Bilateral Internal Thoracic Artery Harvest and Deep Sternal Wound Infection in Diabetic Patients Salil V. Deo, MS, MCh, Ishan K. Shah, MBBS, Shannon M. Dunlay, MD, MS, Patricia J. Erwin, MLS, Chaim Locker, MD, Salah E. Altarabsheh, MD, Barry A. Boilson, MD, Soon J. Park, MD, and Lyle D. Joyce, MD, PhD Divisions of Cardiovascular Surgery and Cardiovascular Diseases, and Medical Education, Mayo Clinic, Rochester, Minnesota; and Division of Cardiovascular Surgery, Princess Alia Heart Institute, Amman, Jordan Background. Coronary artery bypass graft surgery is superior to percutaneous intervention in diabetic pa- tients with multivessel disease. The use of bilateral internal thoracic arteries (BITA) may provide better long- term graft patency, but the risk of postoperative deep sternal wound infection has limited its use in diabetic patients. However, studies have reported conflicting re- sults, and require systematic evaluation. Methods. MEDLINE, EMBASE, World of Science, and the Cochrane library were searched for randomized con- trolled trials and observational studies comparing the incidence of deep sternal wound infection in diabetic patients undergoing either left internal thoracic artery (LITA) or BITA harvest. We used random effect models to compare risk ratios within groups. Results. One randomized controlled trial and 10 obser- vational studies (126,235 diabetic patients: 122,465 LITA, 3,770 BITA) met inclusion criteria. Deep sternal wound infection occurred in 3.1% and 1.6% for the BITA and LITA cohorts, respectively. The risk ratio for deep sternal wound infection development was 1.71 (1.37 to 2.14) for BITA compared with LITA. Patients who underwent skeletonized BITA harvest had a similar risk of deep sternal wound infection compared with LITA (0.9 [0.42 to 2.09]), although pedicled harvest demonstrated in- creased risk (1.77 [1.4 to 2.23]). Early mortality was comparable in the LITA cohort (2.5%) and the BITA cohort (2.3%; p 0.8). Conclusions. The risk of deep sternal wound infection can be minimized in diabetic patients undergoing coro- nary artery bypass graft surgery by performing ITA harvested in a skeletonized manner with meticulous attention to preserving sternal blood flow. Pedicled har- vest is to be discouraged when utilizing both ITA owing to a significant increase in the risk of postoperative deep sternal wound infection. (Ann Thorac Surg 2013;95:862–9) © 2013 by The Society of Thoracic Surgeons C oronary artery bypass graft surgery (CABG) has demonstrated superior long-term survival com- pared with percutaneous therapy for diabetic patients with multivessel disease [1]. Whereas the conventional strategy has been to utilize the left internal thoracic artery (LITA) for grafting to the left anterior descending artery, studies have demonstrated the long-term benefit of bilateral internal thoracic artery (BITA) use for CABG [2, 3]. Unfortunately, the pedicled method of LITA har- vest may reduce sternal blood flow and impair wound healing [4], and the primary reason for avoiding the use of BITA is the risk of deep sternal wound infection (DSWI), which is particularly high among diabetic pa- tients [5]. The meticulous skeletonized technique of ITA harvest was introduced to preserve sternal blood flow, and proponents believe that BITA harvest in this manner will not increase the risk of DSWI. However, available observational studies demonstrate conflicting results. Hence, we have conducted a system- atic review and meta-analysis to compare the risk of DSWI in diabetic patients undergoing CABG with BITA versus LITA, and to evaluate the impact of a pedicled versus a skeletonized BITA harvest on infection risk. Material and Methods Eligibility Criteria Randomized controlled trials (RCT) or observational studies were eligible if they met the following criteria: (1) adult human subjects; (2) patients underwent isolated CABG, either on pump or off pump; and (3) study reported deep sternal wound infection, need for reex- ploration for bleeding, in-hospital mortality, or 30-day mortality in a group with BITA versus LITA. Non-English language studies were excluded. Search Strategy MEDLINE (1950 to August 1, 2012) was searched to identify studies relevant to our research question. Search terms used alone or in combination included diabetes, coronary artery bypass grafting, coronary bypass, CABG, mammary artery, internal mammary artery, unilateral, bilateral, coronary artery, mediastinitis, and sternal in- fection. We limited the search results with a strategy to identify clinical trials, randomized controlled trials, and Accepted for publication Nov 19, 2012. Address correspondence to Dr Deo, Division of Cardiovascular Surgery, Mayo Clinic, Rochester, MN 55901; e-mail: [email protected]. © 2013 by The Society of Thoracic Surgeons 0003-4975/$36.00 Published by Elsevier Inc http://dx.doi.org/10.1016/j.athoracsur.2012.11.068 ADULT CARDIAC

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
AD
ULT
CA
RD
IAC
Bilateral Internal Thoracic Artery Harvest and DeepSternal Wound Infection in Diabetic PatientsSalil V. Deo, MS, MCh, Ishan K. Shah, MBBS, Shannon M. Dunlay, MD, MS,Patricia J. Erwin, MLS, Chaim Locker, MD, Salah E. Altarabsheh, MD,Barry A. Boilson, MD, Soon J. Park, MD, and Lyle D. Joyce, MD, PhD
Divisions of Cardiovascular Surgery and Cardiovascular Diseases, and Medical Education, Mayo Clinic, Rochester, Minnesota; andDivision of Cardiovascular Surgery, Princess Alia Heart Institute, Amman, JordanBackground. Coronary artery bypass graft surgery issuperior to percutaneous intervention in diabetic pa-tients with multivessel disease. The use of bilateralinternal thoracic arteries (BITA) may provide better long-term graft patency, but the risk of postoperative deepsternal wound infection has limited its use in diabeticpatients. However, studies have reported conflicting re-sults, and require systematic evaluation.
