Biomechanics of the Lumbar Intervertebral Disk: A Review GAIL M. JENSEN, MA This article reviews the literature on the biomechanics of the lumbar interverte- bral disk according to: 1) disk structure and properties, 2) biomechanical principles and their application to the disk, 3) biomechanics and intradiskal pressures as they relate to posture, work, and exercise, and 4) prophylactic measures. Key Words: Anatomy, regional; Biomechanics; Intervertebral disk; Preventive med- icine. Low back pain is among the most common of all human disabilities, striking 70 to 80 percent of the population in industrialized society. 1,2 Many of the causes of low back pain are still unknown, yet suffi- cient evidence indicates that both degenerative and mechanical change within the intervertebral disk is one cause. 3-5 The most frequently recommended treatment for these patients with low back pain is physical therapy using various types of modalities and exercises. 6,7 Therefore, physical therapists must not only understand normal and abnormal function- ing of the disk, but also understand the mechanics involved. The purpose of this article is to present the clinical biomechanics of the lumbar intervertebral disk as a basis for prophylactic advice. ANATOMICAL CONSIDERATIONS Structure The intervertebral disk is a unique articular struc- ture, part of a component load-bearing system con- sisting of disks, vertebrae, ligaments, and muscles. The disk, thought to be the most critical component, 4,8,9 absorbs the load and distributes the forces applied to the vertebral column. 4,10 The struc- tures that permit this shock-absorbing, force-distrib- uting ability are the nucleus pulposus, the annulus fibrosis, and the cartilaginous end-plates 11 (Fig. 1). The nucleus pulposus consists of a gelatinous mu- coprotein and mucopolysaccharide structure located posteriorly in the lumbar part of the spine, between the cartilaginous end-plates, and is surrounded by the annulus fibrosis. 10,12 The polysaccharides give the nu- cleus a water-imbibing ability. The water content within the nucleus ranges from 85 to 90 percent of the total nucleus at birth to 70 percent in later years. 13 Pressure within the center of the normal nucleus is never zero, because of a preexisting tension even when the disk is unloaded. This characteristic is known as preload. The preload mechanism in the nucleus allows greater resistance to applied forces. 14,15 Great controversy prevails about the amount of movement of the nucleus during spinal motions. 5,15-17 A normally functioning disk is already located pos- teriorly in the lumbar part of the spine, so there will be a tendency for further posterior displacement with forward spinal movements. For example, spinal flex- ion would result in partial absorption and distribution of the load by the nucleus, with some backward displacement of the nucleus. 15,17 The annulus fibrosis is the laminated, fibrocartila- ginous structure encapsulating the nucleus. In this structure, two sets of fibers cross obliquely to each other at about ±30 degrees in relation to the disk 9,12 (Fig. 2). The annulus may be further divided into three layers, the peripheral portion being attached directly to the cortex of the vertebral body by Shar- pey's fibers and the intermediate and inner portions being attached to the cartilaginous end-plates 5,18 (Fig. 1). Annulus fibers are thicker and more numerous anteriorly than posteriorly (Fig. 3). The posterior and posterior lateral fibers have a more parallel alignment than do the anterior fibers. The posterior annulus fibers are also attached to the posterior longitudinal ligament, which is thinner in the lumbar region than in other spinal regions, 18,19 The disk is separated from adjacent vertebral bod- ies by articular hyaline cartilage or cartilage end- plates. After the age of eight, the cartilaginous end- Ms. Jensen was a lecturer at the Division of Physical Therapy, Stanford University School of Medicine, Stanford, CA, at the time the article was written. She is currently Staff Physical Therapist, Department of Physical Therapy, Menlo Medical Clinic, 1300 Crane St, Menlo Park, CA 94025. This article was submitted July 23, 1979, and accepted November 21, 1979. Volume 60 / Number 6, June 1980 765

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Biomechanics of the Lumbar Intervertebral Disk: A Review
GAIL M. JENSEN, MA
This article reviews the literature on the biomechanics of the lumbar intervertebral disk according to: 1) disk structure and properties, 2) biomechanical principles and their application to the disk, 3) biomechanics and intradiskal pressures as they relate to posture, work, and exercise, and 4) prophylactic measures.
Key Words: Anatomy, regional; Biomechanics; Intervertebral disk; Preventive medicine.
Low back pain is among the most common of all human disabilities, striking 70 to 80 percent of the population in industrialized society.1,2 Many of the causes of low back pain are still unknown, yet sufficient evidence indicates that both degenerative and mechanical change within the intervertebral disk is one cause.3-5 The most frequently recommended treatment for these patients with low back pain is physical therapy using various types of modalities and exercises.6,7 Therefore, physical therapists must not only understand normal and abnormal functioning of the disk, but also understand the mechanics involved. The purpose of this article is to present the clinical biomechanics of the lumbar intervertebral disk as a basis for prophylactic advice.
ANATOMICAL CONSIDERATIONS
Structure
The intervertebral disk is a unique articular structure, part of a component load-bearing system consisting of disks, vertebrae, ligaments, and muscles. The disk, thought to be the most critical component,4,8,9 absorbs the load and distributes the forces applied to the vertebral column.4,10 The structures that permit this shock-absorbing, force-distributing ability are the nucleus pulposus, the annulus fibrosis, and the cartilaginous end-plates11 (Fig. 1).
