CASE REPORT Bilateral parotid gland tuberculosis: A rare occurrence Rajendra Takhar * , Motilal Bunkar, Vinod Jangid, Anil Saxena Dept of Respiratory Medicine, Govt Medical College, Kota 324010, Rajasthan, India Received 22 February 2015; accepted 5 March 2015 Available online 26 March 2015 KEYWORDS Tubercular parotiditis; Bilateral; Diagnosis Abstract Parotid gland tuberculosis is an extremely rare form of extrapulmonary tuberculosis, even in countries where tuberculosis is endemic like India; however, it should be included as one of the differentials of discrete parotid swelling as it generally presents as a slow-growing mass indis- tinguishable from a malignancy and even imaging too, can’t differentiate these clearly. The majority of the previously reported cases were mostly unilateral and diagnosed by histopathological exam- ination of post parotidectomy specimens. Here we are describing a case of tuberculosis of both par- otid glands in a 25 year-old male who was referred to us with bilateral parotid region swelling of two month duration. Tubercular parotiditis was confirmed by demonstration of epithelioid granu- loma and caseous necrosis compatible with TB on fine needle aspiration cytology (FNAC). He was treated with four drug anti-TB regimen (2HERZ + 4HR) leading to full recovery and complete disappearance of swelling and symptoms with no recurrence till one year of follow up. Apart from rarity due to bilateral involvement, this case report highlights the clinical presentation, ultra- sonography and other imaging findings, and significance of FNAC in diagnosis of this uncommon entity reinforcing the fact that the diagnosis of parotid gland tuberculosis requires a high degree of clinical suspicion. ª 2015 The Authors. Production and hosting by Elsevier B.V. on behalf of The Egyptian Society of Chest Diseases and Tuberculosis. This is an open access article under the CC BY-NC-ND license (http:// creativecommons.org/licenses/by-nc-nd/4.0/). Introduction Extra pulmonary tuberculosis (EPTB) is an emerging problem as they have a diagnostic dilemma and management contro- versy. In India, the incidence of EPTB ranges from 20% to 30% [1]. Among EPTB, the involvement of the parotid gland is quite rare even in an endemic country like India and merely hundred cases have been reported in known literature, most of them diagnosed from post parotidectomy specimens [2]. Chronic parotiditis is a very rare disease of the parotid glands, for which various causes have been enumerated, including decreased flow of secretion in the duct (due to inflammation), gland emphysema (due to duct destruction), infectious (e.g. tuberculosis), and non-infectious causes (e.g. Sarcoidosis, autoimmune diseases, Sjogren’s syndrome, malignancy and duct stones). Most of previously reported cases had unilateral tubercular parotiditis. Here we are discussing a case of * Corresponding author at: Qtr No. 1/4, Medical College Campus, Kota, India. Tel.: +91 7442470911, mobile: +91 9784006021. E-mail addresses: [email protected] (R. Takhar), drmotilalbun- [email protected] (M. Bunkar), [email protected] (V. Jangid), [email protected] (A. Saxena). Peer review under responsibility of The Egyptian Society of Chest Diseases and Tuberculosis. Egyptian Journal of Chest Diseases and Tuberculosis (2015) 64, 653–656 HOSTED BY The Egyptian Society of Chest Diseases and Tuberculosis Egyptian Journal of Chest Diseases and Tuberculosis www.elsevier.com/locate/ejcdt www.sciencedirect.com http://dx.doi.org/10.1016/j.ejcdt.2015.03.002 0422-7638 ª 2015 The Authors. Production and hosting by Elsevier B.V. on behalf of The Egyptian Society of Chest Diseases and Tuberculosis. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Egyptian Journal of Chest Diseases and Tuberculosis (2015) 64, 653–656
HO ST E D BY
The Egyptian Society of Chest Diseases and Tuberculosis
Egyptian Journal of Chest Diseases and Tuberculosis
www.elsevier.com/locate/ejcdtwww.sciencedirect.com
CASE REPORT
Bilateral parotid gland tuberculosis: A rare
occurrence
* Corresponding author at: Qtr No. 1/4, Medical College Campus,
Kota, India. Tel.: +91 7442470911, mobile: +91 9784006021.
E-mail addresses: [email protected] (R. Takhar), drmotilalbun-
[email protected] (M. Bunkar), [email protected] (V. Jangid),
[email protected] (A. Saxena).