Methods. MEDLINE, EMBASE, World of Science, andthe Cochrane library were searched for randomized con-trolled trials and observational studies comparing theincidence of deep sternal wound infection in diabeticpatients undergoing either left internal thoracic artery(LITA) or BITA harvest. We used random effect modelsto compare risk ratios within groups.
Results. One randomized controlled trial and 10 obser-vational studies (126,235 diabetic patients: 122,465 LITA,3,770 BITA) met inclusion criteria. Deep sternal wound
infection occurred in 3.1% and 1.6% for the BITA andMayo Clinic, Rochester, MN 55901; e-mail: [email protected].
© 2013 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
LITA cohorts, respectively. The risk ratio for deep sternalwound infection development was 1.71 (1.37 to 2.14) forBITA compared with LITA. Patients who underwentskeletonized BITA harvest had a similar risk of deepsternal wound infection compared with LITA (0.9 [0.42to 2.09]), although pedicled harvest demonstrated in-creased risk (1.77 [1.4 to 2.23]). Early mortality wascomparable in the LITA cohort (2.5%) and the BITAcohort (2.3%; p � 0.8).
Conclusions. The risk of deep sternal wound infectioncan be minimized in diabetic patients undergoing coro-nary artery bypass graft surgery by performing ITAharvested in a skeletonized manner with meticulousattention to preserving sternal blood flow. Pedicled har-vest is to be discouraged when utilizing both ITA owingto a significant increase in the risk of postoperative deepsternal wound infection.
(Ann Thorac Surg 2013;95:862–9)
© 2013 by The Society of Thoracic SurgeonsCoronary artery bypass graft surgery (CABG) hasdemonstrated superior long-term survival com-
pared with percutaneous therapy for diabetic patientswith multivessel disease [1]. Whereas the conventionalstrategy has been to utilize the left internal thoracicartery (LITA) for grafting to the left anterior descendingartery, studies have demonstrated the long-term benefitof bilateral internal thoracic artery (BITA) use for CABG[2, 3]. Unfortunately, the pedicled method of LITA har-vest may reduce sternal blood flow and impair woundhealing [4], and the primary reason for avoiding the useof BITA is the risk of deep sternal wound infection(DSWI), which is particularly high among diabetic pa-tients [5]. The meticulous skeletonized technique of ITAharvest was introduced to preserve sternal blood flow,and proponents believe that BITA harvest in this mannerwill not increase the risk of DSWI.
However, available observational studies demonstrateconflicting results. Hence, we have conducted a system-atic review and meta-analysis to compare the risk ofDSWI in diabetic patients undergoing CABG with BITA
Accepted for publication Nov 19, 2012.
Address correspondence to Dr Deo, Division of Cardiovascular Surgery,
versus LITA, and to evaluate the impact of a pedicledversus a skeletonized BITA harvest on infection risk.
Material and Methods
Eligibility CriteriaRandomized controlled trials (RCT) or observationalstudies were eligible if they met the following criteria: (1)adult human subjects; (2) patients underwent isolatedCABG, either on pump or off pump; and (3) studyreported deep sternal wound infection, need for reex-ploration for bleeding, in-hospital mortality, or 30-daymortality in a group with BITA versus LITA. Non-Englishlanguage studies were excluded.
Search StrategyMEDLINE (1950 to August 1, 2012) was searched toidentify studies relevant to our research question. Searchterms used alone or in combination included diabetes,coronary artery bypass grafting, coronary bypass, CABG,mammary artery, internal mammary artery, unilateral,bilateral, coronary artery, mediastinitis, and sternal in-fection. We limited the search results with a strategy to
identify clinical trials, randomized controlled trials, and0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2012.11.068

863Ann Thorac Surg DEO ET AL2013;95:862–9 STERNAL INFECTION IN DIABETIC PATIENTS
AD
ULT
CA
RD
IAC
observational/cohort studies. Using a similar strategy,EMBASE, Scopus, and the Cochrane Library were alsoqueried through August 1, 2012. References of relevantarticles were also reviewed.
Study SelectionTwo reviewers (I.K.S., S.V.D.) independently screened allstudies for inclusion. In duplicate, these reviewers firstscreened titles and abstracts, then retrieved potentiallyeligible records in full text and considered those forinclusion. Disagreements were resolved by consensus.Agreement between reviewers regarding study inclusionwas assessed using the Cohen � statistic.
