http://msj.sagepub.com/ Multiple Sclerosis Journal http://msj.sagepub.com/content/18/2/210 The online version of this article can be found at: DOI: 10.1177/1352458511419702 2012 18: 210 originally published online 24 August 2011 Mult Scler Jorge Correale, Isabel Peirano and Lucas Romano Benign multiple sclerosis: a new definition of this entity is needed Published by: http://www.sagepublications.com can be found at: Multiple Sclerosis Journal Additional services and information for http://msj.sagepub.com/cgi/alerts Email Alerts: http://msj.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Aug 24, 2011 OnlineFirst Version of Record - Feb 6, 2012 Version of Record >> at HINARI on February 7, 2012 msj.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
http://msj.sagepub.com/Multiple Sclerosis Journal
http://msj.sagepub.com/content/18/2/210The online version of this article can be found at:
DOI: 10.1177/1352458511419702
2012 18: 210 originally published online 24 August 2011Mult SclerJorge Correale, Isabel Peirano and Lucas Romano
Benign multiple sclerosis: a new definition of this entity is needed
Published by:
http://www.sagepublications.com
can be found at:Multiple Sclerosis JournalAdditional services and information for
http://msj.sagepub.com/cgi/alertsEmail Alerts:
http://msj.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Aug 24, 2011 OnlineFirst Version of Record
- Feb 6, 2012Version of Record >>
at HINARI on February 7, 2012msj.sagepub.comDownloaded from
Multiple Sclerosis Journal18(2) 210 –218© The Author(s) 2012 Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1352458511419702msj.sagepub.com
MULTIPLESCLEROSIS MSJJOURNAL
Introduction
Multiple sclerosis (MS) is a disease characterized by a wide range of progression. There is a subgroup of patients who show little or no disease progression and minimal disability many years after initial symptoms are diagnosed; this form is referred to as benign MS (BMS). Prevalence estimates of BMS vary widely in the literature, with authors quoting fig-ures ranging between as low as 5% and as high as 64% of all MS cases.1-8 This is probably due to the use of different defi-nitions, of different study designs (e.g. population-based cohorts vs. hospital-based cohorts), and on whether or not mortality estimates are included in estimation calculations.9
Although there is lack of consensus and much hetero-geneity, the most widely used definition of BMS is an Expanded Disability Status Scale (EDSS) < 3 after a mini-mum of 10 years’ disease duration.2,3,7,9,10 Nevertheless, when applying this score to monitor disease progression, one should bear in mind that it shows relatively low relia-bility and poor responsiveness to disease-related changes, because it is heavily weighted towards motor disability, in
particular ambulation, and not influenced by the presence or severity of other debilitating symptoms such as depres-sion, fatigue, pain or cognitive impairment, which also affect quality of life. Incorporating imaging results would contribute to better characterize BMS, as lower lesion accrual rates and less severe tissue damage would be expected in this disease subtype.
This study aims at a more comprehensive understanding of BMS, beyond physical disability, by providing a more thorough assessment of cognitive function, fatigue, pain,
Benign multiple sclerosis: a new definition of this entity is needed
Jorge Correale1, Isabel Peirano1 and Lucas Romano2
AbstractBackground: To study a cohort of benign multiple sclerosis (BMS) patients beyond physical disability, including the evaluation of cognitive and social function, as well as fatigue, pain and MRI studies.Methods: A cohort of 342 patients was prospectively followed for 10.9 ± 0.71 years. Forty-three patients (12.5%) met the BMS diagnosis criteria [Expanded Disability Status Scale (EDSS) < 3 after at least 10 years’ disease duration], undergo-ing full neurological examination every 6 months. Neuropsychological status, pain, fatigue, social functioning and work-related disability, as well as brain MRIs, were assessed yearly.Results: By the end of follow-up, 20 of 43 BMS patients (47%) had suffered cognitive impairment and 23 (53.3%) referred depression. Furthermore, 21 (48.8%) reported significant changes in pain intensity, with fatigue and environ-mental severity scores significantly increasing over time in 33–35% of patients. Finally, 32 BMS patients (74%) showed significant increase in the number of new or enlarging T2 lesions, gadolinium-enhanced lesions, and persistent black holes, without changes in EDSS. Thirty-five of 43 patients (81%) fulfilling the BMS diagnostic criteria showed significant worsening of cognitive function, fatigue, pain or depression during the 10-year follow-up.Conclusions: Currently accepted criteria for BMS diagnosis may cause overestimation of true prevalence, underscor-ing the need for routine monitoring of non-motor symptoms and imaging studies, to help physicians improve diagnostic accuracy as well as therapeutic decision-making in this subgroup of MS patients.
KeywordsMRI, multiple sclerosis, neuropsychological assessment, prognosis, quality of life.
Date received: 1st June 2011; revised: 11th July 2011; accepted: 18th July 2011
1 Department of Neurology, Institute for Neurological Research Raúl Carrea, FLENI, Buenos Aires, Argentina.
2 Neurology Department, Hospital Privado de Comunidad, Mar del Plata, Argentina.
Corresponding author:Jorge Correale, Raúl Carrea Institute for Neurological Research, FLENI, Montañeses 2325, (1428) Buenos Aires, Argentina. Email: [email protected]
419702 MSJ18210.1177/1352458511419702Correale et al.Multiple Sclerosis Journal
Research Paper
at HINARI on February 7, 2012msj.sagepub.comDownloaded from

Correale et al. 211
imaging studies and social functioning in a clinical cohort of patients fulfilling the current criteria accepted for BMS definition.
Methods
Subjects and study design
A prospective study was conducted based on the analysis of longitudinal clinical and radiological data acquired from a cohort of MS outpatients between 1 April 1997 and 30 April 2009, consecutively selected while undergoing fol-low-up at the Institute for Neurological Research Raúl Carrea [Fundación para la Lucha contra las Enfermedades Neurológicas de la Infancia (FLENI)]. Inclusion was based on the diagnosis of clinically definite relapsing–remitting MS (RRMS) according to the Poser criteria. The study included all MS patients with onset of disease since 1 April 1997. This onset period potentially allowed all patients to reach 10 or more years of disease duration. All of the patients were relapse-free and had not taken steroids for at least 3 months before the assessment. All scheduled outpa-tient follow-up evaluations were conducted by the same neurologist (JC) and included complete neurological exam-ination and EDSS rating every 6 months.
