For instance, a 1 mm error is a smaller proportion of a20 mm inter-bracket distance than a 10 mminterbracket distance
⚫ The T-loop can be activated of up to 6 mm. At
full 6 mm activation, tooth movement occurs in
three phases—tipping, translation, and root
movement.
⚫ For a symmetric, centered spring, the initial
force system applies a M/F ratio of about 6/1 to
the teeth. This results in tipping movement of
the anterior and posterior teeth into the space.
⚫ With about 2 mm of deactivation or space closure
(spring activation = 4 mm), the M/F ratio increases
toward 10/1, resulting in bodily tooth movement or
translation
⚫ With one to two more millimeters of space closure
(spring activation = 2-3 mm), the M/F ratio increases to
12/1 and higher. The high M/F ratio results in root
movement. In typical clinical application, the spring
does not need reactivation until all three phases of
tooth movement have been expressed
The three important criteria in the use of T-loop are:
⚫ T-loop design.
⚫ T-loop pre activation or gabling
⚫ T-loop position
T-loop pre-actication:
This design uses 0.017 x 0.025" TMA wire.
An essential concept in understanding use of T- loop for space
closure is the neutral position. The neutral position is found by
applying the activation moments to the spring without any
horizontal forces. The horizontal force is applied by pulling the T
open from its position
Checking neutral position. Equal
and opposite moments are
applied to spring, no horizontal
forces are applied so that
horizontal arms become parallel,
position of vertical arms are
checked
Trial activation. Horizontal arms are
kept parallel by applying force and
moment. Trial activation adds to
stability of spring shape

.
10
Before the “T” spring in inserted in to the mouth the spring needs
to be prepared as followes:
⚫ Curvature is bent in the occlusal part of the spring . this is the part
of the spring that may deform during activation and therefore,
needs to be over bent and followed by a trial activation. Remove
the excess curvature.
Open the ears in the gingival part of the T-spring and
add some angle on the occlusal part vertical arms so the
neutral position is correct.
Recheck the T-spring on the template which is the guide
for the required angulations.
Group B anchorage is the simplest
form of space closure. The
requirements for space closure
include equal translation of the
anterior and posterior segments into
the extraction space. Equal and
opposite moments and forces are
indicated. A T-loop spring centered
between the anterior (canine) and
posterior (molar) attachments
produces this force system.
T-loop position:
Symmetric Space Closure
-Group B Anchorage
The center position of the spring can be found by
⚫ To determine the amount of distal activation, the
following formula is used to establish spring length.
Distance = ( Inter bracket Distance – Activation ) / 2
⚫ Distance =the length of the anterior and posterior arms.
⚫ Inter bracket Distance = inter-tube distance from the
mesial of the molar tube to the canine auxillary tube.
⚫ Activation= 6mm in this spring
Symmetric Space Closure
-Group B Anchorage
⚫ With the use of a vertical tube at the canine, a 90°
gingival bend at the calculated distance eases
placement and monitoring throughout space closure. If
the canine bracket does not have a vertical tube,
crimpable "cross-tubes" may be attached to the
anterior segment. To insert the T-loop place the spring
in the auxiliary molar tube. Then the 90° bend is
inserted into the canine tube. The distal end is pulled
back until the distal arm is the desired length, which
results in the desired activation (usually 6 mm
Symmetric Space Closure
-Group B Anchorage
⚫ At 6 mm activation, the spring delivers an M/F
ratio of about 6/1 with a horizontal force of
approximately 320- 340 g. The horizontal force
dissipates at a rate of about 60 g/mm. The
tooth movement is expected to follow the
phases -tipping, translation, and root
movement.
Symmetric Space Closure-Group B Anchorage

.
11
⚫ Space closure should be monitored periodically. To
check the remaining activation, the spring is removed
from the canine tube and the remaining activation at
the neutral position is measured. The activation equals
the distance the gingival bend must be pulled mesially
to be inserted into the canine tube. The passive spring
form should also be evaluated since distortions in the
spring shape will alter the force system
⚫ The progress of the space closure is assessed by observing
the amount of remaining space, the the axial inclinations of
the anterior and posterior segments, and the occlusal
relations.
⚫ During the tipping phase the anterior and posterior occlusal
planes angles towards one another due to the segments'
tipped axial inclinations. This angulation corrects during the
root movement. When the occlusal planes regain
parallelism, spring reactivation is indicated.
⚫ The amount of reactivation of the spring should be based on
the space closure requirements at that time
⚫ The biomechanical paradigm forthis space closure problem is toincrease the posterior M/F ratio(beta M/F ratio) relative to theanterior M/F ratio (alpha M/F ratio)
⚫ Utilizing the V-bend principle, theT-loop is positioned closer to theposterior attachment or the molartube. It is not necessary to be veryfar off center to obtain anadequate moment differential, withmost cases requiring only 1-2 mmoff centering.
Maximum Posterior Anchorage
-Group A Space Closure
⚫ Activate the spring 4 mm for Group A space closure.
This reduces the horizontal force without adversely
affecting the moment difference. The moment
difference remains as the space closes and the spring
deactivates. The spring must be reactivated when 2mm
or less of activation remains.
Maximum Posterior Anchorage
-Group A Space Closure
⚫ Because the beta moment is greater than the alpha moment,
a vertical intrusive force acts on the anterior segment. This
intrusive force may exaggerate the tipping tendency and the
steepening of the anterior occlusal plane. Likewise, the
increased beta moment may steepen the posterior occlusal
plane. Maintaining an adequate horizontal force helps reduce
these effects. The posterior occlusal plane can also be
controlled with the use of a high-pull head gear
Maximum Posterior Anchorage
-Group A Space Closure
⚫ It is likely that a root correction stage will be required
following Group- A space closure. The nature of the
root correction needed will depend on the specific
needs of the case. En-masse anterior and posterior
root correction, anterior root correction, or separate
canine root correction are common possibilities
Maximum Posterior Anchorage
-Group A Space Closure

.
12
⚫ At an activation of 3mm, a horizontal force of 118g is
generated. The alpha M/F is 5.8 while the beta M/F is
10.2. At this activation, the anterior segment is undergoing
controlled tipping while the posterior anchorage unit
undergoes translation or root movement. As the spring
deactivates 1mm further during space closure, the beta
M/F ratio increases to 13.8. The spring should be
reactivated at the time.
Maximum Posterior Anchorage
-Group A Space Closure
⚫ Controlled tipping of the anterior teeth through the
range of activation is produced by a relatively
constant M/F of 5-6. Because alpha M < beta M,
vertical forces are produced, an intrusive force
anteriorly and an extrusive one posteriorly
Maximum Posterior Anchorage
-Group A Space Closure
⚫ Posterior protraction is the
most difficult space closure
procedure. The biomechanical
principle reverses the
approach to group A space
closure.
⚫ The alpha moment is
increased relative to the beta
moment. The difficulty results
from this extrusive force, thus
deepening the overbite.
Maximum Anterior Anchorage
-Group C Space Closure:
⚫ In group C space closure with a segmental T-loop, the
spring is positioned closer to the anterior segment. It is
important that the anterior wire segment achieve full
bracket engagement; otherwise, the play with in brackets
reduce the effectiveness of the moment differential. One
or two millimeters closer to the anterior teeth is typically
all that is necessary.
Maximum Anterior Anchorage
-Group C Space Closure:
⚫ Space closure can be expected to proceed with mesial
tipping of the buccal segment. To reduce the horizontal
force, an activation of 4mm is recommended. The
spring should be reactivated approximately every
2mm.
⚫ The major side effects to monitor are loss of anterior
anchorage control. For mandibular molar protraction,
class ll elastics from the mandibular first molar to the
maxillary canine further increases the force on the lower
buccal segment.
⚫ Class lll elastics aid in protracting upper buccal segments,
although protraction headgear may be used to the upper
buccal segments, although compliance may be
questionable

.
13
Many times, because of anterior crowding or a midline
discrepancy, space must be made available through
separate canine retraction. The same treatment
decisions with regard to retraction and anchorage
requirement must be made as are made for enmasse
retraction. The choice of mechanics is determined by
the type of movement desired and anchorage
requirements
Canine retraction:
⚫ Because the force applied is buccal to the centre of
resistance of the canine, a moment is produced on that
canine during separate canine retraction, which will
cause the canine to rotate distal-in while it retracts.
⚫ There are two ways to counteract this moment.
1. Simultaneously applying a force from the lingual
2. Placing anti-rotation bend in to the retraction spring
⚫ Differential anchorage is obtained by the application of
unequal alpha and beta moments.
⚫ The higher moment is applied to the anchorage teeth.
⚫ The differential moments are obtained by applying in
concept of off-center V-bend.
⚫ An off center v - bend in a wire results in unequal
moments. The closer the v - bend to a tooth, higher the
moment applied
⚫ The segmented T-loop approximates a ‘V’- shape.
Centering the T-loop equal between the anterior and
posterior tubes generates equal and opposite moments.
positioning the T- loop slightly off center relative to the
posterior and anterior tubes produces unequal moments.
The spring is positioned closer to anchorage teeth, clinically
the spring usually needs to be 1 to 2mm closer to one side
than to the other side to obtain a differential moment.
A, Spring in passive form after insertion into molar auxiliary tube.
B, Spring in neutral position, activation is horizontal distance spring
must be pulled for insertion into canine vertical tube.
C. Spring activated and inserted into canine tube.
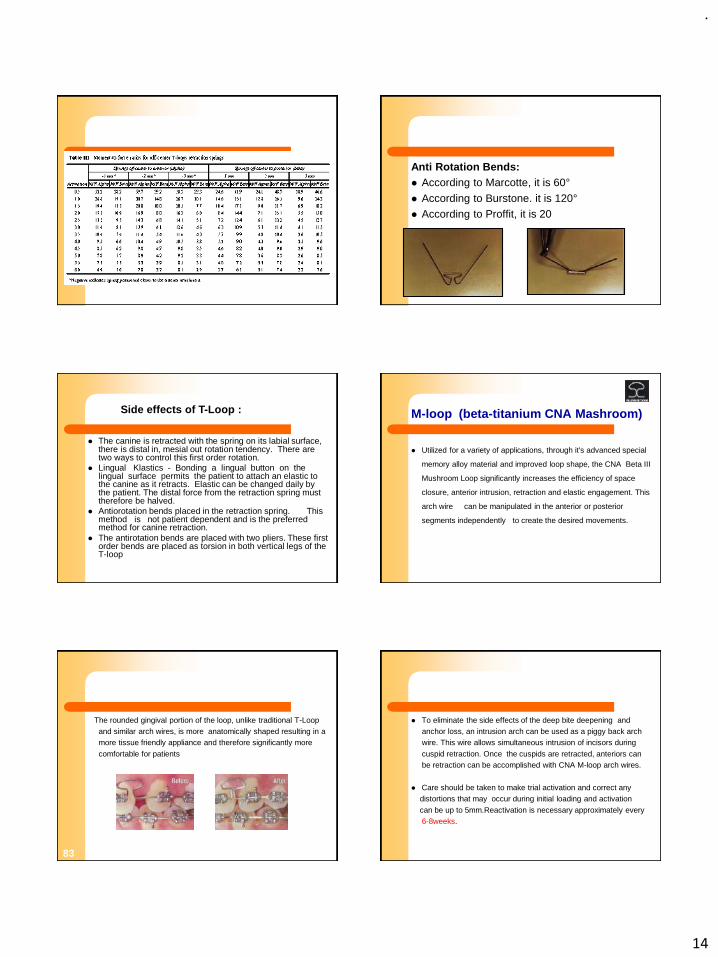
.
14
Anti Rotation Bends:
⚫ According to Marcotte, it is 60°
⚫ According to Burstone. it is 120°
⚫ According to Proffit, it is 20
⚫ The canine is retracted with the spring on its labial surface, there is distal in, mesial out rotation tendency. There are two ways to control this first order rotation.
⚫ Lingual Klastics - Bonding a lingual button on the lingual surface permits the patient to attach an elastic to the canine as it retracts. Elastic can be changed daily by the patient. The distal force from the retraction spring must therefore be halved.
⚫ Antiorotation bends placed in the retraction spring. This method is not patient dependent and is the preferred method for canine retraction.
⚫ The antirotation bends are placed with two pliers. These first order bends are placed as torsion in both vertical legs of the T-loop
Side effects of T-Loop : M-loop (beta-titanium CNA Mashroom)
⚫ Utilized for a variety of applications, through it's advanced special
memory alloy material and improved loop shape, the CNA Beta III
Mushroom Loop significantly increases the efficiency of space
closure, anterior intrusion, retraction and elastic engagement. This
arch wire can be manipulated in the anterior or posterior
segments independently to create the desired movements.
The rounded gingival portion of the loop, unlike traditional T-Loop
and similar arch wires, is more anatomically shaped resulting in a
more tissue friendly appliance and therefore significantly more
comfortable for patients
83
⚫ To eliminate the side effects of the deep bite deepening and
anchor loss, an intrusion arch can be used as a piggy back arch
wire. This wire allows simultaneous intrusion of incisors during
cuspid retraction. Once the cuspids are retracted, anteriors can
be retraction can be accomplished with CNA M-loop arch wires.
⚫ Care should be taken to make trial activation and correct any
distortions that may occur during initial loading and activation
can be up to 5mm.Reactivation is necessary approximately every
6-8weeks.

.
15
M-Loop space closing arch wires
⚫ The contoured mushroom loop evenly transmits forces from and to
the anterior and posterior segments, creating an even and
continuous force for movement throughout treatment.
⚫ Minimal adjustments are needed as the memory attributes of the
wire provide predictable space closure in horizontal, transverse
and vertical directions.
⚫ To increase or decrease incisor torque, create a bend on the
mesial side of the loop.
⚫ For critical anchorage control, bend the posterior leg of the loop
gingival, to promote distal tip back.
⚫ Loops can be spread and opened for retraction or auxiliary springs
or elastomerics can be utilized for retraction
⚫ The arch wire choice for 0.022 bracket
priscription is a preformed M-loop
0.017X0-025 CNA, available with
Std.interloop distances from 26 -46mm.
⚫ Pre –activtion canbe done by seperating
the legs of M-loops approximately 3mm .
Additional gable bend may be placed ,as
needed mesially ti increase anterior
moment(torque) and distal to M-loop to
increase anchorage moment.The wire is
ready to be activated appproximately
4mm (3mm preactivation+ 1mm
activation).
Reactivation is necessary every 6-8
weeks.
⚫ Finishing phase- 0.017X0.025 or
0.018X0.025 CAN wires.
K -Loop
⚫ The K-Loop for Molar Distalization.
⚫ Developed by Valrun Kalra
⚫ Made of .017" X .025" TMA wire.
Legs of appliance bent
down 200.
Wire marked at mesial of
molar tube distal of premolar
bracket.
Bend placed 1 mm distal to distal mark
and 1 mm mesial to mesial mark. Stop
should be well defined and about 1.5mm
long
Wire marked at mesial of molar tube
distal of premolar bracket
Moments and forces produced by K-loop

