Bioequivalence Study Design Considerations Dr. John Gordon Prequalification of Medicines Programme: 2 nd Meeting with Medicine Manufacturers Geneva, April 5, 2011

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Bioequivalence
Study Design Considerations
Dr. John Gordon
Prequalification of Medicines Programme: 2nd Meeting with Medicine Manufacturers
Geneva, April 5, 2011

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 20112 |
Key Output of ProgrammeKey Output of Programme
� A list of prequalified medicinal products used for treatment of HIV/AIDS, malaria, tuberculosis, influenza, and for reproductive health
� To get a product included on the list, a manufacturer provides a comprehensive set of data about the quality, safety and efficacy of its product
� For most products (multisource or generic), this data set will include the results of in vivo bioequivalence tests (clinical trials conducted in healthy volunteers) as evidence of safety and efficacy

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 20113 |
BioequivalenceBioequivalence
Reference Test
Pharmaceutical Equivalent
Products
Possible Differences
Drug particle size, ..
Excipients
Manufacturing process
Equipment
Site of manufacture
Batch size ….
Documented Bioequivalence
= Therapeutic Equivalence

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 20114 |
GuidanceGuidance
“Multisource (generic)
pharmaceutical products: guidelines on registration
requirements to establish interchangeability". In: Fortieth
report of the WHO Expert
Committee on Specifications for
Pharmaceutical Preparations.
Geneva, World Health Organization. WHO Technical
Report Series, No. 937, 2006, Annex 7

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 20115 |
Establishing BioequivalenceEstablishing Bioequivalence
� Comparative pharmacokinetic studies– In vivo comparative bioavailability studies
– Comparison of performance of products based rate and extent of absorption of drug substance from each formulation
• Area under the concentration-time curve (AUC)
• Maximal concentration (Cmax)
• Time to maximal concentration (Tmax)
� Comparative pharmacodynamic studies
� Comparative clinical trials
� Comparative in vitro methods– Biopharmaceutics Classification System (BCS)-based biowaivers

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 20116 |
BCS-based BiowaiverBCS-based Biowaiver
� Eligibility for BCS-based Biowaiver
– General Notes on Biopharmaceutics Classification System
(BCS)-based Biowaiver Applications
� Requirements for BCS-based Biowaiver
– General Notes on BCS-based Biowaiver Applications
– Biopharmaceutics Classification System (BCS)-based
Biowaiver Applications: Anti-Tuberculosis Medicines

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 20117 |
In vivo BE Study
Design
In vivo BE Study
Design
Products being tested
�Comparator product
– WHO provides recommendations
– To be discussed by Dr. Welink
�Test product
– Biobatch of sufficient size
– Consistent with product proposed for market
Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 20118 |
In vivo BE Study
Design
In vivo BE Study
Design
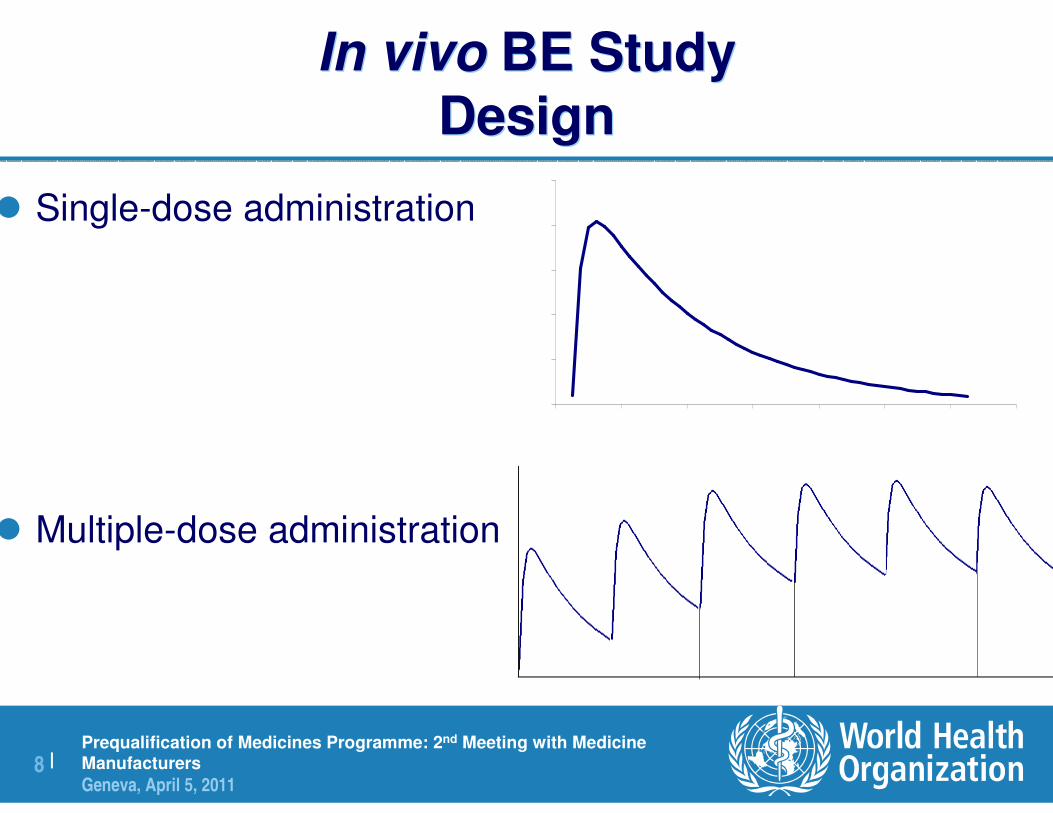
� Single-dose administration
� Multiple-dose administration
Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 20119 |
In vivo BE Study
Design
In vivo BE Study
Design
� Crossover Design– Each subject administered both test and comparator
– Within-subject comparison
– Preferred
� Parallel Design– Each subject administered test or comparator
– Between-subject comparison
– Only recommended for extremely long half-life drugs
– Consult WHO

