Biomarkers in Sepsis Utility or Futility? Dr Andrew Ferguson Consultant in Intensive Care Medicine and Anaesthesia Craigavon Area Hospital

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Biomarkers in SepsisUtility or Futility?
Dr Andrew FergusonConsultant in Intensive Care Medicine and Anaesthesia
Craigavon Area Hospital
Why give this your attention?• Microbes – the WMDs in your ICU• Sepsis is the main killer of general ICU patients
• Anything that helps you beat it is good news
• We need better diagnostic & prognostic tools
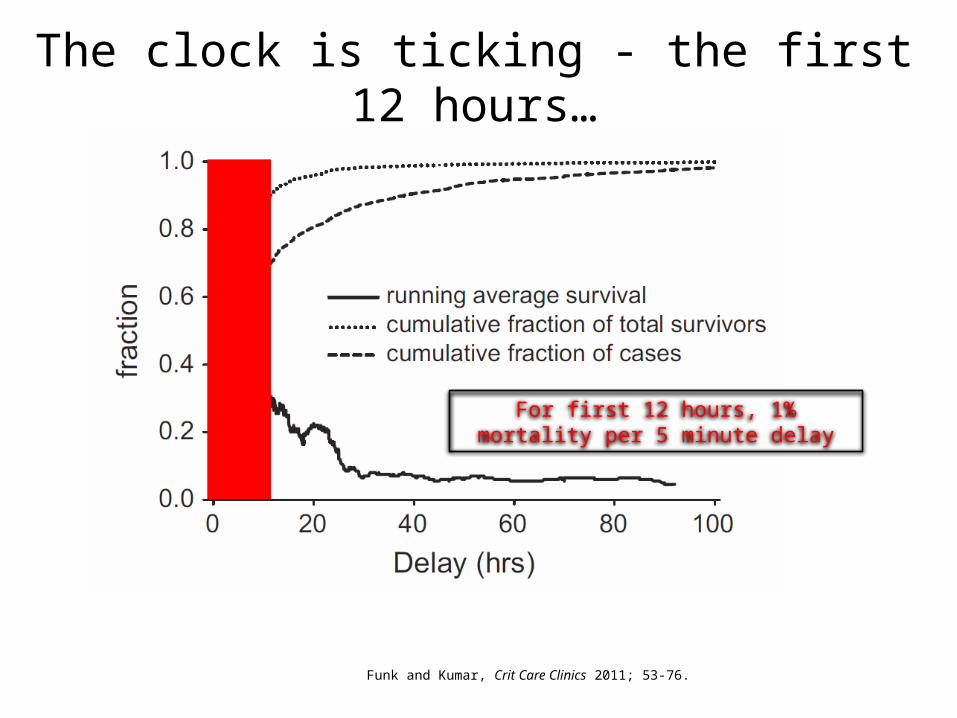
The clock is ticking - the first 12 hours…
Funk and Kumar, Crit Care Clinics 2011; 53-76.
For first 12 hours, 1% mortality per 5 minute delay
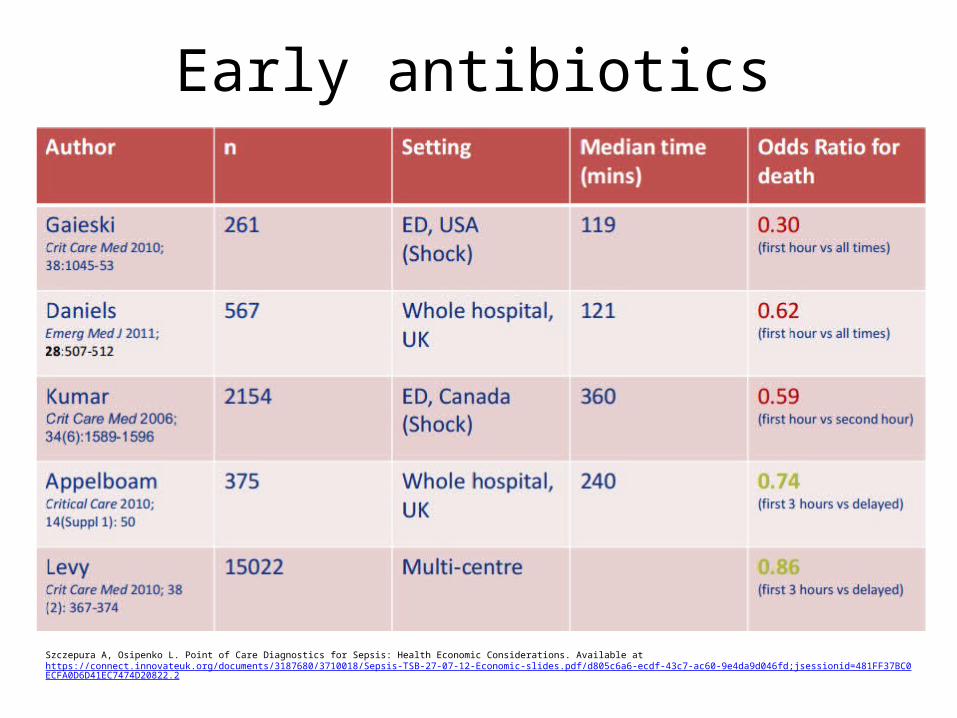
Early antibiotics
Szczepura A, Osipenko L. Point of Care Diagnostics for Sepsis: Health Economic Considerations. Available at https://connect.innovateuk.org/documents/3187680/3710018/Sepsis-TSB-27-07-12-Economic-slides.pdf/d805c6a6-ecdf-43c7-ac60-9e4da9d046fd;jsessionid=481FF37BC0ECFA0D6D41EC7474D20822.2

Early detection is paramount
BUT.…
Conventional detection of sepsis
