Binge Eating Disorder Diagnosis and Treatment Options Timothy D. Brewerton Eating Disorders Program, Department of Psychiatry and Behavioural Sciences, Medical University of South Carolina, Charleston, South Carolina, USA Contents Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351 1. History and Diagnostic Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351 2. Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 353 3. Medical Comorbidity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 353 4. Psychiatric Comorbidity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 354 5. Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 355 5.1 Psychotherapeutic Strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 355 5.2 Psychopharmacological Strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 356 6. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 359 Abstract Binge eating disorder (BED) is a newly proposed eating disorder diagnosis that appears in the appendix of DSM-IV. BED describes a syndrome of recurrent binge eating in the absence of any maladaptive compensatory behaviours. Indi- viduals with BED appear to demonstrate a primary disturbance of eating behavi- our, which in some people may be secondary to affective and/or anxiety disorders. The chronic, recurrent bingeing associated with BED is thought to typically lead to obesity and its accompanying morbidity and mortality. BED is also associated with significant psychiatric comorbidity, including affective, anxiety and person- ality disorders, although the degree of psychopathology is usually not as severe as that of bulimia nervosa. In this paper, the history, diagnosis, epidemiology, associated psychiatric comorbidity and treatment approaches of BED are reviewed. Generally, cognitive-behavioural therapy and/or antidepressant medications are key treatment approaches. DISEASE MANAGEMENT CNS Drugs 1999 May; 11 (5): 351-361 1172-7047/99/0005-0351/$05.50/0 © Adis International Limited. All rights reserved. 1. History and Diagnostic Classification A new diagnostic category called ‘binge eating disorder’ (BED) has been proposed in the appendix of DSM-IV. [1-6] BED is characterised by recurrent episodes of binge eating at least 2 days a week for at least 6 months, which is longer than the 3 months duration of bingeing required for a DSM-IV diag- nosis of bulimia nervosa. BED also requires a sub- jective sense of a loss of control over the binge eating, as well as the presence of at least 3 of 5 specific criteria, including eating more rapidly than usual, eating large quantities of food when not phy- sically hungry, eating alone due to embarrassment, eating until uncomfortably full and feeling self- disgust, guilt or depression after bingeing. [1] A specific syndrome of overeating in the context of obesity was first described by Stunkard, who de-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Binge Eating DisorderDiagnosis and Treatment Options
Timothy D. BrewertonEating Disorders Program, Department of Psychiatry and Behavioural Sciences, Medical Universityof South Carolina, Charleston, South Carolina, USA
ContentsAbstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3511. History and Diagnostic Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3512. Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3533. Medical Comorbidity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3534. Psychiatric Comorbidity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3545. Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 355
5.1 Psychotherapeutic Strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3555.2 Psychopharmacological Strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 356
6. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 359
Abstract Binge eating disorder (BED) is a newly proposed eating disorder diagnosisthat appears in the appendix of DSM-IV. BED describes a syndrome of recurrentbinge eating in the absence of any maladaptive compensatory behaviours. Indi-viduals with BED appear to demonstrate a primary disturbance of eating behavi-our, which in some people may be secondary to affective and/or anxiety disorders.The chronic, recurrent bingeing associated with BED is thought to typically leadto obesity and its accompanying morbidity and mortality. BED is also associatedwith significant psychiatric comorbidity, including affective, anxiety and person-ality disorders, although the degree of psychopathology is usually not as severeas that of bulimia nervosa. In this paper, the history, diagnosis, epidemiology,associated psychiatric comorbidity and treatment approaches of BED are reviewed.Generally, cognitive-behavioural therapy and/or antidepressant medications arekey treatment approaches.
DISEASE MANAGEMENT CNS Drugs 1999 May; 11 (5): 351-3611172-7047/99/0005-0351/$05.50/0
© Adis International Limited. All rights reserved.
1. History and Diagnostic Classification
A new diagnostic category called ‘binge eatingdisorder’ (BED) has been proposed in the appendixof DSM-IV.[1-6] BED is characterised by recurrentepisodes of binge eating at least 2 days a week forat least 6 months, which is longer than the 3 monthsduration of bingeing required for a DSM-IV diag-nosis of bulimia nervosa. BED also requires a sub-
jective sense of a loss of control over the bingeeating, as well as the presence of at least 3 of 5specific criteria, including eating more rapidly thanusual, eating large quantities of food when not phy-sically hungry, eating alone due to embarrassment,eating until uncomfortably full and feeling self-disgust, guilt or depression after bingeing.[1]
Aspecific syndrome of overeating in the contextof obesity was first described by Stunkard, who de-

lineated the ‘night eating syndrome’ in the1950s.[7,8]
Night eating syndrome is similar to, but distinctfrom, BED, which does not have the nocturnal com-ponent as a diagnostic requirement. In night eatingsyndrome, overeating episodes are not necessarilytrue binges; the episodes only occur at night, andthe subsequent anorexia and food restriction occurin the morning. This pattern of restrained eatingduring the day is thought to contribute to the nextcycle of overeating or bingeing at night for bothnight eating syndrome and BED. Other terms haveappeared over the years to describe the phenome-non of severe, recurrent overeating or binge eatingnot complicated by purging, including ‘obese binge-eaters’, ‘compulsive overeaters’[9-11] and the ‘stuff-ing syndrome’.[12]
Since DSM-III was first published in 1980, suchpatients have been classified as ‘eating disorder nototherwise classified’, but this is a nonspecific termand includes a number of subsyndromal features.[13]
The discipline of psychiatry in the US first acknow-ledged binge eating in DSM-III (1980) in the clas-sification of ‘bulimia’, a diagnosis that encompassednot only bingeing, but also purging and preoccupa-tion with body shape and weight.[13] DSM-III-R,the revised edition of DSM-III published in 1987,adopted the term ‘bulimia nervosa’, which was orig-inally coined in 1979 by Russell,[14] who concep-tualised bulimia nervosa as ‘an ominous variant ofanorexia nervosa’.[15] Binge eatingper sewithoutcompensatory anti-obesity behaviours, was not iden-tified as a specific psychiatric syndrome or problemuntil DSM-IV included BED in the Appendix as adiagnosis to be considered.[1]
As psychiatric knowledge has accumulated andevolved over time, so our diagnostic nomenclaturehas evolved to reflect this knowledge and to moreprecisely describe psychiatric disease states. As partof this process, the eating disorders have only re-cently received serious research attention comparedwith other disorders. The inclusion of binge eatingwithout compensatory behaviours as an illness is anatural extension of this evolving process of under-standing the bulimic disorders spectrum. BED is infact a serious behavioural health problem that ap-
pears to have been underrecognised and under-treated. In my opinion, the diagnostic recognitionof BED will allow this group of patients to be fur-ther studied from a clinical research perspective,and it will also allow them to get more accessibleand appropriate treatment. However, the exact boun-daries of the disorder remain to be further deline-ated, and it is likely that eating disorder diagnosticcriteria in general will continue to evolve as ourknowledge base expands, particularly in the area ofgenetics of psychiatric disorders and obesity.
