167 BENIGN PROSTATIC OBSTRUCTION By RONALD W. REID, M.S., F.R.C.S. Surgeon, Essex County HospitaL Consulting Surgeon, Essex County Council Introduction The treatment of prostatic obstruction, to begin with the family doctor's responsibility, is still the business of the general surgeon despite the growth and partition of modem surgery from which urology has evolved. The separation of urology from general surgery has given impetus to the study of those dis- turbances of bladder function arising from pathological changes in the prostate gland, and recent years have seen the introduction and development of many new techniques for the removal of obstructing tissue. The review of benign prostatic obstruction attempted in this paper is based largely upon personal ex- perience, and for this and other reasons cannot in any way be complete. The multiplicity of techniques and the formidable size of the relevant literature render such a task im- possible; omissions and repetition of known facts are bound to occur, for which errors I beg the reader's indulgence. It is important to examine the terms which have been used in the past to describe the condition known clinically as prostatic obstruc- tion. Firstly, enlargement of the gland is not synonymous with obstruction. The majority of old men have some enlargement of the prostate but quite a small proportion of them suffer from disturbing symptoms or retention. Secondly, many of the most severe cases of obstruction have no enlargement of the gland whatever. The prostate gland lies at the neck of the bladder below the internal sphincter and surrounds the first part of the urethra. Its very position gives rise to grounds for con- fusion in diagnosis, and the fact that the bladder, aptly called the mirror of the urinary tract, is disturbed by practically all affections of the urinary system further adds to diagnostic difficulties. There is no doubt that benign adenomatous hypertrophy, known also as senile enlargement or adenoma of the prostate and fibrous hyperplasia or chronic fibrosis together account for the vast majority of cases of obstruction, but many other local conditions interfere with urine outflow. Among these may be mentioned contractures of the vesical orifice above the prostate which show them- selves as bars and bands of hypertrophied muscle. In the prostate itself cysts, abscesses and tuberculosis may cause confusion. Stones and diverticulae in the bladder produce vary- ing degrees of obstruction, strictures and neurogenic inco-ordination may give rise to symptoms superficially resembling those of prostatic obstruction. Whatever the essential pathology, obstruction at the bladder neck causes chronic retention of urine and deteriora- tion of renal function. History In the study of human affairs history is often the key to present problems and a guide to the future, and to this rule surgery is no exception. The student is advised to glance back into the past to learn of the struggles and triumphs of his surgical forefathers before attempting to evaluate the present state of medical knowledge and probe into the future. The symptoms of bladder disorders have been known from times immemorial, and that attempts were made by the ancients to over- come the obstruction is shown by the discovery of catheters in the equipment of Syrian and Egyptian surgeons. Anatomists of the Re- naissance mention the prostate gland, but do not seem to have recognized that it became enlarged and was the cause of urinary dis- turbance. To Lassar, a Venetian physician who died in I563 is attributed the discovery that the bladder could be blocked by swelling of the prostate. This surgeon is said to have practised successfully an incision of the neck copyright. on February 18, 2020 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.23.258.167 on 1 April 1947. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

167
BENIGN PROSTATIC OBSTRUCTIONBy RONALD W. REID, M.S., F.R.C.S.
Surgeon, Essex County HospitaL Consulting Surgeon, Essex County Council
IntroductionThe treatment of prostatic obstruction, to
begin with the family doctor's responsibility,is still the business of the general surgeondespite the growth and partition of modemsurgery from which urology has evolved. Theseparation of urology from general surgery hasgiven impetus to the study of those dis-turbances of bladder function arising frompathological changes in the prostate gland, andrecent years have seen the introduction anddevelopment of many new techniques for theremoval of obstructing tissue. The review ofbenign prostatic obstruction attempted in thispaper is based largely upon personal ex-perience, and for this and other reasons cannotin any way be complete. The multiplicity oftechniques and the formidable size of therelevant literature render such a task im-possible; omissions and repetition of knownfacts are bound to occur, for which errors Ibeg the reader's indulgence.
It is important to examine the terms whichhave been used in the past to describe thecondition known clinically as prostatic obstruc-tion. Firstly, enlargement of the gland is notsynonymous with obstruction. The majorityof old men have some enlargement of theprostate but quite a small proportion of themsuffer from disturbing symptoms or retention.Secondly, many of the most severe cases ofobstruction have no enlargement of the glandwhatever. The prostate gland lies at the neckof the bladder below the internal sphincter andsurrounds the first part of the urethra. Itsvery position gives rise to grounds for con-fusion in diagnosis, and the fact that thebladder, aptly called the mirror of the urinarytract, is disturbed by practically all affectionsof the urinary system further adds to diagnosticdifficulties. There is no doubt that benignadenomatous hypertrophy, known also as
senile enlargement or adenoma of the prostateand fibrous hyperplasia or chronic fibrosistogether account for the vast majority of casesof obstruction, but many other local conditionsinterfere with urine outflow. Among thesemay be mentioned contractures of the vesicalorifice above the prostate which show them-selves as bars and bands of hypertrophiedmuscle. In the prostate itself cysts, abscessesand tuberculosis may cause confusion. Stonesand diverticulae in the bladder produce vary-ing degrees of obstruction, strictures andneurogenic inco-ordination may give rise tosymptoms superficially resembling those ofprostatic obstruction. Whatever the essentialpathology, obstruction at the bladder neckcauses chronic retention of urine and deteriora-tion of renal function.
HistoryIn the study of human affairs history is often
the key to present problems and a guide to thefuture, and to this rule surgery is no exception.The student is advised to glance back into thepast to learn of the struggles and triumphs ofhis surgical forefathers before attempting toevaluate the present state of medical knowledgeand probe into the future.The symptoms of bladder disorders have
been known from times immemorial, and thatattempts were made by the ancients to over-come the obstruction is shown by the discoveryof catheters in the equipment of Syrian andEgyptian surgeons. Anatomists of the Re-naissance mention the prostate gland, but donot seem to have recognized that it becameenlarged and was the cause of urinary dis-turbance. To Lassar, a Venetian physicianwho died in I563 is attributed the discoverythat the bladder could be blocked by swellingof the prostate. This surgeon is said to havepractised successfully an incision of the neck
copyright. on F
ebruary 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.258.167 on 1 A
pril 1947. Dow
nloaded from