.
16
.
200 bends in the appliance legs produces moments that counteract the tipping moments created by the force of the appliance, and these moments are reinforced by the moment of activation as the loop squeezed into place. Thus the molar undergoes a translatory moment instead of tipping
92
200
K-SIR loop
⚫ Simultaneous Intrusion and Retraction of the Anterior teeth
⚫ Designed by VARUN KALRA,
⚫ Retraction of the six anterior teeth under the edgewise system is
usually carried out in two distinc tsteps: canine retraction followed
by incisor retraction. In the Begg and Tip-Edge techniques, on the
other hand, the canines and incisors are retracted enmass .
⚫ Separate canine retraction has the disadvantages of increased
treatment time and the creation of an unesthetic space distal to
the incisors. The rationale for separate retraction in the edgewise
technique is that molar anchorage is conserved. However,
Burstone1 and Nanda2 have demonstrated molar anchorage
control, using non-frictional loop mechanics for en masse
retraction of the anterior teeth,that compares favorably with that of
conventional edgewise sliding mechanicsd en masse.
An appliance for simultaneous intrusion and retraction of the six
anterior teeth should ideally control:
⚫ Magnitude of forces and moments
⚫ Moment-to-force ratio
⚫ Constancy of forces and moments
⚫ Friction
⚫ From a practical standpoint, the appliance should:
⚫ Be easy to fabricate and adjust
⚫ Be comfortable for the patient
⚫ Require a minimal amount of patient cooperation
⚫ Be cost-effective
Appliance Design
⚫ The K-SIR (Kalra Simultaneous Intrusion and Retraction) archwire
is a modification of the segmented loop mechanics of Burstone1
and Nanda.2 It is a continuous .019" X .025" TMA archwire with
closed 7mm X 2mm U-loops at the extraction sites
•To obtain bodily movement and prevent tipping of the teeth into the
extraction spaces, a 90° V-bend is placed in the arch wire at the level of
each U-loop Centered .
•90° V-bend creates two equal and opposite moments (red) that counter
tipping moments (green) produced by activation forces. This V-bend, when
centered between the first molar and canine during space closure, creates
two equal and opposite moments to counter the moments caused by the
activation forces of the closing loops .
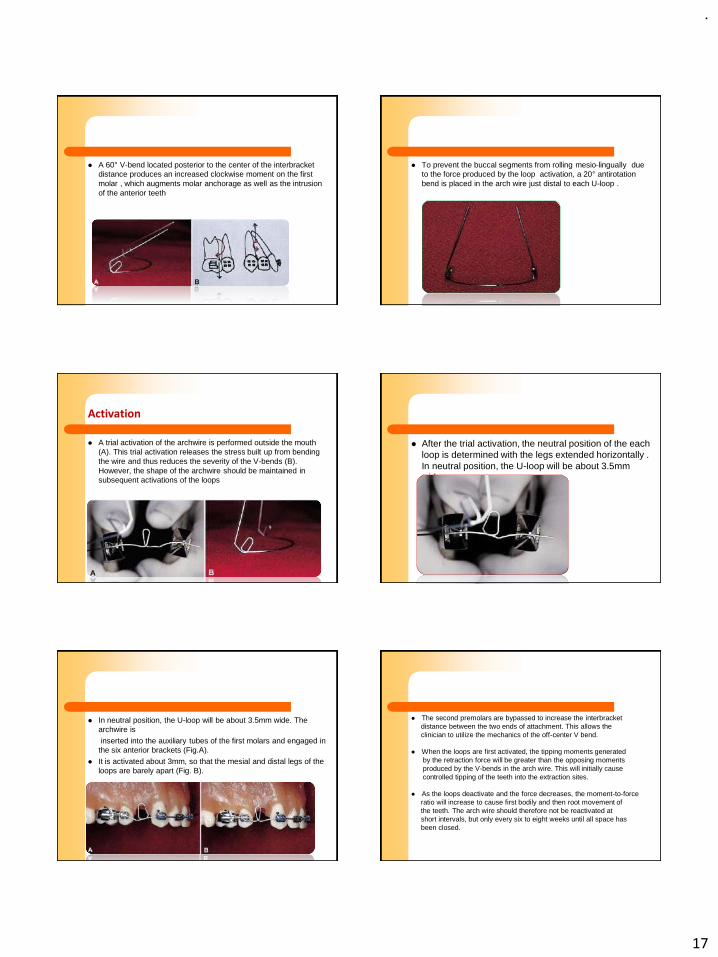
.
17
⚫ A 60° V-bend located posterior to the center of the interbracket
distance produces an increased clockwise moment on the first
molar , which augments molar anchorage as well as the intrusion
of the anterior teeth
⚫ To prevent the buccal segments from rolling mesio-lingually due
to the force produced by the loop activation, a 20° antirotation
bend is placed in the arch wire just distal to each U-loop .
Activation
⚫ A trial activation of the archwire is performed outside the mouth
(A). This trial activation releases the stress built up from bending
the wire and thus reduces the severity of the V-bends (B).
However, the shape of the archwire should be maintained in
subsequent activations of the loops
⚫ After the trial activation, the neutral position of the each
loop is determined with the legs extended horizontally .
In neutral position, the U-loop will be about 3.5mm
wide
⚫ In neutral position, the U-loop will be about 3.5mm wide. The
archwire is
inserted into the auxiliary tubes of the first molars and engaged in
the six anterior brackets (Fig.A).
⚫ It is activated about 3mm, so that the mesial and distal legs of the
loops are barely apart (Fig. B).
⚫ The second premolars are bypassed to increase the interbracket
distance between the two ends of attachment. This allows the
clinician to utilize the mechanics of the off-center V bend.
⚫ When the loops are first activated, the tipping moments generated
by the retraction force will be greater than the opposing moments
produced by the V-bends in the arch wire. This will initially cause
controlled tipping of the teeth into the extraction sites.
⚫ As the loops deactivate and the force decreases, the moment-to-force
ratio will increase to cause first bodily and then root movement of
the teeth. The arch wire should therefore not be reactivated at
short intervals, but only every six to eight weeks until all space has
been closed.

.
18
⚫ Off-center V-bends will generate an extrusive force on the molars,
which is usually undesirable. One of the keys to preventing
unwanted side effects of an appliance is to keep the reactive
forces at a minimum while exerting an optimum level of force on
the teeth to be moved.
⚫ The K-SIR arch wire exerts about 125g of intrusive force on the
anterior segment and a similar amount of extrusive force
distributed between the two buccal segments --generally the first
permanent molars and the second premolars, connected by
segments of TMA wire (Fig. 7A). The force of 125g is effective for
intrusion of the anterior teeth, while the reactive extrusive force on
the buccal segments is countered by the forces of occlusion and
mastication.
⚫ Extrusion of the buccal segments is not usually noted, either
clinically or cephalometrically
Control of Reactive Forces
⚫ Another way to reduce the effects of the reactive force
is to add teeth to the anchorage unit. Including the
second molar will, of course, also increase anchorage
in the anteroposterior direction.
⚫ If even more anchorage is needed to resist both
anterior movement and the extrusive force on the
buccal segments, a high-pull headgear can be added
to the molars.
JCO-Online - VOLUME 35 : NUMBER 9 : PAGES (535-540) 1998
Indications.
⚫ The main indication for the K-SIR archwire is for the
retraction of anterior teeth in a first-premolar extraction
patient who has a deep overbite and excessive overjet,
and who requires both intrusion of the anterior teeth
and maximum molar anchorage.
⚫ However, the archwire can be modified to close
extraction spaces in moderate and minimum
anchorage situations with varying degrees of overbite.
Advantages.
⚫ Its simplicity of design, with a minimal amount of wire in
the loop configuration. It is, therefore, easy to fabricate,
comfortable for the patient, and less likely to cause
tissue impingement. The .019"X .025" TMA provides
sufficient strength to resist distortion, as well as enough
stiffness to generate the required moments.
⚫ At the same time, the design of the arch wire and the
material properties of TMA combine to produce
relatively low forces, a low load-deflection rate, and a
range of activation that allows the appliance to
continue closing space over an eight-week period.
⚫ Due to the frictionless mechanics used for space closure in this
system and the presence of the offcenter V-bend, which acts like
an anchor bend, molar anchorage control is excellent, even
withoutheadgear. The clinician is thus less dependent on patient
cooperation for a successful result in a maximum anchorage
situation.
⚫ Because the intrusion of the six anterior teeth occurs at the same
time as their retraction, and because the canines and incisors are
retracted as a unit, the K-SIR archwire shortens treatment time
compared to conventional edgewise mechanics. In addition, the
en masse retraction of the six anterior teeth prevents the
appearance of an unsightly space distal to the incisors, which
occurs if the canines are retracted separately
Opus Loop:
⚫ Developed by Raymond E. Siatkowski in 1997.
⚫ To achieve net translation, orthodontists have had to add residual moments tothe closing loop arch wire with angulation bends (gable bends) anterior &posterior to the loop.
⚫ Adding these residual moments has several disadvantages:
a) the teeth must cycle through controlled tipping to translation to root movement to achieve net translation.
b) the corect residual loops are difficult to achieve
c) the resulting ever changing PDL stress distribution may not yield the most rapid, least traumatic method of space closure.
⚫ He designed a new spring which delivers a non varying target M/F ratio within the range of 8.0-9.1 mm inherently, without adding residual moments by twist or bends anywhere in the arch wire or loop before insertion
Am J Orthod Dentofac Orthop 1997;112:393-402.)
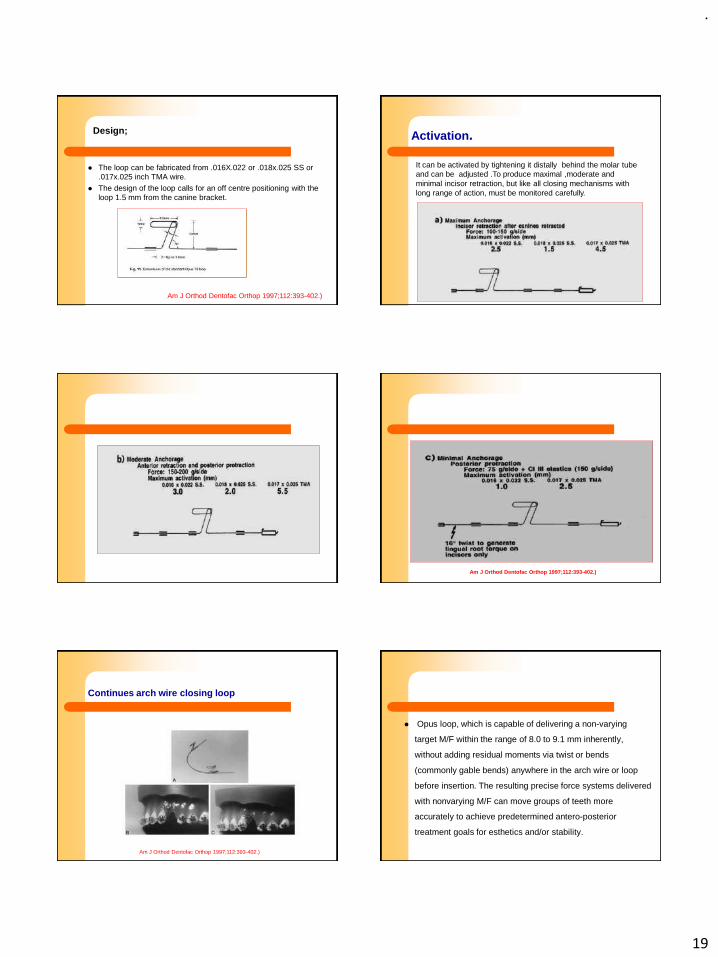
.
19
Design;
⚫ The loop can be fabricated from .016X.022 or .018x.025 SS or
.017x.025 inch TMA wire.
⚫ The design of the loop calls for an off centre positioning with the
loop 1.5 mm from the canine bracket.
Am J Orthod Dentofac Orthop 1997;112:393-402.)
Activation.
It can be activated by tightening it distally behind the molar tube
and can be adjusted .To produce maximal ,moderate and
minimal incisor retraction, but like all closing mechanisms with
long range of action, must be monitored carefully.
Am J Orthod Dentofac Orthop 1997;112:393-402.)
Continues arch wire closing loop
Am J Orthod Dentofac Orthop 1997;112:393-402.)
⚫ Opus loop, which is capable of delivering a non-varying
target M/F within the range of 8.0 to 9.1 mm inherently,
without adding residual moments via twist or bends
(commonly gable bends) anywhere in the arch wire or loop
before insertion. The resulting precise force systems delivered
with nonvarying M/F can move groups of teeth more
accurately to achieve predetermined antero-posterior
treatment goals for esthetics and/or stability.

.
20
Gjessing’s canine retraction spring
⚫ Designed by Paul Gjessnig, Denmark
Spring design
⚫ The resultant spring design, made from
0.016 by 0.022 inch stainless steel wire
.The predominant active element is the
ovoid double helix loop extending 10
mm apically. It is included in order to
reduce the load/deflection of the
spring and is placed gingivally so that
activation will cause a tipping of the
short horizontal arm (attached to the
canine) in a direction that will increase
the couple acting on the tooth.
AJO-DO, Volume 1985 May (353 - 362): - Gjessing
⚫ Height is limited by practical considerations,
so that a double loop is necessary to
incorporate sufficient wire.
⚫ The gently rounded form avoids the effect
of sharp bends onload/deflection and,
through the use of the greatest amount of
wire in the vertical direction, reduction of
horizontal load/deflection is maximized. At
the same time, minimizing horizontal wire
increases rigidity in the vertical plane.
⚫ The smaller loop occlusally is incorporated to
lower levels of activation on insertion in the
brackets in the short arm (couple) and is
formed so that activation further closes the
loops.
⚫ The mesial and distal extensions of the looped
wire segment are angulated both in the
vertical and in the horizontal plane. When the
spring is in place, but prior to activation of the
driving force (neutral spring position, F = 0
gm), static antitip and antirotation couples will
be exerted to the canine
Activation
⚫ The distal driving force is generated by pulling the distal, horizontal leg
through the molar tube. A desirable force level of approximately 160 gm is
obtained when the two sections of the double helix are separated 1 mm.
During the activation the force is matched by an additional couple
(activation couple) arising from the double-helix loop which, in theory,
acts as four lever arms.
⚫ Incorporation of a segment of a circle ("sweep") in the distal leg of the
spring is an adjustment with the purpose of eliminating undesirable ß
moments acting at the second premolar bracket and tending to move the
root apex too far mesially.
⚫ Arch loops used doubly in pairs are
very efficient in moving teeth bodily
in a mesiodistal direction.
⚫ The loop toward which the
movement is to be made is usually a
closed, while that at the other end is
an open loop.
⚫ The arch wire on either side of the
loop is immobilized by the use of
stops.
⚫ The closed loop is opened during
activation and open loop is
compressed.
Double loop or arch loops:

.
21
Disadvantages PG spring
⚫ Difficult to control the position of the canine in all three planes as it
is retracted.
⚫ Enmass retraction using segmental retraction of canines does
not fail safe, because no stops to prevent excessive movement in
wrong direction.
⚫ Missed appointment and a distorted spring can cause potential
problem.
R-loop.
⚫ It can be fabricated by using 0.017 x 0.025” TMA wire
⚫ For a given tooth movement only one combination of force
and moment is correct R Loop can be used for 1st/2nd/3rd
order corrections.
⚫ All combinations of moments and forces are possible low
load deflection /large range of activation
⚫ No inconsistent force systems
⚫ Constancy of Force
⚫ Tooth movement produced by deactivation – friction not an
issue!
⚫ Dissociation of forces and moments possible
⚫ Ccontrol the appliance !!
Dimensions of R -loop
A B
A – mesial of molar tubeB – half of LL = distance between mesial of molar tube and distal of second premolar bracket
A B All bends are made with 442 ( ribbon arch ) plier
Right angle bend atmark B
A B
C
C – sufficient to clear the premolar bracket without interferenceapproximately 6-7 mm

.
22
A B
C
Horizontal bend at C A B
C D
D = L + bracket width (appr.5 mm)
L = distance between mesialof molar tube and distal of second premolar bracket
A B
C D
Vertical bend at D
A B
C D
E
E – equal to the distance between points B and C
A B
C D
E
Horizontal bend at mark E, bend the wire gingivally just short of the vertical segment A B
C D
E
Horizontal bend gingivallyJust short of the vertical leg
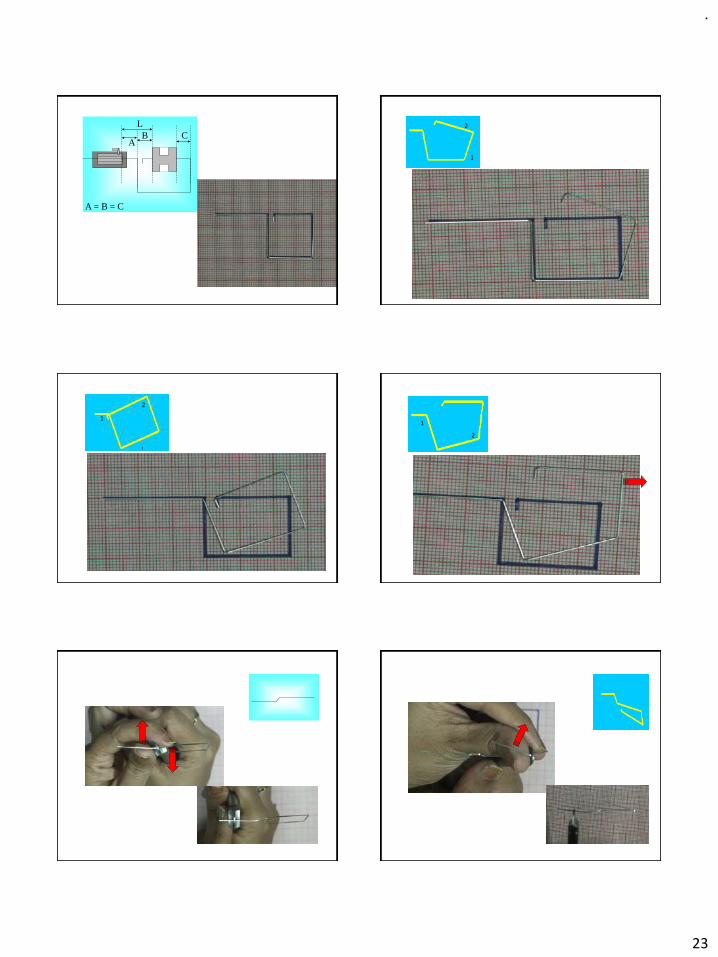
.
23
AB C
A = B = C
L
1
2
1
2
1
2

