Benign Breast Disease Benign Breast Disease Alireza Mohammadzadeh, MD Alireza Mohammadzadeh, MD Thoracic Surgeon Thoracic Surgeon

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Benign Breast DiseaseBenign Breast Disease
Alireza Mohammadzadeh, MDAlireza Mohammadzadeh, MD
Thoracic SurgeonThoracic Surgeon

Benign breast disorders & diseases Benign breast disorders & diseases encompass a wide range of clinical and encompass a wide range of clinical and
pathologic entitiespathologic entities

Understanding of these for Understanding of these for ::
clear explanation to affected womenclear explanation to affected women
appropriate treatment institutedappropriate treatment instituted
unnecessary follow upunnecessary follow up

FibroadenomaFibroadenoma
Predominantly in younger women aged 15 to Predominantly in younger women aged 15 to 25 years25 years
Usually grow to 1 or 2 cm and then are stableUsually grow to 1 or 2 cm and then are stable
Small f. (Small f. (<1cm<1cm) are considered ) are considered normalnormal
Larger f.(Larger f.(<3cm<3cm) are ) are disordersdisorders
Giant f. (Giant f. (>3cm>3cm) are ) are diseasedisease
Multiple f. (more than 5 in one breast) are Multiple f. (more than 5 in one breast) are diseasedisease

UltrasoundUltrasound
BenignBenign– Pure and intensely Pure and intensely
hyperechoichyperechoic– Elliptical shape (wider Elliptical shape (wider
than tall)than tall)– LobulatedLobulated– Complete tine capsuleComplete tine capsule
MalignantMalignant– Hypoechoic, Hypoechoic,
spiculatedspiculated– Taller than wideTaller than wide– Duct extensionDuct extension– microlobulationmicrolobulation

FibroadenomaFibroadenoma

Core-needle biopsyCore-needle biopsy

Treatment Treatment
Surgical removalSurgical removal
Cryoablation Cryoablation
observationobservation

Sclerosing adenosisSclerosing adenosis
Prevalent during childbearing & Prevalent during childbearing & perimenopausal yearsperimenopausal years
No malignant potentialNo malignant potential
Occasionally presents as a palpable massOccasionally presents as a palpable mass
Benign calcificationBenign calcification
Lesions up to 1 cm are called Lesions up to 1 cm are called radial scarradial scar
Larger lesions are called Larger lesions are called complex complex sclerosing sclerosing

Sclerosing adenosisSclerosing adenosis
Mimic of cancerMimic of cancer
On physical examination, by On physical examination, by mammography, at gross pathologymammography, at gross pathology
Wire localized excisionl biopsyWire localized excisionl biopsy

Benign Breast DiseasesBenign Breast Diseases
Glandular breast parenchymaGlandular breast parenchyma– MassMass– Asymmetric nodularityAsymmetric nodularity– PainPain
Nipple-Areolar ComplexNipple-Areolar Complex– DischargeDischarge– RashRash– RetractionRetraction
Surrounding breast skinSurrounding breast skin– DimplingDimpling

ManagementManagement
HistoryHistory
Clinical Breast ExamClinical Breast Exam
Breast imagingBreast imaging
Tissue samplingTissue sampling
TherapyTherapy

HistoryHistory
AgeAge– MenarcheMenarche– PregnancyPregnancy
Breast feedingBreast feeding
– MenopauseMenopause
Family HistoryFamily History
Prior biopsiesPrior biopsies
Hormone therapyHormone therapy

Clinical ExamClinical Exam
InspectionInspection– SkinSkin– SymmetrySymmetry– MassesMasses
PalpablePalpable– GlandGland– Axilla, Supraclavicular Axilla, Supraclavicular
spacesspaces– Nipple-areola complexNipple-areola complex

