Enzymatic cascade system Biochemistry Assignment 2008 Prepared by: Nirajan Neupane B.Sc. Biotechnology 4 th semester Sann Int’l College Gairidhara, Kathmandu Submitted to: Anup Sharma Department of Biotechnology Sann Int’l College

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 1/27
Enzymatic cascade systemBiochemistry Assignment 2008
Prepared by:
Nirajan Neupane
B.Sc. Biotechnology 4th semester
Sann Int’l College
Gairidhara, Kathmandu
Submitted to:
Anup Sharma
Department of Biotechnology
Sann Int’l College
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 2/27
Gairidhara, Kathmandu
Acknowledgements
Enzymatic cascade system is one of the most understood and most interesting
biochemical systems. I feel myself very much providential to prepare an
assignment in cascade system, illustrating the blood coagulation mechanism.
I am very much thankful to Mr. Anup Sharma for providing me the opportunity to
write this assignment on “Enzymatic cascade system”.
In same way I am very much thankful to my friends and all my teachers who
cordially helped me to complete this assignment.
Nirajan Neupane
December 23rd, 2008
2
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 3/27
Contents
• Introduction to enzymatic cascade system……………….4
• The Blood Coagulation cascade system………………….6
• Three types of thrombi…………………………………...7• Platelet activation………………………………………...8
• The coagulation cascade………………………………….9
• Tissue factor pathway…………………………………...10
• Contact activation pathway……………………………...10
• Final common pathway……………………………….....10• The intrinsic pathway lead to the activation
of factor X………………………………………………..13
• The extrinsic pathway also leads to the activation
of factor X but by a different mechanism………………...14
• Final common pathway leads to the activation of
Prothrombin to thrombin………………………………....15
• Conversion of fibrinogen to fibrin is catalyzed by
Thrombin…………………………………………………16• Cofactors of blood coagulation…………………………...17
• Regulators of blood coagulation………………………….18
• Activity of Antithrombin Ш……………………………...19
• Fibrin clots are dissolved by Plasmin…………………….20
• Endothelial cells synthesize prostacyclin & other
compounds that affect clotting & thrombosis…………….21
• Aspirin is an effective antiplatelet drug…………………...21
• Testing of coagulation…………………………………….22
• Advantages of cascade system…………………………….23
• Conclusion………………………………………………...24
• References…………………………………………………25
3
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 4/27
Introduction to enzymatic cascade system
A biochemical cascade is a series of chemical reactions in which the products of
one reaction are consumed in the next reaction. The effect of a regulated change
in the activity of an enzyme is often amplified through a cascade mechanism. Thefirst enzyme acts on a second enzyme, the second on a third, etc. The effect is to
rapidly create a large amount of the active form of the last enzyme in the series.
There are several important biochemical cascade reactions in biochemistry,
including the enzymatic cascades, such as the coagulation cascade and the
complement system, and the signal transduction cascades which ultimately cause
electric potentials to travel through nerves into the brain where they are
interpreted as signals in such events as vision and smell.Elaborate cascades
initiate the clotting of blood and the action of the protective complement system.Cascades systems are involved in controlling transcription and in the regulation of
mammalian pyruvate dehydrogenase, 3-hydroxy-3-methylglutaryl- CoA
reductase and eicosanoids, and glutamine synthetase.
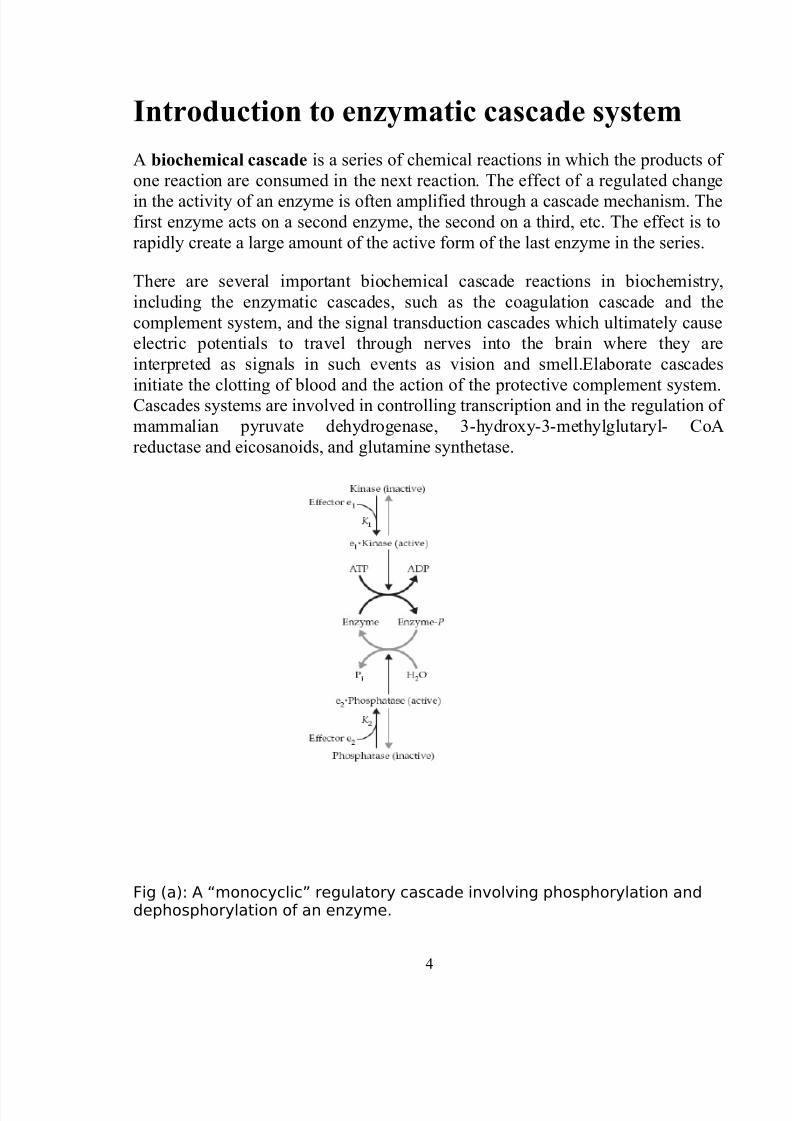
Fig (a): A “monocyclic” regulatory cascade involving phosphorylation anddephosphorylation of an enzyme.
4
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 5/27
Simple cascade mechanisms, such as the one shown in Fig.(a),
can provide a more flexible response to allosteric effectors (such as e1 in the
figure) than if the effector acted directly on the enzyme rather than on the protein
kinase. The cascade also provides amplification. This is especially true if
additional cycles are added. A response can result from the binding of only a
small number of hormone molecules to a receptor in a cell membrane or from
activation of only a few molecules of a protease in the initiation of blood clotting.