• 2 main strategies…• Detection of bacterial pathogen
– Slow and all too often negative• Detection of host response
– NEWS for fever, tachycardia, tachypnoea– “Conventional” lab tests (WBC, CRP etc)– The ICU eyeball test
1
2
What’s wrong with that?• Physiological reserve determines presentation
• Physiological reserve determines trajectory• Misdiagnosis in patients with comorbidity• Recognition of severity is biased• Prognostication is weakened• There might not be an ICU eyeball

Enter the goose and the…
BIOMAR
KERS
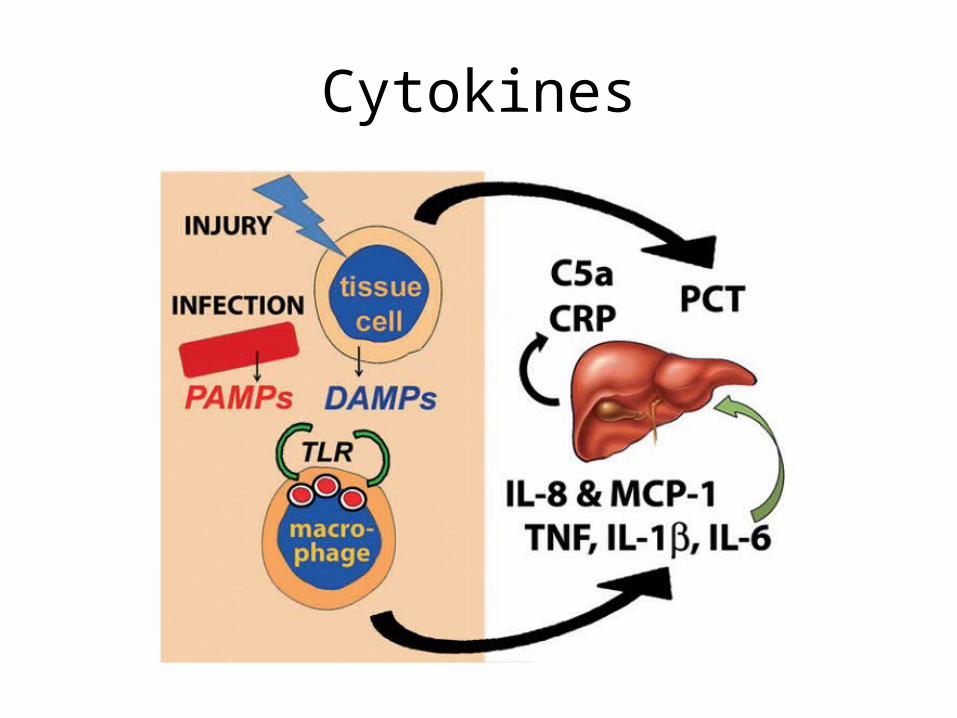
The biomarker paradigm…• Sepsis leads to
– Inflammation– Coagulation– Tissue damage and repair
• The sicker you are, the greater the changes• We can identify biomarkers for these processes
• We can measure these biomarkers• We can stratify severity based on biomarker levels
• We can prognosticate based on biomarker levels
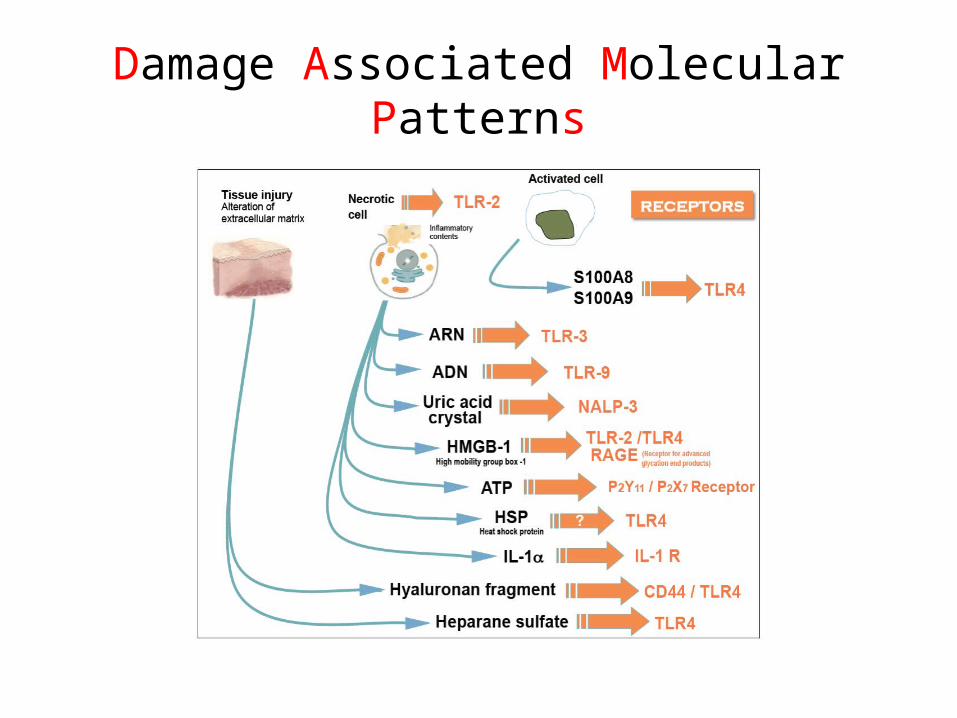
Damage Associated Molecular Patterns
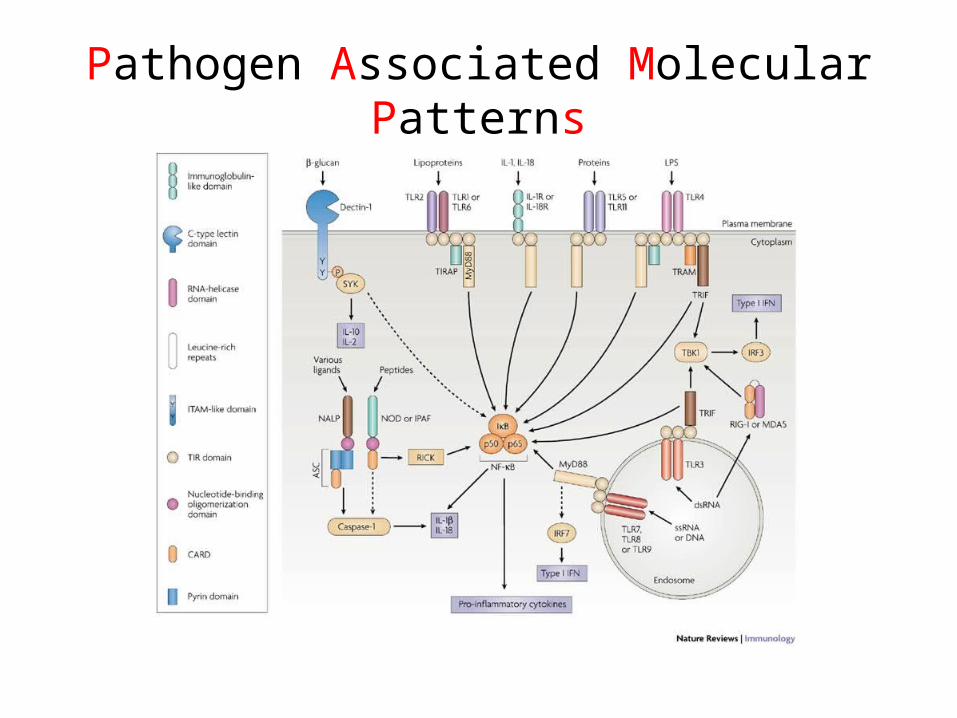
Pathogen Associated Molecular Patterns
Biomarker Candidates• Multiple, and growing all the time
• Some more common in the literature
