Behavioral Rehabilitation of the “Treatment-Refractory” Schizophrenia Patient: Conceptual Foundations, Interventions, and Outcome Data Steven M. Silverstein, Michi Hatashita-Wong, Sandra Wilkniss, Andrew Bloch, Thomas Smith, Adam Savitz, Richard McCarthy, Michael Friedman, and Ken Terkelsen Weill Medical College of Cornell University This article describes an intensive, inpatient behavioral rehabilitation program for patients with schizophrenia who have been considered “treatment-refractory” at state hospitals. The program is a public–private partnership involving state and private hospitals and community residence providers. The essential elements of this program are described, along with the conceptual and philosophical bases of its treatment and examples of staff behaviors critical to treatment success. Outcome data are then discussed to emphasize the point that when evidence-based psychological treatment is implemented with this population, outcomes can be positive in most cases, and therefore, the number of treatment-refractory patients is actually far less than is estimated on the basis of response to medication alone. Schizophrenia is a serious mental disorder that affects approximately 1% of the population worldwide, with a current global incidence cal- culated at over 20 million people (Jablensky, 2000). The consequences of schizophrenia, in terms of both public health costs and effects on lives are enormous. For example, it has been estimated that as many as 10% of all disabled persons in the United States have schizophrenia (Rupp & Keith, 1993), and the disorder ac- counts for 75% of all mental health expendi- tures and approximately 40% of all Medicaid reimbursements (Martin & Miller, 1998). Among people with the disorder, only between 10%–30% are employed at any one time (Att- kisson et al., 1992), and few of these people are able to maintain consistent employment (Policy Study Associates, 1989). Studies have consis- tently found that quality of life among people with schizophrenia is significantly poorer than among the rest of the population (Lehman, Ward, & Linn, 1982). Schizophrenia typically is diagnosed in late adolescence or early adult- hood, and traditionally, approximately 50 –70% of cases are characterized by a chronic, relaps- ing course with high morbidity and permanent disability. In addition, rates of mortality and somatic morbidity are higher in schizophrenia than in the general population (Lieberman & Coburn, 1986), and the rate of attempted suicide equals that of major depression (Simpson & Tsuang, 1996). The economic costs of treating schizophrenia have been estimated to be $62.7 billion (e.g., including direct treatment costs and lost business productivity due to patient and family caretaker work absence; Wu et al., 2005). Several trends have steadily reduced the number of schizophrenia patients residing in state psychiatric hospitals since the mid-1950s. These include pharmacologic and rehabilitative treatment advances, expanded community hous- ing alternatives, and the development of active family and consumer movements but also state hospital closures, forced census reductions, and moving patients to nursing homes and prison mental health wards (Talbott, 2004). It is im- portant to note that many patients with schizo- phrenia continue to have poor outcomes. For example, at least 30% of patients exhibit an inadequate or poor response to conventional Steven M. Silverstein, Michi Hatashita-Wong, Sandra Wilkniss, Andrew Bloch, Thomas Smith, Adam Savitz, Richard McCarthy, Michael Friedman, and Ken Terkelsen, Weill Medical College of Cornell University. Correspondence concerning this article should be ad- dressed to Steven M. Silverstein, who is now at the Uni- versity of Medicine and Dentistry of New Jersey (UMDNJ)—Robert Wood Johnson Medical School, Uni- versity Behavioral Health Care, 151 Centennial Avenue, Piscataway, NJ 08854. E-mail: [email protected] Psychological Services Copyright 2006 by the American Psychological Association 2006, Vol. 3, No. 3, 145–169 1541-1559/06/$12.00 DOI: 10.1037/1541-1559.3.3.145 145

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Behavioral Rehabilitation of the “Treatment-Refractory”Schizophrenia Patient: Conceptual Foundations, Interventions,
and Outcome Data
Steven M. Silverstein, Michi Hatashita-Wong, Sandra Wilkniss, Andrew Bloch,Thomas Smith, Adam Savitz, Richard McCarthy, Michael Friedman, and
Ken TerkelsenWeill Medical College of Cornell University
This article describes an intensive, inpatient behavioral rehabilitation program forpatients with schizophrenia who have been considered “treatment-refractory” at statehospitals. The program is a public–private partnership involving state and privatehospitals and community residence providers. The essential elements of this programare described, along with the conceptual and philosophical bases of its treatment andexamples of staff behaviors critical to treatment success. Outcome data are thendiscussed to emphasize the point that when evidence-based psychological treatment isimplemented with this population, outcomes can be positive in most cases, andtherefore, the number of treatment-refractory patients is actually far less than isestimated on the basis of response to medication alone.
Schizophrenia is a serious mental disorderthat affects approximately 1% of the populationworldwide, with a current global incidence cal-culated at over 20 million people (Jablensky,2000). The consequences of schizophrenia, interms of both public health costs and effects onlives are enormous. For example, it has beenestimated that as many as 10% of all disabledpersons in the United States have schizophrenia(Rupp & Keith, 1993), and the disorder ac-counts for 75% of all mental health expendi-tures and approximately 40% of all Medicaidreimbursements (Martin & Miller, 1998).Among people with the disorder, only between10%–30% are employed at any one time (Att-kisson et al., 1992), and few of these people areable to maintain consistent employment (PolicyStudy Associates, 1989). Studies have consis-tently found that quality of life among peoplewith schizophrenia is significantly poorer than
among the rest of the population (Lehman,Ward, & Linn, 1982). Schizophrenia typically isdiagnosed in late adolescence or early adult-hood, and traditionally, approximately 50–70%of cases are characterized by a chronic, relaps-ing course with high morbidity and permanentdisability. In addition, rates of mortality andsomatic morbidity are higher in schizophreniathan in the general population (Lieberman &Coburn, 1986), and the rate of attempted suicideequals that of major depression (Simpson &Tsuang, 1996). The economic costs of treatingschizophrenia have been estimated to be $62.7billion (e.g., including direct treatment costsand lost business productivity due to patient andfamily caretaker work absence; Wu et al.,2005).
Several trends have steadily reduced thenumber of schizophrenia patients residing instate psychiatric hospitals since the mid-1950s.These include pharmacologic and rehabilitativetreatment advances, expanded community hous-ing alternatives, and the development of activefamily and consumer movements but also statehospital closures, forced census reductions, andmoving patients to nursing homes and prisonmental health wards (Talbott, 2004). It is im-portant to note that many patients with schizo-phrenia continue to have poor outcomes. Forexample, at least 30% of patients exhibit aninadequate or poor response to conventional
Steven M. Silverstein, Michi Hatashita-Wong, SandraWilkniss, Andrew Bloch, Thomas Smith, Adam Savitz,Richard McCarthy, Michael Friedman, and Ken Terkelsen,Weill Medical College of Cornell University.
Correspondence concerning this article should be ad-dressed to Steven M. Silverstein, who is now at the Uni-versity of Medicine and Dentistry of New Jersey(UMDNJ)—Robert Wood Johnson Medical School, Uni-versity Behavioral Health Care, 151 Centennial Avenue,Piscataway, NJ 08854. E-mail: [email protected]
Psychological Services Copyright 2006 by the American Psychological Association2006, Vol. 3, No. 3, 145–169 1541-1559/06/$12.00 DOI: 10.1037/1541-1559.3.3.145
145

antipsychotic medication (Kane, 1989). A re-cent estimate placed the number of patients inthe United States who were unresponsive to orintolerant of these drugs at 800,000 (Wirshinget al., 1999). Although clozapine, which is gen-erally considered to be the most effective sec-ond-generation antipsychotic agent for “treat-ment-refractory” patients, has produced im-provement among many patients, the rate ofclozapine response among conventional medi-cation nonresponders ranges only from 10%–60% (Kane, 1992; Kane et al., 1988; Simpson etal., 1999). Therefore, it can be estimated that380,000–720,000 patients are nonresponsive tocurrent medications, including clozapine. In ad-dition, clozapine is underutilized because of itscost, side effects, and potential medical compli-cations. Furthermore, even when clozapine re-duces symptoms, there is little evidence of cloz-apine-related improvement in work, social, oroverall level of functioning among “treatment-refractory” patients (Wahlbeck et al., 1999). Forother second-generation antipsychotic medica-tions, recent evidence indicates that they are nomore effective than first-generation medications(Lieberman et al., 2005). Compounding thisproblem is that funding for state hospitals (ad-justed for inflation) has decreased since the1980s, and the proportion of professional staffto nonprofessional staff hired is also decreasing,leading to reduced provision of “best-practice”services (Witkin, Atay, & Manderscheid, 1996).
In response to these issues, the Weill MedicalCollege of Cornell University and the NewYork State Office of Mental Health developed aplan to treat “untreatable” patients remaining instate hospitals. The plan involved the establish-ment of a specialized unit at a private hospital totreat so-called treatment-refractory state hospi-tal patients. In addition, beds were made avail-able at residential facilities in the New YorkCity area, so that if/when patients could bedischarged, they could be placed quickly with-out the delay of a long waiting list. This part-nership between a state mental health system,residential facilities, and an academic medicalcenter was seen as a win–win situation. It wouldhelp reduce the numbers of long-stay patients instate psychiatric hospitals that were under pres-sure to reduce their overall censuses, wouldhelp fill beds at a private hospital, and wouldfacilitate community reintegration for patients.Adding to the incentive for the private hospital
was that the care of the patients transferred therewould be billed at the daily (acute care) rate,which was a higher rate than was the practice atstate hospitals, where an extended care rate wasused for long-stay, chronically mentally ill per-sons. No special appropriations of state fundswere given for this program, however, and itwas staffed similarly to other hospital units.Therefore, the program did not require addi-tional funding from either the state or thehospital.
The result of the partnership, called the Sec-ond Chance Program, opened at the Westches-ter Division of the Weill Medical College ofCornell University—New York PresbyterianHospital (NYPH–WD) in January of 1998. Theprogram evolved in several stages. The firstadmissions were in the winter of 1998. Theprogram was running at a full census of 30patients by the summer of 1998. At this time, anumber of problems arose. The program, whichwas the only non-acute unit in the hospital, hadthe highest rate of assaults (on patients andstaff), and relatedly, the highest rates of seclu-sion and restraint in the hospital. There werealso a myriad of other behavior problems, in-cluding poor patient treatment compliance (e.g.,not taking medication, poor adherence to unitroutines and attendance at groups) and poorgrooming and hygiene (e.g., urinating in pro-gram areas, thus requiring all carpeting to beremoved). These problems led to the recogni-tion that additional interventions were neces-sary. As a result, over the next 1.5 years, a seriesof behavioral interventions were initiated (de-scribed later in Method). These initially focusedon treatment compliance and were then ex-tended to encompass a full range of programbehaviors and community living skills.
Recognition that behavioral interventionswere likely to improve program effectivenesswas based on (a) the results of numerous studiesof psychiatric rehabilitation among medicatedschizophrenia patients (see Liberman et al.,2005; Silverstein, 2000, for reviews); (b) dra-matic improvement among long-stay, severelyill schizophrenia inpatients treated in intensive,social-learning-based inpatient programs (Glynnet al., 1994; Menditto et al., 1994; Paul & Lentz,1977; e.g., in the Paul and Lentz study, long-stay hospital patients who were treated in thesocial learning program achieved a 97% dis-charge rate, compared with a 50% rate in tradi-
146 SILVERSTEIN ET AL.

