MEDCH 561P Beta-lactam antibiotics: Penicillins http://botit.botany.wisc.edu/toms_fungi/nov2003.html April 9, 2012 Kelly Lee, Ph.D. H-172J [email protected] Penicillium chrysogenum + Staph. Aureus D-alanyl-D-alanine penicillin nucleus (6-APA) Beta-lactams bind to transpeptidase in place of D-Ala-D-Ala Transpeptidase (a PBP) normally binds to the D-Ala-D-Ala at the end of peptidoglycan precursors to crosslink the peptidoglycan. Beta-lactams such as penicillin mimic D-Ala- D-Ala, occupying the PBP active site and inhibiting crosslinking of peptidoglycan peptide bridges. Cell wall is weakened and this allows autolytic enzymes that degrade the peptidoglycan network to dominate, leading to lysis of the cells. Bactericidal.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MEDCH 561PBeta-lactam antibiotics: Penicillins
http://botit.botany.wisc.edu/toms_fungi/nov2003.html
April 9, 2012Kelly Lee, Ph.D.
Penicillium chrysogenum + Staph. Aureus
D-alanyl-D-alaninepenicillin nucleus (6-APA)
Beta-lactams bind to transpeptidase in place of D-Ala-D-Ala
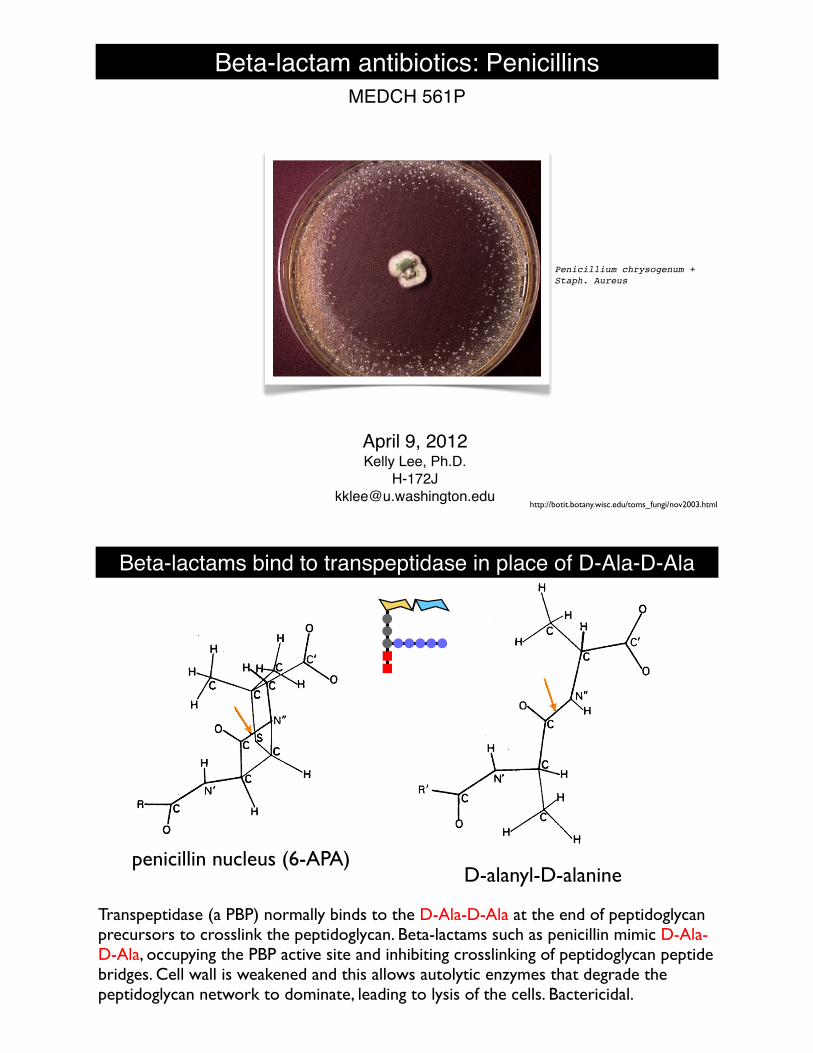
Transpeptidase (a PBP) normally binds to the D-Ala-D-Ala at the end of peptidoglycan precursors to crosslink the peptidoglycan. Beta-lactams such as penicillin mimic D-Ala-D-Ala, occupying the PBP active site and inhibiting crosslinking of peptidoglycan peptide bridges. Cell wall is weakened and this allows autolytic enzymes that degrade the peptidoglycan network to dominate, leading to lysis of the cells. Bactericidal.
Beta-lactams bind to transpeptidase in place of D-Ala-D-Ala
L-Ala
D-Glu
L-Lys Gly Gly Gly Gly Gly
L-Ala
D-Glu
L-Lys Gly Gly Gly Gly Gly
ONAM NAGO NAM NAGO
D-Ala
D-Ala
D-Ala
D-Ala
Gly
5Gly
5
L-Ala
D-Glu
L-Lys
L-Ala
D-Glu
L-Lys
Gly Gly Gly Gly
L-Ala
D-Glu
L-Lys
L-Ala
D-Glu
L-Lys
ONAM NAG
ONAM NAG
O
Gly
5
ONAM NAGO NAM NAGO
D-Ala
D-Ala
D-Ala
D-Ala
D-Alatranspeptidase active site is occupied by beta-lactam and cannot bind D-Ala-D-Ala, thus crosslinking does not take place
bactericidal, provided bacteria is susceptible
beta-lactam
Beta-lactam antibioticsAmoxicillin (penicillin) Cephalexin (cephalosporin)
Imipenem (carbapenem) Aztreonam (monobactam)

Beta-lactam antibiotics
๏ Penicillins๏ Potent, safe, but alone generally narrow spectrum, and susceptible to beta-
lactamases, allergy
๏ Cephalospirins๏ Less susceptible to penicillinases, less allergenic, broader spectrum in later
“generations” (increased Gram- coverage)
๏ Carbapenem๏ IV, broad spectrum, resistant to most beta-lactamases; drugs of last resort
๏ Monobactam๏ IV, Gram- coverage (poor for Gram+), resistant to many beta-lactams
Penicillins G and V
๏ Isolated directly from penicillium molds; fermentation produces large yields
๏ Fairly narrow spectrum of coverage
๏ Highly susceptible to beta-lactamase and penicillinase (e.g. S. aureus) activity
Penicillin G(benzylpenicillin)
Penicillin VPenicillin VK, potassium salt(phenoxymethylpenicillin)
Semi-synthetic penicillins
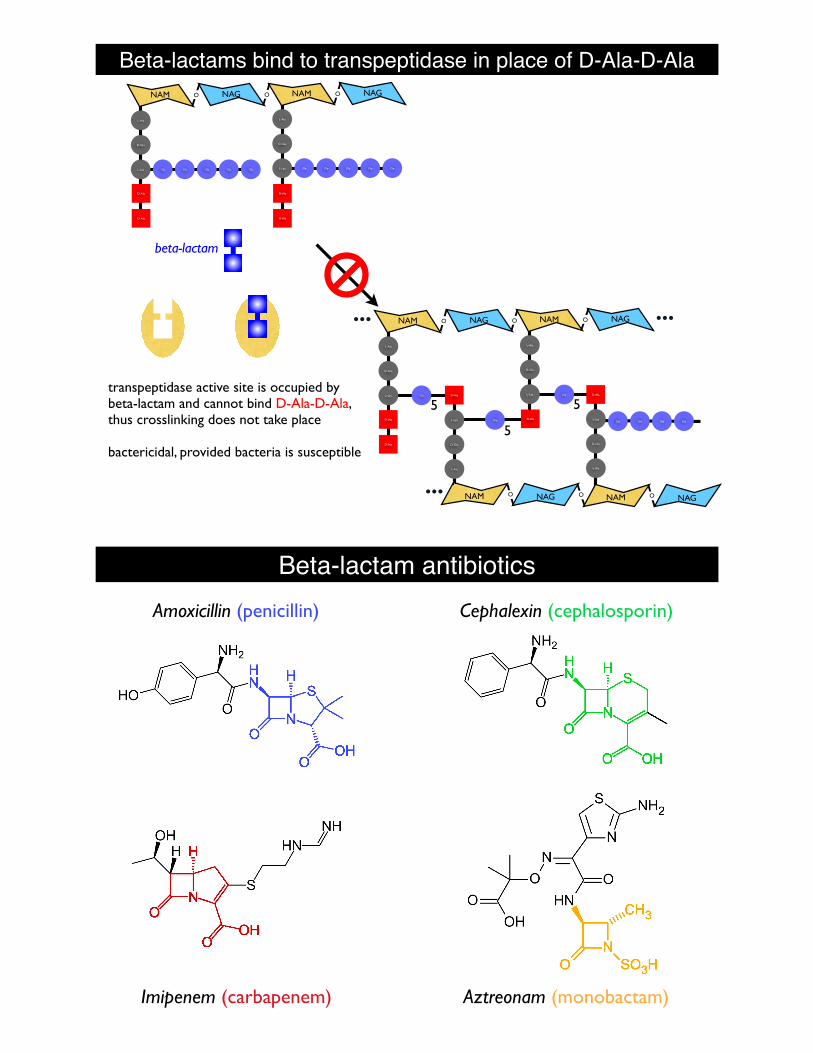
๏ Cleave off natural sidechains with amidase to yield the 6-aminopenicillanic acid (6-APA) core, which can be synthetically substituted w/ other sidechains.