.
24
Dissociation of forces and moments
A B C
A B C
Dissociation of forces and moments
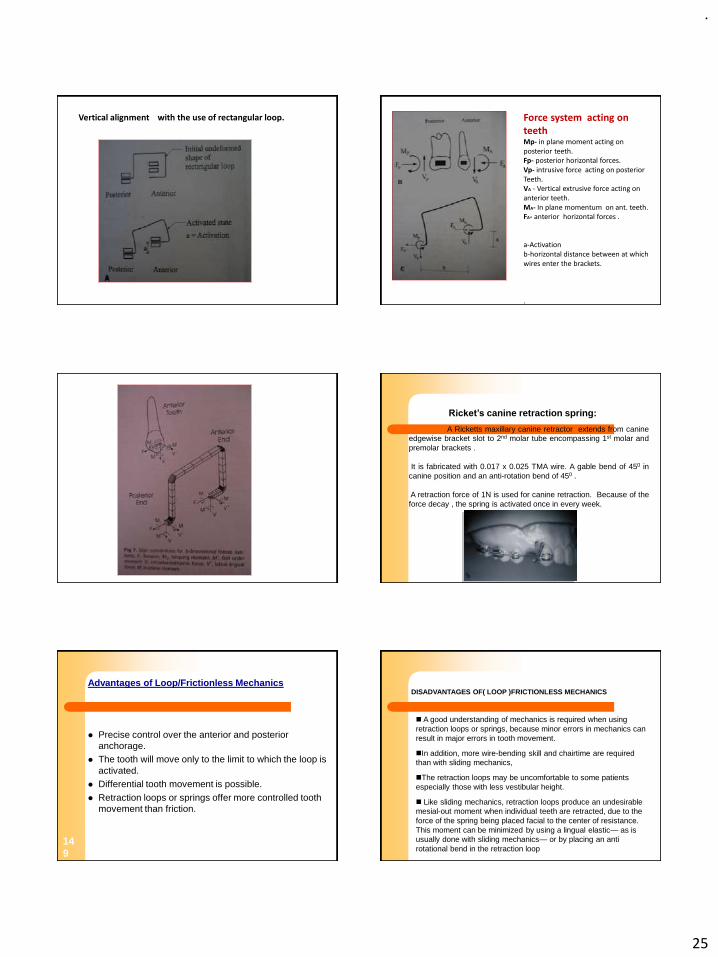
.
25
Vertical alignment with the use of rectangular loop. Force system acting on teethMp- in plane moment acting on posterior teeth.Fp- posterior horizontal forces.Vp- intrusive force acting on posteriorTeeth.VA - Vertical extrusive force acting on anterior teeth.MA- In plane momentum on ant. teeth.FA- anterior horizontal forces .
a-Activationb-horizontal distance between at which wires enter the brackets.
.
A Ricketts maxillary canine retractor extends from canine
edgewise bracket slot to 2nd molar tube encompassing 1st molar and
premolar brackets .
It is fabricated with 0.017 x 0.025 TMA wire. A gable bend of 450 in
canine position and an anti-rotation bend of 450 .
A retraction force of 1N is used for canine retraction. Because of the
force decay , the spring is activated once in every week.
Ricket’s canine retraction spring:
Advantages of Loop/Frictionless Mechanics
⚫ Precise control over the anterior and posterior
anchorage.
⚫ The tooth will move only to the limit to which the loop is
activated.
⚫ Differential tooth movement is possible.
⚫ Retraction loops or springs offer more controlled tooth
movement than friction.
14
9
◼ A good understanding of mechanics is required when using
retraction loops or springs, because minor errors in mechanics can
result in major errors in tooth movement.
◼In addition, more wire-bending skill and chairtime are required
than with sliding mechanics,
◼The retraction loops may be uncomfortable to some patients
especially those with less vestibular height.
◼ Like sliding mechanics, retraction loops produce an undesirable
mesial-out moment when individual teeth are retracted, due to the
force of the spring being placed facial to the center of resistance.
This moment can be minimized by using a lingual elastic— as is
usually done with sliding mechanics— or by placing an anti
rotational bend in the retraction loop
DISADVANTAGES OF( LOOP )FRICTIONLESS MECHANICS

.
26
151
References:• Biomechanics in orthodontics; Michael R. Marcotte.
• Biomechanics in Clinical Orthodontics; Ravindra Nanda.
• Modern Edgewise Mechanics and The segmented Arch Technique. Dr.Charles J. Burstone.
• Clinical Considerations in the Use of Retraction Mechanics. JCO 1991.
• The Rationale of the Segmented Arch. AMJ 1962; 48(11):805-821.
• Common sense mechanics: Part 2. Thomas F. Mulligan. JCO 1979.
• Optimizing anterior and canine retraction. Charles J. Burstone. AJO 1976.
• The K-Loop Molar Distalizing Appliance Valrun Kalra. JCO 1995.
• Simultaneous Intrusion and Retraction of the Anterior Teeth Varun Kalra.JCO 1998.
• Controlled Space Closure with a Statically Determinate Retraction System;Kwangchul Choy, Charles J. Burstone, AO 2002.
152
• A comparison between friction and frictionless mechanics with a newtypodont simulation system. AJODO. 2001;119(3):292-9.
• Biomechanical design and clinical evaluation of a new canine-retractionspring. Gjessing P. AJO 1985;87(5):353-62.
• T-loop position and anchorage control. Kuhlberg AJ, Burstone CJ. AJODO1997; 112(1):12-8.
• Continuous arch wire closing loop design, optimization, and verification.Part I. AJODO 1997; 112(4): 393-402.

.
1
1 2
Role of Nutrition in
orthodontics
Presented by: Dr. Naveen Sharma
3
Contents
• Introduction
• Definitions
• Classification of food
• Proteins. Carbohydrates. Lipids. Vitamins.
• Minerals
• Nutrition and dento facial growth
• Nutritional influence on the periodontium
• Guidelines for evaluation & assessment of nutritional status
• Balanced diet
• Conclusion
• Bibliography
4
Introduction
• Nowadays we live in a very diet conscious
society where more and more people are
adopting a healthy lifestyle through a healthy
diet.
• Evidence for which can be obtained from
knowing the fact that books written on nutrition
and diet are amongst the fastest moving books
off the shelves
5
Definition
• “The science of food, the nutrients and other
substances therein ,their action ,interaction and
balance in relation to health and diseases and the
processes by which the organism ingest, digest, absorbs,
transports ,utilizes and excretes food substances”
- Council of food and nutrition of the
American Medical Association
6
Historical Background
Schneider’s –
• Naturalistic era-(400 B.C-A.D 1750)
• Chemical analytic era(1750-1900)
• Biological era(1900-present)

.
2
7
Historical Background
• Molecular\ cellular era-(1955 –present)
• Guilford -1874 was among the first to advocate
that dietary deficiencies could be an underlying
cause of dentofacial irregularities
8
Definition
• Science of nourishing the body properly or analysis of the effects of food on living organisms.
• Relationship between man and his food and implies the psychological and social as well as the physiological and biochemical aspect
-Yudkin
9
Definitions
• Nutrition is a dynamic process in which the
food that is consumed is utilized for
nourishing the body.
• Diet : The term diet refers to the total oral
intake of substances that furnish nourishment
and/or calories to the body.
10
BASIC FUNCTION OF NUTRIENTS
• Supply energy .
• To promote growth.
• Repair of the body tissues .
• Regulate body processes.
11
Classification of nutrients
• Macronutrients; these are contribute the
main bulk of food.
Eg; proteins. fats and carbohydrates.
• Micronutrients; they are vitamins and
minerals and required in small amounts from
a fraction of a milligram to several grams.
12
Classification of food
✓CLASSIFICATION BY ORIGIN
✓CLASSIFICATION BY CHEMICAL COMPOSITION
✓CLASSIFICATION BY PREDOMINANT FUNCTION
✓CLASSIFICATION BY NUTRITIVE VALUE
.
3
13
Classification of foods
Classification by origin:
Food of animal origin;
Food of vegetable origin;
Classification by chemical composition
proteins
Fats
Carbohydrates
Vitamins
minerals
14
Classification by predominant
function
• Body building food eg; meat. poultry. fish.
eggs. pulses. groundnuts. etc.
• Energy giving food eg; cereals. sugurs.
roots. tubers. fat and oils.
• Protective foods eg; vegitables. fruits and
milk.
15
Classification by nutritive value
• Cereals
• Pulses (legumes)
• Vegetables
• Nuts and oilseeds
• Fruits
• Animal foods
• Fats and oils
• Sugars and jaggery
• Condiments and spices etc.
16
Carbohydrates
• Energy yielding nutrients, is the largest single
component ,aside from water ,of most diets.
• Composed of –
-carbon
-hydrogen
-oxygen
17
Carbohydrates
• Sources-
- rice - sweet potato
-wheat - honey
-bajra - jaggery
-pulses
-vegetables
• Recommended daily intake-440gms. 18
Carbohydrates
Classified as-
• Monosaccharides – eg; glucose ,fructose
,galactose.
• Disaccharides - eg; sucrose , lactose ,maltose
• Polysaccharides- eg; starch, glycogen
,cellulose
• Oligosacchrides-eg; maltotriose

.
4
19
Digestion of carbohydrates
• In mouth by salivary amylase polysaccharides are
converted into disaccharides,
• In stomach by acid further degradation of
molecule takes place,
• In small intestine by pancreatic amylase
completes the breakdown to monosaccharide,
• These monosaccharide then pass through the
small intestinal villi into bloodstream,
20
Carbohydrates
• SUCROSE GLUCOSE + FRUCTOSE
• MALTOSE GLUCOSE + GLUCOSE
• LACTOSE GLUCOSE + GALACTOSE
21
Carbohydrates
• Absorption and storage –
small intestines
stored as glycogen in liver and muscle
• Function –
main source of energy.
1 gm – 4 kcal of energy
22
Summary
• Glycogenesis- surplus glucose converted to
glycogen and stored in liver.
• Glycogenolysis-breakdown of glycogen in
liver to glucose.
• . Glycolysis-in muscle berakdown of glycogen
to pyruvic acid
• Gluconeogenesis or glyconeogenesis-glouse
and glycogen can be synthesised by the liver
from substances which are derived from non
carbhohydrates sources eg;aminoacid,seen
during prolonged starvation.
23
Carbohydrates
• Almost nothing is known of the effect of
carbohydrate deficient diet on the oral cavity.
• Deficiency dosage – less than 440gms per day
leads to underweight,weight
loss,lethargy,anaemia.
24
Carbohydrates
• There is a group of disease which represents a
primary genetically determined disturbance of
the mucopolysaccharide metabolism
.
5
25
Carbohydrates
• Hurler syndrome-
• Clinical features are.
• Head -appears large with prominent
forehead
-puffy eyelids
-nasal congestion with noisy breathing
-shortening and broadening of the mandible
26
Carbohydrates
- wide intergonial distance
- increased arch length from ramus to ramus
• dentition-small and misshaped teeth.
• Soft tissue –gingival hyperplasia.
27
Lipids
• These are the most concentrated energy yielding
group of nutrients.
• Basic structure –molecules of glycerol to which
one to three fatty acid molecules
28
Lipids
• Sources –
-fruits -egg yolk
-vegetables -butter
- milk - ghee
-meat -cereals
-fish
29
Lipids
• Classified as
- saturated
-unsaturated
• Physical properties –
insoluble in water.
less dense than water.
not affected by temperature.
30
Lipids
• Digestion-
stomach- with the help of lingual lipase secreted by the oral salivary gland and gastric lipase secreted from the stomach.
small intestine-emulsified by bile and further broken down by pancreatic lipase then absorbed through the small intestinal villi.
long chain fatty acids are converted into a chylomicron and dumped into the lymph system,which carries the chylomicron to the bloodstream
.
6
31
Lipids
• 30%-free fatty acid combine with bile salts
• 70%-resynthesised immediately to form triglycerides
• Normally the fats stored in adipose tissue.
32
Lipids
Function –
• Source of energy -1gm-9kcal.
• It insulate the body and protect various internal
organs.
• Carrier of the fat soluble vitamins.A,D,E and K
• Source of other essential fatty acids.
33
Lipids
• Disturbances in the lipid metabolism are
not very common but they do occur
-Gauchers disease
-Neimann Pick disease
34
Gauchers disease• Gauchers disease is an autosomal recessive defect
of lipid metabolism.
• Clinical feature
– Hepatosplenomegaly
– Osteolytic disease ensues along with pulmonary
disfuction
– Bone marrow shows diffuse changes numerous
large,fomey,slightly granular cells with small,round
pyknotic nuclei
• Treatment and prognosis;the disease resulting in
death usualy with in first year.
35
Niemann-Pick Disease
• AUTOSOMAL RECESSIVE TRAIT: characterized by
abnormal storage of phospholipids. resulting
from inherited deficiency of sphingomyelinase.
• Treatment and prognosis: symptomatic and
consists mainly of antibiotic for pulmonary
infection. Even organ transplantation also
recommended.
36
Proteins
• The term proteins mean –”to take first place”-
Mulder -1983
• Half the dry weight and 20% of the total weight
of an adult is protein.

.
7
37
Proteins
• Basic structure –
complex substances made up of many amino
acids.
there are 20 different naturally occurring amino
acid that have been identified as the building
blocks for body protein.
38
Proteins
Sources-
-wheat - peanut butter
-milk - peas
-egg white -cottage cheese
-legume -rice
-boiled ham -oatmeal
39
Proteins
• Classified according to functional point of
view
-amino acids -essential amino acids
-non essential amino acid
Classified according to quality of protein
– complete
- incomplete
-complementary
-supplementary 40
Proteins
• Digestion and absorption
-attached to another substance or surrounded by
fat or carbohydrate
Stomach – gastric proteases (pepsin)
Small Intestine – pancreatic enzymes
41
Proteins
• 30 %-absorbed directly
• 70%- chain of two or three AA
dipeptidases amino acids
• Amino acids – enters blood stream
42
Proteins
Functions –
• Essential for growth-hair,skin,nail
• Formation of essential body compounds
• Regulation of the water balance
• Act as buffers
• Protective role
• Transport of nutrients.