POST-GRADUATE MEDICAL JOURNAL
of the bladder through the perineum to relieveretention.There is no doubt that the early history of
prostatic obstruction is inseparably linked upwith that of stone, and that from the Re-naissance onwards itinerant stone cuttersroamed 'throughout Europe hoisting theircoloured poles in the villages which they tem-porarily visited. From the hands of thewandering lithotomists stone cutting passedto the qualified surgeons, and in this countryWilliam Cheseldon was one of the most ableand successful. It is possible that partialprostatectomy was first performed by chancewhen a master stone cutter enucleated part ofthe prostate gland during the passage of alarge stone through the forcibly dilated urethra.John Hunter, Benjamin Brodie and Chopartattempted to relieve prostatic obstruction bytunnelling the prostate with a metal catheter,and Physick of Philadelphia produced a dis-tensable bougie which designed to dilate thenarrow urethra. The first attempt to removeprostatic tissue is attributed to Mercier whodevised a punch with which to tunnel thegland, but most attempts were followed bydisastrous haemorrhage and infection. InI873 Bottini invented a galvanocautery whichoperated in a manner similar to the punch ofMercier with the additional advantage thathaemorrhage was better controlled.
After the introduction of anaesthetics andantiseptic surgery the bladder could be openedfrom above and the prostate easily approached.By i88o suprapubic cystotomy was recognizedas a safe procedure for the relief of retentionand McGill of Leeds advocated excision ofparts of the gland. In the last decade of theigth century the operation of completeenucleation of the adenomatous prostate revo-lutionized bladder surgery. With this radicaloperation two great names are associated, thoseof Freyer and Fuller. In Europe Freyer,whose paper was published in I9OI, is lookedupon as the father ofmodem prostatic surgery,and in America Fuller, whose account ap-peared in I893, is accorded the title. Whoeverfirst practised the new total enucleation, therecan be no doubt that the results were stagger-ingly good. Freyer who was a strong andcourageous surgeon with the finest judgementperformed over i,5oo prostatectomies with a
mortality of 5.3 per cent., a figure of which anypresent day surgeon might well be proud, butcases were carefully selected and there musthave been many turned away. Prostaticsurgery was taken up by the great surgeons ofthe day; before long Young of Baltimoreintroduced his -perineal approach and thesuprapubic was modified by ThompsonWalker, Harris and many more. The last 20years has seen the development of endoscopicprostatectomv by Stem and McCarthy,Bumpus, Thompson and others, 'a departurefrom open surgical techniques which has hadgreat influence on and may eventually revolu-tionize prostatic surgery.
PathologyThe pathology of prostatic obstruction can
conveniently be considered under two head-ings
(a) The, pathological changes occurring inthe gland" itself which cause obstruction tomicturition.
(b) The effects of chronic retention and backpressure upon the bladder, ureters, kidneys andcardiovascular systems.
(a) In the great majority of cases prostaticobstruction is caused by benign adenomatoushypertrophy of the gland, a condition which isetiologically obscure despite much study on thepart of clinicians and pathologists. All classesof the community are affected equally and themarried and celibate alike. This senile en-largement occurs usually in men over 6oyears of age when some growth of the glandnormally occurs. Among the theories ad-vanced have been that the hypertrophy resultsfrom obscure involutionary trends in the endo-crine system, and from changes similar to thosewhich occur in the female at the menopause.The enlargement begins with small nodes ofglandular hyperplasia which are separated fromthe normal parent gland by capsules composedof compiessed normal prostatic tissue. 'Thesenodes, at first small, eiilarge to form irregularclumps which stretch' and distort the prostaticurethra and bulge up into the bladder to forMpedunculated lobes or collars surrounding theinternal urinary meatus. Attempts have beenmade to distinguish the various lobes of theprostate which give rse primarly to obstruc-
I68 AXpril, 1947copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

ABENIGN PROSTATIC OBSTRUCTION
tion, and attention has been drawn to the im-portance of the sub-cervical and sub-trigonalglands. However, little is to be gained by thisdetailed study of local anatomy, for in generalthe lateral lobes show the most marked en-largement; small adenomas may causeobstruction or a mass the size of the fist maygrow before retention occurs. Whatever theirsize adenomatous tumours can invariably beenucleated from their false capsules with easeand satisfactory results.
In diffuse fibrous hyperplasia, a conditionwhich is second in importance to benignadenomatous hypertrophy, there is little doubtthat long standing inflammation plays an im-portant part in etiology. The term hyper-plasia may be inaccurate, suggesting as it doesincrease of tissue formation. It is probablethat chronic prostatitis lies behind this form ofenlargement and that in the early stagesoedema and chronic inflammation with roundcell infiltration causes the gland to enlarge,but that as time goes on the swelling subsidesand scarring follows in the trail of inflamma-tion with shrinkage of the gland. On ex-'amining such a prostate the cut surface isfound to be of even texture, firm, leathery orrubbery and showing none of the sphericalglandular enlargement which characterizesbenign adenomatous hypertrophy. This glandcannot easily be removed whole as its sheathis the true prostatic capsule which is affectedby the diffuse inflammatory change andattempts at enucleation, as would be expected,are associated with tearing of the tissues andgross surgical trauma. Microscopic examina-tion of this gland confirms the gross appearanceand in place of the spherical adenomatousglobes, diffuse infiltration with leucocytes,epithelial degeneration and fibrous changes areseen. In the early stages of diffuse hyper-plasia increased epithelial activity may causeprostatorrhoea, but as degeneration and fibrosisset in the gland compresses the urethracausing increasing obstruction to bladderevacuation, and in some cases inspisatedsecretion leads to the formation of endogenousprostatic calculi.The chronic inflammation of diffuse fibrous
hyperplasia may have its main impact uponthe sub-trigonal glands which lie just insidethe internal meatus under the trigone. In this
inflammation the bladder mucous membraneand the trigonal muscle may take part and abar be formed which proves an effectiveobstacle to micturition. Such bars may existwith or without other changes in the prostategland itself and may require removal as aseparate procedure during the various formsof prostatectomy to be described. They canaccount for post-operative osbtruction unlessadequately treated.
(b) Secondary changes in the urinary tract.In 1917 Young showed that at the beginningof micturition the trigone is depressed by con-traction of the trigonal muscle which pulls themedian and posterior parts of the prostatedownwards to open the internal urinarymeatus. Contraction of the general bladdermusculature follows and the urine is expelled.This movement of the trigone can be easilyconfirmed by cystoscopy. By whatever methodthe prostate obstructs the bladder, whether itis by elongating and distorting the urethra orby compressing it, the onus of opening theinternal sphincter rests with the trigonalmuscle and so one of the earliest signs ofprostatic obstruction is hypertrophy of thismuscle, a,change soon followed by generalbladder hypertrophy. The bladder muscula-ture is normally an even sheet of crossingmuscle bands completely supporting themucous membrane, but in obstruction theintravesical pressure forces pouches of mucousmembrane through the hypertrophied'bands toform saccules or diverticula; this appearanceis characteristic of a bladder obstructed at itsoutlet. The ureters which, by peristalticaction, inject urine into the bladder at frequentintervals are protected by a valvular muscularmechanism at their orifices, sufficient for aconsiderable time to protect the upper urinarytract from increased intravesical pressure, andthere is little doubt that this mechanism re-mains effective for a very long time. However,as the bladder distends the ureteric orificeslose their efficiency and no longer protected,the kidneys must secrete against an increasedload with results to be discussed later. Thereare gounds for believing that the effects ofprostatic obstruction on the kidneys are notalways entirely due to incompetence of theureteral sphincters, but that the enlarginggland itself may actually compress or distort
A,&-impril) I947 I69copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