Neuropsychological testing, pain and fatigue severity, and degree of work-related disability and social functioning were assessed once a year as described below. MS was defined as benign in patients presenting an EDSS score < 3, 10 years after the clinical onset of the disease as a mini-mum. The Lublin and Reingold criteria11 were applied to establish whether the clinical course was RRMS or second-ary progressive MS (SPMS). A particular EDSS score was considered irreversible if it remained unchanged after 12 months of observation. Thirty-five age- and gender-matched healthy volunteers were also studied, 24 women and 11 men, mean age: 37.5 ± 6.2 years (range 26–52 years). None referred previous neurological or systemic diseases potentially affecting central nervous system (CNS) func-tion, and the neurological exam was normal in all cases. Of these individuals, 30 also agreed to come for the same follow-up evaluations (86%; 21 women, 9 men; mean age: 37.3 ± 6.1) as established for BMS patients.
The study was approved by the local ethics committee and all subjects were required to sign written informed-consent forms prior to study entry.
Neuropsychological evaluation
All patients included in the study underwent neuropsycho-logical evaluation exploring the following cognitive domains: (a) attention, concentration and speed of informa-tion processing [Paced Auditorial Serial Attention Test 3 seconds (PASAT-3)];12 (b) immediate and recent memory [Digit Span (DS) and 7/24 Spatial Recall Test (SRT)];13,14 (c) executive function [Wisconsin Card Sorting Test
(WCST)];15 and (d) visual-spatial skills [Visual Form Discrimination Test (VFDT)].16 Test failure was defined as a score at least 2 SDs below mean normative values. Patients failing at least three tests were considered cogni-tively impaired. Finally, depression was examined using the Beck Depression Inventory (BDI).17 Participants requir-ing psychoactive drugs or other substances potentially affecting neuropsychological performance were excluded.
Pain evaluation
To assess pain, participants were asked: ‘Are you currently experiencing, or have you in the past 3 months experienced any pain?’. Patients responding affirmatively were then evaluated using the Brief Pain Inventory-Long Form (BPI-LF).18 Pain syndromes evaluated included: neuro-pathic pain (trigeminal neuralgia, Lhermitte’s sign, dyses-thetic pain), somatic pain (back pain and painful tonic spasms) and visceral pain. Headache, acute pain due to optical neuritis or somatic pain (with the exception of back pain and tonic spasms) are not included.
Other evaluations
Fatigue severity was measured using the Fatigue Severity Scale (FSS).19 For handicap in work and social activities the Environmental Status Scale (ESS) was employed.20 All evaluations were carried out during relapse-free periods, in patients off steroids for at least 6 months.
MRI
Brain MRIs were performed using the same protocol in all patients, at least once a year on a 1.5-T Signa Unit (GE Healthcare, Milwaukee, WI, USA). Five-millimeter axial slices were obtained with T2-weighted, proton density, fast spin echo, fluid attenuation inversion recovery, and T1-weighted sequences, before and after administration of gadolinium (Gd)-diethylene triamine pentaacetic acid (DTPA) (0.1 mmol/kg). Post-contrast images were com-pleted within 15 min after Gd injection. Changes in number of new or enlarging T2 lesions, new Gd-enhanced lesions or persistent black holes were diagnosed in each patient by a single observer, blind to patient clinical status.
Statistical analysis
Group comparisons were assessed using the non-paramet-ric Mann–Whitney test. To correlate patient demographics and clinical characteristics, the Spearman’s coefficient r was used. Potential BMS prognostic factors were analyzed first by logistic regression, followed by univariate analysis to identify possible variables associated with a benign course, and then by multivariate analysis to identify the independent effects of the prognostic factors studied. In all cases p values < 0.05 were taken as significant.
at HINARI on February 7, 2012msj.sagepub.comDownloaded from
212 Multiple Sclerosis Journal 18(2)
Results
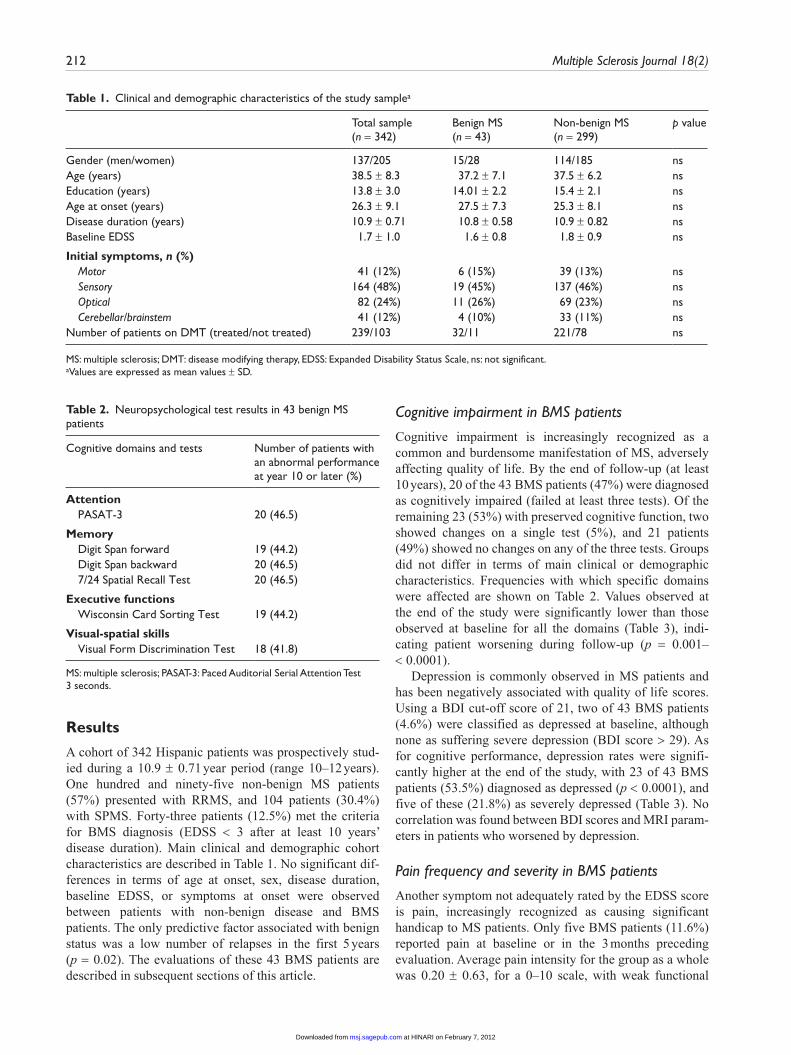
A cohort of 342 Hispanic patients was prospectively stud-ied during a 10.9 ± 0.71 year period (range 10–12 years). One hundred and ninety-five non-benign MS patients (57%) presented with RRMS, and 104 patients (30.4%) with SPMS. Forty-three patients (12.5%) met the criteria for BMS diagnosis (EDSS < 3 after at least 10 years’ disease duration). Main clinical and demographic cohort characteristics are described in Table 1. No significant dif-ferences in terms of age at onset, sex, disease duration, baseline EDSS, or symptoms at onset were observed between patients with non-benign disease and BMS patients. The only predictive factor associated with benign status was a low number of relapses in the first 5 years (p = 0.02). The evaluations of these 43 BMS patients are described in subsequent sections of this article.