.
8
43
Proteins
• The inadequate consumption of protein and
energy as a result of primary dietary deficiency
conditioned deficiency may cause loss of body
mass and adipose tissue ,resulting in protein
energy malnutrition-
• Kwashiorkor
• Marasmus
44
Proteins
• Kwashiorkor –
Definition- protein deficiency with sufficient calorie intake.
Age-6 months and 3yrs -
Clinical Features -growth failure
wasting of muscles
- edema
-enlarged fatty liver
-serum protein low
- flag sign
45
Proteins
• Marasmus
• Definition –starvation in infants with a overall lack
of calorie.
• Age-infants under 1 yr of age
• Feature-wasting of all tissues
-no edema
-no hepatic enlargement
-monkey like face
46
Vitamins
• Defined as organic substances not made by the
body ,which is soluble in either fat or water and
ordinarily is needed in only minute quantities to
act in a variety of metabolic reactions.
47
VITAMINS
FAT SOLUBLE WATER SOLUBLE
48
Vitamins
Fat soluble Water soluble
• Intake is in excess Minimal storage of
of daily body needs dietary excess
• Not excreted Excreted in urine
• Deficiency symptoms Develop rapidly
slow to develop
• Not absolutely necessary Must be supplied in diet

.
9
49
Vitamins
Metabolism of vitamins
• They are released from food during the digestive process but are not digested,
• Water soluble vitamins are absorbed through the small intestine, excess is excreated by the kidney in the urine,
• Fat soluble vitamins are absorbed through the small intestine they are sent to the liver and fat depots and circulate through the blood.
50
Vitamins
• Vitamin A
• Acidic ,alcoholic, aldehyde form.
• Sources –spinach
- carrot, broccoli
-peas ,cabbage
- milk ,cheese
-butter, meat ,fish
-egg, beef
51
Vitamins
• Functions-
-Vision –role in dark adaptation and
vision in dim light
-Helps in bone remodeling.
DRI—approximately 800 mcg/day.
52
Vitamins
• Deficiency-night blindness
-keratinzation of cornea
-bitots spots
- xerosis conjunctiva
- xeropthalmia
- complete blindness
-loss of sense of taste
53
DEFICIENCY
Blindness from xerophthalmia
54
XERODERMA
FOLLICULAR KERATOSIS
.
10
55
ORAL MANIFESTATIONS
56
Vitamins
• Excess Vit A leads to ;
• Headache
• Vomiting
• Double vision
• Hair loss
• Bone abnormalities
• Liver damage
57
Vitamins
• Dentition-disturbances in differentiation and
growth of developing teeth
-calcification of teeth
-retardation of eruption
- disturbances in periodontal tissues.
-failure to form tooth enamel.
-xerostomia.
58
Vitamins
Vitamin D
Group of compounds called as cholicalceferol.
- Source –
- Endogenous synthesis-sunlight
- Exogenous synthesis-deep sea fish ,fish oil,
butter, milk.
59
Vitamins
• Function-
• Maintain normal plasma level of calcium and
phosphorus.
• It is necessary for all animals with a bony
skeleton ,since it facilitates absorption and
utilization calcium and phosphorus for bone
formation
60
Vitamins
DEFICIENCY OF VIT D
1.Rickets in growing child
Clinical features are,
-harrisons sulcus
-Rickets rosary
-pigeon chest
-Bow legs
-Knock knees

.
11
61
Deficiency of Vitamin D.
• Reduction in blood calcium and phosphorus, delayed closure of fontanels.
Disproportionate growth occurs between face and skull. It may cause interference with bone growth.
• It causes retarded eruption of teeth early loss of decidious teeth due to caries.
• Jaw bones become thick.
• Teeth are ir-regularly arranged
62
• Maxilla become narrow and palate becomes high.
• Mandible becomes short.
• Infants with low vitamin D intakes showed delayed
eruption of teeth.
• Increased susceptibility of osseous tissue to muscular
traction as undesirable oral habits.
• Open bite, transverse hypodimensions and misshapen
palate are frequently observed in vitamin D deficiency.
63
Vitamins
2.Osteomalacia –in adults
-osteoid matrix which is laid down fails to
mineralize
Clinical future ;
-vague bony pain
-muscular weakness
-frequent fractures
64
Vitamins
• Excess of Vit D leads to ;
• Nausea,vomiting,and headache.
• Irreversible damage to kidney and cardiovascular
tissue.
• DRI-- approximately 5 to10 mcg/day.
65
Vitamins
• Vitamin E-
• Acts as an antioxidant and protects red blood
cell.
• Sources –vegetable oils, yellow
cornmeal, wheat
bread, egg ,butter .
• Role in human nutrition is poorly
understood.
66
Vitamins
Deficiency of vit E leads to ;
Heamolytic anemia
Excess intake of vit E leads to ;
Nausea
Diarrhea
Cramps and bleeding
Interfereance with anticoagulant drug
DRI—15 mg/day.

.
12
67
Vitamins
Vitamin K
• Basic structures consist of a group called as
quinones
• Sources-green vegetables
-fruits
• Function-it is necessary for the synthesis of
prothrombin.
68
Vitamins• Deficiency of vit K results ;
• Prolonged bleeding
• Increased clotting time
• Oral manifestations are,
• Increased gingival bleeding,
• Prothrombin level <35%--bleeding after tooth brushing,
• Prothrombin level <20%--spontaneous gingival hemorrhage,
• Exess intake of vit K ;
• Interfere with anticoagulants, which could results in hemorrhaging
• DRI—approximately 100 mcg/day
69
Vitamins
Vitamin C (Ascorbic Acid)
• Sources-citrus fruits –orange ,lemon ,grape ,certain vegetables.
• Vit C is Essential for;
• -formation of intracellular substance .
-formation of fibrus tissue matrices of bone.
-formation of tendon and cartilage.
-utilization of iron and calcium .
DRI—approximately 60 mg/day.
70
VITAMIN C
71
Vitamin C deficiency leads to;
In severe deficiency, the gums may become
retracted formation of periodontal pockets.
Loosening of teeth and loss of teeth.
• Vitamin C deficiency produces sub-clinical
scurvy which is related with damage in
development and eruption of the teeth and
formation of hypodimensional osseous bases.
• Exess leads to; Gi upset,diarrhea,and iron
toxicity.
72
Vitamins

.
13
73
Vitamins
74
Vitamins
• B complex-these consist of a group of essential
compounds which are biochemically unrelated
but occur together in some foods
• Sources-green leafy vegetables, cereals ,yeast
,liver, and milk.
75
Vitamin B complexThaimine(B1)
• Source; best source is pork, meat, poultry and egg.
• Function-carbohydrate metabolism.
• Deficiency- BERI BERI
• Dry beri beri-neuromuscular symptoms weakness,
paresthesia, sensory loss, polyneuritis.
• Wet beri beri-CV involvement
• DRI—approximately 1.1mg.
76
Vitamin B complex
Riboflavin(B2)
• Function-cellular respiration
DRI—depends on total calorie intake,energy needs,body size and growth rate. Around 1.1mg.
77
Vitamin B complex
• Vitamin B2 deficiency produces retardation of growth of dentofacial structures.
• A prenatal matarnal riboflavin (B2) deficiency produces anomalies of jaw and teeth; which shows shortness of mandible, and maxilla, cleft palate, severe anomalies of incisor teeth, dentofacial malformations resembled angler’s cl II malocclusion
• -ocular lesions
-cheilosis ,angular stomatitis
-glossitis.
-dermatitis. 78
Vitamins
• Niacin:B-3
• Function-metabolism of fat
• Deficiency-pellagra-dermatitis.
-diarrhoea.
-dementia.
• Exess- facial flushing.
• Liver damage.
• DRI– approxmately 14mg.

.
14
79
Vitamins
• Pyridoxine(B6)
• Function-exact function not known
-fat and protein metabolism
-transmission of neural impulse
• Source-any thing of animal origin
• Deficiency-dermatitis
-glossitis
-angular stomatitis80
Vitamin
• Excess intake of vit B6 –permanent
neurologic damage.
That includes numbness in extremities and
uncoordinated muscle movement.
• DRI—around 1.4mg/day.
81
Vitamins• Vit B-9 (folic acid)
• Function-helps in amino acid synthesis.
• Source-dark green leafy vegetables
• Deficiency-causes fetal neural tube defect and
macrocytic anemia
• DRI—approximately 400mcg/day
82
Vitamin
• Vit B-12 (cobalamine)
• Function-- converts folate into the form in which it can be used to produce red blood cell and nucleic acids for DNA synthesis.
• Deficiency—may cause pernicious anemia.
• DRI—approximately 2.4mcg/day.
83
Summary of deficiency states of vitamins
VITAMINS DEFICIENCY
A XEROPTHALMIA, DRY EYE.
B-1 BERIBERI
B-2 ARIBOFLAVINOSIS
B-3 PELLAGRA
B-6 MICROCYTIC ANEMIA
B-9 NEURAL TUBE DEFECT OF FETUS.
B-12 PERNICIOUS AND MEGALOBLASTIC
ANEMIA.
C SCURVY .
D RICKETS AND OSTEOMALACIA
E HEAMOLYTIC ANEMIA
K HEAMORRAGE –FAILURE TO BLOOD CLOT.
84
Oral deficency symptoms
Vit A-- xerostomia
oral leukoplakia
hyperkerotosis
softeing of skull bone due to <Ca deposition
Vit B-- red swollen lips
burning,smooth,red tongue
ulcerated burning gingiva
Vit C-- bleeding,swollen gums.loose teeth
slow healing.

.
15
85
Oral deficiency symptoms
• Vit D—failure of bone wounds to heal
• enamel hypocalcification
• loss of alveolar bone
• thinning of trabeculation
• Vit E—no known deficiency symptoms
• Vit K-failure of wounds to stop bleeding
86
Minerals
• Macro minerals which are present in relatively high
amount in body -calcium
-phosphorus
-potassium
-sodium
• Micro minerals those which are <0.005% of the body
weight -iron
• -copper
• -manganese
87
MineralsCalcium
• Inert inorganic element which is associated with bone and tooth formation.
• DRI—360mg for infants and 800mg children and adults
• Total calcium in the body is 100-170g
• 99% of which found in hard tissue.
• The level of the blood calcium controlled by parathyroid gland
• Sources-milk and milk products
green leafy vegetables
legumes
citrus fruits
88
Minerals
• Function –
1. Bone formation.
2. Tooth formation.
3. Essential for growth
4. Necessary for blood coagulation
5. Activation of several enzymes and release of certain
hormones
6. Role in the process of impulse transmission at
neuromuscular junction.
89
Factors which influence plasma
Calcium level
• Parathyroid hormone: Increase plasma Ca+ levels and
at the same time <the plasma phosphate level,
• high level of bone matrix stimulates the activity of
osteoclasts this causes demineralization of the matrix.
Ca+ and phosphate are removed
• Regulation of PTH secretion :decrease in Ca+ level
in plasma stimulates PTH secretion and increase in
ionic Ca+ level in plasma inhibits PTH secretion
90
Factors which influence plasma
Calcium level
• Calcitonin :hormone secreted by parafollicular cells of thyroid gland, incerase in Ca+ level stimulate release of calcitonin which in turn decreases the Ca+ in plasma.
• Plasma protein: decrease in these protein will be accompanied by decrease in total Ca+ level.
• Phosphate: Ca+ and PO4+ ions in plasma have reciprocal relationship, increase in serum PO4+ causes a fall in Ca+ ions.

.
16
91
Minerals
Abnormalities of Ca Metabolism –
• Osteoporosis-middle aged women
decreased density of bone
shortening stature
bone fractures
• Osteomalacia –decrease in the mineral content
lack of Vit D.
92
Minerals
93
Minerals
Phosphorus
• 1% of the total body weight.
• Major constituents of bone and teeth
• Regulates the release of energy in the form
of ATP.
94
Clinical Implications
95
Nutrition deficiencies –and
dentofacial growthNutrition and Skeletal Maturation
• Studies have shown
• “prolonged nutritive failure in growing child result in retardation of bone growth centers in the hand and wrist radiographs”.
• Calcium, Vit D and phosphorus are essential for the formation of bone and teeth.
96
Nutrition deficiencies –and
dentofacial growth
• Malformations and prenatal deficiencies-
Dietary intake of the expectant mother is directly
related to the condition of the infant at birth.
• Warkany –showed riboflavin-cleft palate,
shortening of mandible

.
17
97
Nutrition deficiencies –and
dentofacial growth• Evans ,nelson-showed acute folic acid deficiency-cleft palate.
• During hyperplastic phase Nutritional deficiencies leads permanent damage to the tissue
• During hypertrophyic phase bcz of Nutritional deficiencies growth may stop temporarily
Effect of Nutrition on teeth-
Local effect : chemical or physical action on the external surface of the tooth
Systemic effect :important during the tooth development.
Important during matrix formation and calcification
Influenced by maternal, infant and childhood diet.
98
Nutrition deficiencies –and
dentofacial growth
• Role of fluorides-
• Anticariogenic factor.
• Long continued exposure to excessive amounts
may result –dental fluorosis
-skeletal fluorosis
99
Nutrition deficiencies –and
dentofacial growth
• Increased density of various bones .
• Increased calcification of ligaments, tendons and
vague pain in small joints of the hands and feet
• In the most severest form –stiffening of the
spine virtually making the patient immobile.
100
Nutrition deficiencies –and
dentofacial growth
• Nutrition and malocclusion-
• results from various nutrient deficiencies-
abnormal bone growth
-loss of teeth.
-severe caries.
-periodontal breakdown.
101
Nutrition deficiencies –and
dentofacial growth• Vitamins in relation to growth and dentition-
• VitA-disturbances in differentiation and positional growth of the developing teeth.
defective calcification.
Retardation of eruption.
disturbances of periodontal tissues.
102
Nutrition deficiencies –and
dentofacial growth• Vit B-
-loss of apatite
-disturbed digestion.
-Retardation of growth
• Vit C
-disturbed calcification of teeth.
-retarded eruption.
-thickened jawbones.
-narrow maxilla.
-short mandible.
-High vault palate.

.
18
103
Role of nutrition on the
periodontium
• Physical nature of the food-
-soft food vs. fibrous food.
Vitamin deficiency
Vit A leads to keratinizing metaplasia of the epithelium, > susceptability to infection and disturbances in bone growth.
Vit B deficiency leads to gingivitis, glossitis and glossodynia,
angular chelitis and inflamation of oral mucosa
Vit C leads to scurvy
- interferes with bone formation and remodeling of the periodontal bone
• Vit D leads to osteoporosis of alveolar bone and cemental resorption.
104
Role of Nutrition in Root Resorption
• Common iatrogenic problem associated with
orthodontic treatment
• Marshall et.al-greater degree of
resorption in deficient diets.
• Beck –calcium deficiency were more susceptible.
105
Effects of consistency of food
• Throughout its various stages of growth mouth is
affected by complex system of forces generated by
masticatory and respiratory activities.
• Diet that does not supply food of a sufficient hard
consistency does not supply adequate stimulus for
proper mastication resulting in a narrow maxillary arch .
• Similar observations have been made in humans –arch
collapse syndrome.
106
Effects of consistency of food
1. Low level of eruption –posteriors
2. Maxillary arch are narrower.
3. Mandible are shorter and condyles are thinner.
4. Less tonicity of temporalis and masseter.
5. Reduced linear dimension of skull.
107
Effects of consistency of food
• In humans-
• Some authors have proposed-weakening
of the temporomandibular articulation
• Resulting in malocclusion.
108
Nutritional consideration in
orthodontic tooth movement
• Tooth movement involves biologic responses to
orthodontic forces,
• Which may influenced by ascorbic acid.
• Lack of Vit C interferes with collagen synthesis
thus affecting both periodontal ligament and the
formation of osteoid.
• Also affects the stability of orthodontic
correction (ie)it affects retention.

.
19
109
Nutritional considerations in surgical
patient
• The mouth is the portal for entry of food into
the body thus maxillofacial surgery of these
structures may result in impaired food intake
both prior to and after surgery.
• We must ensure adequate nutritional support in
such patient.
• Patient require both an energy source and a
protein source.
110
Nutritional considerations in surgical
patient
• Nutritional considerations in surgical patient Carbohydrates energy source for vital organs like brain.
• Protein is also important for imparting strength to the fracture repair. If it is absent then the wound healing is delayed.
• Vitamin A helps in epithelialization,collagen synthesis and cross linking & fibroblast differentiation,
111
Nutritional considerations in surgical
patient
• Vit D and calcium helps in healing of hard
tissues.
• Vit E acts as an antioxidant and thus reduces the
damage from the free oxygen radical.
• Vit K helps in activation of various clotting
factors and thus essential for blood clot
formation during healing.
112
What is balanced diet??
What does it contain
113
“A balanced diet refers to intake of
appropriate types and adequate
amounts of foods and drinks to supply
nutrition and energy for the
maintainence of
bodycells,tissues,organs and to
support normal growth and function”.
114
Conclusion
• The proper nutritional status of the patient is of utmost
importance in orthodontic treatment, since success
depends on the response of bone to stimulation for the
accomplishment of desired result.
• Only when we begin to understand these vital nutrients
and the role played by each one in the normal
development of orofacial region and the body as a
whole can we realize its relevance in clinical application.
This will facilitate a comprehensive approach to
orthodontic treatment as a whole.