POST-GRADUATE MEDICAL JOURNAL
the lower ends of the ureters thus giving riseto obstruction at the ureteric orifices as well asat the vesical outlet. That such obstructionoccurs in carcinoma is well known but it is notgenerally realized that large simple glands maydo the same thing. Many surgeons have notedthat bladder drainage fails occasionally to re-lieve renal back pressure and that prostatec-tomy is a more satisfactory primary procedure.This paradox can be explained by consideringthe influence of prostatic enlargement on thetrigone as a whole.When pressure in the upper urinary tract
rises the kidneys secrete against a resistanceand the tubules are the first structures to suffer,causing inefficient concentration of urine andpolyuria. To combat increasing resistance,filtration pressure must rise and this in turnreflects upon the cardiovascular system causinghypertension and cardiac hypertrophy. Theold clinicians noted the association of the en-larged prostate and the enlarged heart. Astime goes on renal function deteriorates,uraemia develops and is followed by cardiacfailure with attacks of nocturnal orthopnoeaand pulmonary congestion.At any stage of prostatic obstruction in-
fection may reach the bladder through theurethra or by the blood stream, and theorganisms multiply in the stagnant urine andspread like wild fire to the kidneys, where thedestructive effects of pressure are increasedten-fold. Hence the importance of avoidingcareless instrumentation. Infection once estab-lished leads to rapid deterioration of generalhealth and kidney function, encourages theformation of stones and ,adds greatly to thegravity of the situation.
SymptomatologyThe symptoms of prostatic obstruction are
well known and consist of gradually increasingdifficulty and frequency of micturition, of athin or halting stream and attacks of acute re-tention of urine. They vary in their severityfrom time to time in the same case; they areoften thought by the patient to be natural toold age. Occasionally transient haematuriapresents or the chronic ill health and anaemiaof failing kidneys, and not bladder trouble,sends the man to his doctor. As obstructionof the urine outflow develops so do the muscles
of the bladder hypertrophy in response toincreased work. At first the hypertrophy issufficient to overcome the obstruction andapart from a little delay or urgency there maybe few symptoms, but against increasingobstruction the compensation fails, residualurine makes its appearance and the bladderundergoes progressive and silent dilatation.Frequency then becomes conspicuous and asback pressure makes its mark upon renalfunction a more dilute urine is secreted andpolyuria by day and night further adds to thefrequency. As obstruction and renal failureincrease the patient's nights are more dis-turbed, eneuresis may develop, thirst increaseand lack of sleep and uraemia bring the patientto a sorry state. Should severe infectionsupervene, intolerable frequency, stranguary,haematuria and bladder irritability are followedby chills, pain in the loins and rapid physicaldeterioration. If the patient survives the in-fection without acute retention he developssome immunity, but stones may grow andinfection flares up occasionally in attacks ofepididymitis.
Physical SignsExamination of a case of suspected prostatic
obstruction begins with a general survey of thepatient. Hard and tortuous temple arteries,baldness or deafness and the arcus senilissuggest that the patient is older than his years.Drowsiness, a dry tongue and heavy breathingare characteristic of the uraemic state. Breath-lessness and oedema of the ankles may indi-cate cardiovascular deficiency and call for aninvestigation of the heart, lungs and the bloodpressure and for the advice of a generalphysician before treatment is planned. Thepupillary reactions and tendon reflexes shouldbe checked and the external genitalia andtestes inspected. On examining the abdormena distended bladder may be found, which ifpresent immediately after micturition in-dicates gross retention. If the patient is nottoo fat or muscular, pressure upon the ap-parently empty bladder may cause the desireto pass water, and if urinary infection ispresent the bladder and the kidneys may betender. To examine the prostate per rectumthe knee elbow position is very satisfactory;the gland may also be palpated bimanually
Aprliil, I1947170copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

BENIGN PROSTATIC OBSTRUCTION
with the patient on his side, the knees up andthe abdominal muscles well relaxed. It isimportant to recall that the prpstate gland ispushed down and rotated by the distendedbladder and its size is thereby exaggerated asjudged by rectal examination. For trueassessment the bladder must be empty. Mostsurgeons have their own size indexes for theprostate gland; it has been my practice torecord a gland twice the normal size as beingplus one and an enormous prostate of greatdepth and width and bulging far back intothe rectum as being plus four. The size, con-tours, consistency and fixity of the prostateand the state of the vesicles should be notedand recorded by drawing or on a special chart.
Special ExaminationsBefore a plan is made for the treatment of a
case of recognized or suspected prostaticobstruction the surgeon requires all theevidence he can muster. Firstly an X-rayshould be taken of the whole urinary tract todiscover whether the case is complicated bystones, or unsuspected carcinoma has throwndown secondary deposits in bone. Secondly,since bladder obstruction sooner or laterdamages the kidneys special tests of renalfunction must be carried out to supplementclinical examination. The first sign of in-cipient renal failure is a persistently lowspecific gravity of the urine and nocturia. Thedamaged kidneys cannot concentrate neithercan they perform their excretory functionmainly by day. A persistently low specificgravity of the urine and the passage of largevolumes by night indicate that failure has setin, but the gravity test upon which Freyerplaced so much confidence, is time-consumingand has been supplanted by the estimation ofrenal function by other means. In my opinionthe most reliable and convenient test is theurea content of the blood which normally isless than 45 milligrammes per cent. This testcombined with a sound clinical assessment ofthe case provides all the evidence the surgeonrequires to make his decision, and more com-plicated investigations are time-consumingboth for nursing staff and the laboratory. Inordinary circumstances they need not be pur-sued but they are doubtless of value in theborder-line cases.
A complete examination of the urine shouldbe carried out including culture for bacteria.The presence of albumen, blood, casts or pusindicate that the urinary tract is suffering fromdamage other than that due to simple obstruc-tion. The bacterial content of the urine givesvaluable information on the management of thecase, for heavy infection may require a periodof preliminary bladder drainage before radicalsurgery can be undertaken sith safety. In-formation will also be gained as to the thera-peutic cover necessary during the operationand post-operative period.
It is the custom of many surgeons to pass acatheter and measure the residual urine, for ithas been authoritatively stated that thepresence of 4 oz. or more is an absoluteindication for surgical treatment. The presenceof residual urine is no-single guide or absoluteindication for surgery unless it is large inamount, obvious on abdominal examinationand associated with severe symptoms andsound evidence that renal function is suffering.In the aged and infirm a considerable amountof residual urine is compatible with comfortand safety, and the patient will live longer if heis not subjected to instrumentation and istreated conservatively. However, the amountof residual urine gives important informationand should be determined in every case wereit not for the risks of catheterization. It haslong been known that to pass a catheter on anobstructed bladder without the most asepticprecautions, such as those obtaining in theoperating theatre, is dangerous, for the bladderis easily infected with organisms carried upfrom the pendulous urethra and the con-sequences of ascending urinary infection aredisastrous and unpredictable. To the im-portance of asepsis in every stage of prostaticsurgery the attention of surgeons has oncemore been called by Wilson Hey.
Cystoscopy provides valuable informationupon the exact anatomy of prostatic obstruc-tion and by its use general bladder or trigonalhypertrophy can be seen, and the presence orabsence of diverticula, growth or stonesdetermined. For this purpose the direct visioncystoscope is probably the most convenient asit gives an excellent view of the prostaticurethra and the bladder neck. However, aswith catheterization, cystoscopy is not free
Ai.zarrill 1947 171copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

