Linda L. Clarke, RNC, MN Melodee J. Deutsch, RNC, MS, MPH 1 e becominc A babir- eJ fr e e d 1V Our story begins in Hawaii, an island chain in the middle of the Pacific Ocean. The uniqueness of these islands has as much to do with the diversity of their people as with their wealth of natural beauty. The cultural mosaic of our health plan members and staff at the Moanalua Medical Center in Honolulu-Caucasian, Hawaiian, Japanese, Filipino, Chinese, Samoan-holds our Kaiser Hawaii’s mission, “Caring for Hawaii’s People Like Family,” central to the ebb and flow of island life. Kaiser Permanente serves approximately 200,000 members on four islands: Oahu, Maui, Kauai, and the “Big Island” of Hawaii. At Moanalua, we deliver approximately 2,200 babies each year and provide family-centered care in labor and delivery, antepartum, moth- er-baby, and neonatal intensive care units (NICUs). Total Quality Environment Our story begins in 1991 when Kaiser senior leadership made a commitment to create a total quality care environment. The first step toward total quality management (TQM) was moving our organization from its provider focus to a customer-patient focus. Between 1992 and 1994, managers, supervisors, and other leaders received orientation and training in quality processes. Each was expected to establish a quality team to improve daily work processes. Eager to put our new TQM skills and tools into action, we initiated a patient survey and formed an interdisciplinary team to identify opportunities for improvement in perinatal ser- vices. The Maternal-Child Services Leadership Team met in 1993 and analyzed the survey data. In particular, our customers told us we had a problem with the care and service we were providing to breastfeeding mothers and babies. We had always had an unwritten, inter- 30 Lifelines December 1997

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Linda L. Clarke, RNC, MN
Melodee J. Deutsch, RNC, MS, MPH
1 e
becominc A
babir- eJ
fr e e d 1V Our story begins in Hawaii, an island chain in the middle of the Pacific Ocean.
The uniqueness of these islands has as much to do with the diversity of their
people as with their wealth of natural beauty. The cultural mosaic of our
health plan members and staff at the Moanalua Medical Center in Honolulu-Caucasian,
Hawaiian, Japanese, Filipino, Chinese, Samoan-holds our Kaiser Hawaii’s mission, “Caring
for Hawaii’s People Like Family,” central to the ebb and flow of island life.
Kaiser Permanente serves approximately 200,000 members on four islands: Oahu, Maui, Kauai, and the “Big Island” of Hawaii. At Moanalua, we deliver approximately 2,200 babies each year and provide family-centered care in labor and delivery, antepartum, moth- er-baby, and neonatal intensive care units (NICUs).
Total Quality Environment Our story begins in 1991 when Kaiser senior leadership made a commitment to create a total quality care environment. The first step toward total quality management (TQM) was moving our organization from its provider focus to a customer-patient focus. Between 1992 and 1994, managers, supervisors, and other leaders received orientation and training in quality processes. Each was expected to establish a quality team to improve daily work processes.
Eager to put our new TQM skills and tools into action, we initiated a patient survey and formed an interdisciplinary team to identify opportunities for improvement in perinatal ser- vices. The Maternal-Child Services Leadership Team met in 1993 and analyzed the survey data. In particular, our customers told us we had a problem with the care and service we were providing to breastfeeding mothers and babies. We had always had an unwritten, inter-
30 L i f e l i n e s December 1997
The Ten Steps to Succesful Breastfeeding
1. Have a wriien breastfeeding policy that is routinely communicated to all health care staff.
2. Train all health care staff in skills necessary to implement this policy.
3. Inform all pregnant women about the benefits and management of breastfeeding.
4. Help mothers initiate breastfeeding within one hour of birth.
1. Show mothers how to breastfeed and how to main- tain lactation, even if they should be separated from their infants.
6. Give newborn infants no food or drink other than breast milk, unless medically indicated.
7. Practice rooming-in-allow mothers and infants to remain together-24 hours a day.
8. Encourage breastfeeding on demand.
9. Give no artificial teats or pacifiers to breastfeeding
10. Foster the establishment of breastfeeding support
infants.
groups and refer mothers to them, on discharge from the hospital or clinic.
Source: Baby-Friendly USA.
nal policy to support the choices of our mothers- whether to breastfeed or bottle feed-but we listened carefully to the customer feedback and made a decision to reallocate payroll dollars to hire a lactation nurse specialist, the first step we believed necessary in the process of improving overall customer satisfaction with breastfeeding support in our facility.