One of the existing problems regarding the diag-nosis of BED includes differentiating it from bulimianervosa, nonpurging type, as currently defined byDSM-IV.[16] The nonpurging type of bulimia nervosainvolves fasting and excessive exercise as compen-satory behaviours, as well as binge eating and pre-occupation with body weight and shape.[1] How-ever, it is arguable to what extent the similaritiesbetween the nonpurging type of bulimia nervosaand BED appear to outweigh their differences. Inclinical practice, these disorders tend not to be dis-tinct entities, but rather exist on a continuum. Patientsmay move in and out of specific eating disorderdiagnostic criteria over time. Sometimes it is alsoquite difficult clinically to distinguish between whatare appropriate versus inappropriate bodyweight lossmeasures, such as to what extent exercising is ex-cessive or compulsive. It is notable to this discus-sion that patients with obesity and bingeing behavi-our[17,18]and patients with BED have been reportedto have similar attitudes about body shape and weightcompared with patients with both nonpurging[19]
and purging bulimia nervosa.[20] However, regard-less of what label the syndrome carries, it is clearfrom epidemiological studies that a significant num-ber of people experience clinically significant bingeeating not complicated by compensatory measures.Taken together, this condition, now called BED,certainly warrants further recognition, treatment andresearch.
One laboratory study of patients with obesityand BED compared with patients with obesity butwithout BED confirmed that BED patients eat sig-nificantly more calories during a binge meal than
352 Brewerton
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)

non-BED patients.[21,22] Dietary restraint and/or dis-inhibition appear to play major roles in triggeringbinge episodes.[23-25]
2. Epidemiology
As discussed in section 1, investigators have notedfor several decades that clinically significant re-current binge eating occurs in a significant subsetof obese individuals. As a logical progression ofthis inquiry, the prevalence rates of BED were ini-tially reported in samples of obese patients attendingweightloss programmes or clinics.[3-5] In these co-horts, 20 to 46% of patients were said to endorse BEDcriteria using self-report questionnaires.[3,5,10,11]
However, an important finding has been that pa-tients tend to over-endorse BED symptoms on self-report measures when compared with structuredinterviews using standardised criteria.[8,26,27]
Spitzer and associates reported that the preva-lence of BED in cross-sections of weight controlpatients as assessed by questionnaire was approx-imately 30%, with the rate being slightly higher infemales than males.[3] These same authors went onto complete 2 field studies of nonpatient commu-nity samples and reported a BED prevalence of 3.3and 4.6%, with overall rates again being compar-able in women and men (5.3 and 3.1%, respective-ly).[5] In a sample of college students, the BED pre-valence rate was 2.6%, and likewise there was nosignificant gender difference, which is an impor-tant difference between BED and bulimia nervosapatient groups. The validity of the diagnosis of BEDhas been strengthened by links with impairedfunctioning in occupational and social areas, over-concern with body shape and weight, degree of gen-eral psychopathology and amount of time dieting.Interestingly, there were no significant racial dif-ferences found in BED prevalence rates in any ofthese studies.
Our group surveyed a representative sample ofover 3000 adult women in the US (the NationalWomen’s Study) using a structured, computerisedtelephone interview based directly on proposedDSM-IV criteria for BED and DSM-III-R criteriafor bulimia nervosa.[28-30] Our results indicated that
1.0% of women over the age of 18 years met fulllifetime criteria for BED over and above another2.4% of women who met lifetime bulimia nervosacriteria. Approximately two-thirds of both diagno-stic groups met current diagnostic criteria, whichwas defined as the 12-month prevalence rate. Sig-nificant differences were not found for age, body-weight or race between respondents with BED andthose with bulimia nervosa, although both the BEDand the bulimia nervosa respondents were signifi-cantly younger and heavier than the non-BED/non-bulimia nervosa respondents. Interestingly, whenwe relaxed the binge duration criterion to 3 months(from 6 months), the BED prevalence rate increa-sed to 1.6% (from 1.0%).[28] Because these resultswere acquired from a meticulously controlled, rep-resentative sample, they substantiate that a size-able group of adult women in the US have clini-cally significant bingeing without purging. Theseresults contribute to the credibility of BED.
Results from a structured telephone interviewcompleted in a community-based Californian, USsample indicated that 1.8% of 455 adult womenmet DSM-IV BED criteria.[31] In addition, another3.8% of these women met all BED criteria exceptthat of frequency.
Results from a questionnaire-based communitystudy in Norway of 1849 women indicated that thelifetime prevalence of BED was 3.2%.[32] In a sim-ilar study based on a self-report questionnaire com-pleted in France, the rate of BED was 9 to 15% inbodyweight control samples and 0.7% in a commu-nity sample of 447 nontreatment-seeking women.[33]
A very low BED prevalence in the UK was alsorecently reported.[34] Despite the major methodo-logical differences among these studies, the resultsindicate that the prevalence of BED, like that ofother eating disorders, may indicate some degreeof cultural variability.
3. Medical Comorbidity
Medical conditions associated with BED are es-sentially the same medical conditions that are as-sociated with obesity, including higher mortalityand morbidity from adult-onset (type 2) diabetes
Binge Eating Disorders: Diagnosis and Treatment 353
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)

mellitus, hyperlipidaemias, cardiovascular diseases,several cancers and sleep apnoea. In general, diseaseprevalence increases as bodymass index [bodyweight(kg)/height (m)2] increases.
As the increasingly apparent interrelationshipsbetween psychiatric disorders and obesity are re-cognised, and as the pervasive stigmatisation of boththe mentally ill and the obese in Western culturecontinues, a comprehensive psychiatric perspectiveis going to be needed for optimal evaluation andtreatment of patients with BED. This is especiallytrue given the fact that many medications, both psy-chotropic and nonpsychotropic, are associated withbodyweight gain and subsequent obesity. Hence,clinicians are often faced with the proverbial ‘rockand a hard place’.