Cognitive impairment in BMS patients
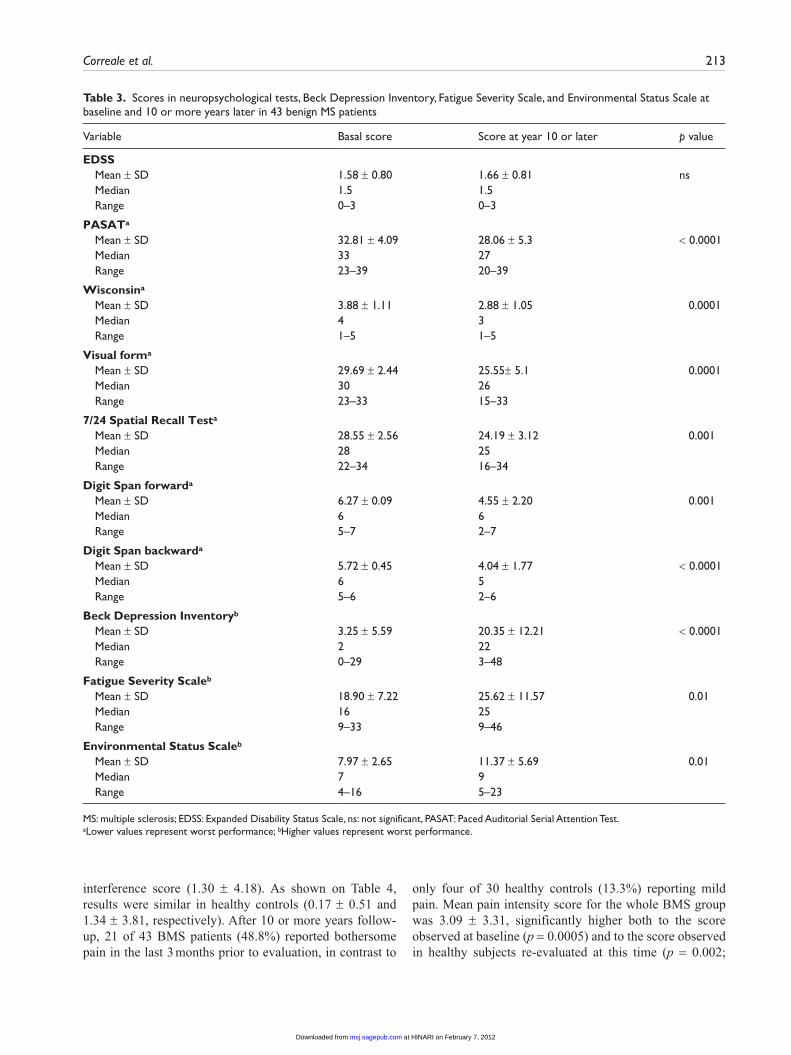
Cognitive impairment is increasingly recognized as a common and burdensome manifestation of MS, adversely affecting quality of life. By the end of follow-up (at least 10 years), 20 of the 43 BMS patients (47%) were diagnosed as cognitively impaired (failed at least three tests). Of the remaining 23 (53%) with preserved cognitive function, two showed changes on a single test (5%), and 21 patients (49%) showed no changes on any of the three tests. Groups did not differ in terms of main clinical or demographic characteristics. Frequencies with which specific domains were affected are shown on Table 2. Values observed at the end of the study were significantly lower than those observed at baseline for all the domains (Table 3), indi-cating patient worsening during follow-up (p = 0.001– < 0.0001).
Depression is commonly observed in MS patients and has been negatively associated with quality of life scores. Using a BDI cut-off score of 21, two of 43 BMS patients (4.6%) were classified as depressed at baseline, although none as suffering severe depression (BDI score > 29). As for cognitive performance, depression rates were signifi-cantly higher at the end of the study, with 23 of 43 BMS patients (53.5%) diagnosed as depressed (p < 0.0001), and five of these (21.8%) as severely depressed (Table 3). No correlation was found between BDI scores and MRI param-eters in patients who worsened by depression.
Pain frequency and severity in BMS patients
Another symptom not adequately rated by the EDSS score is pain, increasingly recognized as causing significant handicap to MS patients. Only five BMS patients (11.6%) reported pain at baseline or in the 3 months preceding evaluation. Average pain intensity for the group as a whole was 0.20 ± 0.63, for a 0–10 scale, with weak functional
Table 1. Clinical and demographic characteristics of the study samplea
Total sample (n = 342)
Benign MS (n = 43)
Non-benign MS (n = 299)
p value
Gender (men/women) 137/205 15/28 114/185 nsAge (years) 38.5 ± 8.3 37.2 ± 7.1 37.5 ± 6.2 nsEducation (years) 13.8 ± 3.0 14.01 ± 2.2 15.4 ± 2.1 nsAge at onset (years) 26.3 ± 9.1 27.5 ± 7.3 25.3 ± 8.1 nsDisease duration (years) 10.9 ± 0.71 10.8 ± 0.58 10.9 ± 0.82 nsBaseline EDSS 1.7 ± 1.0 1.6 ± 0.8 1.8 ± 0.9 ns
Initial symptoms, n (%) Motor 41 (12%) 6 (15%) 39 (13%) ns Sensory 164 (48%) 19 (45%) 137 (46%) ns Optical 82 (24%) 11 (26%) 69 (23%) ns Cerebellar/brainstem 41 (12%) 4 (10%) 33 (11%) nsNumber of patients on DMT (treated/not treated) 239/103 32/11 221/78 ns
MS: multiple sclerosis; DMT: disease modifying therapy, EDSS: Expanded Disability Status Scale, ns: not significant.aValues are expressed as mean values ± SD.