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201110 |
Crossover DesignCrossover Design
� Blood samples are collected and assayed– Before and several times after drug administration. No need after 72 h
� Prior to period 2, pre-dose levels must be <5% of Cmax of 2nd period
� Wash out period must take into account the slow metabolizers
� Minimum wash out: 7 days (1 week)
Period 1 Period 2Wash out

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201111 |
In vivo BE Study
Design
In vivo BE Study
Design
� Crossover Design– Each subject administered both test and comparator
– Within-subject comparison
– Preferred
� Parallel Design– Each subject administered test or comparator
– Between-subject comparison
– Only recommended for extremely long half-life drugs
– Consult WHO

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201112 |
Drugs with long elimination t1/2: ParallelDrugs with long elimination t1/2: Parallel
� Normally wash-out period should not exceed 3-4 weeks
� If a larger wash-out period is necessary a parallel designmay be more appropriate
� Variability will be larger, needs higher sample size
– Parallel design: Total variability (intra+inter)
– Cross-over: Intra-subject variability
� Sampling: Up to 72 h
Group 2: Treatment B
Group 1: Treatment A
Randomization to treatments

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201113 |
In vivo BE Study
Design
In vivo BE Study
Design
� Administration of products under fasted or fed conditions?
� Fasted conditions
– Study conducted under fasted conditions the norm
– Comparator product labeling (SPC)
• Specifies fasted conditions
• Does not specify fasted/fed for administration
• States that either fasted or fed administration
� Fed conditions
– If specified in comparator product labeling (SPC)

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201114 |
In vivo BE Study
Design
In vivo BE Study
Design
Administration of products under fasted or fed conditions?
�Fed conditions
– If specified in comparator product labeling (SPC)
– Type of meal to be consumed
• high-fat, high-calorie meal
• “standard” or typical breakfast
�Administration under both fasted and fed conditions
– Not generally necessary for immediate-release products
– Required for modified-release products

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201115 |
Examples
HIV/AIDS Medicines
Examples
HIV/AIDS Medicines
� Nucleoside/Nucleotide Reverse Transcriptase Inhibitors
– Lamivudine
• Administration with respect to (wrt) food not specified
• Fasted
– Stavudine
• Maybe taken with or without food
• Fasted
– Zidovudine
• Administration with respect to (wrt) food not specified
• Fasted
– Note: as monocomponent products: BCS-based biowaiver