Enzymatic cascades are often employed in biochemical systems to achieve a rapid
response. In a cascade, an initial signal institutes a series of steps, each of which
is catalyzed by an enzyme. At each step, the signal is amplified. For instance, if a
signal molecule activates an enzyme that in turn activates 10 enzymes and each of
the 10 enzymes in turn activates 10 additional enzymes, after four steps the
original signal will have been amplified 10,000-fold.
A striking amplification occurs in visual responses. Under appropriate conditions
a single quantum of light falling on a receptor cell in the retina of an eye can
initiate a nerve impulse. The latter requires the flow of a large number of Na+ ions
across the plasma membrane. It would be hard to imagine how absorption of one
quantum could initiate a photochemical reaction leading to that much sodium
transport without intermediate amplification stages.
Another advantage of cascades is that they may provide ultrasensitive
responses. Not only can a response be sensitive to a higher power than the first of
the concentration of a signaling molecule but also the amplification provided by
the cascade confers a high sensitivity to the response.
Cascade systems also provide for response to more than one allosteric stimulus in
a single pathway. Glycogen catabolism can be initiated in more than one way.
Two pathways are known for initiation of both blood clotting and activation of
the complement system. Many pathways activate the MAP kinase pathway.
5
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 6/27
The Blood Coagulation cascade system
Coagulation is a complex process by which blood forms clots. It is an
important part of hemostasis (the cessation of blood loss from a damaged vessel)whereby a damaged blood vessel wall is covered by a platelet and fibrin
containing clot to stop bleeding and begin repair of the damaged vessel. Disorders
of coagulation can lead to an increased risk of bleeding (hemorrhage) and/or
clotting (thrombosis). Coagulation is highly conserved throughout biology; in all
mammals, coagulation involves both a cellular (platelet) and a protein
(coagulation factor) component. The system in humans has been the most
extensively researched and therefore is the best understood.
Coagulation begins almost instantly after an injury to the blood vessel hasdamaged the endothelium (lining of the vessel). Platelets immediately form a plug
at the site of injury; this is called primary hemostasis. Secondary hemostasisoccurs simultaneously: proteins in the blood plasma, called coagulation factors or
clotting factors, respond in a complex cascade to form fibrin strands which
strengthen the platelet plug.
Hemostasis and thrombosis encompass blood clotting(coagulation) and involve blood vessels, platelet aggregation,and plasma proteins that cause formation or dissolution of
platelet aggregates.In hemostasis, there is initial vasoconstriction of the injuredvessel, causing diminished blood flow distal to the injury. Thenhemostasis and thrombosis share three phases:1. Formation of a loose and temporary platelet aggregate at thesite of injury. Platelets bind to collagen at the site of vessel wallinjury and are activated by thrombin (the mechanism of activation of platelets is described below), formed in thecoagulation cascade at the same site, or by ADP released from
other activated platelets. Upon activation, platelets changeshape and, in the presence of fibrinogen, aggregate to form thehemostatic plug (in hemostasis) or thrombus (in thrombosis).
2. Formation of a fibrin mesh that binds to the plateletaggregate, forming a more stable hemostatic plug or thrombus.
6
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 7/27
3. Partial or complete dissolution of the hemostatic plug orthrombus by plasmin.
Three types of thrombi
Based on the fibrin proportions, thrombi are categorized intothree groups:
(1) The white thrombus is composed of platelets and fibrin andis relatively poor in erythrocytes. It forms at the site of an injuryor abnormal vessel wall, particularly in areas where blood flow israpid (arteries).
(2) The red thrombus consists primarily of red cells and fibrin. Itmorphologically resembles the clot formed in a test tube andmay form in vivo in areas of retarded blood flow or stasis (eg,veins) with or without vascular injury, or it may form at a site of injury or in an abnormal vessel in conjunction with an initiatingplatelet plug.
(3) A third type is a disseminated fibrin deposit in very smallblood vessels or capillaries.
7
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 8/27
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 9/27
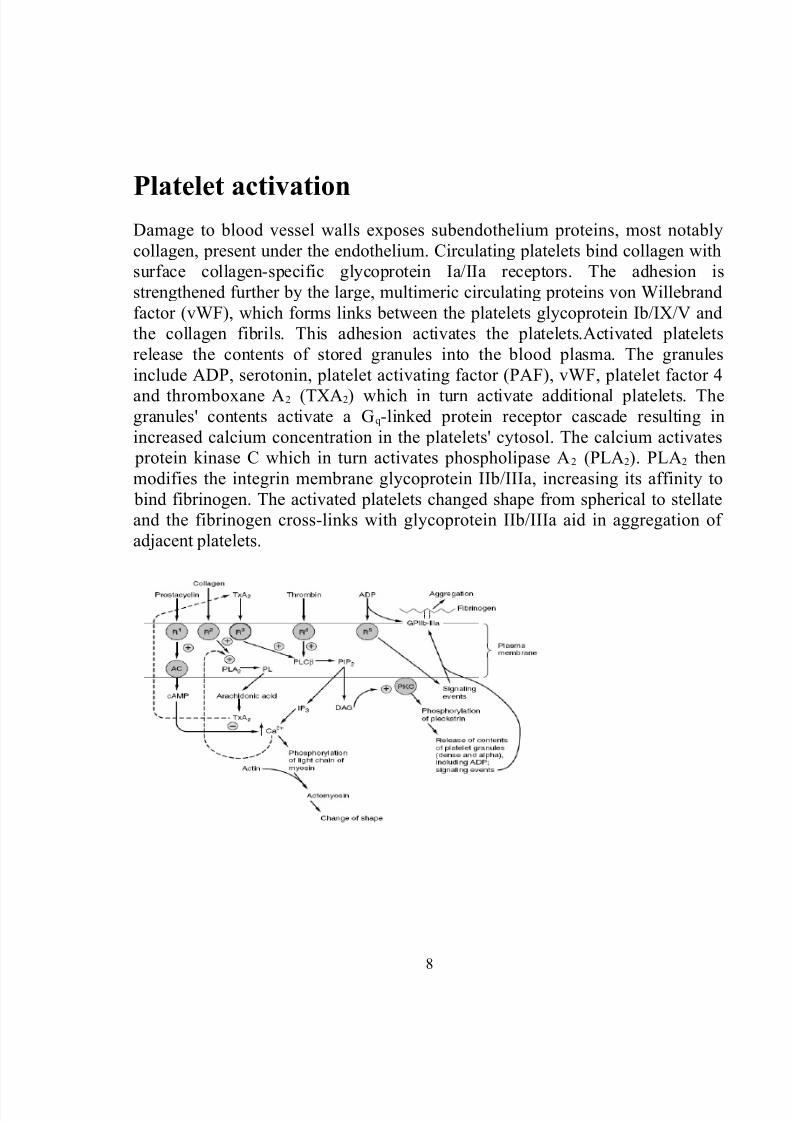
Fig: Platelet activation. The external environment, the plasma membrane, and the inside of a platelet are depicted from top to bottom. Thrombin and collagen are the two mostimportant platelet activators. ADP is considered a weak agonist; it causes aggregation butnot granule release. (GP, glycoprotein; R1–R5, variousreceptors; AC, adenylyl cyclase;
PLA2, phospholipase A2; PL, phospholipids; PLC®, phospholipase C®; PIP2,phosphatidylinositol 4,5-bisphosphate; cAMP, cyclic AMP; PKC, protein kinase C; TxA2,
thromboxane A2; IP3, inositol 1,4,5-trisphosphate; DAG, 1,2-diacylglycerol.
