Hépatites Virales C et B et Infection par le VIH

Benhamou Hcv Hiv Du 2009
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hépatites Virales C et B et Infection par le VIH

Causes de décès d’origine infectieuse dans le monde (2000)
HIV – HBV – HCV : TOP 10
MaladiesMaladiesInfections respiratoiresInfections respiratoiresVIHVIHDiarrhéesDiarrhéesTuberculoseTuberculoseMalaria Malaria RougeoleRougeoleHépatite BHépatite BPertussisPertussisTétanos néonatalTétanos néonatalHépatite CHépatite C
Décès par anDécès par an~3,5 million~3,5 million~3,0 million~3,0 million~2,2 million~2,2 million~2,0 million~2,0 million~1-3 million~1-3 million
~888,000~888,000~750,000~750,000 ~355,000~355,000~300,000~300,000
~ 250,000~ 250,000 Source : CDC, WHO, UNICEF, UNAIDSSource : CDC, WHO, UNICEF, UNAIDS

Viral hepatitis in HIV-infected patients
Hepatotoxicity
of anti-retroviral therapies
Progression to
Cirrhosis
Mortality
Prevalence
Active consideration for treatment of hepatitis
?Controversies
?Accelerated
Higher compare to HBV mono-infected
Major cause of death
7%-10%20%-35%
HBVHCV

Hépatite Chronique C Chez les Patients
Co-infectés par le VIH

Influence of HIV on HCV
• Major cause of mortality
• More severe liver lesions vs HCV mono-infected
• Higher HCV RNA
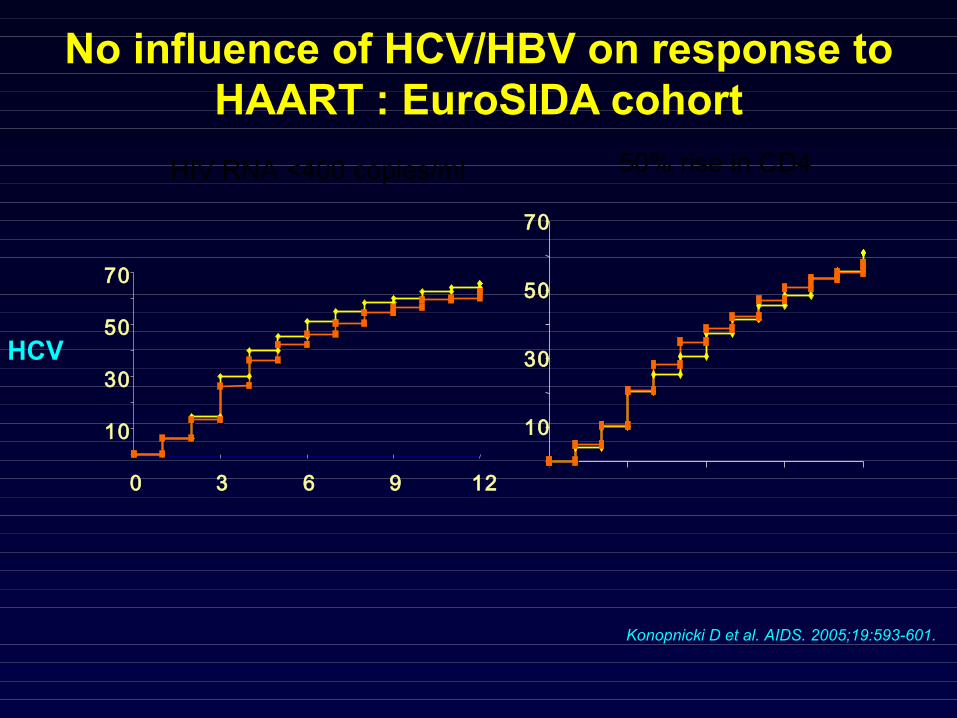
No influence of HCV/HBV on response to HAART : EuroSIDA cohort
Konopnicki D et al. AIDS. 2005;19:593-601.
HIV RNA <400 copies/ml 50% rise in CD4
10
30
50
70
0 3 6 9 12
10
30
50
70
HCV

