Being young, male and experiencing first psychosis: what do we know that works? Max Birchwood www.youthspace.me

Being young, male and experiencing first psychosis: what do we know that works? Max Birchwood .
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Being young, male and experiencing first psychosis: what do we know that works?
Max Birchwood
www.youthspace.me

Picking up on yesterday’s lecture..• Psychoses are predominantly male with onsets
stretching into early adolescence• Young males with psychosis prone to severe social
disability, developing in adolescence and continuing into early adulthood. This group at v high risk of NEET.
• Anti-social and harmful behaviour more prevalent in males and can persist post-onset. But de novo behaviour linked to acting on delusions.

Interventions
• Acting on delusions: can we prevent harm? The case of command hallucinations
• Interventions to prevent NEET: IPS• Overcoming major social disability emerging
from adolescence

Reducing harmful ‘acting on’ delusions
The case of command hallucinations.

UK Daily Mail front pageJune, 2007

• Why are voices so distressing?
• Why do voice hearers act upon them?
The cognitive model of voices: it’s a (pernicious, imbalanced ) interpersonal relationship
Perceived malevolent intent + Perceived power of
voice to act on the intent = susceptibility to comply

BELIEFS[Power; malevolent intent]
EVIDENCESAFETY
BEHAVIOURS
AFFECTFear, guilt, elation,
depression
VOICEACTIVITY
Omniscience:shame; predictions
Control
Threat MitigationActing on voices
Eg. Full Compliance;Partial (appeasement)

Command Hallucinations
• Are common: 53% of all voices• Cause high levels of distress• 48% of stipulate harmful or dangerous actions • 33% comply with CHs• 33% ‘appease’ or show minor compliance but
remain at risk of later compliance


Can we reduce harmful compliance with commanding voices?
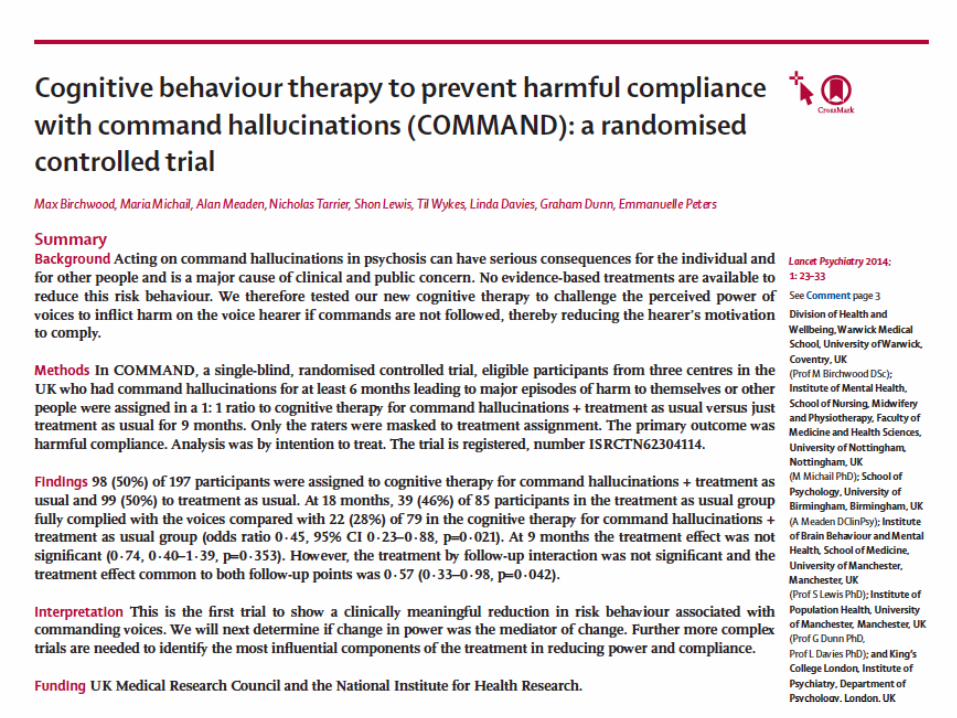

Therapy developed by MB to test out the perceived power of the voice by examining evidence for: a) the omniscience of the voice,b) the apparent ability of the voice to predict the future
and deliver on its threats andc) the voice hearer’s perceived lack of control over
voice activity.

Birmingham(Birchwood, CI)
Manchester(Tarrier/Lewis) London
(Peters/Wykes)
MRC COMMAND trial sites

Design
►Pragmatic comparison of CT+TAU vs TAU
►Single-blind, ITT►Follow-up at 9 and 18 months from
randomisation►Powered by pilot trial (2004, BJ Psych) ►Up to 20 sessions, within 9 month
envelope.Birchwood, et al. "A Multi-Centre, Randomised Controlled Trial of CognitiveTherapy to Prevent Harmful Compliance with Command Hallucinations." BMC Psychiatry 11, (2011). ,

Inclusion criteria
►‘Harmful’ compliance within last 9 months
►Continuous voices for last 6 months and at inclusion
►Schizophrenia spectrum

Primary outcome
Presence of one or more episodes of full compliance within follow-up period.