The coagulation cascade
The coagulation cascade of secondary hemostasis has two pathways, the contact activation pathway (formerly known as the intrinsic pathway) and the tissue
factor pathway (formerly known as the extrinsic pathway) that lead to fibrinformation. It was previously thought that the coagulation cascade consisted of
two pathways of equal importance joined to a common pathway. It is now knownthat the primary pathway for the initiation of blood coagulation is the tissue
factor pathway. The pathways are a series of reactions, in which a zymogen of a
serine protease and its glycoprotein co-factor are activated to become active
components that then catalyze the next reaction in the cascade, ultimately
resulting in cross-linked fibrin. Coagulation factors are generally indicated by
Roman numerals, with a lowercase a appended to indicate an active form.
The coagulation factors are generally serine proteases. There are some
exceptions. For example, FVIII and FV are glycoproteins and Factor XIII is a
transglutaminase. Serine proteases act by cleaving other proteins at specific sites.The coagulation factors circulate as inactive zymogens.
The coagulation cascade is classically divided into three pathways. The tissue factor and contact activation pathways both activate the "final common pathway"
of factor X, thrombin and fibrin.
Initiation of the fibrin clot in response to tissue injury is carriedout by the extrinsic pathway. How the intrinsic pathway isactivated in vivo is unclear, but it involves a negatively chargedsurface. The intrinsic and extrinsic pathways converge in a finalcommon pathway involving the activation of prothrombin tothrombin and the thrombin-catalyzed cleavage of fibrinogen toform the fibrin clot. The intrinsic, extrinsic, and final commonpathways are complex and involve many different proteins.
9
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 10/27
Tissue factor pathway (extrinsic pathway)
The intrinsic clotting pathway is activated by exposure of anionic surfaces on
rupture of the endothelial lining of the blood vessels. These surfaces serve as
binding sites for factors in the clotting cascade. Substances that are released from
tissues as a consequence of trauma to them trigger the extrinsic clotting pathway.
• Contact activation pathway (intrinsic
pathway)
The contact activation pathway begins with formation of the primary complex on
collagen by high-molecular weight kininogen (HMWK), prekallikrein, and FXII
(Hageman factor). Prekallikrein is converted to kallikrein and FXII becomes
FXIIa. FXIIa converts FXI into FXIa. Factor XIa activates FIX, which with its
co-factor FVIIIa form the tenase complex, which activates FX to FXa. The minor role that the contact activation pathway has in initiating clot formation can be
illustrated by the fact that patients with severe deficiencies of FXII, HMWK, and
prekallikrein do not have a bleeding disorder.
• Final common pathway
Thrombin has a large array of functions. Its primary role is the conversion of fibrinogen to fibrin, the building block of a hemostatic plug. In addition, it
activates Factors VIII and V and their inhibitor protein C (in the presence of
thrombomodulin), and it activates Factor XIII, which forms covalent bonds that
crosslink the fibrin polymers that form from activated monomers.
10
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 11/27
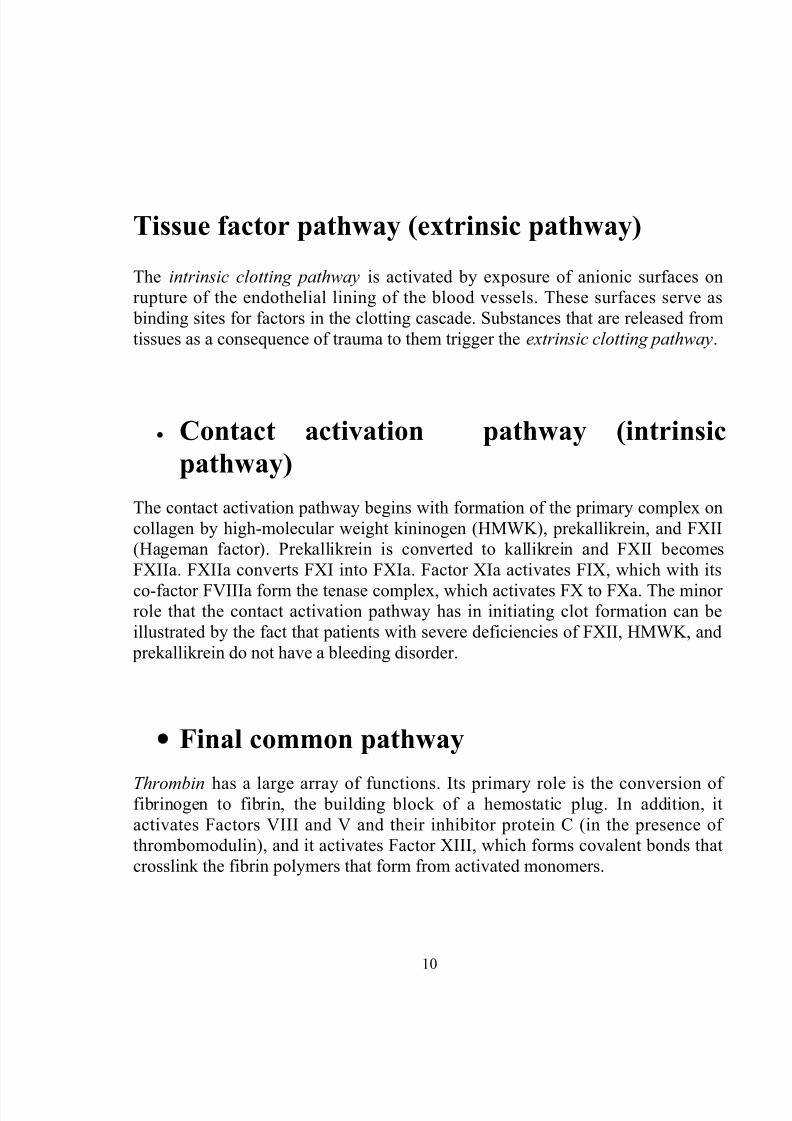
Following activation by the contact factor or tissue factor pathways the
coagulation cascade is maintained in a prothrombotic state by the continued
activation of FVIII and FIX to form the tenase complex, until it is down-regulated
by the anticoagulant pathways.The two pathways interact with each other in vivo.