Table 2. Neuropsychological test results in 43 benign MS patients
Cognitive domains and tests Number of patients with an abnormal performance at year 10 or later (%)
Attention PASAT-3 20 (46.5)
Memory Digit Span forward 19 (44.2) Digit Span backward 20 (46.5) 7/24 Spatial Recall Test 20 (46.5)
Executive functions Wisconsin Card Sorting Test 19 (44.2)
Visual-spatial skills Visual Form Discrimination Test 18 (41.8)
MS: multiple sclerosis; PASAT-3: Paced Auditorial Serial Attention Test 3 seconds.
at HINARI on February 7, 2012msj.sagepub.comDownloaded from
Correale et al. 213
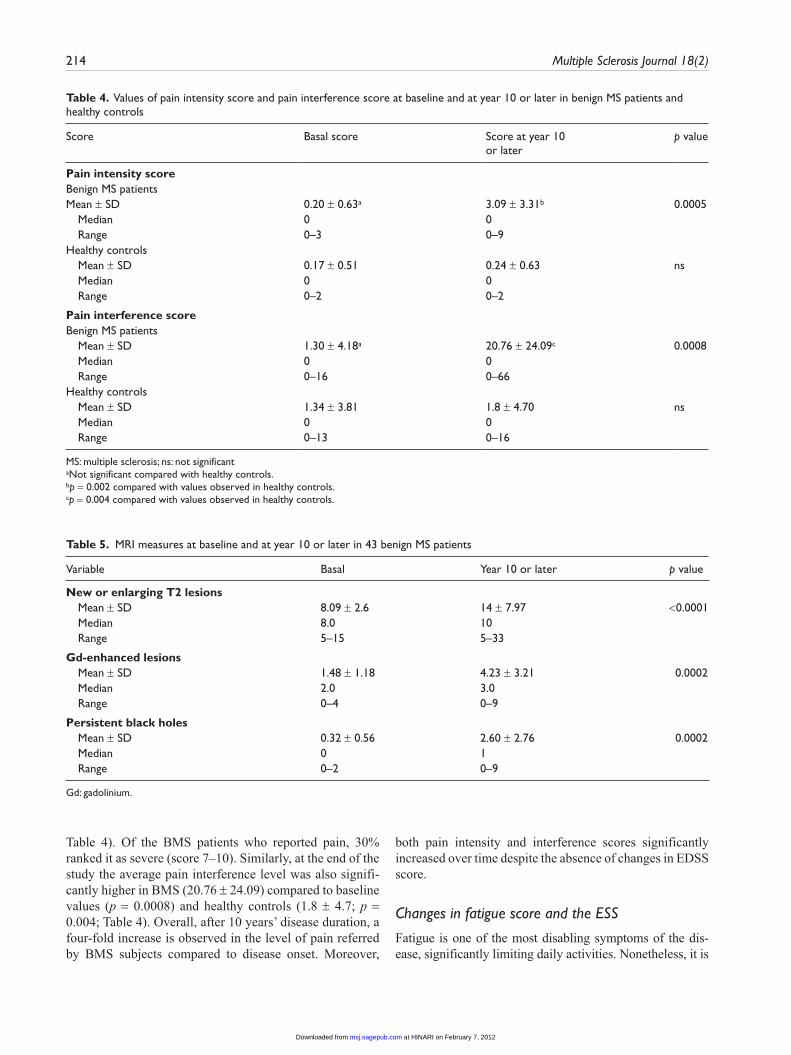
interference score (1.30 ± 4.18). As shown on Table 4, results were similar in healthy controls (0.17 ± 0.51 and 1.34 ± 3.81, respectively). After 10 or more years follow-up, 21 of 43 BMS patients (48.8%) reported bothersome pain in the last 3 months prior to evaluation, in contrast to
only four of 30 healthy controls (13.3%) reporting mild pain. Mean pain intensity score for the whole BMS group was 3.09 ± 3.31, significantly higher both to the score observed at baseline (p = 0.0005) and to the score observed in healthy subjects re-evaluated at this time (p = 0.002;
Table 3. Scores in neuropsychological tests, Beck Depression Inventory, Fatigue Severity Scale, and Environmental Status Scale at baseline and 10 or more years later in 43 benign MS patients
Variable Basal score Score at year 10 or later p value
EDSS Mean ± SD 1.58 ± 0.80 1.66 ± 0.81 ns Median 1.5 1.5 Range 0–3 0–3
PASATa
Mean ± SD 32.81 ± 4.09 28.06 ± 5.3 < 0.0001 Median 33 27 Range 23–39 20–39
Wisconsina
Mean ± SD 3.88 ± 1.11 2.88 ± 1.05 0.0001 Median 4 3 Range 1–5 1–5
Visual forma
Mean ± SD 29.69 ± 2.44 25.55± 5.1 0.0001 Median 30 26 Range 23–33 15–33
7/24 Spatial Recall Testa
Mean ± SD 28.55 ± 2.56 24.19 ± 3.12 0.001 Median 28 25 Range 22–34 16–34
Digit Span forwarda
Mean ± SD 6.27 ± 0.09 4.55 ± 2.20 0.001 Median 6 6 Range 5–7 2–7
Digit Span backwarda
Mean ± SD 5.72 ± 0.45 4.04 ± 1.77 < 0.0001 Median 6 5 Range 5–6 2–6
Beck Depression Inventoryb
Mean ± SD 3.25 ± 5.59 20.35 ± 12.21 < 0.0001 Median 2 22 Range 0–29 3–48
Fatigue Severity Scaleb
Mean ± SD 18.90 ± 7.22 25.62 ± 11.57 0.01 Median 16 25 Range 9–33 9–46
Environmental Status Scaleb
Mean ± SD 7.97 ± 2.65 11.37 ± 5.69 0.01 Median 7 9 Range 4–16 5–23
MS: multiple sclerosis; EDSS: Expanded Disability Status Scale, ns: not significant, PASAT: Paced Auditorial Serial Attention Test.aLower values represent worst performance; bHigher values represent worst performance.
at HINARI on February 7, 2012msj.sagepub.comDownloaded from
214 Multiple Sclerosis Journal 18(2)
Table 4). Of the BMS patients who reported pain, 30% ranked it as severe (score 7–10). Similarly, at the end of the study the average pain interference level was also signifi-cantly higher in BMS (20.76 ± 24.09) compared to baseline values (p = 0.0008) and healthy controls (1.8 ± 4.7; p = 0.004; Table 4). Overall, after 10 years’ disease duration, a four-fold increase is observed in the level of pain referred by BMS subjects compared to disease onset. Moreover,
both pain intensity and interference scores significantly increased over time despite the absence of changes in EDSS score.
