Behavioural and Psychological Symptoms of Dementia in Turkey Engin EKER, MD Istanbul University, Cerrahpaşa Medical School Dept. of Geriatric Psychiatry eneker @ istanbul . edu . tr Regional Symposium on Alzheimer’s Disease and Related Disorders in the Middle East October 1-2,2005 Istanbul ,Turkey

Behavioural and Psychological Symptoms of Dementia in Turkey Engin EKER, MD Istanbul University, Cerrahpaşa Medical School Dept. of Geriatric Psychiatry.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Behavioural and Psychological Symptoms of
Dementia in Turkey
Engin EKER, MDIstanbul University, Cerrahpaşa Medical School
Dept. of Geriatric [email protected]
Regional Symposium on Alzheimer’s Disease and Related Disorders in the Middle East
October 1-2,2005Istanbul ,Turkey

Expected population of Turkey (million) (OECD projections 1997, SIS 1990 & 2000, DPA 2003)
56,561
6667,8 70,4
75
83
0
10
20
30
40
50
60
70
80
90
1990* 1995 2000 2000* 2003* 2010 2020
1990*
1995
2000
2000*
2003*
2010
2020

Elderly Population in Turkey: Highlights Ertan T. IPA Congress.2003
• The proportion of elderly in total population in Turkey is rapidly growing.
>60 y: 1990: 7,1% 2003: 10,8%
>65 y: 1990: 4,3% 2003: 8%
OECD Projection 7,7% in 2020

Behavioral and Psychological Symptoms of Alzheimer Disease
• Behavioral-Agression, hostility, agitation: 60%-Apathy: 70%-Wandering and other motor behavior: 30%-40%
• Psychological-Depression: 20%-50%-Anxiety: 40%-50%-Hallucinations or delusions: 10%-20%Mega Ms et al. Neurology. 1996;46:130-135; Rubin EH etal. J Geriatr Psychiatry Neurol. 1988;1:16-20; Tariot PN et al. Am J Psychiatry. 1993;150:1063-1069.

Why are BPSD Important
• Diminish patient quality of life
• Increase caregiver distress: decrease caregiver quality of life( most of the caregivers may have depressive symptoms)
• Increase cost of care
• Precipitate nursing home placement
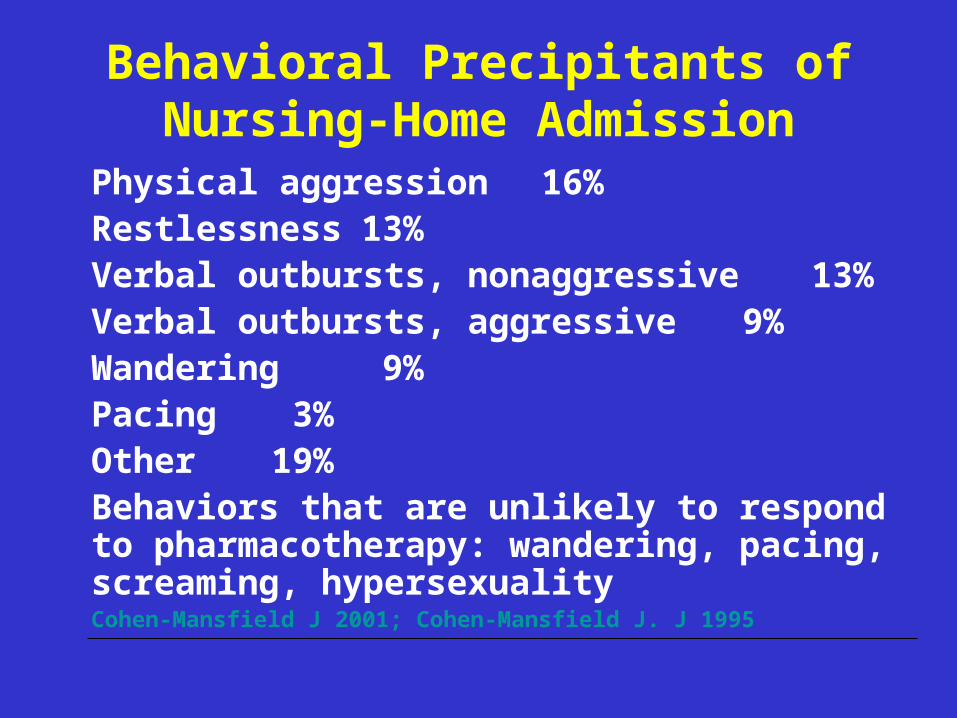
Behavioral Precipitants of Nursing-Home Admission
Physical aggression 16%Restlessness 13%Verbal outbursts, nonaggressive 13%Verbal outbursts, aggressive 9%Wandering 9%Pacing 3%Other 19%
Behaviors that are unlikely to respond to pharmacotherapy: wandering, pacing, screaming, hypersexualityCohen-Mansfield J 2001; Cohen-Mansfield J. J 1995