Obese patients with BED appear to have higherdegrees of both eating- and bodyweight-relatedpathology, body image distortion and body preoc-cupation when compared with obese patients with-out BED.[11,35,36]
It also appears that obese patients who binge eatfind it more difficult to lose bodyweight and re-main in weightloss programmes,[10,37] although inone well controlled study the presence of BED didnot affect outcome of bodyweight loss, nor wasthere a higher withdrawal rate when compared withthe non-BED obese patients.[38] On the contrary, inthe community study by Ferguson and Spitzer, suc-cessful dieters were less likely to meet BED criteriathan unsuccessful dieters.[39] No differences havebeen found in serum lipid levels, thyroid hormonelevels or resting metabolic rate between obese bingeeaters and nonbinge eaters.[40,41]The degree of body-weight cycling or ‘yo-yo dieting’has been reportedto be higher in obese patients with binge eatingcompared with those without bingeing in one,[42]
but not in another, study.[41]
4. Psychiatric Comorbidity
The relationship between eating disorders, in-cluding BED, and other psychiatric disorders hasbeen a significant area of interest to clinicians andresearchers alike. Several investigators have notedthat binge eating occurs in a subset of obese pa-
tients in response to emotional stress, a phenomenawhich has been termed ‘emotional eating’.[43,44] Inone study, BED patients were more likely to over-eat in response to negative emotional states.[19] Di-agnostic studies of obese patients with BED indi-cate higher than expected rates of affective, anxietyand personality disorders, as well as emotional prob-lems in general.[40,42,44-50]In a study of 107 obesewomen meeting BED criteria who completed sev-eral psychometric instruments, there was a signif-icant positive relationship between binge eatingseverity and degree of psychiatric symptomatol-ogy.[44] DeZwaan and colleagues also found a rela-tionship between binge eating and a number of meas-ures of psychopathology.[42]
In a structured telephone interview of a large,nonclinical sample of US women (n = 3006) [theNational Women’s Study], the lifetime prevalenceof major depression was 31% in respondents meet-ing BED criteria and 36% in respondents meetingbulimia nervosa criteria; rates which were signifi-cantly higher than the nonbingeing group (15%).[28]
It is important to note that major depression wasnot present in the majority of respondents, sincesome BED opponents argue that binge eating ismerely a symptom, albeit atypical, of depression.Although these results do not support this hypoth-esis, BED may be associated with subclinical af-fective and perhaps anxiety disorders. A recent studyconfirmed that dysphoric mood states often triggerbinge eating episodes accompanied by a subjectivesense of being out of control.[44] However, thesepatients do not necessarily meet the criteria formajor depression at the time of bingeing, or ever.In a study of the chronological relationship betweenthe times of onset of bingeing, dieting and depres-sion, it was found that BED patients on averagetended to begin bingeing during adolescence be-fore the onset of dieting, obesity or depression.[51]
At any rate, the higher rates of depression associ-ated with BED are compatible with an affect dys-regulation hypothesis for binge eating.
In the National Women’s Study, Dansky and col-leagues also discovered that the lifetime prevalenceof post-traumatic stress disorder was 21% in BED
354 Brewerton
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)

respondents compared with 9% in the nonbingeingrespondents.[28] In contrast with bulimia nervosa,the rates of crime victimisation experiences, inclu-ding rape, molestation, attempted sexual assault andaggravated assault, were comparable with the non-BED/non-bulimia nervosa group. Nevertheless, thehigher rate of lifetime post-traumatic stress disor-der in the patients with BED imply that they mayhave been exposed to other types of traumatic eventsor experiences more frequently in comparison withthe people without BED or bulimia nervosa. In astudy of a clinical sample, there was no significantdifference in reported rates of sexual abuse in BEDversus non-BED obese patients, but BED patientsdid have significantly higher rates of panic disor-der and personality disorders than the non-BEDobese patients.[47]
In clinical practice, patients with BED often re-port histories of significant family dysfunction as-sociated with emotional abuse and/or neglect, ifnot overt childhood physical and/or sexual abuse.Hodges and colleagues reported results from theFamily Environment Scale in 131 patients with aneating disorder presenting for evaluation and treat-ment, including 43 with BED.[52] Significantly lowerscores were found on the activity-recreation subscalefor the BED group compared with the anorexia ner-vosa, bulimia nervosa and anorexia nervosa plusbulimia nervosa groups. Results also indicated thatthe patients with BED perceived their families tobe less cohesive compared with the anorexia ner-vosa patients, but not the bulimia nervosa patients.In addition, the patients with BED had higher con-trol and conflict subscale scores, and lower cohe-siveness, expressiveness, independence, intellectual-cultural and activity-recreation subscale scores, whencompared with 2 healthy control samples previous-ly published.
Impulsive behaviours, such as compulsive buy-ing and kleptomania, have been reported in patientswith BED.[53] In addition, higher rates of cluster Band C personality disorders, but not substance abusedisorders, have been reported in patients withBED.[47,49]Furthermore, the rates of alcoholism inthe family members of patients with BED were
significantly higher.[47] Given these data, resear-chers have placed BED within the continuum ofcompulsive-impulsive disorders[53] as well as theaffective spectrum disorders.[54]
5. Treatment
5.1 Psychotherapeutic Strategies
Studies indicate that behavioural treatments forobesity tend to only work in the short term for thevast majority of patients attempting to lose body-weight.[37] However, patients with BED seem to berelatively less responsive to these commonly em-ployed treatment strategies. Even if bodyweight issuccessfully reduced in the short term, BED pa-tients may be more apt to relapse in the long term.Converging evidence suggests that dietary restraintor overt dieting has a disinhibiting effect on over-eating or bingeing and consequently contributes tothe marked bodyweight fluctuations that are typi-cal of these patients’ histories. Importantly, the psy-chiatric comorbidity and/or emotional issues arenot addressed in strictly behavioural forms of treat-ment and may therefore contribute to refractorinessand/or relapse. Patients with BED usually have avariety of needs that are best approached from theperspective of the biopsychosocial model. A mul-tidisciplinary approach is therefore usually requir-ed for optimal evaluation and treatment, includingnetworking among all professionals involved, e.g.the patient’s primary care provider, psychiatrist,psychotherapist, dietician, physical therapist, etc.