Peer review under responsibility of The Egyptian Society of Chest
Diseases and Tuberculosis.
http://dx.doi.org/10.1016/j.ejcdt.2015.03.0020422-7638 ª 2015 The Authors. Production and hosting by Elsevier B.V. on behalf of The Egyptian Society of Chest Diseases and TubeThis is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Rajendra Takhar *, Motilal Bunkar, Vinod Jangid, Anil Saxena
Dept of Respiratory Medicine, Govt Medical College, Kota 324010, Rajasthan, India
Received 22 February 2015; accepted 5 March 2015
Available online 26 March 2015
KEYWORDS
Tubercular parotiditis;
Bilateral;
Diagnosis
Abstract Parotid gland tuberculosis is an extremely rare form of extrapulmonary tuberculosis,
even in countries where tuberculosis is endemic like India; however, it should be included as one
of the differentials of discrete parotid swelling as it generally presents as a slow-growing mass indis-
tinguishable from a malignancy and even imaging too, can’t differentiate these clearly. The majority
of the previously reported cases were mostly unilateral and diagnosed by histopathological exam-
ination of post parotidectomy specimens. Here we are describing a case of tuberculosis of both par-
otid glands in a 25 year-old male who was referred to us with bilateral parotid region swelling of
two month duration. Tubercular parotiditis was confirmed by demonstration of epithelioid granu-
loma and caseous necrosis compatible with TB on fine needle aspiration cytology (FNAC). He was
treated with four drug anti-TB regimen (2HERZ + 4HR) leading to full recovery and complete
disappearance of swelling and symptoms with no recurrence till one year of follow up. Apart from
rarity due to bilateral involvement, this case report highlights the clinical presentation, ultra-
sonography and other imaging findings, and significance of FNAC in diagnosis of this uncommon
entity reinforcing the fact that the diagnosis of parotid gland tuberculosis requires a high degree of
clinical suspicion.ª 2015 The Authors. Production and hosting by Elsevier B.V. on behalf of The Egyptian Society of Chest
Diseases and Tuberculosis. This is an open access article under the CC BY-NC-ND license (http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Extra pulmonary tuberculosis (EPTB) is an emerging problemas they have a diagnostic dilemma and management contro-versy. In India, the incidence of EPTB ranges from 20% to
30% [1]. Among EPTB, the involvement of the parotid gland
is quite rare even in an endemic country like India and merelyhundred cases have been reported in known literature, most ofthem diagnosed from post parotidectomy specimens [2].Chronic parotiditis is a very rare disease of the parotid glands,
for which various causes have been enumerated, includingdecreased flow of secretion in the duct (due to inflammation),gland emphysema (due to duct destruction), infectious (e.g.
tuberculosis), and non-infectious causes (e.g. Sarcoidosis,autoimmune diseases, Sjogren’s syndrome, malignancy andduct stones). Most of previously reported cases had unilateral
tubercular parotiditis. Here we are discussing a case of
rculosis.

654 R. Takhar et al.
bilateral tubercular parotiditis in a 25 year old male diagnosedby fine needle aspiration cytology and successfully treated withanti-TB drugs.
Case presentation
A 25 years old non-smoker, non-alcoholic male having symp-
toms of swelling in bilateral parotid region since two monthsreferred from the ENT department with suspicion of chronicparotiditis to the outpatient department of pulmonary medi-
cine for assessment. Initially the swelling was non tender whichlater on became pain full. Before attending our OPD, he hadreceived broad spectrum antibiotics for 15 days but didn’t
get any improvement. There was no history of constitutionalsymptom, hoarseness of voice and difficulty in deglutination.He also denied for personal or contact history of tuberculosis
and any oro-dental surgical procedure recently.Local examination of parotid region revealed two firm,
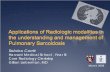
non-mobile, tender swellings of 3 · 3 cm and 2 · 2 cm on theright side (Fig. 1) and 1 · 1 cm on the left side. Swelling
extended antero-posteriorly from sub-mandibular angle toear lobe on the right side and just beneath the angle ofmandible on the left side. There was no sinus or discharge from
swelling and facial nerve was intact. Oral examination showedbilateral diffuse parotid enlargement which was soft to firm inconsistency with normal overlying skin.