I72 POST-GRADUATE MEDICAL JOURNAL April, I947
from danger and should on no account beadopted as an out-patient 'procedure, butshould be reserved for the moment beforeoperation.
Differential DiagnosisThe differential diagnosis of prostatic
obstruction resolves itself into the considera-tion of causes other than those within theprostate which may interfere with the bladderfunction and urine outflow, and the examina-tion of the exact nature of the prostaticpathology. 'Frequency and polyuria arisefrom general diseases, especially those affectingthe circulatory system and kidneys. Tabesdorsalis and other affections of the centralnervous system interfere with bladder functionand cause chronic retention; cystitis, tuber-culosis, stone and, bladder new growths mayproduce symptoms easily confused with thoseof prostatic obstruction, and in the urethrastrictures may simulate and accompanyprostatic enlargement. By a careful attentionto history, physical examination, X-ray andlaboratory investigations, the differentialdiagnosis can be narrowed down to, prostaticabnormalities. The exact nature of thepathological change in the gland cannot alwaysbe determined until microscopy after opera-tion, but generally speaking the finger in therectum will solve the problem. Benignadenomatous hypertrophy gives rise torounded elastic swellings which move in amass freely within the pelvis. Diffuse fibroushyperplasia *causes some enlargement of thegland, in which case it is leathery, broad andflat, or slightly bulging and later on as fibrosissupervenes it is contracted and hard. It is.always movable. in the pelvic cavity, harderthan benign hypertrophy but not stony andfixed as in carcinoma. Calculi may be felt inthe fibrous gland and may be confused withthe somewhat similar nodularity of tuber-culosis- or carcinoma. Tuberculosis of theprostate is invariably associated with tuber-culosis of the vesicles. and. very often dise;asein. the testicles and kidneys, and when sus-pected a general survey of the urinary systemshould be undertaken and examination madeof the urine for tubercle' bacilli. Carcinomamay arise in a previously normal or.abnormalprostate and characteristically feelslike a stony
plaque which obscures the median groove andupper margin of the gland, extends later to thepelvic cellular tissue to fix it and finally spreadsround the rectum along the pelvic floor todeposit secondaries in bone. Confirmatorychanges in the serum acid phosphatase levelmay be found.To sum up the main points in the investiga-
tion of a case of prostatic obstruction, most in-formation can be gained by general clinicalexamination, X-rays are important for dis-covery of stone or secondary deposits frommalignant disease, the blood urea test is thesimplest and most reliable index of renaldamage and detailed examination of the urineis,essential before the plan of treatment can becarried out. More complex investigationssuch as intravenous pyelography, urea clear-ance tests and cystoscopy apart from animmediate pre-operative procedure, thoughessential in the. difficult case, are, in myexperience, unnecessary as a routine if clinicalstudy is thorough.
ComplicationsThe complications of prostatic obstruction
are many, affecting not only the genito-urinarytract but the cardiac and pulmonary systems aswell, and they include many of those con-ditions which may properly be called thediseases of old age. Commonly encounteredare
(I) Acute retention of urine.(2) Cystitis and ascending renal infections.(3) Diverticulum.(4) Bladder stone.(5) Epididymo-orchitis.(6) Uraemia.
Acute RetentionAcute retention of urine, precipitated by ex-
posure to cold, over indulgence in drink,-infection or any acute illness- such as fracture orpneumonia, is sometimes the first symptom. ofprostatic obstruction in which case the gland isoften large and soft and prone to congestion,and the kidneys unaffected. In other cases,the acute attack follows long standing chronicretention-with advanced renal damage. Thetwo conditions should be distinguished for thefirst variety often responds to simple treatment
copyright. on F
ebruary 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.258.167 on 1 A
pril 1947. Dow
nloaded from