๏ Alter the spectrum, stability, bioavailability, resistance to penicillinases
๏ Examples: amino-penicillins (amox, amp), nafcillin, dicloxacillin, piperacillin
Penicillin G Penicillin V
6-APA
Rside chainaffects activity,
lactamase susceptibility, immunogenicity
Penicillins general features
๏ Still widely prescribed and effective for bacteria that are not resistant
๏ Amoxicillin still one of the most widely used antimicrobials (#5 drug overall)
๏ Very potent, bactericidal, if pathogen is sensitive, MIC~0.02µg/ml
๏ Fairly broad spectrum overall, especially for semi-synthetic derivatives in combination w/ beta-lactamase inhibitors
๏ Generally very safe (good selective toxicity); targets the cell wall, which is unique to bacteria
๏ Penicillin allergies:
๏ One of the highest reported causes of a drug allergy, however actual incidence is believe to be somewhat lower than the 10% reported
Penicillin allergy
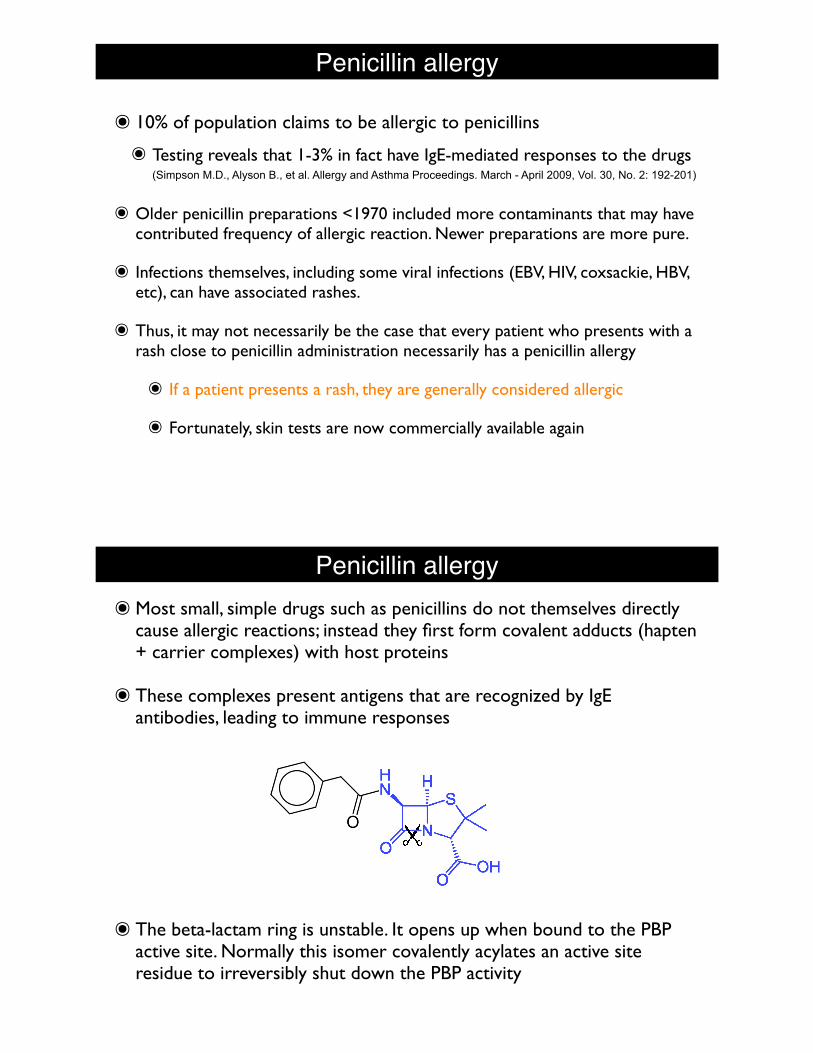
๏ 10% of population claims to be allergic to penicillins
๏ Testing reveals that 1-3% in fact have IgE-mediated responses to the drugs (Simpson M.D., Alyson B., et al. Allergy and Asthma Proceedings. March - April 2009, Vol. 30, No. 2: 192-201)
๏ Older penicillin preparations <1970 included more contaminants that may have contributed frequency of allergic reaction. Newer preparations are more pure.
๏ Infections themselves, including some viral infections (EBV, HIV, coxsackie, HBV, etc), can have associated rashes.
๏ Thus, it may not necessarily be the case that every patient who presents with a rash close to penicillin administration necessarily has a penicillin allergy
๏ If a patient presents a rash, they are generally considered allergic
๏ Fortunately, skin tests are now commercially available again
Penicillin allergy
๏ The beta-lactam ring is unstable. It opens up when bound to the PBP active site. Normally this isomer covalently acylates an active site residue to irreversibly shut down the PBP activity
๏Most small, simple drugs such as penicillins do not themselves directly cause allergic reactions; instead they first form covalent adducts (hapten + carrier complexes) with host proteins
๏ These complexes present antigens that are recognized by IgE antibodies, leading to immune responses
Penicillin allergy
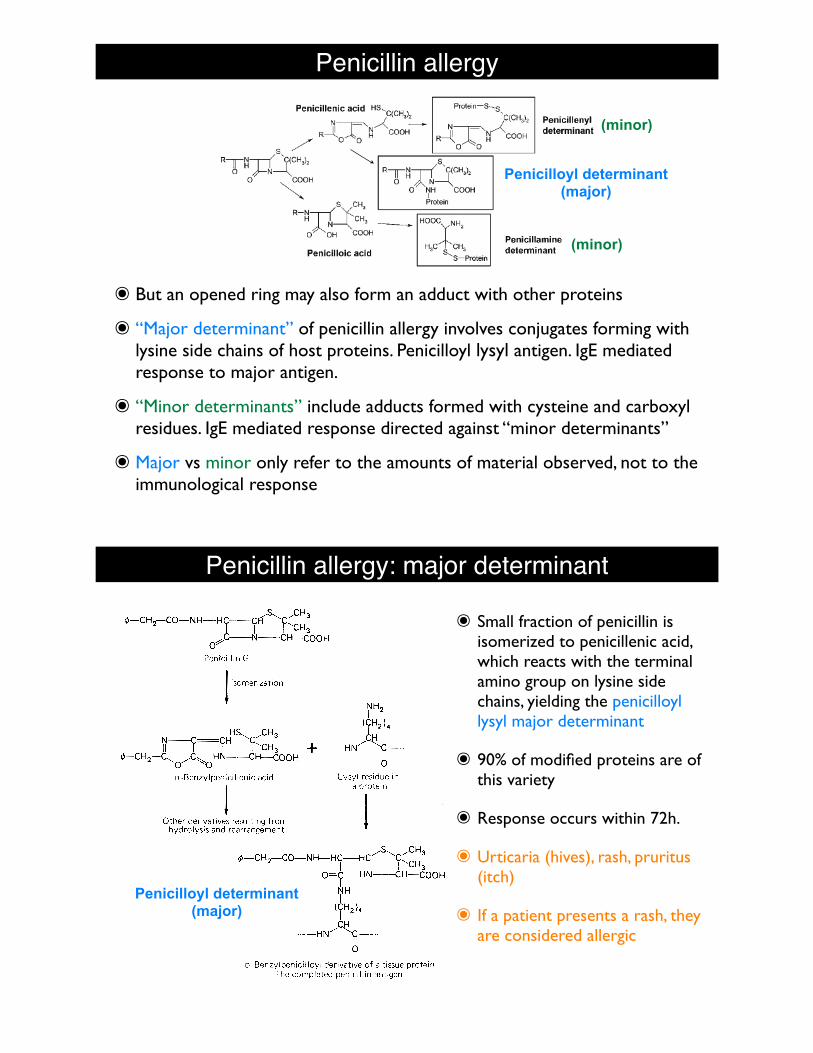
๏ But an opened ring may also form an adduct with other proteins
๏ “Major determinant” of penicillin allergy involves conjugates forming with lysine side chains of host proteins. Penicilloyl lysyl antigen. IgE mediated response to major antigen.
๏ “Minor determinants” include adducts formed with cysteine and carboxyl residues. IgE mediated response directed against “minor determinants”
๏ Major vs minor only refer to the amounts of material observed, not to the immunological response
Penicilloyl determinant(major)
(minor)
(minor)
Penicillin allergy: major determinant
21
e) allergy
This is considered the "major determinant" of penicillin allergy. The "minor determinants"
are a variety of other penicillin breakdown products.
1) immediate - urticaria, pruritus, shock; occurs within 60 min – rare but highly feared; 1gE mediated and directed against minor determinants
2) accelerated - rash; occurs within 72 h - common (5-10% of treated); 1g M and 1g E directed against major determinant
3) late - fever, urticaria; occurs > 72 h – rare; 1g M and 1g E
4) incidence - 5% show (+) reaction with skin test using penicilloyl polylysine (Prepen !) 50-70% of (+) have clinical Sx on amin. of penicillins - mostly rash <1% of (+) have serious reaction; overall incidence is about <.02%, <.0014% " death semisynthetic show # reactions; oral show # reactions relative to parenteral doses
but an allergy to one penicillin means that the patient would be assumed to have a problem with any penicillin
allergy to penicillin does not necessarily mean allergy to cephalosporins but cross reactivity does occur (~10%); rule: if patient has serious reaction to a penicillin, don't give any beta lactam except aztreonam
ampicillin " 9.5% allergy; this is due, in part, to the chemical nature of ampicillin, i.e. not all ampicillin induced rashes are true penicillin allergies. Amoxicillin has a somewhat lower incidence
densensitization protocols can be employed if infection requires penicillin therapy for an allergic patient
a rare interstitial nephritis is sometimes seen which may be a type of allergic reaction
Penicilloyl determinant(major)
๏ Small fraction of penicillin is isomerized to penicillenic acid, which reacts with the terminal amino group on lysine side chains, yielding the penicilloyl lysyl major determinant
๏ 90% of modified proteins are of this variety
๏ Response occurs within 72h.