tional custodial care, and 1200% improvementin adaptive, social, cognitive, and instrumentaloutcomes, compared with negligible improve-ments with other treatment models); (c) a meta-analysis of 106 studies indicating that combinedpsychosocial and pharmacologic treatment dem-onstrated outcomes that were 0.39 standard de-viations better than with medication alone, inaddition to relapse rates that were 20% lowerover a 12-month period (Mojtabai, Nicholson,& Carpenter, 1998); and (d) evidence that clo-zapine can enhance responsiveness to intensiveinpatient behavioral rehabilitation (Menditto etal., 1996), but also that medication doses (andside effects) can often be dramatically reducedwhen patients are treated in such programs(Paul & Lentz, 1977).
The purpose of this article is threefold. First,we review conceptual and philosophical issuesinvolved in establishing and maintaining theward. Second, we describe program compo-nents at program, group, and individual inter-vention levels. Finally, we review outcomedata.
Method
Conceptual Foundations of the SecondChance Program
Ethical Issues in Recruitment, Retention,Clinical Practice, and Ensuring PatientRights
From the earliest phase of program develop-ment, we decided to recruit “typical” treatment-refractory patients and not the type of patientsthat are typically enrolled in treatment outcomestudies (e.g., no comorbidity, history of treat-ment compliance). Therefore, the admission cri-terion for the program was the presence of aserious mental illness that was severe enough topreclude discharge from a state hospital evenafter 3 years of consecutive admission. In most,but not all, cases, patients had diagnosis of apsychotic disorder. After the second year of theprogram, as referrals increased and as the be-havioral milieu was increasingly tailored forpatients with schizophrenia and related disor-ders, the inclusion criteria required that all pa-tients have a primary diagnosis of a psychoticdisorder. The only exclusion criterion was thatpatients not be actively assaultive or predatory
toward other patients. This was necessary be-cause the program was not staffed sufficiently tocope with openly aggressive patients. Neverthe-less, the program accepted many patients withhistories of violence and who demonstrated pe-riodic violent acts. The majority of patients ad-mitted to the program had comorbid substanceabuse histories, and many had histories of ar-rests and of serving time in jail or prison.
Admission to the Second Chance Program iscompletely voluntary. Patients learn about theprogram either through periodic informationalgroup meetings, led by Second Chance staff, ontheir state hospital inpatient units, or throughtreatment team members in individual meetings.In the latter cases, if interest in being transferredis expressed, these meetings are followed up bya discussion with a Second Chance Programsocial worker to receive further information.Only patients who express interest in going tothe program are transferred. Once admitted tothe program, patients could be transferred backto the referring state hospital at their request.During the first 5 years of the program, thisoccurred only once.
Critics of behavioral programs often arguethat such programs can be punitive and abusive.In fact, this is true of any treatment program.The Second Chance Program ensured that hu-mane treatment was actually being delivered byusing several approaches. These included (a)making explicit the consequences of positiveand negative behaviors, (b) linking these behav-iors to specific rewards and privileges, (c) en-suring that more rewards than fines are givenout, and (d) holding staff accountable for thetype and frequency of feedback they give topatients. Paul (2000) argued that, because pro-grams that use these approaches are also asso-ciated with shorter length of stays, greater pa-tient improvement, and higher discharge ratesthan typical long-term inpatient programs, theyare in fact the most humane form of long-termtreatment for people with serious mental illness(Paul, 2000).
Several processes were used to ensure thathigh-quality care was delivered to patients onthe Second Chance Program. First, the programdirector would routinely review the data sheets(see below), which staff were required to initialwhen observing/recording a positive or inappro-priate patient behavior. Through this process, itcould be determined whether all staff were ac-
147TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

tively reinforcing positive behavior and doingthis more than prompting in response to inap-propriate behaviors (although the latter was stillexpected to occur). If it was determined thatstaff were not having enough contact with pa-tients and/or that not enough of this contact wasfocused on positive behaviors, this was reportedto the staff member’s discipline supervisor, andit became an issue for supervision. Second,yearly, full-day staff training workshops andweekly staff meetings were held to review ex-pectations for staff behavior and to model ap-propriate staff behavior. Third, yearly perfor-mance improvement projects were implementedwhere data were collected on aspects of theprogram. These projects included examiningpatient improvement and examining staff be-havior (rated through an observer) at varioustimes throughout the day, using a coding systemsimilar to Paul and Lentz’s (1977) Staff–Resi-dent Interaction Chronograph. Data from suchprojects are routinely reported back to staff. Inrare cases when a new staff member was un-willing or unable to comply with program ex-pectations, they received counseling from theirsupervisor.
Finally, we note that, wherever possible, pa-tients chose which rewards would be available.For example, patient responses to a survey com-pleted during a community meeting guided ini-tial and subsequent purchases for the tokenstore. This ensured that items in the store wouldindeed be reinforcing, by virtue of having per-sonal meaning to the patients. Similarly, it wasclear that patients valued having time off theunit and having cigarettes to smoke. Therefore,the token store included cigarettes in its inven-tory, and the program used time off the unit asthe major reward. The latter was determined bypatient levels, which could change every 7 dayson the basis of the prior week’s frequency ofvarious behaviors (see below). All patientslearned (through staff and a patient handbook,but mainly from other patients) that differentpoint totals, reflecting various levels of perfor-mance of specific behaviors (see below), led todifferent amounts of time allowed off the unit,with increasing levels of independence fromstaff built into this system as well (e.g., athigher levels, patients could be outside withoutstaff supervision). Because only patients on thehighest levels could engage in certain behav-iors, such as smoking and shopping at local
stores, patients were highly motivated to per-form the behaviors necessary to earn theselevels.
It should also be noted that the highest priv-ilege levels approximated community living.For example, patients on the highest level wererequired to eat all of their meals off the unit,either in the hospital cafeteria (paid for by thehospital) or in a local restaurant. This combina-tion of linking personally meaningful rewardsto appropriate behaviors, and then fostering areduction in dependency on the treatment unitupon achievement of high privilege levels, com-bined to both motivate patients to behave incommunity-appropriate ways and give thempractice in functioning in the community.
Philosophy Toward Program Staff
It is rare to find a treatment program wherethe moment-to-moment interactions that occurthroughout the day between patients and staffare viewed as the most critical aspects of treat-ment. However, programs based on this ideahave been highly successful. For example, Pauland Lentz (1977) demonstrated that a programbased on operant and social-learning principles,applied during all waking hours by all staff,produced significantly better outcomes amonglong-term patients than other programs. In Pauland Lentz’s demonstration, every staff memberwas seen as an important facilitator of the pro-cess of change and was trained in the philoso-phy and treatment techniques of behavioraltreatment in general and of schizophrenia inparticular.
The Process Model of PsychiatricRehabilitation
Effective psychiatric rehabilitation involvesdirecting treatment toward four processes: skillacquisition, skill performance, generalization,and cognition (Corrigan & McCracken, 1997).Stated differently, an effective treatment pro-gram must include techniques to facilitate thelearning of new or lost skills, to motivate pa-tients to perform those behaviors throughout thetreatment environment, to promote skill perfor-mance in the real world, and to address thecognitive deficits that interfere with skill acqui-sition and performance. Consistent with this
148 SILVERSTEIN ET AL.

model, the Second Chance Program incorpo-rated interventions targeting each process.
Manualized skill training interventions are aneffective method for teaching specific commu-nity living skills. A number of effective skillstraining interventions have been developed andstandardized through the University of Califor-nia, Los Angeles (UCLA) Center for Psychiat-ric Rehabilitation (Liberman et al., 2005; Wal-lace et al., 2001). These therapies target specificskill areas, including grooming and hygiene,basic conversation skills, social problem solv-ing, friendship and dating, recreation and lei-sure activities, substance abuse prevention,medication and symptom management, andcommunity reentry.
Promoting performance of skills involvesmotivating patients to perform, outside of thegroup setting (i.e., in the program environment),what they are learning in the skills traininggroups. Incentive systems, such as token econ-omies and privileging systems, are designed toreward individuals for performing adaptiveskills both while in groups and while in thetreatment environment. An important compo-nent to promoting skills performance is to havestaff utilize appropriate prompting and feedbacktechniques (see below for specific techniques)throughout the day. This helps to reinforceadaptive behavior and thereby increase overallcoping skills.
Generalization often involves working withfamily members who will have contact with thepatient after discharge. Accordingly, wheneverthe patient is spending time off the unit (e.g., onpass with family, at local stores, at the hospitalcafeteria, or on an interview), he or she andaccompanying people should be encouraged topractice the socially appropriate and adaptivebehaviors that are taught, modeled, and prac-ticed in the treatment program.
Whereas skills deficits are associated withpoorer community functioning, cognitive defi-cits have been shown to limit the acquisition ofnew skills (Green, 1996). The cognitive deficitscommonly associated with schizophrenia in-clude impairment in attention, vigilance, verbalmemory, and executive functions such as theability to plan, sequence, initiate, and engage inproblem solving. These problems have only re-cently become the foci of treatment. Some treat-ments attempt to improve the cognitive deficits(Brenner et al., 1992, 1994; Spaulding, Flem-
ing, et al., 1999; Spaulding, Reed, et al., 1999),whereas others aim to provide patients withcompensatory strategies (Velligan & Bow-Thomas, 2000).
The Need to Focus on Multiple Levels ofTreatment
An effective psychiatric rehabilitation pro-gram can be conceptualized as simultaneouslyproviding treatment to the patient on three lev-els: (a) the program environment, or ward, lev-el; (b) the group therapy level; and (c) theindividual interaction level. The ward level maybe of primary importance within a behavioralprogram because structures such as the tokeneconomy and the programwide emphasis on thepromotion of adaptive behavior work synergis-tically to create a prosthetic environmentwherein the consequences of behavior are im-mediate and very clear to all patients. Becausepatients with schizophrenia are known to sufferfrom major cognitive deficits, this prostheticenvironment serves a necessary compensatorymechanism. For example, patients with impair-ment in executive functioning show a poor abil-ity to plan and organize behavior and havedifficulty anticipating the consequences of theirbehavior. However, while participating in theprogram, feedback about inappropriate or bi-zarre behaviors is given directly and consis-tently by trained staff along with helpfulprompts about how to behave in a more appro-priate or adaptive manner.
As mentioned earlier, group level interven-tions target skills acquisition and performancein various areas of independent living skills.Other group level interventions focus on relax-ation and stress reduction; anger management;healthy living skills, such as diet and exercise;and spirituality as a coping strategy. Ideally,skills training groups should be held at leastthree times per week, with no more than 8patients per group.
Intervention at the individual level is con-ducted through moment-to-moment interactionswith staff, individualized cognitive interven-tions, behavior contracts, and psychotherapy.Individually administered cognitive interven-tions can be effective in situations in whichpatient attention span precludes active engage-ment in, and benefit from, group-based methodsof cognitive treatment. Interventions have been
149TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

developed that target attention span (Massel,Corrigan, Liberman, & Milan, 1991; Silversteinet al., 2001) and overall cognitive functioning(Van der Gaag, 1992), in addition to those thathelp patients cope with delusions and halluci-nations (Hatashita-Wong & Silverstein, 2003;Spaulding et al., 1986). Behavior contracts areoften necessary when patients demonstrate be-haviors that are not changed sufficiently byother interventions. Behavior contracts can beviewed as individualized token economies. Fora behavior contract to be effective, it must beclearly understood by both the patient and staff,include incentives for the patient to behave dif-ferently, and follow behavioral guidelines.Guidelines for effective contracts are available(Heinssen, Levendusky, & Hunter, 1995), as aremethods for training staff in their development(Silverstein & Jewell, 2002).
Functional Analysis
Functional analysis involves determiningwhich antecedents and consequences are con-trolling behavior. Once this is known, a behav-ior plan can be developed to change these con-ditions in order to modify the target behavior.This general strategy is sometimes referred to as“the A-B-C model” with A, B, and C referringto antecedents, behaviors, and consequences.Each component of the A-B-C model is equallyimportant. For example, it is important to spe-cifically define the behavior being measured sothat all staff working with an individual canagree when it is or is not occurring. It is impor-tant to look at the consequences of the behaviorbecause this can reveal why it is performed. Forexample, on some inpatient units, patients donot get much attention from staff unless theybegin yelling or acting aggressively. Staff areoften surprised that, although there are rapidand severe consequences for aggressive behav-ior, a patient’s rate of aggression may still go upbecause the attention and contact from staff maybe experienced as pleasurable. In such cases,understanding that the attention is rewardingallows staff to set up plans to systematicallyreinforce appropriate behaviors and to avoidreinforcing inappropriate ones. It is equally im-portant to understand the circumstances inwhich a behavior is most likely to occur or whatantecedent events are associated with the onsetof the behavior. Understanding antecedents can
allow staff to teach patients new and more ap-propriate responses or ways to avoid situationsthat lead to inappropriate behavior.
Program Components
Patient barriers to discharge often involveinadequate living skills more than symptom lev-els. Therefore, a combination of milieu manage-ment, group skills training, and individualizedinterventions were implemented in the SecondChance Program to address patients’ behavioralexcesses and deficits. For a summary of pro-gram components, see Table 1.
The milieu management system involves apoint-based system for on- and off-ward privi-lege determination (described later). In addi-tion, the program uses a token economy, whichcan be thought of as a prosthetic environmentfor people with severe cognitive deficits. Withinthe token economy, feedback for appropriateand inappropriate behaviors is given moreclearly and frequently than in more typical en-vironments, and consequences, in terms of re-wards and penalties, are immediately linked tobehaviors. All of these specific interventionspromote learning. Patients earn tokens for meet-ing specific, individualized (based on their priorperformance) behavioral targets, which can beeither targets for the behaviors noted below, orseveral aspects of group behavior, including
Table 1Components of the Second Chance Program
Program components
Token economy (with token store)Point/level system (including programmed reduction in
reliance on program reinforcers)Weekly review of data on prior week’s behavior
frequenciesObservational ratings of multiple classes of behaviorFunctional assessmentMultimodal Functional Model assessments and treatment
planningMedication education groupSkills training groups (with and without attention
shaping)Cognitive rehabilitation (group and individual)Recreational activitiesBehavior contractsStaff behaviors: Positive reinforcement, extinction, three-
step procedure, differential reinforcementTime-out
150 SILVERSTEIN ET AL.