After hiring a lactation expert in early 1994, we formed the Lactation Advisory Workgroup, known fondly as “The LAW.” This dedicated, committed core group included nurses, nurse practitioners, and physi- cians from inpatient units, outpatient clinics, home care, and alternative care settings. The lactation nurse specialist coordinated the group’s efforts with input from the nurse executive. The perinatal nurse managers served as ad hoc members.
From our TQM training, we knew that a ~ ~~
Linda L. Clarke, RNC, MN, is a nurse manag- er in the neonatal intensive care unit, and Melodee I . Deutsch, RNC, MS, MPH, is a nurse executive for Maternal-Child Services, at the Moanalua Medical Center in Honolulu, HI. The authors gratefully acknowledge Me1 Clarke for the assistance in and support of the prepa- ration of this article. Baby-Friendly- is a registered trademark of Baby-Friendly USA and UNICEE
common strategy for quality improvement groups was to search for a “best practices” or model program. While reviewing the literature, the LAW discovered The Baby-FriendlyTM Hospital Initiative, which is a global program sponsored by the World Health Organization and the United Nations Children’s Fund (UNICEF) to encourage and recognize hospitals and birthing centers that offer optimal levels of lactation care. The Baby- FriendlyTM Hospital Initiative is administered in the U.S. through Baby-Friendly USA in Sandwich, MA, which was organized this year to raise the awareness of, and locally implement, the initiative.
Healthy People 2000 Goals of having 75 percent of newborns breastfeeding at hospital discharge by the year 2000 and 50 percent of newborns continuing breastfeeding for at least six months. The Baby- FriendlyTM Hospital Initiative plans to accomplish these goals by defining essential practices within hospitals and birthing centers that enable successful breastfeeding, according to Dr. Karin Cadwell, PhD, RN, IBCLC, chair of Baby-Friendly USA.
developed from the San Diego Lactation Program) authored breastfeeding policies advocating the forma- tion of interdisciplinary teams in hospitals that would be responsible for implementing lactation programs and ongoing educational activities (Powers et al, 1994). Wellstart worked with the World Health Organization and UNICEF to develop the cornerstone of the Baby- FriendlyTM Initiative. That definition of practice comes through what is called the “Ten Steps to Successful Breastfeeding” (Baby-Friendly USA, 1997):
The Baby-FriendlyTM Hospital Initiative supports US
As early as the 1980s, Wellstart International (which
1. Have a written breastfeeding policy that is routinely communicated to all health care staff.
2. Train all health care staff in skills necessary to implement this policy.
3. Inform all pregnant women about the benefits and management of breastfeeding.
4. Help mothers initiate breastfeeding within one hour of birth.
5. Show mothers how to breastfeed and how to main- tain lactation, even if they should be separated from their infants.
breast milk, unless medicaily indicated. 6. Give newborn infants no food or drink other than
32 L i f e l i n e s December 7997
13,000 hmyxtdk li424.W
7. Practice rooming-in-allow mothers and infants to remain together-24 hours a day.
8. Encourage breastfeeding on demand. 9. Give no artificial teats or pacifiers to breastfeeding
infants.
groups and refer mothers to them, on discharge from the hospital or clinic.
10. Foster the establishment of breastfeeding support
Hospitals that want to be recognized with the Baby- FriendlyTM Award can use the program to improve breastfeeding within their facility. In turn, they’ll receive a Certificate of Intent from the program, and upon suc- cessful completion of an assessment by Baby-Friendly USA the hospital will receive the Baby-Friendly Award. To date, 11 U.S. hospitals have been awarded Baby- FriendlyTM designations, although globally more than 13,000 hospitals have received the award. According to Baby-Friendly USA, more than 300 U.S. hospitals are now working their way through the program.
Working toward the Award In April 1994, we issued our letter of intent to become Baby-Friendlym, and on June 21, 1994, we received notice we were one of the first 200 hospitals and birthing centers in the U.S. to receive a Certificate of Intent. We celebrated. Then the real work began.