Mortalité chez les patients VIH en FranceÉtude du groupe GERMIVIC
Influence du VIH sur le VHC Mortalité liée à l’atteinte hépatique
Caboub et al, CID 2001; Rosenthal et al, AIDS 2003.
0102030405060708090
100
1995 1997 2001 2003
%
Mortalité Globale Mortalité liée au Sida Mortalité liée au foie CHC
8
91,6
1,56,9
2
84,5
6,6 8,8
1
48,7
14,3
36,7
1
47
12,6
40,4

Impact of HAART on liver related mortality
Qurishi N et al, Lancet 2003
Days of observation
500040003000200010000
Surv
ival
1.1
0.9
0.7
0.5
0.3
p < 0,0001
HAART
ARV
Untreated
6000 6000500040003000200010000
1.1
0.9
0.7
0.5
0.3
p < 0,018
HAART
ARV
UntreatedSurv
ival
Global Mortality Liver Mortality
Days of observation

Progression to cirrhosisinfluence of alcohol and immune
status
0
1
2
3
4
5 10 15 20 25 30 35 40
CD4<200/µLOH>50 g/j
CD4 <200/µLOH <50 g/j
CD4 >200/µLOH<50 g/j
HIV-OH<50 g/j
Benhamou et al. Hepatology 1999;30:1054-1058
Estimated duration of HCV infection
Fibrosis(METAVIR)

Timing for Anti-HCV and ARV initiation
- Monitor HIV- Anti-HCV recommended (if indicated)
- ARV recommended- ARV before anti-HCV
HIV/HCVHIV mono-infected
Monitor> 350 CD4 cells/µL and< 500 CD4 cells/µL
ARV possible : - High HIV RNA and - Rapid CD4 decline
> 200 CD4 cells/µL and < 350 CD4 cells/µL
ARV recommended< 200 CD4 cells/µL
Adapted from IAS–USA panel guidelines. Yeni P. at al. JAMA, 2004
CD4>350 :• Fibrosis progression rate is reduced• CD4 decline to « dangerous » level if anti-VHC is initiated
Alberti et al. 1st ECCC. J Hepatol. 2005

Treatment of chronic hepatitis C
Genotype 2/3 Genotype 1/4
< 800 000 UI/mL > 800 000 UI/ml
PEG IFN2 (a:180 /b:1.5 µg)RBV 800 mg48 w
Fibrosis: >2
HCV RNA
Fibrosis: 0/1
PEG IFN2 (a:180 /b:1.5 µg)RBV 1000-1200 mg48 w
Rx differed
Alberti et al. 1st ECCC. J Hepatol. 2005

PEG IFN/RBVVirological response
29%
38%
14%
29%
15%21%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
ACTG APRICOT RIBAVIC
EOT SVR
GT 1GT 4
80%
64%68%
73%
53%
31%
62%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
ACTG APRICOT Laguno RIBAVIC
EOT SVR
GT 1/4 GT 2/3
RBV 800 mg 24 weeks
Torriani F et al. NEJM 2004. Carrat F et al. JAMA 2004. Laguno C ett al. AIDS 2004. Chung R. NEJM. 2004
GT2/3,
Rx
48 w

APRICOT(overall SVR 40%)
PRESCO(overall SVR 50%)
Pat
ien
ts (
%)
all 48 weeks therapy
HIV-pos; low RBV dose
0
10
30
40
Geno 1 Geno 3
29%
62%
50
20
n=176 n=95
Geno 1 Geno 3
36%
72%
n=191
24, 48 or 72 weeks therapy
HIV-pos; weight-based RBV
n=152
Ramos et al. J Viral Hepat (in press)