arriving on time, participating, and staying forthe entire group. The Second Chance Programhas a token store, open 6 days/week, at whichpatients can either deposit coupons for later use(using a computerized token store banking sys-tem) or spend them on items including food,personal grooming products, clothes, maga-zines, and games. Adding the token system ontothe point system ensured that even lower func-tioning patients, who were too impaired to beable to achieve the highest privilege levels,would be motivated to meet their behavioraltargets. An important feature of the token econ-omy system is that, as patients progress throughthe system and their behavior begins to ap-proach community standards, external reinforc-ers are used less and social and internal controlsare relied upon more. At first, patients receivetokens and praise as they meet each target be-havior. Later, reward is in the form of praise andsocial reinforcement from staff and self-satis-faction with meeting targets. Reinforcement ofdesirable behavior also moves over time fromimmediate to delayed reinforcement. As pa-tients achieve higher levels in the system, theyno longer receive tokens immediately on com-pletion of a target behavior. Rather, at the end ofthe week, they receive credits at the token store,with the number of credits being equivalent tothe number of tokens they would have earnedon a daily basis during the past week (like apaycheck). Thus, later stages of the system ap-proximate experiences that they will encounterin the community (i.e., delayed reinforcement).An additional feature is that the system isweighted heavily toward reinforcing positivebehaviors as opposed to penalizing inappropri-ate behaviors, an approach that has been shownto be more successful than systems based pri-marily on penalties.
The point and token systems are based on acomprehensive assessment system that includesthe following: (a) daily ratings on 10 aspects ofappearance and grooming (e.g., hair clean, haircombed, wearing different clothes than yester-day); (b) daily ratings on 10 aspects of roomcleanliness (e.g., no clothes on floor, bed made);(c) daily ratings on 10 meal behavior criteria(e.g., eating with utensils, not taking other peo-ple’s food), rated at every meal; and (d) dailyratings on 10 aspects of preparation for sleep(e.g., not sleeping in clothes worn during theday, pillowcase on pillow). Patients receive
points for successful completion of each crite-rion and extra points and a token if they reachthe target that staff set for them on the basis oftheir performance during the prior 2 weeks(note that if a target is met consistently for 2weeks, it is raised by 1 point for the followingweek; if it is missed for 2 weeks, it is loweredby 1 point). Performance relative to these crite-ria is recorded on specialized behavior check-lists (see below).
In addition, patients are rated on the pres-ence/absence of approximately 30 different in-appropriate and appropriate behaviors as theyoccur throughout each day. At the end of eachweek, the total number of points earned and lostis totaled, and the resulting number determinestheir level of on-ward and off-ward privilegesfor the next 7 days. All of these data are enteredinto a software application developed by StevenM. Silverstein. The output, given to each patientand all staff each week, includes frequencycounts of each behavior during the week thatjust ended. Customized reports and graphs, de-picting data over user-specified time intervals,can also be easily created from within this pro-gram using preexisting macros. These data areuseful for treatment planning and for informingpatients about progress in the program and be-haviors that need further change.
In addition to the milieu management sys-tems, the Second Chance Program offers a fullrange of skills training and recreational groups,including all of the groups in the UCLA Socialand Independent Living Skills series. All ofthese groups operate to reinforce attentivenessand participation during group sessions (see de-scription of attention-shaping procedures laterin this article), in addition to promoting learningof the specific group content area. Becausesome patients have specific problem areas thatare not addressed sufficiently by milieu or groupinterventions, individualized behavior contractsand cognitive rehabilitation strategies are usedwhen necessary (see below for examples).
Specific Procedures to Promote BehaviorChange
This section covers a number of procedures,including the following: observational rating ofcritical behaviors; linkage of privilege levelwith performance level of behaviors; the tokeneconomy; staff–patient interaction; techniques
151TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

to promote therapy engagement, behavior con-tracting; and designing individualized cognitionenhancing interventions. These procedures bor-row heavily from the pioneering work of Pauland Lentz (1977), Menditto et al. (1994), Spaul-ding et al. (1986; Spaulding & Sullivan, 1992),and Liberman (Corrigan & Liberman, 1994;Liberman, 1992).
Observational rating of critical behavior.Every successful rehabilitation program forschizophrenia patients provides frequent feed-back to patients and staff regarding behavior.For this to occur, formal procedures for datacollection and reporting need to be instituted.On the basis of the work of Paul and Lentz(1977) and of Menditto, Valdes, and Beck(1994), we developed behavior checklists forstaff to use when observing and rating behaviorsthat are critical for community success. Thenumber and specific type of daily behavioralchecklists to be completed by staff can be cus-tomized to the needs of any program. However,it is important that the behaviors chosen forobservation and rehabilitation correspond towhat is known about the needs of chronicschizophrenia patients and not simply to thosebehaviors that staff may find aversive (Paul etal., 1997). Ideally, behaviors are chosen as aresult of a combination of existing data on pa-tient disabilities, as well as staff observationsabout behaviors that represent barriers tomore effective functioning in the program. Itis then important that staff work together withthe program leader to develop user-friendlyinstruments for recording data and systemsfor data management and reporting (Corrigan& McCracken, 1997; Silverstein, Bowman, &McHugh, 1997). Behavioral checklists shouldclearly list the behavioral criteria, individualclient names, and their identified behavioraltargets.
Observational Assessment Using BehaviorChecklists
Appearance. Each morning at 8:30, eachtreatment team coordinator meets with his/her 10 patients in a group setting. One of thecritical functions of this group is to reviewpatient grooming and hygiene. Using the Ap-pearance checklist, each patient’s performanceis reviewed one at a time. Each patient is askedto stand and is then asked about each of the 10
criteria. The group leader and other staff presentpraise the patient for each criterion that is metand remind the patient that for each criterionthat is not met, they will lose a point toward thepossible 10 points they could earn for the morn-ing appearance check. Once this procedure hasbeen established with a group, it can be usefulfor patients to rate other patients. This promotesattention skills in the patient doing the ratingand a greater sense of group cohesion amongthe group as a whole. The final score for eachday of the week is listed on a chart on an easel.On this chart, patient names are in the leftmostcolumn, followed by their target, and followedfurther by spaces for each day of the week.These spaces are filled in each morning. Inaddition, a staff member at the meeting com-pletes the Appearance checklist, and the datafrom this form are entered into the patient datatracking program. Patients receive tokens formeeting their appearance targets, as well as forgroup behaviors (e.g., participation for the du-ration of the group).
Room and area. While patients are in the8:30 a.m. meeting, a designated nursing staffmember goes to each patient’s room and com-pletes the Room and Area checklist. Near theend of the 8:30 meeting, this staff memberattends each of the three groups to review pa-tient completion of the room and area criteria.Patients are informed which criteria they met,and which they did not, and reminded that ifthey complete the latter tomorrow, they can getmore points towards their privilege level for thefollowing week. Data recording procedures arethe same as for the appearance check. Again,patients receive tokens in addition to extrapoints for meeting their target level.
Meals. Patients who earn the highest privi-lege level are required to eat each of their mealsoff the unit in the hospital cafeteria, as part ofthe movement toward increased approximationof community demands as patients progressthrough the program. For the patients eating onthe unit, however, behaviors during mealtimesare recorded on the Meal Behaviors checklist.Patients receive feedback during meals regard-ing which criteria are being met and which arenot. For those patients who demonstrate unac-ceptable meal behaviors, coaching and model-ing of appropriate meal behaviors are providedby staff assigned to eat their meals with the unitclients.
152 SILVERSTEIN ET AL.

Evening appearance check. The EveningAppearance checklist allows staff to rate a num-ber of behaviors associated with personal ap-pearance and room cleanliness at the end of theday. This helps ensure that patients remain wellgroomed throughout the day and that theirrooms remain clean. Specific problems that thischecklist was designed to reduce include chang-ing into inappropriate types or amounts of cloth-ing after the morning appearance check, sleep-ing at night in clothes worn during the day, andsleeping without pillowcases or sheets. Patientsare given feedback individually as their room ischecked before bedtime.
Socially inappropriate behaviors. In addi-tion to checklists that are completed at specifictimes of the day, occurrences of inappropriatebehaviors are recorded throughout the day asthey occur, using event sampling procedures, onthe Socially Inappropriate Behaviors checklist.Behaviors recorded on this checklist includefailure to wake up on time, verbal and physicalabuse, sexually inappropriate behavior, bizarrebehavior, and treatment noncompliance. Allstaff are responsible for recording inappropriatebehaviors. Patients lose points for acting in so-cially inappropriate ways, with the amount ofpenalty points for the different behaviorsweighted according to dangerousness or sever-ity. Staff are required to place their initials nextto their mark on the checklist in case furtherclarification is needed at a later date. However,before recording an incident on this checklist,staff are required to identify the behavior to thepatient, tell them the consequence in terms ofpoints lost, and suggest a more appropriatemeans of getting their needs met.
Socially appropriate behaviors. It is criticalboth that patients receive feedback about appro-priate behavior on a frequent basis and that staffare trained to consistently do this. To accom-plish these goals, the program also uses a check-list for socially appropriate behaviors. Behav-iors coded on this sheet include the following:starting a conversation appropriately; keeping aconversation going by asking questions or gen-erating new topics; ending a conversation ap-propriately; responding appropriately to a state-ment that another person has to end the conver-sation now; tolerating a stressful situationwithout engaging in inappropriate behaviors;providing assistance to another person, etc. It ispart of the program philosophy that more feed-
back should be given to patients about appro-priate behaviors than about inappropriate be-haviors. Therefore, program leaders routinelynote the number of behaviors coded on eachsheet and work with staff continually to ensurethat staff are “catching” patients engaging inpositive behavior. As with the Socially Inappro-priate Behaviors checklist, staff are required togive feedback to a patient if they record a be-havior on the sheet.
Group worksheets. Behavioral observationoccurs in treatment groups as well, alongsidepresentation of the material being taught to pa-tients. Patients receive points for arriving ontime, for participating, and for staying for theentire group. Patients also receive tokens formeeting each of these goals. Participation isdefined for each group member in each groupby the group leader. This is because obstacles tomeaningful participation vary across patients.For example, one patient might need to interruptless, whereas another patient might need todemonstrate more spontaneous speech. Thesedata are recorded on group worksheets designedjust for observation in group therapies.
Feedback to patients. Data from the behav-ior checklists are entered into the data trackingprogram by a secretary. Each Tuesday, the pro-gram produces reports of the frequencies ofeach behavior over the prior 7 days. All reportsare given to all staff, and each patient is givenhis/her individual report the next day at the 8:30meeting. These reports serve a number of pur-poses in addition to informing staff of patientfunctioning in important areas. For example,they convey the message to patients that theyare responsible for the privileges that they earn.In this way, patients are discouraged from ap-proaching staff to beg or negotiate for a higherprivilege level, which is a form of dependentand institutionalized behavior, in part fosteredby programs in which staff/program conse-quences for patient behaviors are unpredictableand vary between one staff member and an-other. When questions come up about levels,staff can review the report with the patient andstress the point that control of privilege level isin the hands of the patient. Having the reportallows staff to highlight to patients how theyhave improved week to week and/or to point outwhy a level was dropped and what needs to bedone in the next 7 days to regain lost privileges.
153TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