The nucleus pulposus consists of a gelatinous mu-coprotein and mucopolysaccharide structure located posteriorly in the lumbar part of the spine, between
the cartilaginous end-plates, and is surrounded by the annulus fibrosis.10,12 The polysaccharides give the nucleus a water-imbibing ability. The water content within the nucleus ranges from 85 to 90 percent of the total nucleus at birth to 70 percent in later years.13
Pressure within the center of the normal nucleus is never zero, because of a preexisting tension even when the disk is unloaded. This characteristic is known as preload. The preload mechanism in the nucleus allows greater resistance to applied forces.14,15
Great controversy prevails about the amount of movement of the nucleus during spinal motions.5,15-17
A normally functioning disk is already located posteriorly in the lumbar part of the spine, so there will be a tendency for further posterior displacement with forward spinal movements. For example, spinal flexion would result in partial absorption and distribution of the load by the nucleus, with some backward displacement of the nucleus.15,17
The annulus fibrosis is the laminated, fibrocartilaginous structure encapsulating the nucleus. In this structure, two sets of fibers cross obliquely to each other at about ±30 degrees in relation to the disk9,12
(Fig. 2). The annulus may be further divided into three layers, the peripheral portion being attached directly to the cortex of the vertebral body by Shar-pey's fibers and the intermediate and inner portions being attached to the cartilaginous end-plates5,18 (Fig. 1). Annulus fibers are thicker and more numerous anteriorly than posteriorly (Fig. 3). The posterior and posterior lateral fibers have a more parallel alignment than do the anterior fibers. The posterior annulus fibers are also attached to the posterior longitudinal ligament, which is thinner in the lumbar region than in other spinal regions,18,19
The disk is separated from adjacent vertebral bodies by articular hyaline cartilage or cartilage end-plates. After the age of eight, the cartilaginous end-
Ms. Jensen was a lecturer at the Division of Physical Therapy, Stanford University School of Medicine, Stanford, CA, at the time the article was written. She is currently Staff Physical Therapist, Department of Physical Therapy, Menlo Medical Clinic, 1300 Crane St, Menlo Park, CA 94025.
This article was submitted July 23, 1979, and accepted November 21, 1979.
Volume 60 / Number 6, June 1980 765
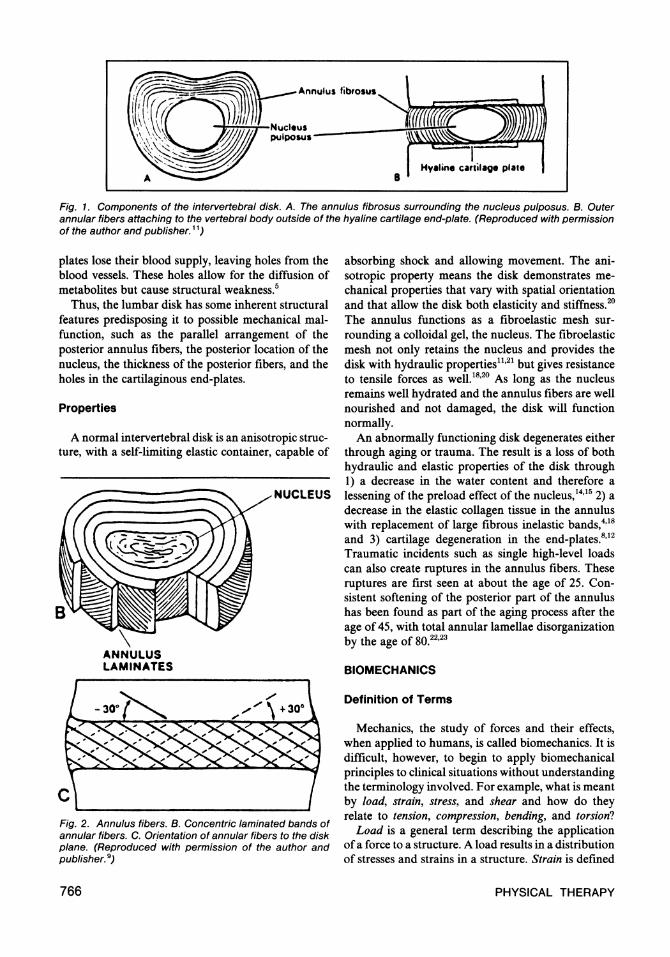
Fig. 1. Components of the intervertebral disk. A. The annulus fibrosus surrounding the nucleus pulposus. B. Outer annular fibers attaching to the vertebral body outside of the hyaline cartilage end-plate. (Reproduced with permission of the author and publisher.11)
plates lose their blood supply, leaving holes from the blood vessels. These holes allow for the diffusion of metabolites but cause structural weakness.5
Thus, the lumbar disk has some inherent structural features predisposing it to possible mechanical malfunction, such as the parallel arrangement of the posterior annulus fibers, the posterior location of the nucleus, the thickness of the posterior fibers, and the holes in the cartilaginous end-plates.
Properties
A normal intervertebral disk is an anisotropic structure, with a self-limiting elastic container, capable of
Fig. 2. Annulus fibers. B. Concentric laminated bands of annular fibers. C. Orientation of annular fibers to the disk plane. (Reproduced with permission of the author and publisher.9)
absorbing shock and allowing movement. The anisotropic property means the disk demonstrates mechanical properties that vary with spatial orientation and that allow the disk both elasticity and stiffness.20
The annulus functions as a fibroelastic mesh surrounding a colloidal gel, the nucleus. The fibroelastic mesh not only retains the nucleus and provides the disk with hydraulic properties11,21 but gives resistance to tensile forces as well.18,20 As long as the nucleus remains well hydrated and the annulus fibers are well nourished and not damaged, the disk will function normally.
An abnormally functioning disk degenerates either through aging or trauma. The result is a loss of both hydraulic and elastic properties of the disk through 1) a decrease in the water content and therefore a lessening of the preload effect of the nucleus,14,15 2) a decrease in the elastic collagen tissue in the annulus with replacement of large fibrous inelastic bands,418
and 3) cartilage degeneration in the end-plates.8,12
Traumatic incidents such as single high-level loads can also create ruptures in the annulus fibers. These ruptures are first seen at about the age of 25. Consistent softening of the posterior part of the annulus has been found as part of the aging process after the age of 45, with total annular lamellae disorganization by the age of 80.22,23
BIOMECHANICS
Definition of Terms
Mechanics, the study of forces and their effects, when applied to humans, is called biomechanics. It is difficult, however, to begin to apply biomechanical principles to clinical situations without understanding the terminology involved. For example, what is meant by load, strain, stress, and shear and how do they relate to tension, compression, bending, and torsion!