Most clinicians who work with BED patientsshare the common treatment philosophy of initiallymaking the goal of bodyweight loss secondary tothe primary goal of decreasing or eliminating bingeeating and normalising eating behaviour. In addition,addressing associated psychiatric disorders and/oremotional symptoms often must take precedencein order for successful treatment to occur.
Guided by the successes in treating bulimia ner-vosa,[55,56] major depression and most anxiety dis-orders, recent well controlled studies[57-61] usingmanual-driven cognitive-behavioural therapy haveshown great promise in the treatment of BED. In
Binge Eating Disorders: Diagnosis and Treatment 355
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)

cognitive-behavioural therapy, specific attention isdirected toward the patient’s behaviour and thoughtpatterns instead of the traditional focus on associ-ated feelings, intrapsychic conflicts and other psy-chodynamic issues, such as transference. In addi-tion, cognitive-behavioural therapy places a strongemphasis on education, monitoring of food intake,identifying cognitive distortions (or false beliefs)and replacing them with rational or reality-basedthoughts. So far, there has been one uncontrolledtrial[62] and a few controlled trials of cognitive-behavioural therapy in BED[57-61] (table I). Evenless well studied is the effect of interpersonal psy-chotherapy on BED (table I), which has also beenfound to be helpful in both patients with major de-pression and those with bulimia nervosa.[56,58,59]
Taken together, the preponderance of evidencesupports the premise that effective treatment forpatients with BED, at least in the short term, shouldfocus first on reducing binge eatingper seas wellas on establishing a regular meal pattern with littleor no snacking, particularly before bedtime. In ad-dition, identifying and challenging distorted thoughtsassociated with this eating disorder is warranted. Ifbingeing and its associated dietary restraint and dis-inhibition are controlled, then some degree of body-
weight loss is often a natural outcome. As a result,patients may also have more energy to begin a rea-sonable exercise programme, starting off and pro-gressing very slowly, and consequently becomingless depressed and anxious.
In patients with significant concomitant psychi-atric comorbidity (usually mood and/or anxiety dis-orders) psychotherapeutic strategies will of courseneed to address these disorders as well. Further-more, when patients are unresponsive to reason-able trials of psychotherapeutic and/or behaviouralapproaches, then psychopharmacological interven-tions should be considered as adjunctive treatment.
5.2 Psychopharmacological Strategies
Because of the convincing links between sero-tonin (5-hydroxytryptamine; 5-HT) dysregulationand affective, anxiety and eating disorders,[63] clin-ical researchers have speculated that the selectiveserotonin reuptake inhibitors (SSRIs) could possi-bly be effective treatments for obesity as well asBED. The published results from controlled studiesare summarised in table II.[64-67]
Preliminary results from open-label drug stud-ies in patients with BED using SSRIs other thanfluoxetine and fluvoxamine, e.g. paroxetine, have
Table I. Psychotherapy studies in binge eating disorder (BED) and related conditions
Reference Patients Treatment Duration(weeks)
Results
Telch et al.[57] 44 women with nonpurgingbulimia nervosa
CBT vs wait list 10 94% decrease in binge eating with CBT(79% abstinent) vs 9% decrease with no Tx
Wilfrey et al.[58] 55 women with nonpurgingbulimia nervosa
CBT vs IPT vs waitlist
16 Both CBT (48%) and IPT (71%)significantly reduced binge eatingcompared with no Tx (10%). Goodfollow-up data at 6 and 12 months
Smith et al.[59] 8 obese women with bingeeating
Open CBT 16 81% decrease in binge eating
Eldredge et al.[60] 44 women and 2 men with BEDnot responsive to CBT andbodyweight loss Tx
Extended CBT vswait list followingCBT andbodyweight loss Tx
36 (total) Extending CBT led to improvement in 67%of patients previously unresponsive
Agras et al.[61] 93 obese women with BED notresponsive to 12 weeks of CBT
CBT followed bybodyweight loss Tx
52 weekfollow-up
Reductions in binge eating and abstinencerates were mostly maintained. Successfulbodyweight loss linked to binge abstinence
Agras et al.[62] 43 women and 7 men with BEDnot responsive to CBT
IPT added to CBT(12 weeks)
24 (total) No added benefit of IPT to CBTnonresponders
CBT = cognitive-behavioural therapy; IPT = interpersonal psychotherapy; Tx = treatment.
356 Brewerton
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)

demonstrated notable reductions in binge frequen-cy (see McElroy et al.[53] for review). More con-trolled studies in patients with BED using new gen-eration antidepressants are definitely required, butagents which inhibit serotonin reuptake show somepromise.
Reports of studies involving tricyclic antidep-ressants (TCAs) indicate their possible usefulnessin binge eaters, despite their relative lack of neuro-transmitter specificity and more numerous adverseeffects and complications compared with newer anti-depressants (table II).[68,69] TCAs, especially desi-pramine, may hence offer some relief as pharmaco-logical treatments for BED, as well as for bulimianervosa. In clinical practice, however, it is gener-ally advised that the initial psychopharmacological
treatment strategy involves an SSRI.[54] The TCAsare commonly associated with bodyweight gain,probably resulting from a combination of inducedhyperphagia via stimulation of hypothalamic nor-adrenergic pathways as well as a decrease in meta-bolic rate. However, among the TCAs, desipramineis probably the least likely to cause these adverseeffects.
