Original Article Betahistine Exacerbates Amikacin Ototoxicity Annals of Otology, Rhinology & Laryngology 1–8 © The Author(s) 2014 Reprints and permissions: sagepub.com/journalsPermissions.nav DOI: 10.1177/0003489414557020 aor.sagepub.com Fadlullah Aksoy, MD 1 , Remzi Dogan, MD 2 , Orhan Ozturan, MD 1 , Yavuz Selim Yildirim, MD 1 , Bayram Veyseller, MD 1 , Alper Yenigun, MD 3 , and Burak Ozturk, MD 4 Abstract Objective: Betahistine augments cochlear blood flow and is currently used as an efficient therapeutic agent. Amikacin is used in a wide range of areas, but its ototoxic effect continues to be problematic. This study investigates the effect of betahistine on amikacin-induced ototoxicity. Methods: Thirty-two healthy rats were randomized to 4 groups of 8 rats in each group (amikacin, amikacin + betahistine, betahistine, and no treatment). Amikacin was administered intramuscularly to groups 1 and 2 for 14 days. Betahistine was delivered by oral gavage to groups 2 and 3 for 21 days. Distortion-product otoacoustic emissions (DPOAE) and auditory brainstem response (ABR) tests were conducted on all rats. Results: There were significant decreases in the DPOAE levels and significant increases in the ABR thresholds of the amikacin and amikacin + betahistine groups on the 7th, 14th, and 21st days, as compared to their basal values. The DPOAE levels of the amikacin + betahistine group significantly decreased on days 7, 14, and 21, and the ABR thresholds significantly increased on the same days, as compared to the amikacin group. Conclusion: Our study implies that amikacin’s ototoxic effects are augmented by the concurrent use of betahistine. Experimental and clinical research, supported by histopathological studies, is needed to affirm our findings. Keywords ABR, amikacin, betahistine, DPOAE, ototoxicity Introduction Betahistine dihydrochloride augments cochlear blood flow by blocking histamine H3 receptors. 1 It also partially acti- vates postsynaptic histamine H1 and H2 receptors. 2 Betahistine dihydrochloride has a widespread use in the treatment of tinnitus and Ménière’s, since it enhances oxy- genation by augmenting blood flow to the inner ear. 3 It was demonstrated that betahistine was efficient in decreasing the frequency of attacks in Ménière’s disease. 4 Various experimental animal studies conducted with laser Doppler flowmetry demonstrated that betahistine aug- mented cochlear blood flow by inducing vasodilation at the inner ear, 5-7 whereas the systemic vascular effect of betahis- tine was in favor of a reduction of blood flow. 5 Studies showed that the clinical efficiency of betahistine and the amount of cochlear blood flow were dose related. 8,9 A recent study by Ihler et al 9 attested that betahistine doses of up to 160 mg/kg/day caused an increase in cochlear blood flow, whereas doses above that level produced no further changes. Amikacin is an antibiotic of the aminoglycoside group, used in a wide range of areas. 10-12 Amikacin is used for the treatment of severe infections, especially when a synergistic action is required, and with close observation of its ototoxic and nephrotoxic side effects. 13,14 After its injection, amika- cin permeates inner ear fluid where it damages the hair cells. 15 Typically, the ototoxic effect of amikacin is neurosenso- rial, nonsyndromic, bilateral, and progressive, and it affects the higher frequencies. 16 Previous studies demonstrated that chemicals that increased cochlear blood flow also increased the ototoxic effect of amikacin. 13,17 1 Bezmialem Vakif University, Department of Otorhinolaryngology, Fatih, Istanbul, Turkey 2 Bayrampasa State Hospital, Department of Otorhinolaryngology, Bayrampasa, Istanbul, Turkey 3 Karaman State Hospital, Department of Otorhinolaryngology, Karaman, Turkey 4 Bezmialem Vakif University, Faculty of Health Sciences, Department of Audiology, Fatih, Istanbul, Turkey Corresponding Author: Remzi Dogan, MD, Bayrampasa State Hospital, Department of Otorhinolaryngology, İsmetpasa mah, Kenar sokak, Bayrampasa, Istanbul 34094, Turkey. Email: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Downloaded from aor.sagepub.com by guest on October 31, 2014
Original Article
Betahistine Exacerbates Amikacin Ototoxicity
Annals of Otology, Rhinology & Laryngology 1–8 © The Author(s) 2014 Reprints and permissions: sagepub.com/journalsPermissions.nav DOI: 10.1177/0003489414557020 aor.sagepub.com
Fadlullah Aksoy, MD1, Remzi Dogan, MD2, Orhan Ozturan, MD1, Yavuz Selim Yildirim, MD1, Bayram Veyseller, MD1, Alper Yenigun, MD3, and Burak Ozturk, MD4
Abstract Objective: Betahistine augments cochlear blood flow and is currently used as an efficient therapeutic agent. Amikacin is used in a wide range of areas, but its ototoxic effect continues to be problematic. This study investigates the effect of betahistine on amikacin-induced ototoxicity. Methods: Thirty-two healthy rats were randomized to 4 groups of 8 rats in each group (amikacin, amikacin + betahistine, betahistine, and no treatment). Amikacin was administered intramuscularly to groups 1 and 2 for 14 days. Betahistine was delivered by oral gavage to groups 2 and 3 for 21 days. Distortion-product otoacoustic emissions (DPOAE) and auditory brainstem response (ABR) tests were conducted on all rats. Results: There were significant decreases in the DPOAE levels and significant increases in the ABR thresholds of the amikacin and amikacin + betahistine groups on the 7th, 14th, and 21st days, as compared to their basal values. The DPOAE levels of the amikacin + betahistine group significantly decreased on days 7, 14, and 21, and the ABR thresholds significantly increased on the same days, as compared to the amikacin group. Conclusion: Our study implies that amikacin’s ototoxic effects are augmented by the concurrent use of betahistine. Experimental and clinical research, supported by histopathological studies, is needed to affirm our findings.