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201116 |
Examples
HIV/AIDS Medicines
Examples
HIV/AIDS Medicines
� Nucleoside/Nucleotide Reverse Transcriptase Inhibitors
– Didanosine (enteric-coated)
• Delayed-release formulation
• Two studies required: Fasted and fed conditions
– Tenofovir disoproxil fumarate
• US labeling of comparator: “The dose is one 300 mg tablet once daily
taken orally, without regard to food.”
• European labeling of comparator: “…(one tablet) once daily taken orally
with food.”
• Either accepted

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201117 |
Examples
HIV/AIDS Medicines
Examples
HIV/AIDS Medicines
� Non-Nucleoside Reverse Transcriptase Inhibitors
– Efavirenz
• Fed administration increases bioavailability but also increases adverse events
• Comparator labeling recommends administration on an empty stomach
• Fasted
– Nevirapine
• Administration with respect to (wrt) food not specified
• Fasted

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201118 |
Examples
HIV/AIDS Medicines
Examples
HIV/AIDS Medicines
� Protease Inhibitors
– Atazanavir
• Administration with food increases bioavailability and decreasesvariability
• Fed
– Ritonavir
• Administration with food improves absorption
• Fed
– Atazanavir / ritonavir combination
• Fed
• Standard breakfast

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201119 |
Examples
Tuberculosis Medicines
Examples
Tuberculosis Medicines
� First-line treatments
– Ethambutol
• Administration not affected by food
• Fasted
– Isoniazid
• Administration on an empty stomach
• Fasted
– Pyrazinamide
• Administration preferably without food
• Fasted
– Note: as monocomponent products: BCS-based biowaiver

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201120 |
Examples
Tuberculosis Medicines
Examples
Tuberculosis Medicines
� First-line treatments
– Rifampicin
• “It is recommended that oral rifampin be administered once daily, either 1 hour before or 2 hours after a meal with a full glass of water.”
• Fasted
� Second-line treatments
– Cycloserine
• Maybe taken with or without food
• Fasted

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201121 |
Examples
Tuberculosis Medicines
Examples
Tuberculosis Medicines
� Second-line treatments
– Levofloxacin
• Administration with respect to (wrt) food not specified
• Fasted
• Eligible for BCS-based biowaiver
– Ofloxacin
• “…should not be taken within two hours of magnesium/aluminium containing antacids, sucralfate, zinc or iron preparations…”
• Administration with respect to (wrt) food not specified
• Fasted
• Eligible for BCS-based biowaiver

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201122 |
Examples
Malaria Medicines
Examples
Malaria Medicines
� Artemisinin-based fixed dose oral combination
formulations
� Artemether + Lumefantrine
– Artemether
• Bioavailability increased when taken with food (x2)
– Lumefantrine
• Bioavailability increased when taken with food
– x16 increase with high fat meal
– x2 increase with lower fat meal
– Fed conditions (“standard” breakfast)

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201123 |
Examples
Malaria Medicines
Examples
Malaria Medicines
� Artemisinin-based fixed dose oral combination
formulations
� Artesunate + Amodiaquine
– Artesunate
• Bioavailability decreased when taken with food
– Amodiaquine
• Bioavailability increased when taken with high fat meal
– Labeling states “should not be taken with a high-fat meal”
– Fasted

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201124 |
Examples
Malaria Medicines
Examples
Malaria Medicines
� Artemisinin-based fixed dose oral combination or co-
blister formulations
� Artesunate + Mefloquine
– Artesunate
• Bioavailability decreased when taken with food
– Mefloquine
• Bioavailability increased when taken with food (40%)
• Labeling states “Should not be taken on an empty stomach”
– Fed
– “Standard” breakfast, not high-fat meal

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201125 |
Examples
Reproductive Health Medicines
Examples
Reproductive Health Medicines
� Oral hormonal contraceptives
� Ethinyl estradiol + levonorgestrel
– Administration with respect to (wrt) food not specified
– Fasted

Prequalification of Medicines Programme: 2nd Meeting with Medicine
Manufacturers
Geneva, April 5, 201126 |
Typical DesignTypical Design
� Single-dose administration
� Cross-over (within-subject) comparison
� Administration with or without food– Fasted study is the norm
– Labeling of the comparator product is the guide
• Bioavailability / pharmacokinetics
• Adverse events
� Consultation with Programme encouraged
Related Documents