Load is a general term describing the application of a force to a structure. A load results in a distribution of stresses and strains in a structure. Strain is defined
766 PHYSICAL THERAPY
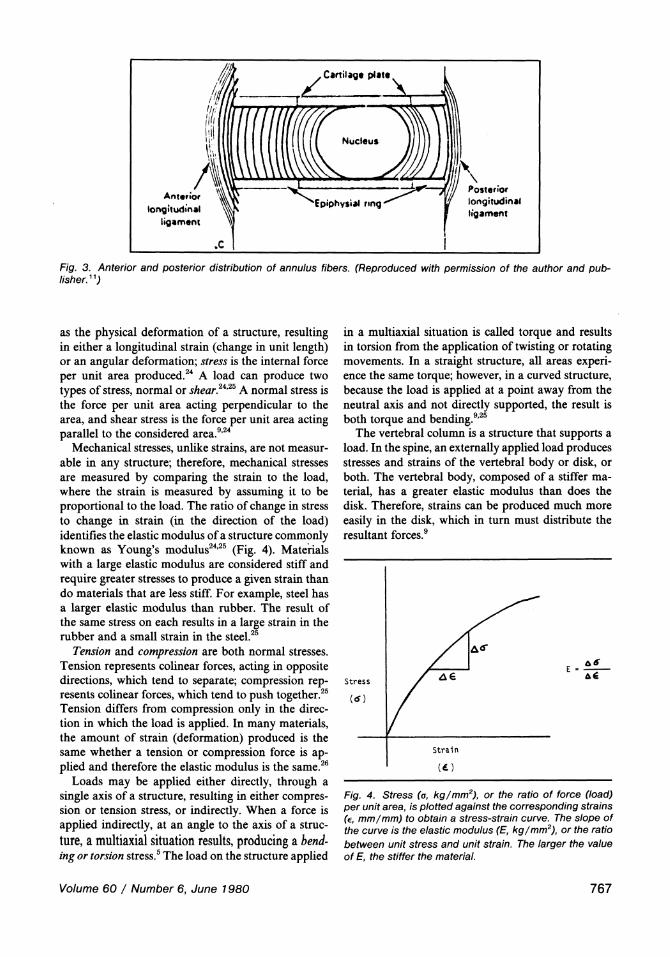
Fig. 3. Anterior and posterior distribution of annulus fibers. (Reproduced with permission of the author and publisher.11)
as the physical deformation of a structure, resulting in either a longitudinal strain (change in unit length) or an angular deformation; stress is the internal force per unit area produced.24 A load can produce two types of stress, normal or shear.24,25 A normal stress is the force per unit area acting perpendicular to the area, and shear stress is the force per unit area acting parallel to the considered area.9,24
Mechanical stresses, unlike strains, are not measurable in any structure; therefore, mechanical stresses are measured by comparing the strain to the load, where the strain is measured by assuming it to be proportional to the load. The ratio of change in stress to change in strain (in the direction of the load) identifies the elastic modulus of a structure commonly known as Young's modulus24,25 (Fig. 4). Materials with a large elastic modulus are considered stiff and require greater stresses to produce a given strain than do materials that are less stiff. For example, steel has a larger elastic modulus than rubber. The result of the same stress on each results in a large strain in the rubber and a small strain in the steel.25
Tension and compression are both normal stresses. Tension represents colinear forces, acting in opposite directions, which tend to separate; compression represents colinear forces, which tend to push together.25
Tension differs from compression only in the direction in which the load is applied. In many materials, the amount of strain (deformation) produced is the same whether a tension or compression force is applied and therefore the elastic modulus is the same.26
Loads may be applied either directly, through a single axis of a structure, resulting in either compression or tension stress, or indirectly. When a force is applied indirectly, at an angle to the axis of a structure, a multiaxial situation results, producing a bending or torsion stress.5 The load on the structure applied
in a multiaxial situation is called torque and results in torsion from the application of twisting or rotating movements. In a straight structure, all areas experience the same torque; however, in a curved structure, because the load is applied at a point away from the neutral axis and not directly supported, the result is both torque and bending.9,25
The vertebral column is a structure that supports a load. In the spine, an externally applied load produces stresses and strains of the vertebral body or disk, or both. The vertebral body, composed of a stiffer material, has a greater elastic modulus than does the disk. Therefore, strains can be produced much more easily in the disk, which in turn must distribute the resultant forces.9
Fig. 4. Stress (a, kg/mm2), or the ratio of force (load) per unit area, is plotted against the corresponding strains (є, mm/mm) to obtain a stress-strain curve. The slope of the curve is the elastic modulus (E, kg /mm2), or the ratio between unit stress and unit strain. The larger the value of E, the stiffer the material.
Volume 60 / Number 6, June 1980 767
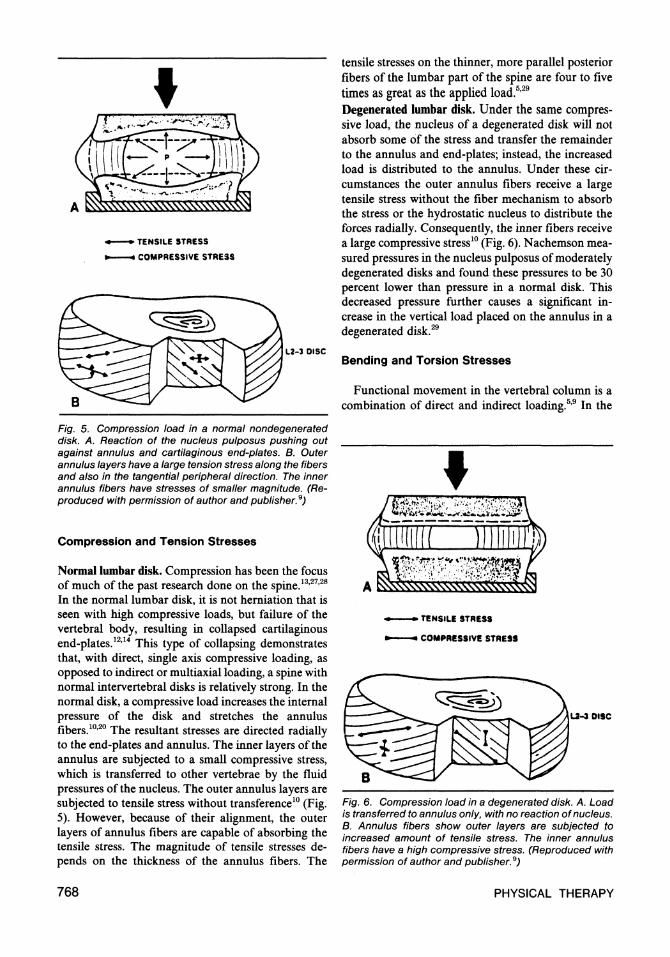
Fig. 5. Compression load in a normal nondegenerated disk. A. Reaction of the nucleus pulposus pushing out against annulus and cartilaginous end-plates. B. Outer annulus layers have a large tension stress along the fibers and also in the tangential peripheral direction. The inner annulus fibers have stresses of smaller magnitude. (Reproduced with permission of author and publisher.9)
Compression and Tension Stresses
Normal lumbar disk. Compression has been the focus of much of the past research done on the spine.13,27,28