In our organization, the measure of success for any project is the ability to balance the needs of the health plan member for quality of care and service with cost- effective resources utilization. Because we set out first to meet customer needs, our decision to strive for becom- ing Baby-Friendlym grew out of wanting to fulfill that objective. Interestingly, we never asked for permission to pursue the Baby-FriendlyTM Award. We believed in total quality managemen5 we trusted the process. We had a supportive organizational culture, and we pursued the goal because it was the right thing to do for our CUS-
tomers. It fulfilled our mission of “Curing for Hawaii’s
People Like Fumily. ” That wave of energy carried us from vision in 1994 to the award in 1997
Implementing Baby-Friendlym How did we begin? We organized the “Ten Steps” into related groupings and set priorities. Because steps 1 and 2 focus on policy development and staff education, they provided a logical place to begin. Our existing policy was studied, revised, and implemented. It became the foundation for the rest of the plan. We have since learned that our foresight was right on target: When we provided prenatal education, we found that we had a higher percentage of mothers choosing to breastfeed. Our goal in educating women wasn’t to force them into a choice, or to make them feel guilty if they chose bottle feeding instead of breastfeeding. Rather, we wanted to be able to fully support their decisions when those deci- sions were made in the context of complete information about breastfeeding and bottle feeding.
We developed a curriculum for staff education. Faculty for the course included the lactation program coordinator, staff nurses, nurse practitioners, and a clinical nurse specialist, which, in our case, all hap- pened to be certified by the International Board of Lactation Consultant Examiners. All perinatal nurses completed a 16-hour workshop followed by a 3-hour supervised clinical experience. The course qualified
Strategies for Successful Organizational Change
1. Develop an interdisciplinary core team to oversee the project. Include key players across the continu- um. It is vital for success.