Indeed, both are needed for proper clotting, as evidenced by clotting disorders
caused by a deficiency of a single protein in one of the pathways.
11

8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 12/27
Fig: The pathways of blood coagulation. The intrinsic and extrinsic pathwaysare indicated. The events depicted below factor Xa are designated the finalcommon pathway, culminating in the formation of cross-linked fibrin. Newobservations (dotted arrow) include the finding that complexes of tissuefactor and factor VIIa activate not only factor X (in the classic extrinsic
pathway) but also factor IX in the intrinsic pathway. In addition, thrombinand factor Xa feedback-activate at the two sites indicated (dashed arrows).
Table (a): Numerical system for nomenclatureof blood clotting factors. The numbers indicatethe order in which the factors have beendiscovered and bear no relationship to the order
12
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 13/27
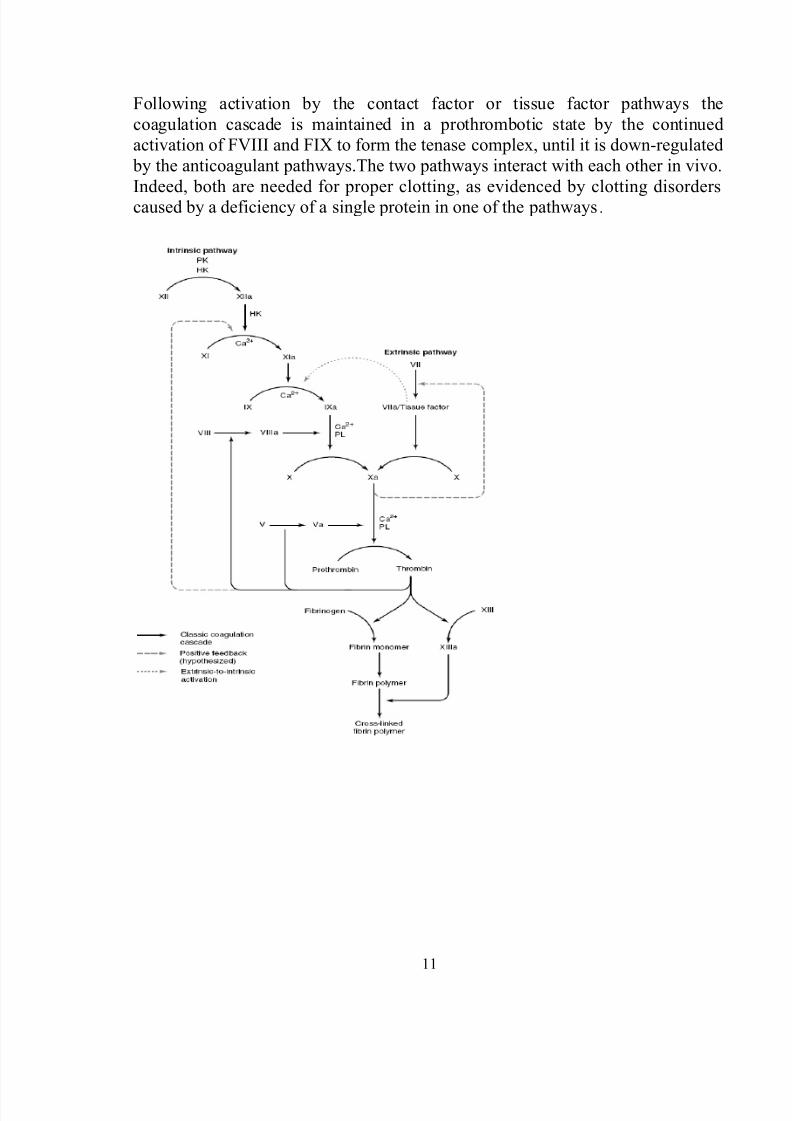
Table (b): The functions of theproteins involved in bloodcoagulation.
The intrinsic pathway leads to the activation of
Factor X
The intrinsic pathway involves factors XII, XI, IX, VIII, and X aswell as prekallikrein, highmolecular- weight (HMW) kininogen,Ca2+, and platelet phospholipids. It results in the production of factor Xa (by convention, activated clotting factors are referredto by use of the suffix a). This pathway commences with the“contact phase” in which prekallikrein, HMW kininogen, factorXII, and factor XI are exposed to a negatively charged activatingsurface. In vivo, the proteins probably assemble on endothelialcell membranes, whereas glass or kaolin can be used for in vitrotests of the intrinsic pathway. When the components of thecontact phase assemble on the activating surface, factor XII isactivated to factor XIIa upon proteolysis by kallikrein. This factor
XIIa, generated by kallikrein, attacks prekallikrein to generatemore kallikrein, setting up a reciprocal activation.
Factor XIIa, once formed, activates factor XI to XIa and alsoreleases bradykinin (a nonapeptide with potent vasodilatoraction) from HMW kininogen. Factor XIa in the presence of Ca2+
activates factor IX, to the serine protease, factor IXa. This in turncleaves an Arg-Ile bond in factor X (56 kDa) to produce thetwochain serine protease, factor Xa. This latter reaction requires
the assembly of components, called the tenase complex, onthe surface of activated platelets: Ca2+ and factor VIIIa, as wellas factors IXa and X. It should be noted that in all reactionsinvolving the Gla-containing zymogens (factors II, VII, IX, and X),the Gla residues in the amino terminal regions of the moleculesserve as high-affinity binding sites for Ca2+. For assembly of thetenase complex, the platelets must first be activated to expose
13
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 14/27
the acidic (anionic) phospholipids, phosphatidylserine andphosphatidylinositol, that are normally on the internal side of the plasma membrane of resting, nonactivated platelets. FactorVIII (330 kDa), a glycoprotein, is not a protease precursor but a
cofactor that serves as a receptor for factors IXa and X on theplatelet surface. Factor VIII is activated by minute quantities of thrombin to form factor VIIIa, which is in turn inactivated uponfurther cleavage by thrombin.