๏ Urticaria (hives), rash, pruritus (itch)
๏ If a patient presents a rash, they are considered allergic

Penicillin allergy: major determinant
๏ Small fraction of penicillin is isomerized to penicillenic acid, which reacts with the terminal amino group on lysine side chains, yielding the penicilloyl lysyl major determinant
๏ 90% of modified proteins are of this variety
๏ Response occurs within 72h.
๏ Urticaria (hives), rash, pruritus (itch)
๏ If a patient presents a rash, they are considered allergic
Penicillin allergy: minor determinant
๏ “Minor determinants”: Result from reaction of other breakdown products with cysteine residues on proteins to form penicillenyl and penicillamine conjugates
๏ These determinants are associated with serious reactions such as anaphylaxis, shock
๏ Usually appear within 1h of administration; immediate hypersensitivity (IgE)
๏ Anaphylaxis in1:5,000-10,000 treatments (0.01-0.02%)
๏ ~0.0015% fatal outcome
Penicilloyl determinant(major)
(minor)
(minor)

Penicillin allergy: testing๏ What is available?
๏ PrePen (AllerQuest); back on the market as of May, 2010
๏ Skin test (puncture or intradermal) containing the benzylpenicilloyl major determinant on a polylysine carrier; those who show a positive test (wheal and flare on skin) to PrePen have IgE against the major determinant and are classified as penicillin allergic
๏ PrePen does not include the minor determinant. Fresh, diluted PenG may be added to for the minor determinant.
PRE-PEN®benzylpenicilloyl polylysine injection, solution
Skin Test Antigen
DESCRIPTION:PRE-PEN® (benzylpenicilloyl polylysine injection USP) is a sterile solution ofbenzylpenicilloyl polylysine in a concentration of 6.0 X 10-5 M (benzylpenicilloyl)in 0.01 M phosphate buffer and 0.15 M sodium chloride. The benzylpenicilloylpolylysine in PRE-PEN is a derivative of poly-l-lysine, where the epsilonamino groups are substituted with benzylpenicilloyl groups (50-70%) formingbenzylpenicilloyl alpha amide. Each single dose ampule contains 0.25 mLof PRE-PEN.
PRE-PEN has the following structure:
CLINICAL PHARMACOLOGY:PRE-PEN is a skin test antigen reagent that reacts specifically with ben-zylpenicilloyl IgE antibodies initiating the release of chemical mediatorswhich produce an immediate wheal and flare reaction at a skin test site. Allindividuals exhibiting a positive skin test to PRE-PEN possess IgE againstthe benzylpenicilloyl structural group which is a hapten. A hapten is a lowmolecular weight chemical that conjugates with a carrier (e.g. poly-l-lysine)resulting in the formation of an antigen with the hapten’s specificity. Thebenzylpenicilloyl hapten is the major antigenic determinant in penicillin-allergic individuals. However, many individuals reacting positively to PRE-PENwill not develop a systemic allergic reaction on subsequent exposure totherapeutic penicillin, especially among those who have not reacted topenicillins in the past. Thus, the PRE-PEN skin test determines the presenceof penicilloyl IgE antibodies which are necessary but not sufficient for acuteallergic reactions due to the major penicilloyl determinant.
Non-benzylpenicilloyl haptens are designated as minor determinants, sincethey less frequently elicit an immune response in penicillin treated individuals.The minor determinants may nevertheless be associated with significantclinical hypersensitivity. PRE-PEN does not react with IgE antibodies directedagainst non-benzylpenicilloyl haptens.
INDICATIONS AND USAGE:PRE-PEN is indicated for the assessment of sensitization to penicillin(benzylpenicillin or penicillin G) in patients suspected to have clinicalpenicillin hypersensitivity. A negative skin test to PRE-PEN is associatedwith an incidence of immediate allergic reactions of less than 5% after theadministration of therapeutic penicillin, whereas the incidence may be morethan 50% in a history-positive patient with a positive skin test to PRE-PEN.These allergic reactions are predominantly dermatologic. Whether a negativeskin test to PRE-PEN predicts a lower risk of anaphylaxis is not established.Similarly, when deciding the risk of proposed penicillin treatment, there arenot enough data at present to permit relative weighing in individual casesof a history of clinical penicillin hypersensitivity as compared to positive skintests to PRE-PEN and/or minor penicillin determinants.
CONTRAINDICATIONS:PRE-PEN is contraindicated in those patients who have exhibited either asystemic or marked local reaction to its previous administration. Patientsknown to be extremely hypersensitive to penicillin should not be skin tested.
WARNINGS:The risk of sensitization to repeated skin testing with PRE-PEN is notestablished. Rarely, a systemic allergic reaction including anaphylaxis(see below) may follow a skin test with PRE-PEN. To decrease the risk ofa systemic allergic reaction, puncture skin testing should be performedfirst. Intradermal skin testing should be performed only if the puncturetest is entirely negative.
PRECAUTIONS:General:No reagent, test, or combination of tests will completely assure that areaction to penicillin therapy will not occur.
The value of the PRE-PEN skin test alone as a means of assessing the risk ofadministering therapeutic penicillin (when penicillin is the preferred drug ofchoice) in the following situations is not established:
1. Adult patients who give no history of clinical penicillin hypersensitivity.2. Pediatric patients.
In addition, the clinical value of PRE-PEN where exposure to penicillin issuspected as a cause of a current drug reaction or in patients who areundergoing routine allergy evaluation is not known. Likewise, the clinical valueof PRE-PEN skin tests alone in determining the risk of administering semi-synthetic penicillins (phenoxymethyl penicillin, ampicillin, carbenicillin,dicloxacillin, methicillin, nafcillin, oxacillin, amoxicillin), cephalosporin-derived antibiotics, and penem antibiotics is not known.
In addition to the results of the PRE-PEN skin test, the decision to administeror not administer penicillin should take into account individual patient factors.Healthcare professionals should keep in mind the following:
1. A serious allergic reaction to therapeutic penicillin may occur in apatient with a negative skin test to PRE-PEN.
2. It is possible for a patient to have an anaphylactic reaction to ther-apeutic penicillin in the presence of a negative PRE-PEN skin test anda negative history of clinical penicillin hypersensitivity.
3. If penicillin is the drug of choice for a life-threatening infection,successful desensitization with therapeutic penicillin may be possibleirrespective of a positive skin test and/or a positive history of clinicalpenicillin hypersensitivity.
Pregnancy – Pregnancy Category C:Animal reproduction studies have not been conducted with PRE-PEN. It isnot known whether PRE-PEN can cause fetal harm when administered to apregnant woman or can affect reproduction capacity. The hazards of skintesting in such patients should be weighed against the hazard of penicillintherapy without skin testing.
ADVERSE REACTIONS:Occasionally, patients may develop an intense local inflammatory responseat the skin test site. Rarely, patients will develop a systemic allergic reaction,manifested by generalized erythema, pruritus, angioedema, urticaria,dyspnea, hypotension, and anaphylaxis. The usual methods of treating askin test antigen-induced reaction — the applications of a venous occlusiontourniquet proximal to the skin test site and administration of epinephrineare recommended. The patient should be kept under observation forseveral hours.
DOSAGE AND ADMINISTRATION:SKIN TESTING DOSAGE AND TECHNIQUESkin testing responses can be attenuated by interfering drugs (e.g. H1-antihistamines and vasopressors). Skin testing should be delayed until theeffects of such drugs have dissipated, or a separate skin test with histaminecan be used to evaluate persistent antihistaminic effects in vivo. Due to therisk of potential systemic allergic reactions, skin testing should be performedin an appropriate healthcare setting under direct medical supervision.
Puncture Testing:Skin testing is usually performed on the inner volar aspect of the forearm. Theskin test antigen should always be applied first by the puncture technique.After preparing the skin surface, apply a small drop of PRE-PEN solutionusing a sterile 22-28 gauge needle. The same needle can then be used tomake a single shallow puncture of the epidermis through the drop ofPRE-PEN. Very little pressure is required to break the epidermal continuity.Observe for the appearance of a wheal, erythema, and the occurrence ofitching at the test site during the succeeding 15 minutes at which time thesolution over the puncture site is wiped off. A positive reaction consists ofthe development within 10 minutes of a pale wheal, sometimes withpseudopods, surrounding the puncture site and varying in diameter from 5to 15 mm (or more). This wheal may be surrounded by a variable diameterof erythema, and accompanied by a variable degree of itching. The mostsensitive individuals develop itching quickly, and the wheal and erythema areprompt in their appearance. As soon as a positive response as definedabove is clearly evident, the solution over the scratch should be immediatelywiped off. If the puncture test is either negative or equivocally positive (lessthan 5 mm wheal with little or no erythema and no itching), an intradermaltest may be performed.
NHR
CH
NH
H
H
R = Benzylpenicilloyl or H
n > 40
H
S
COCO COOHN C
CH
NHNHNH CH CH CHCO CO COO
]2
C CCH2 CH( )3 2
4
NHR
CH ][[ 24
NHR
CH ][ 24
3+
๏ A patient may only exhibit an IgE-mediated response to the minor determinant
๏ Ideally a penicillin allergy test would include both major and minor determinants
Penicillin allergy๏ For patients who have a positive skin test (PrePen+PenG), 40-70% may exhibit an
anaphylactic reaction if penicillin were to be administered
๏ For patients who have a negative skin test, 1-3% may exhibit a reaction (usually mild) when penicillin is administered
๏ If minor determinants are not included (i.e. PenG), 3-10% of allergic patients may be missed by Pre-Pen
๏ Desensitization. If penicillin or beta-lactam is absolutely needed for patient with penicillin allergy, desensitization protocols are available (e.g. oral desensitization with PenV). Must be carefully monitored.