BENIGN PROSTATIC OBSTRUCTION
such as rest, morphia and hot baths and in thelast resort the passage of a catheter with fullasepsis, while the second type demands themost careful decompression to avoid pre-cipitating renal haemorrhage and irreversiblefailure. If a catheter is used, careful asepsis,good local' anaesthesia, generous lubricationand extreme gentleness must be employed,The best instrument is the Foley self-retainingcatheter which, having a distensible bag at itstip, requires no penile strapping to keep it in.Thus secretion drains freely out provided thecatheter is smaller than the urethral calibreand urethritis and epididymitis are avoided.It is wiser also to leave a catheter in situ ratherthan employ repeated passage which maycarry up infection. It can be removed whenthe general lines of treatment have beensettled. Should a soft rubber catheter notpass, a bicoud6 gum elastic may be gentlytried, but silver instruments should beeschewed. Damage to the urethra or prostateby rough instrumentation prejudices thepatient's chances of safe recovery.
If catheterization is impossible or dangerous,suprapubic cystotomy or aspiration is calledfor. The latter procedure, though less satis-factory than cystotomy is simple, but in myexperience neither satisfactory nor safe.
(2) CystitisInfection may reach the obstructed bladder
from the blood stream or by instrumentation.In its severe form, fortunately uncommon,symptoms are always aggravated, acute re-tention may supervene, the invasion mayspread to the kidneys giving rise to chills, feverand septic pyelonephritis with all its disastrousconsequences. Severe infection with obstruc-tion is an absolute indication for free drainageof the bladder, forced fluids and properlychosen chemotherapy. As prolonged drainageis usually necessary cystotomy is more satis-factory than the indwelling catheter which maycause an aggravating urethritis and epididy-mnitis.
(3) DiverticulumDiverticula of the bladder, so easily over-
looked, are large sacs unsupported by vesicalmuscle, and art not to be confused with thesmall sac-s--pushed into the" bladder wall by
increased intravesical pressure. The latterare of little significance and disappear whenobstruction is relieved, but the former,although they owe their growth to bladderobstruction, do not diminish in size when theoutflow is cleared but remain as cul de sacswhich will harbour great quantities of urineand foster infection. Prostatic obstructioncomplicated by diverticulum cannot be curedby prostatectomy alone, and in suitablepatients the diverticulum should be removedfirst and the bladder drained suprapubicallyfor a week or two before an attack is made uponthe prostate through the suprapubic wound orby other methods. If prostatectomy is done inthe presence of a large diverticulum, bladdersepsis is certain to be troublesome and thesubsequent diverticulectomy made moredifficult by scar tissue.
(4) Bladder StoneStone and prostatic obstruction have long
been confused. Long standing obstruction,especially with infection, favours the formationof stones which do not always give rise to theclassical symptoms of stranguary, stammeringbladder and painful stoppages. For thisreason all cases should be examined by X-ray,including in the field the kidneys and bladder.Large or multiple stones should undoubtedlybe removed by suprapubic cystotomy, and ifother conditions allow the prostate may beenucleated at the same time. Small stones,and those lying above the fibrous type ofprostate can be crushed and removed withBigelow's evacuator, the obstruction beingtreated at the same time by endoscopicresection.
(5) EpWididymo-orchitisThis complication occurs more often after
prosjatectomy than before, and most surgeonsadvise pre-operative division of the vas as aprophylactic measure. There seems littledoubt that infection spreads along the vasfrom the urethra or prostatic bed. Beforeoperation this complication occurs if an in-dwelling catheter is so applied as to interferewith the natural drainage of secretions causedby the catheter foreign. body. Too large acatheter, rough work and subsequent oedema,tight-straps and -caked dressings on -the glans
A,pril, I947 173copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

POST-GRADUATE MEDICAL JOURNAL
penis, all interfere with urethral drainage andpredispose to ascending infection. Chemo-therapy, attention to asepsis and to catheterfitting with adequate support of the testes bywadding, have in my experience eliminatedthis complication; so much so that tying thevasa has been abandoned for 5 years.Epididymo-orchitis is uncommon after thetransurethral operation, possibly due to thefact that little damage is done to the prostaticbed and the patient is never confined to bedfor more than a few days.
(6) UraemniaIt is a remarkable fact that the kidneys can
withstand the effects of back pressure for yearswithout gross damage provided that, amongother things, the ureteric orifices are neitherobstructed nor incompetent, and that fromsevere impairment complete recovery ispossible. Unrelieved obstruction in time leadsto renal failure and uraemia, a metabolicdisaster associated with, but not caused by, arise in the urea content of the blood. Thetreatment of uraemia, the clinical picture ofwhich is well known, consists of the relief ofthe causative obstruction and of measures toincrease the output of urine.
Obstruction must be relieved gradually if itis of long standing and the renal function de-pressed. It is usual to drain the bladder bycatheter or suprapubic tube and to attach tothe outlet some mechanism such as a trans-fusion drip feed and clip which will control therate of decompression. Haemorrhage in-dicates too much haste and generally I2 to 24hours must elapse before the urine is let runfree.
Unless the kidneys are irrevocably damageddiuresis will follow decompression providedthe blood pressure is maintained. This is amost important factor for the kidneys cannotsecrete unless the blood pressure is sufficientto maintain a vigorous glomerular circulation.Shock and debility should be treated by plasmaor blood transfusion if need be 'until theestimated normal blood pressure is restored.At the same time the patient must drink veryfreely and nurses must encourage or bully him,especially if he is drowsy. Morphia and othersedatives should be avoided lest the patient'sdrowsiness is increased, his drinking aban-
doned and his blood pressure lowered, all ofwhich put him on the path to renal failure.Intravenous fluids, particularly saline, shouldbe used with the greatest care for in the sickand aged the pulmonary circulation is easilyoverloaded with subsequent oedema of thelungs. Oedema of the lungs induces anoxiawhich, in turn, causes more oedema andanoxia of the heart muscle and the renalcortex. In the presence of a failing heart anddropping blood pressure, intravenous fluidscan easily seal the patient's fate and should beused only in the presence of definite signs ofdehydration and when other methods of takingfluids fail.
TreatmentThe treatment of prostatic obstruction
cannot be bound by hard and fast rules; itsaim is the saving of life and restoration ofnormal micturition by removal of obstructingtissue; it depends upon three main con-siderations:
(i) Obstruction is caused by many differentpathological changes in or near the prostategland, for the treatment of which have beendevised many operations, none suitable forevery case. From the point of view of thetechnical problems involved, the causes ofsimple obstruction fall naturally into twogroups. Benign adenomatous hypertrophy,the big group, different from all others in thatthe obstructing tissue-can be cleanly enucleatedfrom its false capsule with satisfactory results.On the contrary, diffuse fibrous hyperplasiaand the common forms of bar cannot be soenucleated and must be resected either by openoperation or through the urethra. Enucleationis one of the simplest techniques in operativesurgery, transurethral resection one of themore difficult.
(2) Prostatic obstruction generally affectsthe aged whose general physique is fit towithstand neither the strain of a long or severeoperation whatever its intrinsic technicalmerits, nor protracted illness and recumbency.Be it allowed that among the cases are manymiddle aged and fit men, the fact remains thatthey do not provide the real problem. Anoperation suitable for them may be quite un-safe for the aged; conversely, what is safe for
April, 1947I74copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

BENIGN PROSTATIC OBSTRUCTION
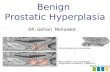
Ascending pyelogram showing dilatation of upperurinary tract due to enlarged prostate.
In this case there is no obstruction of the ureter.
ApFril, I947 175copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

POST-GRADUATE MEDICAL JOURNAL
Foley catheter with bag empty and full.
AAA,Pril, 1947I76copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

BENIGN PROSTATIC OBSTRUCTION
Gershom Thompson resectoscope with fenestra closed.
177Ap,ril, I947copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

POST-GRADUATE MEDICAL JOURNAL
Head of Gershom Thompson resectoscope with fenestra open showing circular blade and diathermy electrode.
I78 -zApril, 1947copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