.
20
115
Bibliography• Contemporary orthodontics-Proffit
• Current Principles and Techniques –Graber Vanarsdall
• Nutrition and oral health-Pollack
• Introductory nutrition-Helen Andrews
• Principles of nutrition-Wilson,Fisher
• Clinical dietetics and nutrition-F.P.Antia
• Basic pathology-Robbins
• Pathology for dental students-Harsh Mohan
• DCNA :25 (1) 1981
• Cheraskin,E., and Riungsdorf, W.M,: Biology of the orthodontic patient . 1; plasma ascorbic acid levels. Angle Orthod., 39:325,1969.
• Litton, S.F., Orthodontic tooth movement during an ascorbic acid deficiency. Am. J. orthod., 65:290,1974
• Jones, N B.: dietary needs of the oral surgery patient with comparision of dietary supplements. J Oral Surg., 28:892, 1970
• McCanlies, J M., Alexander. C.M., robdent., J. H., et al.: effect of vitamin C on the mobility and stability of guinea pig incisors under the influence of orthodontic force. Angle Orthod., 31:257:1961

.
1
ORAL HABITS
Presented by: Dr. Lavesh Pandey
CONTENTS
-Introduction-Definitions-Muscle Physiology of Stomatognathic system-Development of Habit-Classifications of Habits-Various factors to be considered before approaching towards anyparticular habit-Habit as a cause of malocclusion-Various Factors which determine the outcome of habit practice-Various deleterious oral Habits
a. Thumb/ digit suckingb. Tongue thrust/infantile swallow habitc. Mouth breathingd. Bruxisme. Lip habitsf. Finger nail biting habitsg. Self-injurious habits/masochistic habits
Although oral habits are being dealt by dentist especially byPedodontist and orthodontist Since long time, but till Todaythis Particular abnormal/normal entity is not fully known.Time-to-Time various hypothesis & explanations have beengiven by various authors but none of it specifically delineatethe habitsThose which are normal for a particular age group and others,which are deleterious to stomatognathic system. The mainreason for this difficulty is that a habit may be a part of normaldevelopment, a symptom associated with deep-rootedPsychological disturbance or a habit may be a result ofabnormal facial growth.
Though this is difficult to delineate it, but at the same time it isimportant to have differentiation of abnormal from normalbecause If normal development get disturbed unknowinglyand at the same time If abnormal growth or undererlyingpsychological cause let continue without interfering at propertime/age it will lead to long lasting effect on stomatognathicsystem its growth & development and psychologicaldevelopment of child.
Habit ?
When Considering habit as such, it should be kept in mind
that whether these performances are just habits or necessity
of an individual to perform e.g. mouth breathing can be
considered as a habit only if there is no underlying cause
e.g. nasal blockage which make it necessary for a individual
to breath through mouth.
Another important characteristic associated with all
habits is that these performances are learned pattern of
abnormal muscle function; in other words, habits are
nothing but altered muscular function/force balance.
This important association necessitate the
understanding of normal physiologic function of
stomatognathic system which will be dealt later.
DEFINITIONS
Dorland (1957) – Dorland defined habit in general “as a fixed or
constant practice established by frequent repetition.”
Buttesworth(1961)- defined habit as a frequent or constant
practice or acquired tendency which has been fixed by frequent
repetition
Both these general definition of any habit highlight one
common fact that it takes time for habit to get established by
frequent repetitions. this time duration and frequent repetitions
ultimately establish habit at unconscious/ subunconsious level
which is the ultimate depth of psychological association with
habits. These general definitions of habit hold true for oral habits
also.
Mathewson (1982) particularly highlighted the muscular
involvement In oral habit. According to him, oral habit can be
defined as learned pattern of muscular contractions.
Development of habit
Development of habit should not be confused with one normal
developmental Phenomenon Instinct. Newborn infant develops
some Instincts composed of elementary reflexes. An instinct is
one where the pattern and order are inherited while in habit,
pattern and order are acquired. If these acquired pattern and
order are repeated over a long Period of time, it becomes habit.
At beginning infant/child makes an effort by frequent learning and
practice, later on muscles start responding rapidly. It has been
established by psychologist through various studies that
unconscious mental pattern of child develops from five sources
named instinct, Insufficient or incorrect outlet to energy, pain or
discomfort, abnormal physical size of parts, imitation of or
imposition of others.
.
2
Muscle physiology of stomatognathic system
Before going into details of oral habits , it is important
to know the basic muscle physiology of this complex and
integrated system. It is necessary and important because as already
mentioned all habit express their deleterious effects through
muscles functions, Interestingly which is under the control of an
individual, but not easy for an individual to directly change this set
pattern within a short period of time because all these events are
associated at unconscious level. These muscle forces, which at a
time went wrong and produced untoward effects will be managed
and channelized properly to bring back the stomatognathic system
to normal healthy and efficient level from where it was taken away.
Basic muscle characteristics
There are various Physiologic characteristics of muscle which
explain their role as a guard to direct various Growth processes to right
direction
Among all them, the following properties are important in relation to
our field
Muscle elasticity – muscle in its non active form i.e. not undergoing
contraction is no way exception to rule of elasticity and this property
express itself as a rubber band effect which is evident within structural
limitation and individual characteristic of muscle.
Contractility- quality of contractility i.e. ability of tissue to decrease
its longitudinal dimension is unique characteristic of muscle.
Muscle tone- skeletal muscle always maintain a level of partial
contraction i.e. no muscle is in a full relaxation state. This special
property is important in maintenance of precise counter balancing force
in orofacial region which is ultimately responsible for stability of
whatever an orthodontists particularly; and any other specialty which
plays with stomatognathic system; achieve by its best efforts.
Myostatic or stretch reflex - This is caused by pull on muscle’s
attachment to its supporting tissue e.g. when a dentists pulls patients
lips, he encounters increasing resistance of lip muscle and associated
altered movement of tongue. This property comes in play when
functional examination of tongue is done.
These properties are not the only properties of muscles. There are
various other unique properties e.g. All or none law, resting length
law etc. But these mentioned four properties will be helpful in
understanding of two important muscular mechanism which keep
equilibrium among various forces.
Buccinator mechanism
This mechanism explain one interesting finding that if bones
always yield to pressure / forces and muscles are always in a
definite amount of contraction by virtue of muscle tone, than why
bone of orofacial region doesn’t yield to these muscular forces.This
fact can be explained by counter-balancing forces of Buccinator
mechanism
Two parts of this counter balancing system are forces from outside
the dentition/outside alveolar process and those from inside the oral
cavity.
Dentition is literally wrapped around externally from forces of
orbicularis oris muscle, fibers of this muscle intermingles postero-
laterally with buccinators muscle, which in turn joins internally at
pterygomandibular raphe with fibers of superior constrictor of
pharynx which ultimately joins mid- cranial base prominence named
Pharyngeal tubercle.
These forces are counter balanced by forces of large muscular
organ tongue. Rest mild balancing forces which precisely balance
this system are those from periodontal ligaments through a
phenomenon called active stabilisation.
Triangular force concept
This muscular force balance comes into picture
especially in case of swallowing. This hypothesis explains that it is
wrong to blame tongue thrust as a cause for anterior open bite
malocclusion. It discards the term tongue thrust because tongue
doesn’t thrust forward during swallowing because during
swallowing greater extent of physical stress of orofacial
musculature is posterior and lateral direction with the minimal
amount of anterior stress.
From all this brief discussion of muscle physiology and their
integrated role and action, it looks important and vital that the
ultimate goal for correction of deleterious effects produced by
habits should be focused to achieve normal muscular function/
force balance. Though it takes time, but it is possible to convert
back musculature to their proper structure & function.
.
3
Classification of habits
-Obsessive habits (deep rooted)
- Intention habits e.g. digit sucking, nail biting
- Masochistic/self injurious habits e.g. gingival stripping habit
-Non-obsessive (easy learned and easy to drop)
-Unintentional e.g. chin propping
-Functional habits
e.g. mouth breathing
Bruxism
Tongue threshing etc
Various Authors have classified habits e.g.
James (1923) - useful habits
- harmful habits
Kingsley (1958) - Functional oral habits
- Muscular habits
- Combined
Morris and Bohana (1969)
-Pressure/non Pressure habits
-Biting habits
Klein (1971) -empty habits
-meaningful habits
Finn (1987)
-Compulsive habit
-Non-compulsive habit
-Primary habit
-Secondary habit
Though some authors have classified habits as beneficial habits
and harmful habits, but if looked in strict sense, it is not valid
classification e.g. breathing, mastication is classified in
Beneficial habit group as it was the thought that these habits
help in beneficial way in growth and development of orofacial
system. Although it is true about their beneficial contibution in
normal development, but these are not habit but are normal
physiologic function
Deleterious oral habits
These habits are sometime called pernicious oral habits. But
this is misnomer as word pernicious mean fatal which may risk life
as in medical field one common example is pernicious anemia.
Though oral habits may cause marked damage to structure and
function of stomatognathic system, but in strict sense it cannot be
considered as pernicious.
Factors to be considered while dealing with oral habits
One should not jump into instant diagnosis of any mild deviation
of normality as habit. Various factors should be considered
before making any relevant diagnosis and subsequent treatment
plan if needed.
1. Can the habit be considered normal for any particular age
group or stage of development. Thumb sucking may be
considered normal up to age of 3-4 years
2. Why the child has acquired habit.
3. What are the psychologic Implications of allowing the child to
continue the habit or forceful interruption of habit. If a habit is
being forcefully interrupted e.g. thumb sucking , child may
substitute tongue thrusting habit for thumb sucking.
4.Is that habit is harmful or potentially harmful to mouth or related
oral structure. it is important for any habit that it should be
analyzed whether it will or may lead to malocclusion and
associated problem. e.g. being a orthodontist it is imp that
tongue thrusting habit should be intervented only if it had
produced malocclusion or has potential to do so. If tongue
thrusting is related to only speech difficulties than only speech
therapy is indicated.

.
4
5. If habit is harmful, will the damage to mouth and dentition will
disappear spontaneously when habit is discontinued or the
deleterious effects will persists. It is known that if thumb sucking
habit is discontinued in its initial phase i.e. in primary dentition
there will be no untoward effect on permanent dentition. reverse of
this sequence is also true ie sometimes correction of malocclusion
will lead to elimination of habit.e.g. in case of simple tongue thrust
habit, elimination of anterior open bite will eventually eliminate
habit.
6. When is it reasonable to desire that habit be broken. This
highlights very important dimension in management of habit,
time .It is wrong for trying to eliminate each and every habit
when it is diagnosed first because as already mentioned some habit
are part of normal development of child. Thumb sucking especially
in first year of life is absolutely normal and essential physiologic
activity. Similarly infantile swallow up to the age of 1 ½ years i.e.
up to the time of eruption or deciduous molars is essentially
normal physiologic activity.
7. What appropriate means to be used to discourage habit
Other basic factors which should be consider when planing
treatment for any habit are
a) Rationale- since problem is of controlling a biologic process
hence rational for therapy should be basically physiologic and
not mechanical. Attempt should be always to alter the neuro-
muscular reflex which will aid in muscular relearning. If any
mechanical device is under consideration for any particular
case, it should have sound rationalse
b) Primacy of malocclusion-it should be determined whether
malocclusion is of primary or secondary concern. If
malocclusion is of primary nature that it has given origin to
habit, then malocclusion should be treated primarily & habit
will get corrected itself.
c) Type of pre- existing malocclusion and facial morphology.
Various habits may require different approach especially
regarding mechanotherapy, but one common approach to all
habits is the psychological counseling and developing good
rapport with the child because it is ultimately child who has to
give up habit.
Digit sucking
Digit sucking may involve either thumb or finger but most of
the times thumb is involved in this habit. In few cases where
chin is prominent eg in class III skeletal pattern it is easier for
child to place finger rather than thumb.
Digit sucking may be defined as placement of
digit(thumb/finger) into various depth into mouth.
Possible etiologic factors
As with all habits, no single factor can explain the cause for digit
sucking habit. Various theories have been proposed. But before
going to causative factors it s interesting to note that time of
initiation of digit sucking habit is related to some underlying
predisposing factor e.g. if a child starts digit sucking habit in first
few weeks of life it is typically related to feeding problem. Few
children develop digit sucking at time of eruption of primary teeth
as teething device particularity during painful eruption of primary
molars ; still later few children develop this habit to relieve
emotional and psychological stress.
.
5
All digit sucking habits should be studied further for their
psychological implications.. Habits may be related to hunger,
satisfying sucking instinct, Insecurity, or even as a desire to
attract attention. For successful habit elimination therapy,
possible underlying cause should be identified.
Theories of various causative factors in thumb sucking habit
1. Classic Freudian theory (sigmund Freud, 1905 ) according to
this theory, especially during first year of life oral cavity is the
primary sensory site which derives pleasure from sucking. Hence
it is considered normal for child to perform this habit.
2 Oral derive theory ( sears and wise 1982) according to this
theory oral derive is established by prolonged breast feeding.
Hence according to this theory digit sucking habit is not due to
frustration of weaving but is due to prolong nursing which
established very strong oral devices for sucking
3. Learning theory (Davidson 1967) this theory advocates that
non-nutritive sucking habit stems from an adaptive response. Infants
associate sucking with such pleasurable feeling as hunger and later
on these events are recalled by sucking the suitable object available
mainly digit.
4.Rooting and placing reflex theory(by Johnson and larson1993)
it combines the psychoanalytic theory of sigmund Freud and
learning theory. This theory states that all children posses an
inherent biologic derive for sucking. Rooting and placing reflex---
whenever anything is placed in mouth it initiates sucking reflex.
This reflex is common in infants of all mammals
Eventhough various theories have been put forward to explain digit-
sucking habit, no single particular cause may be labeled as causative
factor.
Grades of digit sucking
Subtelny (1973) has graded thumb sucking into 4 types
Type A:- whole digit is placed inside the mouth with pad of
thumb pressing against hard Palate and at same time maxillary
and mandibular anterior contact is present.
this type is most common type of thumb sucking habit patterns
Type B:-Thumb is placed into the oral cavity without touching
the vault of palate while at same time maxillary and mandibular
anterior contact is present.
Type C:-thumb is placed into mouth just beyond the first joint
and contacts the hard palate and only the maxillary incisors,
there is no contact with mandibular incisors.
Type D:- This is the least common type of all pattern of thumb
sucking habit. Very little portion if thumb is placed into mouth.
Factors influencing the effect of thumb/digit sucking on
dentition.
There are various factors which will modify the effect
Of habit performance on dentition.
These factors are
1 Pattern of habit performance
2 Various parameters of habit i.e. frequency, duration and
intensity.
Pattern of habit performance
The most common pattern is placement of thumb inside the oral
cavity in such a manner that thumb- print area rest against rugae
of hard palate. Index finger may curle over the bridge of nose
or rolled into first with other fingers. In this pattern, thumb is
resting against the both upper and lower incisors which lead to
proclination of upper incisors and retroclination of lower
incisors.