Interpersonal Techniques for OptimizingPositive Outcomes
Perhaps the most critical aspect of treatmentin a rehabilitation program is the moment-to-moment interactions between staff and patientsthroughout the day. Indeed, recent data suggestthat the number of positive staff statements topatients is a strong predictor of community ten-ure after hospital discharge among people withserious mental illness (Coleman & Paul, 2001).The number of such interactions that occur, orthe potential number that could occur (since thenumber is typically less than optimal; Paul &Lentz, 1977), can be used to provide much morefeedback and support than any combination ofgroups or other experiences patients typicallyreceive while inpatients. Unfortunately, how-ever, it is rare to see a discussion of how staff–patient interactions can be optimized to promotesuccessful treatment outcome. Therefore, be-low, we provide information about interactivetechniques that we have found to be particularlyuseful in facilitating positive rehabilitation out-comes. We begin the discussion by focusing ongeneral guidelines for staff behavior. This isfollowed by a discussion of specific promptingand intervention techniques.
Guidelines for Staff Behavior in theProgram Environment
Reinforce only appropriate behavior. Staffneed to always reinforce desirable and appro-priate behaviors immediately. Participantsshould receive verbal praise and tokens/pointswhenever they have demonstrated full partici-pation or have met a behavioral target duringactivities, groups, tasks, or other informal inter-actions with staff. If unsuccessful or inappropri-ate behaviors occur, staff should specify to theclient the reason why a point or token was notearned, and they should be sure to follow thisexplanation with a prompt for the client’s nextopportunity to earn his or her token.
Use the method of shaping. When patientsare not yet functioning at a level of performancethat meets their target criterion, staff shouldreinforce approximations of the desired behav-ior. The approximations should be specificallydefined in treatment planning meetings so thatstaff from all disciplines are able to consistentlyfocus on the appropriate performance criteria.
Similar to the targets for behavior checklists,these performance criteria are systematically in-creased as clients successfully meet or exceedthe targets assigned to them.
Feedback should be specific. Wheneverpoints and tokens are given, staff should alwaysspecify for which behavior or criterion the in-dividual has earned the praise, points, and/ortoken. An example is “You did a really good jobof setting your sheets and straightening yourpillow on the bed. You earned 10 points andmet your Room Check target this morning.Keep up the good work.” Whenever possible,point awards, praise, and tokens should be givenin the presence of other patients. This increasesthe effects of the social reinforcement and pro-vides examples of appropriate behaviors by peermodels for the others.
Do not reinforce failures. It can be difficultfor staff not to give attention to a patient whenhe/she is failing something. However, this onlyreinforces the behavior of failing. Occasionally,it is appropriate to make conversation with aresident who is failing something, but this istypically in structured groups/activities andtakes the form of a prompt sequence (see Thethree-step technique below).
Reinforce exemplar behaviors. Any exem-plar, helping, and model behaviors should bepraised and acknowledged with positive verbaland nonverbal reinforcement. Extra tokens canbe given for behaviors that are not already re-inforced by other means (e.g., not on the behav-ioral checklists or not an aspect of group par-ticipation target). Examples of socially appro-priate behaviors include cooperative behaviorswith other patients and a variety of chores andsmall jobs that staff can think of or that thepatient volunteers to do.
Interactive Techniques for ManagingInappropriate Patient Requests andBehaviors
This section describes several techniques fordealing with inappropriate behavior during one-on-one interactions with patients.
Extinction. Staff should ignore a patientwhen he/she is talking in ways that do not makesense, demanding something that staff cannotdeliver, asking questions that have been askedseveral times already, and so forth. If a patientis mixing appropriate talk or appropriate behav-
154 SILVERSTEIN ET AL.

ior with inappropriate talk/behavior, staff shouldrespond only to the reality-based speech (i.e.,the technique of differential reinforcement).Undesirable behavior should be ignored unlessit would result in an infraction on the Inappro-priate Behaviors checklist. In this case, staffshould prompt the patient using the three-steptechnique described below. When extinction isto be used as a staff response to specific behav-iors, it is important that all staff are informedand follow through with the procedure. Theeffect of having even one staff member respondto the behavior creates an intermittent reinforce-ment schedule, which will make the behavioreven more difficult to reduce in frequency.
The three-step technique. The three-steptechnique is a sequence of prompts that shouldbe used when the target behavior requires morethan the use of extinction to reduce. This tech-nique also assists the patient in identifying al-ternatives to the inappropriate behavior. It con-sists of the following sequence of steps.
1. Reflect feelings/intentions. After the pa-tient’s request, start out with a statement, inmatter-of-fact terms, regarding what the patientis feeling (e.g., “I can see you want me to helpyou right now”; or “I can see you feel angryright now”). Doing this can help make peoplefeel “listened to” and can counteract preexistingnegative feelings.
2. State the limits of the situation. The formof this statement should be as follows: “[Thebehavior you’re engaging in] is inappropriate,and when people here do that, [this] happens.”Staff are instructed not to use the words you orI in these cases (e.g., “I’m going to drop you alevel,” or “When you do that points are takenaway from you.”). More appropriate staff com-ments would be “When a person does that onthis unit, they are not able to earn certain priv-ileges.” By depersonalizing the interaction, staffreduce the chance of aggressive behavior beingdirected at them and promote generalization ofappropriate behavior beyond the current context.
3. Prompt the patient to use alternative be-haviors. Typically, when a patient is actinginappropriately, he/she is trying to get some-thing but is doing the wrong thing to get it.Therefore, for the third part of the three-steptechnique, point out what the patient could do toget what he/she wants. Patients with chronicpsychotic disorders may have difficulty gener-ating alternatives or thinking into the future. As
a result, staff should help patients generate andname alternatives to their inappropriate behav-ior when patients cannot do this on their own.
It is important that staff practice the three-step technique often. Staff typically report thatit feels unnatural, awkward, and difficult at first.The program director must remind staff thatthese feelings are typical when learning newskills. Another common difficulty comes withdelivery of the three-step sequence in an un-emotional tone of voice. When the patient’sfeelings are acknowledged and reality is statedin a matter-of-fact way, the patient then expe-riences the situation as a struggle with reality,instead of as a struggle with staff. This pro-motes directing problem-solving activities to-ward their own behavior and environment, asopposed to simply trying to get staff to changethings.
Time-out. Time-out involves removing thepatient from all sources of reinforcement. Dur-ing the time-out, the patient cannot receive so-cial attention from staff or peers and does nothave access to other items that are reinforcing,such as food, TV, radio, and magazines. Thisprocedure has been researched extensively, andresults demonstrate its effectiveness in eliminat-ing many inappropriate behaviors such as ag-gression, stealing, self-injury, and so forth.
Time-out can be used to de-escalate and man-age agitation. However, staff should alwaysmake efforts to avoid the need for time-out.This means that staffers need to be alert to anypatient escalation and, whenever possible, useother interventions (e.g., encouragement, prompt-ing, redirection) to guide the patient’s behaviorin a more appropriate direction prior to theoccurrence of any more serious infractions.
When other interventions fail and time-out isneeded, the following steps should be taken:
1. Identify for the patient, the behavior theyhave engaged in that is resulting in a time-out.
2. Tell them what the consequences are forthat behavior (i.e., time-out and a mark off forthe behavior on the Socially Inappropriate Be-havior checklist, with an associated point losstoward next week’s level).
3. Tell them how and when they will com-plete the time-out.
Staff should be straightforward and matter-of-fact but not cold or harsh. In addition, staffshould not discuss or debate anything with thepatient. Patients should be instructed to go to
155TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

the designated time-out area, and staff shouldignore all attempts to engage them in a discus-sion about the incident leading to the time-out.About 5–10 min is generally an adequateamount of time for a time-out. Patient rooms areundesirable as time-out areas because there aretoo many personal items that may serve as asource of reinforcement.
It is helpful if patients for whom time-outsmight be necessary are identified early in treat-ment, before an actual time-out is required. Ifthis is done, then the details of the time-out forthe patient can be worked out in advance, in-cluding having certain details contributed by thepatient in the form of an advance directive.These details include the behaviors that willlead to staff indicating that a time-out is neces-sary, the place where the time-out will takeplace, and the duration of the time-out.
Occasionally, a patient will refuse to begin atime-out. In such cases, staff should avoid ar-guing with the patient. At first, the patientshould be reminded that all privileges will bewithheld until the time-out is completed. Afterthat, if the patient continues to argue, he/sheshould simply be told “The time out will beginwhen you are in your time-out place.” If apatient leaves a time-out before the allottedtime, he/she should begin the period over.
It is important that all staff stick to theseguidelines and use the techniques describedabove. If, for example, most staff are using theextinction, three-step prompt, and time-out pro-cedures correctly, but 1–2 staff members decidethat they “don’t have the energy” and give in toinappropriate requests, then intermittent rein-forcement has occurred, making the behavioreven more difficult to reduce in the future.
Behavior Contracting
Behavior contracts are an effective and col-laborative approach to treating people withschizophrenia (Heinssen, Levendusky, & Hunter,1995; Levendusky et al., 1983, 1994), and tech-niques are available to train staff in their devel-opment (Jewell, Silverstein, & Stewart, 2001).Behavior contracts can be critical because it isoften the case that a patient has a specific trou-bling behavior that is not addressed adequately(if at all) by manualized treatments such asskills training groups. Procedures for develop-ing behavior contracts include a number of tech-
niques, such as functional analysis, incentivesystems, and appropriate use of prompting andshaping. It is important that patients be involvedin the development of their contract and thatthey understand it. Several key principles areinvolved in developing and using behavior con-tracts. One is that a series of contracts is typi-cally required. As a result, it is important thatthe initial contract be focused on a behavior forwhich there is a high likelihood of success inachieving change. This behavior may not be thebehavior that staff believes is most troublesomefor them. However, the positive behavioral mo-mentum created by initial success will facilitatelater efforts to modify more challenging behav-iors. A second principle is that a system tocollect reliable and valid data should be put inplace as part of the contract, if it does notalready exist as part of the general treatmentprogram structure. Having these data will allowfor rational discussions between the patient andstaff members about progress toward contractgoals and what changes are required, both in thecontract and in the patient’s behavior. Third, acontract should typically not be in place formore than 2 weeks. Patients and staff often losemomentum as contracts extend past this time.To prevent this, contracts should be updatedevery 1–2 weeks, on the basis of data and otherfeasibility issues. This keeps patient and staffmotivation at maximal levels and also allowsfor the shaping of behavior to occur. Fourth, thecontract should clearly define the target behav-ior and the staff response. It should not besimply one or more statements that the patientwill perform some behavior, along with a linefor a signature. It is often useful to have sepa-rate columns for patient and staff behavior. Forexample, a line under “patient behavior” mightsay, “If I arrive at breakfast by 7:30 a.m.,then. . . ,” and a line under the “staff behavior”column might say, “Staff will praise me forcoming on time and allow me 1 hour of TVwatching time in the afternoon.” Finally, a con-tract should typically not focus on more thantwo to three behaviors at any given time. It isimportant to have a long-term perspective onbehavior change and to use the method of shap-ing, rather than expecting that a single behaviorcontract can eliminate multiple inappropriatebehaviors immediately.
An example of a successful behavior contracton the Second Chance Program involved a
156 SILVERSTEIN ET AL.

young female patient in her early 20s who hada psychotic disorder. After admission to theunit, she would frequently swallow, or claim toswallow, dangerous objects such as jewelry,pencil points, erasers, marbles, and so forth.This would lead to long periods of seclusion orto being observed by a staff member while inher room. Functional analysis of this patient’sbehavior elucidated three important situations:(a) her reports of swallowing objects (whichX-rays later revealed to be false) occurred dur-ing times when she was not receiving attentionfrom staff (e.g., after all groups had ended forthe day) or after another patient received a greatdeal of staff attention, whether it was praise ora seclusion/restraint incident after a dangerousbehavior; (b) when in seclusion or being ob-served by certain nursing staff or mental healthworkers, these staff would hold long conversa-tions with the patient, including during hermeals; and (c) when engaging in appropriatebehavior (e.g., watching television, reading),staff rarely interacted with the patient. The hy-pothesis was generated that the patient’s behav-ior was a method to receive attention from staffand that this was being reinforced by her receiv-ing intense 1:1 attention from staff after report-ing a behavior that would lead to seclusion orroom restriction. Therefore, a behavior plan wasset up that required staff to heavily reinforce thepatient with verbal praise and special couponseach time they observed her engaging in a pre-specified set of appropriate behaviors. A systemwas set up wherein these coupons could becashed in for time spent on special activities thatthe patient liked (5 coupons was worth 1 hr ofpainting with materials to be provided bystaff, 20 coupons earned 1:1 time with a staffmember, etc.). In addition, staff were to haveonly the minimal amount of verbal contact re-quired with the patient during seclusion andrestraint incidents. The goal of this plan was toincrease the frequency of socially appropriatebehaviors and extinguish the inappropriatemethods of seeking staff attention. Ultimately,it was hoped that, after successive contracts inwhich reinforcement was made more intermit-tent, the patient would be internally motivatedto engage in socially appropriate behaviors as aresult of their intrinsically motivating qualities.This behavior contract led to a significant re-duction in dangerous and socially inappropriatebehaviors. In the 3 weeks prior to the introduc-
tion of the plan, the patient averaged 9.7 seclu-sion room incidents per week. After the plan,this average was 0.71 over the next 7 weeks,with all of these incidents coming after a staffmember inappropriately reinforced a sociallyinappropriate behavior.
Interventions for Cognitive Impairment
It is now generally accepted that mostschizophrenia patients experience cognitivedifficulties and that the presence of severecognitive deficits interferes with the ability toengage in psychosocial treatment, leading topoorer outcomes (Green, 1996; Silverstein,Schenkel, et al., 1998). Although a number ofcognitive rehabilitation interventions havebeen developed for schizophrenia, their ef-fects in most cases have been minimal (al-though see Bell et al., 2003, for an exception),and, to date, none of the techniques havedemonstrated efficacy with the most cogni-tively impaired patients (Silverstein & Wilkniss,2004). Although the treatment techniques de-scribed earlier help to create a simplified envi-ronment in which positive and negative conse-quences of behavior are more immediate andfrequent than normal, it is still the case thatpatients with severe cognitive impairments maybenefit less than other patients. Therefore, it iscritical that, for cognitively impaired patients, amajor focus of treatment involve improvingtheir ability to attend to information that ispresented to them and to actively participate intreatment.
Below, we discuss several techniques that weand others have found useful in accomplishingthis goal with this population. It is important tonote that patients may be inattentive for differ-ent reasons, including a sustained attention def-icit, poor motivation, sedation due to medica-tion, or distractibility due to hallucinations ordisturbing thoughts. In the following discus-sion, we focus on treating inattentiveness,whether it is due to primary or secondary neg-ative or positive symptoms.
Procedures for Improving Attentivenessand Participation in Groups
For severely disabled patients with very shortattention spans, techniques based on the behav-
157TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