Data AbstractionData were abstracted from the articles using a prespeci-fied data abstraction form. Quality of included studieswas assessed with the Newcastle-Ottawa scale for obser-vational studies and the Jadad scale for randomizedcontrolled trials.
OutcomesDeep sternal wound infection was defined by the variousauthors to include any one of the following: isolation ofan organism from culture of mediastinal tissue or fluid,visual evidence of mediastinitis, chest instability, or feverassociated with the presence of purulent drainage [6].
Statistical AnalysisWe used the software Review Manager 5.1 (RevMan5.1, Cochrane Collaboration, Copenhagen, Denmark).The meta-analysis has been reported according to thePreferred Reporting Items for Systematic Reviews andMeta-Analyses guidelines [7]. Each dichotomous out-come is reported as a risk ratio (RR) with a 95%confidence interval (CI). Aggregation of the overallrates of the outcomes of interest was performed withthe Mantel-Haenszel method [8]. Yates correction wasimplemented if a cell contained a zero in the 2 � 2contingency table [9]. Studies without events in bothcases and control groups cannot contribute to themeta-analytic component [10]. Random-effects modelswere chosen over fixed effects models (which generallygive more narrow CI), as their assumptions account forthe presence of variability among studies. Results fromrandomized trials and observational studies were firstpooled separately for each outcome. Then a formal testfor interaction between the pooled estimates was per-formed, and if not significant, results from trials andobservational studies were pooled.
For determining long-term survival, the hazard ratiowith 95% CI for all-cause mortality was abstracted fromthe studies that presented long-term outcome data.When this information was not readily available, indirectmethods initially described [11] and simplified by Tier-ney and colleagues [12] were implemented to obtain anobserved-expected and variance values from the avail-able data. The pooled hazard ratio was then obtainedfrom the observed-expected and variance values using
the Peto method, which is a fixed-effects model.We used the I2 statistic, which estimates the percent-age of total variation across studies that is due to heter-ogeneity rather than chance. Suggested thresholds forheterogeneity were used, with I2 values of 25% to 49%,50% to 74%, and 75% or greater indicative of low, mod-erate, and high heterogeneity [13]. Publication bias wasassessed using the Funnel plot method. A p value of lessthan 0.05 was used as the level of significance for allanalyses.
Forest plots are graphical representations of the riskratios from each study along with the pooled event rateand risk ratio obtained after statistical analysis. Thesquare box depicts the weight of each study, with thehorizontal lines depicting the range of the individual riskratios with 95% CI. The diamond demonstrates thepooled risk ratio with 95% CI.
Results
Search Results and Study CharacteristicsThe search identified 267 potentially relevant citations(Fig 1). After review, nine articles were eligible for inclu-sion. An additional two studies were included afterreference list review [14–24]. The � statistic for the finalprocess of selection was 0.90. The studies were graded forquality as per the Newcastle-Ottawa scale. This methoduses three criteria—selection, comparability and out-come—to determine the quality of the study. A star isgiven for each point, and the maximum score that a studycan obtain is 9. Further information regarding the scalecan be obtained online [25].
The characteristics of included studies are shown inTables 1 and 2. One RCT and 10 observational studies(126,235 diabetic patients: 122,465 in the LITA cohort and3,770 in the BITA cohort) were analyzed to obtain thepooled estimates.
ITA Harvest TechniqueThe technique of ITA harvest has been explicitly statedin the majority of the articles. Skeletonized bilateralharvest of the ITA was performed by five groups [15,18, 20, 23, 24], whereas two studies adopted a pedicledITA harvest with a careful consideration toward pre-serving sternal perfusion [14, 16]. The article by Tag-gart and coworkers [21] is a RCT conducted on amultiple-institution basis; as the technique of ITAharvest is not clearly mentioned, we consider that apedicled approach was utilized as this is presently theconventional method for ITA harvest. A similar pre-sumption was utilized in the article written by Savageand colleagues [19] analyzing The Society of ThoracicSurgeons database, a multiple-institution pooled data-base. Puskas and colleagues [17] mention that ITAharvest was surgeon dependent but do not describeevents stratified by the technique of harvest. Individ-ual communication from the respective authors of theabove articles also confirmed an inability to stratify thepatients as per technique of ITA harvest. To determine
if this assumption changed the results of our overall
864 DEO ET AL Ann Thorac SurgSTERNAL INFECTION IN DIABETIC PATIENTS 2013;95:862–9A
DU
LTC
AR
DIA
C
study, we performed sensitivity analysis and comparedrisk ratios including and excluding the three studies.
Deep Sternal Infection Comparing LITA and BITAHarvestData regarding the incidence of DWSI were availablefrom all 11 studies. The RR of developing DSWI forpatients undergoing BITA harvest was 1.71 (1.37 to2.14; p � 0.001) as compared with patients undergoingLITA alone (Fig 2A). Heterogeneity was not observed(I2 � 0%). The funnel plot was symmetric (Fig 2B),indicating an absence of publication bias. There was nodifference in results observed from the RCT versus thecohort studies (p value for interaction � 0.34).