In the normal lumbar disk, it is not herniation that is seen with high compressive loads, but failure of the vertebral body, resulting in collapsed cartilaginous end-plates.12,14 This type of collapsing demonstrates that, with direct, single axis compressive loading, as opposed to indirect or multiaxial loading, a spine with normal intervertebral disks is relatively strong. In the normal disk, a compressive load increases the internal pressure of the disk and stretches the annulus fibers.10,20 The resultant stresses are directed radially to the end-plates and annulus. The inner layers of the annulus are subjected to a small compressive stress, which is transferred to other vertebrae by the fluid pressures of the nucleus. The outer annulus layers are subjected to tensile stress without transference10 (Fig. 5). However, because of their alignment, the outer layers of annulus fibers are capable of absorbing the tensile stress. The magnitude of tensile stresses depends on the thickness of the annulus fibers. The
tensile stresses on the thinner, more parallel posterior fibers of the lumbar part of the spine are four to five times as great as the applied load.5,29
Degenerated lumbar disk. Under the same compressive load, the nucleus of a degenerated disk will not absorb some of the stress and transfer the remainder to the annulus and end-plates; instead, the increased load is distributed to the annulus. Under these circumstances the outer annulus fibers receive a large tensile stress without the fiber mechanism to absorb the stress or the hydrostatic nucleus to distribute the forces radially. Consequently, the inner fibers receive a large compressive stress10 (Fig. 6). Nachemson measured pressures in the nucleus pulposus of moderately degenerated disks and found these pressures to be 30 percent lower than pressure in a normal disk. This decreased pressure further causes a significant increase in the vertical load placed on the annulus in a degenerated disk.29
Bending and Torsion Stresses
Functional movement in the vertebral column is a combination of direct and indirect loading.5,9 In the
Fig. 6. Compression load in a degenerated disk. A. Load is transferred to annulus only, with no reaction of nucleus. B. Annulus fibers show outer layers are subjected to increased amount of tensile stress. The inner annulus fibers have a high compressive stress. (Reproduced with permission of author and publisher.9)
768 PHYSICAL THERAPY
spine the stresses most likely to produce trauma are bending and torsion, which reflect the combinations of shear, compression, and tension forces.5'9'26
Bending involves simultaneous tension, compression, and some shear stresses at different locations in the disk. Bending in forward flexion, lateral flexion, or extension of the spine results in a tensile stress on the convex side of the annulus and a compressive stress, caused by the body weight, on the concave side. The side of the annulus under tension stretches, while the side under compression bulges.5,9 When undergoing bending, a structure will have maximum stress at the outer surface24,25 (Fig. 7). In the vertebral column this means the outer peripheral surfaces of the annulus will be subjected to the highest tensile stresses on the convex side and the highest compressive stresses on the concave side.20,26
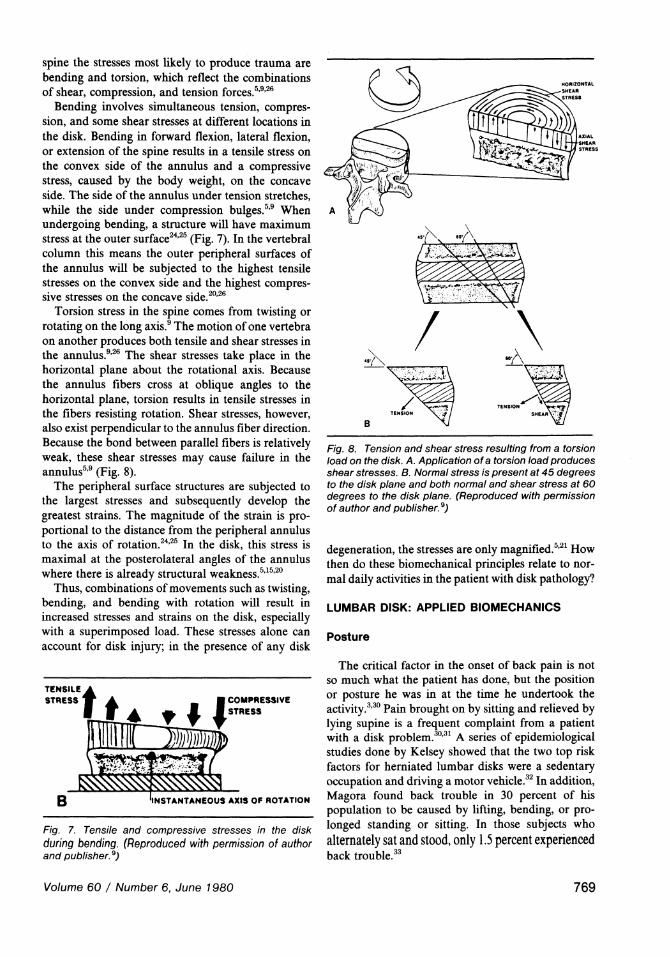
Torsion stress in the spine comes from twisting or rotating on the long axis.9 The motion of one vertebra on another produces both tensile and shear stresses in the annulus.9,26 The shear stresses take place in the horizontal plane about the rotational axis. Because the annulus fibers cross at oblique angles to the horizontal plane, torsion results in tensile stresses in the fibers resisting rotation. Shear stresses, however, also exist perpendicular to the annulus fiber direction. Because the bond between parallel fibers is relatively weak, these shear stresses may cause failure in the annulus5,9 (Fig. 8).