๏ Examples where this might be indicated:
๏ Strep. pyogenes is still sensitive to penicillins, and they are potent
๏ Syphilis (caused by the spirochete Treponema pallidum) in pregnant women.
http://www.cdc.gov/std/treatment/2006/penicillin-allergy.htm
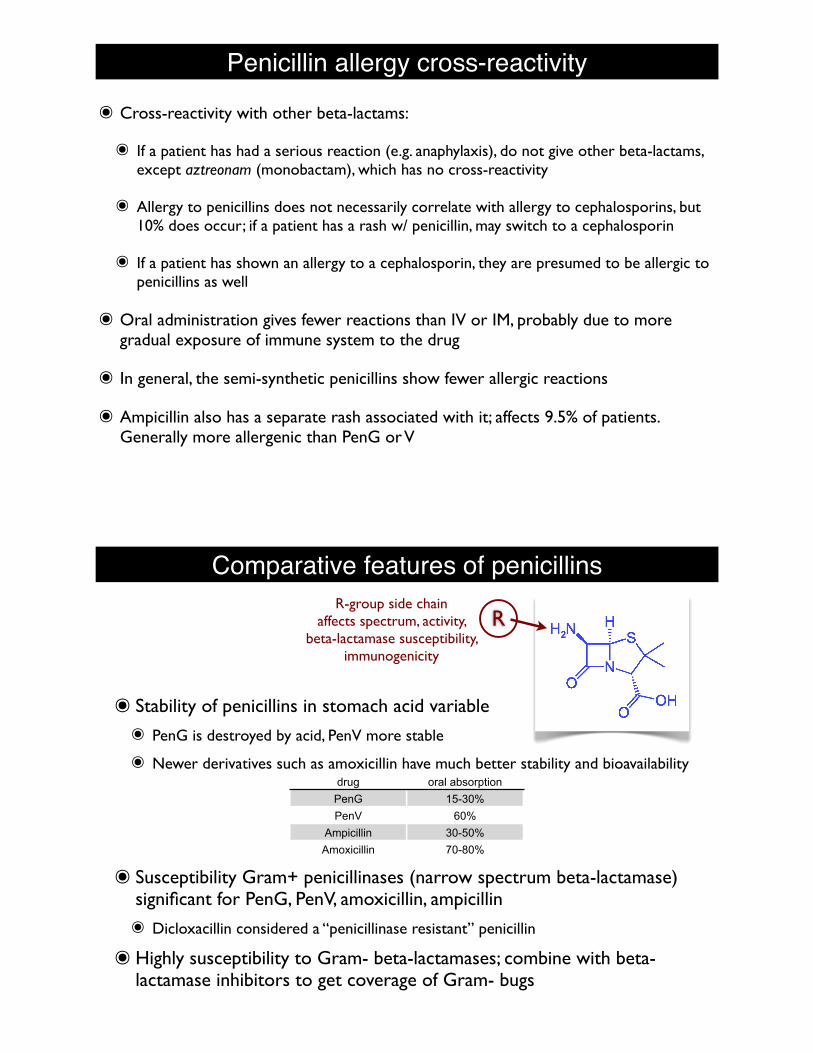
Penicillin allergy cross-reactivity๏ Cross-reactivity with other beta-lactams:
๏ If a patient has had a serious reaction (e.g. anaphylaxis), do not give other beta-lactams, except aztreonam (monobactam), which has no cross-reactivity
๏ Allergy to penicillins does not necessarily correlate with allergy to cephalosporins, but 10% does occur; if a patient has a rash w/ penicillin, may switch to a cephalosporin
๏ If a patient has shown an allergy to a cephalosporin, they are presumed to be allergic to penicillins as well
๏ Oral administration gives fewer reactions than IV or IM, probably due to more gradual exposure of immune system to the drug
๏ In general, the semi-synthetic penicillins show fewer allergic reactions
๏ Ampicillin also has a separate rash associated with it; affects 9.5% of patients. Generally more allergenic than PenG or V
Comparative features of penicillins
๏ Stability of penicillins in stomach acid variable๏ PenG is destroyed by acid, PenV more stable
๏ Newer derivatives such as amoxicillin have much better stability and bioavailability
๏ Susceptibility Gram+ penicillinases (narrow spectrum beta-lactamase) significant for PenG, PenV, amoxicillin, ampicillin๏ Dicloxacillin considered a “penicillinase resistant” penicillin
๏Highly susceptibility to Gram- beta-lactamases; combine with beta-lactamase inhibitors to get coverage of Gram- bugs
RR-group side chain
affects spectrum, activity, beta-lactamase susceptibility,
immunogenicity
drug oral absorptionPenG 15-30%PenV 60%
Ampicillin 30-50%Amoxicillin 70-80%

General features of penicillins๏Not significantly metabolized. Significant amounts are excreted in
unmodified, active form in urine. PenG ~80% excreted within 3-4h.๏ Can be effective therapeutic for urinary tract infections (UTI)
๏ Frequent dosing required
๏ Co-administered with probenicid to inhibit renal excretion. Increases plasma concentrations of penicillins and cephalosporins ~2x.
๏ Low penetration to cerebrospinal fluid unless inflammation is present
Properties of Penicillins
23
TABLE 1 - Properties of Penicillins
Type of penicillin Structure (R group) Oral
absorption
Routes of
admin.
1. "Natural:
Penicillin G
Penicillin V
poor
60-70%
IV, IM
PO
2. Amino
Ampicillin
Amoxicillin
30-50%
70-90%
PO, IV, IM
PO
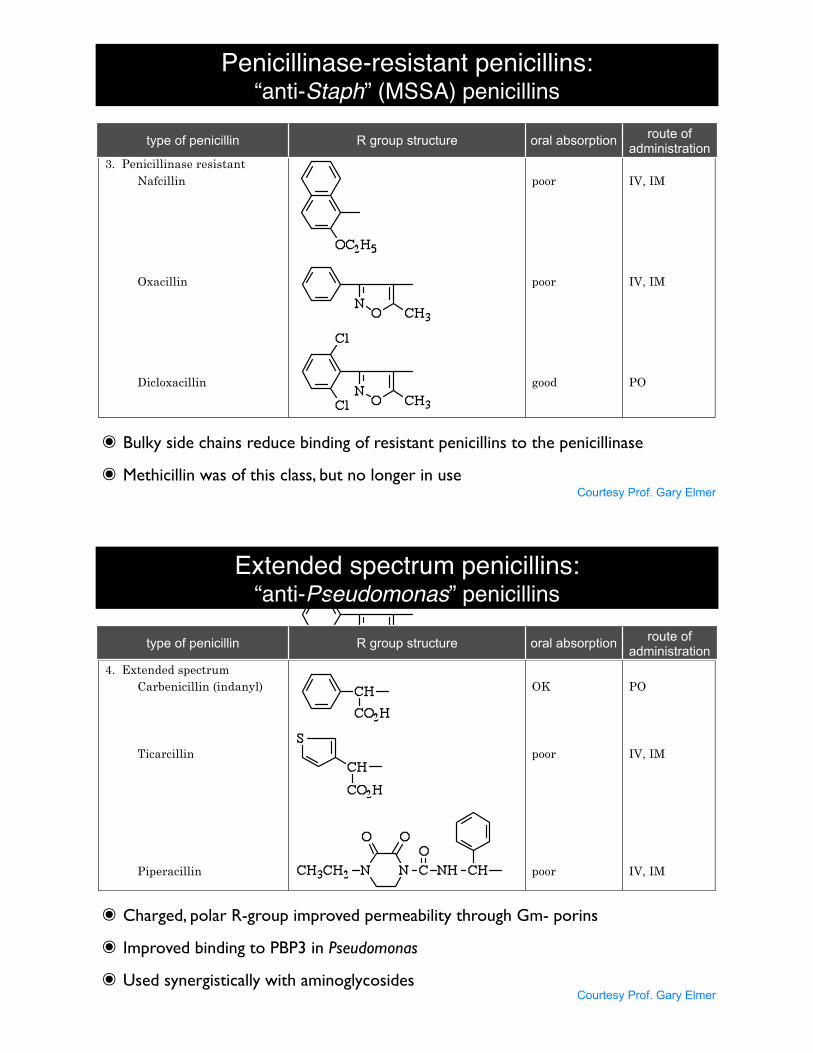
3. Penicillinase resistant
Nafcillin
Oxacillin
Dicloxacillin
poor
poor
good
IV, IM
IV, IM
PO
4. Extended spectrum
Carbenicillin (indanyl)
Ticarcillin
Piperacillin
OK
poor
poor
PO
IV, IM
IV, IM
type of penicillin R group structure oral absorption route of administration
Courtesy Prof. Gary Elmer
๏ Amino penicillins, more polar, better Gram- porin penetration
Penicillinase-resistant penicillins:“anti-Staph” (MSSA) penicillins
23
TABLE 1 - Properties of Penicillins
Type of penicillin Structure (R group) Oral
absorption
Routes of
admin.
1. "Natural:
Penicillin G
Penicillin V
poor
60-70%
IV, IM
PO
2. Amino
Ampicillin
Amoxicillin
30-50%
70-90%
PO, IV, IM
PO
3. Penicillinase resistant
Nafcillin
Oxacillin
Dicloxacillin
poor
poor
good
IV, IM
IV, IM
PO
4. Extended spectrum
Carbenicillin (indanyl)
Ticarcillin
Piperacillin
OK
poor
poor
PO
IV, IM
IV, IM
type of penicillin R group structure oral absorption route of administration
Courtesy Prof. Gary Elmer
๏ Bulky side chains reduce binding of resistant penicillins to the penicillinase
๏ Methicillin was of this class, but no longer in use
Extended spectrum penicillins:“anti-Pseudomonas” penicillins
Courtesy Prof. Gary Elmer
23
TABLE 1 - Properties of Penicillins
Type of penicillin Structure (R group) Oral
absorption
Routes of
admin.