Impact of HCV RNA on SVR
61 63
18
61
0
20
40
60
80
100
≤800,000n=46
>800,000n=130
≤800,000n=28
>800,000n=67
Prop
ortio
n of
pat
ient
s
Torriani F et al. NEJM. 2004.
GT 1 GT 2/3
21 (43 %)49> 5000 cp/mL
23 (35 %)6650-5000 cp/mL
72 (42 %)173< 50 cp/mL
HIV RNA
90 (47 %)216≥ 350 /µL
26 (36 %)72< 350 /µL
8 (47 %)17< 200/µLCD4
SVRN
Cooper D. et al, XV AIDS Conference
HCV RNA
Liver evaluatio
n for
GT1, high H
CV RNA

APRICOTSVR according to Rx exposure
*Patients violated the rule if ≥1 of the three targets were not achieved Opravil M. et al. 45th ICAAC 2005; Abstract 2038
39%
SV
R r
ate
(%)
SV
R r
ate
(%)
≥80/80/80exposure
0
10
20
30
40
50
11%
<80/80/80exposure*
62
29%
Allpatients
n = 176 114
69%
SV
R r
ate
(%)
SV
R r
ate
(%)
≥70/70/70exposure
0
20
40
60
80
100
26%
<70/70/70exposure*
27
59%
Allpatients
n = 111 84
GT1 GT2/3

VR n (%) PPV (%) NPV (%)
G1 G2/3 G1 G2/3 G1 G2/3
119 (68)
83 (87)
39 70
93
92
71 (40)
76 (80)
58 74
90 84
Week 4
≥1 log10 drop
≥2 log10 drop
HCV RNA -ve 22 (13)
35 (37)
82
94
79
57
148 (84)
89 (94)
34
66 96
100
110 (63)
84 (88)
45
70
98
100
60 (34)
68 (72)
70
82
92
89
log10 drop
Week 12
≥1 log10 drop
≥2
HCV RNA -ve
Torriani F, et al. 45th ICAAC 2005; Abstract 1024
APRICOT

PEG IFN/RBV : Specific AE• Liver decompensation : 10% of cirrhotic pts
• Pl., Bilirubin, P alc, Hb and ddI• Compensated cirrhosis: No ddI, Monitoring +++
• Mitochondiral toxicity (1%-3%)• ddI (d4T) (RR x23)• No ddI – (d4T ?)• Monitor : Amylase, lipase, lactic acid
• Anemia : Hb <8 g/dL : 3.8%• AZT (RR x2)• Use EPO
• Neutropenia : Neutrophils <750: 2-11%• Use GCSF
Alberti A et al. 1st ECCC. J Hepatol. 2005 .Torriani F et al. NEJM 2004. Carrat F et al. JAMA 2004. Chung R et al. NEJM. 2004

CONCLUSION
• HCV coinfection: X30 in HIV vs general population
• HCV coinfection major cause of mortality and
morbidity in HIV population
• Less than 20% of the Patients have received anti-
HCV therapy in Europe
• Coinfected patients should be actively considered for
HCV therapy

Hépatite Chronique B Chez les Patients
Co-infectés par le VIH

VHB et VIH
• Prévalence de HBsAg x10 chez les VIH+ vs VIH-
• Contamination sexuelle et UDIV• Virus sauvage/virus pre core: 80% / 15%
• Réactivation en cas d’immunodepression sévère
• HCB plus sévère chez les patients VIH
• Dépistage et prévention (vaccination)

HIV/CHB CoinfectionInfluence of HAART
• Increases duration of HBV by improving survival
• Increases the risk of ALT flares related to
– Immune restoration– Hepatotoxicity
• (Severe) reactivation– Low CD4– ARV discontinuation– LAM resistance
• Inhibition of HBV replication associated with histological improvement (LAM, FTC, TDF)
• LAM reduces liver decompensation
?
Proia et al. Am J Med 2000. Wit et al. JID 2002. Benhamou et al. J Hepatol 2005. Bruno et al. Gastroenerol 2002. Bonacini et al. Gastroenterol 2002. Puoti et al. Antiviral Ther 2004. Gouskos AIDS 2004