2. Develop an implementation plan and work the plan. Don‘t be afraid to reassess and reprioritize as you collect data and gain experience. If there is no plan, you will be overwhelmed.
3. Develop and implement a staff educationhraining program early in the project. It changes attitudes and behaviors and builds a critical mass of committed people.
4. Identify indicators of success early. Measure and assess them regularly. Use the information to make continuous improvements as you go. It builds support across the organization.
plan. Discuss the role of each player. Share the suc- cess measures. Be positive. Be flexible. Be willing to listen and make changes as the project evolves. Open communication is the key.
6. Stay focused on the vision. It will motivate you when nothing else does.
7. Celebrate! Reward your staff and yourself!
5. Involve all players. Paint the big picture. Share the
Source: Melodee Deutsch, RNC, MS, MPH.
December 1997 L i f e l i n e s 33
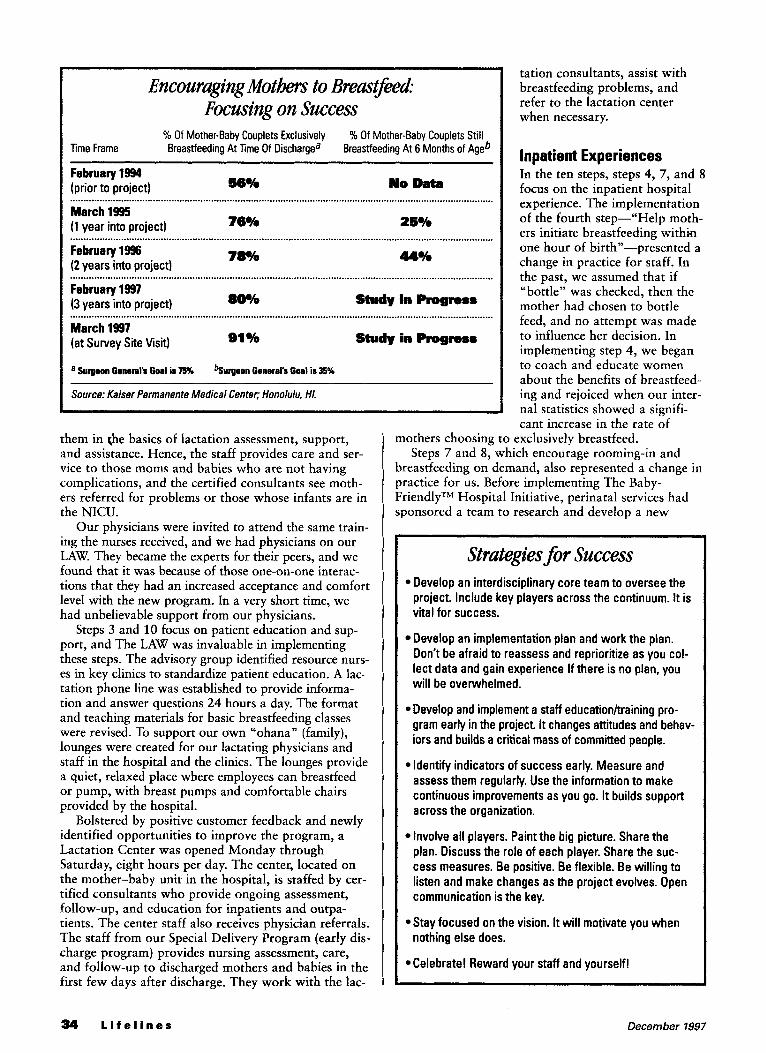
Encouraging Motks to Bwast&md.- Focusing on Success
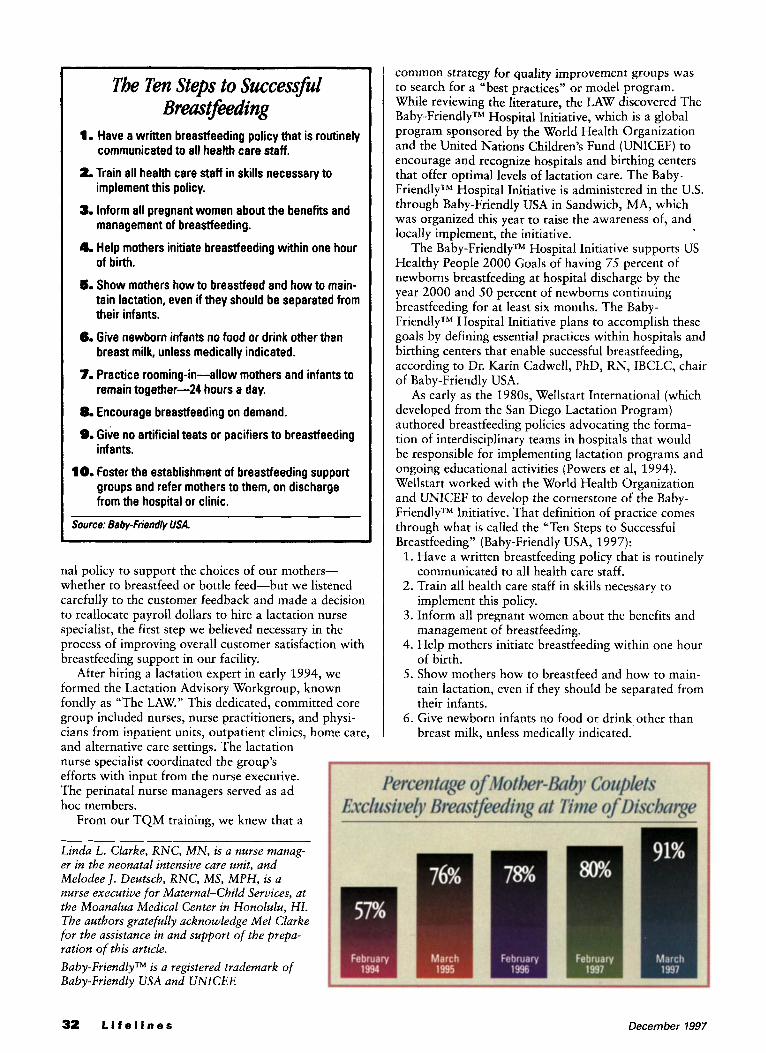
% Of Mother-Baby Couplets Exclusively Breastfeeding At Time Of Dischargea
% Of Mother-Baby Couplets Still Breastfeeding At 6 Months of Age6 Time Frame
February 1!W (prior to project) 56% No Data
March 1995 (1 year into project) 76% 25%
7836 February 1996 (2 years into project)
February 1997 (3 years into project) 8W/o Study in Rogreu
March 1997 (at Survey Site visit) 91%
a Surgeon Genaml’s Goal is 5% %urgeon Ganaralf Goal is 35%
Study in Pmgmu
Source: Kaiser Permanente Medical Center; Honolulu, HI.
them in t,he basics of lactation assessment, support, and assistance. Hence, the staff provides care and ser- vice to those moms and babies who are not having complications, and the certified consultants see moth- ers referred for problems or those whose infants are in the NICU.
Our physicians were invited to attend the same train- ing the nurses received, and we had physicians on our LAW. They became the experts for their peers, and we found that it was because of those one-on-one interac- tions that they had an increased acceptance and comfort level with the new program. In a very short time, we had unbelievable support from our physicians.