1. "Natural:
Penicillin G
Penicillin V
poor
60-70%
IV, IM
PO
2. Amino
Ampicillin
Amoxicillin
30-50%
70-90%
PO, IV, IM
PO
3. Penicillinase resistant
Nafcillin
Oxacillin
Dicloxacillin
poor
poor
good
IV, IM
IV, IM
PO
4. Extended spectrum
Carbenicillin (indanyl)
Ticarcillin
Piperacillin
OK
poor
poor
PO
IV, IM
IV, IM
type of penicillin R group structure oral absorption route of administration
๏ Charged, polar R-group improved permeability through Gm- porins
๏ Improved binding to PBP3 in Pseudomonas
๏ Used synergistically with aminoglycosides

Antimicrobial spectrum of penicillins
penicillin type Staph penicillinase resistance?
Gram- beta-lactamase
resistance?useful coverage route of
administration
Penicillin G no noGram+; S. pyogenes,some neisseria (Gm-) IV
Penicillin V no no Gram+; some neisseria PO
Ampicillin(aminopenicillin) no no Gram+; some Gram- due
to better porin penetration IV, IM
Amoxicillin(aminopenicillin) no no Gram+; some Gram- due
to better porin penetration PO
Nafcillin(penicillinase-
resistant)yes no Staph (not MRSA) IV, IM
Oxacillin(penicillinase-
resistant)yes no Staph (not MRSA) IV, IM
Dicloxacillin(penicillinase-
resistant)yes no Staph (not MRSA) PO
Antimicrobial spectrum of penicillins
penicillin type Staph penicillinase resistance?
Gram- beta-lactamase
resistance?useful coverage route of
administration
Piperacillin(extended spectrum) no
bit better than ticarcillin; usually combined w/ a
lactamase inhibitor e.g. tazobactam
Gram+anaerobes
*PseudomonasEnterobacteriaciae
{Enterobacter,E.Coli,
Klebsiella,Serratia,
Salmonella,Shigella,
Providencia,Citrobacter,
Proteus}
IV, IM
Ticarcillin(extended spectrum) no
no; usually combined w/ a
lactamase inhibitor, e.g. clavulanic acid
similar to pip. IV, IM

Beta-lactamase inhibitors
๏ Used to overcome beta-lactamase-related resistance to beta-lactams; not effective against all beta-lactamases, however
๏ Bind to beta-lactamase active site and irreversibly inactivate them by forming a covalent linkage to the active site serine
๏ Minimal antibiotic activity by themselves๏ Combination therapy with beta-lactam antibiotics๏ Example: Augmentin (amoxicillin + clavulanic acid)
clavulanic acid sulbactam tazobactam
Penicillins combined with beta-lactamase inhibitors
penicillin typeStaph beta-lactamase
(penicillinase) resistance?
Gram- beta-lactamase
resistance?useful coverage route of
administration
Amoxicillin+
clavulanate(Augmentin ®)
yes yes broad PO
Ampicillin+
sulbactam(Unisyn ®)
yes yes broad IM, IV
Ticarcillin+
clavulanate(Timentin ®)
yes yes broad IV, IM
Piperacillin+
tazobactam(Zosyn ®)
yes yes broad IV, IM
Penicillins combined with beta-lactamase inhibitors
๏Generally would like to use as narrow spectrum of antibiotic as possible so as to reduce impact on non-pathogenic flora and so as to maintain balance, prevent overgrowth (e.g. C. difficile, Candida yeast)
๏ But often we do not know the bacterial target, or may have a super-infection involving multiple species
Common infections๏ Sinusitus๏ 30-40% S. pneumoniae๏ 20% H. influenzae๏ 20% M. catarrhalis
๏Acute otitis media (middle ear infection)๏ By age 3, up to 70% of children have experienced at least 1 infection๏ 15-25% M. catarrhalis; 90-95% of these isolates produce beta-lactamases๏ 40% S. pneumoniae; 30% penicillin-resistant (PRSP)๏ 30% H. influenzae; 30% produce beta-lactamases
๏Community-acquired pneumonia๏ 50-80% S. pneumonia๏ 2-18% H. influenzae๏ 2-5% S. aureus๏ ~5% anaerobes๏ ~5% other Gram-
๏ By comparison: Hospital-acquired pneumonia๏ Pseudomonas aeruginosa๏ Staph. aureus๏ Klebsiella pneumoniae๏ Enterobacteriaceae (Enterobacter, E. coli, Proteus, Serratia marcescens, A. baumanii)

๏Streptococcus pneumoniae: Gram+
๏ Pneumonia (500,000 cases/yr); S. pneumo the most common cause
๏ ~40,000 cases/yr of invasive pneumococcal infection
๏ 28% resistant to at least one antibiotic
๏ 11% resistant to 3 or more antibiotics
๏ Sinusitis and otitis media (7,000,000 cases/yr)
๏ Sepsis (55,000 cases/yr)
๏ Meningitis (6,000 cases/yr)
๏ Penicillins front-line drugs, but now 30% is
penicillin resistant (PRSP), also multi-drug
resistance is observed
๏ Vaccine helping to reduce prevalence
of antibiotic resistance
Respiratory, sinus and ear infections: S. pneumoniae
๏Haemophilus influenzae: Gram-, aerobe/facultative anaerobe
๏ Opportunistic commensal bacteria
๏ Pneumonia
๏ Sinusitis
๏ Otitis media (middle ear infection)
๏ Vaccine (HiB conjugate vaccine) is available
and has reduced frequency of invasive infections
relating to encapsulated serotype B
๏ 30% beta-lactamase producing
๏ Some show modified PBPs conferring
penicillin resistance, but ceph. may
be effective, macrolides, fluoroquinolones
Respiratory, sinus and ear infections: H. influenzae

Respiratory, sinus and ear infections: M. catarrhalis๏Moraxella catarrhalis: Gram-, aerobic, commensal found in upper resp. tract
๏Carriage in children up to 75%, in adults only 1-3%, esp in fall and winter
๏ Emerged as pathogen, esp for children, adults w/ COPD, immune compromised
๏Otitis media (middle ear infection)
๏ Pneumonia
๏ Bronchitis
๏ Sinusitis
๏Meningitis, sepsis more rare
๏ Lower respiratory tract infections
๏COPD patients
๏ Pneumonia in elderly
๏Hospital outbreaks
Other common, big bugs๏Strep. pyogenes: Gram+; “group A streptococcus” (GAS), beta-hemolytic
๏ Sometimes part of flora, nonpathogenic, asymptomatic
๏ Skin and wound infections
๏ 10,000,000 cases/yr infection: impetigo, cellulitis
๏ 4500 cases/yr invasive infection: necrotizing fasciitis
๏ Strep throat
๏ Scarlet fever
๏ Streptococcal toxic shock
๏Acute rheumatic fever; autoimmune reaction
triggered by Strep. pyogenes
๏ Penicillin is the drug of choice, very little
resistance has emerged; for those penicillin
allergic, macrolides, clindamycin
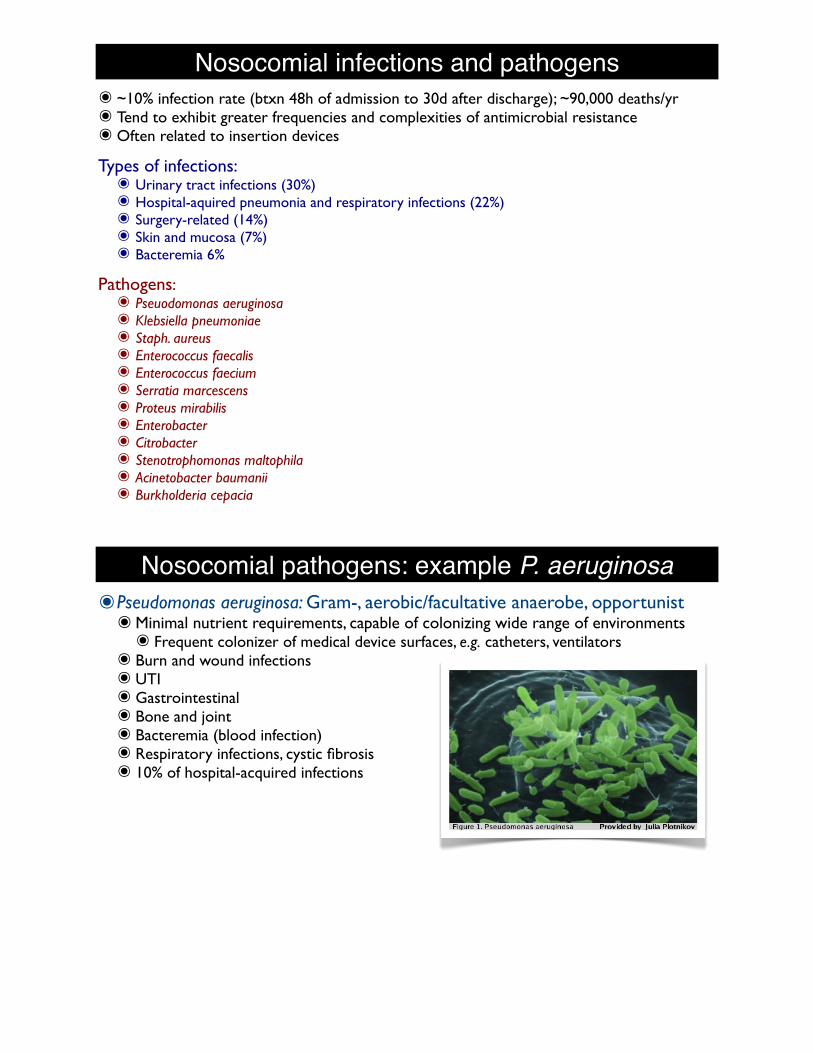
Nosocomial infections and pathogens๏ ~10% infection rate (btxn 48h of admission to 30d after discharge); ~90,000 deaths/yr๏ Tend to exhibit greater frequencies and complexities of antimicrobial resistance๏ Often related to insertion devices
Types of infections:๏ Urinary tract infections (30%)๏ Hospital-aquired pneumonia and respiratory infections (22%)๏ Surgery-related (14%)๏ Skin and mucosa (7%)๏ Bacteremia 6%
Pathogens:๏ Pseuodomonas aeruginosa๏ Klebsiella pneumoniae๏ Staph. aureus๏ Enterococcus faecalis๏ Enterococcus faecium๏ Serratia marcescens๏ Proteus mirabilis๏ Enterobacter๏ Citrobacter๏ Stenotrophomonas maltophila๏ Acinetobacter baumanii๏ Burkholderia cepacia
Nosocomial pathogens: example P. aeruginosa๏Pseudomonas aeruginosa: Gram-, aerobic/facultative anaerobe, opportunist๏Minimal nutrient requirements, capable of colonizing wide range of environments๏ Frequent colonizer of medical device surfaces, e.g. catheters, ventilators
๏ Burn and wound infections๏ UTI๏ Gastrointestinal๏ Bone and joint๏ Bacteremia (blood infection)๏ Respiratory infections, cystic fibrosis๏ 10% of hospital-acquired infections
๏ Significant antimicrobial resistance๏ Biofilm formation๏ Low cellular permeability to antibiotics๏ Selective porin channels and loss of expression of some porins๏ E.g. oprD porin deletion leads to lack of imipenem penetration, MIC goes from 1-2µg/
ml to 8-32µg/ml๏ Overexpress outer-membrane protein (oprH) that stabilize lipopolysaccharide, which
aminoglycoside usually interacts with to penetrate cell๏ Efflux pumps๏ MexAB: beta-lactams, fluoroquinolones๏ MexXY: aminoglycosides๏ MexEF: carbapenems, fluoroquinolones

๏Pseudomonas aeruginosa: Gram-, aerobic/facultative anaerobe, opportunist๏Minimal nutrient requirements, capable of colonizing wide range of environments๏ Frequent colonizer of medical device surfaces, e.g. catheters, ventilators
๏ Burn and wound infections๏ UTI๏ Gastrointestinal๏ Bone and joint๏ Bacteremia (blood infection)๏ Respiratory infections, cystic fibrosis๏ 10% of hospital-acquired infections