Treatment of BED with monoamine oxidase in-hibitors (MAOIs) is of dubious value in patientswho by definition are out of control of their eatingand who would have difficulty maintaining therequired restriction of tyramine-rich foods. How-ever, MAOIs should be a consideration in distinctcases of atypical depression (characterised by hyper-phagia, hypersomnia and anxiety) that have not
Table II. Psychopharmacological studies in binge eating disorder (BED) and related conditions
Reference Patients Treatment Duration Results
Marcus et al.[45] 45 obese women with andwithout binge eating
Fluoxetine +behaviourmodification vsplacebo + behaviourmodification
52 weeks Presence of binge eating did not predictbodyweight loss, which was greater with drug
Greeno & Wing[64] 50 overweight women withand without BED
Fluoxetine vs placebo 4-6 days Fluoxetine significantly reduced bingefrequency vs placebo irrespective of BEDstatus
Darga et al.[65] 45 women with obesity Fluoxetine vs placebo 52 weeks Significant early bodyweight loss withfluoxetine, but effect disappeared by end of 1year because of regain
Hudson et al.[67] 85 patients with BED (77women and 8 men)
Fluvoxamine vsplacebo
9 weeks Fluvoxamine significantly reduced bingefrequency and increased rate of BMI reduction
McCann & Agras[68] 23 women with nonpurgingbulimia nervosa
Desipramine vsplacebo
12 weeks 63% decrease and 60% abstinence withdesipramine vs 16 and 15%, respectively,with placebo
Alger et al.[69] 22 patients with bulimia and33 with obesity and bingeing
Imipramine vsnaltrexone vs placebo
8 weeks Imipramine and naltrexone significantlyreduced duration of binge episodes inpatients with obesity and bingeing andbulimia, respectively
Guy-Grand et al.[70] 822 obese patients (662women and 160 men)
Dexfenfluramine vsplacebo
52 weeks Dexfenfluramine significantly reducedbodyweight vs placebo
Stunkard et al.[71] 28 women with BED Dexfenfluramine vsplacebo
8 weeks Dexfenfluramine significantly reduced bingefrequency vs placebo
Marrazzi et al.[72] 36-year-old woman with BED Naltrexone vsplacebo (single case,crossover design)
18 weeks Naltrexone reduced binge eating vs placebo,especially at high dosage (400 mg/day)
Drewnowski etal.[73]
41 women (16 with obesityand binge eating and 25 withnormal bodyweight)
Naloxone vsbutorphanol vsplacebo
Single dose(acute IVbolus)
Naloxone reduced intake of sweet and highfat foods in patients with obesity and bingeingvs butorphanol and placebo
BMI = bodymass index; IV = intravenous.
Binge Eating Disorders: Diagnosis and Treatment 357
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)
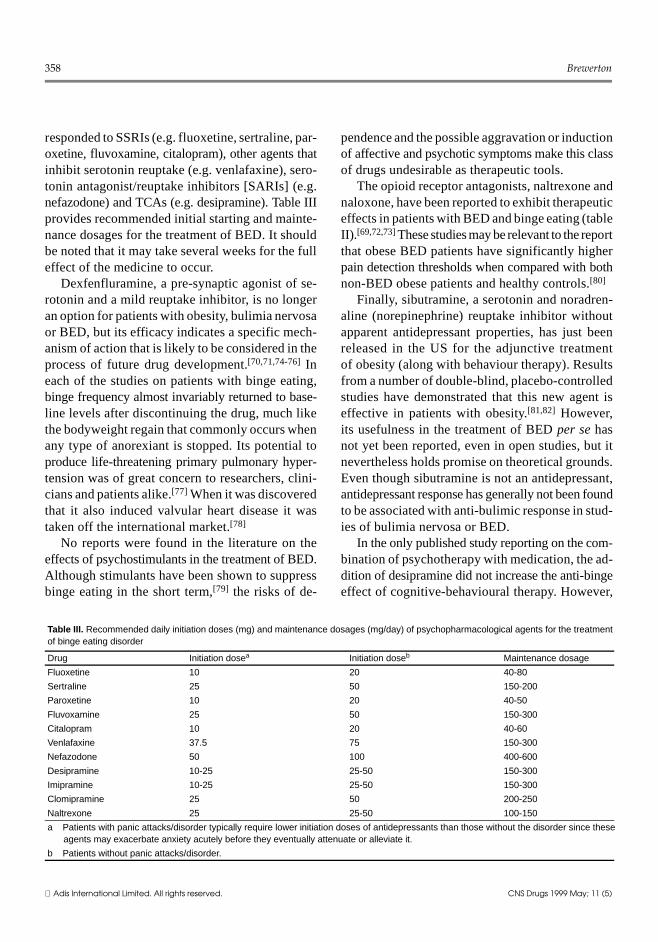
responded to SSRIs (e.g. fluoxetine, sertraline, par-oxetine, fluvoxamine, citalopram), other agents thatinhibit serotonin reuptake (e.g. venlafaxine), sero-tonin antagonist/reuptake inhibitors [SARIs] (e.g.nefazodone) and TCAs (e.g. desipramine). Table IIIprovides recommended initial starting and mainte-nance dosages for the treatment of BED. It shouldbe noted that it may take several weeks for the fulleffect of the medicine to occur.
Dexfenfluramine, a pre-synaptic agonist of se-rotonin and a mild reuptake inhibitor, is no longeran option for patients with obesity, bulimia nervosaor BED, but its efficacy indicates a specific mech-anism of action that is likely to be considered in theprocess of future drug development.[70,71,74-76] Ineach of the studies on patients with binge eating,binge frequency almost invariably returned to base-line levels after discontinuing the drug, much likethe bodyweight regain that commonly occurs whenany type of anorexiant is stopped. Its potential toproduce life-threatening primary pulmonary hyper-tension was of great concern to researchers, clini-cians and patients alike.[77] When it was discoveredthat it also induced valvular heart disease it wastaken off the international market.[78]
No reports were found in the literature on theeffects of psychostimulants in the treatment of BED.Although stimulants have been shown to suppressbinge eating in the short term,[79] the risks of de-
pendence and the possible aggravation or inductionof affective and psychotic symptoms make this classof drugs undesirable as therapeutic tools.
The opioid receptor antagonists, naltrexone andnaloxone, have been reported to exhibit therapeuticeffects in patients with BED and binge eating (tableII).[69,72,73]These studies may be relevant to the reportthat obese BED patients have significantly higherpain detection thresholds when compared with bothnon-BED obese patients and healthy controls.[80]
Finally, sibutramine, a serotonin and noradren-aline (norepinephrine) reuptake inhibitor withoutapparent antidepressant properties, has just beenreleased in the US for the adjunctive treatmentof obesity (along with behaviour therapy). Resultsfrom a number of double-blind, placebo-controlledstudies have demonstrated that this new agent iseffective in patients with obesity.[81,82] However,its usefulness in the treatment of BEDper sehasnot yet been reported, even in open studies, but itnevertheless holds promise on theoretical grounds.Even though sibutramine is not an antidepressant,antidepressant response has generally not been foundto be associated with anti-bulimic response in stud-ies of bulimia nervosa or BED.