The extrinsic pathway also leads to the
activation of Factor X but by different
mechanism
Factor Xa occurs at the site where the intrinsic and extrinsic
pathways converge and lead into the final common pathway of blood coagulation. The extrinsic pathway involves tissue factor,factors VII and X, and Ca2+ and results in the production of factorXa. It is initiated at the site of tissue injury with the exposure of tissue factor on subendothelial cells. Tissue factor interactswith and activates factor VII (53 kDa), a circulating Gla-containing glycoprotein synthesized in the liver. Tissue factoracts as a cofactor for factor VIIa, enhancing its enzymatic activityto activate factor X. The association of tissue factor and factor
VIIa is called tissue factor complex. Factor VIIa cleaves thesame Arg-Ile bond in factor X that is cleaved by the tenasecomplex of the intrinsic pathway. Activation of factor X providesan important link between the intrinsic and extrinsic pathways.Another important interaction between the extrinsic and intrinsicpathways is that complexes of tissue factor and factor VIIa alsoactivate factor IX in the intrinsic pathway. Indeed, the
14
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 15/27
formation of complexes between tissue factor and factorVIIa is now considered to be the key process involved ininitiation of blood coagulation in vivo. The physiologicsignificance of the initial steps of the intrinsic pathway, in which
factor XII, prekallikrein, and HMW kininogen are involved, hasbeen called into question because patients with a hereditarydeficiency of these components do not exhibit bleedingproblems. Similarly, patients with a deficiency of factor XI maynot have bleeding problems. The intrinsic pathway may actuallybe more important in fibrinolysis than in coagulation, sincekallikrein, factor XIIa, and factor XIa can cleave plasminogen andkallikrein can activate singlechain urokinase.Tissue factor pathway inhibitor (TFPI) is a major physiologicinhibitor of coagulation. It is a protein that circulates in the blood
associated with lipoproteins. TFPI directly inhibits factor Xa bybinding to the enzyme near its active site. This factor Xa-TFPIcomplex then inhibits the factor VIIa-tissue factor complex.
Final common pathway involves the activation of
prothrombin to thrombin
In the final common pathway, factor Xa, produced by either theintrinsic or the extrinsic pathway, activates prothrombin (factorII) to thrombin (factor IIa), which then converts fibrinogen tofibrin.
The activation of prothrombin, like that of factor X, occurs on thesurface of activated platelets and requires the assembly of aprothrombinase complex, consisting of platelet anionic
phospholipids, Ca2+, factor Va, factor Xa, and prothrombin.Factor V (330 kDa), a glycoprotein with homology to factor VIIIand ceruloplasmin, is synthesized in the liver, spleen, and kidneyand is found in platelets as well as in plasma. It functions as acofactor in a manner similar to that of factor VIII in the tenasecomplex. When activated to factor Va by traces of thrombin, itbinds to specific receptors on the platelet membrane and forms
15
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 16/27
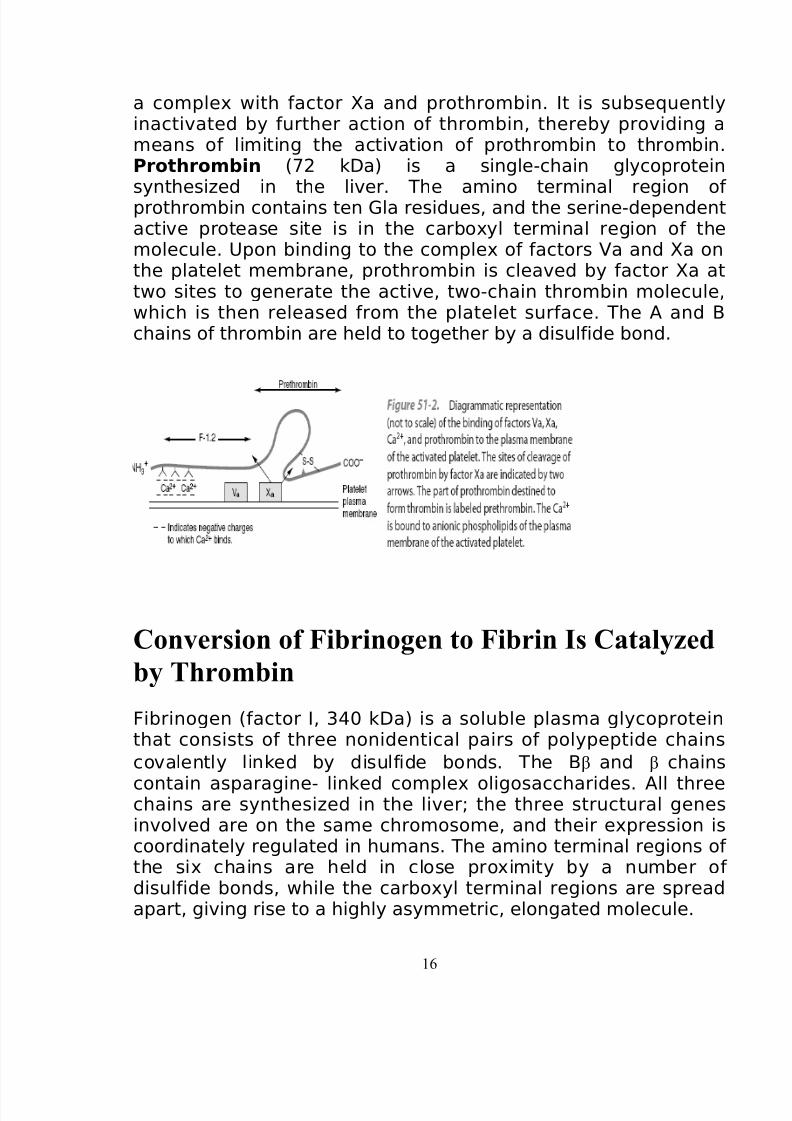
a complex with factor Xa and prothrombin. It is subsequentlyinactivated by further action of thrombin, thereby providing ameans of limiting the activation of prothrombin to thrombin.Prothrombin (72 kDa) is a single-chain glycoprotein
synthesized in the liver. The amino terminal region of prothrombin contains ten Gla residues, and the serine-dependentactive protease site is in the carboxyl terminal region of themolecule. Upon binding to the complex of factors Va and Xa onthe platelet membrane, prothrombin is cleaved by factor Xa attwo sites to generate the active, two-chain thrombin molecule,which is then released from the platelet surface. The A and Bchains of thrombin are held to together by a disulfide bond.