Influence of HIV on HBVHIV in HBsAg positive patients (compared to HBV mono-
infected):
– Increases the risk of chronicity after HBV contamination
– Reduces the seroconversion rates to anti-HBe and anti- HBs
– Increases HBV replication
– Increases reactivation rate (related to CD4 decline)
– Accelerates fibrosis progression
– Increases the risk of liver decompensation, HCC and liver deathBodsworth, JID 1989 ; Hadler, JID 1991 ; Krogsgaard, Hepatology 1987 ; Bodsworth, JID 1989 ; Gilson, AIDS 1997. Piroth, J Hepatol 2002
Vogel Cancer Res 1991; Corallini Cncer Res 1993 ; Altavilla Am J Pathol 2000 ; Bodsworth, JID 1989 ; Mills, Gastroenterol 1990 ; Goldin, J Clin Pathol 1990 ;Gilson, AIDS 1997 ; Thio, Lancet 2002. RR 8.3 (4.8-14.3) ; Di Martino, Gastroenterol 2002 ; Colin : Hepatol 1999 ; Di Martino, Gastroenterol ;
Perillo, Ann Int Med 1986 ; McDonald, J Hepatol 1987 ; Colin, Hepatology 1999 ; Gilson, AIDS 1997

<.0001
<.0001
N=54
2 (2-2)29.6%
134.7
N=469
1 (1-2)16
130.1
Liver biopsy*
Fibrosis (median)- Cirrhosis (%)
Inflammation (median)- A2/3 (%)
<.000162.1%37.8HBVDNA> 6 log (%)
<.000134.8%17.1LAM-R HBV (%)
<.000178.8%49.9HBeAg + (%)
NS57 (47-74)29.1
50 (45-56)26.7
Median ALTALT< 2xULN (%)
PHIV positiveN=164
HIV negativeN=504
Assessed by the METAVIR scoring system.
HBsAg+ vs HBsAg+/HIVGHPS cohort
Benhamou et al CROI 2005

Liver Mortality Rate (per 1000 PY)MACS
0
2
4
6
8
10
12
14
16
HIV-/HBV- HIV-/HBV+ HIV+/HBV- HIV+/HBV-
Thio et al. Lancet 2004

0
0.25
0.50
0.75
1
0 75 150 225 300
Follow up (months)
Pro
po
rtio
n o
f p
atie
nts
fre
e
Of
live
r d
eco
mp
ensa
tio
nHIV – (n=504)
HIV + (n=164)
P=0.004
Liver decompensation in HBsAg+
Benhamou et al. CROI 2005

Anti-HBV therapy
• Objective: Decrease liver inflammation and fibrosis progression
• Criteria for anti-HBV initiation:– HBV DNA
• AgHBe+ > 20 000 UI/ml• AgHBe- > 2000 UI/ml
– Histology• METAVIR A≥2 F≥2
Thresholds based on HBV mono-infected knowledgeMay be used in HIV/HBV co-infected patients

HIV/HBV: Treatment
Licensed for Treatment of CHB
• Lamivudine
• Adefovir dipivoxil
• Entecavir*
• IFN/Pegylated IFN
Licensed for Treatment of HIV Only with Demonstrated Anti-HBV Activity
• Tenofovir DF
• Emtricitabine
* USA

-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0 4 8 12 20 28 36 44 52
Time in Weeks
Me
dia
n c
ha
ng
e in
log
HB
V D
NA
Lamivudine Placebo
Serum HBV DNA
Dore GJ, et al. J Infect Dis. 1999;180:607-613.
HIV/HBVLamivudine
-2.7 log10 copies/mL

Lo
g10
HB
V D
NA
24 22 20 20 1733 33 33 33 3310 10 10 7 7
FTC HBV+HIVFTC HBV
d4T HBV+HIV
FTC is not licensed for the treatment of HBV.Raffi F. IAS Conference, July 13-16, 2003, Abstract # 215.
FTC HBV+HIV
d4T HBV+HIV
FTC in Chronic HBV (FTCB-102)
HIV/HBVFTC