Keywords ABR, amikacin, betahistine, DPOAE, ototoxicity
Introduction
Betahistine dihydrochloride augments cochlear blood flow by blocking histamine H3 receptors.1 It also partially acti- vates postsynaptic histamine H1 and H2 receptors.2
Betahistine dihydrochloride has a widespread use in the treatment of tinnitus and Ménière’s, since it enhances oxy- genation by augmenting blood flow to the inner ear.3 It was demonstrated that betahistine was efficient in decreasing the frequency of attacks in Ménière’s disease.4
Various experimental animal studies conducted with laser Doppler flowmetry demonstrated that betahistine aug- mented cochlear blood flow by inducing vasodilation at the inner ear,5-7 whereas the systemic vascular effect of betahis- tine was in favor of a reduction of blood flow.5 Studies showed that the clinical efficiency of betahistine and the amount of cochlear blood flow were dose related.8,9 A recent study by Ihler et al9 attested that betahistine doses of up to 160 mg/kg/day caused an increase in cochlear blood flow, whereas doses above that level produced no further changes.
Amikacin is an antibiotic of the aminoglycoside group, used in a wide range of areas.10-12 Amikacin is used for the treatment of severe infections, especially when a synergistic
action is required, and with close observation of its ototoxic and nephrotoxic side effects.13,14 After its injection, amika- cin permeates inner ear fluid where it damages the hair cells.15
Typically, the ototoxic effect of amikacin is neurosenso- rial, nonsyndromic, bilateral, and progressive, and it affects the higher frequencies.16 Previous studies demonstrated that chemicals that increased cochlear blood flow also increased the ototoxic effect of amikacin.13,17
1Bezmialem Vakif University, Department of Otorhinolaryngology, Fatih, Istanbul, Turkey 2Bayrampasa State Hospital, Department of Otorhinolaryngology, Bayrampasa, Istanbul, Turkey 3Karaman State Hospital, Department of Otorhinolaryngology, Karaman, Turkey 4Bezmialem Vakif University, Faculty of Health Sciences, Department of Audiology, Fatih, Istanbul, Turkey Corresponding Author: Remzi Dogan, MD, Bayrampasa State Hospital, Department of Otorhinolaryngology, İsmetpasa mah, Kenar sokak, Bayrampasa, Istanbul 34094, Turkey. Email: [email protected]

Downloaded from aor.sagepub.com by guest on October 31, 2014
2 Annals of Otology, Rhinology & Laryngology Betahistine dihydrochloride is prescribed in relatively
high doses and for long-term use. Amikacin use can be vitally important, especially in the treatment of resistant infections. When facing a necessity for the concurrent use of amikacin and betahistine, it is essential to know whether amikacin-induced ototoxicity and the resultant hearing loss will be more pronounced. The objective of our study is to evaluate the concurrent use of amikacin and betahistine with audiologic tests (otoacoustic emissions and auditory brainstem audiometry) and biochemical parameters to see whether the combination alters amikacin’s ototoxic effect. Our study aims to investigate the probable side effects when ototoxic drugs are used together with drugs increasing cochlear blood flow.
Materials and Methods
Experimental Design
After the approval of the Animal Research Local Ethics Committee, 32 healthy female Wistar Albino rats (200-240 g) were included in the study. Rats with a positive Preyer reflex were chosen, endoscopic ear examinations were con- ducted, and any rat with an outer or middle ear pathology was excluded from the study group. Rats were kept in an environment that was illuminated for 12 hours and dark- ened for 12 hours, had a temperature of 21°C ± 1°C, with free access to food and water, and with a background noise below 50 dB. The animals were used in accordance with The Guide for the Care and Use of Laboratory Animals.18
Rats were assigned to 4 groups with 8 rats in each group: group 1 (amikacin = AK), group 2 (amikacin + betahistine = AK+BTH), group 3 (betahistine = BTH), and group 4 (no treatment group = NTG). Betahistine dihydrochloride was administered to groups 2 and 3 for 21 days by oral gavage, at a dose of 48 mg/kg/day. Amikacin was administered intramuscularly to groups 1 and 2 for 14 days, at a dose of 600 mg/kg/day. No drugs were administered to group 4. At the beginning of the study, and at days 7, 14, and 21, all rats were anesthetized by intraperitoneal ketamine hydrochlo- ride (40 mg/kg) and xylazine (5 mg/kg), and distortion- product otoacoustic emissions (DPOAE) and auditory brainstem response (ABR) tests were conducted.