ioral principle of shaping have demonstratedeffectiveness in increasing attentiveness andpromoting the learning of new skills. Shaping isthe application of several fundamental tech-niques of learning to bring about new behavioror to modify a certain aspect of an existingbehavior. As such, shaping can be viewed as amethod to achieve operant conditioning, withattention being the response that is targeted. Theprimary technique involved is differential rein-forcement of successive approximations. Ratherthan waiting for the complete behavior (e.g., a20-min attention span) to occur before offeringreinforcement, reinforcement is provided forsuccessive approximations or steps toward thefinal behavior. When the initial step toward abehavior (e.g., 4 min of continuous attention)has been reinforced and occurs fairly regularly,the criterion for reinforcement is advanced tothe next step (e.g., 5 min of continuous atten-tion). This sequence of reinforcing, changingcriteria for reinforcement, fading reinforcers forprevious versions of the behavior and limitingreinforcers to behavior meeting the new crite-rion, is then repeated until the behavior resem-bles the final desired response. A strength ofshaping is, therefore, that it allows for specificlearning techniques to be used in order to de-velop and strengthen behavior that does notnormally occur or that occurs at a very lowfrequency. It is this feature that makes it suit-able for the treatment of patients whose severelyimpaired attention spans preclude them fromactive participation in other forms of psychos-ocial treatment, including many forms of neu-rocognitive remediation.
Three forms of attention-shaping training aredescribed below. The first procedure involvespatients working separately. The last two pro-cedures described involve integrating attentionshaping into an existing skills group format.
Shaping duration of classroom work. Usingassignments consisting of paper-and-penciltasks focusing on practical language and math-ematics skills, we can integrate attention-shap-ing procedures into a classroom environment.Classes should be held frequently, for instance,three times daily during weekdays. Target timesfor on-task behavior are initially quite brief(30–60 s), and two to three trials are typicallyrequired per session, meaning that the durationof the class time increases as participants in-crease the duration of their on-task behavior.
Two staff members are needed for this interven-tion. One leads the class. The second staff mem-ber, or change agent, focuses on patient atten-tiveness. Patients receive prompting and en-couragement as necessary throughout thesession, and on successful completion of eachtrial, they receive specific verbal praise, a shap-ing chip (see below), a small food snack, and aprompt specifying the requirements for the nexttrial—all from the change agent. After success-ful completion of the last trial, a participationtoken is awarded. Tokens can be used to “pur-chase” a variety of goods or privileges (e.g.,snacks, coffee, grounds passes, TV time) fromthe ward token store. As the training partici-pants demonstrate success with each target forseveral sessions, targets are gradually increased,typically in 30- to 60-s increments, until theparticipant consistently completes two consec-utive 10-min trials.
Menditto et al. (1991) used this shaping pro-cedure to increase the attention span of 7 foren-sic inpatients with severe and persistent schizo-phrenia or schizoaffective disorder. The averagelength of stay for these patients was 10.4 years,and they were considered to be among the mostill and least responsive patients in the hospital.After 12 months of training, 6 of the 7 patientshad demonstrated substantial improvements inattentional functioning, with 4 of these gradu-ating from the attention-shaping classes andprogressing to more traditional academicclasses on the ward. They continued to performquite well in those classes, with a 1-year fol-low-up showing successful completion of aca-demic class assignments, on average, 84% ofthe time. Similar results were reported by Belluset al. (1998), using procedures identical to thoseof Menditto et al. (1991), and by Silverstein,Pierce, et al. (1998).
Integrating shaping and skills training pro-cedures—Technique 1. Silverstein et al. (1999)identified inattentive behaviors characteristic ofeach patient and then used shaping techniquesto improve these behaviors and facilitate acqui-sition of new knowledge and skills during groupsessions. The following steps are used in thisprocedure:
1. Baseline sampling: The most problematicverbal or nonverbal inattentive behavior is iden-tified for each patient. Nonverbal behaviors(e.g., eyes open, head up, eye contact withspeaker) are rated each minute using interval-
158 SILVERSTEIN ET AL.

sampling procedures, and verbal behaviors(e.g., responding within 5 s, making spontane-ous relevant comments, making irrelevant com-ments) are rated using event-sampling proce-dures. One or two noninteractive observersrecord the individualized target behaviors andreport their frequency at 15-min intervals, whenthe group leader pauses to allow this feedbackto be reported. In the Silverstein et al. (1999)study, patient goals initially reflected an averageof 4 weeks baseline, pre-shaping performance.
2. Introducing the shaping intervention: Afterinitiation of shaping procedures, at each 15-minreview period, patients who meet or exceedtheir goal (e.g., 60% of that period with theirhead up) receive a shaping chip. Patients turn intheir shaping chips at the end of the groupsession and receive a token or some other in-centive (e.g., 25 cents) for each shaping chipearned.
3. As patients begin to exceed their goalsconsistently, the criteria are increased to facili-tate continued progress.
Silverstein et al. (1999) demonstrated the ef-fectiveness of this integrated shaping-skillstraining approach. All participants demon-strated significant increases in attentive behav-ior using this procedure. Additionally, theyshowed that the method of intervention can betailored to meet individual needs. One individ-ual did not respond initially to the 15-min rein-forcement schedule; therefore, the shaping pro-cedure was adjusted to accommodate his severelevel of attention deficit. A continuous rein-forcement schedule was implemented whereinhe was given 5 cents and a piece of candy eachtime he opened his eyes. This eventually led toincreases from 10% to over 80% of the time inkeeping his eyes open, with subsequent greaterspontaneity and participation, as well as re-sponses that were more relevant to the group.
Integrating shaping and skills training pro-cedures—Technique 2. This technique sets thesame criteria for each patient (see Table 2 forcriteria) but varies the attentiveness durationrequired to earn shaping chips. This type ofgroup can be run with as few as two staffmembers: one to serve as the group leader andanother to serve as the change agent. The latteris the person who observes patient attentive-ness, uses verbal prompts and praise, and deliv-ers shaping chips when subtargets are met. This
person does not serve as a co-therapist for thegroup.
In this type of group, the change agent rein-forces each patient with verbal praise and ashaping chip each time a subtarget (e.g., 4 minof continuous attention) is met. When a shapingchip is given, patients are reminded of the sub-target they just achieved. When a patient meetsa class target (i.e., required number of subtar-gets for the session), he/she is explicitly praisedfor this as well. Whenever a patient meets eithera subtarget or a class target, this should be notedon the board or easel (by the therapist or co-therapist or change agent). This provides bothauditory and visual reminders of the patient’ssuccess. It is understood that this reinforcementby the change agent may briefly interrupt thegroup, although with experience, disruption isnegligible.
Whereas shaping chips are distributed duringclass upon meeting subtarget criteria, tokens aredistributed at the end of the group only. Whentokens are distributed, they are handed to pa-tients by the therapist or co-therapist, and thereason for earning the token is briefly reviewed
Table 2Criteria for Attentive and Inattentive Behaviors inIntegrated Attention Shaping and Skills TrainingGroups
Criteria behavior
Paying attentionHead upEyes openLooking at therapist/video/role-play
ParticipatingResponds to questions, requests, instructions within 5
secondsResponses are relevant (i.e., on topic)Responses consist of more than one or two words
when indicatedParticipates in role-playsMakes spontaneous commentsAnswers questions when trainer addresses whole
groupNot paying attention
Talking out loud or to selfMaking irrelevant commentsMaking irrelevant gesturesGesturing not in response to anyone in the roomArguing, yelling, screaming, etc.Staring off into spaceGetting out of chairLeaving group without permission
159TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

within the context of verbal praise. Further-more, the patient should be informed of thelevel of participation required to earn a token inthe next class.
If a token is not earned, therapists shouldnevertheless praise patients for something pos-itive about their performance in class that day.They should also clarify why the patients didnot earn a token for the class. The therapistshould then remind patients when the next classmeets and tell them that they will have anotherchance to improve their attention span and toearn a token in that class.
Subtargets are systematically increased aftertwo consecutive successful classes at the currentlevel and decreased after two consecutive fail-ures to achieve tokens at the current level. Thetypical schedule of subtargets is 30 s, 1 min, 2min, and so on, up to 10 min. Patients who canattend for 10 consecutive min are then shaped todo this twice, three times, and then four or moretimes during the group session.
When subjects engage in participation-inter-fering behavior, group leaders should give anegative prompt followed by a positive prompt(see example at the end of this paragraph).Continued participation-interfering behaviorshould be ignored, unless it is so disruptive thatit significantly impairs the ability of others tocontinue to participate, in which case the indi-vidual must be asked to leave the group. Whenthe behavior is corrected and the individual getsback on task, verbal praise should be given.This sequence can be repeated but only after theindividual resumes appropriate participation.All prompts should include specification of be-haviors and reference to the reinforcer forachieving class targets—for example: “Bob,you are talking out loud about stuff not relatedto our discussion. If you continue to do that, youwon’t be able to earn your participation token.If you can get back involved with our discus-sion, you’ll still be able to earn that token.”
Initial data from the use of this techniquehave been positive, with large effect sizes (Sil-verstein et al., 2005). Current efforts to refine itfurther include having patients participate in thegeneration of their own goals, as opposed tobasing them solely on performance in the pre-vious two groups. This technique will involvebroadening the range of behavioral targets fromduration of attentiveness to a range of behaviorsinvolved in attending and participating mean-
ingfully in tasks and groups. This collaborativemethod has been reported to be effective inshaping behavior among outpatients withschizophrenia (Skinner, Skinner, & Armstrong,2000).
Response to Requests (RTRs)
RTR procedures1 are used for patients withthe most severe disabilities and are used beforeestablishing time targets (e.g., before typicalshaping procedures). The idea behind RTRs isto elicit responses in typically unresponsive pa-tients. Patients are asked to engage in a simplebehavior. Typically, in therapy groups, thesebehaviors involve the demonstration of a basicsocial response (e.g., repeating a phrase, repeat-ing a phrase while keeping eyes open, lookingup at the group leader for 3 s). Goals are ini-tially set low (e.g., one or two instances of thedesired behavior) and are gradually increased(e.g., to five consecutive successful RTRs). Inmost cases, the change agent will prompt thepatient for the RTR while the group leader isconducting the group (but the group leader canalso initiate an RTR). When the therapist be-lieves that the patient is sufficiently responsivethat he/she could maintain on-task behavior forat least 30 s in a group setting using shapingprocedures, then the patient no longer has goalsframed in terms of RTRs; rather, he/she beginshaving time interval goals.
Individualized Cognitive Interventions
Some patients have cognitive difficulties thatare best addressed in an individual setting. Of-ten, the intervention must be designed specifi-cally for that patient because the nature of theproblem is such that it is not addressed bycurrently available treatments. For example, acommon problem in schizophrenia is distracti-bility secondary to persistent auditory halluci-nations. For patients with this problem, we havehad success using a modified dichotic listeningprocedure to enable patients to practice, andeventually master, the ability to disattend toirrelevant information. This has been reported
1 We thank Anthony Menditto for introducing us to theRTR technique, which is based on the earlier work of Pauland Lentz (1977).
160 SILVERSTEIN ET AL.