Five studies compared the risk of DSWI after skeleton-ized BITA versus LITA harvest. The pooled incidence ofDSWI was 2.8%, 3.1%, and 2.3% in the skeletonized BITA,pedicled BITA, and LITA groups, respectively. The risk ofDSWI was similar among patients undergoing skeleton-ized BITA versus LITA (RR 0.94, 95% CI: 0.42 to 2.09; Fig3A). However, studies where a pedicled approach wasimplemented or presumed were associated with in-creased risk of DSWI compared with LITA (RR 1.82, 95%CI: 1.42 to 2.33; Fig 3B). Sensitivity analysis of the pedi-
Records iden�fied database searching(n =5470)
Scre
enin
g In
clud
ed
Elig
ibili
ty
Iden
�fic
a�on
R(
Fig 1. Flowchart from the PRISMAguidelines demonstrates the methodfor selection of the included articles.From Moher et al [7]. For more in-formation, go to: www.prisma-state-ment.org. (BITA � bilateral internalthoracic artery; LITA � left internalthoracic artery.)
cled cohort including and excluding the articles by Tag-
gart and coworkers [21], Savage and associates [19], andPuskas and coworkers [17] was not statistically significant(p � 0.64).
MortalityIn-hospital and 30-day mortality was reported in sixstudies (2,808 patients in the BITA cohort and 121,099 inthe LITA cohort). There was no difference in observedmortality among patients undergoing BITA versus LITA(Fig 4).
Reexploration for BleedingOnly two studies [16, 24] reported on the need forreexploration for mediastinal bleeding. The risk ofreexploration after BITA harvest was increased ascompared with LITA harvest with a RR of 2.00 (95% CI:1.12 to 3.56). Although Kinoshita and associates [24]have utilized a skeletonized technique, Momin andcolleagues [16] have implemented a pedicled methodof ITA harvest.
Late MortalityFour studies discussed the long-term results of BITA
h Addi�onal records iden�fied through other sources (n =5)
s a�er duplicates removed )
Records Screened (n = 267)
Records Excluded (n =230)
Full-text ar�cles assessed for Eligibility (n = 37)
Full-text ar�cles excluded, with Reasons (n = 26) Reasons for exclusion: 1. Ar�cle related to only either BITA or LITA = 15 2. Review ar�cle=2 3. Poor Quality of the ar�cle=3 4. Le�er to Editor=1 5. Editorial comment=1 6. Non-English ar�cle without transla�on=2 7. Inability to iden�fy events in the diabe�c subgroup of pa�ents =2
Studies included in qualita�ve Synthesis (n = 9)
Studies included in quan�ta�ve Synthesis (meta-analysis) (n = 11)
throug
ecordn =267
grafting in diabetic patients as compared with the use of
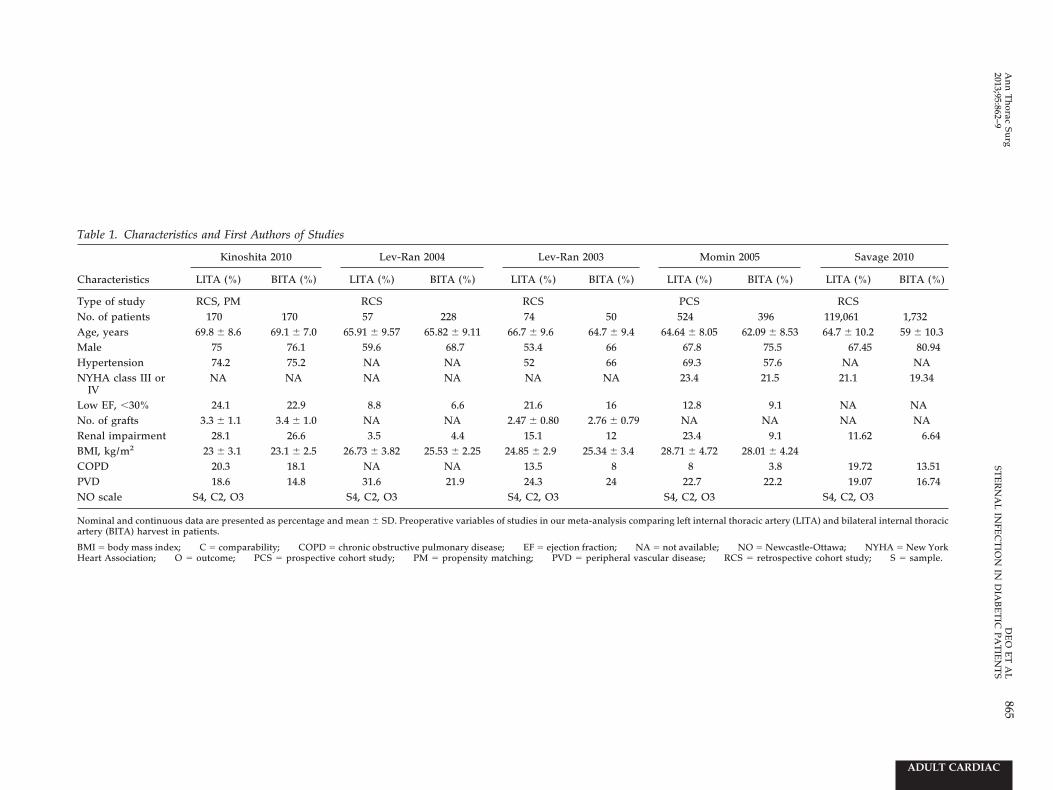
Table 1. Characteristics and First Authors of Studies
Characteristics
Kinoshita 2010 Lev-Ran 2004 Lev-Ran 2003 Momin 2005 Savage 2010
LITA (%) BITA (%) LITA (%) BITA (%) LITA (%) BITA (%) LITA (%) BITA (%) LITA (%) BITA (%)