Steps 3 and 10 focus on patient education and sup- port, and The LAW was invaluable in implementing these steps. The advisory group identified resource nurs- es in key clinics to standardize patient education. A lac- tation phone line was established to provide informa- tion and answer questions 24 hours a day. The format and teaching materials for basic breastfeeding classes were revised. To support our own “ohana” (family), lounges were created for our lactating physicians and staff in the hospital and the clinics. The lounges provide a quiet, relaxed place where employees can breastfeed or pump, with breast pumps and comfortable chairs provided by the hospital.
identified opportunities to improve the program, a Lactation Center was opened Monday through Saturday, eight hours per day. The center, located on the mother-baby unit in the hospital, is staffed by cer- tified consultants who provide ongoing assessment, follow-up, and education for inpatients and outpa- tients. The center staff also receives physician referrals. The staff from our Special Delivery Program (early dis- charge program) provides nursing assessment, care, and follow-up to discharged mothers and babies in the first few days after discharge. They work with the lac-
Bolstered by positive customer feedback and newly
tation consultants, assist with breastfeeding problems, and refer to the lactation center when necessary.
Inpatient Experiences In the ten steps, steps 4, 7, and 8 focus on the inpatient hospital experience. The implementation of the fourth step--“Help moth- ers initiate breastfeeding withia one hour of birth”-presented a change in practice for staff. In the past, we assumed that if “bottle” was checked, then the mother had chosen to bottle feed, and no attempt was made to influence her decision. In implementing step 4, we began to coach and educate women about the benefits of breastfeed- ing and rejoiced when our inter- nal statistics showed a signifi- cant increase in the rate of
mothers choosing to exclusively breastfeed. Steps 7 and 8, which encourage rooming-in and
breastfeeding on demand, also represented a change in practice for us. Before implementing The Baby- FriendlyTM Hospital Initiative, perinatal services had sponsored a team to research and develop a new
Strategies for Success Develop an interdisciplinary core team to oversee the project. Include key players across the continuum. It is vital for success.
Don’t be afraid to reassess and reprioritize as you col- lect data and gain experience If there is no plan, you will be overwhelmed.
Develop an implementation plan and work the plan.
Develop and implement a staff educationhraining pro- gram early in the project It changes attitudes and behav- iors and builds a critical mass of committed people.
Identify indicators of success early. Measure and assess them regularly. Use the information to make continuous improvements as you go. It builds support across the organization.
plan. Discuss the role of each player. Share the suc- cess measures. Be positive. Be flexible. Be willing to listen and make changes as the project evolves. Open communication is the key.
nothing else does.
Involve all players. Paint the big picture. Share the
Stay focused on the vision. It will motivate you when
Celebrate! Reward your staff and yourself!
34 L i f e l i n e s December 1997
model of patient care. We were still p the traditional laboddelivery-postpar ery concept, but knew that we wan newborns in the rooms with the mothers. A new moth- er-baby unit was devised, and on a beautiful tropical morning in February 1995, we moved our first m&er and baby together from labor and delivery to the newly blessed mother-baby unit.
We no longer have an admission nursery-the new- borns stay with the mom in her room at all times. Our only nursery is in our NICU. And in those special cir- cumstances where perhaps mom is out of the room for a postpartum sterilization, we encourage the fathers, sup- port persons, and other family members to stay with the baby and continue to feed it the mother’s expressed breast milk. If there’s no one to stay with the baby, the nurses either stay in the room with the baby or take himher out to the nurses’ station-we didn’t want to put anything permanent into place that might become an old central nursery again. All nursing care, physician examinations, laboratory work, hearing screening, and even picture-taking are done at the mother’s bedside. The new family is assigned to one nurse who, with the guidance of an interdisciplinary care map, coordinates the care to meet individual mom and baby needs. These earlier steps helped us with the Ten Steps of the Baby- FriendlyTM Initiative.
Artificial Methods Steps 6 and 9 focus on feeding the baby breast milk only and restraining from artificial teats and pacifiers. The campaign to discourage pacifiers for well babies had begun before getting the Baby-FriendlyTM Award and was well under way. We had already established a policy to purchase only those suitable for the prema- ture or ill infant and keep them in the NICU. Parents of healthy infants are cautioned about the confusion and problems associated with pacifier use before breast feeding.