๏ Significant antimicrobial resistance๏ Biofilm formation๏ Low cellular permeability to antibiotics๏ Selective porin channels and loss of expression of some porins๏ E.g. oprD porin deletion leads to lack of imipenem penetration, MIC goes from 1-2µg/
ml to 8-32µg/ml๏ Overexpress outer-membrane protein (oprH) that stabilize lipopolysaccharide, which
aminoglycoside usually interacts with to penetrate cell๏ Efflux pumps; multi-drug efflux pumps transport across BOTH membranes๏ MexAB: beta-lactams, fluoroquinolones๏ MexXY: aminoglycosides๏ MexEF: carbapenems, fluoroquinolones
Nosocomial pathogens: example P. aeruginosa
๏ P. aeruginosa significant antimicrobial resistance (cont.)๏ Beta-lactamase expression๏ AmpC “cephalosporinase” (not susceptible to inhibitors)๏ Extended spectrum beta-lactamases (cephs, pens), sensitive to inhibitors๏ Carbapenemases
๏ Modified targets๏ Mutated DNA gyrase to decrease fluoroquinolone activity๏ Altered ribosomal targets for streptomycin but anti-pseudomonal aminoglycosides
are available๏ These resistance mechanisms may be observed in various combinations, strain and
isolate dependent
within the cytoplasm. The modifying enzymes are plasmid-mediated, consequently spontaneous mutations in cellsduring antibiotic treatment does not lead to over-expression of the enzymes, as seen with the chromosomalb-lactamases. Acquisition of the genes for the modifyingenzymes would require transfer from strains bearing theplasmids. Currently treatment of P. aeruginosa infections inCF with aerosolized tobramycin does not appear to haveresulted in increased resistance rates18.
Changes in targets
This mechanism of resistance results from mutationalchanges in target enzymes which result in maintenance oftheir vital role in cell metabolism but resistance to theaction of selective inhibition by antibiotics. In P. aeruginosa itis most commonly encountered with the quinolonesthrough mutation in the gyrA gene encoding the A subunitof the target enzyme, DNA gyrase19. Together with activeefflux this accounts for the current level of resistance seenin CF strains. Changes in the structure of the ribosome 30Ssubunit (the aminoglycoside target) influence streptomycinsensitivity but not that of the anti-pseudomonal aminoglyco-sides. Alteration in the penicillin-binding proteins ofP. aeruginosa resulting in resistance to b-lactams has beenreported but is not currently a major problem in CFstrains20.
Biofilms and resistance
In CF lung infections P. aeruginosa grows as aggregates ofcells (microcolonies) encased in a protective alginatepolysaccharide. This mode of growth also occurs onsurfaces, where it is referred to as a biofilm. Thecharacteristic property of all biofilms is their remarkableresistance to eradication by physical and biochemicaltreatments, including antibiotics21. Although this recalci-trance has been recognized for many years its biologicalbasis has still not been thoroughly explained. Factors whichmight partly explain the resistance phenotype include thehigh bacterial cell density and physical exclusion of theantibiotic. Physiological changes might occur in cells withinthe biofilm involving a general stress response, in which keymetabolic processes are shut down and protectivemechanisms induced22. It is clear that cells in the biofilm,like free-living ‘planktonic’ cells, can sense the presence ofother cells (quorum sensing) and alter their propertiesaccordingly23.
Finally, the population of cells within a biofilm isheterogeneous, containing fast- and slow-growing cells,some resistant through expression of inactivating enzymesand efflux pumps, others conspicuously not expressing suchsystems. The overall resistance is therefore dependent uponan interaction between the entire population of cells and
therapy needs to be directed against a multicellularcommunity21.
CONCLUSIONS AND IMPLICATIONS FORTHERAPY
Table 2 summarizes the contribution of different mechan-isms to the current resistance levels of P. aeruginosaencountered in CF. Restricted permeability and effluxare common components of the resistance phenotype forb-lactams, aminoglycosides and quinolones and areessentially fundamental properties of the organism. Theinnate antibiotic resistance of P. aeruginosa results from therestricted permeability of the cell wall and is enhanced bythe activity of efflux systems.
The occurrence of more specific mechanisms involvinginactivation and changes in targets reflects the selectivepressure resulting from heavy reliance on these agents inCF. For example, spontaneous mutations can increase theexpression of chromosomal b-lactamase genes. Thesemutants will be selected under the pressure of antibioticusage, especially where monotherapy is employed.
The increased recognition of the role of efflux systems ingeneral antibiotic resistance has led to a search for effluxpump inhibitors as therapeutic adjuncts.
Similarly, an understanding of the complex interactionin biofilm communities may eventually lead to novelstrategies for their control. However, P. aeruginosa hasalways proven to possess an answer to antibiotic therapy,the ominous size of its genome and current lack ofknowledge of the function of many of its genes suggests thatthis will continue to be the case whatever new therapies aredevised.
REFERENCES
1 Hancock RE. Resistance mechanisms in Pseudomonas aeruginosa and othernonfermentative gram-negative bacteria. Clin Infect Dis 1998;1(suppl):S93–9 25
J O U R N A L O F T H E R O Y A L S O C I E T Y O F M E D I C I N E S u p p l e m e n t N o . 4 1 V o l u m e 9 5 2 0 0 2
Table 2 Summary of resistance mechanisms of P. aeruginosa in cystic
fibrosis
Antibiotic
Permeability
and efflux Inactivation
Changes in
targets
b-lactams +++ +++ +
Aminoglycosides ++ ++ 7
Quinolones +++ 7 +++
Polymyxins 7 7 +
+++ most commonly encountered; ++ common; + reported but rare; 7 not reported
Lambert PA, J. Royal Soc. Med., (2002) 95(suppl.41):22
Nosocomial pathogens: example P. aeruginosa
Notable UW formulary penicillins: Pen GPenicillin G Spectrum:
๏ Gram+ cocci๏ S. pyogenes: minimal resistance observed, does not produce beta-lactamases๏ S. pneumoniae: modified PBP in 30-40% gave rise to PRSP (penicillin resistant S. pneumo),
not due to beta-lactamase๏ most common cause of CAP (community-aquired pneumonia) 50-80%๏ very common cause of otitis media ~35%
๏ S. viridans: usually still sensitive๏ Endocarditis (heart valve infection)
๏ Enterococcus faecalis: Pen G, amoxicillin generally effective๏ But note, E. faecium: highly resistant to Pen G (92%) and vancomycin
๏ Gram+ rods๏ Clostridium tetani (tetanus), C. perfringens (gangrene, food poisoning) sensitive,
but C. difficile resistant
๏ Gram- cocci๏ Neisseria meningitidis: PenG can penetrate meninges due to inflammation, sensitive๏ But, N. gonorrhoeae no longer sensitive due to beta-lactamases
๏ Gram- rods: mostly resistant๏ E.g. Enterobacteriaceae, Pseudomonas, H. influenzae
๏ Helical and spirochetes:๏ Treponema pallidum (syphilis): sensitive to Pen G still๏ Helicobacter pylori (stomach ulcers): not Pen G; amox + clarithromycin (macrolide) + PPI
Notable UW formulary penicillins: Pen G
Bicillin® L-A
Bicillin® C-R(penicillin G benzathine andpenicillin G procaine injectable suspension)Disposable Syringefor deep IM injection only
WARNING: NOT FOR INTRAVENOUS USE. DO NOT INJECT IN TRAVENOUSLY OR ADMIX WITH OTHER INTRAVENOUS SOLUTIONS. THERE HAVE BEEN REPORTS OF INADVERTENT INTRAVENOUS ADMIN-ISTRATION OF PENICILLIN G BENZATHINE WHICH HAS BEEN ASSOCIATED WITH CARDIORESPIRA-TORY ARREST AND DEATH. Prior to administration of this drug, carefully read the WARNINGS, ADVERSE REACTIONS, and DOSAGE AND ADMINISTRATION sections of the labeling.