• Linked to the main underlying processes– Inflammation– Coagulation– Tissue damage– Tissue repair
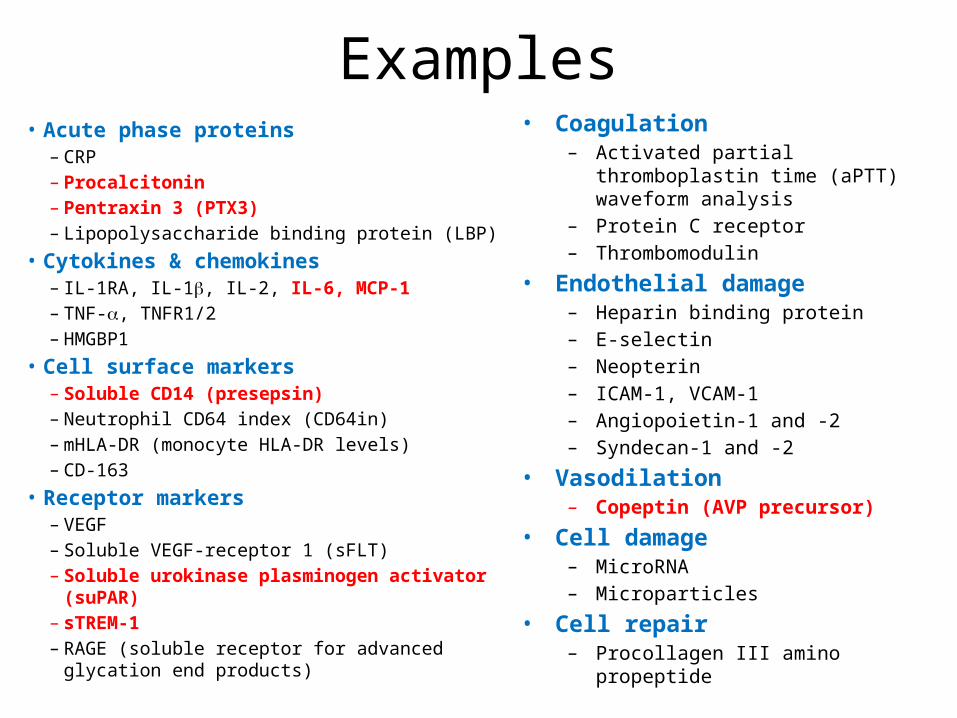
Examples• Acute phase proteins
– CRP– Procalcitonin– Pentraxin 3 (PTX3)– Lipopolysaccharide binding protein (LBP)
• Cytokines & chemokines– IL-1RA, IL-1b, IL-2, IL-6, MCP-1– TNF-a, TNFR1/2– HMGBP1
• Cell surface markers– Soluble CD14 (presepsin)– Neutrophil CD64 index (CD64in)– mHLA-DR (monocyte HLA-DR levels)– CD-163
• Receptor markers– VEGF– Soluble VEGF-receptor 1 (sFLT)– Soluble urokinase plasminogen activator (suPAR)
– sTREM-1– RAGE (soluble receptor for advanced glycation end products)
• Coagulation– Activated partial
thromboplastin time (aPTT) waveform analysis
– Protein C receptor– Thrombomodulin
• Endothelial damage– Heparin binding protein– E-selectin– Neopterin– ICAM-1, VCAM-1– Angiopoietin-1 and -2– Syndecan-1 and -2
• Vasodilation– Copeptin (AVP precursor)
• Cell damage– MicroRNA– Microparticles
• Cell repair– Procollagen III amino
propeptide
Questions to be answered
• Does the biomarker aid diagnosis?• Does it provide additional prognostic info?– For outcome– For progression/decline
• Better than the ICU eye?• Better than scoring systems?