The results

Consent, completion and follow-up
►27/242 (11%) declined consent►83.5% completed the intervention►164/197 (83.2%) completed 18 month
follow-up

28%46%
Primary outcome:compliance to 18 months
TAU CTCH+TAU
Pre= 100% , both groups
Odds ratio = 0.45 (95% confidence interval 0.23 to 0.88, p=0.021)
The estimate of the treatment effect common to both follow-up points was 0.57 (95% confidence interval 0.33 to 0.98, p=0.042)


Supported employment programmes, sometimes referred to as individual placement and support(IPS), are any approach to vocational rehabilitation that attempts to place service users in competitive employment immediately. Supported employment can begin with a short period of preparation, but this has to last less than 1 month and not involve work placement in a sheltered setting, training or transitional employment.
Supported employment






Reducing severe social disabilityarising from adolescence.
The SUPEREDEN trial

Inclusion criteria: • Receiving support from early intervention
service for 12 month, but• Continued low level of structured activity
(defined as 30 hours or less per week on the Time Use Survey).
Who is it targeted at?

Social Recovery orientated Cognitive Behavioural Therapy (SR-CBT)
• To overcome blocks to activity (eg. Hopelessness, social anxiety, family acceptance, stigma); and to create motivation to change (‘where would you like to be in 5 years?’)
• Delivered by accredited CBT therapist/Clinical Psychologist
• SRCBT is delivered in three stages: - Stage 1: Developing a Formulation - Stage 2: Preparing for new activities - Stage 3: Engaging in new activities

Stage 1: Developing a Formulation. This consists of assessment and history taking with respect to personal motivation, premorbid hopes/expectations and goals which have either been changed or altered with respect to the impact of illness.
The focus is on identifying meaningful personal goals which can be linked with achievable day-to-day activity targets and thus address motivation and hopelessness. This often involves validation and acceptance of real barriers, threats and difficulties, while focusing on promoting hope for social recovery.

Stage 2: Preparing for new activities. Cognitive work at this stage involves promoting a sense of agency and addressing hopelessness, feelings of stigma and negative beliefs about self and others. The client and therapist work to identify pathways to meaningful new activities. Where relevant this includes referral to relevant vocational agencies, community providers of social or sports activities, employers or education providers.

Stage 3: engaging in new activities.
This involves the active promotion of social activity, work, education and leisure linked to meaningful goals. Promotion of activity occurs through behavioural experiments, while managing symptoms of anxiety and low level psychotic symptoms.
Therapists will combine therapist and case management roles for example, by adopting an assertive outreach worker style of contact, most frequently visiting people at home, or community or in education settings.
Therapists a adopt a pragmatic and problem-solving approach in assisting people to improve the time spent in constructive activities. This often involves setting up joint interviews with community activity providers and family members to discuss and overcome potential problems and blockages to social recovery.

• 12 months into EIS• Low level of structured activity after at least one year
of treatment in EIS(defined as 30 hours or less per week)= ‘social disability’ or ‘severe social disability’.
Participants

Primary hypothesis is that the intervention will lead to improvements in the time spent in structured activity.
Secondary hypotheses the intervention will: (a) reduce levels of depression and hopelessness and (b) improve negative symptoms.
Objectives

• Single blind, ITT trial comparing Social Recovery-oriented Cognitive Behavioural Therapy plus standard care from an EIS with standard care from an EIS.
• The intervention will last for 9 months with assessments at: baseline, end of therapy (9ms); and at 6 months after end of therapy (15 months).
• The assessments will be conducted by independent
assessors, blind to treatment allocation.
Design

10/155 in some level of paid employment.
Mean 7.45 hours (1.5-15)
At baseline

Baseline data: complex co-morbidities
SIAS= 39.5 (15.3). 56% above threshold for social anxiety
BDI= 18.7 (11.8) 46% ‘moderate or severe’; 19% ‘severe’


Sorry!Results expected by June 2015
Male gender and psychosis
• Young males at highest risk.• Adolescent social withdrawal, anti-social behaviour
and emotional dysregulation = risk factors for psychosis, not ‘precursors’ of psychosis.
• Social disability and harm behaviours have little to do with presence vs absence of ‘positive’ symptoms. Needs new interventions, as they can persist and affect life chances.
• There are good and emerging interventions for these, which do not presuppose treating the ‘disease’
Related Documents
![Birchwood Rai Kansas - OC Flock Management Inc Birchwood Rai... · Birchwood Rai Kansas [CAN] S113192 DAM: Birchwood Classic Jolene: 2005 West National Junior Champion Saanen 1-1](https://static.cupdf.com/doc/110x72/5fcbc9f11a8e552e991049f8/birchwood-rai-kansas-oc-flock-management-inc-birchwood-rai-birchwood-rai.jpg)