Rx OnlyTo reduce the development of drug-resistant bacteria and maintain the effectiveness of Bicillin C-R and other anti-bacterial drugs, Bicillin C-R should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.DESCRIPTIONBicillin C-R (penicillin G benzathine and penicillin G pro-caine injectable suspension) contains equal amounts of the benzathine and procaine salts of penicillin G. It is available for deep intramuscular injection.Penicillin G benzathine is prepared by the reaction of diben-zylethylene diamine with two molecules of penicillin G. It is chemically designated as (2S,5R,6R)-3,3-Dimethyl-7-oxo-6-(2-phenylacetamido)-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid compound with N,N’-dibenzyleth-ylenediamine (2:1), tetrahydrate. It occurs as a white, crystalline powder and is very slightly soluble in water and sparingly solu-ble in alcohol. Its chemical structure is as follows:
Molecular Formula Molecular Wt. (C16H18N2O4S)2 16H20N2 2O 981.19
Penicillin G procaine, (2S,5R,6R)-3,3-Dimethyl-7-oxo-6-(2-phenylacetamido)-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid compound with 2-(diethylamino)ethyl p-aminobenzoate (1:1) monohydrate, is an equimolar salt of procaine and penicillin G. It occurs as white crystals or a white, microcrystalline powder and is slightly soluble in water. Its chemical structure is as follows:
Molecular Formula Molecular Wt. C16H18N2O4 13H20N2O2 2O 588.72
Each disposable syringe (2 mL size) contains the equivalent
of 1,200,000 units of penicillin G comprising: the equivalent of 600,000 units of penicillin G as the benzathine salt and the equivalent of 600,000 units of penicillin G as the pro-caine salt in a stabilized aqueous suspension with sodium citrate buffer; and as w/v, approximately 0.5% lecithin, 0.55% carboxymethylcellulose, 0.55% povidone, 0.1% methylparaben, and 0.01% propylparaben.Bicillin C-R injectable suspension in the disposable-syringe formulation is viscous and opaque. Read CONTRAINDICA-TIONS, WARNINGS, PRECAUTIONS, and DOSAGE AND ADMINISTRATION sections prior to use.CLINICAL PHARMACOLOGYGeneralPenicillin G benzathine and penicillin G procaine have a low solubility and, thus, the drugs are slowly released from intramuscular injection sites. The drugs are hydrolyzed to penicillin G. This combination of hydrolysis and slow absorption results in blood serum levels much lower but more prolonged than other parenteral penicillins.Intramuscular administration of 600,000 units of Bicillin C-R in adults usually produces peak blood levels of 1.0 to 1.3 units per mL within 3 hours; this level falls to an average concentration of 0.32 units per mL at 12 hours, 0.19 units per mL at 24 hours, and 0.03 units per mL at seven days.Intramuscular administration of 1,200,000 units of Bicillin C-R in adults usually produces peak blood levels of 2.1 to 2.6 units per mL within 3 hours; this level falls to an average concentration of 0.75 units per mL at 12 hours, 0.28 units per mL at 24 hours, and 0.04 units per mL at seven days.Approximately 60% of penicillin G is bound to serum pro-tein. The drug is distributed throughout the body tissues in widely varying amounts. Highest levels are found in the kid-neys with lesser amounts in the liver, skin, and intestines. Penicillin G penetrates into all other tissues and the spinal fluid to a lesser degree. With normal kidney function, the drug is excreted rapidly by tubular excretion. In neonates and young infants and in individuals with impaired kidney function, excretion is considerably delayed.MicrobiologyPenicillin G exerts a bactericidal action against penicillin-susceptible microorganisms during the stage of active multiplication. It acts through the inhibition of biosynthesis of cell-wall mucopeptide. It is not active against the peni-cillinase-producing bacteria, which include many strains of staphylococci. The following in vitro data are available, but their clinical sig-nificance is unknown. Penicillin G exerts high in vitro activity against staphylococci (except penicillinase-producing strains), streptococci (Groups A, C, G, H, L, and M), and pneumococci. Other organisms susceptible to penicillin G are Neisseria gonorrhoeae, Corynebacterium diphtheriae, Bacillus anthracis, Clostridia species, Actinomyces bovis, Streptobacillus moniliformis, Listeria monocytogenes, and Leptospira species. Treponema pallidum is extremely sus-ceptible to the bactericidal action of penicillin G.Susceptibility Test: If the Kirby-Bauer method of disc sus-ceptibility is used, a 10-unit penicillin disc should give a zone greater than 28 mm when tested against a penicillin-susceptible bacterial strain.
Bicillin® C-R(penicillin G benzathine andpenicillin G procaine injectable suspension)Disposable Syringefor deep IM injection only
WARNING: NOT FOR INTRAVENOUS USE. DO NOT INJECT IN TRAVENOUSLY OR ADMIX WITH OTHER INTRAVENOUS SOLUTIONS. THERE HAVE BEEN REPORTS OF INADVERTENT INTRAVENOUS ADMIN-ISTRATION OF PENICILLIN G BENZATHINE WHICH HAS BEEN ASSOCIATED WITH CARDIORESPIRA-TORY ARREST AND DEATH. Prior to administration of this drug, carefully read the WARNINGS, ADVERSE REACTIONS, and DOSAGE AND ADMINISTRATION sections of the labeling.
Rx OnlyTo reduce the development of drug-resistant bacteria and maintain the effectiveness of Bicillin C-R and other anti-bacterial drugs, Bicillin C-R should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.DESCRIPTIONBicillin C-R (penicillin G benzathine and penicillin G pro-caine injectable suspension) contains equal amounts of the benzathine and procaine salts of penicillin G. It is available for deep intramuscular injection.Penicillin G benzathine is prepared by the reaction of diben-zylethylene diamine with two molecules of penicillin G. It is chemically designated as (2S,5R,6R)-3,3-Dimethyl-7-oxo-6-(2-phenylacetamido)-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid compound with N,N’-dibenzyleth-ylenediamine (2:1), tetrahydrate. It occurs as a white, crystalline powder and is very slightly soluble in water and sparingly solu-ble in alcohol. Its chemical structure is as follows:
Molecular Formula Molecular Wt. (C16H18N2O4S)2 16H20N2 2O 981.19
Penicillin G procaine, (2S,5R,6R)-3,3-Dimethyl-7-oxo-6-(2-phenylacetamido)-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid compound with 2-(diethylamino)ethyl p-aminobenzoate (1:1) monohydrate, is an equimolar salt of procaine and penicillin G. It occurs as white crystals or a white, microcrystalline powder and is slightly soluble in water. Its chemical structure is as follows:
Molecular Formula Molecular Wt. C16H18N2O4 13H20N2O2 2O 588.72
Each disposable syringe (2 mL size) contains the equivalent
of 1,200,000 units of penicillin G comprising: the equivalent of 600,000 units of penicillin G as the benzathine salt and the equivalent of 600,000 units of penicillin G as the pro-caine salt in a stabilized aqueous suspension with sodium citrate buffer; and as w/v, approximately 0.5% lecithin, 0.55% carboxymethylcellulose, 0.55% povidone, 0.1% methylparaben, and 0.01% propylparaben.Bicillin C-R injectable suspension in the disposable-syringe formulation is viscous and opaque. Read CONTRAINDICA-TIONS, WARNINGS, PRECAUTIONS, and DOSAGE AND ADMINISTRATION sections prior to use.CLINICAL PHARMACOLOGYGeneralPenicillin G benzathine and penicillin G procaine have a low solubility and, thus, the drugs are slowly released from intramuscular injection sites. The drugs are hydrolyzed to penicillin G. This combination of hydrolysis and slow absorption results in blood serum levels much lower but more prolonged than other parenteral penicillins.Intramuscular administration of 600,000 units of Bicillin C-R in adults usually produces peak blood levels of 1.0 to 1.3 units per mL within 3 hours; this level falls to an average concentration of 0.32 units per mL at 12 hours, 0.19 units per mL at 24 hours, and 0.03 units per mL at seven days.Intramuscular administration of 1,200,000 units of Bicillin C-R in adults usually produces peak blood levels of 2.1 to 2.6 units per mL within 3 hours; this level falls to an average concentration of 0.75 units per mL at 12 hours, 0.28 units per mL at 24 hours, and 0.04 units per mL at seven days.Approximately 60% of penicillin G is bound to serum pro-tein. The drug is distributed throughout the body tissues in widely varying amounts. Highest levels are found in the kid-neys with lesser amounts in the liver, skin, and intestines. Penicillin G penetrates into all other tissues and the spinal fluid to a lesser degree. With normal kidney function, the drug is excreted rapidly by tubular excretion. In neonates and young infants and in individuals with impaired kidney function, excretion is considerably delayed.MicrobiologyPenicillin G exerts a bactericidal action against penicillin-susceptible microorganisms during the stage of active multiplication. It acts through the inhibition of biosynthesis of cell-wall mucopeptide. It is not active against the peni-cillinase-producing bacteria, which include many strains of staphylococci. The following in vitro data are available, but their clinical sig-nificance is unknown. Penicillin G exerts high in vitro activity against staphylococci (except penicillinase-producing strains), streptococci (Groups A, C, G, H, L, and M), and pneumococci. Other organisms susceptible to penicillin G are Neisseria gonorrhoeae, Corynebacterium diphtheriae, Bacillus anthracis, Clostridia species, Actinomyces bovis, Streptobacillus moniliformis, Listeria monocytogenes, and Leptospira species. Treponema pallidum is extremely sus-ceptible to the bactericidal action of penicillin G.Susceptibility Test: If the Kirby-Bauer method of disc sus-ceptibility is used, a 10-unit penicillin disc should give a zone greater than 28 mm when tested against a penicillin-susceptible bacterial strain.