Changes in fatigue score and the ESS
Fatigue is one of the most disabling symptoms of the dis-ease, significantly limiting daily activities. Nonetheless, it is
Table 4. Values of pain intensity score and pain interference score at baseline and at year 10 or later in benign MS patients and healthy controls
Score Basal score Score at year 10 or later
p value
Pain intensity scoreBenign MS patientsMean ± SD 0.20 ± 0.63a 3.09 ± 3.31b 0.0005 Median 0 0 Range 0–3 0–9 Healthy controls Mean ± SD 0.17 ± 0.51 0.24 ± 0.63 ns Median 0 0 Range 0–2 0–2
Pain interference scoreBenign MS patients Mean ± SD 1.30 ± 4.18a 20.76 ± 24.09c 0.0008 Median 0 0 Range 0–16 0–66 Healthy controls Mean ± SD 1.34 ± 3.81 1.8 ± 4.70 ns Median 0 0 Range 0–13 0–16
MS: multiple sclerosis; ns: not significantaNot significant compared with healthy controls.bp = 0.002 compared with values observed in healthy controls.cp = 0.004 compared with values observed in healthy controls.
Table 5. MRI measures at baseline and at year 10 or later in 43 benign MS patients
Variable Basal Year 10 or later p value
New or enlarging T2 lesions Mean ± SD 8.09 ± 2.6 14 ± 7.97 <0.0001 Median 8.0 10 Range 5–15 5–33
Gd-enhanced lesions Mean ± SD 1.48 ± 1.18 4.23 ± 3.21 0.0002 Median 2.0 3.0 Range 0–4 0–9
Persistent black holes Mean ± SD 0.32 ± 0.56 2.60 ± 2.76 0.0002 Median 0 1 Range 0–2 0–9
Gd: gadolinium.
at HINARI on February 7, 2012msj.sagepub.comDownloaded from
Correale et al. 215
only minimally evaluated in the EDSS score. At baseline, the mean FSS score for the 43 BMS patients was 18.90 ± 7.22. None presented severe fatigue (score > 36). In contrast, after 10 years or more, mean FSS scores increased consi-derably (25.62 ± 11.57; p = 0.01; Table 3). FSS score pro gression was observed over time in 14 BMS patients (33%); of these 13 (93%) had severe fatigue. The frequency and intensity of fatigue was not significantly different between patients treated with disease-modifying therapies or untreated patients. Moreover, fatigue severity was independ-ent of BDI. As for fatigue evaluation, at disease onset BMS patients had lower ESS scores (7.97 ± 2.65), compared to 10 or more years later (11.37 ± 5.69; p = 0.01; Table 3). Fifteen BMS patients (35%) had progressively worse ESS scores, particularly for items exploring social activities and work status. Additional analysis showed ESS scores were higher in cognitively impaired BMS patients (p = 0.01). ESS scores were also higher for BMS patients with depression (BDI > 21) than those without depression (p = 0.03).
MRI in BMS patients
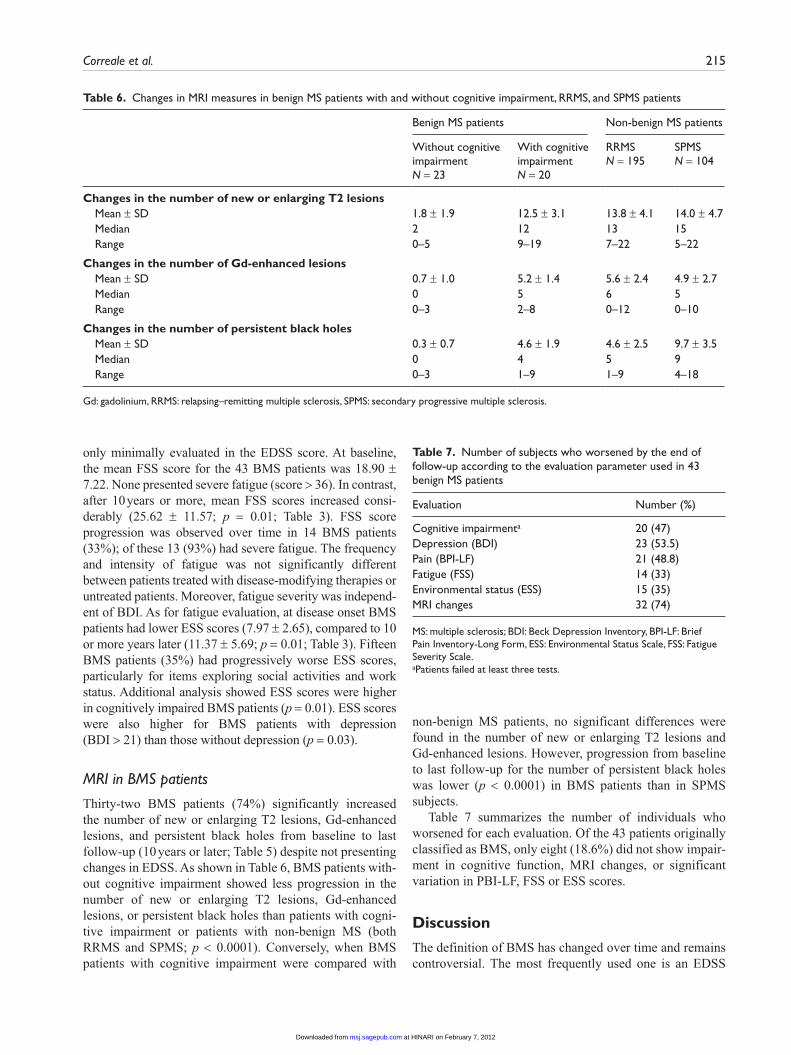
Thirty-two BMS patients (74%) significantly increased the number of new or enlarging T2 lesions, Gd-enhanced lesions, and persistent black holes from baseline to last follow-up (10 years or later; Table 5) despite not presenting changes in EDSS. As shown in Table 6, BMS patients with-out cognitive impairment showed less progression in the number of new or enlarging T2 lesions, Gd-enhanced lesions, or persistent black holes than patients with cogni-tive impairment or patients with non-benign MS (both RRMS and SPMS; p < 0.0001). Conversely, when BMS patients with cognitive impairment were compared with
non-benign MS patients, no significant differences were found in the number of new or enlarging T2 lesions and Gd-enhanced lesions. However, progression from baseline to last follow-up for the number of persistent black holes was lower (p < 0.0001) in BMS patients than in SPMS subjects.