Conversion of Fibrinogen to Fibrin Is Catalyzed
by Thrombin
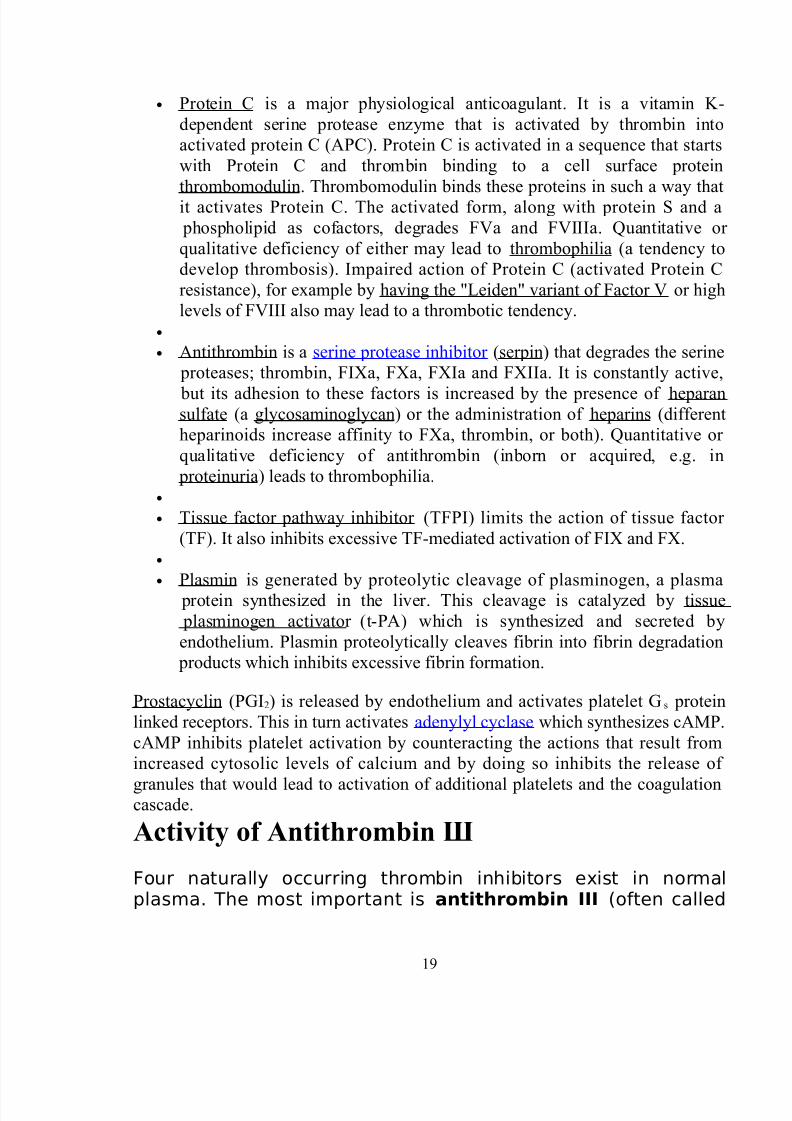
Fibrinogen (factor I, 340 kDa) is a soluble plasma glycoproteinthat consists of three nonidentical pairs of polypeptide chains
covalently linked by disulfide bonds. The Bβ and β chains
contain asparagine- linked complex oligosaccharides. All threechains are synthesized in the liver; the three structural genesinvolved are on the same chromosome, and their expression iscoordinately regulated in humans. The amino terminal regions of the six chains are held in close proximity by a number of disulfide bonds, while the carboxyl terminal regions are spreadapart, giving rise to a highly asymmetric, elongated molecule.
16
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 17/27
The A and B portions of the A and
Bβ chains,designated fibrinopeptides A (FPA) and B (FPB),respectively, at the amino terminal ends of the chains, bearexcess negative charges as a result of the presence of aspartate
and glutamate residues, as well as an unusual tyrosine O-sulfatein FPB. These negative charges contribute to the solubility of fibrinogen in plasma and also serve to prevent aggregation bycausing electrostatic repulsion between fibrinogen molecules.Thrombin (34 kDa), a serine protease formed by theprothrombinase complex, hydrolyzes the four Arg- Gly bonds
between the fibrinopeptides and the α and β portions of the
Aα and Bβ chains of fibrinogen. The release of thefibrinopeptides by thrombin generates fibrin monomer, whichhas the subunit structure (α, β , γ)2. Since FPA and FPB containonly 16 and 14 residues, respectively, the fibrin molecule retains98% of the residues present in fibrinogen. The removal of thefibrinopeptides exposes binding sites that allow the molecules of fibrin monomers to aggregate spontaneously in a regularlystaggered array, forming an insoluble fibrin clot. It is theformation of this insoluble fibrin polymer that traps platelets, redcells, and other components to form the white or red thrombi.
This initial fibrin clot is rather weak, held together only by thenoncovalent association of fibrin monomers.
In addition to converting fibrinogen tofibrin, thrombin also converts factor XIII to factor XIIIa. This factoris a highly specific transglutaminase that covalently cross-linksfibrin molecules by forming peptide bonds between the amide
groups of glutamine and the ∑-amino groups of lysine residues,yielding a more stable fibrin clot with increased resistance toproteolysis.
Cofactors of blood coagulation
Various substances are required for the proper functioning of the coagulation
cascade:
17
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 18/27
• Calcium and phospholipid (a platelet membrane constituent) are required
for the tenase and prothrombinase complexes to function. Calcium
mediates the binding of the complexes via the terminal gamma-carboxy
residues on FXa and FIXa to the phospholipid surfaces expressed by
platelets as well as procoagulant microparticles or microvesicles shedded
from them. Calcium is also required at other points in the coagulation
cascade.
• Vitamin K is an essential factor to a hepatic gamma-glutamyl carboxylase
that adds a carboxyl group to glutamic acid residues on factors II, VII, IX
and X, as well as Protein S, Protein C and Protein Z. In adding the gamma-
carboxyl group to glutamate residues on the immature clotting factors
Vitamin K is itself oxidized. Another enzyme, Vitamin K epoxidereductase, (VKORC) reduces vitamin K back to its active form. Vitamin K
epoxide reductase is pharmacologically important as a target for
anticoagulant drugs warfarin and related coumarins such as
acenocoumarol, phenprocoumon and dicumarol. These drugs create a
deficiency of reduced vitamin K by blocking VKORC, thereby inhibiting
maturation of clotting factors. Other deficiencies of vitamin K (e.g. in
malabsorption), or disease (hepatocellular carcinoma) impairs the function
of the enzyme and leads to the formation of PIVKAs (proteins formed in
vitamin K absence) this causes partial or non gamma carboxylation and
affects the coagulation factors ability to bind to expressed phospholipid.