4
5
6
7
8
9
10
0 12 24 36 48
ETV PBO
5.56
HB
V D
NA
(lo
g1
0 c
op
ies/
ml)
9.19
4.79
5.63
Weeks
RDZ double binded phase All the patients: ETV 1.0 mg
HIV/HBV LAM-R: ETV
Pessoa et al. ICAAC 2005

HB
V D
NA
(lo
g10
co
pie
s/m
l)
- 6.2 log10 c/ml p<0.001*
-7.0
-6.0
-5.0
-4.0
-3.0
-2.0
-1.0
0.0
0 24 48 72 96 120 144 168 192
ADV (weeks)
- 5.9 log10 c/ml p<0.001*
- 4.7 log10 c/ml P<0.001* - 5.5 log10 c/ml
p<0.001*
31 29 31 30 31 29 27†27n = 35
†27 patients remain on study
* p<0.001 Wilcoxon Sign Rank Test
Benhamou et al, Lancet, 2001 & J Hepatol in press
HBV DNA HBV DNA (< 2.6 log(< 2.6 log1010 copies/ml) copies/ml) 8/358/35
HBeAg negativationHBeAg negativation 3/33*3/33*
HBe seroconversion HBe seroconversion 2/33*2/33*
HIV/HBV LAM-RADV

Median (Q1-Q3) HBV DNA in HBeAg+ (n=72)
Benhamou Y, et al. Hepatology 2006 (in press)
HIV/HBVTDF
Months of TDF
*Roche Cobas Amplicor, LLQ 200 copies/mL

Peters M et al. CROI 2005.
-7
-6
-5
-4
-3
-2
-1
0
0 12 24 36 48
ADVTDF
HB
V D
NA
(lo
g 10 c
/mL)
*
ADV 25 24 23 20 18 17
TDF 27 26 23 18 17 18
HIV/HBVADV vs TDF
*Roche Cobas Amplicor, LLQ 200 copies/mL

NoyesyesYES?YesPoorAnti HIV activity
?
49%
?
3.6
wt, preC, LAM-R??
24
51
ETV*
wt, preC, LAM-R
wt, preC LAM-R
wt, preCwt, preCwt, preCAnti-HBV activity
ADV*TDF*FTCLAMIFN
33-50%
35-66%
7%
4 - 5.4
48-144
35
?
12-20%
9%
26%**
12-24
87
???Histological improvement
??30-50%ALT response
4%?11%HBe seroconv.
4.432.7HBV DNA decline (log cp/ml)
24-484848Duration (weeks)
20033215No. of patients
* Added to LMV in the majority of the cases. ** < 6log copies/ml
HIV/HBV: anti-HBV therapy
Wong DK et al. Gastroenterology 1995. Di Martino V et al. Gastroenterology 2002. Dore GJ et al. J Infect Dis 1999.Benhamou Y et al. Hepatology 1996. Pessoa W et al. CROI 2005. Raffi F et al. 2003 IAS. Peter M et al. CROI 2005..Ristig MB et al. J Infect Dis. 2002. Benhamou Y et al. N Engl J Med. 2003.
Benhamou Y et al. Lancet 2001 and AASLD, 2003

HBV resistance
Lai C et al. N Engl J Med 1998. Leung N et al. J Hepatol 1999. Chang T et al. Antiv Ther 2000. Benhamou Y et al. Hepatology 1999. Benhamou Y et al. Lancet 2001 and AADSL 2003. Data on file. NV-02B-003. Idenix.
HIV/HBV HIV/HBV HBV HBV
0
00
0
0
0
0
50
90
0
4%
024%
18
4%
9
19%24
38
49
67%
0
10
20
30
40
50
60
70
80
90
1
3
LMV
FTC LdT ADV
LMV+L
dTETV
LMV
LMV+A
DV
LMV+T
DF
ETV +
LAM
Years
Patien
ts (%)
Patien
ts (%)

Treatment Algorithm Patients with Compensated Disease
and No indication for HIV therapy

Treatment Algorithm Patients with Compensated Disease
and indication for HIV therapy
Related Documents