to reduce distractibility from hallucinations andto improve the ability to focus on relevant tasks(Hatashita-Wong & Silverstein, 2003; Spauld-ing et al., 1986). A second example of an indi-vidualized cognitive intervention involves theuse of Thematic Apperception Test (TAT) cardswithin the context of providing reinforcementfor increasing the frequency of stories generatedto stimulus cards, over several weeks of treat-ment (Murray, 1943; Spaulding, 1986). Thistechnique has been reported to reduce cognitiverigidity, paranoia, and aggressiveness amongaggressive patients.
Results
Basic Statistics
During the first 4 years of the program, theSecond Chance Program admitted 190 patients,or approximately 1 per week. Of these patients,67% were male. Sixty-three percent of admis-sions were African-American, 17% Caucasian,and 20% Latino. The mean age of patientswas 38.32 (SD � 9.63). All patients were trans-ferred directly from state hospitals, where theyhad resided for a minimum of 3 years, in accor-dance with program admission policy. Themean length of stay at the state hospital prior totransfer to the program was 7.42 years, with arange of 3–21 years.
Although patients admitted to the SecondChance Program were considered treatment-re-fractory, 78% were discharged from the pro-gram. The remaining 22% of patients were un-able to be discharged and were transferred backto the state hospital, either because of continuedbehavioral dysfunction or because of an inabil-ity to obtain a residential placement in the com-munity. After 4 years of program operation,67% of patients ever admitted to the programwere living in the community. The remaindereither were transferred back to the state hospitalthat referred them or were discharged to thecommunity from the Second Chance Programbut have subsequently been rehospitalized. Innearly all cases, discharged patients moved intoa supervised housing arrangement. Theseranged from typical supported housing settings,in which patients had their own or a sharedapartment, to group homes in the suburbs ofNew York City. In a small number of cases, a
patient lived with family members afterdischarge.
Median length of stay among the 78% ofpatients discharged from the program was 87days (M � 110), which is considerably lowerthan the duration of their tenure at the statehospital. Forty-nine percent of discharged pa-tients were rehospitalized on the program atleast one time. Among rehospitalized patients,the mean duration of community tenure beforereadmission was 176 days. When admissionsare divided into first versus readmissions (to theSecond Chance Program), mean length of stayfor first hospitalizations was 145 days, whereasfor readmissions it was 67 days. Overall, thesedata suggest that the Second Chance Programhas been successful at discharging formerlytreatment-refractory patients back to the com-munity: The discharge rate was high, the read-mission rate was typical for this population,readmitted patients averaged half a year in thecommunity before rehospitalization, and lengthsof stay during readmission were relatively brief.
Selected Findings on Treatment Effects
Early in the development of the program,before the initiation of the behavioral proce-dures described earlier, blood levels of medica-tion suggested that patients were not taking theirmedication at the prescribed doses. To addressthis, staff instituted a policy wherein morningmedications were administered during groupsessions. Patients were expected to stay for theentire 45-min session; leaving the session re-sulted in taking a second dose of medication.The group sessions themselves involved discus-sion of medication and side-effect issues, aswell as discharge planning. As a result of thisintervention, medication blood levels ap-proached expected levels. In addition, the rateof violent behaviors was significantly reduced.Table 3 compares data on restraint and seclu-sion from the 9 months in 1999 after this inter-vention to data from the same 9-month periodduring 1998. As can be seen, significant differ-ences were obtained, indicating that the newmedication groups led to significant improve-ment in patient behavior.
Despite the effectiveness of the morningmedication group intervention, seclusion andrestraint episodes were still considered to beoccurring at an unacceptably high rate. To ad-
161TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS
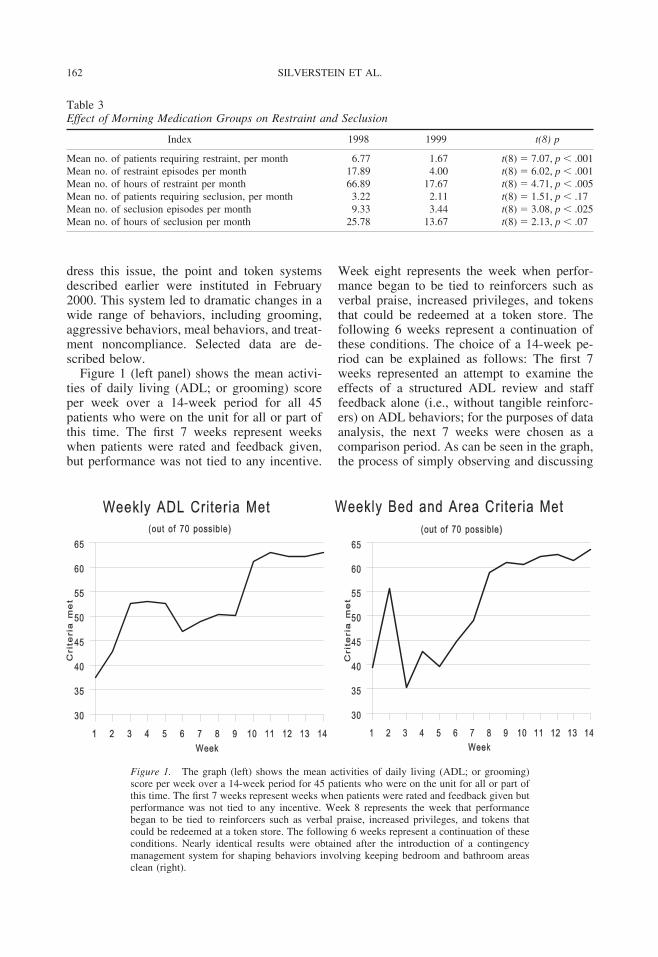
dress this issue, the point and token systemsdescribed earlier were instituted in February2000. This system led to dramatic changes in awide range of behaviors, including grooming,aggressive behaviors, meal behaviors, and treat-ment noncompliance. Selected data are de-scribed below.
Figure 1 (left panel) shows the mean activi-ties of daily living (ADL; or grooming) scoreper week over a 14-week period for all 45patients who were on the unit for all or part ofthis time. The first 7 weeks represent weekswhen patients were rated and feedback given,but performance was not tied to any incentive.
Week eight represents the week when perfor-mance began to be tied to reinforcers such asverbal praise, increased privileges, and tokensthat could be redeemed at a token store. Thefollowing 6 weeks represent a continuation ofthese conditions. The choice of a 14-week pe-riod can be explained as follows: The first 7weeks represented an attempt to examine theeffects of a structured ADL review and stafffeedback alone (i.e., without tangible reinforc-ers) on ADL behaviors; for the purposes of dataanalysis, the next 7 weeks were chosen as acomparison period. As can be seen in the graph,the process of simply observing and discussing
Table 3Effect of Morning Medication Groups on Restraint and Seclusion
Index 1998 1999 t(8) p
Mean no. of patients requiring restraint, per month 6.77 1.67 t(8) � 7.07, p � .001Mean no. of restraint episodes per month 17.89 4.00 t(8) � 6.02, p � .001Mean no. of hours of restraint per month 66.89 17.67 t(8) � 4.71, p � .005Mean no. of patients requiring seclusion, per month 3.22 2.11 t(8) � 1.51, p � .17Mean no. of seclusion episodes per month 9.33 3.44 t(8) � 3.08, p � .025Mean no. of hours of seclusion per month 25.78 13.67 t(8) � 2.13, p � .07
Figure 1. The graph (left) shows the mean activities of daily living (ADL; or grooming)score per week over a 14-week period for 45 patients who were on the unit for all or part ofthis time. The first 7 weeks represent weeks when patients were rated and feedback given butperformance was not tied to any incentive. Week 8 represents the week that performancebegan to be tied to reinforcers such as verbal praise, increased privileges, and tokens thatcould be redeemed at a token store. The following 6 weeks represent a continuation of theseconditions. Nearly identical results were obtained after the introduction of a contingencymanagement system for shaping behaviors involving keeping bedroom and bathroom areasclean (right).
162 SILVERSTEIN ET AL.

grooming behaviors in a public forum seemedto improve performance. However, a significantfurther improvement occurred after the imple-mentation of the reinforcement procedures,which were believed to be necessary both tofurther improve performance and to maintainthe higher level of functioning. This longitudi-nal series reveals a significant effect over time,with a repeated measures analysis based onmaximum likelihood estimation procedures,and specifying a first-order autoregressive co-variance structure, Wald �2(13) � 278.40, p �.0005. In addition, a contrast comparing thefirst 7 weeks against the last 7 weeks revealed asignificant difference, Wald �2(1) � 31.08, p �.0005. Nearly identical results were obtainedafter the introduction of a contingency manage-ment system for shaping behaviors that in-volved keeping bedroom and bathroom areasclean (see Figure 1, right panel). Here, therewas again a significant effect over time, Wald�2(13) � 605.82, p � .0005; as well as asignificant difference between the weeks beforeand the weeks after the system was introduced,Wald �2(1) � 142.94, p � .0005, thus demon-strating that the effect was not solely due togiving patients increased feedback about theirperformance. Note that these graphs reflectscores averaged across all patients who were onthe unit during this 14-week period, includingnew admissions and patients who were dis-charged before the end of that period. The datacan thus be seen as reflecting a real change inthe functioning of the unit as a whole rather thanjust improvement among a single group of pa-tients who were admitted at Week 1.
In addition to numerous examples of specificbehaviors improving as a result of the unitwideapplication of behavior-shaping procedures, therates of seclusion and restraint continued todecrease. Figure 2 demonstrates the averagemonthly total of seclusion room incidents from2000 and 2001, compared with the data notedearlier from the 2 earlier years. As can be seen,the inception of specific behavioral rating pro-cedures and feedback processes has led to fur-ther reduction in aggressive behaviors.
Although modeling change at the level of theunit as a whole can provide important informa-tion about program effectiveness, additionaluseful information can result from modeling atthe patient level first. Consideration of individ-ual differences in response to treatment can be
undertaken on humanitarian grounds alone;however, it is also supported by data. For ex-ample, in the repeated measures analysis ofvariance discussed earlier, tracking ADL dataover 14 weeks for 45 patients, the fixed effect ofweek (i.e., number of weeks since the initiationof the contingency management system forgrooming behaviors) accounted for 50% of thevariance in patient change over time. However,the random effect of patient accounted for closeto an additional 20% of the variance in the data,an effect which is larger than the R-squaredvalue in many treatment studies. This suggeststhat the patient being treated is an importantdeterminant of responsiveness to the interven-tion and implies that attention should be paid tobaseline characteristics and to tracking individ-ual response profiles, as opposed to only groupeffects, as part of overall quality improvementefforts. Such analyses can also allow for a de-termination as to whether subgroups exist thatmay be responding differently to treatment.
To accomplish modeling beginning at thepatient level, the following procedures can beused: (a) For each variable of interest (e.g.,verbal abuse, grooming), each patient is char-acterized according to three parameters—themean of their responses over time, their slope(or degree of change) over time, and their vari-ability around their own trend line; (b) thesevalues are entered into cluster analyses to de-termine whether meaningful subgroups exist(Kupper & Hoffman, 2000). With this strategy,meaningful subgroups have been identified on anumber of variables. Figure 3 demonstrates pa-
Seclusion Room Incidents per Month
0
2
4
6
8
10
1998 1999 2000 2001
Year
# o
f in
cid
ents
Figure 2. Number of seclusion room incidents per monthon the unit.
163TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

tient data on the aforementioned three dimen-sions plotted on a 3-dimensional graph, where itcan be seen that subgroups exist. These datarepresent a summary score of combined verbaland physical abuse incidents.
Figure 4 demonstrates examples of patients clos-est to the centroid of each of the four clusters iden-tified for this abuse variable. In each graph, the x-axisrepresents time (week in the program), and the y-axisrepresents the number of abuse incidents per week,on a scale ranging from 0 to 10. As can be seen inthese graphs, some patients rarely demonstrate abu-sive behavior, whereas others do frequently. Amongthose groups, however, some are more variable thanothers, and different degrees of change over time(slope) are evident. The identification of sub-groups in this fashion has important treatmentimplications, including the early developmentof behavior contracts for patients who dem-onstrate significant abuse behavior and/or arelikely to show minimal improvement withmilieu management alone and the identifica-tion of (and teaching staff and patients about)early warning signs for patients who demon-strate significant variability and frequency ofan inappropriate behavior. An additional goalfor future research is the determination ofwhether patients with different courses oftreatment responsiveness have different long-term outcomes.
Figure 3. Pyramid plot expressing relationships betweenabuse parameters: Mean (x-axis), slope (z-axis), and vari-ability (expressed as standard error; y-axis). On the z-axis,toward the back is more positive (indicating, in this case, anincreased frequency of abuse behaviors over time), andtoward the front is more negative (indicating decreasingscores). Each “pyramid” represents a single patient.
Figure 4. The four graphs depict examples of representative patients from each of fourverbal/physical abuse clusters. In each graph, the x-axis represents time (week in the program), andthe y-axis represents the number of abuse incidents per week on a scale ranging from 0 to 10.
164 SILVERSTEIN ET AL.