Audiologic Evaluation
DPOAE. The GSI Audera device was used for DPOAE mea- surements in evaluating the animals’ peripheral hearing. The smallest size elastic tympanometry probe was used for the rats. Emissions were performed in General Diagnostic mode, and both DPgram and input-output (I/O) measure- ments were taken. Otoacoustic emissions were measured using stimuli at different frequencies and intensities. Pri- mary stimulus intensities were adjusted to (veya equalized
at) 65 dB (L1 = L2). The 2 different frequencies (f1 and f2) were set as f2 / f1 = 1.10. The DPgram measurements were performed at frequencies of 3000, 4008, 5004, 6000, 6996, 8004, 9012, 10008, 11004, and 12000 Hz. During measure- ments, DPOAEs with a noise intensity of 3 dB and higher at 2f1-f2 frequency were accepted as positive. ABR. Auditory brainstem response measurements were con- ducted in a silent room with the Viasys Medelec Synergy device, using subdermal needle electrodes (Technomed Europe, Maastricht, the Netherlands). ER 3A insert ear- phones were used to provide click stimuli in alternating polarities. Filter was set at 30 to 1500 Hz, repetition rate was set at 21/sc, and the time window was set at 25 msc. For signal averaging, 1024 samples were taken. Initially, stimuli were presented at 80 dB nHL intensity, and the intensity level was reduced in 20 dB steps until close to the threshold value. Then, the intensity level was reduced in 10 dB steps until the threshold value was reached. At least 2 tracks were generated for each measurement to test behavior reproduc- ibility, and the thresholds were cross-checked. The ABR threshold was defined as the lowest intensity level where the III wave was observed. TAS, TOS, OSI Measurements
Measuring the total antioxidant status (TAS), the combined activity of all antioxidants, provides an overall evaluation of the entire antioxidant status.19 Total oxidant status (TOS) is an indicator of the overall oxidant status of the patients.20
Oxidant status index (OSI) is the ratio of TOS/TAS and is a mean to calculate oxidative stress in the body; comparing TAS and TOS is thought to be a better indicator of the over- all oxidative stress. For measuring those parameters, blood samples taken from all rats in all groups were centrifuged at 3000 cycles for 15 minutes, and the serum was separated and stored in −80°C. After all samples were thus prepared, TAS and TOS values were worked out with the relevant kit (Rel Assay Diagnostics, Gaziantep, Turkey), and OSI val- ues were calculated with the relevant formula (OSI = TOS / TAS × 100). Statistical Analysis
Statistical analysis was carried out using the Statistical Package for the Social Sciences version 16.0 software for Windows (SPSS Inc, Chicago, Illinois, USA). All quantita- tive variables were estimated using measures of central location (ie, mean and median) and measures of dispersion (ie, standard deviation [SD]). Data normality was checked using the Kolmogorov-Smirnov tests of normality.
One-way analysis of variance (ANOVA) was used for intergroup comparisons of DPOAE values, ABR values, and biochemical parameters (the difference among groups
Downloaded from aor.sagepub.com by guest on October 31, 2014
Aksoy et al 3
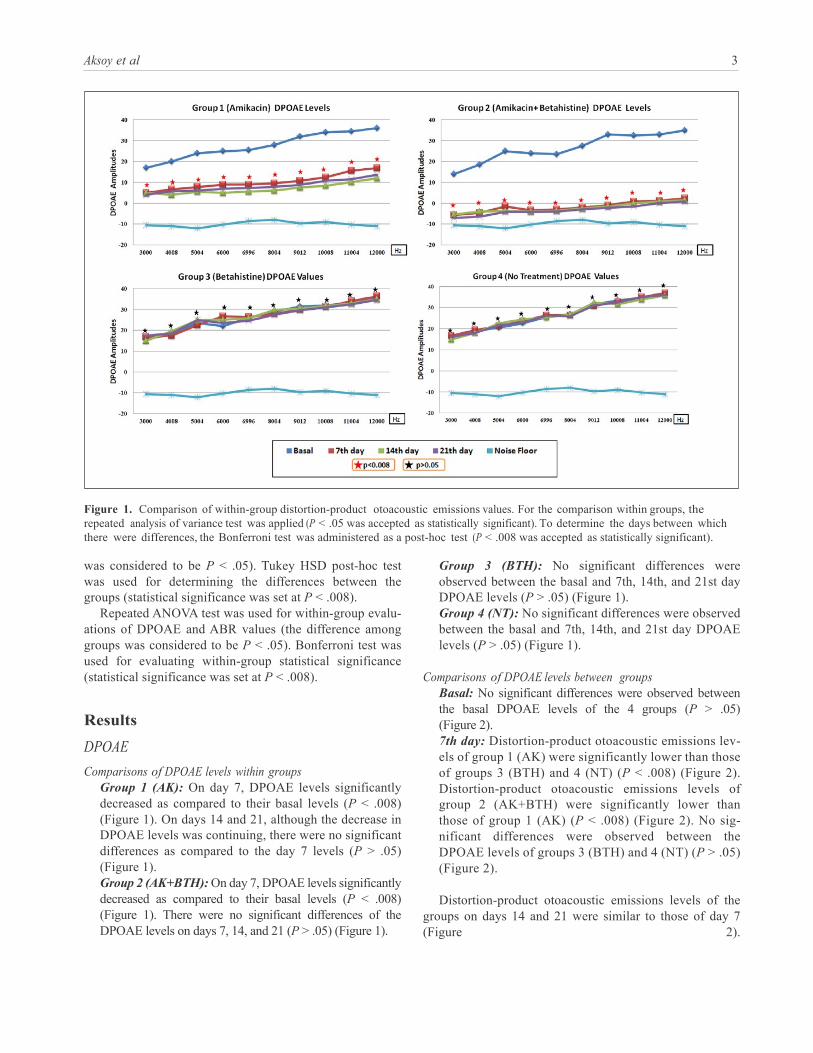
Figure 1. Comparison of within-group distortion-product otoacoustic emissions values. For the comparison within groups, the repeated analysis of variance test was applied (P < .05 was accepted as statistically significant). To determine the days between which there were differences, the Bonferroni test was administered as a post-hoc test (P < .008 was accepted as statistically significant).
was considered to be P < .05). Tukey HSD post-hoc test was used for determining the differences between the groups (statistical significance was set at P < .008).