.
6
Various parameters of habit that dictate the severity of
malocclusion.
Intensity- It implies that how vigorously habit is performed.
Thumb/ digit may be kept Passively in mouth or may be sucked
with enthusiasm
Frequency- It denotes how often habit is practiced i.e. only for
few minutes or child is never without digit in mouth.
Duration-It indicates the total time period of habit being
practice e.g. it maybe years or only months
Deformities/Malocclusion that develop because of habit
practice will depend on interaction of all these factors.
Maxillary incisors experience labial and apical forces
whereas mandilbular incisors are pressed lingually & apically
Because digit is placed in palate area which displaces the tongue
inferiorly and Laterally between posterior teeth, it disturb the
balance of buccinators mechanism forces and shift balance to
overall increased buccued forces to maxillary dention (because of
lower tongue position)
Typical malocclusion that develops is
- Labial flaring of maxillary incisors which lead to spacing
between these teeth.
- Lingually collapsed mandibular incisors with crowding
- these factors lead to increased over jet & decreased overbite
- Less frequent but quite possible is bilateral posterior cross bite
due to collapsed maxillary denture under the influence of buccal
forces
- Deep palatal vault because of direct pressure from thumb and
also exaggerated appearance of this deep vault due to narrow
maxillary arch.
- There is no evidence that digit sucking may induce any change
in molar relationship as believed earlier that prolonged digit
sucking may precipitate class II molar Relationship.
- Melsen et al has reported that prolonged sucking may
predispose to abnormal swallowing habit.
- Apart from malocclusion in few cases , prolong sucking may
cause skeletal change. E.g mandibular postural retraction may
develop if weight of hand or arm continuously force mandible to
assume retracted position in order to comfortably performs habit.
- Open bite developed due to thumb sucking habit may predispose
to simple tongue thrust habit because this open bite has to be
sealed by tongue
- Because of altered forces balance in and around maxillary
complex, it becomes almost impossible for nasal floor to drop
vertically to its expected normal position during growth This lead
to narrow nasal floor and high palatal vault.
-Upper lip becomes hypotonic and lower lip hyperactive
since orbicularis oris muscle has to elevate lower lip
between malposed incisors during swallow. This abnormal
muscle adaptation stabilizes the deformation produced by
sucking habit, in other words it prevent spontaneous
correction of malocclusion even after stoppage of habit
Development of habit may be divided into three distinct
phases of Phase I, Phase II, Phase III
Phase I- Normal and sub clinically significant sucking
This phase extends from birth to 3 year of age. Almost all
children develop transient thumb sucking & considered
normal for this age. But it should be checked whether child
show tendency for ‘Thumb specific” type of vigorous sucking.
If so, a definite prophylactic approach should be undertaken
e.g use of specific nuk- sucker nipple.
Phase 11 – clinically significant sucking
This Phase extends from age of 3 years to 6-7 years . Presence
of sucking During this Phase should be attended more
seriously because
.
7
-It’s a indication of possible clinically significant underlying cause e.g.
most commonly anxiety and emotional disturbance.
-It is the best time to solve dental problems related to thumb sucking.
Definite programme for habit correction should be considered.
PhaseIII - Intractable sucking
This phase denotes definite and significant deleterious effects of habit.
Usually malocclusion associated with phase of habit is not self-correcting.
DIAGNOSIS
1) History-
As during dental appointment a child may seldom indulge in habits
so proper history should be taken
-Enquire the feeding pattern and parental care
-Questions regarding the frequency, intensity and duration of habit.
-Presence of other related habits e.g. tongue thrust etc should be
evaluated.
2) Clinical findings-Various clinical finding say suggest or
substantiate the presence of habit e.g.
-Clean pulp of thumb and short nail
-Dento-alveolar pattern i.e. typical flaring of maxillary
incisors and collapsed crowded lower anterior
-Excessive /vigorous thumb sucking may cause irritated and
reddened palatal rugae area
Various other clinical features (manifestations) as described
earlier may support the diagnosis of digit sucking habit.
Management
Factors to be considered
The single most important factor to be considered in
management is age of child, up to age of 3-4 years this habit is
considered normal
It’ true that if digit-sucking habit has potential to cause
malocclusion it should be treated; but there are certain type of
malocclusion which should be taken into consideration e.g.
straight profile with firm class I occlusion may withstand effects
of thumb sucking better than class II skeletal pattern.
Occasionally it is been reported that thumb sucking habit may
be beneficial in class III malocclusion and facial pattern.
Various steps in management
Control of habit –usually begin in phase I1 problem. Habit
should be discussed with child in very friendly atmospheres.
To show the importance of correcting such habits, which will
develop child’s interest and demand to correct habit; study
models and photographs of patients who had similar problems
of habit can be shown. Both pre treatment and post treatment
records should be shown. During this phase, only child is
given importance and habit is not discussed in presence of
parents. To parents it should be made clear that this habit
should not be a part of family discussion.
During this time, various reminding methods may be used to
help child. E.g.: Time –charts are very useful.
One interesting concept is developed by Dunlop called
Dunlop’s Beta-hypothesis. He believed that if any child in
asked to concentrate on the .Performance of act(i,e habit) at the
time he practice , it will slowly force the child to stop that
particular act.
Child is asked to sit in front of mirror and deliberately perform
thumbs sucking habit and observing him- self as he indulges in
habit.
Phase III
It is better to have psychologist consultation because most of
children in this phase of habit practice have underlying
psychological problems. Counseling, behavior modification etc
Procedure should be undertaken even in this phase, but it may need
appliance therapy.
Choice of appliance
Any appliance no matter how ideal it is , should never be placed in
child’s mouth or used as reminding device against the child’s will
because ultimately its child’s co-operation rather than appliance
itself which is going to make outcome successful. Ideal appliance,
which will be used for this purpose-
a) Should offer no restraint to normal muscular function and growth
b) Should not involve parents
c) Should not attach shame with its use
.
8
Removable appliances
Various removable appliances may be used e.g. palatal crib,
palatal rake , palatal / lingual arch with spurs, Hawley’s retainer
with spurs.
Lingual arch with a spurs is best in achieving breakage of
reflex activities of thumb sucking. A clear and immediate
discomfort / pain will keep on reminding neuromuscular system
reflex even without any involvement of child as when child is
sleeping.
Fixed mechanotherapy
Even though fixed appliances do not involve Child’s direct
involvement and cooperation, it should not be placed against
child’s will. The only indication of these appliances is when child
wanted to cooperate but have frequently broken or lost the
appliance. All these appliances prevent placement of thumb into
mouth with comfort..Deciduous or permanent molar are banded and
lingual arch is soldered to these bands with interlacing wires in
area of anterior hard palate.
Quad halix- frequently these patient have constricted maxillary
arch which need expansion, a quad halix is given which serves
both purposes i.e habit brekage & maxillary expansion. Anterior
two halix of this appliances prevent comfortable placements of
thumb at rugae area.
This over line approach should be gradually applied . one should
never jump directly to mechanotherapy. If this attempted without
gaining chind’s cooperation and trust; it is going to fail. Always
Child’s effort and cooperation should be praised and reinforced.
TONGUE THRUSTING
Tongue thrusting and infantile swallow habits are related
so closely to each other that it is very difficult to differentiate
and describe them individually. infantile swallow is a complex
muscular function aberration in which tongue thrusting is one
component.
Development of normal / mature swallow is unique and
advantageous muscular developmental aspect which guide the
correct movements of one particular muscular organ of body,
tongue which is being distinguished from all other muscles by
the fact that it is the only muscle which is joined to bone only at
one end, the other end( tip of tongue) is free.
Definitions of Tongue thrust
Brauer (1965) : A tongue thrust is said to be present if tongue is
observed thrusting inbetween, and teeth did not close in centric
occlusion during deglutition.
Tulley (1969) : He states tongue thrust as the forward movement
of tongue tip between the teeth to meet the lower lip during
deglutition and in phonation, so that tongue becomes interdental.
Barber (1975) : Tongue thrust is an oral habit with persistence of
an infantile swallow pattern during childhood and adolescence and
thereby produces an open bite and protrusion of anterior teeth .
Schneider (1982) : Tongue thrust is a forward placement of tongue
between the anterior teeth and against the lower lip during
swallowing.
Classification of Tongue thrust
-Etiologic classification – since tongue thrust may be associated
with many factors, it is helpful to classify tongue thrust depending
on underlying cause.
.Physiologic : It comprises tongue thrust associated with
physiologically normal infantile swallow of infancy.
.Habitual : Habitual tongue thrust is the continuation of tongue
thrust even after the correction of underlying causative
malocclusion. Eg If simple tongue thrust continue after correction
of anterior open bite.
.Functional : When tongue thrust mechanism is adaptive behaviour
developed to achieve some function eg to achieve a normal oral
seal in case of anterior open bite.
.Anatomic : Eg a person with enlarge tongue (macroglossia).

.
9
Clinical classification
James s. Brauer & Holt classified tongue thrust habit
depending on deformity it cause
Type 1 : non deforming tongue thrust
Type 2 : deforming anterior tongue thrust
Type 3 : deforming lateral tongue thrust
Type 4 : deforming anterior + lateral tongue thrust
Etiology of tongue thrust :
Fletcher has identified various factors which may lead to
tongue thrust.
I. Learned behaviour (ie a type of habit)
-Prolonged thumb sucking habit
-Prolong period of soreness of gums and teeth keeping
teeth apart during swallowing hence changing the
swallowing pattern.
-Improper bottle feeding
-During mixed dentition, tongue held in open spaces
which lead to habitual mobile activity of tongue.
-Prolonged period of tonsillar enlargement and soreness
which changes the position of tongue for patient comfort.
II Maturation
-Late maturation from infantile swallow to mature swallow.
-Tongue thrust is a part of normal childhood behavioural
pattern which gradually modifies as lingual spaces and
suspensory system changes.
-III. Mechanical restriction
-Constricted dental arches force the tongue to assume
lowered and forward position
-Macroglossia forces the tongue forward to properly
manipulate the bolus
Enlarged tonsills and adanoids
IV Neurologic disturbances
-Hyposensitivity of palate precipitate crude pattern of food
manipulation and swallowing.
-Disruption in tactile sensory control and coordination
-Motor disability and loss of precision in oral function
V Psychogenic factors
-Substitution of tongue thrust for forcibly discontinued
thumb sucking.
-Exaggerated motor function of tongue
VI Genetic factors
-Inherited variation in orofacial forms
-Inherited orbicularis oris hypertrophy resulting from
specific anatomical variation and neuromuscular interplay.
-Genetic mouth behaviour predetermined pattern .
General implication of tongue thrust habit in various forms of
malocclusion.
Though it is not yet established cause and effect relationship
between tongue thrust and malocclusion, it is seen that tongue thrust
and / or particular posture / position of tongue may be associated with
particular type of malocclusion.
Class I malocclusion: Most common type of malocclusion seen in class
I cases with tongue thrust habit is anterior open bite. Occasionally
bimaxillary protrusion is partly attributed to tongue abnormality being
large or posture forward causing forward positioning of both arches.
Class II malocclusion: Class II div 1 malocclusion is particularly
associated with abnormal orofacial musculature tongue being one of
them. Because of reduced space due to backwardly placed mandible,
tongue assume a higher posture.
Class III malocclusion: Since lower jaw is protruded, more space is
available for tongue in floor of mouth which leads to lower posture of
tongues. Unbalanced buccal forces lead to constricted maxillary arch
and deep palatal vault.
Various forms of tongue habits
Simple tongue thrust :
It is defined as tongue thrust with teeth together swallow.
It is usually associated with history of thumb / digit sucking habit
eventhough this predisposing habit no longer be practiced.
Prolonged thumb sucking habit lead to development of anterior open
bite which necessitate tongue to form anterior oral seal. So this
simple tongue thrusting habit is almost always adaptive response to
open bite malocclusion rather than being cause of it .
Malocclusion associated with simple tongue thrust is well
circumscribed anterior open bite.
.
10
Complex Tongue Thrust
Defined as tongue thrust with teeth apart swallow.
Complex tongue thrust is likely to be associated with chronic
nasorespiratory distress, tongilitis etc.
When tonsils are enlarged and inflammed, root of tongue in
its normal posture and position encroach enlarged faucial pillars
causing pain and discomfort. To avoid this discomfort, mandible
reflexly drops down separating teeth and providing room for tongue
to thrust forward during swallow for more comfort. Hence pain and
lessened space in throat precipitate new forward posture of tongue
and new swallowing reflex.
In case of chronic mouth breathing, large free way space is
present because of dropping down of mandible and protruding
tongue to provide adequate airway. Since maintenance of airway is
more demanding and vital than normal swallow, so later is
conditioned for the necessity of mouth breathing. Jaws are thrust
held apart during swallow so that tongue may remain in protracted
position.
Malocclusion associated with complete tongue thrust has two
distinguished features
.Poor occlusal fit. There is no firm intercuspation when
study models are oriented together. This finding is unique
for malocclusion associated with complex tongue thrust.
Reason for this is that since teeth are not held in centric
occlusion during swallowing, which over a prolonged period
of time lead to instability of this natural occlusal fit.
.Generalized anterior open bite
Unlike simple anterior tongue thrust, open bite produced by
complex tongue thrust is diffuse.
Occasionally there may not be a open bite with complex tongue
thrust if tongue is positioned evenly on top of all teeth during
swallow.
Abnormal tongue posture
Abnormal tongue posture is not a habit as such especially
endogenous type . But it is worth to mention it along with thrusting
habits because malocclusion associated with both of these is almost
similar ie open bite.
Abnormal tongue posture produces more obvious open bite than
tongue thrust because abnormal posture is maintained almost all the
time unlike thrust which occur only during swallow.
There are two forms of protracted abnormal tongue posture.
1. Endogenous
2. Acquired
Endogenous type abnormal posture
Usually during eruption of teeth, tongue adapt a posture confined
within dental arches. But some children because of unknown factors
keep tongue anteriorly between incisors. Though occasionally this
abnormal posture may produce marked open bite, but interestingly
most of times incisor relationship is stable inspite of abnormal posture.
Acquired abnormal tongue posture
This usually result from chronic pharyngitis, tonsillitis etc. but
may also present in cases with narrow maxilla. Posterior open bite
associated with abnormal tongue habit is actually most of times due to
abnormal tongue posture.
When maxilla is expanded with RME, this will lead to
correction of adaptive posture and posterior open bite.
Regarding prognosis, prognosis of acquired abnormal posture
is better than endogenous type because specific cause may be
eliminated in case of acquired one.
4 Retained infantile swallow
Infantile / visceral swallow is normal for infants upto age of
11/2 year beyond which this immature type of swallowing pattern
get change to mature swallow through transition period.
Retained infantile swallow is rare but if present, it has poor
prognosis. So it is very important to diagnose this rare entity
correctly, which require knowledge of infantile and mature swallow
pattern features. Various characteristic features differentiate mature
from immature swallow.
Infantile swallow
Infantile swallow is one of the good example that whatever might be
best suited at one time for a particular physiologic need / situation may
become problem after a specific time.
Infantile swallow pattern is unique and sophisticated in various
ways
-In neonates, stomatognathic musculature is most sophisticated
musculature in whole body.
-Discrete unilateral response of tongue towards the side of
stimulation is not found in any other muscle in body.
-Mouth is primary sensory input area of child especially during first
6 months.
-Suckling is a rhythmic activity which need great assistance of
tongue & orofacial musculature. As child see source of nutrition,
head is extended towards the source ( e.g during breast feeding),
infant closes lips around nipple like a sphinctor, jaws kept apart,
tongue comes in between gum pads followed by rhythmic
depression of cheek, bobbing of hyoid bone and fast backward and
forward movements of tongue.

.
11
Muscle most likely responsible for maximum share of suckling work
is Genioglossus. Characteristic features of infantile swallowing (by
Moyer)
-Jaws are apart with tongue between gum pads
-Mandible is stabilised primarily by contraction of facial
muscles and interposed tongue.
This is an important features because usually children with infantile
swallow have expressionless faces as muscles of facial expression are
performing heavy duty of stabilising mandible instead of performing
delicate facial expression
Swallow is guided and greatly controlled by sensory exchange
between lips and tongue.
Transition period
This period characterize the transition of infantile swallow to
mature swallow. This takes places gradually and starts with eruption of
deciduous teeth especially deciduous molars. In normally developing
and maturing child, mature swallow may be observed by age of 1 ½
years. Most characteristic feature during transition period is diminished
activity of buccinator muscle.
Moyer has stated following characteristics of mature
swallowing pattern.
-Teeth are together during swallowing.
-Mandible is stabilised by muscles of mastication rather than muscles
of facial expression.
-Tongue tip held against palate above and behind the upper incisors.
-Minimal contraction of lips
Other features of mature swallow are
-Mandibular posture is no longer prognothic
-Tongue no longer plunges forward and backward as needed in suckling
/ immature swallow.
Phases of mature swallow
Knowledge of various phases of mature swallow helps in
differentiating mature swallow from immature swallow and moreover
various activities of muscles during swallowing may be known which helps
in correlating various types of abnormalities associated with swallowing
problems.
There are four integrated phases of mature swallow
.Preparatory phase :
It begins with entry of food into mouth
-food is converted into bolus which lies on tongue-at this stage, oral cavity becomes sealed unit as tongue presses against
-soft palate posteriorly
-buccal teeth and soft tissue laterally
-lips and teeth anteriorly- Jaws stabilized by muscles of mastication.Oral phase
-Opening of posterior aspect of sealed oral cavity
-Soft palate seals off nasal cavity-Posterior part of tongue drops down and moves backward
-Various peristaltic types movement of tongue..
Pharyngeal phase
Food moves from oral cavity to pharynx and whole pharyngeal complex
reflexly move upward
Eosophageal phase :
Food passes through pharynx to eosophagus and is involuntry in control.
During this phase still going on, tongue and palate return to their original
position for next swallowing cycle.
Important questions after considering all these normal and immature
swallowing pattern is that “Is there any altered muscular force balance
occuring with infantile swallow which may lead to deliterious effect
on dentition”.
This question is still unexplained fully especially with regard to tongue.
Acc. to proffit, altered tongue activity is adaptives response rather than as
causative factor in malocclusion.
One logic to substantiate this hypothesis is that if tongue really cause
malocclusion (eg anterior open bite) then it must express its ill effects on
deciduous dentition because infantile to mature swallow transition occur
at age 1 ½ years.
Effect of altered tongue movement
Acc. to Garliner, tongue may act as impeding force or as a
moving force. Impeding force prevent any natural movement of
dental units (eg prevent eruption of teeth). But as moving force, it
actually moves the teeth.
Simple anterior swallow :
Simple anterior swallow is characterized by anterior position
of tongue during swallow. Tongue may be hitting against the upper
incisor or protruding in between upper and lower incisors.
While it hit against the incisors, it act as moving force and
cause labial flarring of these teeth. But when tongue protrude
between upper and lower incisors, it act as impeding force which
may (if present during eruption of incisors) prevent eruption of
incisors and hence anterior openbite .
complex swallowing problem.
In this type, the abnormality of musculature extend from
molar to moral. Malocclusion seen is open bite which is not limited
to anterior region.
Unilateral swallowing problem
Tongue moves at 45angle against the dentition in bicuspid
and molar areas and stress of this force may manifest as open bite
from lateral incisor to first molar.
Bilateral swallowing problem
Characterized by bilateral depression in molar areas but some
occlusion may be present in anterior region
With all these 4 swallowing problem, the effects produced on
dentition are not only because of tongue itself but because of
involvement of various other muscles eg :