The Reasons of Prevalence and Presentation of BPSD in Different
Cultures Culturally related factors • The concepts of dementia and behavioural disturbances in society (The typical features of dementia are widely recognized
and named “Chinnan (literally childishness) in Kerala (Shaji et al. 2003) • The tolerance of symptoms in dementia• • Not always possible direct observation of the patient by clinician• No cultural appropriateness of rating scales
• Availabity of primary and secondary care services for demented patients with BPS
• • A

Beds for Demented Patients in Turkey
• 10% of the beds in all old age homes run by the Health Ministry and Municipalities are spared for demented and physically debilated patients
• These patients are separated from the rest of the building
• Some voluntary groups are engaged in looking after these patients
• The staff working in these parts of old age is well trained

Services for Elderly People With Acute Psychiatric Problems
• There are three specialist geropsychiatric unit in Istanbul
• The first geropsychiatric unit was organized in Cerrahpaşa Medical School,Istanbul University in 1993
• The elderly with psychiatric problems are mostly placed in general psychiatry departments and are treated by general psychiatrists

Older People and the Informal Health Care System in Turkey
• In Turkey, families, friends and neighbours are extensively involved in the care of older people
• Demented patients are cared for mostly by their spouses,eldest daughters ,or daughter in-law
• Families approach instutional care as a last resort (Eker,1995)
• The Directoriate of Social Work and Care has developed a project recently “taking care of the elderly at home”

BPSD in Turkish AD(Eker; Ertan; Engin, 2003)
SAMPLE : 213 probable and possible AD
cases
EVALUATION: DSM-IV (APA, 1994)
The Turkish vers. MMSE
(Güngen, Ertan, Eker, 1998)
GDS (Reisberg et al. 1982)
Behave-AD (Reisberg et al. 1987)
Neuroimagine technics (CT, MRI)
Genetic studies (Apo E4)

Age, Gender, Educational Level, Total BEHAVE-AD Score, the MMSE Turkish
Score (in 213 AD Cases)
Age, years 74,01±8(45-95)Female, % 68.5Education, years 7.6 ±5(0-17)Disease duration 4.3 ±3(1-20)The MMSE score 15.6 ±7(0-30)Behave-AD score l0.8 ± 9 (0-47)Patients with symptoms 91.9%

RESULTS (II)Stage Specific Mean BAHAVE-AD in Turkish
AD patients Subcategory Scores Stage 3(n:24) Stage 4(n:50) Stage 5(n:74) Stage
6(n:56) Paranoid ordelusional ideat 0.75 ±2(0-10) 1.6 ± 1.5(0-7) 1.8 ±1.9(0-7) 4.4 ±3.5(0-15) Hallucinations 0.036 ±0.2(0-1) 0.6 ±1.3(0-5) 0.7 ±1.3(0-5) 1.9 ±2.6(0-13)Activitydisturbances 0.42 ±0.9(0-3) 1.6 ±1.8(0-8) 1.7 ±1.8(0-7) 3.7 ±2.8(0-9)Aggressiveness 0.53 ±1.3(0-6) 1.4 ±2(0-7) 1. ±1.7(0-9) 2.5 ±3(0-9)Diurnal rhythmdisturbances 0.43 ±0.9(0-3) 0.6 ±1(0-3) 0.4 ±0.9(0-3) 1.3 ±1.4(0-3)AffectiveDisturbances 0.53 ±0.9(0-3) 1.2 ±1.73(0-5) 0.8 ±1.29(0-6) 1.5 ±1.57(0-6)Anxieties andPhobias 0.75 ±0.9(0-3) 1.8 ±2.26(0-8) 2.08 ±2.1(0-6 2.7 ±2.6(0-11)

Stage specific severity of each Behave AD subcategory
in Turkish AD patiens
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
Stage 3 Stage 4 Stage 5 Stage 6
DelusionsHalluc.Activity dist.AgressivenessDiurnal rhythmAffect. Dist.Anxiety

RESULTS (III)Most Frequent Symptoms in Turkish AD
Patients (in 213 cases)% n
Purposeless activity 49.3 (105)“People are stealing things” delusion 44.6 (95)Wandering 42.7 (91)Fear of being left alone 40.8 (87)Tearfulness 40.4 (86)Inappropriate activity 38.5 (82)Depressed mood: other 37.6 (80)Anxiety regarding upcoming events 36.6 (78)Verbal outbursts 36.2 (77)Day/night disturbances 33.8 (72)Visual halucinations 26.3 (56)