Repeated ANOVA test was used for within-group evalu- ations of DPOAE and ABR values (the difference among groups was considered to be P < .05). Bonferroni test was used for evaluating within-group statistical significance (statistical significance was set at P < .008).
Results
DPOAE
Comparisons of DPOAE levels within groups Group 1 (AK): On day 7, DPOAE levels significantly decreased as compared to their basal levels (P < .008) (Figure 1). On days 14 and 21, although the decrease in DPOAE levels was continuing, there were no significant differences as compared to the day 7 levels (P > .05) (Figure 1). Group 2 (AK+BTH): On day 7, DPOAE levels significantly decreased as compared to their basal levels (P < .008) (Figure 1). There were no significant differences of the DPOAE levels on days 7, 14, and 21 (P > .05) (Figure 1).
Group 3 (BTH): No significant differences were observed between the basal and 7th, 14th, and 21st day DPOAE levels (P > .05) (Figure 1). Group 4 (NT): No significant differences were observed between the basal and 7th, 14th, and 21st day DPOAE levels (P > .05) (Figure 1).
Comparisons of DPOAE levels between groups
Basal: No significant differences were observed between the basal DPOAE levels of the 4 groups (P > .05) (Figure 2). 7th day: Distortion-product otoacoustic emissions lev- els of group 1 (AK) were significantly lower than those of groups 3 (BTH) and 4 (NT) (P < .008) (Figure 2). Distortion-product otoacoustic emissions levels of group 2 (AK+BTH) were significantly lower than those of group 1 (AK) (P < .008) (Figure 2). No sig- nificant differences were observed between the DPOAE levels of groups 3 (BTH) and 4 (NT) (P > .05) (Figure 2).
Distortion-product otoacoustic emissions levels of the
groups on days 14 and 21 were similar to those of day 7 (Figure 2).

Downloaded from aor.sagepub.com by guest on October 31, 2014
4 Annals of Otology, Rhinology & Laryngology
Figure 2. Comparison of between-group distortion-product otoacoustic emissions values. For the comparison between groups, the 1-way analysis of variance test was applied (P < .05 was accepted as statistically significant). Tukey’s HSD was administered as a post- hoc test to identify within-group differences (P < .008 was accepted as statistically significant).
ABR
Comparisons of ABR thresholds within groups Group 1 (AK): The ABR thresholds significantly increased on the 7th day of the study (35.4 ± 4.17), as compared to their basal values (17.8 ± 3.08) (P < .008) (Figure 3). No significant differences were observed in the ABR thresholds on days 7, 14, and 21 (35.4 ± 4.17, 36.5 ± 3.97, 37.2 ± 5.01, respectively) (P > .05) (Figure 3). Group 2 (AK+BTH): The ABR thresholds significantly increased on the 7th day of the study (49.6 ± 5.04), as compared to their basal values (19.6 ± 4.61) (P < .008) (Figure 3). No significant differences were observed in the ABR thresholds on days 7, 14, and 21 (49.6 ± 5.04, 52.8 ± 3.24, 53.2 ± 3.85, respectively) (P > .05) (Figure 3). Group 3 (BTH): There were no significant differences between the basal and 7th, 14th, and 21st day ABR thresholds (20.2 ± 4.68, 21.5 ± 5.27, 20.7 ± 4.11, 19.7 ± 3.76, respectively) (P > .05) (Figure 3). Group 4 (NT): There were no significant differences between the basal and 7th, 14th, and 21st day ABR thresholds (20.9 ± 3.28, 22.0 ± 4.19, 21.9 ± 5.56, 20.5 ± 4.37, respectively) (P > .05) (Figure 3).