April, I947 BENIGN PROSTATIC OBSTRUCTION
the aged must be safer still for the middle agedprovided always that the method gives satis-factorv results.
(3) In many instances the patient is wornout, the urinary tract infected, the kidneysdamaged or the cardiovascular and pulmonarysystems embarrassed. The surgeon must takeaccount of these and other factors in planningtreatment and the advice of a physician shouldbe freely taken. Treatment on general linesand prophylaxis for complications should becarried on throughout for the operation is but astep, important but not paramount in thescheme.
Preliminary DrainageSince prostatic obstruction causes retention
of urine, in some cases complete, in otherspartial, the question of preliminary drainage isof importance. Acute retention must be re-lieved unless the patient can be transferred tohospital and have his prostate removed withina few hours. Chronic retention is oftenassociated with sepsis and renal failure orother complications rendering immediateprostatectomy dangerous, and the only hope ofrelief and improvement lies in adequatedrainage. Drainage relieves back pressureupon embarrassed kidneys and allows freeexit of infected urine but at the same time thetube introduces infection into the bladderwhich may be sterile so far. Despite WilsonHey's advocacy of primary prostatectomy foracute retention regardless of complications,most surgeons would agree that there arecertain definite indications for simple drainageas follows
(a) Acute retention.(b) Gross bladder sepsis.(c) Advanced renal failure.(d) Extreme feebleness of the patient and
cardiovascular degeneration.Drainage of the bladder can be effected
either by indwelling catheter or suprapubiccystotomy. The indwelling catheter is simplein use, drains the bladder from its lowest pointand, provided it is of small size and passed andfixed without damage to the- urethra, it can beretained for 2 or 3 weeks. The Foley typecatheter has many great advantages. Chang-ing the catheter does nothing but carry up into
the bladder infected secretion from, thependulous urethra. Suprapubic cystotomyhas the great advantage that drainage can bemaintained for an indefinite time and unlessthere are sound reasons for opening the bladderfreely, the tube should be inserted under alocal anaesthetic by the trocar and cannula suchas that devised by Riches. By this' meansactive surgery is kept to the minimum-anadvantage in the aged. The tube should beinserted high in the bladder, taking care toavoid the peritoneum, in order that the obliquehigh stoma may subsequently close easily.There is nothing more trying to shut than afibrous fistula situated upon the symphysispubis.
In the absence of complications there isnothing to be .gained by preliminary drainageof any kind and the sooner a direct attack ismade upon the obstruction the better for thepatient. With complications, efficient drainagecombined with hydrotherapy and suitableantiseptics diminish infection and prostaticcongestion, and improve renal function, thusmaking the subsequent major operation safer.
Operative TreatmentThe operations commonly employed for the
relief of prostatic obstruction are listed andgrouped below. The steps of many of theseoperations are well known, and no attempt willbe made to give details of technique; only'thebroad outline can be described,
A. SUPRAPUBIC CYSTOTOMY.B. TRANSVESICAL PROSTATECTOMY.
(I) Simple enucleation with open drain-age. (Freyer-Fuller operation.)
(2) Simple enucleation with open haemo-stasis and drainage. (ThompsonWalker operation.)
(3) Simple enucleation with restoration oftrigone, closure of bladder andcatheter drainage. (Harris operation.)
(4) Simple enucleation with open haemo-stasis, closure of the bladder andcatheter drainage. (Wilson, Heyoperation.)
C. EXTRAVESICAL PROSTATECTOMY.(i) Perineal prostatectomy. (Young's
operation.)
copyright. on F
ebruary 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.258.167 on 1 A
pril 1947. Dow
nloaded from

180 POST-GRADUATE MEDICAL JOURNAL April, 1947
(2) Retropubic prostatectomy. (Millin'soperation.)
D. TRANSURETHRAL PROSTATECTOMY.(i) Electro-resection of Stern, McCarthy,
Kirwin and others.(2) Cold punch of Braasch, Bumpus,
Thompson, Emmett and others.
Suprapubic CystotomySuprapubic cystotomy unless performed as a
temporary measure is a confession of failure.Unfortunately many old and feeble patientsare fit for nothing more than this simpleoperation which, despite the simplicity, carriesa high mortality. In my series the mortality isin the neighbourhood of 30 per cent., which isevidence of the extreme debility of rejectedcases. It is the common experience of mostsurgeons, however, that many cases sufferingfrom advanced failure including gross oedemaand ascites may, in the course of time, recoversufficiently to warrant a more radical operation.It is surprising how prolonged bladder drain-age reduces the size of the soft prostate andhow easily normal micturition can be restoredin what were once impossible cases by a smalltransurethral resection. The steps of supra-pubic cystotomy are well known but I wouldstress the importance of doing the operationunder local anaesthesia and using the simplesttechnique possible.
Transvesical ProstatectomySimple enucleation of the prostate with
open drainage is one of the most satisfactoryoperations in surgery, for by it all the obstruct-ing tissue is removed, haemorrhage can easilybe controlled by packing or haemostatic bagsand closure of the bladder wound usually takesplace within 20 days. The operation can beperformed by anyone -with average surgicalknowledge and skill, but it is often associatedwith 'considerable shock, with reactionaryhaemorrhage and bladdet sepsis, with severaldays complete recumbency and many weeksinvalidism. Simple though it is to perform,this operation is severe, and in average handscarries a mortality of io or more per cent. Ifthe rejects and the failures are taken into con-sideration the results cannot be looked uponwith complacency. The more careful control
of haemorrhage advocated by ThompsonWalker gives better results, but the operationis more prolonged and severe and greatersurgical skill is required for its performance.Thompson Walker with his great experienceand care carried out this operation withbrilliant results. Ten years ago Harris intro-duced his operation in which haemorrhage wascontrolled by ligature and suture and theprostatic bed was covered with flaps of vesicalmucosa and the bladder closed. This idealoperation in Harris's hands produced goodresults, but it is a severe procedure for theaged requiring a long anaesthetic, and suturingthe raw area interferes with drainage and maycause spreading pelvic cellulitis and post-operative obstruction due to scar tissue.Failure to secure complete haemastasis hascaused many surgeons to modify this operationby inserting a fine suprapubic tube, a safetymeasure which does not detract from thevalue of the operation. Wilson Hey of Man-chester has practised primary prostatectomvin all cases despite complete retention or a highblood urea and his results are most impressive.He stresses the importance of a most rigidaseptic technique, and having removed theprostate and controlled haemorrhage with thefree use of the diathermy, he passes a catheterretrograde from the bladder to the penileurethra, thus avoiding pushing up organismsfrom the pendulous urethra, when the catheteris inserted in the usual manner. At the end ofthe operation the bladder is closed, filled withcitrate and connected to a closed drainagesystem. I have not been able to achieve thedegree of haernastasis required for primarybladder closure without the very heavy use ofthe diathermy, but my limited experience ofthis operation is so far satisfactory. Sepsis andsloughing have not occurred nor has there beenbleeding with returning blood pressure. Thereseems to me no reason why this operationcould not be made safer by the insertion of afine suprapubic tube as in the modified Harrisoperation, nor would it seem that much isgained by the somewhat tedious insertion ofthe catheter in retrograde direction.
Extravesical ProstatectomyIn cxtravesical prostatectomv the gland can
be approached from behind through the
copyright. on F
ebruary 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.258.167 on 1 A
pril 1947. Dow
nloaded from