In the only published study reporting on the com-bination of psychotherapy with medication, the ad-dition of desipramine did not increase the anti-bingeeffect of cognitive-behavioural therapy. However,
Table III. Recommended daily initiation doses (mg) and maintenance dosages (mg/day) of psychopharmacological agents for the treatmentof binge eating disorder
Drug Initiation dosea Initiation doseb Maintenance dosage
Fluoxetine 10 20 40-80
Sertraline 25 50 150-200
Paroxetine 10 20 40-50
Fluvoxamine 25 50 150-300
Citalopram 10 20 40-60
Venlafaxine 37.5 75 150-300
Nefazodone 50 100 400-600
Desipramine 10-25 25-50 150-300
Imipramine 10-25 25-50 150-300
Clomipramine 25 50 200-250
Naltrexone 25 25-50 100-150
a Patients with panic attacks/disorder typically require lower initiation doses of antidepressants than those without the disorder since theseagents may exacerbate anxiety acutely before they eventually attenuate or alleviate it.
b Patients without panic attacks/disorder.
358 Brewerton
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)

bodyweight lossper sewas facilitated by the combin-ation.[83] More time and knowledge will be requiredto determine how similar the pharmacological mech-anisms underlying binge eating reduction are tothose underlying bodyweight reductionper se. How-ever, whether the addition of cognitive-behaviouraltherapy to antidepressants enhances response hasnot yet been determined, but my clinical impres-sion is that it does help.
Future avenues to more effective pharmacolog-ical treatments for BED will most likely followobesity research studies, as well as new develop-ments in the treatment of bulimia nervosa. Undercurrent investigation are agents that enhanceenergy expenditure and which target leptin and itsreceptors, neuropeptide satiety agents, e.g. neuro-peptide Y, cholecystokinin and obesity genes.[84]
6. Conclusion
In summary, the proposed diagnostic entity inDSM-IV of BED appears to be a well validatedcondition characterised by recurrent binge eatingwithout compensatory behaviours of any type. BEDdiffers from bulimia nervosa, nonpurging type, bythe absence of fasting or excessive exercise as away of counteracting the inevitable bodyweight gaineffects of binge eating. However, in the clinicalsetting these conditions may be difficult to distin-guish from each other given their overlap in symp-toms as well as inconsistencies in self-report. Thelifetime prevalence of BED in US women is ap-proximately 1%, and a sizeable proportion (up to30%) of those seeking bodyweight loss treatmentin bariatric programmes will also meet the criteria.It is essential that the diagnosis of BED not be basedon self-report alone, since over reporting is possi-ble. Although a self-report instrument may serve asa useful screening tool, actual diagnoses should bebased on structured clinical interviews.
BED is often associated with specific medicaland psychiatric comorbidities, especially obesityand its complications, affective disorders and anx-iety disorders, particularly panic disorder and post-traumatic stress disorder. Both psychotherapeuticand psychopharmacological treatment strategies show
efficacy in the studies done so far, but the field isyoung. Current data suggest starting with cogni-tive-behavioural therapy and aggressively treatingassociated psychiatric comorbidity, perhaps withan SSRI such as fluoxetine or fluvoxamine. If thisfails, a trial of desipramine, nefazodone, venlafax-ine or naltrexone/naloxone should be a considera-tion. In all cases a comprehensive risk-benefit anal-ysis (of both treatment and nontreatment) must beconducted before treatment is initiated.
References1. American Psychiatric Association. Diagnostic and statistical
manual of mental disorders. 4th ed. Washington, DC: Amer-ican Psychiatric Press, 1994
2. Spitzer RL, Devlin MJ, Walsh BT, et al. Binge eating disorder:to be or not to be in DSM-IV. Int J Eat Dis 1991; 10: 627-9
3. Spitzer RL, Yanovski S, Wadden T, et al. Binge eating disorder:its further validation in a multisite study. Int J Eat Dis 1993;13: 137-53
4. Spitzer RL, Stunkard A, Yanovski S, et al. Binge eating disordershould be included in DSM-IV: a reply to Fairburn et al.’s‘The classification of recurrent overeating: the binge eatingdisorder proposal’. Int J Eat Dis 1993; 13: 161-9
5. Spitzer RL, Yanovski S, Wadden T, et al. Binge eating disorder:its further validation in a multisite study. Int J Eat Dis 1993;13: 137-53
6. Brody ML, Walsh BT, Devlin MJ. Binge eating disorder: reli-ability and validity of a new diagnostic category. J ConsultClin Psychol 1994; 62: 381-6
7. Stunkard AJ. Eating patterns and obesity. Psychiatr Q 1959; 33:284-94
8. Stunkard AJ, Berkowitz R, Wadden T, et al. Binge eating dis-order and the night-eating syndrome. Int J Obesity 1996; 20:1-6
9. Loro AD Jr, Orleans CS. Binge eating in obesity: preliminaryfindings and guidelines for behavioral analysis and treatment.Addict Behav 1981; 6: 155-66
10. Marcus MD, Wing RR. Binge eating among the obese. AnnBehav Med 1987; 9: 23-7
11. de Zwaan MD, Mitchell JE. Binge eating in the obese. Ann Med1992; 24: 303-8
12. Kornhaber A. The stuffing syndrome. Psychosomatics 1970; 11(6): 580-4
13. American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders. 3rd ed. Washington, DC: Amer-ican Psychiatric Press, 1980
14. American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders. 4th ed. Washington, DC: Amer-ican Psychiatric Press, 1987
15. Russell GFM. Bulimia nervosa, an ominous variant of anorexianervosa. Psychol Med 1979; 9: 429-48
16. Spitzer RL. Nonpurging bulimia nervosa and binge eating dis-order. Am J Psychiatry 1991; 148: 1097-8