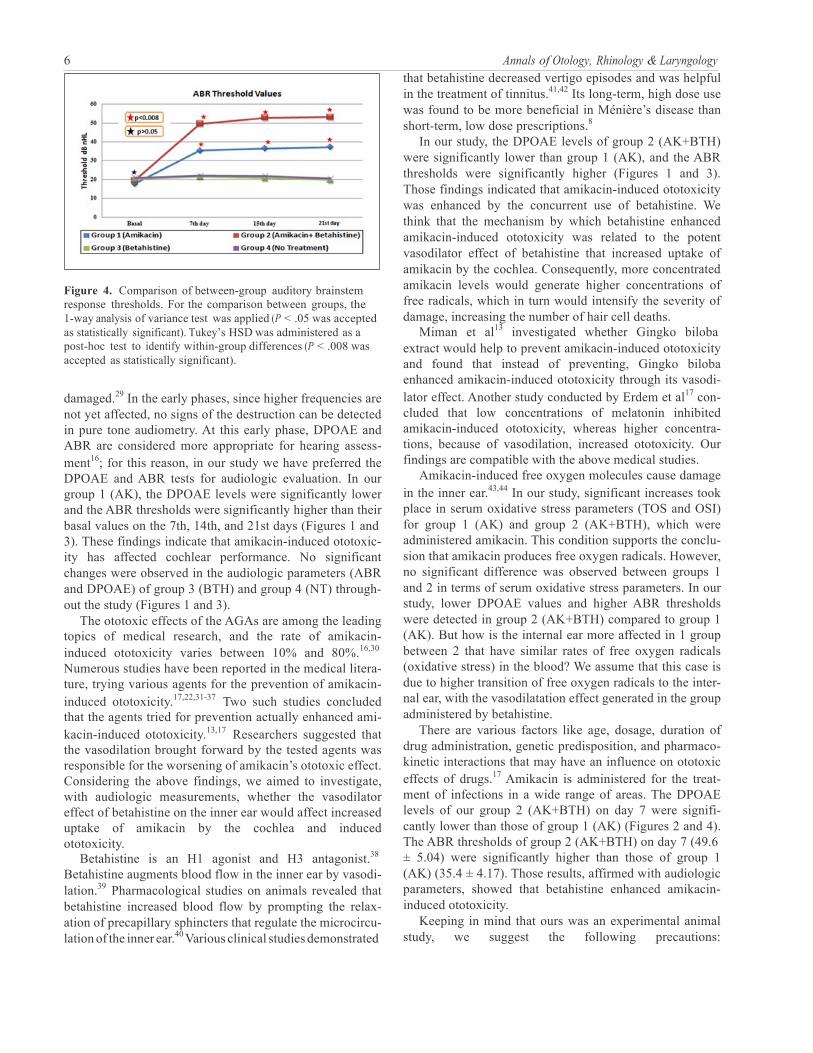
Comparisons of ABR thresholds between groups Basal: There were no significant differences between the basal ABR thresholds of the 4 groups (P > .05) (Figure 4). 7th day: The ABR threshold of group 1 (AK) (35.4 ± 4.17) was significantly higher than those of groups 3 (BTH) and 4 (NT) (21.5 ± 5.27, 22.0 ± 4.19, respec- tively) (P < .008) (Figure 4). The ABR threshold of group 2 (AK+BTH) (49.6 ± 5.04) was significantly higher than that of group 1 (AK) (35.4 ± 4.17) (P < .008) (Figure 4). There were no significant differences between the ABR thresholds of groups 3 (BTH) and 4 (NT) (P > .05) (Figure 4).
Auditory brainstem response thresholds of the 4 groups
on days 14 and 21 were similar to those of day 7 (Figure 4). Biochemical Parameters
TOS. In our study, the TOS value of group 1 (AK) had sig- nificantly increased compared to group 3 (BTH) and group 4 (NT) (P < .008) (Table 1). Also, the TOS value of group

Downloaded from aor.sagepub.com by guest on October 31, 2014
Aksoy et al 5
Figure 3. Comparison of within-group auditory brainstem response thresholds. For the comparison within group, the repeated analysis of variance test was applied (P < .05 was accepted as statistically significant). To determine the days between which there were differences, the Bonferroni test was administered as a post-hoc test (P < .008 was accepted as statistically significant).
2 (AK+BTH) had significantly increased compared to group 3 (BTH) and group 4 (NT) (P < .008) (Table 1). No significant difference is available between group 1 (AK) and group 2 (AK+BTH) in terms of TOS values (P > .05) (Table 1).
TAS. No significant difference is available in terms of TAS values among all groups (P > .05).
OSI. In our study, the OSI value of group 1 (AK) signifi- cantly increased compared to group 3 (BTH) and group 4 (NT) (P < .008) (Table 1). Also, the OSI value of group 2 (AK+BTH) had significantly increased compared to group 3 (BTH) and group 4 (NT) (P < .008) (Table 1). No significant difference is available between group 1 (AK) and group 2 (AK+BTH) in terms of OSI values (P > .05) (Table 1).
Discussion
Aminoglycoside antibiotics (AGAs) are currently used in a wide range of areas due to their powerful efficacy, rapid bactericidal activity, and low cost, despite their serious side effects (ototoxicity and nephrotoxicity).21,22 Aminoglycoside
antibiotics induce hearing loss and vestibular dysfunction through damaging inner ear structures (the cochlea and ves- tibule).23 Cochlear injury can cause permanent hearing loss, whereas damage to the vestibular apparatus can cause ver- tigo, ataxia, and/or nystagmus.24 Since cochlear injury leads to the loss of hair cells, the damage is irreversible.25
Aminoglycoside antibiotics are cited among the leading causes of irreversible hearing loss.19 Aminoglycoside anti- biotics exert their ototoxic effects by triggering the forma- tion of free radicals in the inner ear, which in turn cause permanent damage to the sensory receptor cells and related neurons.20 Damage in the organ of corti initially begins at the outer hair cells of the basal turn and progresses toward the cochlear apex.26
Amikacin is a semisynthetic aminoglycoside produced by the acetylation of kanamycin A. This structural charac- teristic renders amikacin resistant to bacterial enzymes that inactivate natural aminoglycosides like gentamicin, kana- mycin, and tobramycin; thus, amikacin has the widest spec- trum of activity among the AGAs.27 Whereas amikacin is primarily cochleotoxic, it also has a moderate vestibulo- toxic effect.28 When the whole organ of corti is damaged, the stria vascularis and the VIII nerve can also be
Downloaded from aor.sagepub.com by guest on October 31, 2014
6 Annals of Otology, Rhinology & Laryngology
Figure 4. Comparison of between-group auditory brainstem response thresholds. For the comparison between groups, the 1-way analysis of variance test was applied (P < .05 was accepted as statistically significant). Tukey’s HSD was administered as a post-hoc test to identify within-group differences (P < .008 was accepted as statistically significant).