Type of study RCS, PM RCS RCS PCS RCSNo. of patients 170 170 57 228 74 50 524 396 119,061 1,732Age, years 69.8 � 8.6 69.1 � 7.0 65.91 � 9.57 65.82 � 9.11 66.7 � 9.6 64.7 � 9.4 64.64 � 8.05 62.09 � 8.53 64.7 � 10.2 59 � 10.3Male 75 76.1 59.6 68.7 53.4 66 67.8 75.5 67.45 80.94Hypertension 74.2 75.2 NA NA 52 66 69.3 57.6 NA NANYHA class III or
IVNA NA NA NA NA NA 23.4 21.5 21.1 19.34
Low EF, �30% 24.1 22.9 8.8 6.6 21.6 16 12.8 9.1 NA NANo. of grafts 3.3 � 1.1 3.4 � 1.0 NA NA 2.47 � 0.80 2.76 � 0.79 NA NA NA NARenal impairment 28.1 26.6 3.5 4.4 15.1 12 23.4 9.1 11.62 6.64BMI, kg/m2 23 � 3.1 23.1 � 2.5 26.73 � 3.82 25.53 � 2.25 24.85 � 2.9 25.34 � 3.4 28.71 � 4.72 28.01 � 4.24COPD 20.3 18.1 NA NA 13.5 8 8 3.8 19.72 13.51PVD 18.6 14.8 31.6 21.9 24.3 24 22.7 22.2 19.07 16.74NO scale S4, C2, O3 S4, C2, O3 S4, C2, O3 S4, C2, O3 S4, C2, O3
Nominal and continuous data are presented as percentage and mean � SD. Preoperative variables of studies in our meta-analysis comparing left internal thoracic artery (LITA) and bilateral internal thoracicartery (BITA) harvest in patients.
BMI � body mass index; C � comparability; COPD � chronic obstructive pulmonary disease; EF � ejection fraction; NA � not available; NO � Newcastle-Ottawa; NYHA � New YorkHeart Association; O � outcome; PCS � prospective cohort study; PM � propensity matching; PVD � peripheral vascular disease; RCS � retrospective cohort study; S � sample.
865A
nn
Th
oracSu
rgD
EO
ET
AL
2013;95:862–9ST
ER
NA
LIN
FEC
TIO
NIN
DIA
BE
TIC
PA
TIE
NT
S
ADULT CARDIAC

Table 2. Characteristics and First Authors of Studies
Characteristics
De Paulis 2005 Tavolacci 2003 Taggart 2010a Gansera 2001 Puskas 2012 Wendler 2001b
LITA (%) BITA (%) LITA (%) BITA (%) LITA (%) BITA (%) LITA (%) BITA (%) LITA (%) BITA (%) DM (%) NDM (%)
Type of study RCS RCS RCT RCS RCS RCSNo. of patients 450 450 177 79 1,554 1,318 2,184 1,487 2,715 812 174 402Age, years 62.1 � 8.5 56.2 � 10.3 69 � 7.6 60 � 8.6 63.5 � 9.1 63.7 � 8.7 65.5 � 9.0 64.4 � 9.4 63.9 � 10.8 58.4 � 10.1 63 � 8 62 � 9Male 84.4 88.6 77.7 78.2 86.1 85.1 76.3 81.4 67 84 68 83Hypertension 40 37 NA NA 78.3 77.1 NA NA 86.29 79.92 NA NANYHA class III
or IVNA NA NA NA 20.8 22.3 NA NA NA NA NA NA
LVEF 52 � 10 53 � 11 NA NA NA NA 60.6 � 15.1 62.1 � 14.6 49.7 � 12.8 51.7 � 11.2 55 � 16 60 � 16No. of grafts 2.7 � 0.5 2.8 � 0.4 NA NA 81.74%c 81.7%c NA NA NA NA 93%c 83%c
Renal disease 2.8 7.7 NA NA NA NA 0.6 0.9 11.86 4.06 9.5 8.5Diabetes
mellitus27.5% 29.1 NA NA 23.4 23.9 27 28.1 44.67 28.57 100 0
BMI, kg/m2 27.6 � 12 27 � 3.5 NA NA 28.1 � 4.1 28.3 � 4.0 26.6 � 3.3 26.9 � 3.4 29.5 � 6.4 28.9 � 5.0 NA NACOPD 5.3 16 NA NA NA NA NA NA 16.79 7.88 NA NAPVD 13.1 14.2 NA NA 7.6 6.6 NA NA 15.87 11.08 16 11NO scale S4, C1, O3 S3, C2, O3 NA S3, C1, O3 S4, C2, O3 S3, C1, C3
a Taggart, being a randomized control trial (RCT), cannot be graded using the Newcastle-Ottawa (NO) scale. b Wendler present preoperative characteristics stratified by the presence of diabetesmellitus. c Percentage of patients having more than three grafts.