Through physical examination excluded clubbing, cyanosis,dilated veins, pedal oedema, organomegaly and lym-phadenopathy. Examinations of other systems were normalincluding respiratory system with normal chest skiagram PA
view. Laboratory investigations revealed no abnormalityexcept raised ESR (140 mm in first hour). Routine blood tests,including sugar (fasting), renal and liver function tests, urine
analysis, ECG and Ultra-sonography (USG) of the abdomenshowed no abnormality. HIV serology was also negative.Monteux test was positive with induration of 20 · 20 cm in
48 h. The sputum smear examination was negative for acid fastbacilli (AFB). No calcification was found in sialogram of theparotid gland. Anti-Nuclear Antibody, Rheumatoid Factor
and Anti-ds DNA were negative and serum ACE titre wasnormal, further excluding the possibility of sarcoidosis andother autoimmune disorders.
Figure 1 Swelling in the right parotid region with some local
application over it.
USG of the parotid region showed enlarged bilateral paro-tid gland (right > left) with hypo echoic rounded solid masslike lesions within the architecture of the right parotid gland
with the absence of calcification and cystic degeneration(Fig. 2a). An intra-parenchymal lesion seen just near to theglandular region was bulging through a breach in the gland
surface into the extra glandular space (Fig. 2b). Arterial typeof vascularity found in the lesion during colour doppler study(Fig. 3). USG guided fine needle aspiration cytology of the
swellings from both sides showed granulomatous epithelioidcell clusters, macrophages and caseation necrosis, suggestiveof tubercular parotid lymphadenitis (Fig. 4). AFB smearprepared from FNAC sample was also positive, confirming
our diagnosis of tubercular parotiditis. The patient was treatedwith four drugs (Isoniazid, Rifampicin, Ethambutol andPyrazinamide) anti-TB regimen (CAT I RNTCP) for
2 months, followed by two drugs (Isoniazid, Rifampicin) for4 months. With the six month of therapy, he showed acomplete resolution of swellings and no recurrence even after
one year follow up.
Discussion
Tuberculosis has been a major cause of suffering and deathsince times immemorial and it is one of chronic necrotisinggranulomatous diseases with various manifestations and a
wide distribution. It affects both pulmonary and extra-pulmonary organs. Extra pulmonary sites vary from cervicallymph node, bone, skin, meninges, abdomen and many more,but the involvement of parotid glands is exceedingly rare and
bilateral involvement is even more uncommon [3]. First caseof tubercular parotiditis was diagnosed in 1893 by C DePoali [2].
Parotid tuberculosis can occur both as primary with theabsence of pulmonary TB like in our patient or concurrentlywith pulmonary TB. Parotid gland and lymph nodes involve-
ment may occur in two ways. The First pathways involveascending infection of salivary gland through Stenson’s ductor accompanied lymph node, where tubercular bacilli liberate
infection to the oral cavity. Haematogenous or lymphaticspread from another distant primary lung focus is the secondpathway [4]. According to some authors spread by lymphaticvessels, particularly from infected tonsils and external auditory
canal, plays an important role [5]. The salivary glandstuberculosis is more commonly seen because of secondarypathways than as primary itself but in our case chest skiagram
was normal excluding the pulmonary tuberculosis as thesource of tubercular infection.
Clinical presentation of tubercular parotiditis mimics to the
neoplastic pathology and it usually presents as a unilaterallocalised and progressive chronic swelling or abscess in theparotid region. Presentation may vary from an acute infectiousprocess to an indolent chronic presentation. It is almost
impossible to differentiate clinically from other inflammatorydiseases of salivary gland when AFB is negative fromStenson’s duct secretion or saliva. The differential diagnosis
includes malignancy of parotid gland, mumps, sarcoidosis,actinomycosis, etc.
Ultrasonographic examination of the parotid swelling plays
a major role in the diagnosis of parotid tuberculosis. Due totheir superficial location high resolution ultrasound is able to

Figure 2 (a and b) USG of the parotid region showing enlarged parotid gland with hypo echoic rounded solid lesions within the
architecture of the right parotid gland with absence of calcification and cystic degeneration (Fig. 2a). An intra-parenchymal lesion seen
just near to the glandular region, which is bulging through a breach in the gland surface into the extra glandular space (arrow head)
(Fig. 2b).