.
12
-weakness of orbicularis oris muscle owing to fact that
protrusion of tongue in simple anterior swallow seals the oral
cavity preventing need of normal function of orbicularis oris.
This weakened muscle exaggerate the effect of tongue as
moving forces on incisors because there is no adequate counter
balancing force from labial side by orbicularis oris.
Weak masseter muscle
Normal masseter muscle activity depend on contact between
posterior teeth. Presence of tongue between posterior teeth Prevent
full expression of masseter muscle activity which on long term basis
cause disuse atrophy of massester.
This weakened massester muscle further reinforce the
infantile swallow because normal masseter muscle activity is not
there to support & stabilize mandible during mature swallow.
Hyperactivity of mentalis muscle because extensive movement of
lower lip occur during immature swallow.
Diagnosis :
History
History should include following
-Information regarding any other oral habits eg thumb sucking, mouth
breathing
-Information regarding any infection of upper respiratory system,
inflammed tonsils for long duration.
-Information regarding the swallowing pattern of sibling for possible
hereditary etiologic factors.
-Information regarding parameters of habit performance eg
intensity,duration and frequency.
Examination
It is very important to do proper functional analysis to
determine the specific type of habit and possible involved factors.
Perverted swallowing habit should be detected and corrected early to
facilitate normal development of dentition and palate.
Functional analysis of tongue
Tongue and lip functions are synchronized in their
activities. Thus it is possible to get idea about abnormal tongue
function from observed lip musculature. Eg : In infantile swallow
pattern with tongue thrust, lower lip also shows marked activity.
Ideally tongue should be examined without displacing
either tongue or lips because when lips and cheeks are retracted
with mouth mirror, normal tongue activity may be inhibited.
A) Posture of tongue
Tongue is examined for posture while mandible is at
physiologic rest position. One way is to trace this posture from
cephalogram taken with mandible at rest position. Clinically it is
evaluated by asking Patient to sit in upright position, & then tongue
and lip relationship examined gently. In this position, dorsum of
tongue should touch palate lightly and tip resting in lingual fossa or
at crevices of mandibular incisors.
Next tongue is observed during various swallow. During
normal mature swallow tip of tongue should touch curvature of palate
just behind the maxillary incisors.
As during swallowing it may be difficult to observe various
tongue movement and position directly, an indirect method is given
by Dr. Everitt Payne et al called Payne technique.
This technique measures where exactly tongue hit during
normal swallowing.
The revealing substances used in this technique is orabase. With 1%
sodium fluorescien solution in water soluble base. Procedure is as follow
-Tongue is dried at areas where revealing substance is to be placed.
-A thin layer of substance is coated over the dry portion of tongue and
patient is asked to swallow.
-Black light technique (i.e dark room facility) will show exactly where all
tongue moved during swallow because in dark room, sodium fluoresciene
will glow.
Swallow
Swallow is a complex integrated physiologic process which is
entirely a muscular activity. As various muscles are involved, specific and
definite stress patterns are observed in swallowing. Normal swallow
procede as follow
-Tongue tip placed just behind maxillary incisors.
-Midpoint of tongue is raised to top of oral cavity i.e against hard
palate.
-Tongue moves against hard palate in posterior direction tipping at
45so that posterior part of tongue will lie against the pharyngeal
wall.
-Simultaneous with tongue action, buccinator and masseter
-muscle extert lateral forces against dentition.
-Orbicularis oris generates posterior force against maxillary
anterior teeth.
Hence 3 major muscle groups are activated
.Tongue – tongue itself is very strong muscle which
counter-act the force of buccinator, masseter and
orbicularis oris muscles.
.Masseter and buccinator
These muscles get activated during each swallow. Failure
in activation of these muscles is caused by either placement
of tongue between posterior teeth or poor posterior
occlusion.
.Orbicularis oris muscle
Acts as stabilizing force. Hence act as natural anterior
retainer for maxillary incisors. These various stress pattern
and their significance is well understood by triangular
force effect.

.
13
Methods of swallow examination
-patient is ask to sit upright with unsupported back and head.
-Observe unnoticed various swallow.
-Then small amount of water is placed in mouth and patient is asked
to swallow.
Various events that occur in mature swallow (which act as guide to
differentiate mature from immature swallow) are
-Mandible raises to bring teeth together during swallow.
-Lips touch lightly without any obvious movements.
-Facial muscles do not show any obvious contractions.
-Hand is placed over temporalis muscle and patient is asked to
swallow. If Contraction of temporalis felt, it indicates that
stabilization and elevation of mandible during swallow is brought by
contraction of muscle of mastication.
-Lower lip is held gently with fingers or a tongue depressor is placed
over lower lip. Individuals with normal swallowing completes the
swallowing cycle with no movement of lip.
Those patient who have immature swallowing will feel that their
swallowing act is inhibited by finger held lip because strong
mentalis and lip contraction are needed for mandibular stabilization
in teeth apart swallow.
Functional features of various types of swallow
1. Normal infantile swallow :
This is seen in infants below the age of 1½ year beyond which a
normally growing child show mature swallow.
-Tongue lies between gum pads
-Mandible stabilized by muscles of facial expression, buccinator
being the most prominent.
-Reduced activity of buccinator is a feature of transition from
infantile to mature swallow.
-Most characteristic feature of cessation of infantile swallow is
appearance of contraction of mandibular elevators during swallow
to stabilize the mandible.
2. Mature swallow
-Contraction of mandibular elevators
-Very little / minimal lip and cheek contraciton)
Mild activity of lips may be seen with mature swallow during mixed
dentition period because spaces are present due to some missing teeth
as a part of transition of dentition. So lips show mild contraction to
secure the oral seal.
3. Simple tongue thrust swallow
-Typical contraction of lips, mentalis.
-Normal contraction of mandibular elevator as teeth are
together during this swallow.
-This type of tongue thrust is a adaptive response to existing
malocclusion ie anterior open bite.
-Inflammed tonsils in mild form that do not impart tooth apart
swallow may lead to simple tongue thrust swallow.
In prolonged cases of tonsiller enlargement or inflammation,
eventually complex tongue thrust will develop.
Complex tongue thrust swallow
-characterized by absence of contraction of masticatory muscles ie teeth
are not held together during complex tongue thrust swallow.
-Facial and mentalis muscles show obvious contraction.
Retained infantile swallow
Defined as predominant persistence of infantile swallowing reflex
after arrival of permanent teeth.
-True retained infantile swallow is rare.
-There is very strong contraction of lips and facial muscle even to the
extent that massive grimace is evident.
-Particular noticeable contraction is of buccinator muscle.
-Patient has inexpressive faces because muscles of facial expression are
involved in stabilization of mandible.
-Patient suffer with severe masticatory difficulty as most of the times
only one molar in each quadrent is in occlusion. Mastication usually
occur between tongue tip and palate because of inadequacy of occlusion.
Hence a typical history of soft diet is frequently found in patient with
retained infantile swallow. Gag threshold is also low.
Management of abnormal tongue thrust and swallowing habits.
At this point, particular type of muscle abnormality (habit) should be
identified because different type of habits need different line of
management and also with different prognosis.
Various factors to be considered before any treatment planing are
1. Age : Although transition from infantile to mature swallow should
occur at age of 1½ years, but treatment should not start before eruption
of permanent incisor unless untill obvious malocclusion occur in
deciduous dentition. This is because occasionally some children are late
maturers and therefore infantile swallow pattern may remain to some
extent in deciduous dentition period.
But if habit does persist during eruptive stages of permanent teeth
eg permanent incisors it should be taken seriously because as already
mentioned, tongue may act as impeding force and prevent eruption of
permanent teeth & causing anterior open bite.

.
14
2. Associated manifestation :
As with any other habit, treatment is not recommended unless it
has affected dentition or speech. But a watch should be kept on suspected
cases where habit has potential to produce malocclusion.
3. Malocclusion – sometimes malocclusion itself is a cause for habit, as
anterior open bite may lead to simple anterior tongue thrust habit. So in
those cases, correction of malocclusion itself will lead to spontaneous
correction of habits
4 Associated other habits
If patient has thumb sucking habit with tongue thrusting habit, thumb
sucking habit should be eliminated first.
5 .Associated problems of orofacial system :
If patient has problems which act as cause for tongue thrust, than those
causative factors should be removed first eg enlarged & inflammed tonsils
of chronic nature should be treated / removed first.
6 Speech defects
Tongue thrust (complex tongue thrust) may be associated with
speech defects eg ‘s ‘ lisp. In those case, orthodontic and speech therapy
should be considered together.
Treatment modalities
1 .Training for correct swallow and posture /position of tongue
.Myofunctional exercises
2 .Mechanotherapy for habit breakage
3 Surgical treatment
4 Speech therapy
Myofunctional exercises
1. For tongue
2. For masseter
Masseter count to ten exercise
3. For lips
4. For swallow
1 a)For tip of tongue
One elastic swallow
5/16 inch elastic is placed on tip of tongue. Patient is guided to
place this elastic with tongue tip at correct desired position i.e just
posterior to incissive papilla, then asked to clench back teeth, open
the lips and swallow.
It is important that exercise should be performed with lips
apart; reason being to break reflex action where tongue tries to
touch closed tips.
For tip of tongue
For mid portion of tongue
For posterior part of
tongue
1 b)Tongue hold exercise
Same 5/16 inch elastic is placed on tip of tongue but to hold this
elastic slightly posterior to incissive papilla for prescribed period of
time. Gradually holding time is increased from 5 minutes to 1 hour.
This is the only exercise in initial plan of therapy which is
performed with closed tips reason for this is.
-To stimulate nasal rather than oral breathing by forcing the lips to
close.
-To accustom patient to negative pressure which occur during
swallowing act
-This tongue hold exercise also places the entire tongue in mouth at
proper position.
Exercise for mid portion of tongue
Two elastic swallow
two 5/16 inch elastics, one on tip and other an mid point of tongue
are placed. patient is instructed to place tongue tip at predetermined
position (i.e just posterior to incissive papilla) and other mid elastic
on hard palate and than swallow. This corrects the abnormal
tongue position in infantile swallow where tongue tip is placed
lower and mid portion is collapsed
Hold pull exercise
Tip and mid point of tongue an placed at correct pre determined
position. With this position, mandible is opened gradually. Purpose
of this exercise is to keep front and mid portion of tongue at proper
position during swallowing.
Exercise for posterior part of tongue
There elastic swallow
Three 5/16 elastics are placed, one on tip, other on mid point of
tongue and 3rd on posterior part, but care should be taken not to keep
posterior elastic too backward otherwise patient may swallow it.
During normal swallow, posterior part of tongue is pressed against
the pharyngeal wall
This exercise is also performed with lips open to break tongue lip
reflex.

.
15
Exercise for masseter
Reason for prescribing masseter muscle exercise is that in
complex tongue thrust when teeth are apart during swallowing,
masseter muscle is not activated and on long term basis this muscle
undergoes disuse atrophy. Masseter muscle is much required
during normal swallow to elevate and stabilize mandible.
Masseter count to ten exercise
This is an isometric resistance exercise which strengthen masseter
muscle. Patient is asked to clench posterior teeth forcefully and
counting ten. Exercise should be performed frequently in morning
and evening.
Exercise for lips
As noted earlier, tip and tongue actions are synchronized so its
important that lips functions should also be proper for proper
swallowing.
Tug of war and button pull exercise
Both these exercises are to strengthen the lip musculature.
A string is tied to two buttons usually size of a quater and one button is
placed between lips of patient and other is held by parent in tug of war
Exercise or by the patient himself in case of button pull exercise
Mashmallow twist exercise
Excellent strengthning exercise for lower lip. Specially designed kits are
available with plastic discs weighing exactally same one another. String
is placed in patient’s mouth and patient lifts discs by extending lower lip.
Number of discs are increased gradually when patient lifts discs
comfortably until total become ten.
Exercise for swallow
Once patient has masterd muscle exercises for tongue, lips and masseter,
this integrated muscular activity is brought into normal mature
swallowing pattern.
Elastic for tongue exercises are replaced by liquid food and
patient is guided to perform mature swallow act. once patient becomes
comfortable with liquid food, solid food replaces liquid food.
Subconscious therapy
Once voluntary conscious swallowing pattern is learned by
child, then ultimate success lies in the conversion of this conscious
swallowing to subconscious/ unconscious swallowing behaviour.
Subconscious therapy is divided into three parts
•Time charts
•Subliminal therapy
•Auto- suggestion
Time charts
There charts remind patient to perform correct swallowing pattern at
specific times of day which will set a correct swallowing picture in
patient’s mind. The most important thing about these time charts is
that this recall must occur at exactly same time everyday
Day time
Sunday Morning Noon Night
To
Sunday
Subliminal therapy
child is asked to place a reminding sign within sight of place where
he/she eats. This reminding signs aids in subliminal recall, everytime
child eats.
Auto suggestion
Patient is asked to swallow correctly six time just before going for
sleep and than repeat six times “I will swallow correctly all night” .
.
Mechanotherapy for correction of Tongue Trusting habit.
Both fixed and removable appliances can be used to restrain
the various tongue movement. Fixed appliances should never be
used without child’s co-operation , otherwise child will take it as
punishment.
Purposes of appliances
-Tongue Thrust correcting appliances tend to force tongue downward
and backward. These appliances are more effective when they form a
sort of picket fence behind lower incisors, as with palatal spurs. spurs
are bent downward and their correct position is attained with normal
posterior occlusion during swallow.
-Appliances also re-educate tongue position so that dorsum of tongue
approximates palatal vault and tip of tongue contacts the palatal rugae
area.
This proper position of dorsum of tongue prevent lateral spreading
and consequent lateral pressure on dentition during swallow.
Removable appliances
Variety of modifications of Hawley’s appliance may be
used e.g. Tongue rake, tongue crib, Tongue spikes.
Most efficient is tongue spikes with sharp ends as it
brakes the reflex of tongue thrusting. Patient may feel
discomfort for initial few days but tongue adapts rapidly.
These removable appliance may be kept for 4-6 months .
Advantage of Howley’s appliance is that at same time
of habit correction, minor irregularities of teeth can be
corrected .

.
16
Fixed habit breaking appliance
Tongue spike may be used as fixed appliance by soldering
lingual arch with spikes to molar bands.
If tongue crib is soldered similarly as tongue spike , it may
be unsuccessful because the tongue pressure transmitted through
crib to molars may actually move entire upper arch forward.
Fixed tongue spike require 4-6 month time period to
correct habit.
Oral screen
Oral screen is another effective means of habit correction
with added advantage that being a myofunctional appliance, the
various deleterious forces may be transmitted to desired direction
as beneficial forces. For tongue thrust habit correction, combine
oral and vestibular screens are formed.
Miscellaneous appliances
Depending on patient’s over all treatment plan, some otherappliances may also correct tongue thrust habit along with theirintended function e.g. Activator may prevent tongue thrusting inanterior and lateral direction.
Surgical options
Very rarely a surgical treatment may be needed for correction oftongue Posture and position as in case of Macroglossia whichneccesitate partial glossectomy.
In cases where chronically enlarged tonsils poseproblems for habit correction, tonsils should be removed.
Prognosis
Prognosis of simple anterior tongue thrust is excellent and mostof times get spontaneously corrected once underlying cause i.e.Anterior open bite is corrected.
Prognosis for complex tongue thrust is poor.
For retained infantile swallow, prognosis is very poor.
Mouth Breathing
Mouth breathing is always abnormal, whether it is a habit or
necessity due to blockage of normal upper respiratory passage.
New born infants are obligate nasal breather and slowly this
pattern shifts to facultative nasal breathing i.e. a child/person may
breath through mouth but primary breathing is through nasal route.
Then one question arises “why one should breath through nose and
not through mouth”.
There are various physiologic factors associated with nasal
breathing which protect respiratory system. Important one are
humidification and warming of air, filtration of various harmful
particles. As will be mentioned later, nasal breathing is essential for
normal growth and development of stomatognathic system.
From this discussion, it is clear that a person will always try to
breath through nose and not from mouth. Hence, if someone breath
through mouth because of some underlying factors e.g. nasal
obstruction, Anatomically abnormal lips etc., it can not be termed
habit as these factors force individual for mouth breathing. But if
he/she continue to breath through mouth even after elimination of
underlying cause, then it can be termed as habit.
so initiation of mouth breathing is not a habit but continuation
beyond a particular time i.e after removal of cause, it becomes
habit.
Definition
Sassouni (1971) defined mouth breathing as habitual respiration
through mouth instead of nose.
Merele (1980) suggested term oro–nasal breathing instead of
mouth breathing because according to him, breathing is never
100% through mouth whatever may be the cause for mouth
breathing.
Classification
Finn (1987) classified mouth breathing into
1. Anatomic
Anatomic mouth breather is one whose short upper lip does not
permit complete closure of lips along with lower lip without
effort
2. Obstructive
This group include those individuals who have partial / almost
complete obstruction to normal flow of air through nasal passage.
3. Habitual
this group include those who continue to breath through
mouth even after removal of nasal obstruction.