BENIGN PROSTATIC OBSTRUCTION
perineum, or from in front across the cave ofRetzius. In the early part of the century,Hugh Hampden Young invented his perinealoperation by which can be removed not onlyadenomatous tumours but fibrous glands andcarcinoma. The operation has modifications,but basically consists of an approach to theposterior surface of the gland through theperineum, incision of the capsule and removalof all obstructing tissue. Haemorrhage is con-trolled under direct vision, stones can be re-moved from the bladder and the normalanatomical arrangements are restored by sutureafter a tube has been inserted into the bladder.The perineal operation has given brilliantresults in the hands of Young and his followers,but it has never been really popular in thiscountry. My experience of this operation istoo limited for comments to be of value, as thefew cases in which this operation was employedwere excellent surgical risks and could havebeen cured by almost any method, there wereno deaths, and the two complications incon-tinence and fistula were not encountered. Itis my impression that the operation cannot becarried out in the aged with impunity.
Retropubic prostatectomy. It is no exaggera-tion to say that in 1945 the urological worldwas startled by the introduction of retropubicprostatectomy. Millin, whose experience ofprostatic surgery in England is unrivalled, didnot accept the limitations implied by theknown methods of prostatectomy and devisedhis own approach. Briefly Millin's operationconsists of exposing the anterior surface of theprostate through the cave of Retzius. Haemor-rhage, chiefly from the dorsal penile vein,having been checked by diathermy or ligature,the true and false capsules are incised trans-versely and a line of. cleavage sought. Theadenomatous masses are separated by blunt orscissor dissection in a downward directionuntil the urethra at the apex of the prostate iscleared all round. This structure is severedand the mass turned upwards and dissectedfree until it is attached to the bladder solely bya cuff of mucous membrane, which is thendivided and the tumour removed. The open-ing into the bladder is enlarged by extisionof a wedge from the truncated cuff to avoidpost-operative obstruction by a diaphragm anda catheter is passed' up the urethra into the
bladder. Haemostasis is secured by amplesuture of the prostatic capsule and theabdomen is closed with simple drainage of theretropubic space. The catheter is attached toa closed drainage system and is removed in3 to 7 days. This operation gives good results,haemorrhage from the bladder is uncommon,normal micturition is soon re-established andthe wound heals by first intention. Everyoperation has its disadvantages and in the caseof Millin's they are, in my experience, asfollows
(a) In fat men the approach to the anteriorsurface of the prostate is through a deep darkhole, haemorrhage can be troublesome beforethe capsule is incised, and unless the operatorpossesses considerable experience and specialequipment, the operation takes time, requiresdeep anaesthesia and causes shock.
(b) Unless dissection is light and careful, orif rough enucleation be substituted for suchcare, quite severe shock develops particularlyin the aged patient. In my experience thisshock is more severe than would be expectedin a similar prostatectomy by the Freyer-Fuller technique.
(c) Reactionary haemorrhage may cause apelvic haematoma, which, if infected goes on topelvic cellulitis.
(d) The fibrous prostate cannot readily beseparated from the capsule without severetrauma.
(e) Unless the vesical opening be enlarged,a diaphragm may develop, cause post-prostatectomy obstruction and require re-section. This occurred in two out of my firstseven cases.
(f) The catheter may slip out and bedifficult to replace..
Lest it be thought that the disadvantagesweigh heavily, retropubic prostatectomy is, inmy opinion, a great advance in prostaticsurgery. It is not so simple as transvesicialenucleation, it is not yet an operation for theoccasional prostatectomist, but in the hands ofMillin it gives excellent results.
Transurethral ProstatectomyTransurethral resection is the oldest opera-
tion devised for the relief of prostatic obstruc-tion by removing tissue, for more than ioo
AprzO,l, I947 1,8Icopyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

POST-(GRADUATE MED:ICAL JOURNAL
years ago' Mercier invented his punch, andmany- similar instruments -have since beenintroduced.- .Hugh- Young, and KennethWalker used their punches.30 years ago, butmodern resection is .an operation of the last15. years' and is associated with the names ofStern -and McCarthy,. of Bumpus, Braasch,Thompson, Emmett -and others*. There islittle doubt that the modern operation islargely American in origin and development.
In the Stern-McCarthy- operation prostatictissue is removed by the diathermy loop whicheffects haemostasis as it cuts. The method isverv useful for small fibrous glands and forcarcinoma but it is difficult to remove muchtissue and, in my limited experience, not easyto be sure where the cuts are being made.However, the Stern-McCarthy method iswidely used in Europe and America and inskilled hands and suitable cases the results aregood..The cold punch resectoscope, a modification
of the direct vision cysto-urethroscope, con-tains a sliding circular knife which cuts awayparts of prostatic tissue engaged in a terminalfenestra. The pieces are washed 'into thebladder by a continuous-stream of lotion andwithdrawn by suction.,.With the Gershom-Thompson resectoscope,
the instrument with which I am most familiar,larger amounts of prostatic tissue can be re-moved at one. sitting. The operation iscarried out under. low spinal anaesthesia, theresectoscope which 'is of large calibre, is passedwith the. greatest care as the urethra is easilydamaged, an accident which invariably pro-duces troublesome strictures, the inside of thebladder, the internal urinary meatus and theprostatic urethra insp?ected and a decisionmade as to whether the case is one suitable forthe '-method.' 'Large adenomatous prostatesweighing over ioo gm. are extremely difficultto resect, but as t'he operator becomes moreexperienced so will he be able' to take moretissue including the-difficult lateral and intra-vesical lobes. 'The removal of bars and fibrougglands is relatively easy 'and a sufficiency oftissue can be simply removed from a car-cinoma.
Resection starts with removal of part of themedian' lobe and' then each lateral lobe istaken separately and haemostasis secured
before passing on to the opposite side. Thecutting may,proceed briskly until the a,pex ofthe gland is reached where care must be takenlest the external sphincter be damaged. To cutbelow the verumontanum is disastrous. Asthe operation -is completed the fibrous capsuleshould be seen all round except in front,. andbleeding points should be controlled with thediathermy electrode. Provided resection isclean and haemostasis careful and, providedalso, the patient's blood pressure has notdropped unduly, the resectoscope is with-drawn with the bladder full. Pressure uponthe pubis should produce a good urinarystream if results are to be satisfactory. AFoley catheter is then inserted and the bag isdistended with 20 ccs. -of lotion and drawndown into the prostatic cavity. Careful adjust-ment of the bag and variations in the amount offluid in it are required to control bleedingcompletely. At the end of the operation thepatient is returned to the ward where bladderwashes are usually continued at, frequentintervals to avoid clotting. This bladderlavage requires considerable skill but in myexperience it is not necessary, and it is a- moresatisfactory procedure to fill the bladder withI per cent; citrate solution and connect thecatheter to an aseptic drainage bottle when thepatient returns to the ward. If the' operationhas been properly carried, out bleeding ismoderate and clotting never occurs.
It is essential during the operation to main-tain the patient's blood pressure at a reasonablelevel or shock may develop and the urinarysecretion diminish. The patient must' drinkfre,ely as his urine is the best form of bladderwash.
Critics of punch prostatectomy point 'outthat complete'removal is impossible and thatrecurrence or carcinoma may follow. Thiscriticism is justifiable' but the experienced'operator can remove the whole prostate at oneor two sittings. Recurrence of obstruction isunlikely except with very inadequate removalof large adenomatous glands. The' fibroustype of gland does not cause recurring obstruc-tion provided a moderate amount of tissuehas been taken away. The main advantagesof this operation in my experience are that verylittle shock is produced, good results canfollow the removal of a small amount of ti:sue
i8z. zlpril, ;'I947copyright.
on February 18, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.258.167 on 1 April 1947. D
ownloaded from