Table 7 summarizes the number of individuals who worsened for each evaluation. Of the 43 patients originally classified as BMS, only eight (18.6%) did not show impair-ment in cognitive function, MRI changes, or significant variation in PBI-LF, FSS or ESS scores.
Discussion
The definition of BMS has changed over time and remains controversial. The most frequently used one is an EDSS
Table 6. Changes in MRI measures in benign MS patients with and without cognitive impairment, RRMS, and SPMS patients
Benign MS patients Non-benign MS patients
Without cognitive impairment N = 23
With cognitive impairment N = 20
RRMS N = 195
SPMS N = 104
Changes in the number of new or enlarging T2 lesions Mean ± SD 1.8 ± 1.9 12.5 ± 3.1 13.8 ± 4.1 14.0 ± 4.7 Median 2 12 13 15 Range 0–5 9–19 7–22 5–22
Changes in the number of Gd-enhanced lesions Mean ± SD 0.7 ± 1.0 5.2 ± 1.4 5.6 ± 2.4 4.9 ± 2.7 Median 0 5 6 5 Range 0–3 2–8 0–12 0–10
Changes in the number of persistent black holes Mean ± SD 0.3 ± 0.7 4.6 ± 1.9 4.6 ± 2.5 9.7 ± 3.5 Median 0 4 5 9 Range 0–3 1–9 1–9 4–18
Gd: gadolinium, RRMS: relapsing–remitting multiple sclerosis, SPMS: secondary progressive multiple sclerosis.
Table 7. Number of subjects who worsened by the end of follow-up according to the evaluation parameter used in 43 benign MS patients
Evaluation Number (%)
Cognitive impairmenta 20 (47)Depression (BDI) 23 (53.5)Pain (BPI-LF) 21 (48.8)Fatigue (FSS) 14 (33)Environmental status (ESS) 15 (35)MRI changes 32 (74)
MS: multiple sclerosis; BDI: Beck Depression Inventory, BPI-LF: Brief Pain Inventory-Long Form, ESS: Environmental Status Scale, FSS: Fatigue Severity Scale.aPatients failed at least three tests.
at HINARI on February 7, 2012msj.sagepub.comDownloaded from

216 Multiple Sclerosis Journal 18(2)
score < 3 after at least 10 years from disease onset.2,3,7,9,10 However, different cut-offs for disease duration and disa-bility EDSS levels have been used.5,6,21–23 These definitions are all based on retrospective evaluations, and for the time being no strong clinical, demographic, genetic, laboratory or radiological prognostic markers predicting a benign course exist.23 Indeed, longitudinal studies have frequently shown that patients with BMS can develop a secondary progressive course, or suffer more severity and accumulate disability over time,3,6,23–25 thus leading physicians to treat early rather than for the clinical outcome to manifest.
This report provides prospectively acquired, longitudi-nal clinical, environmental, and MRI data from BMS patients. In this cohort, BMS incidence was 12.5% after 10.9 ± 0.71 years follow-up. However, 35 of 43 patients (81%) meeting the BMS definition criteria significantly showed worsened cognitive functions, fatigue, pain, or depression over the years, ultimately mirrored by signifi-cant changes in the ESS, with a negative impact on items exploring social activities and work status in particular. Moreover, of 43 patients defined as BMS, 32 (74%) showed MRI disease progression over time (new or enlarging T2 lesions, Gd-enhanced lesions, and persistent black holes) similar to those findings in RRMS or SPMS patients.
Our results are in line with previous studies suggesting that cognitive impairment, fatigue and depression may be relevant in patients with BMS, despite relative sparing of motor abilities. In a recent study conducted in 163 BMS patients, cognitive dysfunction, significant fatigue and depression were found in over 45% of patients, with nega-tive impact on social and work activities.26 Interestingly, these rates were comparable to those reported in MS patients at large. Moreover, neuropsychological testing results and brain MRI measurements showed that risk of progression in BMS patients was enhanced by male gender, baseline cognitive impairment and baseline T1 lesion bur-den.27 This is an important observation which confirms neuropsychological functioning as another important meas-ure of brain integrity. In contrast to our prospective study, most of these investigations had a cross-sectional design. To assess the temporal evolution of structural and func-tional changes, prospective assessments are more accurate than cross-sectional studies with retrospective assessments.
In line with our observations, several MRI studies have not been able to show major differences in the number of brain T2 lesions in patients with BMS and RRMS or SPMS, despite major differences in disability.28-30 Two factors have been proposed as responsible for these findings. First, lesion location in eloquent CNS regions,31 and second, lower accumulation rate of disease burden in BMS patients, which might increase efficiency of cortical reorganization mechanisms following MS injury.30,32
Considerable effort has been undertaken to identify prognostic factors in MS. The only one we found associ-ated with benign status was a low number of relapses in the
first 5 years. In line with this finding, natural history studies have reported a significant association between the number of relapses in the early years of the disease and the subse-quent development of disability.33,34 However, others have failed to find any association between the number of attacks in early MS and disability outcome,35,36 and the debate over this issue continues. Some authors have indicated that younger age at onset, optic neuritis as first attack, female gender, and longer first remission are significantly associ-ated with a benign course of MS.2,33,34,37 However, we did not find onset symptoms to have a predictive effect on dis-ease severity, as was also the case for other authors.3,38,39 Likewise, age at onset8,38 and sex3,8,38 were not significantly associated with benign status in our study when other fac-tors are controlled for.