Breast MassBreast Mass
Breast CystsBreast Cysts– Fluid-filled Fluid-filled – 1 out of every 14 women1 out of every 14 women
50% multiple and recurrent50% multiple and recurrent
– Hormonally influencedHormonally influenced– Needle aspiratedNeedle aspirated
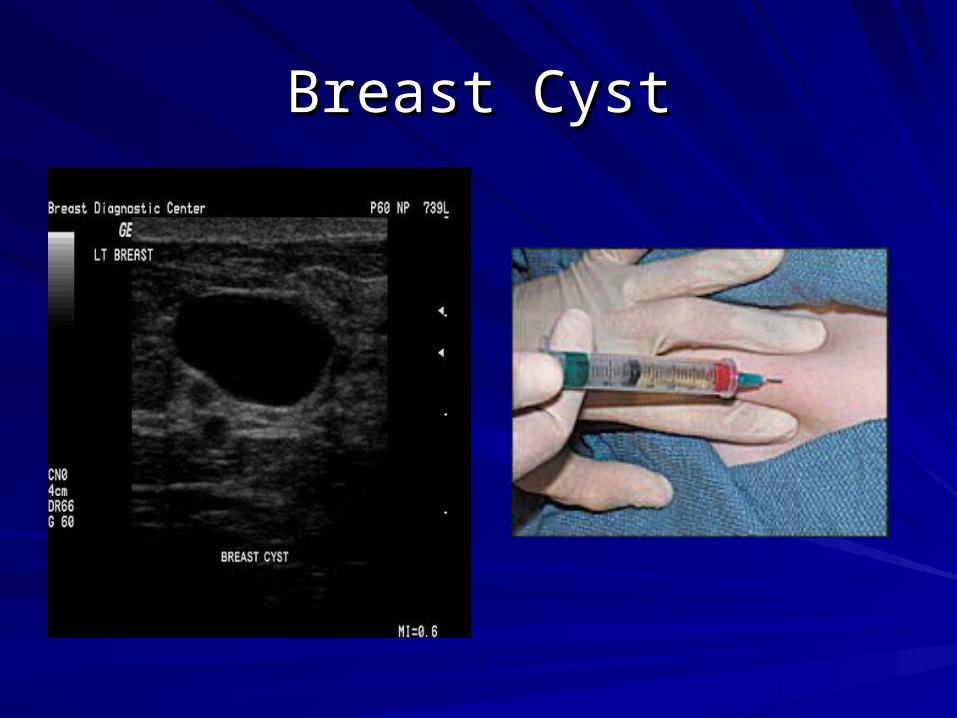
Breast CystBreast Cyst

Breast MassBreast Mass
Phyllodes TumorPhyllodes Tumor– Proliferation of connective tissue with ductal Proliferation of connective tissue with ductal
elementselementsWhorled and cellular stromaWhorled and cellular stroma
– Firm, lobulatedFirm, lobulated– 2 to 40 cm in size2 to 40 cm in size– 10% malignant10% malignant– TreatmentTreatment
Wide excisionWide excision


Fibrocystic DiseaseFibrocystic Disease
Clinical, mammographic and histologic Clinical, mammographic and histologic findingsfindings
Exaggerated response from hormones Exaggerated response from hormones and growth factorsand growth factors– Cyclical painCyclical pain– Nodularity – upper outer quadrantsNodularity – upper outer quadrants

Fibrocystic DiseaseFibrocystic Disease
HistologyHistology– AdenosisAdenosis– Apocrine metaplasiaApocrine metaplasia– FibrosisFibrosis– Duct ectasiaDuct ectasia– Mild ductal hyperplasiaMild ductal hyperplasia

Fibrocystic DiseaseFibrocystic Disease
Risk FactorsRisk Factors– Dense breastDense breast– Sclerosing adenosisSclerosing adenosis– Atypical ductal, papillary, or lobular Atypical ductal, papillary, or lobular
hyperplasiahyperplasia

Breast PainBreast Pain
Cyclical pain – hormonalCyclical pain – hormonal– Dull, diffuse and bilateralDull, diffuse and bilateral– Luteal phaseLuteal phase– TreatmentTreatment
ReassuranceReassuranceNSAIDSNSAIDSEvening primrose oilEvening primrose oil
Non-cyclical painNon-cyclical pain– Non-breast vs breastNon-breast vs breast– ImagingImaging– TreatmentTreatment
ReassuranceReassuranceNSAIDSNSAIDSEvening primrose oilEvening primrose oil

Breast InfectionsBreast Infections
MastitisMastitis– Generalized cellulitis of the breastGeneralized cellulitis of the breast– Ascending infection Ascending infection subareolar ductssubareolar ducts
commonly occurs during lactationcommonly occurs during lactation– Staph. aureusStaph. aureus
– Erythema, pain, tendernessErythema, pain, tenderness