Nominal and continuous data are presented as percentage and mean � SD. Preoperative variables of studies in our meta-analysis comparing left internal thoracic artery (LITA) and bilateral internal thoracicartery (BITA) harvest in patients. The diabetic patients in these articles are a subset of the entire study.
BMI � body mass index; C � comparability; COPD � chronic obstructive pulmonary disease; DM � diabetes mellitus; LVEF � left ventricular ejection fraction; NA � notavailable; NDM � no diabetes mellitus; NYHA � New York Heart Association; O � outcome; PVD � peripheral vascular disease; RCS � retrospective cohort study; S � sample.
866D
EO
ET
AL
An
nT
horac
Surg
STE
RN
AL
INFE
CT
ION
IND
IAB
ET
ICP
AT
IEN
TS
2013;95:862–9
ADULTCARDIAC

867Ann Thorac Surg DEO ET AL2013;95:862–9 STERNAL INFECTION IN DIABETIC PATIENTS
AD
ULT
CA
RD
IAC
a single thoracic artery [17, 18, 23, 24]. Whereas twoarticles presented data at the end of 5 years [18, 24],survival was compared for a period of 7 and 8 years byLev Ran and associates [23] and Puskas and colleagues[17], respectively. Patients who received BITA had
improved long-term survival compared with those whoreceived LITA (hazard ratio 0.46, 95% CI: 0.37 to 0.57; p �0.0001; I2 � 24%}. However, as these results are based onobservational studies, selection bias may have impactedthe differences in observed outcome.
Fig 2. (A) Forest plot demonstrating the riskratio of deep sternal wound infection betweenleft internal thoracic artery (LITA) and bilat-eral internal thoracic artery (BITA) harvest inthe included studies. The pooled estimate with95% confidence intervals (CI) is depicted as adiamond. (B) The symmetry of the funnel plotdemonstrates absence of publication bias inthe included studies. (RR � risk ratio.)
Fig 3. Forest plots demonstrating the risk ratiofor deep sternal wound infection in patientsundergoing (A) skeletonized (SK) bilateral in-ternal thoracic artery (BITA) harvest and (B)pedicled (PD) BITA harvest. (CI � confidenceinterval; LITA � left internal thoracic artery.)

868 DEO ET AL Ann Thorac SurgSTERNAL INFECTION IN DIABETIC PATIENTS 2013;95:862–9A
DU
LTC
AR
DIA
C
Comment
Coronary artery bypass grafting is superior to percu-taneous intervention in diabetic patients with multi-vessel disease [26], with the ITA providing the incre-mental benefit [27]. The innate resistance of the ITA toatherosclerosis, intimal hyperplasia, and medial calci-fication [28] persists in diabetic patients, who demon-strate a tendency toward increased vasoreactivity andocclusion of saphenous vein grafts [29]. Although theuse of BITA increases long-term survival [2, 3], it hasalso been associated with increased risk of DWSI andmediastinitis [30].
This systematic review and meta-analysis of 11 studiesevaluating the risk of DWSI in diabetic patients under-going CABG with BITA versus LITA demonstrates im-portant results. While BITA was associated with in-creased risk of DSWI compared with LITA, this waslimited to patients with a pedicled harvesting approach,whereas patients treated with skeletonized harvest hadno difference in risk of DWSI compared with patientstreated with LITA. Based on these results, BITA using askeletonized approach may confer the benefits of im-proved long-term graft patency while minimizing asso-ciated risk of DSWI. We also found no difference inshort-term mortality among diabetic patients treatedwith BITA versus LITA in this study.
The technique of skeletonization during BITA harvestdid not increase the risk of DSWI as compared with theharvest of a single internal thoracic artery. Isolated stud-ies comparing sternal blood flow after skeletonized BITAharvest have demonstrated improved flow after skeleton-ized bilateral harvest compared with the pedicledmethod [31], but this is likely one of the many factors indetermining occurrence of DSWI as studies demonstrat-ing similar flows have also been reported [32].