The peripheral surface structures are subjected to the largest stresses and subsequently develop the greatest strains. The magnitude of the strain is proportional to the distance from the peripheral annulus to the axis of rotation.24,25 In the disk, this stress is maximal at the posterolateral angles of the annulus where there is already structural weakness.5,15,20
Thus, combinations of movements such as twisting, bending, and bending with rotation will result in increased stresses and strains on the disk, especially with a superimposed load. These stresses alone can account for disk injury; in the presence of any disk
Fig. 7. Tensile and compressive stresses in the disk during bending. (Reproduced with permission of author and publisher.9)
Fig. 8. Tension and shear stress resulting from a torsion load on the disk. A. Application of a torsion load produces shear stresses. B. Normal stress is present at 45 degrees to the disk plane and both normal and shear stress at 60 degrees to the disk plane. (Reproduced with permission of author and publisher.9)
degeneration, the stresses are only magnified.5,21 How then do these biomechanical principles relate to normal daily activities in the patient with disk pathology?
LUMBAR DISK: APPLIED BIOMECHANICS
Posture
The critical factor in the onset of back pain is not so much what the patient has done, but the position or posture he was in at the time he undertook the activity.3,30 Pain brought on by sitting and relieved by lying supine is a frequent complaint from a patient with a disk problem.30,31 A series of epidemiological studies done by Kelsey showed that the two top risk factors for herniated lumbar disks were a sedentary occupation and driving a motor vehicle.32 In addition, Magora found back trouble in 30 percent of his population to be caused by lifting, bending, or prolonged standing or sitting. In those subjects who alternately sat and stood, only 1.5 percent experienced back trouble.33
Volume 60 / Number 6, June 1980 769
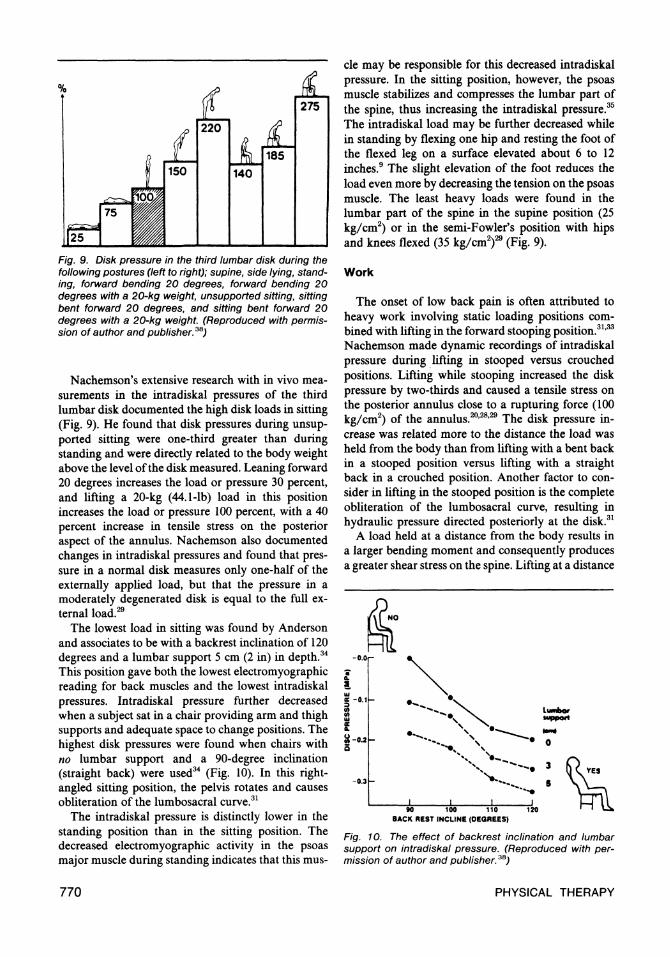
Fig. 9. Disk pressure in the third lumbar disk during the following postures (left to right); supine, side lying, standing, forward bending 20 degrees, forward bending 20 degrees with a 20-kg weight, unsupported sitting, sitting bent forward 20 degrees, and sitting bent forward 20 degrees with a 20-kg weight. (Reproduced with permission of author and publisher.38)
Nachemson's extensive research with in vivo measurements in the intradiskal pressures of the third lumbar disk documented the high disk loads in sitting (Fig. 9). He found that disk pressures during unsupported sitting were one-third greater than during standing and were directly related to the body weight above the level of the disk measured. Leaning forward 20 degrees increases the load or pressure 30 percent, and lifting a 20-kg (44.1-lb) load in this position increases the load or pressure 100 percent, with a 40 percent increase in tensile stress on the posterior aspect of the annulus. Nachemson also documented changes in intradiskal pressures and found that pressure in a normal disk measures only one-half of the externally applied load, but that the pressure in a moderately degenerated disk is equal to the full external load.29
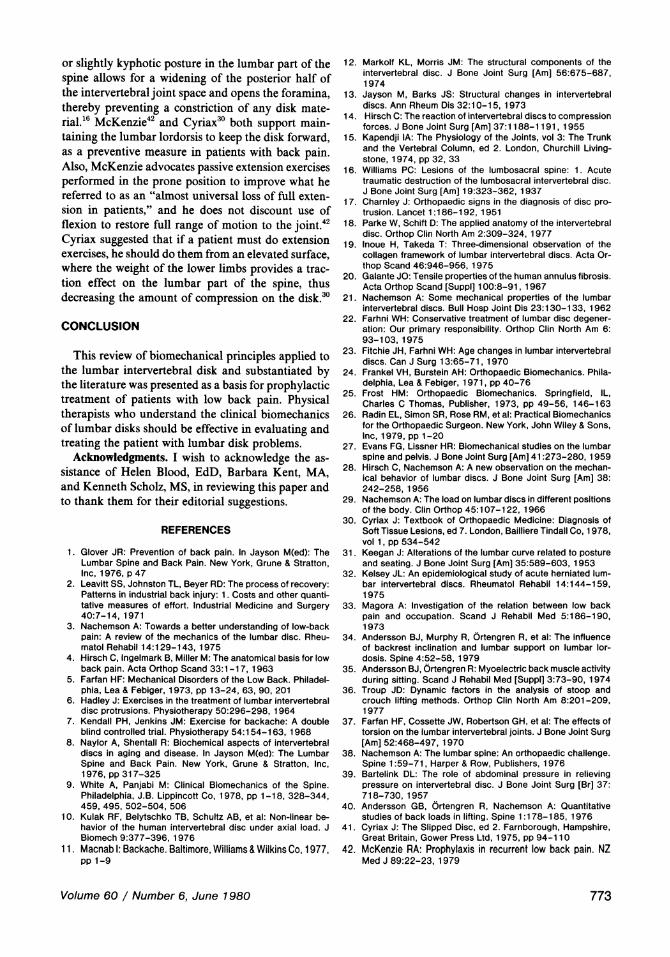
The lowest load in sitting was found by Anderson and associates to be with a backrest inclination of 120 degrees and a lumbar support 5 cm (2 in) in depth.34
This position gave both the lowest electromyographic reading for back muscles and the lowest intradiskal pressures. Intradiskal pressure further decreased when a subject sat in a chair providing arm and thigh supports and adequate space to change positions. The highest disk pressures were found when chairs with no lumbar support and a 90-degree inclination (straight back) were used34 (Fig. 10). In this right-angled sitting position, the pelvis rotates and causes obliteration of the lumbosacral curve.31
The intradiskal pressure is distinctly lower in the standing position than in the sitting position. The decreased electromyographic activity in the psoas major muscle during standing indicates that this mus
cle may be responsible for this decreased intradiskal pressure. In the sitting position, however, the psoas muscle stabilizes and compresses the lumbar part of the spine, thus increasing the intradiskal pressure.35
The intradiskal load may be further decreased while in standing by flexing one hip and resting the foot of the flexed leg on a surface elevated about 6 to 12 inches.9 The slight elevation of the foot reduces the load even more by decreasing the tension on the psoas muscle. The least heavy loads were found in the lumbar part of the spine in the supine position (25 kg/cm2) or in the semi-Fowler's position with hips and knees flexed (35 kg/cm2)29 (Fig. 9).