MastitisMastitis
TreatmentTreatment– AbxAbx– Continue to breast Continue to breast
feedfeed– Close follow-upClose follow-up
Breast AbscessBreast Abscess
AbscessAbscess– Breast tissueBreast tissue– TreatmentTreatment
AbxAbx
Needle aspirationNeedle aspiration
Incision and drainageIncision and drainage

Nipple DischargeNipple Discharge
PhysiologicPhysiologic– BilateralBilateral– Involves multiple ducts Involves multiple ducts – Heme (-)Heme (-)– Non-spontaneousNon-spontaneous

Nipple DischargeNipple Discharge
PathologicPathologic– UnilateralUnilateral– SpontaneousSpontaneous– Heme (+)Heme (+)
Most common cause intraductal papillomaMost common cause intraductal papilloma

Bloody Nipple DischargeBloody Nipple Discharge

Intraductal PapillomaIntraductal Papilloma
Single ductSingle duct
BenignBenign
4% of intraductal ca4% of intraductal ca

ImagingImaging
MammographyMammography
UltrasoundUltrasound
MRIMRI

MammographyMammography
Screening toolScreening tool– Age of 40Age of 40
Estimated reduction Estimated reduction in mortality 15-25%in mortality 15-25%
10% false positive 10% false positive raterate
Densities & Densities & calcificationscalcifications



CalcificationCalcification
MacrocalcificationsMacrocalcifications– Large white dotsLarge white dots– Almost always noncancerous and require no Almost always noncancerous and require no
further follow-up. further follow-up.
MicrocalcificationsMicrocalcifications– Very fine white specks Very fine white specks – Usually noncancerous but can sometimes be Usually noncancerous but can sometimes be
a sign of cancer.a sign of cancer.– Size, shape and patternSize, shape and pattern




BI-RADSBI-RADS
BI-RADS BI-RADS ClassificationClassification
FeaturesFeatures
00 Need additional imagingNeed additional imaging
11 Negative – routine in 1 yrNegative – routine in 1 yr
22 Benign finding – routine in 1 yrBenign finding – routine in 1 yr
33 Probably benign, 6mo follow-upProbably benign, 6mo follow-up
44 Suspicious abnormality, biopsy Suspicious abnormality, biopsy recommendedrecommended
55 Highly suggestive of malignancy; Highly suggestive of malignancy; appropriate action should be takenappropriate action should be taken

UltrasoundUltrasound
Not a screening toolNot a screening tool
Palpable vs cysticPalpable vs cystic
Mammographic detected lesionMammographic detected lesion


UltrasoundUltrasound

Malignant or Benign

Malignant vs Benign

MRIMRI
High risk patientsHigh risk patients– Personal history of breast caPersonal history of breast ca– LCIS, atypiaLCIS, atypia– 11stst degree relative with breast cancer degree relative with breast cancer– Very dense breastVery dense breast
High sensitivity (95-100%)High sensitivity (95-100%)– 10-20% will have a biopsy10-20% will have a biopsy

MRIMRI
Pre Gad Post Gad Color Overlay

DiagnosisDiagnosis
Fine needle aspiration Fine needle aspiration – CytologyCytology
Core biopsyCore biopsy– Image guidedImage guided– StereotacticStereotactic
Excisional biopsyExcisional biopsy– Needle localizationNeedle localization

FNAFNA
Fast, inexpensiveFast, inexpensive
96% accuracy96% accuracy
Institution dependentInstitution dependent
Unable to differentiate Unable to differentiate b/w in situ vs CAb/w in situ vs CA

Core Needle BiopsyCore Needle Biopsy
14-18 gauge spring loaded needle14-18 gauge spring loaded needle
TissueTissue
Multiple Multiple


Large Core BiopsyLarge Core Biopsy
6-14 gauge core6-14 gauge core
Large samplesLarge samples
Single insertionSingle insertion

Core biopsy Vacuum Assisted

Excisional BiopsyExcisional Biopsy
Atypical lesionsAtypical lesions
LCISLCIS
Radial scarRadial scar
Atypical papillary lesionsAtypical papillary lesions
Radiologic-pathologic discordanceRadiologic-pathologic discordance
PhyllodesPhyllodes
Inadequate tissue harvestingInadequate tissue harvesting
Related Documents