The intent of the sixth step is that formula is treat- ed as any other dietary supplement and is purchased. With the support of hospital administration and our purchasing department, we negotiated contracts with our vendors. The contracts cover the purchase of for- mula, nipples, and supplies given to moms for storing breast milk. No discharge packs are given, and no lit- erature printed by formula companies is distributed in the hospital.
Step 5 focuses on separation of mother and baby and emphasizes continued breastfeeding even when sep- arated. We considered it the most challenging step for hospitals that provide high-risk maternity care and neonatal intensive care. We were fortunate. Long before we knew about the Baby-FriendlyTM Initiative, the physicians and nurses in our NICU encouraged and supported the use of breast milk as the primary source of nutrition for premature and sick babies. However, we had inconsistent methods for obtaining and storing the breast milk. The policies and practice were revised based on current recommendations. Cup feeding of expressed breast milk instead of nipple feeding is now standard practice in our NICU. More importantly,
genefits of a Comprehensive hetation Program
Improved Can, and Service to Members Continuity of care and service across the outpatient-
Prevention of critical events related to inaccurate or
High level service to young families at a criical time
inpatient-home-community continuum
inconsistent information and triage
Utilization of Resources
Fewer telephone calls to physicians, advice nurses, clinics and emergency services
Fewer unnecessary visits to physicians, clinics and emergency services
Prevention of critical incidents resulting in hospital readmission
Promotion of health in women; breastfeeding decreases incidence of abuse and breast cancer
Prevention of infant and childhood illnesses; breast- fed babies are healthier
Prevention of criiical events leading to risk manage- ment issues
Positive Public Image
First comprehensive program in the state
Highly valued service for women making health care
Quality oriented and customer focused
Retention and recruitment of health plan members
decision for their families
mothers and fathers at the bedside are taking of nurses, bottles, and pacifiers.
Kangaroo Care, originally encouraged to B development and enhance the well-being of ture infant, is practiced in our unit as a first step in encouraging suckling and latch-on for infants separated from their mothers. These tiny, fragile babies teach us what nature has always known-nurturing is a recipro- cal process and mothers and babies do it best.
In the Process Implementing the Baby-Friendlym Initiative creates sig- nificant challenges for an organization. We identified the three overall types of challenges in identifying our implementation strategies: the facility, the policies and procedures, and the people. Because people can manage a facility and make it work and people can change poli- cies and procedures to match their practice, we decided our greatest investment of time and energy would be with staff.
customer needs and were motivated to learn. Although We believed a majority of our nurses wanted to meet
December 7997 L i f e l i n e s 35
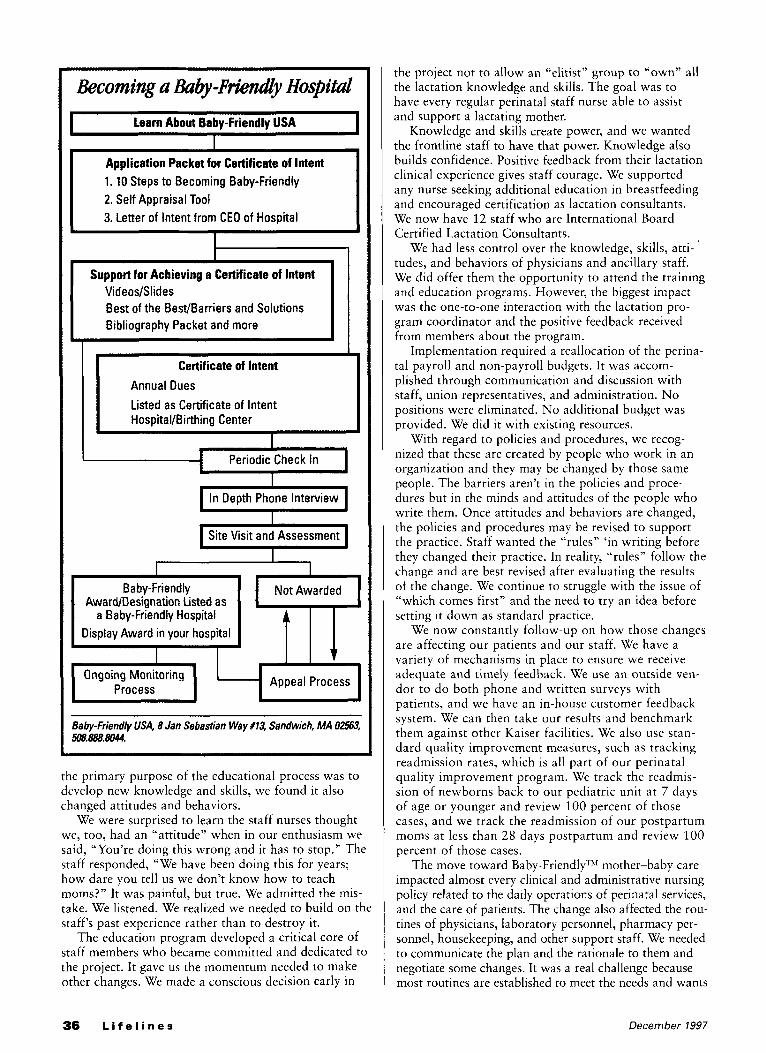
Becoming a &by-F&dy Hospital I learn About Babv-Friendlv USA
Application Packet for Certificate of Intent 1. 10 Steps to Becoming Baby-Friendly 2. Self Appraisal Tool 3. Letter of Intent from CEO of Hospital
Support for Achieving a Certificate of Intent VideoslSlides Best of the BestBarriers and Solutions Bibliography Packet and more
Certificate of Intent Annual Dues Listed as Certificate of Intent Hospital/Birthing Center
~
I Periodic Check In
I In Depth Phone Interview
I Site Visit and Assessment
I
1 I
I I Baby-Friendly Not Awarded
AwardIDesignation Listed as
I I
a Baby-Friendly Hospital Display Award in your hospital
Appeal Process
Baby-Friendly USA, 8 Jan Sebastian Way f13, Sandwich, MA 0256 508.888.8044.
the primary purpose of the educational process was to develop new knowledge and skills, we found it also changed attitudes and behaviors.