Api,. I947 BENIGN PROSTATIC'OB'STRUCTION4 183
and the operation can be abandoned at anytime. Chest complications are uncommon,post-operative discomfort trivial, and thepatient is kept in bed for not more than 24 or48 hours. It is, therefore, very suitable for theaged alid feeble and these advantages are ap-preciated by the middle aged.'
ConclusionsBefore the merits of the various methods of
treating prostatic obstruction are discussed, itis well to recall to mind-the aims of treatment-the savi'ng of life and the restoration ofnormal bladder function-and to rememberthat probably ;in no other field of surgery is thehuman material less robust.
Prostatic obstruction is a very commondisease affecting old men when they should beexpecting some peace and comfort. Nopractitioner is without experience of the con-dition, and no hospital without its beds andeven wards for' prostatics. Many operatibnshave been devised for .the treatment of thiscondition, some simple, many complex, and solong as general surgeons have to perform themajority of prostatectomies the choice of treat-ment must remain largely individual andsimple methods must hold the field.
In considering the merits of any operationthe number of cases rejected as unfit and con-demned to permanent suprapubic cystotomymust be taken into account, also the morbidityassociated with temporary drainage and thedangers of more than one. operation must beremembered. It is probably true that thesafest and simplest operation is suprapubiccystotomy of the Freyer-Fuller type after aperiod of temporary drainage, and I think thisoperation must remain the most widely useful,but it may be supplanted by Millin's prosta-tectomy which shows great promise. WilsonHey's recent results are excellent but hisoperation has nQt yet been widely adopted, so afinal verdict cannot be given. Transurethralprostatectomy, the most difficult of all is, inmy opinion, the operation of the future for it isapplicable in every case. It can be done in oneor more stages, and it is performed by themasters with a mortality of less than i percent. Although America is still the home ofthis operation, it is gaining ground in England
as recent publications by Wardill and Stewartshow.
All the methods described above give ex-cellent results if carried out properly, and noneis particularly prone to complications. Somerequire longer recumbency than others, someproduce greater shock and are, therefore, notsuitable for all comers. My preference is toperform prostatectomy with the cold punchin all cases except those with 'very large, softadenomatous glands,' and 'for these' I findMillin's operation the most' satisfactory.To conclude I will' qtiote the opinion of the
late Dr. 'Hugh Cabot, one of the greatesturologists'The real nub of! the question'turns upon
the.decision as to who is -to treat by- operationthese people with obstructing prostates. Ifthey are to be treated in the future, as in thepast, largely by the general and, perhaps,occasional surgeon, then';the indicatiodi is foran operative method as .nearly fool proof asmay be. But this does not seem, a very highideal for surgical practice
'It 'is, perhaps, safe to guess that supra-pubic prostatectomy. will long hold.,a placewhere expert urologists are not available.Perineal pros-tatectomy will have to fight'it outwith the transurethral resectionist$.. Both ofthe operations require prolonged training,great skill and dexterity, and large experience.Given these in equal measure, I suspet.thatthe younger generation, armed, with betterequipment, will win the day for transurethraloperations.'
BIBLIOGRAPHYBUMPUS, HERMON C. (1936), Cabot's " Modern Urology."CABOT, HUGH (1936), ".Modern `LJrI6gy.?' Hen)K,iKmpon.EMMETT, JOHN L. (I943), J. Urol., 49, 6.FREYER (IgoI), B.M.J., ii, I25; Ibid (1902), i, 249 and ii, 245;
(1942), Ibid; (I903), i, S98 -FULLER (I895) " Cutam and Genito-jrinar, Disease," p.23.HARRIS, S. H. (1928), " Prostatectomy with Complete Closure,"
Y. Coll. Surgeons, Australasia, x, 65.HARRIS, S. H. (1928), Med. J. Australia, 2, 288.HEY, WILSON (I945), B. J. Surg., 33, 129, 41.KIRWIN, T. J. (Ia93I), 7. Surg. Gynec. and Obstet., 52, 1007.McCARTHY, J. F. (I93s), 7. Urol., 26, 695.McGILL, . (1888), Trans. Clin. Soc., London, xxi, 52.MILLIN, TERENCE (I945), Lancet, Dec., I. 'STERN, MAXIMILIAN (1926), Pays. Therapy, 44,439.STERN, MAXIMILIAN (1926), J.A.M.A., 87, 1726.STEWART, H. H. (945), B.M.Y.WALKER, KENNETH M. (1923), " Diseases of Male Organs of
Generation," Oxford Med. Publications, London.THOMSON-WALKER, J. W. (1930), Tr. Med. Soc., Londmo,
53, 143.WARDILL, W. E. M. (I94I), Lancet, Aug., 2.
YOUNG,AHUGH HAMPDEN (90o3), Y.A.M.A., ii, 999.
copyright. on F
ebruary 18, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.258.167 on 1 A
pril 1947. Dow
nloaded from
Related Documents