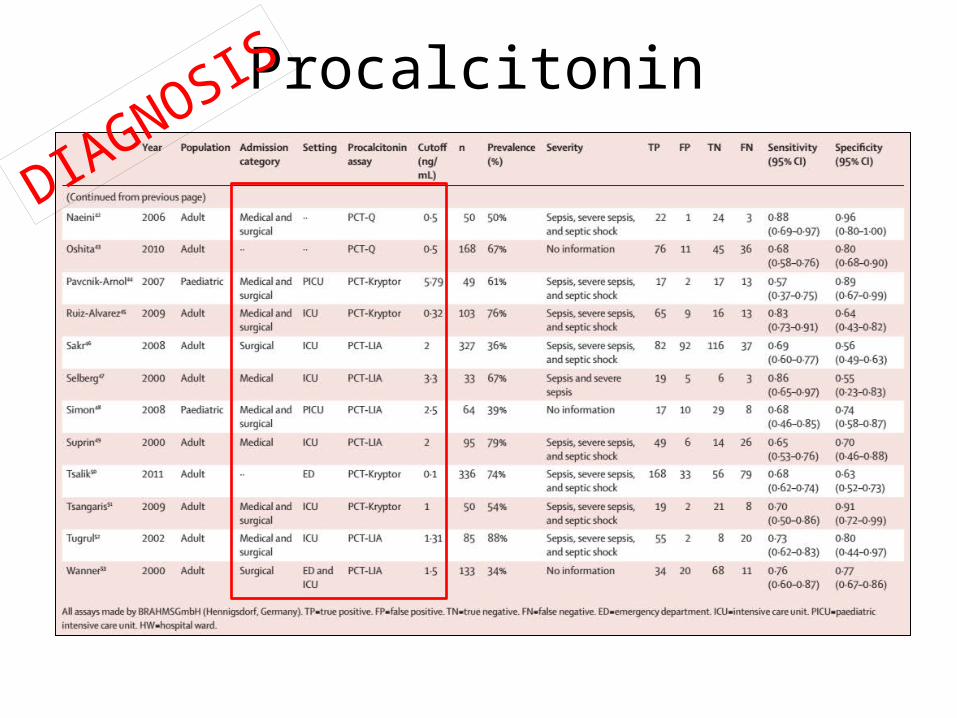
Procalcitonin• Bacterial infections
– > ubiqitous CALC-1 gene expression– > release of PCT from all parenchymal tissues
– Procalcitonin (PCT) increases after 2-3 hours after induction e.g. by endotoxin
– Falls with successful treatment
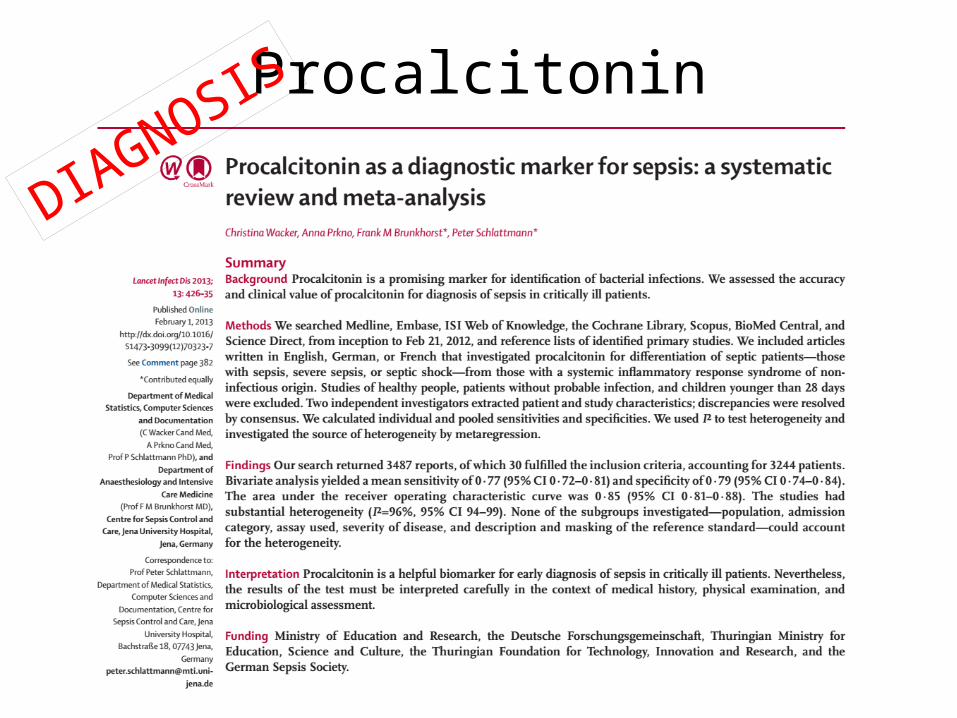
Procalcitonin
DIAGNO
SIS
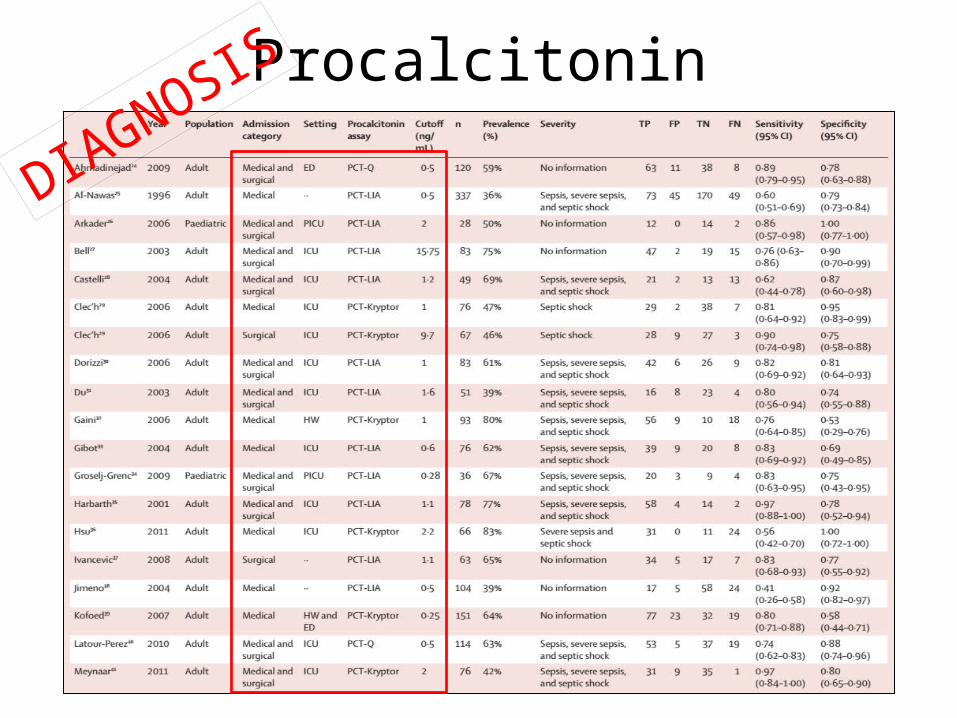
Procalcitonin
DIAGNO
SIS
ProcalcitoninDIA
GNOSIS
Procalcitonin
DIAGNO
SIS