Work
The onset of low back pain is often attributed to heavy work involving static loading positions combined with lifting in the forward stooping position.31,33
Nachemson made dynamic recordings of intradiskal pressure during lifting in stooped versus crouched positions. Lifting while stooping increased the disk pressure by two-thirds and caused a tensile stress on the posterior annulus close to a rupturing force (100 kg/cm2) of the annulus.20,28,29 The disk pressure increase was related more to the distance the load was held from the body than from lifting with a bent back in a stooped position versus lifting with a straight back in a crouched position. Another factor to consider in lifting in the stooped position is the complete obliteration of the lumbosacral curve, resulting in hydraulic pressure directed posteriorly at the disk.31
A load held at a distance from the body results in a larger bending moment and consequently produces a greater shear stress on the spine. Lifting at a distance
Fig. 10. The effect of backrest inclination and lumbar support on intradiskal pressure. (Reproduced with permission of author and publisher.38)
770 PHYSICAL THERAPY
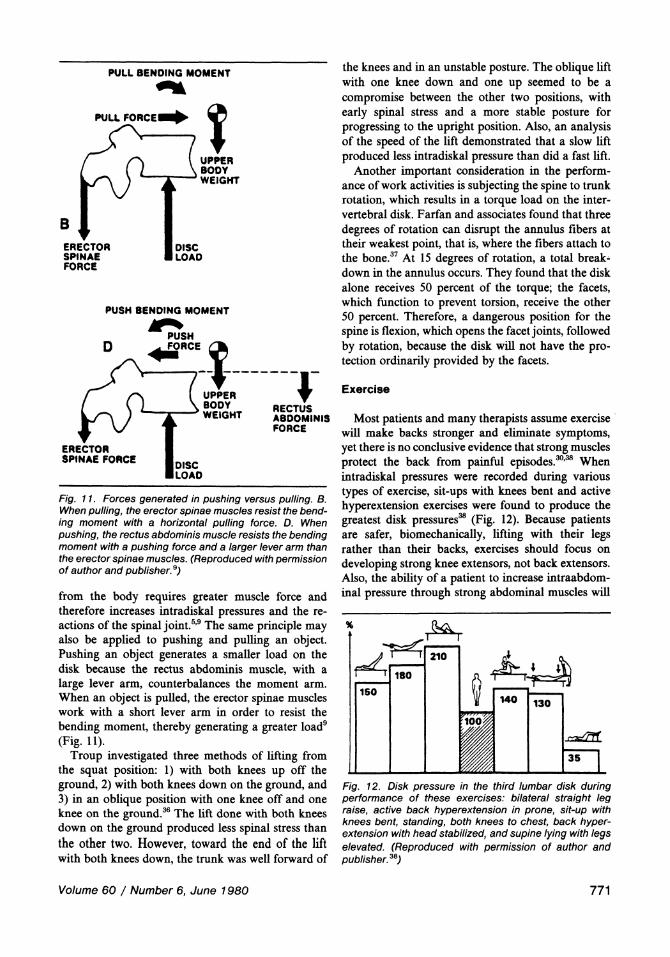
Fig. 11. Forces generated in pushing versus pulling. B. When pulling, the erector spinae muscles resist the bending moment with a horizontal pulling force. D. When pushing, the rectus abdominis muscle resists the bending moment with a pushing force and a larger lever arm than the erector spinae muscles. (Reproduced with permission of author and publisher.9)
from the body requires greater muscle force and therefore increases intradiskal pressures and the reactions of the spinal joint.5,9 The same principle may also be applied to pushing and pulling an object. Pushing an object generates a smaller load on the disk because the rectus abdominis muscle, with a large lever arm, counterbalances the moment arm. When an object is pulled, the erector spinae muscles work with a short lever arm in order to resist the bending moment, thereby generating a greater load9
(Fig. 11). Troup investigated three methods of lifting from
the squat position: 1) with both knees up off the ground, 2) with both knees down on the ground, and 3) in an oblique position with one knee off and one knee on the ground.36 The lift done with both knees down on the ground produced less spinal stress than the other two. However, toward the end of the lift with both knees down, the trunk was well forward of
the knees and in an unstable posture. The oblique lift with one knee down and one up seemed to be a compromise between the other two positions, with early spinal stress and a more stable posture for progressing to the upright position. Also, an analysis of the speed of the lift demonstrated that a slow lift produced less intradiskal pressure than did a fast lift.
Another important consideration in the performance of work activities is subjecting the spine to trunk rotation, which results in a torque load on the intervertebral disk. Farfan and associates found that three degrees of rotation can disrupt the annulus fibers at their weakest point, that is, where the fibers attach to the bone.37 At 15 degrees of rotation, a total breakdown in the annulus occurs. They found that the disk alone receives 50 percent of the torque; the facets, which function to prevent torsion, receive the other 50 percent. Therefore, a dangerous position for the spine is flexion, which opens the facet joints, followed by rotation, because the disk will not have the protection ordinarily provided by the facets.