The present meta-analysis pools data from 11 studies,each having small individual rates of DSWI. Only onerandomized trial comparing single versus bilateral ITA indiabetic patients [21] has been performed and was in-cluded in our review. The 10 remaining studies areobservational in nature, and hence, the feasibility of BITAbased on coronary anatomy, patient factors, and surgeonpreference may have influenced the choice of single orbilateral ITA grafting. Nevertheless, we believe that theincluded studies are quite representative of the averagepatient undergoing CABG. Patients with chronic obstruc-tive airway disease, obesity, on steroid therapy, and withpoor left ventricular ejection fraction have been repre-
Fig 4. Forest plot demonstrating the risk ratiofor early/30-day mortality in patients under-going left internal thoracic artery (LITA) andbilateral internal thoracic artery (BITA) har-vest in the included studies. (CI � confidenceinterval.)
sented in the pooled study group.
The long-term survival benefit of bilateral internalthoracic artery over the use of a single internal thoracicartery is well established in the literature. In our pooledstudy, long-term mortality was only examined in BITAversus LITA in four cohort studies. This pooled analysisresulted in a 54% decreased risk of long-term mortality indiabetic patients treated with BITA rather than a singleinternal thoracic artery. The Kaplan-Meier survival curveby Puskas and colleagues [17] demonstrates that thesurvival advantage improves over the follow-up period.However, while one study [24] did attempt to minimizethe impact of selection bias on differences in observedoutcomes by performing a propensity-based analysis, wecannot exclude the possibility that lower risk patientswere treated with BITA. This inherent selection bias mayvery well have contributed to our observed results. Tag-gart and investigators [21] from the Arterial Revascular-ization Trial group are conducting the first randomizedmultiple-institution controlled trial comparing outcomeof BITA and LITA, with 10-year mortality as their primaryendpoint. Their preliminary 1-year data have suggestedthat diabetic patients treated with BITA have improvedsurvival compared with a single internal thoracic artery,and final results are awaited [21]. That should encouragesurgeons to offer this option to diabetic patients under-going coronary artery bypass grafting in spite of theslightly higher risk of sternal wound infection in the earlypostoperative period.
Study Limitation and StrengthsThis systematic review and meta-analysis does havesome limitations. Most included studies were observa-tional in nature, and patient selection for specific thera-pies may contribute to results observed. However, theresults from the sole RCT included did not differ signif-icantly from the other studies. Furthermore, we did notobserve any significant heterogeneity in our pooled re-sults, underscoring the robustness of our data despite apredominance of cohort studies. We also could not eval-uate the role that postoperative glycemic control playedin the outcomes observed. However, we have no reasonto believe this would systematically differ between pa-tients treated with BITA versus LITA. While our review isat high risk of publication bias given the inclusion ofobservational studies containing small numbers of pa-tients, our funnel plot findings did not point towardsignificant publication bias in results. Three studies didnot explicitly state the technique of BITA harvest, and we
assumed that a pedicled method was implemented. Yet,
869Ann Thorac Surg DEO ET AL2013;95:862–9 STERNAL INFECTION IN DIABETIC PATIENTS
AD
ULT
CA
RD
IAC
sensitivity analysis failed to demonstrate a significantchange in risk ratios with this assumption.
However, this analysis also has several strengths. Thisis the first systematic review and meta-analysis to ad-dress the important clinical question of whether BITAincreases the risk of DSWI in diabetic patients, and toinvestigate whether risk may be minimized using askeletonized approach. By pooling data from a number ofsmall studies, we have demonstrated that the excess riskof DSWI with BITA is attributable to use of a pedicledapproach.
In conclusion, the risk of DSWI can be minimized indiabetic patients undergoing CABG by performing ITAharvested in a skeletonized manner with meticulousattention to preserving sternal blood flow. Pedicled har-vest is to be discouraged when utilizing BITA owing to asignificant increase in the risk of postoperative DSWI.
References
1. Bypass Angioplasty Revascularization Investigation (BARI)Investigators. Comparison of coronary bypass surgery withangioplasty in patients with multivessel disease. N EnglJ Med 1996;335:217–25.
2. Pick AW, Orszulak TA, Anderson BJ, Schaff HV. Singleversus bilateral internal mammary artery grafts: 10-yearoutcome analysis. Ann Thorac Surg 1997;64:599–605.
3. Lytle BW, Blackstone EH, Loop FD, et al. Two internalthoracic artery grafts are better than one. J Thorac Cardio-vasc Surg 1999;117:855–72.
4. Parish MA, Asai T, Grossi EA, et al. The effects of differenttechniques of internal mammary artery harvesting on ster-nal blood flow. J Thorac Cardiovasc Surg 1992;104:1303–7.
5. Mastrobuoni S, Gawad N, Price J, et al. Use of bilateralinternal thoracic artery during coronary artery bypass graftsurgery in Canada: the bilateral internal thoracic arterysurvey. J Thorac Cardiovasc Surg 2012;144:874–9.
6. Mangram AJ, Horan TC, Pearson ML, SIlver LC, Jarvis WR.Guideline for prevention of surgical site infection, 1999.Hospital Infection Control Practices Advisory Committee.Infect Cont Hosp Epidemiol 1999;20:250–78.
7. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferredreporting items for systematic reviews and meta-analyses:the PRISMA statement. PLoS Med 2009;6:e1000097.