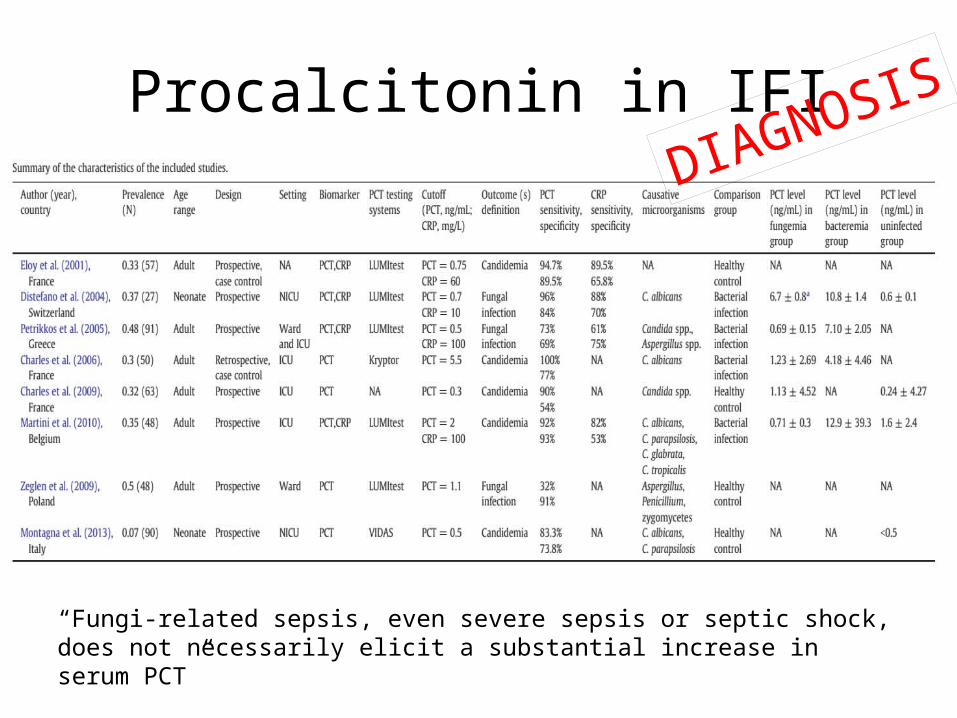
Procalcitonin in IFI
“Fungi-related sepsis, even severe sepsis or septic shock, does not necessarily elicit a substantial increase in serum PCT”
DIAGNOSIS
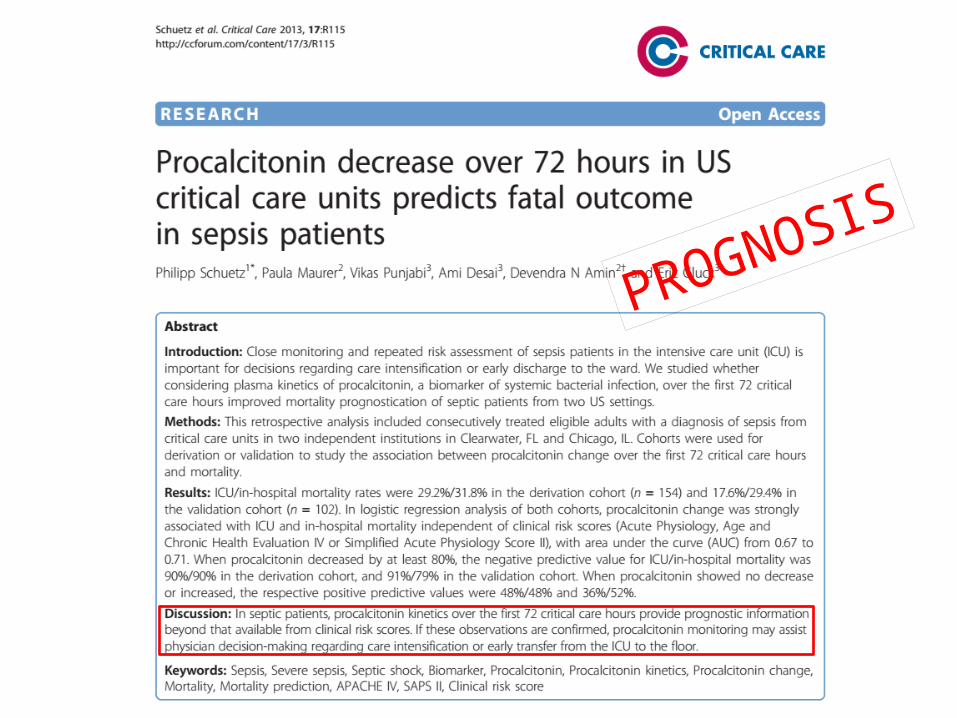
PROGNOSIS
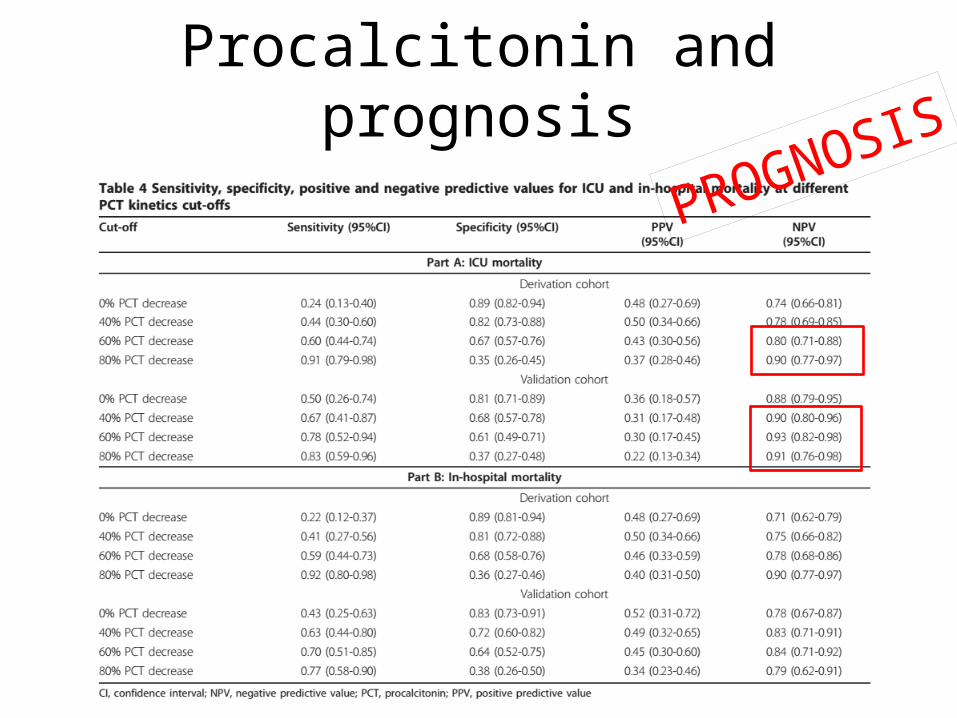
Procalcitonin and prognosis
PROGNOSIS
Where next?
Cytokines
Cytokines - IL-6• Can be reliably measured• Not specific for sepsis (hence
not diagnostic)• PROGNOSTIC tool