There are of course some limitations to this study. First, it was not population-based and patients may not entirely reflect the overall group of BMS subjects. Nevertheless, although our population was clinic-based and a potential selection bias towards more severe cases cannot be ruled out, this does not alter the core finding, namely that patients included in the study met the current BMS criteria. Furthermore, because of the longitudinal design of the study, structural and functional changes in the cohort were clearly demonstrated over time. Second, because this study was started in 1997, not all patients were evaluated with the more contemporary cognitive test batteries such as the Minimal Assessment of Cognitive Function in Multiple Sclerosis (MACFIMS), however, the tests included still assessed attention, concentration and speed of information processing, immediate and recent memory, executive func-tion and visual-spatial skills, which are the most commonly affected cognitive domains in MS patients. Finally, recent years have seen the introduction of several new MRI tech-niques, improving the limited correlation between T2-weighted images and patient clinical disability.40 Given that this study was initiated over 10 years ago, the most recent MRI techniques have not been included. However, no changes in scanner hardware or software were intro-duced during the follow-up period. Results of recent MRI studies indicate that while there appear to be no differences between BMS and RRMS patients in terms of T2-lesion load, there are in fact differences in other MRI parameters such as magnetization transfer,41 magnetic resonance spec-troscopy,42 diffusion tensor MRI,32,43,44 functional MRI,32,45 and general brain atrophy.43,46 These studies used cross-sectional design or only had very short follow-up periods, and consequently their results do not allow assessment of changes over time. Therefore, caution is needed before drawing firm conclusions on MS dynamics, and longitudi-nal studies are warranted to confirm these findings.
Overall, the results of this study indicate that although our patients met currently accepted criteria for BMS, clini-cal symptoms as well as radiological images progressed over time, causing major impact on everyday life activities.
at HINARI on February 7, 2012msj.sagepub.comDownloaded from
Correale et al. 217
Nevertheless, it is also true that a certain number of MS patients remain free of long-term physical or cognitive dis-ability. Indeed, subclinical cases of MS have been described in sibling studies47 and post-mortem examinations.48 These observations suggest that a less aggressive form of MS may exist, but harder to identify and more complex than previ-ously thought.
It is likely that the currently accepted criteria for BMS may cause overestimation of its true incidence, underscor-ing the need for routine monitoring of non-motor symp-toms and of CNS imaging. A need to reassess the current clinical definition of BMS clearly exists. This information would in turn optimize patient management and provide clues to improve therapeutic decision-making in this sub-group of patients.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Dr. Correale is a board member of Merck-Serono Argentina, Biogen-Idec LATAM, and Merck-Serono LATAM. Dr. Correale has received reimbursement to develop educational presentations for Merck-Serono Argentina, Merck-Serono LATAM, Biogen-Idec Argentina, and TEVA-Tuteur Argentina as well as profes-sional travel/accommodations stipends. Dr Peirano has no disclosures to report. Dr Romano has no disclosures to report.
References
1. Poser S, Wikström J and Bauer HJ. Clinical data and the identification of special forms of multiple sclerosis in 1271 cases studied with a standardized documentation system. J Neurol Sci 1979; 40: 159–168.
2. Thompson AJ, Hutchinson M, Brazil J, Feighery C and Martin EA. A clinical and laboratory study of benign mul-tiple sclerosis. Q J Med 1986; 58: 69–80.
3. Hawkins SA and McDonell GV. Benign multiple sclero-sis? Clinical course, long term follow up and assessment of prognostic factors. J Neurol Neurosurg Psychiatry 1999; 67: 148–152.
4. Benedikz J, Stefánsson M, Guomundsson J, Jónasdóttir A, Fossdal R, Gulcher J, et al. The natural history of untreated multiple sclerosis in Iceland. A total population-based 50 year prospective study. Clin Neurol Neurosurg 2002; 104: 208–210.
5. Pittock SJ, McClelland RL, Mayr WT, Jorgensen NW, Weinshenker BG, Noseworthy J, et al. Clinical implications of benign multiple sclerosis: a 20-year population-based follow-up study. Ann Neurol 2004; 56: 303–306.
6. Sayao AL, Devonshire V and Tremlett H. Longitudinal follow-up of “benign” multiple sclerosis at 20 years. Neurol-ogy 2007; 68: 496–500.
7. Costelloe L, Thompson A, Walsh C, Tubridy N and Hutchin-son M. Long-term clinical relevance of criteria for designat-ing multiple sclerosis as benign after 10 years of disease. J Neurol Neurosurg Psychiatry 2008; 79: 1245–1248.
8. Glad SB, Nyland HI, Aarseth JH, Riise T and Myhr KM. Long-term follow-up of benign multiple sclerosis in Hordaland County, Western Norway. Mult Scler 2009; 15: 942–950.
9. Ramsaransing GS and De Keyser J. Benign course in multiple sclerosis: a review. Acta Neurol Scand 2006; 113: 359–369.
10. Glad S, Nyland H and Myhr KM. Benign multiple sclerosis. Acta Neurol Scand 2006; 183: 55–57.
11. Lublin FD and Reingold SC. Defining the clinical course of multiple sclerosis: results of an international survey. National Multiple Sclerosis Society (USA) Advisory Committee on Clinical Trials of New Agents in Multiple Sclerosis. Neurol-ogy 1996; 46: 907–911.
12. Gronwall DM. Paced auditory serial addition task: a measure of recovery from concussion. Percept Mot Skills 1977; 44: 367–373.
13. Wechsler D. Manual for the Wechsler Adult Intelligence Scale Revised. New York: Psychological Corporation, 1981. 1–156.
14. Rao SM, Hammeke TA, McQuillen MP, Khatri BO and Lloyd D. Memory disturbance in chronic progressive mul-tiple sclerosis. Arch Neurol 1984; 41: 625–631.
15. Heaton RK. Wisconsin Card Sorting Test Manual. Odessa, Florida: Psychological Assessment Resources, 1981; 1–230.
16. Benton AL, Hamsker KS, Varney NR and Spreen O. Contri-butions to neuropsychological assessment: a clinical man-ual. Oxford: Oxford University Press (USA), 1983; 1–165.
17. Beck AT, Ward CH, Mendelson M, Mock J and Erbaugh J. An inventory for measuring depression. Arch Gen Psychia-try 1961; 4: 561–571.
18. Cleeland CS and Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore 1994; 23: 129–138.
19. Krupp LB, LaRocca NG, Muir-Nash J and Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol 1989; 46: 1121–1123.
20. Mellerup E, Fog T, Raun N, et al. The socio-economic scale. Acta Neurol Scand 1981; 64 (Suppl 87): 130–138.
21. Lauer K and Firnhaber W. Epidemiological investigations into multiple sclerosis in Southern Hesse. V. Course and prognosis. Acta Neurol Scand 1987; 76: 12–17.
22. Patti F, Russo P, Pappalardo A, Macchia F, Civalleri L and Paolillo A. Predictors of quality of life among patients with multiple sclerosis: an Italian cross-sectional study. J Neurol Sci 2007; 252: 121–129.
23. Glad SB, Aarseth JH, Nyland H, Riise T and Myhr KM. Benign multiple sclerosis: a need for a consensus. Acta Neu-rol Scand Suppl 2010; 122 (190): 44–50.