17. Cash TF. Binge-eating and body images among the obese: afurther evaluation. J Soc Behav Personal 1991; 6: 367-76
18. Wilson GT, Nonas CA, Rosenblum GD. Assessment of bingeeating in obese patients. Int J Eat Dis 1993; 13: 25-33
Binge Eating Disorders: Diagnosis and Treatment 359
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)
19. Eldredge KL, Agras WS. Weight and shape overconcern andemotional eating in binge eating disorder. Int J Eat Dis 1996;19: 73-82
20. Raymond NC, Mussell MP, Mitchell JE, et al. An age-matchedcomparison of subjects with binge eating disorder and bulimianervosa. Int J Eat Dis 1995; 18: 135-43
21. Goldfein JA, Walsh BT, LaChaussee JL, et al. Eating behaviorin binge eating disorder. Int J Eat Dis 1993; 14: 427-31
22. Yanovski SZ, Leet M, Yanovski JA, et al. Food selection andintake of obese women with binge-eating disorder. Am J ClinNutr 1992; 56: 975-80
23. Marcus MC, Wing RR, Lamparski DM. Binge eating and di-etary restraint in obese patients. Addict Behav 1985; 10: 163-8
24. Yanovski SZ, Sebring NG. Recorded food intake of obese womenwith binge-eating disorder before and after weight loss. Int JEat Dis 1994; 15: 135-50
25. Yanovski SZ. The chicken or the egg: binge eating disorder anddietary restraint [abstract]. Appetite 1995; 24 (3): 258
26. Greeno CG, Marcus MD, Wing RR. Diagnosis of binge eatingdisorder: discrepancies between a questionnaire and clinicalinterview. Int J Eat Dis 1995; 17: 153-60
27. Nangle DW, Johnson WG, Carr-Nangle REC, et al. Binge eatingdisorder and the proposed DSM-IV criteria: psychometric an-alysis of the questionnaire of eating and weight patterns. IntJ Eat Dis 1994; 16: 147-57
28. Dansky BS, Brewerton TD, Kilpatrick DG, et al. The nature andprevalence of binge eating disorder in a national sample ofwomen. In: Widiger TA, Frances AJ, Pincus HA, et al., editors.DSM-IV Sourcebook. Washington: APA Press, Inc., 1998:515-31
29. Brewerton TD, Dansky BS, Kilpatrick DG, et al. The preva-lence of binge eating disorder in United States women. Syl-labus and Proceedings of the 149th Annual Meeting of theAmerican Psychiatric Association; 1996 May 5-9; New York(NY). Washington, DC: American Psychiatric Press: 76
30. Dansky BS, Brewerton TD, O’Neil PM, et al. The national wo-men’s study: relationship of crime victimization and PTSD tobulimia nervosa. Int J Eat Dis 1997; 21: 213-28
31. Bruce B, Agras WS. Binge eating in females: a population-based investigation. Int J Eat Dis 1992; 12: 365-75
32. Gotestam KG, Agras WS. General population-based epidemio-logical study of eating disorders in Norway. Int J Eat Dis 1995;18: 119-26
33. Basdevant A, Pouillon M, Lahlou N, et al. Prevalence of bingeeating disorder in different populations of French women. IntJ Eat Dis 1995; 18: 309-15
34. Robertson DN, Palmer RL. The prevalence and correlates ofbinge eating in a British community sample of women with ahistory of obesity. Int J Eat Dis 1997; 22: 323-7
35. Mussell MP, Mitchell JE, de Zwaan M, et al. Clinical charac-teristics associated with binge eating in obese females: a de-scriptive study. Int J Obesity 1996; 20: 324-31
36. Mussell MP, Peterson CB, Weller CL, et al. Differences in bodyimage and depression among obese women with and withoutBED. Obesity Res 1996; 4: 431-9
37. Keefe PH, Wyshogrod D, Weinberger E, et al. Binge eating andoutcome of behavioral treatment of obesity: a preliminaryreport. Behav Res Ther 1984; 22: 319-21
38. Ho KSI, Nichman MZ, Taylor WC, et al. Binge eating disorder,retention, and dropout in adult obesity program. Int J Eat Dis1995; 18: 291-4
9. Ferguson DJ, Spitzer RL. Binge eating disorder in a commu-nity-based sample of successful and unsuccessful dieters. IntJ Eat Dis 1995; 18: 167-72
40. Wadden TA, Foster GD, Letizia KA, et al. Metabolic, anthro-pometric, and psychological characteristics of obese bingeeaters. Int J Eat Dis 1993; 14: 17-25
41. Adami GF, Gandolfo P, Campostano A, et al. Obese binge eat-ers: metabolic characteristics, energy expenditure and dieting.Psychol Med 1995; 25: 195-8
42. de Zwaan MD, Mitchell JE, Seim HC, et al. Eating related andgeneral psychopathology in obese females with binge eatingdisorder. Int J Eat Dis 1994; 15: 43-52
43. Ganley RM. Emotions and eating in obesity: a review of theliterature. Int J Eat Dis 1989; 8: 343-61
44. Telch CF, Agras WS. Obesity, binge eating and psychopathol-ogy: are they related? Int J Eat Dis 1994; 15: 53-61
45. Marcus MD, Wing RR, Ewing L, et al. Psychiatric disordersamong obese binge eaters. Int J Eat Dis 1990; 9: 69-77
46. Fichter MM, Quadflieg N, Brandl B. Recurrent overeating: anempirical comparison of binge eating disorder, bulimia ner-vosa, and obesity. Int J Eat Dis 1993; 14: 1-16
47. Yanovski SZ, Nelson JE, Dubbert BK, et al. Association ofbinge eating disorder and psychiatric comorbidity in obesesubjects. Am J Psychiatry 1993; 150: 1472-9
48. Antony MM, Johnson WG, Carr-Nangle RE, et al. Psychopa-thology correlates of binge eating and binge eating disorder.Compr Psychiatry 1994; 35: 386-92
49. Specker S, de Zwaan M, Raymond N, et al. Psychopathologyin subgroups of obese women with and without binge eatingdisorder. Compr Psychiatry 1994; 35: 185-90
50. Kuehnel RH, Wadden TA. Binge eating disorder, weight cy-cling, and psychopathology. Int J Eat Dis 1995; 15: 321-9
51. Mussell MP, Mitchell JE, Weller CL, et al. Onset of binge eating,dieting, obesity, and mood disorders among subjects seekingtreatment for binge eating disorder. Int J Eat Dis 1995; 17:395-401
52. Hodges EL, Cochrane CE, Brewerton TD. Family character-istics of binge eating disorder patients. Int J Eat Dis 1998; 23:145-51