– Increased mortality as level rises– Increased risk of progression to severe sepsis/shock
Chemokines• IL-8• MCP-1 (monocyte chemoattractant protein 1)
• IL-8 can be used as diagnostic tool in sepsis
• MCP-1 can be used as PROGNOSTIC tool– Mortality risk
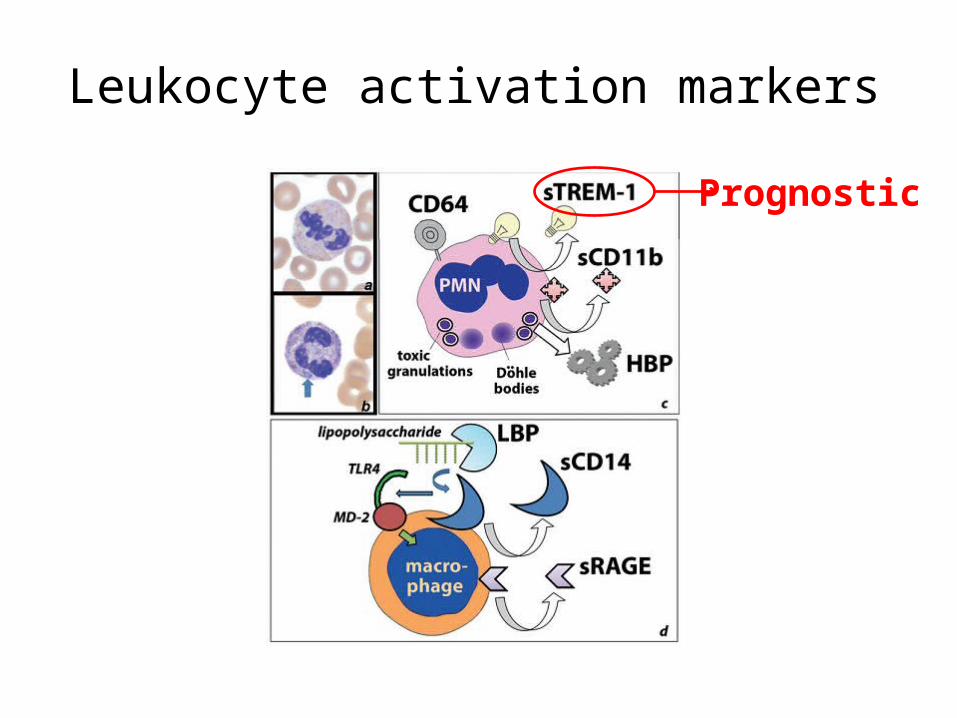
Leukocyte activation markers
Prognostic
Pentraxin 3• Pentraxins are liquid-phase PAMP receptors
• “Short” pentraxins include CRP (bet you didn’t know that!) as is serum amyloid P component (SAP)