We were surprised to learn the staff nurses thought we, too, had an “attitude” when in our enthusiasm we said, “You’re doing this wrong and it has to stop.” The staff responded, “We have been doing this for years; how dare you tell us we don’t know how to teach moms?” It was painful, but true. We admitted the mis- take. We listened. We realized we needed to build on the staff’s past experience rather than to destroy it.
The education program developed a critical core of staff members who became committed and dedicated to the project. It gave us the momentum needed to make other changes. We made a conscious decision early in
the project not to allow an “elitist” group to “own” all the lactation knowledge and skills. The goal was to have every regular perinatal staff nurse able to assist and support a lactating mother.
Knowledge and skills create power, and we wanted the frontline staff to have that power. Knowledge also builds confidence. Positive feedback from their lactation clinical experience gives staff courage. We supported any nurse seeking additional education in breastfeeding and encouraged certification as lactation consultants. We now have 12 staff who are International Board Certified Lactation Consultants.
We had less control over the knowledge, skills, atti- tudes, and behaviors of physicians and ancillary staff. We did offer them the opportunity to attend the training and education programs. However, the biggest impact was the one-to-one interaction with the lactation pro- gram coordinator and the positive feedback received from members about the program.
tal payroll and non-payroll budgets. It was accom- plished through communication and discussion with staff, union representatives, and administration. No positions were eliminated. No additional budget was provided. We did it with existing resources.
With regard to policies and procedures, we recog- nized that these are created by people who work in an organization and they may be changed by those same people. The barriers aren’t in the policies and proce- dures but in the minds and attitudes of the people who write them. Once attitudes and behaviors are changed, the policies and procedures may be revised to support the practice. Staff wanted the “rules” ‘in writing before they changed their practice. In reality, “rules” follow the change and are best revised after evaluating the results of the change. We continue to struggle with the issue of “which comes first” and the need to try an idea before setting it down as standard practice.
are affecting our patients and our staff. We have a variety of mechanisms in place to ensure we receive adequate and timely feedback. We use an outside ven- dor to do both phone and written surveys with patients, and we have an in-house customer feedback system. We can then take our results and benchmark them against other Kaiser facilities. We also use stan- dard quality improvement measures, such as tracking readmission rates, which is all part of our perinatal quality improvement program. We track the readmis- sion of newborns back to our pediatric unit at 7 days of age or younger and review 100 percent of those cases, and we track the readmission of our postpartum moms a t less than 28 days postpartum and review 100 percent of those cases.
impacted almost every clinical and administrative nursing policy related to the daily operations of perinatal services, and the care of patients. The change also affected the rou- tines of physicians, laboratory personnel, pharmacy per- sonnel, housekeeping, and other support staff. We needed to communicate the plan and the rationale to them and negotiate some changes. It was a real challenge because most routines are established to meet the needs and wants
Implementation required a reallocation of the perina-
We now constantly follow-up on how those changes
The move toward Baby-Friendly ’” mother-baby care
36 L i f e l i n e s December 1997
of the provider rather than those of the member/patient. Open communication and a willingness to listen led US to consensus on key issues. We continue to involve key play- ers in planning change and program improvement.