8. Mantel N, Haenszel W. Statistical aspects of the analysis ofdata from retrospective studies of disease. J Natl Cancer Inst1959;22:719–48.
9. Friedrich JO. Adhikari NK, Beyene J. Inclusion of zero totalevent trials in meta-analyses maintains analytic consistencyand incorporates all available data. BMC Med Res Methodol2007;7:5.
10. Higgins JPT, Green S, eds. Cochrane handbook for system-atic reviews of interventions, version 5.1.0. The CochraneCollaboration, 2011. Available from: www.cochrane-handbook.org.
11. Parmar MK, Torri V, Stewart L. Extracting summary statis-tics to perform meta-analyses of the published literature forsurvival endpoints. Stat Med 1998;17:2815–34.
12. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR.Practical methods for incorporating summary time-to-eventdata into meta-analysis. Trials 2007;8:16.
13. Higgins JP, Thompson SG, Deeks JJ, ALtman DG. Measuringinconsistency in meta-analyses. BMJ 2003;327:557–60.
14. Gansera B, Gunzinger R, Angelis I, et al. End of the millen-nium. End of the single thoracic artery graft? Two thoracicarteries—standard for the next millennium? Thorac Cardio-vasc Surg 2001;49:10–5.
15. Wendler O, Hennen B, Markwirth T, et al. Complete arterialrevascularization in the diabetic patient: early postoperativeresults. Thorac Cardiovasc Surg 2001;49:5–9.
16. Momin AU, Deshpande R, Potts J, et al. Incidence of sternalinfection in diabetic patients undergoing bilateral internalthoracic artery grafting. Ann Thorac Surg 2005;80:1765–72.
17. Puskas JD, Sadiq A, Vassiliades TA, Kilgo PD, Lattouf OM.Bilateral internal thoracic artery grafting is associated withsignificantly improved long-term survival, even among dia-betic patients. Ann Thorac Surg 2012;94:710–6.
18. Lev-Ran O, Mohr R, Amir K, et al. Bilateral internal thoracicartery grafting in insulin-treated diabetics: should it beavoided? Ann Thorac Surg 2003;75:1872–7.
19. Savage EB, Grab JD, O’Brien SM, et al. Use of both internalthoracic arteries in diabetic patients increases deep sternalwound infection. Ann Thorac Surg 2007;83:1002–6.
20. De Paulis R, de Notaris S, Scaffa R, et al. The effect ofbilateral internal thoracic artery harvesting on superficialand deep sternal infection: the role of skeletonization. J Tho-rac Cardiovasc Surg 2005;129:536–43.
21. Taggart DP, Altman DG, Gray AM, et al. Randomized trial tocompare bilateral versus single internal mammary coronaryartery bypass grafting: 1-year results of the Arterial Revas-cularisation Trial (ART). Eur Heart J 2010;31:2470–81.
22. Tavolacci MP, Merle V, Josset V, et al. Mediastinitis aftercoronary artery bypass graft surgery: influence of the mam-mary grafting for diabetic patients. J Hosp Infect 2003;55:21–5.
23. Lev-Ran O, Braunstein R, Nesher N, et al. Bilateral versussingle internal thoracic artery grafting in oral-treated dia-betic subsets: comparative seven-year outcome analysis.Ann Thorac Surg 2004;77:2039–45.
24. Kinoshita T, Asai T, Nishimura O, et al. Off-pump bilateralversus single skeletonized internal thoracic artery grafting inpatients with diabetes. Ann Thorac Surg 2010;90:1173–9.
25. Newcastle-Ottawa scale. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
26. Brooks MM, Jones RH, Bach RG, et al, for the BARI Inves-tigators. Predictors of mortality and mortality from cardiaccauses in the Bypass Angioplasty Revascularization Investi-gation (BARI) randomized trial and registry. Circulation2000;101:2682–9.
27. Endo M, Tomizawa Y, Nishida H. Bilateral versus unilateralinternal mammary revascularization in patients with diabe-tes. Circulation 2003;108:1343–9.
28. Kaufer E, Factor SM, Frame R, Brodman RF. Pathology of theradial and internal thoracic arteries used as coronary arterybypass grafts. Ann Thorac Surg 1997;63:1118–22.
29. Karasu C, Soncul H, Altan VM. Effects of non-insulin depen-dent diabetes mellitus on the reactivity of human internalmammary artery and human saphenous vein. Life Sci 1995;57:103–12.
30. Grossi EA, Esposito R, Harris LJ, et al. Sternal woundinfections and use of internal mammary artery grafts. J Tho-rac Cardiovasc Surg 1991;102:342–7.
31. Dos Santos Filho EC, Moraes Neto FR, Silva RA, Moraes CR.Should the diabetics have the internal thoracic artery skel-etonized? Assessment of sternal perfusion by scintillogra-phy. Revista Brasil Cirurg Cardiovasc 2009;24:157–64.
32. Nishi H, Mitsuno M, Tanaka H, et al. Decreasing sternum
microcirculation after harvesting the internal thoracic artery.Eur J Cardiothorac 2011;40:240–4.
Related Documents