• Pentraxin-3 involved in:– complement activation– pathogen opsonisation– self versus modified-self versus non-self discrimination
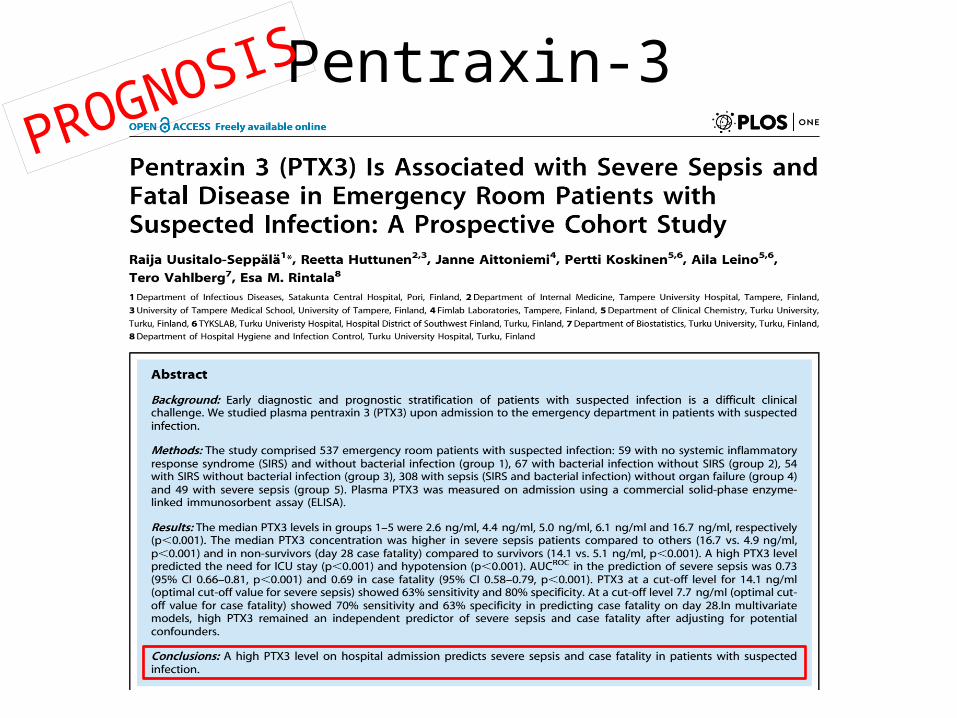
Pentraxin-3PROGN
OSIS
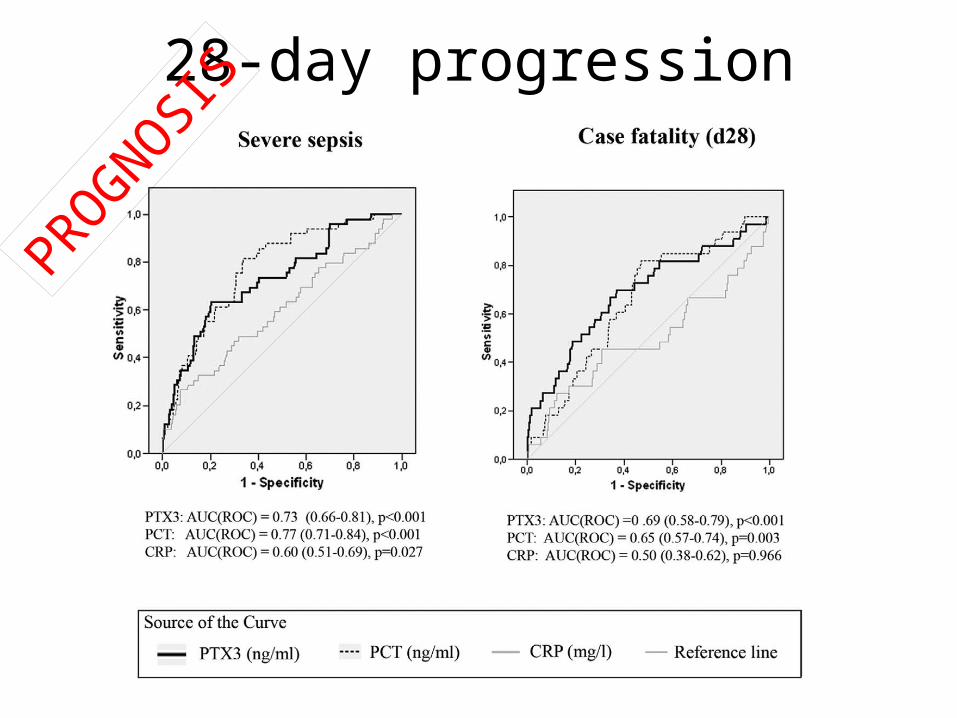
28-day progressionPROGNOSIS
DIAGNOSIS

PROGNOSIS
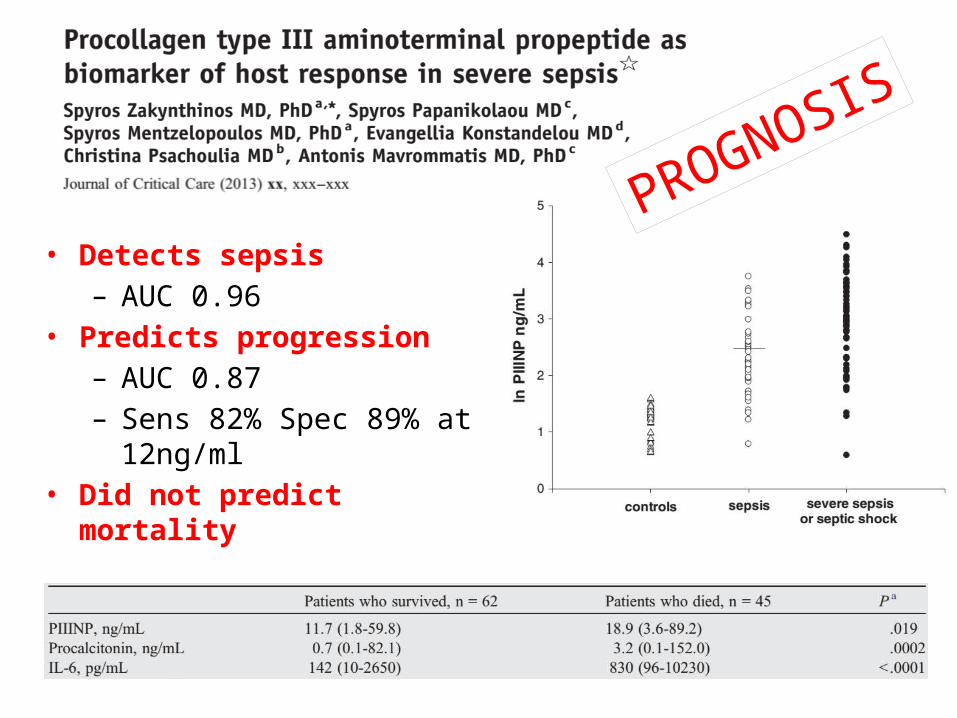
• Detects sepsis– AUC 0.96
• Predicts progression– AUC 0.87– Sens 82% Spec 89% at 12ng/ml
• Did not predict mortality
PROGNOSI
S
Is it really that simple?