Exercise
Most patients and many therapists assume exercise will make backs stronger and eliminate symptoms, yet there is no conclusive evidence that strong muscles protect the back from painful episodes.30,38 When intradiskal pressures were recorded during various types of exercise, sit-ups with knees bent and active hyperextension exercises were found to produce the greatest disk pressures38 (Fig. 12). Because patients are safer, biomechanically, lifting with their legs rather than their backs, exercises should focus on developing strong knee extensors, not back extensors. Also, the ability of a patient to increase intraabdominal pressure through strong abdominal muscles will
Fig. 12. Disk pressure in the third lumbar disk during performance of these exercises: bilateral straight leg raise, active back hyperextension in prone, sit-up with knees bent, standing, both knees to chest, back hyperextension with head stabilized, and supine lying with legs elevated. (Reproduced with permission of author and publisher.36)
Volume 60 / Number 6, June 1980 771

further decrease the intradiskal load and enhance lifting ability.39'40
PROPHYLAXIS
Back pain may be caused and aggravated by mechanical factors, especially by those factors related to posture. Increased emphasis on prophylaxis could well lead to a decrease in recurring back pain episodes. Physical therapists must first have a thorough understanding of applied biomechanics of the lumbar part of the spine, however, before establishing preventive programs.
Postural Activities
Sitting is a posture involved in most daily activities and many occupational situations. Obviously, when a patient is suffering from back pain, sitting for long periods of time should be avoided. If a patient must sit, proper lumbar support incorporating a back rest inclined slightly posteriorly relieves the intradiskal pressure. The level at which the support is placed is important. In order to have a maximum effect, the lumbar support should distribute the disk pressure over the largest possible area. The support must be able to vary in size and height. The seat should tilt back slightly to accommodate the buttocks, but be high enough from the floor to prevent excessive hip flexion and eliminate the lumbar concavity.9,41
The height of the seat should allow adequate thigh support, as well as comfortable placement of the patient's feet. The free space below the seat should allow for the placement of the feet beneath the seat in rising.31 Frequent change of position in sitting is important if the patient is to vary the compressive load on a degenerated disk. A chair with arm supports provides additional support and enhances the opportunity for changing positions.41
Although the sitting posture often makes performing manual tasks easier, two points must be remembered: frequent change of position to relieve the compressive stress and proper design of a chair as outlined above.
The patient must also be aware of what position he uses while lying down or sleeping, inasmuch as nearly one-third of a lifetime is spent in this position. Bending in a kyphotic posture for a prolonged period of time may cause excessive stress on the posterior aspect of the disk. A firm mattress that prevents a flexed posture is preferable. The firmness of the mattress supports the patient's spine. The patient should rise up out of bed by rolling to his side, swinging his legs over the side of the bed, and pushing up with his arms to a sitting position, instead of sitting up directly from the lying position and twisting the body.41
Work Activities
Lifting objects is an activity performed frequently in any working environment, whether it be domestic or industrial. The critical factor in lifting is to keep the load close to the body, which reduces the moment arm at the spinal joints and requires less muscle force, thereby decreasing the intradiskal pressures.9 The lift should be done with the legs, not the back. Just before lifting, a deep breath should be taken to increase the intrathoracic and intraabdominal pressure, which in turn reduces the disk pressure.39, 40 The load should remain close to the body in going from a flexed knee to an erect position. Once in the standing position, the load should be placed on the ilium, which transmits the weight to the lower extremity and bypasses the lumbar part of the spine. An alternate method of picking up an object from the floor is to maintain a straight back and flex from the hips, then remain standing on one leg, kick the other leg out straight back, and proceed to bend over to pick up the object.41
If an object must be moved, pushing is preferable to pulling.9 Any activity that requires lifting something and then rotating the spine, as in throwing an object, should be carefully done in two straight motions instead of a twisting motion. Loads should not be lifted suddenly, but smoothly.36 Work involving contact with the floor or ground should be done in a quadrupedal position. The use of tables at the proper height is essential. Patients with back pain should alter their work environment or, if alterations are not possible and back pain becomes chronic, pursue a different line of work.40, 41
Exercise
As mentioned previously, the most important muscle groups for using proper body mechanics are the quadriceps femoris and the abdominal muscles.9,30
Strong quadriceps femoris muscles are necessary for lifting a load in a crouched position with a straight back and bent legs. Strong abdominal muscles help decrease intradiskal pressures. Strengthening abdominal muscles isometrically is preferable to the commonly used sit-ups because the sit-up position causes a large increase in intradiskal pressure.29
The use of flexion, extension, or hyperextension exercises for disk reduction or prevention of recurrence of displacement is a highly controversial issue.16,30,42 The guiding factor in a therapist's administration of any exercise program for a patient with low back pain should be the therapist's reassessment of any change in that particular patient's signs and symptoms with the performance of the exercises. William's premise for flexion exercises is that a straight
772 PHYSICAL THERAPY
or slightly kyphotic posture in the lumbar part of the spine allows for a widening of the posterior half of the intervertebral joint space and opens the foramina, thereby preventing a constriction of any disk material.16 McKenzie42 and Cyriax30 both support maintaining the lumbar lordorsis to keep the disk forward, as a preventive measure in patients with back pain. Also, McKenzie advocates passive extension exercises performed in the prone position to improve what he referred to as an "almost universal loss of full extension in patients," and he does not discount use of flexion to restore full range of motion to the joint.42
Cyriax suggested that if a patient must do extension exercises, he should do them from an elevated surface, where the weight of the lower limbs provides a traction effect on the lumbar part of the spine, thus decreasing the amount of compression on the disk.30
CONCLUSION
This review of biomechanical principles applied to the lumbar intervertebral disk and substantiated by the literature was presented as a basis for prophylactic treatment of patients with low back pain. Physical therapists who understand the clinical biomechanics of lumbar disks should be effective in evaluating and treating the patient with lumbar disk problems.
Acknowledgments. I wish to acknowledge the assistance of Helen Blood, EdD, Barbara Kent, MA, and Kenneth Scholz, MS, in reviewing this paper and to thank them for their editorial suggestions.