.
17
Etiology
Apart from anatomically short upper hip, the other cause for
mouth breathing is nasal obstruction.
This airway obstruction may be due to
- enlarged turbinates
- Deviated nasal septum (DNS)
- Allergic rhinities, nasal polyps
- Obstructive sleep apnoea.
Although many times Adenoid faces characterized by long narrow
face and nasal passage are associated with mouth breathing, but it is
not very clear that whether this particular pattern is due to mouth
breathing or it develops to facilitate mouth breathing. It is noted that
in a parson with Adenoid faces, a moderate local factor may obstruct
nasal passage which may not do so in normal child.
The only direct effect of mouth breathing is mouth breathing
gingivitis and increased risk of caries especially in maxillary
Anterior Region. Then, “How does mouth breathing can lead
to malocclusion”.
The Answer lies in the fact that mouth breathing necessitates
altered facial musculature balance by lowering the position of
tongue and mandible in order to keep oral airway patent. If these
postural changes are maintained, anterior lower facial height
would increase and posterior teeth will supra-erupt.Unless vertical
growth of ramus is present, mandible will rotate downward and
backward opening the bite anteriorly and increasing overjet.
Increased stretch of cheek may exert pressure and cause
narrowing of maxillary arch.
DIAGNOSIS
History
History is very important because it may give clue of
underlying etiologic factor.
Parents should be asked whether child had / have frequent
occurrenc of tonsillitis, allergic rhinitis etc; or if child frequently adopt
lip apart posture.
Examination for moth breathing
Observe the patient unoticed when he/ she sit comfortably on
chair. Initially patient might have anxiety which may lead to mouth
breathing even in some normal children. Most obvious observation that
can be made is lip apart posture. In normal relex individual, lips are
touching lightly. But in mouth breather, lips will be definitely apart at
rest for passage of air. Lips will be dry, scaly because of continuos
drying and this may predispose to lip wetting habit. Same drying effect
predispose for mouth breathing gingivitis and increased risk of dental
caries.
Functional Examination
Ask the patient to take a deep breath. A mouth breatherwhen asked to close his / her lips and take deep breath, there willbe no appreciable charge in size and shape of external nares incontrast to normal nasal breather which show dilatation of naresduring lips closed deep breathing because nasal breathers normallydemonstrate good reflex control of alar muscle which control thesize and shape of external nares.
Various clinical tests may be performed to demonstrateabsence of nasal breathing and also to differentiate betweenblocked right or left nostril.
1 Water holding test
This is most commonly performed test in clinics. Patient is asked to hold water in mouth for a prescribed period of time. It is obvious that if child is mouth breather, it will be impossible for child to hold water in mouth.
2. Mirror test
A two sided mirror is placed in horizontal / oblique directionbetween nose and mouth. If child is nasal breather, there will befog on side of mirror facing towards nose.
3. Butterfly test – it is to differentiate nasal obstruction betweenright and lift nostril. A small butterfly shape piece of cotton isplaced on upper lip and observed. The side of nose which ispatent, will cause fluttering of cotton on respective side.
4. Inductive plethysmography (Rhinomanometry)
This is only reliable test to quantify the amount of air which isactually passing through nose and mouth. long face children mayhave less then 40% of nasal breathing.
5. Cephalometrics
Cephalometric may show the amount of nasopharyngeal space,size of adenoids etc especially if cephalograms are taken fromvarious angles.
Management
Treatment consideration
Age – self-correction of mouth breathing could be expected as
child mature unless there is an obvious and marked nasal
obstruction. This is due to the fact that there is an increase in nasal
passage as child grows especially if obstruction was due to
enlarged adenoids.
E.N.T Consultation
almost all the time cause of mouth breathing is nasal obstruction,
so any E.N.T pathology should be ruled out before any habit
correction attempt.

.
18
Treatment
Elimination of cause – Any underlying cause must be
removed e.g nasal obstruction
Interception of habit
Even after removal of causative factor if habit persist,
following measures should be taken
Exercises
1. Physiologic exercises
2. lip exercises
physiologic exercises
Deep breathing exercises are done in morning and evening. Child is
instructed to raise arms sideways and take deep inhalation through
nose. After a short period of time, arms are dropped to sides and air
is exhaled through mouth.
lip exercises
These exercises are aimed to restore normal size, posture and
functional tone of lips.
But before these exercises are attempted, any malocclusion which
prevent proper functioning of lips (i.e preventing proper lip seal)
should be eliminated e.g Bimax. protrusion.
lips of chronic mouth breather are abnormal in following respects
- under development of upper lip i.e. short upper lip.
- Lower lip is flabby and hypotoned.
Voluntary muscle exercises and normal functioning will restore these
structures to their correct size and optimal size, tone and functioning
provided such exercises are performed routinely.
The various exercises are
.lip elongating exercises
. Wilson exercise
lip elongating / stretching exercise
Modeling compound of adequate amount & in
mouldable form is placed in Anterior Vestibule so that it
fills whole vestibule plus some of material extend between
incisors on which patient bites and make permanent
indentation which will later on help in stabilization of
device when in use.
Device is used by asking patient to place it in
mouth and then try to bring lips together. This exercise is
very helpful especially in case of short upper lip. A more
durable from of same device can be made from acrylic.
Wilson’s Exercise (by William E. Wilson)
This exercise is very helpful when under grown
and hypotoned lips are due to chronic mouth breathing.
This exercise develops orbicularis oris and associated
muscles establishing normal muscular tone around mouth
opening plus stimulating nasal passage by heavy rush of air
through one nostril at a time
Technique
Child is instructed to perform this technique as follow
- Stand in front of mirror
- close teeth and lips without forcefull action
- Contract the muscles at left corner of mouth causing left cornerto be pulled backward and upward.
- palmer surface of left hand fingers are placed on right cheek,and now press this cheek tissue forward and to left, at the same timeholding the right nostril closed with index figure of left hand. Tissuesat left corner of mouth must continue in contraction all through thismuscle pulling with left hand fingers.
- While tissues at left corner are still contracted and right cheekis under pressure by fingers, breath deeply 3 times through the leftnostril.
- Relax the muscle and remove left hand.
- Perform similar procedure on opposite sides.
- Perform this habit 3 times thrice a day.
Appliances for correction of mouth breathing
Oral / Vestibule screen
It is most effective way to re-establish nasal breathing by
preventing air entering into oral cavity.
vestibule screen made of acrylic with holes is very effective.
Holes should be blocked gradually as child start feeling comfortable
and ultimately all the holes are closed.
A modification of this conventional vestibular screen is given
by Holtz where a ring is placed in Anterior portion of screen at level
of inter-labial gap. Advantage of this modification is that it can be
used as lip exercise device.

.
19
Maxillothorax Therapy (by Macaray 1960)
This therapy uses a activator made up of aluminum withwhich development of dental arches and dental base relationshipcan be corrected along with correction of mouth breathing.
This stable aluminum activator is incorporated at angle ofmouth with horizontal hooks to which expanding rubber bands areattached.
Child holds activator in mouth and at the same timecarries out exercises as follow
Child stands with his back against the wall, rises andlowers on his toes and at the same time performing lightly forcedbreathing with tightly closed lips.
As from the name itself it is indicative that this exercisehelps in throrax / chest expansion along with correction of mouthbreathing.
Lip habits
Normal hip anatomy and function are important for
speaking, eating and maintaining a balanced occlusion.
Lip habit may involve either of lips but predominantly lower
hip is involved.
Definition
Lip habit may be defined as those habits that involve
manipulation of lip/ lips and perioral structures.
Types of lip habits
Two types of lip habits
- wetting the lips with tongue
- pulling the lips into mouth between the teeth (Schneider
1982)
lip sucking habit has potential to produce malocclusion if
practiced with sufficient intensity and frequency. lip wetting is not
a problem for occlusion.
Lip Sucking
It is commonly associated with lower lip where lip is
pulled between teeth and clinically lips are characterized by
reddened, irritated areas below vermilion border.
An important but distinct variation of lip sucking habit is
Mentalis habit.
Mentalis muscle originates on labial surface of mandible in arch
of apices of mandibular incissors. Its fibre get extended inferiorly
crossing over the midline and intersecting and inserting into soft
tissue of chin. Function of mentalis muscle is to lift the lower lip.
When muscle is flexed, skin of chin appear puckered.
lip sucking and mentalis habits may be differentiated by
the fact that in case of lip sucking, entire lip including vermilion
border is pulled into mouth whereas in mentalis habit, vermilion
border of lower lip is often everted with lingual aspect elevated
into mouth and a sublabial contracture line develops between lip
and chin. Vermilion border of lower hip may be relocated further
out side mouth because of continuous drawing and wetting.
But regarding development of malocclusion, lip sucking and
mentalis habit have similar effect as in both cases lip in wedged
between upper and lower incisors and on long term bases, it will
cause proclination of upper incisors with development of spaces
& collapsed , crowded lower incisors.
Menatalis habit along with hyperactive inferior orbicularis
oris may cause gingivitis in mandibular anterior region due to
continuous Irritation.
This clinical finding is important because presence of
gingivitis in mandibular anterior region without involving
maxillary anterior region( which is characterstick site in case of
mouth breathing gingivitis ) may indicate hyperactive mentalis
muscle.

.
20
Etiology
1. Malocclusion
Class II Div 1 malocclusion with large overjet and deep bite
predispose to lip sucking habit because child tend to produce
normal lip seal during swallowing by placing lower lip
posterior to maxillary incisors.(called lip trap )
2 Habits – Thumb sucking habit my predispose to lip
sucking habit by increasing overjet.
3 Emotional stress – This may increase the intensity and
duration of lip sucking habit.
Management
Associate factors which predispose to habit e.g class II Div
1 malocclusion or increased overjet due to previous thumb
sucking should be eliminated.
A self disciplinory approach where child reinforces
himself that he will not indulge in habit is very effective because
most of them are adolescent.
Lip Bumper
lip bumper acts as both reminding device and habit
interrupting appliance by making it difficult to draw the lip
between anterior teeth.
Bruxism
Bruxism is grinding of teeth especially at night. Strictly speaking
it can not be considered habit because almost all the times there is a
definite underlying etiologic factor e.g occlusal discrepancies.
But if habitual grinding continues even after removal of
causative factor, then it can be considered as habit.
Definitions
Ramfjord (1966) –Ramfjord defines bruxism as a habitual
grinding of teeth where individual is not chewing or
swallowing.
Vanderas (1995) defined bruxism as non functional movement
of mandible with or without an audible sound occurring during
day or night.
Manifestation
Signs and symptoms of bruxism depend on frequency,intensity, duration of habit and age of patient.
1. Occlusal Trauma
Bruxism may lead to teeth mobility which is more in morning dueto nocturnal bruxing activity.
2. Attrition
Typical wear facets are seen on occlusal table of posterior teeth. Ifbruxism habit is performed as lateral functioning, incisal wear isalso common especially tip of canines.
3 Muscle tenderness
Patient give history of muscle tenderness espcially in morning. On palpation, lateral pterygoid and masseter are common to show this tenderness.
4 T.M.J disorder
Prolong habit will lead to clicking, crepitates in TMJ and deviation of mandible on closure because habit is usually performed more on one particular side.
.
21
Etiology
1. CNS – Etiology of bruxixomania could be from certain definite
cortical lesions e.g children with cerebral palsy and mental
retardation.
2. Occlusal discrepancies – Improper interdigitation of teeth is
most common cause for bruxism.
3. Psychological factors – Teeth grinding could be a
manifestation of inability to express emotions such as anxiety,
anger etc.
4. Genetics – Genetics may be factor because there is a reported
incidence bruxism in certain families.
5. Occupational factor – Competition sports may lead
to clenching which later on may turn as habit.
6. Systemic factors – deficiency of mg2+ has been
reported as one of the cause.
7. Gingival and periodontal factors – chronic gingival
and periodontal lesion e.g. chronic periodontal abscess
may impart teeth grinding habit as patient feel comfort.
Diagnosis
History is very important. patient is asked about
muscular tenderness in morning. Occasionally patient may not
be aware of habit if only nocturnal bruxism in present. In those
cases parents may provide information regarding habit.
ExaminationTypical wear facets on occlusal table are evident.
By using articulating paper, underlying occlusal disharmony
may be find out.
Treatment
Occlusal splints and occlusal adjustments are usually
sufficient to correct habit. But most important part is that nothing
should be considered without removing the occlusal interference by
occlusal adjustments. Removal of interference result in immediate
disappearance of habitual grinding if occlusal disharmony is the
sole cause.
Occlusal splints are indicated to deprogramme the existing
muscular pattern. Soft splints are advisable with flat occlusal
surfaces so that manidibular movements will be free in all
planes which breaks the reflex response of muscles
established during habit.
2. Restorative treatment – If attrition is very sever which
pose threat for pulpal integrity, adequate restorative treatment
should be provided as initial measure.
3. Psychotherapy / Relaxation training.
If patient perform habit mainly due to stresses, a psychological
counseling is needed so that patient may avoid provocative
behavior.
4 Biofeedback is one of the means. In this technique patient is
allowed to view EEG Monitor while the mandible is postured with
minimal muscular activity.
.
22
3 Physiotherapy
If musculo-skeletal pain and stiffness are present, a brief
course of physiotherapy is advisable because indirectly it
also helps patient’s psychological relaxation.
4 Symptomatic treatment
Pain reliving drugs may be used. Other means for pain
relieve are TENS and Acupuncture methods.
Finger nail biting Habit.
This is one of the most common habit in adolescent and
Adults.
Age of occurrence
Nail biting is absent before age of 3, incidence rises
from 4-6 year of age and remain stable between 7 and 10
year and rises to peak during adolescence.
Persistent nail biting may be indicative of emotional
problem.
In teenage, nail biting habit may be substituted by pen /
pencil biting etc..
Rarely nail biting habit may cause malocclusion
because psychosocial pressure act as restraining
stimulus for habit performance. But if habit is practiced
with optimal frequency & intensity, minor rotation,
mild crowding may develop
3 Physiotherapy
If musculo-skeletal pain and stiffness are present, a
brief course of physiotherapy is advisable because
indirectly it also helps patient’s psychological
relaxation.
4 Symptomatic treatment
Pain reliving drugs may be used. Other means for pain
relieve are TENS and Acupuncture methods.
Diagnosis
• History and examination of finger nail will reveal the habit.
Management Psychologic counseling is sufficient in most of
cases. Avoid punitive methods e.g Scolding, nagging etc because as
habit is commonly due to emotional disturbance, these punitive
methods may exaggerate the emotional problems.
•If child is cooperative, various reminding methods may be used e.g
nail polish, application of mild bitter substances on fingers and
nails.
Self Injurious Habits
(Masochistic / Sadomasochistic habits)
These are self injurious habits where patient enjoys inflicting
damage to himself. It is very rare in normal children but can be seen in
mentally restarted children.
Definition
These habits may be defined as Repetitive acts that result in physical damage
to individual.

.
23
Etiology
1. Organic – Various syndromes and syndrome like
diseases e.g Lesch – Nyhan disease and De Lange’s syndromes
may be causative factors which lead to repetitive biting of lip,
finger, cheek, knee etc.
2. Functional – This can be further divided into-----
Type A – These are injuries superimposed on pre-existing
Lesion e.g a child with skin lesion of fingers perform finger
nail biting habit so skin lesion doesn’t heal.
Type B – These include injuries secondary to another
established habit. E.g Rotation of thumb with thumb suking habit
may damage soft tissue of hard palate.
Type C – it include injuries of unknown or complex etiology.
Treatment : Always with these habits, treatment should be initiated
with psychotherapy because almost all these patient have strong
emotional or psychopathic features.
Palliative Treatment
It is the adjunctive therapy e.g bandages for
ulceration etc.
Mechanotherapy
Vestibular screen will prevent unconscious
damaging act e.g. cheek biting while sleeping. Mechano
therapy may also includes use of restraints and protective
padding.
Related Documents