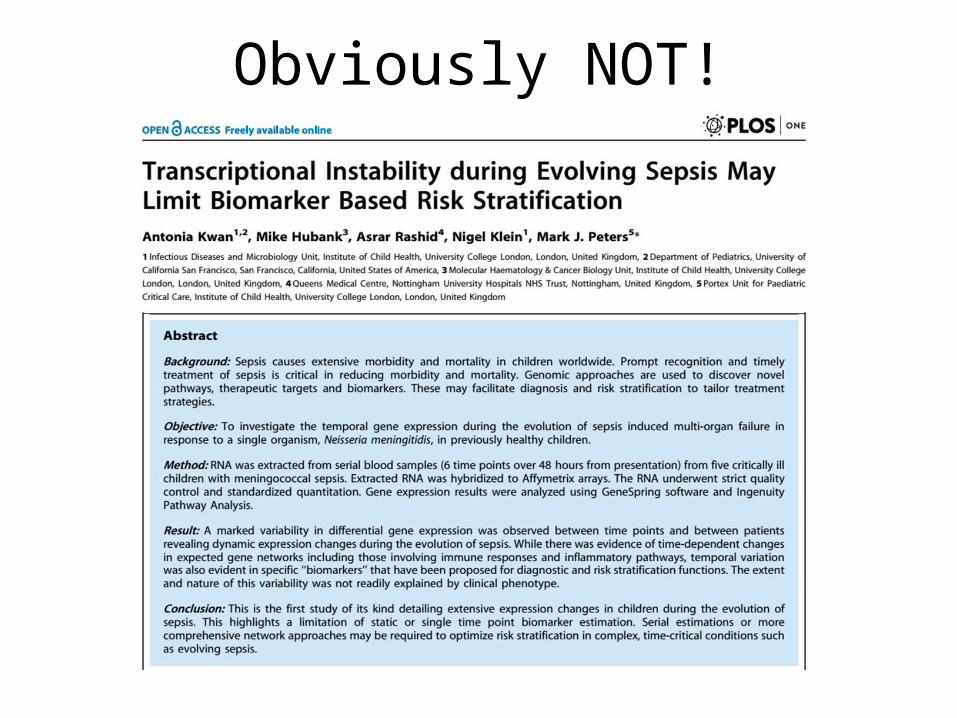
Obviously NOT!
The Future

Fatty acid b2 oxidation issue in non-survivors v survivors related to carnitine shuttle
(defective fatty acid transfer into mitochondria). Detectable at presentation.
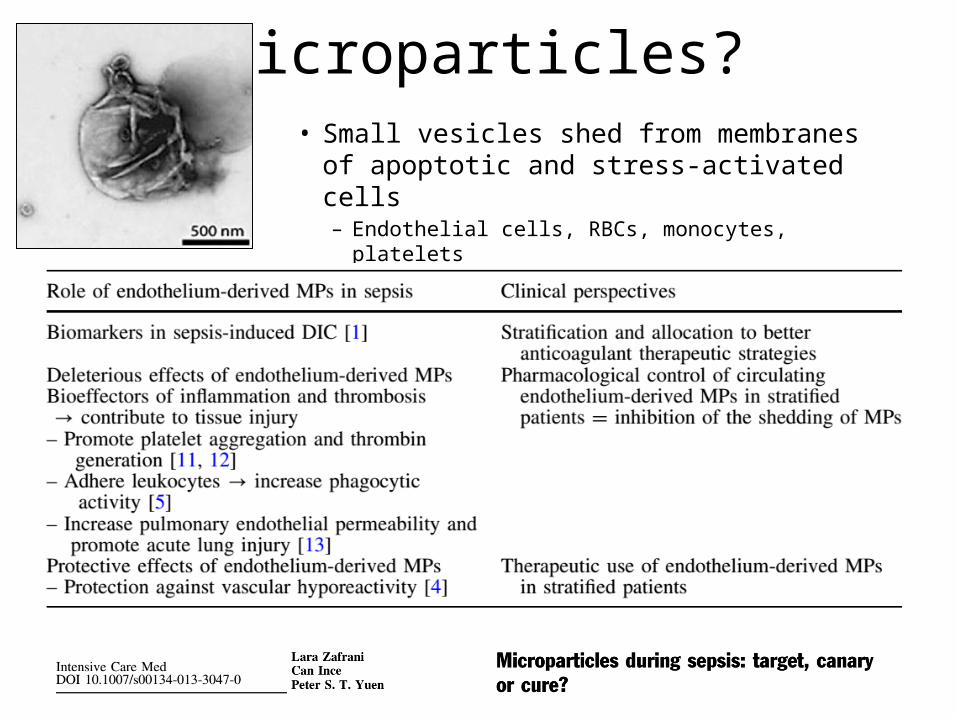
Microparticles?• Small vesicles shed from membranes of apoptotic and stress-activated cells– Endothelial cells, RBCs, monocytes, platelets
Conclusion• Utility• Earlier detection of disease• Earlier detection of high risk sub-groups
• Earlier recognition of treatment success
• Earlier de-escalation• Adjunctive prognostication
Thank you
Related Documents









![Review Article An Update on Sepsis Biomarkers...sequential organ failure assessment (SOFA) score [4], recommended for assessing organ dysfunction in sepsis criteria-3 [1], runs the](https://static.cupdf.com/doc/110x72/5f32800362b92645966bf002/review-article-an-update-on-sepsis-biomarkers-sequential-organ-failure-assessment.jpg)