Bicillin® C-R+
Penicillin GIM formulations:๏ Procaine/Pen G๏ IM shot (including the local anesthetic procaine)
๏ Benzathine/Pen G (Bicillin® L-A and Bicillin® C-R)๏ IM shot (not IV- cardiac arrest, black bo x warnin)๏ Low levels of PenG (but close to MIC) persist for 14-20 days๏ Bicillin L-A has all Pen G bound with benzathine๏ Bicillin C-R has half of Pen G bound with benzathine and half with procaine๏ E.g. @ day 14, 0.02 µg/ml PenG, MIC for S. pneumo ~0.03µg/ml๏ Syphilis (only Bicillin L-A; FDA warning on confusion with C-R, C-R not for syphilis)
black box warning
Notable UW formulary penicillins: Pen VPenicillin V Spectrum:
๏ Similar spectrum to Pen G, but PO; acid stable but food interferes w/ absorption
๏ Difficult to achieve as high concentrations as for Pen G (not PO), so primarily for more moderate infections
๏ Since PO, as w/ all self-dosed antibiotics, counsel to complete the full course
๏ Caution about allergies, diarrhea
Notable UW formulary penicillins: AmpicillinAmpicillin Spectrum: note, w/o beta-lactamase inhibitor, similar to Pen G
๏ Used in combination w/ aminoglycoside for E. faecalis
๏ Even though amp can penetrate the outer Gram- bacterial membrane, many Gram- bugs produce beta-lactamases that can degrade ampicillin. For example:
๏ E. coli (80-90% of UTIs), 50% resistant to ampicillin due to beta-lactamase production
๏ Proteus mirabilis (UTIs), 30% resistant
๏ N. meningitidis generally sensitive, but some produce penicillinase
๏ N. gonorrhoeae significant penicillinase production now
๏ H. influenzae ~30% produce beta-lactamases
๏ Most nosocomial pathogens are resistant either due to innate impermeability or several resistance mechanisms including beta-lactamase production
๏ Note, significant enterohepatic recycling (as w/ bile acids): unmodified amp re-secreted into bile many cycles, leading to high intestinal levels of the drug. Potentially useful for Shigella, Salmonella, enteric infections. But, also greater risk of adverse effects such as diarrhea and C. difficile overgrowth.
Notable UW formulary penicillins: AmpicillinAmpicillin + Sulbactam spectrum (IV, IM):๏ Inclusion of beta-lactamase inhibitor (sulbactam) increases coverage of Gram- to also include:
๏ M. catarrhalis (otitis media, pneumo, sinusitis)
๏ H. influenzae (otitis media, pneumo, sinusitis)
๏ S. pneumoniae (otitis media, pneumo, sinusitis)
๏ Non-MRSA S. aureus, MSSA.
๏ Klebsiella
๏ Enterobacter
๏ E. coli
๏ N. gonorrhoeae
๏ Good activity against anaerobes
Notable UW formulary penicillins: AmoxicillinAmoxicillin Spectrum: similar spectrum to ampicillin (PO)
๏ Since oral absorption is better, less amox makes into enterohepatic recycling, less perturbation of gut flora, but also less effective w/ enteric infections than amp
๏ Ear, nose, throat infections, otitis media
๏ S. pneumoniae, S. pyogenes, H. influenzae
๏ Resistance to amox alone can be problematic; combination w/ inhibitor can be effective
๏ Still widely prescribed for otitis media
Amoxicillin + Clavulante spectrum (PO):๏ Similar spectrum to Amp + Sulbactam
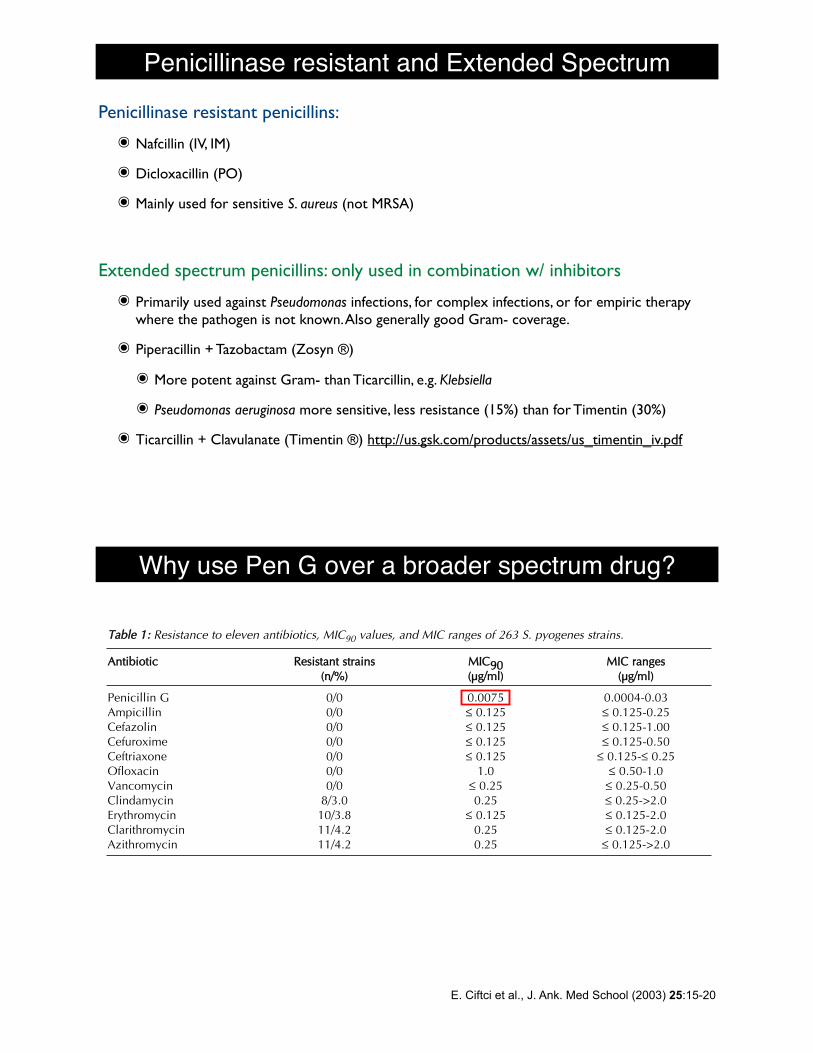
Penicillinase resistant and Extended SpectrumPenicillinase resistant penicillins:
๏ Nafcillin (IV, IM)
๏ Dicloxacillin (PO)
๏ Mainly used for sensitive S. aureus (not MRSA)
Extended spectrum penicillins: only used in combination w/ inhibitors
๏ Primarily used against Pseudomonas infections, for complex infections, or for empiric therapy where the pathogen is not known. Also generally good Gram- coverage.
๏ Piperacillin + Tazobactam (Zosyn ®)
๏ More potent against Gram- than Ticarcillin, e.g. Klebsiella
๏ Pseudomonas aeruginosa more sensitive, less resistance (15%) than for Timentin (30%)
๏ Ticarcillin + Clavulanate (Timentin ®) http://us.gsk.com/products/assets/us_timentin_iv.pdf
Why use Pen G over a broader spectrum drug?
around the world during the past three decades(4-10). This resistance has been temporallyrelated to increased or excessive use of macrolideantibiotics. Because of this relation, it isimportant to determine the geographic
prevalence of resistant S. pyogenes to facilitateclinical care and to address public healthconcerns.
Our study shows that penicillin is active for S.pyogenes in low MIC values. This finding is
17ERG N FT , LKER DO RU, HALUK G R Z, AHMET DERYAAYSEV, ERDAL NCE
TTaabbllee 11:: Resistance to eleven antibiotics, MIC90 values, and MIC ranges of 263 S. pyogenes strains.
AAnnttiibbiioottiicc RReessiissttaanntt ssttrraaiinnss MMIICC9900 MMIICC rraannggeess((nn//%%)) ((µµgg//mmll)) ((µµgg//mmll))
Penicillin G 0/0 0.0075 0.0004-0.03Ampicillin 0/0 ! 0.125 ! 0.125-0.25Cefazolin 0/0 ! 0.125 ! 0.125-1.00Cefuroxime 0/0 ! 0.125 ! 0.125-0.50Ceftriaxone 0/0 ! 0.125 ! 0.125-! 0.25Ofloxacin 0/0 1.0 ! 0.50-1.0Vancomycin 0/0 ! 0.25 ! 0.25-0.50Clindamycin 8/3.0 0.25 ! 0.25->2.0Erythromycin 10/3.8 ! 0.125 ! 0.125-2.0Clarithromycin 11/4.2 0.25 ! 0.125-2.0Azithromycin 11/4.2 0.25 ! 0.125->2.0
TTaabbllee 22:: Penicillin G MBC/MIC ratios of S. pyogenes strains.
MMBBCC//MMIICC NNuummbbeerr ooff ssttrraaiinnss
1 2462 154 28 0
16 032 0
Total 263
FFiigguurree 11:: Penicillin G MIC and MBC values of S. pyogenes strains.
E. Ciftci et al., J. Ank. Med School (2003) 25:15-20
Related Documents