REFERENCES
1. Glover JR: Prevention of back pain. In Jayson M(ed): The Lumbar Spine and Back Pain. New York, Grune & Stratton, Inc. 1976, p 47
2. Leavitt SS, Johnston TL, Beyer RD: The process of recovery: Patterns in industrial back injury: 1. Costs and other quantitative measures of effort. Industrial Medicine and Surgery 40:7-14, 1971
3. Nachemson A: Towards a better understanding of low-back pain: A review of the mechanics of the lumbar disc. Rheumatol Rehabil 14:129-143, 1975
4. Hirsch C, Ingelmark B, Miller M: The anatomical basis for low back pain. Acta Orthop Scand 33:1-17, 1963
5. Farfan HF: Mechanical Disorders of the Low Back. Philadelphia, Lea & Febiger, 1973, pp 13-24, 63, 90, 201
6. Hadley J: Exercises in the treatment of lumbar intervertebral disc protrusions. Physiotherapy 50:296-298, 1964
7. Kendall PH, Jenkins JM: Exercise for backache: A double blind controlled trial. Physiotherapy 54:154-163, 1968
8. Naylor A, Shentall R: Biochemical aspects of intervertebral discs in aging and disease. In Jayson M(ed): The Lumbar Spine and Back Pain. New York, Grune & Stratton, Inc. 1976, pp 317-325
9. White A, Panjabi M: Clinical Biomechanics of the Spine. Philadelphia, J.B. Lippincott Co, 1978, pp 1-18, 328-344, 459, 495, 502-504, 506
10. Kulak RF, Belytschko TB, Schultz AB, et al: Non-linear behavior of the human intervertebral disc under axial load. J Biomech 9:377-396, 1976
11. Macnab I: Backache. Baltimore, Williams & Wilkins Co, 1977, pp 1-9
12. Markolf KL, Morris JM: The structural components of the intervertebral disc. J Bone Joint Surg [Am] 56:675-687, 1974
13. Jayson M, Barks JS: Structural changes in intervertebral discs. Ann Rheum Dis 32:10-15, 1973
14. Hirsch C: The reaction of intervertebral discs to compression forces. J Bone Joint Surg [Am] 37:1188-1191, 1955
15. Kapendji IA: The Physiology of the Joints, vol 3: The Trunk and the Vertebral Column, ed 2. London, Churchill Livingstone, 1974, pp 32, 33
16. Williams PC: Lesions of the lumbosacral spine: 1. Acute traumatic destruction of the lumbosacral intervertebral disc. J Bone Joint Surg [Am] 19:323-362, 1937
17. Charnley J: Orthopaedic signs in the diagnosis of disc protrusion. Lancet 1:186-192, 1951
18. Parke W, Schift D: The applied anatomy of the intervertebral disc. Orthop Clin North Am 2:309-324, 1977
19. Inoue H, Takeda T: Three-dimensional observation of the collagen framework of lumbar intervertebral discs. Acta Orthop Scand 46:946-956, 1975
20. Galante JO: Tensile properties of the human annulus fibrosis. Acta Orthop Scand [Suppl] 100:8-91, 1967
21. Nachemson A: Some mechanical properties of the lumbar intervertebral discs. Bull Hosp Joint Dis 23:130-133, 1962
22. Farhni WH: Conservative treatment of lumbar disc degeneration: Our primary responsibility. Orthop Clin North Am 6: 93-103, 1975
23. Fitchie JH, Farhni WH: Age changes in lumbar intervertebral discs. Can J Surg 13:65-71, 1970
24. Frankel VH, Burstein AH: Orthopaedic Biomechanics. Philadelphia, Lea & Febiger, 1971, pp 40-76
25. Frost HM: Orthopaedic Biomechanics. Springfield, IL, Charles C Thomas, Publisher, 1973, pp 49-56, 146-163
26. Radin EL, Simon SR, Rose RM, et al: Practical Biomechanics for the Orthopaedic Surgeon. New York, John Wiley & Sons, Inc. 1979, pp 1-20
27. Evans FG, Lissner HR: Biomechanical studies on the lumbar spine and pelvis. J Bone Joint Surg [Am] 41:273-280, 1959
28. Hirsch C, Nachemson A: A new observation on the mechanical behavior of lumbar discs. J Bone Joint Surg [Am] 38: 242-258,1956
29. Nachemson A: The load on lumbar discs in different positions of the body. Clin Orthop 45:107-122, 1966
30. Cyriax J: Textbook of Orthopaedic Medicine: Diagnosis of Soft Tissue Lesions, ed 7. London, Bailliere Tindall Co, 1978, vol 1, pp 534-542
31. Keegan J: Alterations of the lumbar curve related to posture and seating. J Bone Joint Surg [Am] 35:589-603, 1953
32. Kelsey JL: An epidemiological study of acute herniated lumbar intervertebral discs. Rheumatol Rehabil 14:144-159, 1975
33. Magora A: Investigation of the relation between low back pain and occupation. Scand J Rehabil Med 5:186-190, 1973
34. Andersson BJ, Murphy R, Örtengren R, et al: The influence of backrest inclination and lumbar support on lumbar lordosis. Spine 4:52-58, 1979
35. Andersson BJ, Örtengren R: Myoelectric back muscle activity during sitting. Scand J Rehabil Med [Suppl] 3:73-90, 1974
36. Troup JD: Dynamic factors in the analysis of stoop and crouch lifting methods. Orthop Clin North Am 8:201-209, 1977
37. Farfan HF, Cossette JW, Robertson GH, et al: The effects of torsion on the lumbar intervertebral joints. J Bone Joint Surg [Am] 52:468-497, 1970
38. Nachemson A: The lumbar spine: An orthopaedic challenge. Spine 1:59-71, Harper & Row, Publishers, 1976
39. Bartelink DL: The role of abdominal pressure in relieving pressure on intervertebral disc. J Bone Joint Surg [Br] 37: 718-730, 1957
40. Andersson GB, Örtengren R, Nachemson A: Quantitative studies of back loads in lifting. Spine 1:178-185, 1976
41. Cyriax J: The Slipped Disc, ed 2. Farnborough, Hampshire, Great Britain, Gower Press Ltd, 1975, pp 94-110
42. McKenzie RA: Prophylaxis in recurrent low back pain. NZ Med J 89:22-23, 1979
Volume 60 / Number 6, June 1980 773
Related Documents