damaged.29 In the early phases, since higher frequencies are not yet affected, no signs of the destruction can be detected in pure tone audiometry. At this early phase, DPOAE and ABR are considered more appropriate for hearing assess- ment16; for this reason, in our study we have preferred the DPOAE and ABR tests for audiologic evaluation. In our group 1 (AK), the DPOAE levels were significantly lower and the ABR thresholds were significantly higher than their basal values on the 7th, 14th, and 21st days (Figures 1 and 3). These findings indicate that amikacin-induced ototoxic- ity has affected cochlear performance. No significant changes were observed in the audiologic parameters (ABR and DPOAE) of group 3 (BTH) and group 4 (NT) through- out the study (Figures 1 and 3).
The ototoxic effects of the AGAs are among the leading topics of medical research, and the rate of amikacin- induced ototoxicity varies between 10% and 80%.16,30
Numerous studies have been reported in the medical litera- ture, trying various agents for the prevention of amikacin- induced ototoxicity.17,22,31-37 Two such studies concluded that the agents tried for prevention actually enhanced ami- kacin-induced ototoxicity.13,17 Researchers suggested that the vasodilation brought forward by the tested agents was responsible for the worsening of amikacin’s ototoxic effect. Considering the above findings, we aimed to investigate, with audiologic measurements, whether the vasodilator effect of betahistine on the inner ear would affect increased uptake of amikacin by the cochlea and induced ototoxicity.
Betahistine is an H1 agonist and H3 antagonist.38
Betahistine augments blood flow in the inner ear by vasodi- lation.39 Pharmacological studies on animals revealed that betahistine increased blood flow by prompting the relax- ation of precapillary sphincters that regulate the microcircu- lation of the inner ear.40 Various clinical studies demonstrated
that betahistine decreased vertigo episodes and was helpful in the treatment of tinnitus.41,42 Its long-term, high dose use was found to be more beneficial in Ménière’s disease than short-term, low dose prescriptions.8
In our study, the DPOAE levels of group 2 (AK+BTH) were significantly lower than group 1 (AK), and the ABR thresholds were significantly higher (Figures 1 and 3). Those findings indicated that amikacin-induced ototoxicity was enhanced by the concurrent use of betahistine. We think that the mechanism by which betahistine enhanced amikacin-induced ototoxicity was related to the potent vasodilator effect of betahistine that increased uptake of amikacin by the cochlea. Consequently, more concentrated amikacin levels would generate higher concentrations of free radicals, which in turn would intensify the severity of damage, increasing the number of hair cell deaths.
Miman et al13 investigated whether Gingko biloba extract would help to prevent amikacin-induced ototoxicity and found that instead of preventing, Gingko biloba enhanced amikacin-induced ototoxicity through its vasodi- lator effect. Another study conducted by Erdem et al17 con- cluded that low concentrations of melatonin inhibited amikacin-induced ototoxicity, whereas higher concentra- tions, because of vasodilation, increased ototoxicity. Our findings are compatible with the above medical studies.
Amikacin-induced free oxygen molecules cause damage in the inner ear.43,44 In our study, significant increases took place in serum oxidative stress parameters (TOS and OSI) for group 1 (AK) and group 2 (AK+BTH), which were administered amikacin. This condition supports the conclu- sion that amikacin produces free oxygen radicals. However, no significant difference was observed between groups 1 and 2 in terms of serum oxidative stress parameters. In our study, lower DPOAE values and higher ABR thresholds were detected in group 2 (AK+BTH) compared to group 1 (AK). But how is the internal ear more affected in 1 group between 2 that have similar rates of free oxygen radicals (oxidative stress) in the blood? We assume that this case is due to higher transition of free oxygen radicals to the inter- nal ear, with the vasodilatation effect generated in the group administered by betahistine.
There are various factors like age, dosage, duration of drug administration, genetic predisposition, and pharmaco- kinetic interactions that may have an influence on ototoxic effects of drugs.17 Amikacin is administered for the treat- ment of infections in a wide range of areas. The DPOAE levels of our group 2 (AK+BTH) on day 7 were signifi- cantly lower than those of group 1 (AK) (Figures 2 and 4). The ABR thresholds of group 2 (AK+BTH) on day 7 (49.6 ± 5.04) were significantly higher than those of group 1 (AK) (35.4 ± 4.17). Those results, affirmed with audiologic parameters, showed that betahistine enhanced amikacin- induced ototoxicity.
Keeping in mind that ours was an experimental animal study, we suggest the following precautions:

Downloaded from aor.sagepub.com by guest on October 31, 2014
Aksoy et al 7
Table 1. Biochemical Parameters.