Figure 3 Color Doppler study showing an arterial type of
vascularity.
Figure 4 FNAC showing epithelioid cell granuloma with
macrophages. (10·).
Bilateral parotid gland tuberculosis 655
demonstrate whether the lesion is within the parotid gland or isin periparotid area, differentiation in between benign and
malignant neoplasms. Sonographically parotid tuberculosiscan be classified in two types: parenchymal and periparotidtype. The parenchymal type is the most common and appearsas a diffusely enlarged, comparatively hypoechoic gland as in
our case, with or without focal intraparotid anechoic zones.The periparotid type appears as hypoechoic nodules locatedin the peripheral zone of the hyperechoic parotid gland, consis-
tent with enlarged periglandular lymph nodes [6]. The colourdoppler of the parotid gland is also not specific and varies fromavascular to highly vascular lesions [4]. On contrast enhanced
CT scan, the presence of central lucency with thick walled rimenhancing lesion is suggestive of tubercular pathology. OnMRI, the lesions usually appear hypointense on T1 and hyper-intense on T2 weighted images with homogenous contrast
enhancement which is a nonspecific finding [7]. Non invasiveinvestigations such as USG, CT and MRI scan are sensitivebut not specific in detecting intraparotid tubercular lesions.
Presence of granuloma and caseous necrosis in the histopatho-logical examination of the biopsied material is necessary forfinal diagnosis. Findings of USG-guided fine needle aspiration
cytology (FNAC) correlates well with postoperative histologi-cal findings with an overall accuracy of 86–89% [8].
Four drug regimen (rifampicin, isoniazid, ethambutol and
pyrazinamide) in the intensive phase followed by two drugs(rifampicin and isoniazid) in continuation phase is a recom-mended treatment regimen even in this pauci-bacillary extrapulmonary form of tuberculosis [9].
Conclusion
Parotid gland tuberculosis specially bilateral involvement is a
rare form of the extra pulmonary TB, usually presenting aschronic swelling or mass. Therefore, it is recommended toperform tuberculosis work-up for such patients especially in
endemic countries like India. The early diagnosis and suspicionare required to avert the need for surgery which may be a

656 R. Takhar et al.
hazardous procedure in a medically treatable condition as seenin our case. Medical management with the anti-tuberculardrugs thus prevents the economic burden for patients as well
as surgical scar mark over cosmo-sensitive area.
Conflict of interest
We have no conflict of interest to declare.
References
[1] V.K. Arora, R. Gupta, Directly observed treatment for
tuberculosis, Indian J. Tuberc. 53 (2006) 77–83.
[2] A.K. Janmeja, S.K. Das, S. Kochhar, U. Handa, Tuberculosis of
the parotid gland, Indian J. Chest Dis. Allied Sci. 45 (2003) 67–
69.
[3] A.L. Hamdan, U. Hadi, N. Shabb, Tuberculosis parotitis: a
forgotten entity, Otolaryngol. Head Neck Surg. 126 (2002) 581–
582.
[4] V. Gupta, K. Patankar, A. Shinde, C. Bhosale, A. Tamhane,
Tuberculosis of the parotid gland. Case Reports in Radiology,
vol. 2012, Article ID 278793, 3 pages.
[5] L. Alex, M. Balkrishan, A. Kittyavirah, Tuberculosis of parotid
gland – a case report, Indian J. Radiol. Imaging 16 (4) (2006)
689–690.
[6] R.A.S. Kushwaha, S. Kant, S.K. Verma, Sanjay, S. Mehra,
Isolated metacarpal bone tuberculosis: a case report, Lung India
16 (25) (2008) 17–29.
[7] H. Birkent, S. Karahatay, T. Akcam, et al, Primary parotid
tuberculosis mimicking parotid neoplasm: a case report, J. Med.
Case Rep. 2 (2008) (article 62).
[8] Y.H. Chou, C.M. Tiu, C.Y. Liu, et al, Tuberculosis of the
parotid gland: Sonographic manifestations and sonographically
guided aspiration, J. Ultrasound Med. 23 (2004) 1275–1281.
[9] World Health Organization, Treatment of Tuberculosis:
Guidelines for National Programs, WHO/CDS/TB/2010, WHO,
2010.
Related Documents