Regulators of blood coagulation
Five mechanisms keep platelet activation and the coagulation cascade in check.
Abnormalities can lead to an increased tendency toward thrombosis:
18
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 19/27
• Protein C is a major physiological anticoagulant. It is a vitamin K-
dependent serine protease enzyme that is activated by thrombin into
activated protein C (APC). Protein C is activated in a sequence that starts
with Protein C and thrombin binding to a cell surface protein
thrombomodulin. Thrombomodulin binds these proteins in such a way that
it activates Protein C. The activated form, along with protein S and a
phospholipid as cofactors, degrades FVa and FVIIIa. Quantitative or
qualitative deficiency of either may lead to thrombophilia (a tendency to
develop thrombosis). Impaired action of Protein C (activated Protein C
resistance), for example by having the "Leiden" variant of Factor V or high
levels of FVIII also may lead to a thrombotic tendency.
•
• Antithrombin is a serine protease inhibitor (serpin) that degrades the serine
proteases; thrombin, FIXa, FXa, FXIa and FXIIa. It is constantly active,
but its adhesion to these factors is increased by the presence of heparan sulfate (a glycosaminoglycan) or the administration of heparins (different
heparinoids increase affinity to FXa, thrombin, or both). Quantitative or
qualitative deficiency of antithrombin (inborn or acquired, e.g. in
proteinuria) leads to thrombophilia.
•
• Tissue factor pathway inhibitor (TFPI) limits the action of tissue factor
(TF). It also inhibits excessive TF-mediated activation of FIX and FX.
•
• Plasmin is generated by proteolytic cleavage of plasminogen, a plasma
protein synthesized in the liver. This cleavage is catalyzed by tissue
plasminogen activator (t-PA) which is synthesized and secreted by
endothelium. Plasmin proteolytically cleaves fibrin into fibrin degradation
products which inhibits excessive fibrin formation.
Prostacyclin (PGI2) is released by endothelium and activates platelet Gs protein
linked receptors. This in turn activates adenylyl cyclase which synthesizes cAMP.
cAMP inhibits platelet activation by counteracting the actions that result from
increased cytosolic levels of calcium and by doing so inhibits the release of
granules that would lead to activation of additional platelets and the coagulationcascade.
Activity of Antithrombin Ш
Four naturally occurring thrombin inhibitors exist in normalplasma. The most important is antithrombin III (often called
19
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 20/27
simply antithrombin), which contributes approximately 75% of the antithrombin activity.Antithrombin III can also inhibit the activities of factors IXa, Xa,XIa, XIIa, and VIIa complexed with tissue factor. α2-
Macroglobulin contributes most of the remainder of theantithrombin activity, with heparin cofactor II and α1-antitrypsin acting as minor inhibitors under physiologicconditions. The endogenous activity of antithrombin III is greatlypotentiated by the presence of acidic proteoglycans such asheparin. These bind to a specific cationic site of antithrombin III,inducing a conformational change and promoting its binding tothrombin as well as to its other substrates. This is the basis forthe use of heparin in clinical medicine to inhibit coagulation. Theanticoagulant effects of heparin can be antagonized by strongly
cationic polypeptides such as protamine, which bind strongly toheparin, thus inhibiting its binding to antithrombin III. Individualswith inherited deficiencies of antithrombin III are prone todevelop venous thrombosis, providing evidence thatantithrombin III has a physiologic function and that thecoagulation system in humans is normally in a dynamic state.
20

8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 21/27
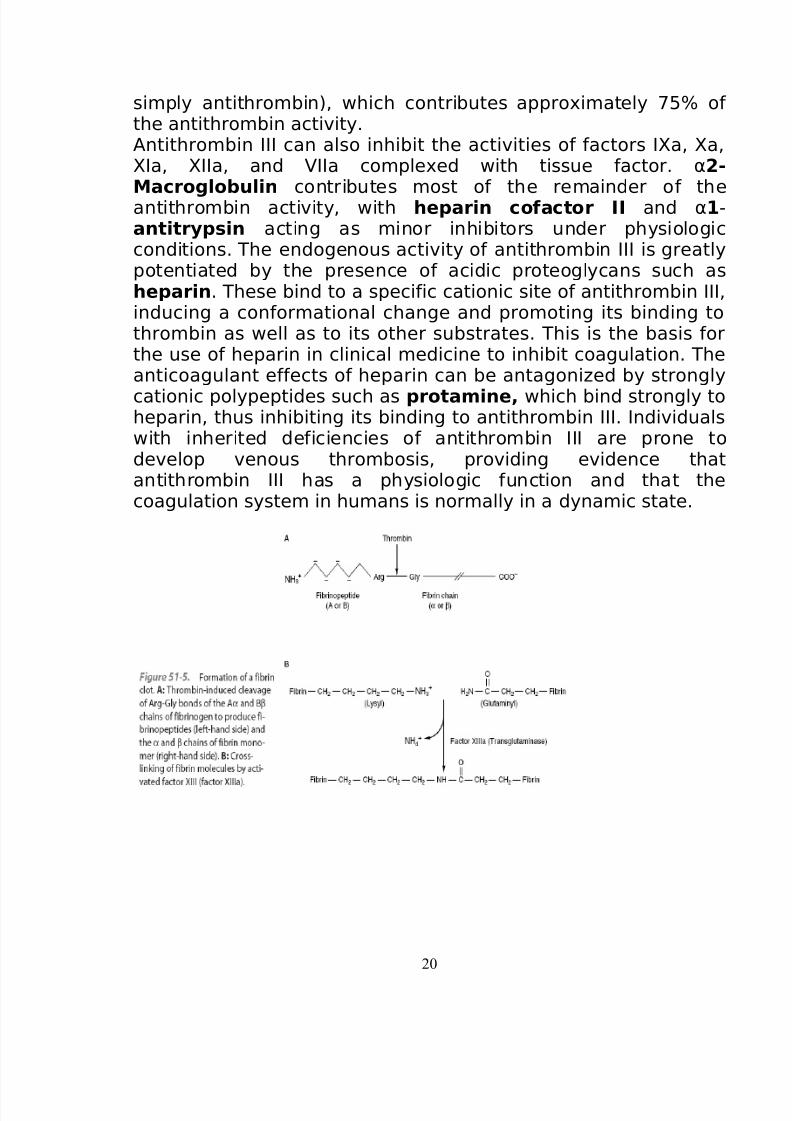
Fibrin Clots Are Dissolved by Plasmin
The coagulation system is normally in a state of dynamic
equilibrium in which fibrin clots are constantly being laid downand dissolved. This latter process is termed fibrinolysis.Plasmin, the serine protease mainly responsible for degradingfibrin and fibrinogen, circulates in the form of its inactivezymogen, plasminogen (90 kDa), and any small amounts of plasmin that are formed in the fluid phase under physiologicconditions are rapidly inactivated by the fastacting plasmininhibitor, α2-antiplasmin. Plasminogen binds to fibrin and thusbecomes incorporated in clots as they are produced; sinceplasmin that is formed when bound to fibrin is protected from
α2-antiplasmin, it remains active. Activators of plasminogenof various types are found in most body tissues, and all cleavethe same Arg-Val bond in plasminogen to produce the twochainserine protease, plasmin. Tissue plasminogen activator(alteplase; t-PA) is a serine protease that is released into thecirculation fromvascular endothelium under conditions of injuryor stress and is catalytically inactive unless bound to fibrin. Uponbinding to fibrin, t-PA cleaves plasminogen within the clot togenerate plasmin, which in turn digests the fibrin to form soluble
degradation products and thus dissolves the clot. Neitherplasmin nor the plasminogen activator can remain bound tothese degradation products, and so they are released into thefluid phase, where they are inactivated by their naturalinhibitors. Prourokinase is the precursor of a second activator of plasminogen, urokinase. Originally isolated from urine, its mainaction is probably in the degradation of extracellular matrix. Thesites of action of five proteins that influence the formation andaction of plasmin.