Discussion
In this article, we have summarized a specialtyprogram for returning “treatment-refractory” pa-tients with long stays in public psychiatric hospi-tals back into the community. The features of theprogram and outcome data were described. Ourresults are similar to those of previous reportsusing behaviorally oriented inpatient programs(e.g., Liberman et al., 2005; Paul & Lentz, 1977),and they testify to the strength of social-learningbased procedures when utilized correctly. An im-portant factor in the correct use of these proce-dures is the establishment of a behaviorally ori-ented program philosophy in which all staff pro-vide consistent responses to patients.
The interpersonal techniques described in thisarticle, along with the group and milieu interven-tions, combine to form an intensive treatment en-vironment where patients receive a great deal ofpositive and corrective feedback about their be-haviors. In our experience, for the majority ofpatients who are considered treatment refractory,such interventions are all that is required. Even themajority of aggressive patients can be helped by acombination of milieu-based feedback, behaviorcontracts, and groups targeting appropriate socialskills, problem-solving skills, and anger manage-ment (Wilkniss, Silverstein, & Hunter, 2004).However, there are patients for whom this is notenough. Typically, patients who need additionalintervention are those who have severe attentionaldeficits. For such patients, we recommend the useof attention-shaping procedures, as well as thedevelopment of novel techniques targeting thespecific phenomenon interfering with attention(e.g., hallucinations). We have found that the useof these interventions, in combination with behav-ioral treatment techniques in the milieu andgroups in general, create a powerful treatmentenvironment in which even the most impairedpatients can begin to see themselves as being ableto succeed. This glimmer of hope is often enoughto increase motivation to engage further in treat-ment, which is a necessary factor in producingpositive outcomes.
It is not clear at this point what the relativecontributions of the individual program compo-nents are to the overall outcome. Previous dataindicate that the structure of a behavioral milieucan improve functioning and that the addedeffects of single interventions, while important,are relatively small, compared with milieu ef-
fects (Silverstein & Wilkniss, 2004; Spaulding,Fleming, et al., 1999; Spaulding, Reed, et al.,1999; Wong, 1996). Also, determination of spe-cific contributions of individual interventions inreal-world programs outside of research con-texts is fraught with difficulty. Both practicallyand ethically, there are problems in introducingand removing interventions that appear to ben-efit patients. In addition, many interventions areinextricably linked. For example, observationalratings and verbal feedback are linked to tokendistribution, which is linked to the use of thetoken store. Therefore, in many cases, it wouldbe difficult to evaluate the effectiveness of sin-gle components in isolation. In an effort toproduce the most effective program, the SecondChance Program utilized evidence-based interven-tions (e.g., token economy, manualized skillstraining approaches, cognitive rehabilitation), thusminimizing the likelihood that specific interven-tions would be ineffective in general. The chal-lenge in such a program is to ensure that eachpatient receives treatment that is maximally tai-lored to his/her individual needs and delivered bystaff that consistently demonstrate high levels offidelity to established procedures.
The population treated in the Second ChanceProgram represents the most severe end of thedisability continuum among chronic schizo-phrenia patients. Within this context, it is nota-ble that the program achieved a discharge rateclose to 80%, a median length of stay of 3months (compared with over 7 years prior tobeing transferred), and a 2-year rehospitaliza-tion rate (49%) lower than that found in manypharmaceutical company-sponsored studies thattypically recruit healthier and more medication-compliant patients. Still, a number of lessonswere learned that could inform future efforts togenerate better outcomes. The two most obvi-ous areas where improvement is possible in-volve program organization and aftercare is-sues. These are discussed briefly below.
Programs based in a clear treatment philoso-phy, such as social-learning-based inpatientprograms, work best when there is a clear pro-gram leader, and all staff report to that leader(Liberman & Corrigan, 1994). In the case of theSecond Chance Program, however, staff re-ported to their discipline heads, who were notpart of the treatment program and who weretypically more invested in promoting the statusof discipline members than in ensuring the in-
165TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

tegrity of the treatment program. Nowhere wasthis more evident than with nursing staff, whotypically resisted changing over to the behav-ioral program. A number of procedures that hadbeen long valued by nursing staff and that couldbe viewed as existing for their conveniencerather than for patient benefit (e.g., the practiceof “quiet time,” wherein patients were fined ifthey came out of their rooms between 2:00 and4:00 p.m.) were eliminated as part of the newprogram. This inevitably led to staff conflicts,delays in implementing specific procedures,lack of faithful implementation on the part ofresistant staff, staff counseling, and, in somecases, to reassignment of staff to other units inthe hospital. In some cases, however, staff whohad been in the hospital for many years butwhose behavior was consistently inappropriatefor the program (e.g., yelling at patients, notusing interpersonal techniques such as the3-step technique) were not transferred to otherunits, even after repeated documentation of in-appropriate behavior to the discipline chief, be-cause of political factors. These situations havebeen in existence since the opening of the pro-gram and continue to represent an obstacle tomaximum treatment effectiveness.
A second rate-limiting factor with outcomeswas the relative lack of outpatient residentialfacilities and treatment programs that were be-haviorally oriented. Although the original part-nership between state hospitals, the private hos-pital, and residence providers ensured that pa-tients could be transferred in and out of theSecond Chance Program, no plan existed toensure continuity of care after discharge. Thiswas a problem because, although relapse can beconsidered inevitable in some cases (because oflife stress and/or illness severity), in our expe-rience, the majority of readmissions were ne-cessitated by the lack of behavioral treatmentsavailable at community residences and treat-ment facilities. This problem was most pro-nounced for patients who had been on a seriesof behavior contracts. Although these were of-ten explained to staff at sites where the patientswould be living and/or receiving treatment, wewere typically told that there was no way anyindividualized treatment could be given to thepatient. This led to many instances of behaviorproblems, which were usually the factor respon-sible for the patient being readmitted to theProgram. There were also many instances in
which outpatient psychiatrists changed patientmedication immediately after they become re-sponsible for the patient’s care. This happenedmost often for patients on clozapine, whichmany outpatient psychiatrists did not wish tocontinue, often for fear of liability if a patientdeveloped complications due to a reduced whiteblood cell count. The effect of changing medi-cations, in the absence of data suggesting thatthis needed to be done, was often a worseningof symptoms and/or behavior, thus requiringrehospitalization.
The partnership that led to the formation ofthe Second Chance Program involved severalinstitutions and agencies, including the NewYork State Office of Mental Health, and repre-sented a relatively unique level and scale ofcooperation. To address the aftercare problemsnoted earlier, an extension of the original part-nership would have been necessary. At a mini-mum, staff in selected outpatient treatment sitesand residential facilities would have to betrained in the social-learning model, and ongo-ing monitoring of staff fidelity to treatment prin-ciples would have to become standard operatingprocedure at these sites. Such an effort was notsupported by the state office of mental health,and even if it had, it would have been logisti-cally difficult to carry out because of the dis-tance between the hospital where the SecondChance Program was located and the agencies.Moreover, because staff at each hospital/agencywere full-time employees at their workplace,job descriptions did not include travel to, andtraining of staff at, other sites. It would seemthat, ideally, a dedicated staff of “experts”would be involved in both the establishment ofthe inpatient unit and the training of communi-ty-based staff. An alternative is the declining-contact aftercare model described by Paul andLentz (1977) in which discharged patients metwith hospital staff with gradually reducing fre-quency in the months after discharge. In thecase of the Second Chance Program, however,this option was not implemented because ofalready high workloads of the inpatient staff,the distance between patient residences and thehospital, and the lack of a case manager groupthat could have facilitated this effort.
Despite these real-world difficulties, the de-velopment of the Second Chance Program indi-cates that it is possible for different stakeholdersto work together to forge solutions that can
166 SILVERSTEIN ET AL.

improve the lives of long-stay patients who areconsidered treatment refractory in state hospitalsettings. As was demonstrated long ago (e.g.,Atthowe & Krasner, 1968; Ayllon & Azrin,1968; Paul & Lentz, 1977), delivery of optimal,social-learning-based treatment can lead to areduction of inappropriate behaviors, increasedfrequency of appropriate behaviors, and suc-cessful transition from being reliant on externalreinforcers (e.g., tokens) to self-control of be-havior based on intrinsic and social reinforce-ment. The existence of the Second Chance Pro-gram, however, which was staffed with a regu-lar hospital staffing pattern, raises the issue ofwhy similar outcomes are not routinely pro-duced in state hospital and other long-stay set-tings. This speaks to the need for greater aware-ness of evidence-based interventions forchronic schizophrenia and a willingness to de-vote attention to the dissemination, implemen-tation, and maintenance of such programs. Thisis a complex issue that requires intervention ona number of levels, including increasing thenumber of graduate programs in clinical psy-chology that offer training in this area, raisingthe status of psychologists in psychiatric hospi-tal settings so that their potential contributionsare realized (Jewell & Silverstein, 1999) andchanging the benchmarks by which hospitalprogram outcomes are evaluated (to include,among other variables, the implementation ofbest practices, the assessment of functional im-provement of patients, and the degree to whichstaff adhere to the program model). Althoughbest practices initiatives do not always include afocus on people with chronic schizophrenia(Silverstein et al., 2002), enough is now knownabout how to help this group (Liberman et al.,2005; Silverstein et al., 2006) so that failure nolonger need be an option.
References
Atthowe, J. M., & Krasner, L. (1968). Preliminaryreport on the application of contingent reinforce-ment procedures (token economy) on a “chronic”psychiatric ward. Journal of Abnormal Psychol-ogy, 73, 37–43.
Attkisson, R. F., Crook, J., Karno, M., Lehman, A.,McGlashan, T. H., Meltzer, H. Y., et al. (1992).Clinical services research. Schizophrenia Bulle-tin, 18, 561–626.
Ayllon, T., & Azrin, N. H. (1968). The token econ-omy: A motivational system for therapy and reha-bilitation. New York: Appleton-Century-Crofts.
Bell, M. Bryson, G., & Wexler, B. (2003). Cognitiveremediation of working memory deficits: Durabil-ity of training effects in severely impaired and lessseverely impaired schizophrenia. Acta Psychiat-rica Scandinavica, 108, 101–109.
Bellus, S. B., Kost, P. P., Vergo, J. G., & Dinezza,G. J. (1998). Improvements in cognitive function-ing following intensive behavioural rehabilitation.Brain Injury, 12, 139–145.
Brenner, H., Hodel, B., Roder, V., & Corrigan, P.(1992). Treatment of cognitive dysfunctions andbehavioral deficits in schizophrenia. SchizophreniaBulletin, 18, 21–26.
Brenner, H., Roder, V., Hodel, B., Kienzle, N., Reed,D., & Liberman, R. (1994). Integrated psycholog-ical therapy for schizophrenic patients. Toronto,Ontario, Canada: Hogrefe & Huber.
Coleman, J. C., & Paul, G. L. (2001). Relationshipbetween staffing ratios and effectiveness of inpa-tient psychiatric units. Psychiatric Services, 52,1374–1379.
Corrigan, P. W., & Liberman, R. P. (Eds.). (1994).Overview of behavior therapy in psychiatric hos-pitals. Behavior therapy in psychiatric hospitals(pp. 1–38). New York: Springer.
Corrigan, P. W., & McCracken, S. G. (1997). Inter-active staff training: Rehabilitation teams thatwork. New York: Plenum Press.
Glynn, S. M., Liberman, R. P., Bowen, L., Kuehnel,T., Marshall, B. D., & Gnanamuthu, S. (1994). Theclinical research unit at Camarillo State Hospital.In P. W. Corrigan & R. P. Liberman (Eds.), Be-havior therapy in psychiatric hospitals (pp. 39–60). New York: Springer.
Green, M. F. (1996). What are the functional conse-quences of neurocognitive deficits in schizophrenia?American Journal of Psychiatry, 153, 321–330.
Hatashita-Wong, M., & Silverstein, S. M. (2003).Coping with voices: Selective attention training forpersistent auditory hallucinations in treatment re-fractory schizophrenia. Psychiatry, 66, 255–261.
Heinssen, R. K., Levendusky, P. G., & Hunter, R. H.(1995). Client as colleague: Therapeutic contract-ing with the seriously mentally ill. American Psy-chologist, 50, 522–532.
Jablensky, A. (2000). Epidemiology of schizophre-nia: The global burden of disease and disability.European Archives of Psychiatry and ClinicalNeuroscience, 250, 274–285.
Jewell, T. C., & Silverstein, S. M. (1999). The role ofthe psychologist in the state hospital. New YorkState Psychologist, 11, 11–15.
Jewell, T. C., Silverstein, S. M., & Stewart, D. A.(2001). Evaluation of a manualized program toteach staff to write behavior contracts for people
167TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS

with schizophrenia. Psychiatric RehabilitationSkills, 5, 255–271.
Kane, J. (1989). The current status of neuroleptics.Journal of Clinical Psychiatry, 50, 322–328.
Kane, J. (1992). Clinical efficacy of clozapine intreatment of refractory schizophrenia: An over-view. British Journal of Psychiatry, 18(Suppl. 17),41–54.
Kane, J., Honigfeld, G., Singer, J., Meltzer, H., & theClozaril Collaborative Study Group. (1988). Clo-zapine for the treatment-resistant schizophrenic: Adouble-blind comparison with chlorpromazine. Ar-chives of General Psychiatry, 45, 789–796.
Kupper, Z., & Hoffmann, H. (2000). Course patternsof psychosocial functioning in schizophrenia pa-tients attending a vocational rehabilitation pro-gram. Schizophrenia Bulletin, 26, 683–700.
Lehman, A. F., Ward, N. C., & Linn, L. S. (1982).Chronic mental patients: The quality of life issue.American Journal of Psychiatry, 139, 1271–1276.
Levendusky, P. G., Berglas, S., Dooley, C. P., &Landau, R. J. (1983). Therapeutic Contract Pro-gram: Preliminary report on a behavioral alterna-tive to the token economy. Behavior Research andTherapy, 21, 137–142.
Levendusky, P. G., Willis, B. S., & Ghinassi, F. A.(1994). The therapeutic contracting problem: Acomprehensive continuum of care model. Psychi-atric Quarterly, 65, 189–208.
Liberman, R. P. (1992). Handbook of psychiatricrehabilitation. Boston: Allyn & Bacon.
Liberman, R. P., & Corrigan, P. W. (1994). Imple-menting and maintaining behavior therapy pro-grams. In P. W. Corrigan & R. P. Liberman (Eds.),Behavior therapy in psychiatric hospitals (pp.201–219). New York: Springer.
Liberman, R. P., Kopelowicz, A., & Silverstein,S. M. (2005). Psychiatric rehabilitation. In B. J.Sadock & V. A. Sadock (Eds.), Kaplan and Sa-dock’s comprehensive textbook of psychiatry (8thed., pp. 3884–3930). Baltimore: Lippincott, Wil-liams, & Wilkins.
Lieberman, A. A., & Coburn, A. F. (1986). Thehealth of the chronically mentally ill: A review ofthe literature. Community Mental Health Jour-nal, 22, 104–116.
Lieberman, J. A., Stroup, T. S., McEvoy, J. P.,Swartz, M. S., Rosenheck, R. A., Perkins, D. O., etal. (2005). Effectiveness of antipsychotic drugs inpatients with chronic schizophrenia. New EnglandJournal of Medicine, 353, 1209–1223.
Martin, B. C., & Miller, L. S. (1998). Expendituresfor treating schizophrenia: A population-basedstudy of Georgia Medicaid recipients. Schizophre-nia Bulletin, 24, 479–488.
Massel, H. K., Corrigan, P. W., Liberman, R. P., &Milan, M. A. (1991). Conversation skills trainingof thought-disordered schizophrenic patients
through attention focusing. Psychiatry Re-search, 38, 51–61.
Menditto, A. A., Valdes, L. A., & Beck, N. C. (1994).Implementing a comprehensive social-learningprogram within the forensic psychiatric service ofFulton State Hospital. In P. W. Corrigan & R. P.Liberman (Eds.), Behavior therapy in psychiatrichospitals (pp. 61–78). New York: Springer.
Menditto, A. A., Baldwin, L. J., O’Neal, L. G., Beck,N. C. (1991). Social learning procedures for in-creasing attention and improving basic skills inseverely regressed institutionalized patients. Jour-nal of Behavior Therapy and Experimental Psychi-atry, 22, 265–269.
Menditto, A. A., Beck, N. C., Stuve, P., Fisher, J. A.,Stacy, M., Logue, M. B., & Baldwin, L. J. (1996).Effectiveness of clozapine and a social learningprogram for severely disabled psychiatric inpa-tients. Psychiatric Services, 47, 46–51.
Mojtabai, R., Nicholson, R. A., Isohanni, M., Jones,P., & Partennen, U. (1998). Role of psychosocialtreatments in management of schizophrenia: Ameta-analytic review of controlled outcome stud-ies. Schizophrenia Bulletin, 24, 569–587.
Murray, H. A. (1943). Thematic Apperception Test.Cambridge, MA: Harvard University Press.
Paul, G. L. (2000). Evidence-based practices in in-patient and residential facilities. The Clinical Psy-chologist, 53, 3–11.
Paul, G. L., & Lentz, R. J. (1977). Psychosocialtreatment of chronic mental patients: Milieu vs.social learning programs. Cambridge, MA: Har-vard University Press.
Paul, G. L., Stuve, P., & Cross, J. V. (1997). Real-world inpatient programs: Shedding somelight—A critique. Applied and Preventive Psychol-ogy: Current Scientific Perspectives, 6, 193–204.
Policy Study Associates. (1989). Best practice studyof vocational rehabilitation services to severelymentally ill persons. Washington, DC: Rehabilita-tion Services Administration, Department ofEducation.
Rupp, A., & Keith, S. J. (1993). The costs of schizo-phrenia: Assessing the burden. Psychiatric Clinicsof North America, 16, 413–423.
Silverstein, S. M. (2000). Psychiatric rehabilitation ofschizophrenia: Unresolved issues, current trendsand future directions. Applied and Preventive Psy-chology, 9, 227–248.
Silverstein, S. M., Bowman, J., & McHugh, D.(1997). Strategies for hospital-wide disseminationof psychiatric rehabilitation interventions. Psychi-atric Rehabilitation Skills, 2, 1–23.
Silverstein, S. M., Hatashita-Wong, M., Solak, B. A.,Uhlhaas, P., Landa, Y., Wilkniss, S. M., et al.(2005). Effectiveness of a two-phase cognitive re-habilitation intervention for severely impaired
168 SILVERSTEIN ET AL.

schizophrenia patients. Psychological Medi-cine, 35, 829–837.
Silverstein, S. M., & Jewell, T. C. (2002). Effective-ness of a psychiatric rehabilitation training pro-gram for community services staff. PsychiatricRehabilitation Skills, 6, 53–61.
Silverstein, S. M., Menditto, A., & Stuve, P. (2001).Shaping attention span: An operant condition pro-cedure for improving neurocognitive functioning inschizophrenia. Schizophrenia Bulletin, 27, 247–257.
Silverstein, S. M., Pierce, D. L., Saytes, M., Hems,L., Schenkel, L., & Streaker, N. (1998). Behavioraltreatment of attentional dysfunction in chronic,treatment-refractory schizophrenia. PsychiatricQuarterly, 69, 95–105.
Silverstein, S. M., Schenkel, L. S., Valone, C., &Nuernberger, S. (1998). Cognitive deficits andpsychiatric rehabilitation outcomes in schizophre-nia. Psychiatric Quarterly, 69, 169–191.
Silverstein, S. M., Spaulding, W. D., & Menditto,A. A. (2006). Schizophrenia: Advances in evi-dence-based practice. Toronto, Ontario, Canada:Hogrefe & Huber.
Silverstein, S. M., Valone, C., Jewell, T. C., Corry,R., Nghiem, K., Saytes, M., & Potrude, S. (1999).Integrating shaping and skills training techniquesin the treatment of chronic, treatment-refractoryindividuals with schizophrenia. Psychiatric Reha-bilitation Skills, 3, 41–58.
Silverstein, S. M., & Wilkniss, S. (2004). The futureof cognitive rehabilitation of schizophrenia.Schizophrenia Bulletin, 30, 679–692.
Silverstein, S. M., Wilkniss, S., & Bloch, A. (2002).Best practices: Don’t forget about the sickest pa-tients. [Letter to the editor.] Psychiatric Ser-vices, 53, 1032–1033.
Simpson, G. M., Josiassen, R. C., Stanilla, J. K., deLeon, J., Nair, C., Abraham, G., et al. (1999).Double-blind study of clozapine dose response inchronic schizophrenia. American Journal of Psy-chiatry, 156, 1744–1750.
Simpson, J. C., & Tsuang, M. T. (1996). Mortalityamong patients with schizophrenia. SchizophreniaBulletin, 22, 485–499.
Skinner, C. H., Skinner, A. L., & Armstrong, K. J.(2000). Analysis of a client-staff-developed shap-ing program designed to enhance reading persis-tence in an adult diagnosed with schizophrenia.Psychiatric Rehabilitation Journal, 24, 52–57.
Spaulding, W. D., Fleming, S. K., Reed, D., Sullivan,M., Storzbach, D., & Lam, M. (1999). Cognitivefunctioning in schizophrenia: Implications for psy-chiatric rehabilitation. Schizophrenia Bulletin, 25,275–289.
Spaulding, W. D., Reed, D., Sullivan, M., Richard-son, C., & Weiler, M. (1999). Effects of cognitivetreatment in psychiatric rehabilitation. Schizophre-nia Bulletin, 25, 657–676.
Spaulding, W. D., Storms, L., Goodrich, V., & Sul-livan, M. (1986). Applications of experimentalpsychopathology in psychiatric rehabilitation.Schizophrenia Bulletin, 12, 560–577.
Spaulding, W. D., & Sullivan, M. (1992). From lab-oratory to clinic: Psychological methods and prin-ciples in psychiatric rehabilitation. In R. P. Liber-man (Ed.), Handbook of psychiatric rehabilitation(pp. 30–55). Boston: Allyn & Bacon.
Talbott, J. A. (2004). Lessons learned about thechronic mentally ill since 1955. Psychiatric Ser-vices, 55, 1152–1159.
van Der Gaag, M. (1992). The results of cognitivetraining in schizophrenic patients. Delft, the Neth-erlands: Eburon.
Velligan, D. I., & Bow-Thomas, C. C. (2000). Twocase studies of cognitive adaptation training foroutpatients with schizophrenia. Psychiatric Ser-vices, 51, 25–29.
Wahlbeck, K., Cheine, M., Essali, A., & Adams, C.(1999). Evidence of clozapine’s effectiveness inschizophrenia: A systematic review and meta-anal-ysis of randomized trials. American Journal ofPsychiatry, 156, 990–999.
Wallace, C. J., Liberman, R. P., Kopelowicz, A., &Yaeger, D. (2001). Psychiatric rehabilitation. In N.Andreasen & G. O. Gabbard (Eds.), Treatment ofpsychiatric disorders: The DSM–IV edition (pp.1093–1112). Washington, DC: American Psychi-atric Press.
Wilkniss, S. M., Silverstein, S. M., & Hunter, R.(2004). Nonpharmacologic treatment of aggres-sion and violence in individuals with psychosis.Contemporary Psychiatry, 3, 1–8.
Wirshing, D. A., Marshall, B. D., Jr., Green, M. F.,Mintz, J., Marder, S. R., & Wirshing, W. C.(1999). Risperidone in treatment-refractoryschizophrenia. American Journal of Psychiatry,156, 1374–1379.
Witkin, M. J., Atay, J., & Manderscheid, R. W.(1996). Trends in state and county mental hospitalsin the U.S. from 1970 to 1992. Psychiatric Ser-vices, 47, 1079–1081.
Wong, S. E. (1996). Psychosis. In M. Mattini & B.Thyer (Eds.), Finding solutions to social prob-lems: Behavioral strategies for change (pp. 319–343). Washington, DC: American PsychologicalAssociation.
Wu, E. Q., Birnbaum, H. G., Shi, L., Ball, D. E.,Kessler, R. C., Moulis, M., & Aggarwal, J. (2005).The economic burden of schizophrenia in theUnited States in 2002. Journal of Clinical Psychi-atry, 66, 1122–1129.
Received May 26, 2005Revision received March 23, 2006
Accepted April 17, 2006 �
169TREATMENT-REFRACTORY SCHIZOPHRENIA PATIENTS
Related Documents