Group TOS (µmol H O 2 2
Eqv/L) TAS (µmol TroloxEqv/L) OSI (TOS / TAS × 100)
Group 1 (amikacin), mean ± SD 5.75 ± 1.03 0.99 ± 0.72 0.058 ± 0.003 « «
Group 2 (amikacin +betahistine), mean ± SD 6.17 ± 0.98 1.07 ± 0.86 0.057 ± 0.020 Group 3 (betahistine), mean ± SD « 3.93 ± 1.75 1.14 ± 0.25 0.034 ± 0 017
«
Group 4 (no treatment), mean ± SD 4.36 ± 0.86 1.22 ± 0.41 0.035 ± 0.022
1-Way ANOVA (between groups)a P = .0001 P >.05 P = .0001
Abbreviations: ANOVA, analysis of variance; OSI, oxidant status index; TAS, total antioxidant status; TOS, total oxidant status. aFor the comparison between groups, the 1-way ANOVA test was used (P < .05 was accepted as statistically significant). Tukey’s HSD was administered as a post-hoc test to identify within-group differences (P < .008 was accepted as statistically significant) ( P > .008) «( P < .008).
1. In infections where amikacin administration is man-
datory, if and when vestibular symptoms (Ménière’s, tinnitus) are added to the picture, betahistine admin- istration should be postponed or should be replaced by a different agent that does not have a vasodila- tory effect on the inner ear.
2. In vestibular disorders where high dose, long-term use of betahistine is required (like Ménière’s), when antibiotherapy is required, an agent other than ami- kacin should be preferred.
3. Further experimental and clinical studies focused on the use of vasodilating agents that might enhance AGA-induced ototoxicity should be prompted.
Conclusion
Our study demonstrated with audiologic measurements (DPOAE and ABR) that the concurrent use of betahistine and amikacin could enhance amikacin-induced ototoxicity. Further experimental and clinical studies, including histo- pathological and laser Doppler flowmetry data, are needed to affirm our findings.
Declaration of Conflicting Interests The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
1. Arrang JM, Garbarg M, Quach TT, et al. Actions of betahis- tine receptors in the brain. Eur J Pharmacol. 1985;111:73-84.
2. Timmerman H. Histamine H3 ligands: just a pharmacological tool or potential therapeutic agents? J Med Chem. 1990;33: 4-11.
3. Chavez H, Vega R, Valli P, et al. Action mechanism of beta- histine in the vestibular end organs. Acta Otorhinolaryngol Ital. 2001;21:8-15.
4. James A, Thorp M. Meniere’s disease. Clin Evid. 2005;14: 659-665.
5. Laurikainen E, Miller JF, Pyykko I. Betahistine effects on cochlear blood flow: from the laboratory to the clinic. Acta Otolaryngol Suppl. 2000;544:5-7.
6. Lamm K, Arnold W. The effect of blood flow promoting drugs on cochlear blood flow, perilymphatic pO(2) and audi- tory function in the normal and noise-damaged hypoxic and ischemic guinea pig inner ear. Hear Res. 2000;141:199-219.
7. Laurikainen E, Miller JM, Nuttall AL, Quirk WS. The vas- cular mechanism of action of betahistine in the inner ear of the guinea pig. Eur Arch Otorhinolaryngol. 1998;255(3): 119-123.
8. Strupp M, Hupert D, Frenzel C, et al. Long-term prophylactic treatment of attacks of vertigo in Meniere’s disease—com- parison of a high with a low dosage of betahistine in an open trial. Acta Otolaryngol. 2008;128:520-524.
9. Ihler F, Bertlich M, Sharaf K, Strieth S, Strupp M, Canis M. Betahistine exerts a dose-dependent effect on cochlear stria vascularis blood flow in guinea pigs in vivo. PLoS One. 2012;7(6):e39086.
10. Chen KS, Bach A, Shoup A, Winick NJ. Hearing loss and ves- tibular dysfunction among children with cancer after receiv- ing aminoglycosides. Pediatr Blood Cancer. 2013;60(11): 1772-1777.
11. Sharp PM, Saenz CA, Martin RR. Amikacin (BB-K8) treat- ment of multiple-drug resistant Proteus infections. Antimicrob Agents Chemother. 1974;5(5):435-438.
12. Wrześniok D, Beberok A, Otręba M, Buszman E. Modulation of melanogenesis and antioxidant defense system in melano- cytes by amikacin. Toxicol In Vitro. 2013;27(3):1102-1108.
13. Miman MC, Ozturan O, Iraz M, Erdem T, Olmez E. Amikacin ototoxicity enhanced by Ginkgo biloba extract (EGb 761). Hear Res. 2002;169:121-129.
14. Rizzi MD, Hirose K. Aminoglycoside ototoxicity. Curr Opin Otolaryngol Head Neck Surg. 2007;15(5):352-357.
15. Forge A, Schacht J. Aminoglycoside antibiotics. Audiol Neurootol. 2000;5:3-22.

Downloaded from aor.sagepub.com by guest on October 31, 2014
8 Annals of Otology, Rhinology & Laryngology 16. Murillo-Cuesta S, Contreras J, Cediel R, Varela-Nieto I.
Comparison of different aminoglycoside antibiotic treat- ments to refine ototoxicity studies in adult mice. Lab Anim. 2010;44(2):124-131.
17. Erdem T, Ozturan O, Iraz M, Miman MC, Olmez E. Dose dependent dual effect of melatonin on ototoxicity induced by amikacin in adult rats. Eur Arch Otorhinolaryngol. 2005;262(4):314-321.
18. Institute for Laboratory Animal Research, National Research Council. The Guide for the Care and Use of Laboratory Animals. 7th ed. Washington, DC: National Academy of Sciences; 1996.