53. McElroy SL, Keck PE, Phillips KA. Kleptomania, compulsivebuying, and binge eating disorder. J Clin Psychiatry 1994; 56Suppl. 4: 14-26
54. Hudson JI, Carter WP, Pope HG. Antidepressant treatment ofbinge eating disorder: research findings and clinical guide-lines. J Clin Psychiatry 1988; 57 Suppl. 8: 73-9
55. Mitchell JE, Pyle R, Eckert ED, et al. A comparison of antide-pressants and structured intensive group psychotherapy in thetreatment of bulimia nervosa. Arch Gen Psychiatry 1990; 47:149-57
56. Fairburn CG, Jones R, Peveler RC, et al. Three psychologicaltreatments for bulimia nervosa. Arch Gen Psychiatry 1991;48: 463-9
57. Telch CF, Agras WS, Rossiter EM, et al. Group cognitive-be-havioral treatment for the nonpurging bulimic: an initial eval-uation. J Consult Clin Psychol 1990; 58: 629-35
58. Wilfrey DE, Agras WS, Telch CF, et al. Group cognitive-behav-ioral therapy and group interpersonal psychotherapy for thenonpurging bulimic individual: a controlled comparison. JConsult Clin Psychol 1993; 61: 296-305
59. Smith DE, Marcus MD, Kaye W. Cognitive-behavioral treat-ments of obese binge eaters. Int J Eat Dis 1992; 12: 257-62
60. Eldredge KL, Agras WS, Arnow B, et al. The effects of extendingcognitive-behavioral therapy for binge eating disorder amonginitial treatment nonresponders. Int J Eat Dis 1997; 21 (4):347-52
360 Brewerton
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)
61. Agras WS, Telch CF, Arnow B, et al. One-year follow-up ofcognitive-behavioral therapy for obese individuals with bingeeating disorder. J Consult Clin Psych 1997; 65: 343-7
62. Agras WS, Telch CF, Arnow B, et al. Does interpersonal therapyhelp patients with binge eating disorder who fail to respondto cognitive-behavioral therapy? J Cons Clin Psychol 1995;63: 356-60
63. Brewerton TD. Toward a unified theory of serotonin dysregula-tion in eating and related disorders. Psychoneuroendocrinol1995; 20: 561-90
64. Greeno CG, Wing RR. A double-blind, placebo controlled trialof the effect of fluoxetine on dietary intake in overweightwomen with and without binge-eating disorder. Am J ClinNutr 1996; 64: 267-73
65. Darga LL, Carroll-Michals L, Botsford SJ, et al. Fluoxetine’seffect on weight loss in obese subjects. Am J Clin Nutr 1991;54: 321-5
66. Marcus MD, Wing RR, Ewing L, et al. A double-blind, placebo-controlled trial of fluoxetine plus behavior modification in thetreatment of obese binge-eaters and non-binge eaters. Am JPsychiatry 1990; 147: 876-81
67. Hudson JI, McElroy SL, Raymond N, et al. Fluvoxamine in thetreatment of binge eating disorder: a multicenter placebo-con-trolled, double-blind trial. Am J Psychiatry 1998; 155: 1756-62
68. McCann UD, Agras WS. Successful treatment of nonpurgingbulimia nervosa with desipramine: a double-blind, placebo-controlled study. Am J Psychiatry 1990; 147: 1509-13
69. Alger SA, Schwalberg MD, Bigaouette JM, et al. Effect of atricyclic antidepressant and opiate antagonist on binge-eatingbehavior in normoweight bulimic and obese, binge-eating sub-jects. Am J Clin Nutr 1991; 53: 865-71
70. Guy-Grand B, Appelbaum M, Crepaldi G, et al. Internationaltrial of long-term dexfenfluramine in obesity. Lancet 1989;II: 1142-4
71. Stunkard AJ, Berkowitz R, Tanrikut C, et al. d-Fenfluraminetreatment of binge eating disorder. Am J Psychiatry 1996;153: 1455-9
72. Marrazzi MA, Markham KM, Kinzie J, et al. Binge eating dis-order: response to naloxone. Int J Obesity 1995; 19: 143-5
73. Drewnowski A, Krahn DD, Demitrack MA, et al. Naloxone, anopiate blocker, reduces the consumption of sweet high-fatfoods in obese and lean female binge eaters. Am J Clin Nu-trition 1995; 61: 1206-12
74. Robinson PH, Checkley SA, Russell GFM. Suppression of eat-ing by fenfluramine in patients with bulimia nervosa. Br JPsychiatry 1985; 146: 169-76
75. Russell GFM, Checkley SA, Feldman J, et al. A controlled trialof d-fenfluramine in bulimia nervosa. Clin Neuropharmacol1988; 11 Suppl. 1: S146-59
76. Blouin AG, Blouin JH, Perez EL, et al. Treatment of bulimiawith fenfluramine and desipramine. J Clin Psychopharmacol1988; 8: 261-9
77. Abenhaim L, Moride Y, Brenot F, et al. Appetite-suppressantdrugs and the risk of primary pulmonary hypertension. Inter-national Primary Pulmonary Hypertension Study Group. NEngl J Med 1996; 335: 609-16
78. Connolly HM, Crary JL, McGoon MD, et al. Valvular heartdisease associated with fenfluramine-phentermine. N Engl JMed 1997; 337: 581-8
79. Ong YL, Checkley SA, Russell GFM. Suppression of bulimicsymptoms with methylamphetamine. Br J Psychiatry 1983;143: 288-93
80. Raymond NC, de Zwaan M, Faris PL, et al. Pain thresholds inobese binge-eating disorder subjects. Biol Psychiatry 1995;37: 202-4
81. Bray GA, Ryan DH, Gordon D, et al. A double-blind random-ized placebo-controlled trial of sibutramine. Obesity Res 1996;4: 263-70
82. Lean ME. Sibutramine - a review of clinical efficacy. Int J Obe-sity Rel Metab Dis 1997; 21 Suppl. 1: S30-6
83. Agras WS, Telch CF, Arnow B, et al. Weight loss, cognitive-be-havioral, and desipramine treatments in binge eating disorder.An addictive design. Behav Ther 1994; 25: 225-38
84. Weiser M, Frishman WH, Michaelson MD, et al. The pharma-cologic approach to the treatment of obesity. J Clin Pharmacol1997; 37: 453-73
Correspondence and reprints: Prof. Timothy D. Brewerton,Eating Disorders Program, Department of Psychiatry andBehavioural Sciences, Medical University of South Caro-lina, 67 President Street, Suite 553, PO Box 250861, Charles-ton, South Carolina 29425, USA.E-mail: [email protected]
Binge Eating Disorders: Diagnosis and Treatment 361
Adis International Limited. All rights reserved. CNS Drugs 1999 May; 11 (5)
Related Documents