The 10/66 Dementia Group: Behavioral and Psychologiacal Symptom of Dementia in
developing Countries (Int. Psychogeratrics 2004)
• Method:Mild and moderate cases (CDR) Main care
giver 21 centers in 17 developing countries
Community screening Interview for dementia and geriatric mental state schedule (GMS)
• Result:At least one BPS was reported in 70,9% of
the 555 participants.
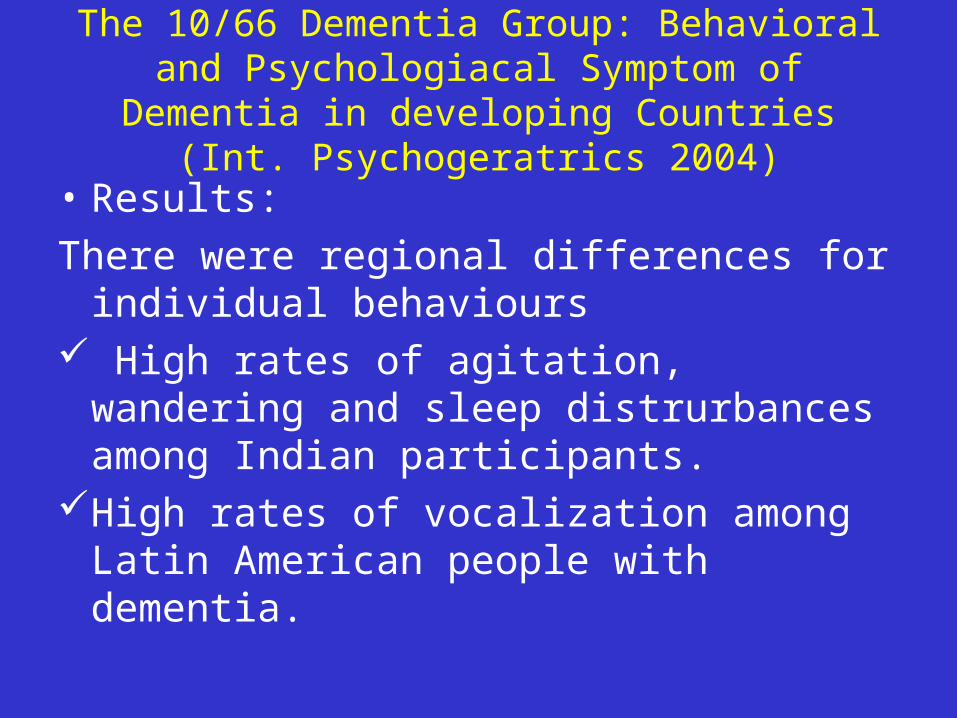
The 10/66 Dementia Group: Behavioral and Psychologiacal Symptom of Dementia in
developing Countries (Int. Psychogeratrics 2004)
• Results:
There were regional differences for individual behaviours
High rates of agitation, wandering and sleep distrurbances among Indian participants.
High rates of vocalization among Latin American people with dementia.

The 10/66 Dementia Group: Behavioral and Psychologiacal Symptom of Dementia in
developing Countries (Int. Psychogeratrics 2004)
• Results: Overall, numbers of reported BSD were
highest in India, intermediate in Latin America and lowest in China.
Depression, anxiety and schizophreniform, paranoid psychosis were commonest among people from Latin America and least common in China.

Delusions in Turkish Patients with AD :Could
Analysing Specific Delusions be More Helpful
ErtanT, Eker E, Engin F et al.2005(I)• Aim: To analyse factors associated with presence
of delusions to find out whether in individual analysis of delusions in the same group would be more informative
• Method :n:185 AD patiens(DSM-IV) MMSE, GDS,Behave-AD Dependent variable :one of the delusions Independent variables: gender,age, education,disease duration,GDS stage ,and
presence of each type hallucination,and remaining types of delusions
Logistic regression analysis was used

Delusions in Turkish Patients with AD:Could Analysing Specific Delusions be More helpful
(Ertan T,Eker E,Engin F.et al 2005)(II)
Result and Conclusions:• None of the delusions was associated with
age ,duration of disease ,and education• Female gender was associated with only one
delusion (delusions of theft)• Disease stage(GDS :Stage 6) was associated with
two delusions(delusion of home is not home and delusion of infidelity( negative association)
• Delusions of theft were also independently predicted by delusions imposter and visual hallucination

Conclusions (I)
• BPSD is still a novel subject in Turkey. Lack of experienced medical staff in Turkey
• Psychiatrists, neurologists, GPs are just having necessary information on the subject
• AD patients are seen by the psychiatrists and neurologists at late stage (stage 5&6)
• Absence of formal services for demented patient • No regular home visit system

Conclusions (II)
• Rating scales (Such as GDS;CDR) and measurements for noncognitive symptoms (Behave-AD; NPI; ADAS-non cognitive) are used only by minority neurologists and psychiatrists

Conclusions (III)
• There are no trained GP, community nurses, social workers
• We should educate family and professional caregivers
• We need more validation studies of observer –rated BPSD screening scale
• We need cross cultural studies on BPSD developing countries
Related Documents