19. Strupp M, Arbusow V. Acute vestibulopathy. Curr Opin Neurol. 2001;14:11-20.
20. Rybak LP, Kelly T. Ototoxicity: bioprotective mechanisms. Curr Opin Otolaryngol Head Neck Surg. 2003;11:328-333.
21. Oliveira AA, Campos Mde S, Murashima Ade A, Rossato M, Hyppolito MA, Oliveira JA. Persistence of the otoprotective effect: how long does otoprotection against amikacin lasts? Braz J Otorhinolaryngol. 2012;78(6):47-50.
22. Pavlidis P, Maurer J, Apostolidou E, Kekes G, Kouvelas D. Memantine’s action against aminoglycoside-induced ototoxicity [published online August 6, 2013]. Eur Arch Otorhinolaryngol.
23. Roland JT Jr, Cohen NL. Vestibular and auditory ototoxicity. In: Cummings CW, Frederickson JM, Harker LA, Krause CJ, Schuller DF, Richardson MA, eds. Otolaryngology & Head and Neck Surgery. 3rd ed. St Louis, MO: Mosby; 1998:3186-3197.
24. Segal JA, Skolnick P. Polyamine-like actions of aminogly- cosides and aminoglycoside derivatives at NMDA receptors. Eur J Pharmacol. 1998;347:311-317.
25. Meyers RM. Ototoxic effects of gentamicin. Arch Otolaryngol. 1970;95:160-162.
26. Selimoglu E. Aminoglycoside-induced ototoxicity. Curr Pharm Des. 2007;13(1):119-126.
27. Kitasato I, Yokoda M, Inouye S, Igarashi M. Comparative ototoxicity of ribostamycin, dactimicin, dibekacin, kana- mycin, amikacin, tobramycin, gentamicin, sisomicin and netilmicin in the inner ear of guinea pigs. Chemotherapy. 1990;36(2):155-168.
28. Fausti A, Henry A, Schaffer I, et al. High frequency audio- metric monitoring for early detection of aminoglycoside oto- toxicity. J Infect Dis. 1992;165:1026-1032.
29. Stavroulaki P, Vossinakis IC, Dinopoulou D, Doudounakis S, Adamopoulos G, Apostolopoulos N. Otoacoustic emissions for monitoring aminoglycoside-induced ototoxicity in chil- dren with cystic fibrosis. Arch Otolaryngol Head Neck Surg. 2002;128:150-155.
30. Shayaninasab M, Fatololoomi M, Behnood F, Alizamir A. Relationship between serum ferritin level and amikacin oto- toxicity. Oman Med J. 2012;27(4):297-299.
31. Conlon BJ, Aran JM, Erre JP, Smith DW. Attenuation of aminoglycoside-induced cochlear damage with the metabolic antioxidant alpha-lipoic acid. Hear Res. 1999;128:40-44.
32. Nekrassov V, Sitges M. Vinpocetine protects from aminogly- coside antibiotic-induced hearing loss in guinea pig in vivo. Brain Res. 2000;868:222-229.
33. Oliveira JA, Canedo DM, Rossato M, Andrade MH. Self- protection against aminoglycoside ototoxicity in guinea pigs. Otolaryngol Head Neck Surg. 2004;131:271-279.
34. Lecain E, Omri B, Behar-Cohen F, Tran Ba Huy P, Crisanti P. The role of PKCzeta in amikacin-induced apoptosis in the cochlea: prevention by aspirin. Apoptosis. 2007;12(2): 333-342.
35. Berkiten G, Salturk Z, Topaloğlu I, Uğraş H. Protective effect of pentoxifylline on amikacin-induced ototoxicity in rats. Am J Otolaryngol. 2012;33(6):689-692.
36. Amora Lde A, Murashima Ade A, Rossato M, et al. The effects of hyperbaric oxygen therapy upon ototoxic injuries pro- duced by amikacin in guinea pigs. Braz J Otorhinolaryngol. 2013;79(3):342-348.
37. Bayindir T, Filiz A, Iraz M, et al. Evaluation of the protective effect of Beta glucan on amikacin ototoxicity using distortion product otoacoustic emission measurements in rats. Clin Exp Otorhinolaryngol. 2013;6(1):1-6.
38. Strupp M, Brandt T. Current treatment of vestibular, ocular motor disorders and nystagmus. Ther Adv Neurol Disord. 2009;2(4):223-239.
39. Dziadziola JK, Laurikainen EL, Rachel JD, et al. Betahistine increases vestibular blood flow. Otolaryngol Head Neck Surg. 1999;120:400-405.
40. Botta L, Mira E, Valli S, et al. Effects of betahistine metabolites on frog ampullar receptors. Acta Otolaryngol. 2000;120:25-27.
41. Mira E, Guidetti G, Ghilardi L, et al. Betahistine dihydrochlo- ride in the treatment of peripheral vestibular vertigo. Eur Arch Otorhinolaryngol. 2003;260:73-77.
42. Schmidt JT, Huizing EH. The clinical drug trial in Menière’s disease with emphasis on the effect of betahistine SR. Acta Otolaryngol Suppl. 1992;497:1-189.
43. Jiang H, Sha SH, Schacht J. NF-kappaB pathway protects cochlear hair cells from aminoglycoside-induced ototoxicity. J Neurosci Res. 2005;79:644-651.
44. Maridonneau-Parini I, Harpey C. Effect of trimetazidine on membrane damage induced by oxygen free radicals in human red cells. Br J Clin Pharmacol. 1985;20(2):148-151.
Related Documents