21
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 22/27
Endothelial Cells Synthesize Prostacyclin &Other Compounds That Affect Clotting &
Thrombosis
The endothelial cells in the walls of blood vessels makeimportant contributions to the overall regulation of hemostasisand thrombosis. These cells synthesize prostacyclin (PGI2), apotent inhibitor of platelet aggregation, opposing the action of
thromboxane A2. Prostacyclin acts by stimulating the activity of adenylyl cyclase in the surface membranes of platelets. Theresulting increase of intraplatelet cAMP opposes the increase inthe level of intracellular Ca2+ produced by IP3 and thus inhibitsplatelet activation. Endothelial cells play other roles in theregulation of thrombosis. For instance, these cells possess anADPase, which hydrolyzes ADP, and thus opposes its aggregatingeffect on platelets. In addition, these cells appear to synthesizeheparan sulfate, an anticoagulant, and they also synthesize
plasminogen activators, which may help dissolve thrombi.Analysis of the mechanisms of uptake of atherogeniclipoproteins, such as LDL, by endothelial, smooth muscle, andmonocytic cells of arteries, along with detailed studies of howthese lipoproteins damage such cells is a key area of study inelucidating the mechanisms of atherosclerosis
22
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 23/27
Aspirin Is an Effective Antiplatelet Drug
Certain drugs (antiplatelet drugs) modify the behavior of platelets. The most important is aspirin (acetylsalicylic acid),which irreversibly acetylates and thus inhibits the plateletcyclooxygenase system involved in formation of thromboxaneA2, a potent aggregator of platelets and also a vasoconstrictor.Platelets are very sensitive to aspirin; as little as 30 mg/d (oneaspirin tablet usually contains 325 mg) effectively eliminates thesynthesis of thromboxane A2. Aspirin also inhibits production of
prostacyclin (PGI2, which opposes platelet aggregation and is avasodilator) by endothelial cells, but unlike platelets, these cellsregenerate cyclooxygenase within a few hours. Thus, the overallbalance between thromboxane A2 and prostacyclin can beshifted in favor of the latter, opposing platelet aggregation.Indications for treatment with aspirin thus include managementof angina and evolving myocardial infarction and also preventionof stroke and death in patients with transient cerebral ischemicattacks.
Testing of Coagulation
Numerous tests are used to assess the function of the coagulation system:
• Common: aPTT, PT (also used to determine INR ), fibrinogen testing (often
by the Clauss method), platelet count, platelet function testing (often by
PFA-100).
• Other: TCT, bleeding time, mixing test (whether an abnormality corrects if
the patient's plasma is mixed with normal plasma), coagulation factor assays, antiphosholipid antibodies, D-dimer , genetic tests (eg. factor V
Leiden, prothrombin mutation G20210A), dilute Russell's viper venom
time (dRVVT), miscellaneous platelet function tests, thromboelastography
(TEG or ROTEM), euglobulin lysis time (ELT).
23
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 24/27
The contact factor pathway is initiated by activation of the "contact factors" of
plasma, and can be measured by the activated partial thromboplastin time (aPTT)
test.
The tissue factor pathway is initiated by release of tissue factor (a specific cellular
lipoprotein), and can be measured by the prothrombin time (PT) test. PT results
are often reported as ratio (INR value) to monitor dosing of oral anticoagulants
such as warfarin.
The quantitative and qualitative screening of fibrinogen is measured by the
thrombin clotting time (TCT). Measurement of the exact amount of fibrinogen
present in the blood is generally done using the Clauss method for fibrinogen
testing. Many analysers are capable of measuring a "derived fibrinogen" level
from the graph of the Prothrombin time clot.
If a coagulation factor is part of the contact or tissue factor pathway, a deficiency
of that factor will affect only one of the tests: thus hemophilia A, a deficiency of
factor VIII, which is part of the contact factor pathway, results in an abnormally
prolonged aPTT test but a normal PT test. The exceptions are prothrombin,
fibrinogen and some variants of FX which can only be detected by either aPTT or
PT. If an abnormal PT or aPTT is present additional testing will occur to
determine which (if any) factor is present as aberrant concentrations.
Deficiencies of fibrinogen (quantitative or qualitative) will affect all screening
tests.
Advantages of cascade system
The greatest benefit of the enzymatic cascade system in biochemical system is to
achieve the quick response. In a cascade, an initial signal institutes a series of
steps, each of which is catalyzed by an enzyme. At each step, the signal is
amplified. For instance, if a signal molecule activates an enzyme that in turn
activates 10 enzymes and each of the 10 enzymes in turn activates 10 additionalenzymes, after four steps the original signal will have been amplified 10,000-fold.
Cascade systems provide ultrasensitive responses. Not only can a response be
sensitive to a higher power than the first of the concentration of a signaling
molecule but also the amplification provided by the cascade confers a high
sensitivity to the response.
24
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 25/27
8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 26/27

8/6/2019 Bio Chemistry Assignment
http://slidepdf.com/reader/full/bio-chemistry-assignment 27/27
Related Documents