24. Weinshenker BG, Bass B, Rice GP, Noseworthy J, Carriere W, Baskervielle J, et al. The natural history of multiple scle-rosis: a geographically based study. I. Clinical course and disability. Brain 1989; 112: 133–146.
25. Hirst C, Ingram G, Swingler R, Compston DA, Pickersgill T and Robertson NP. Change in disability in patients with mul-tiple sclerosis: a 20-year prospective population-based anal-ysis. J Neurol Neurosurg Psychiatry 2008; 79: 1137–1143.
26. Amato MP, Zipoli V, Goretti B, Portaccio E, De Caro MF, Ricchiuti L, et al. Benign multiple sclerosis: cognitive, psy-chological and social aspects in a clinical cohort. J Neurol 2006; 253: 1054–1059.
at HINARI on February 7, 2012msj.sagepub.comDownloaded from
218 Multiple Sclerosis Journal 18(2)
27. Portaccio E, Stromillo ML, Goretti B, Zipoli V, Siracusa G, Battaglini M, et al. Neuropsychological and MRI measures predict short-term evolution in benign multiple sclerosis. Neurology 2009; 73: 498–503.
28. Koopmans RA, Li DK, Grochowsky E, Cutler PJ and Paty DW. Benign versus chronic progressive multiple sclerosis: magnetic resonance imaging features. Ann Neurol 1989; 25: 74–81.
29. Filippi M, Barker GJ, Horsfield MA, Sacares PR, Macmanus DG, Thompson AJ, et al. Benign and secondary progressive multiple sclerosis: a preliminary quantitative MRI study. J Neurol 1994; 241: 246–251.
30. Filippi M, Campi A, Mammi S, Martinelli V, Locatelli T, Scotti G, et al. Brain magnetic resonance imaging and mul-timodal evoked potentials in benign and secondary progres-sive multiple sclerosis. J Neurol Neurosurg Psychiatry. 1995; 58: 31–37.
31. Filippi M, Campi A, Colombo B, Pereira C, Martinelli V, Baratti C, et al. A spinal cord MRI study of benign and sec-ondary progressive multiple sclerosis. J Neurol 1996; 243: 502–505.
32. Rocca MA, Ceccarelli A, Rodegher M, Misci P, Riccitelli G, Falini A, et al. Preseved brain adaptive properties in patients with benign multiple sclerosis. Neurology 2010; 74: 142–149.
33. Weinshenker BG, Bass B, Rice GP, Noseworthy J, Carriere W, Baskervielle J, et al. The natural history of multiple scle-rosis: a geographically based study. 2. Predictive value of the early clinical course. Brain 1989; 112: 1419–1428.
34. Confavreux C, Vukusic S and Adelaine P. Early clinical pre-dictors and progression of irreversible disability in multiple sclerosis: an amnesic process. Brain 2003; 126: 770–782.
35. Fog T and Linnemann F. The course of multiple sclerosis in 73 cases with computer-designed curves. Acta Neurol Scand Suppl 1970; 47: 3–175.
36. Patzold U and Pocklington P. Course of multiple sclerosis. First results of a prospective study carried out of 102 MS patients from 1976–1980. Acta Neurol Scand 1982; 65: 248–266.
37. Runmarker B and Andersen O. Prognostic factors in a mul-tiple sclerosis incidence cohort with twenty-five years of follow-up. Brain 1993; 116: 117–134.
38. Kurtzke JF, Beebe GW, Nagler B, Kurland LT and Auth TL. Studies on the natural history of multiple sclerosis – 8. Early prognostic features of the later course of the illness. J Chronic Dis 1977; 30: 819–830.
39. Tremlett H, Paty D and Devonshire V. Disability progres-sion in multiple sclerosis is slower than previously reported. Neurology 2006; 66: 172–177.
40. Rovaris M, Barkhof F, Calabrese M, De Stefano N, Fazekas F, Miller DH, et al. MRI features of benign multiple sclerosis: toward a new definition of this disease phenotype. Neurology 2009; 72: 1693–1701.
41. Amato MP, Portaccio E, Stromillo ML, Goretti B, Zipoli V, Siracusa G, et al. Cognitive assessment and quantitative magnetic resonance metrics can help to identify benign mul-tiple sclerosis. Neurology 2008; 71: 632–638.
42. Rigotti DJ, Gonen O, Grossman RI, Babbs JS, Falini A, Benedetti B, et al. Global N-acetylaspartate declines even in benign multiple sclerosis. AJNR Am J Neuroradiol 2011; 32: 204–209.
43. Rovaris M, Riccitelli G, Judica E, Possa E, Caputo D, Ghezzi A, et al. Cognitive impairment and structural brain damage in benign multiple sclerosis. Neurology 2008; 71: 1521–1526.
44. Benedetti B, Rocca MA, Rovaris M, Caputo D, Zaffaroni M, Capra R, et al. A diffusion tensor MRI study of cervical cord damage in benign and secondary progressive multiple sclerosis patients. J Neurol Neurosurg Psychiatry 2010; 81: 26–30.
45. Giorgio A, Portaccio E, Stromillo ML, Marino S, Zipoli V, Battaglini M, et al. Cortical functional reorganization and its relationship with brain structural damage in patients with benign multiple sclerosis. Mult Scler 2010; 16: 1326–1334.
46. Gautier SA, Berger AM, Liptak Z, Duan Y, Egorova S, Buckle GJ, et al. Rate of brain atrophy in benign vs early multiple sclerosis. Arch Neurol 2009; 66: 234–237.
47. Tienari PJ, Salonen O, Wikström J, Valanne L and Palo J. Familial multiple sclerosis: MRI findings in clinically affected and unaffected siblings. J Neurol Neurosurg Psy-chiatry 1992; 55: 883–886.
48. Mackay RP and Hirano A. Forms of benign multiple scle-rosis. Report of two “clinical silent” cases discovered at autopsy. Arch Neurol 1967; 17: 588–600.
at HINARI on February 7, 2012msj.sagepub.comDownloaded from
Related Documents








![Primary tracheal schwannoma a review of a rare entity ......include benign, intermediate, and malignant tumors [1]. Neurogenic tumors of the tracheobronchial tree are ex-tremely rare](https://static.cupdf.com/doc/110x72/60f7b75799a3976448468c79/primary-tracheal-schwannoma-a-review-of-a-rare-entity-include-benign-intermediate.jpg)