The decision to purchase formula and formula prod- ucts is a major barrier for some facilities, and since hos- pitals typically receive them for free from manufacturers there’s typically little knowledge about the quantity or cost of the stock used. We tracked our usage of items for several months to develop an estimate of the cost, which was approximately $25,000 last year on all prod- ucts for the mother-baby unit and the NICU. Some nurses and physicians thought it was impractical to refuse “free” products. We believed it was a practical decision in keeping with our new plan of providing the best in service and education to our customers. It was the right time to do the right thing.
looking Ahead We were successful in implementing the Ten Steps. In May 1997, we received a letter stating, “I am pleased to inform you that Kaiser Permanente Moanalua Medical Center, Honolulu, Hawaii, has officially been designated a Baby-FriendlyTM Hospital, the second in the United States and the first in Hawaii.”
determination to meet customer needs pushed us to becoming Baby-FriendlyTM. The vision endures and
Passion created the dream, energy gave it life, and a
Baby -Friend@ r‘‘ Hospitals As of October 1997, the following U.S. hospitals have received the Baby-Friendly” Award:
Alice Peck Day Memorial Hospital; Lebanon, NH
Cottage Grove Hospital Birthing Center; Cottage
Evergreen Hospital Medical Center; Kirkland, WA
Grove, OR
(Note: Evergreen was the first U.S. hospital to receive the award)
Franciscan Hospital; Mt. Airy Campus; Cincinnati, OH
Goleta Valley Cottage Hospital; Santa Barbara, CA
Kaiser Permanente Medical Center; Honolulu, HI
Mid-Michigan Regional Medical Center; Midland, MI
Miles Memorial Hospital; Damariscotta, ME
PeaceHealth Nurse Midwifery; Eugene, OR
Reading Birth and Women’s Center; Reading, PA
Women’s Health and Birth Center; Santa Rosa, CA
For information about the Baby-FriendlyTM Hospital Initiative, contact:
1 Baby-Friendly USA
, 8 Jan Sebastian Way, #13 Sandwich, M A 02563
, (508) 888-8044
expands. There is no end to our story-only new oppor- tunities. We continue to provide education and training to nurses, physicians, and other support staff. We have taken the program to our neighbor island staff and clin- ic facilities. We plan to open more mother’s lounges in outlying clinics and ancillary locations. The lactation center concept will be expanded to be strategically located clinics elsewhere on Oahu so new moms and babies may be seen closer to home. We hope to make the lactation phone line available to the community as a service of Kaiser Permanente.
Knowing that research and education will dictate more revisions in the future, we have revised policies, procedures, teaching forms, and care maps. The sale of lactation supplies in the lactation center has outgrown our fee-for-service expertise. The business is being trans- ferred to our “over-the-counter” pharmacy.
For us, it has never been about the award or recog- nition. It’s about healthy babies who can grow to be healthy children in nurturing families. It’s about a phi- losophy of care-an attitude communicated by care- givers in an environment of love, assistance, and encouragement. + References Baby-Friendly USA: Implementing the UNICEF Baby-Friendly
Hospital Initiative in the United States. (1997). Commemorative, August 1997. Baby-Friendly, USA; Sandwich, MA: Author.
Bridges, W. (1980). Transitions. New York: Addison-Wesley Publishing Co., Inc.
Bridges, W. (1991). Managing transitions. New York: Addison- Wesley Publishing Co.
Heifetz, M. L. (1993). Leading change, overcoming chaos. Berkeley, CA: Ten Speed Press.
Powers, N. G., Naylor, A. J., & Wester, R. (1994). Hospital policies: Crucial to breastfeeding success. Seminars in Perinatology, 18, 517-524.
US Committee for UNICEFlWellstart International. (March 1996). US Baby-Friendly Hospital Initiative Guidelines and Criteria.
US Committee for UNICEFlWellstart International. (March 1996). The Guidelines and Evaluation Criteria for HospitaVBirthing Center Level Implementation of the United States Baby-Friendly Hospital Initiative.
December 1997 L i f e l i n e s 37
Related Documents