Basic Psychological Treatments: Cognitive Behaviour Therapy (CBT) Dr Simon Reid Milligan Forensic Psychologist Roseberry Park Hospital, Tees, Esk and Wear Valleys (TEWV) NHS Foundation Trust

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Basic Psychological Treatments: Cognitive Behaviour Therapy (CBT)
Dr Simon Reid Milligan
Forensic Psychologist
Roseberry Park Hospital,
Tees, Esk and Wear Valleys (TEWV) NHS Foundation Trust
Session outline
1. Theory • Background
- Behavioural Theory
- Cognitive Theory
- CBT assumptions
• Levels of Thoughts
- Core Beliefs (Schemas)
- Underlying Assumptions
- Negative Automatic Thoughts
• Compensatory Strategies
• Problems
• Example
Session outline
2. Therapy
• Principles of CBT
• Assessment
• Treatment strategies
• Questions
NICE guidelines recommend CBT for a wide range of mental disorders. It is commonly used as a psychological treatment for:
• Depression
• Anxiety
• Phobias (including Social Phobia)
• Panic Disorder
• OCD
• GAD
• PTSD
• Schizophreniform disorders
• Bipolar Disorder
• Problems associated with some personality disorders (BPD, APD)
• Pain management
Theoretic model
• Two broad assumptions:
(i) bio-psychosocial context – development and maintenance of disorders
(ii) perception and agency are the focus of therapy
• Problematic thoughts, feelings and behavioural patterns are learned via the same processes of normal thoughts, feelings and behaviour
• Therapy
- constituent habits which comprise the disorder are identified through interview and observation
- involves coaching adaptive patterns of thoughts, feelings and behaviours
- challenge non-adaptive beliefs
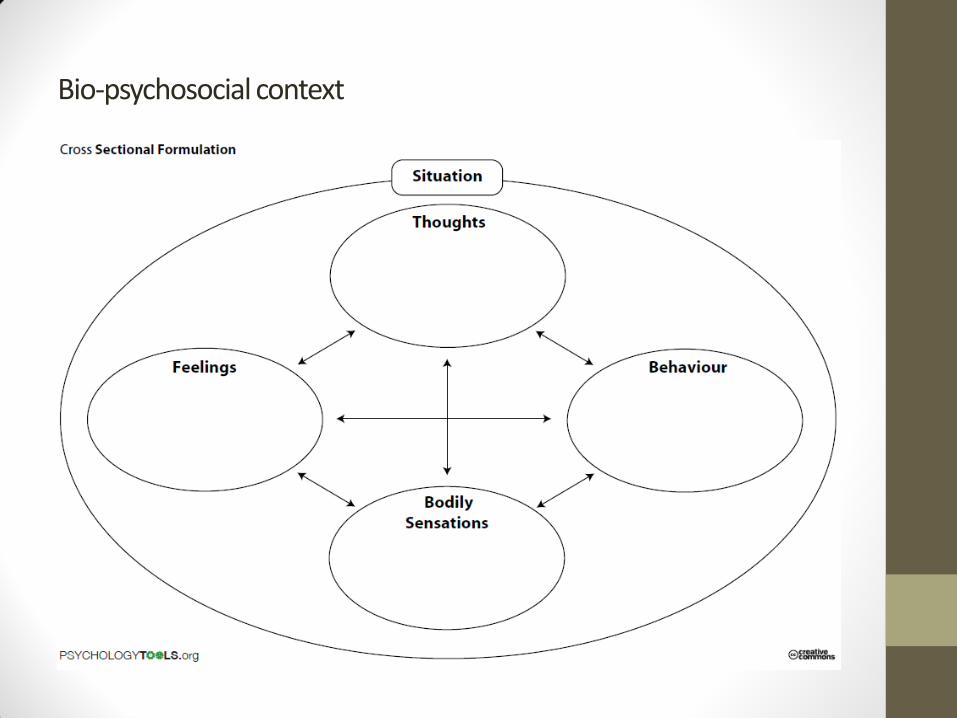
Bio-psychosocial context
Behavioural Theory
• Behaviour is functional – it serves a purpose, even if it’s maladaptive
• Patterns of behaviour are the result of learning and anticipated consequence (conscious or not)
• Emphasis is on the external antecedents and consequences
• Antecedent – Behaviour - Consequence
Behavioural Theory
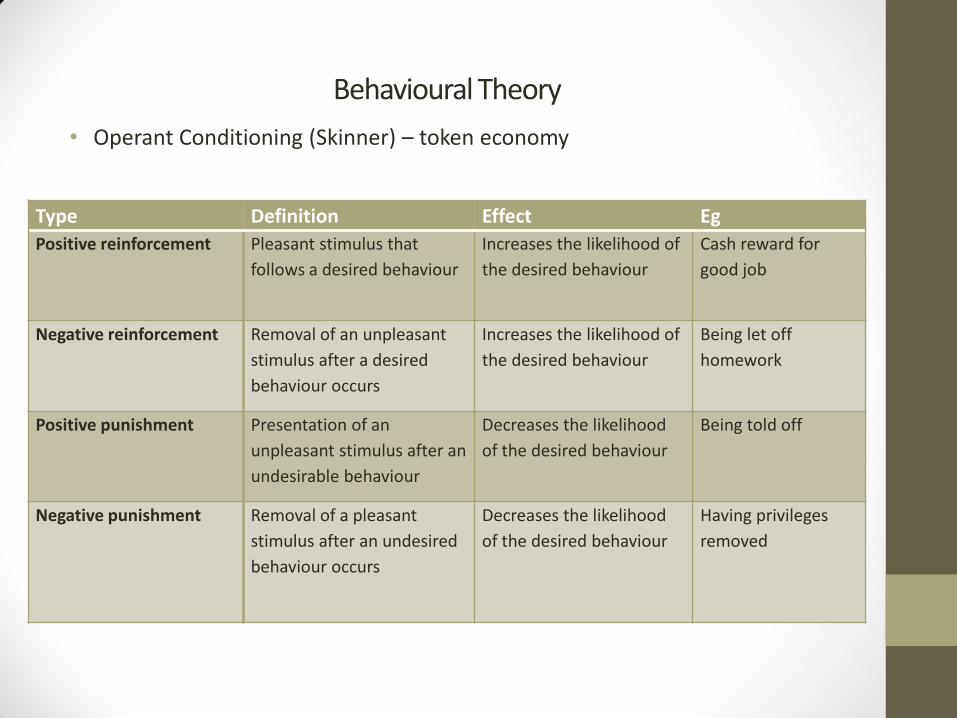
• Operant Conditioning (Skinner) – token economy
Type Definition Effect Eg
Positive reinforcement Pleasant stimulus that
follows a desired behaviour
Increases the likelihood of
the desired behaviour
Cash reward for
good job
Negative reinforcement Removal of an unpleasant
stimulus after a desired
behaviour occurs
Increases the likelihood of
the desired behaviour
Being let off
homework
Positive punishment Presentation of an
unpleasant stimulus after an
undesirable behaviour
Decreases the likelihood
of the desired behaviour
Being told off
Negative punishment Removal of a pleasant
stimulus after an undesired
behaviour occurs
Decreases the likelihood
of the desired behaviour
Having privileges
removed
REINFORCEMENT – increases likelihood of a behaviour (makes you want to do it again)
Positive reinforcement
• gives you something desirable
REINFORCEMENT
Negative reinforcement
• Takes something aversive away
PUNISHMENT – makes you less likely to do something
Positive punishment
• Gives you something aversive

PUNISHMENT
Negative Punishment
• taking away something you want
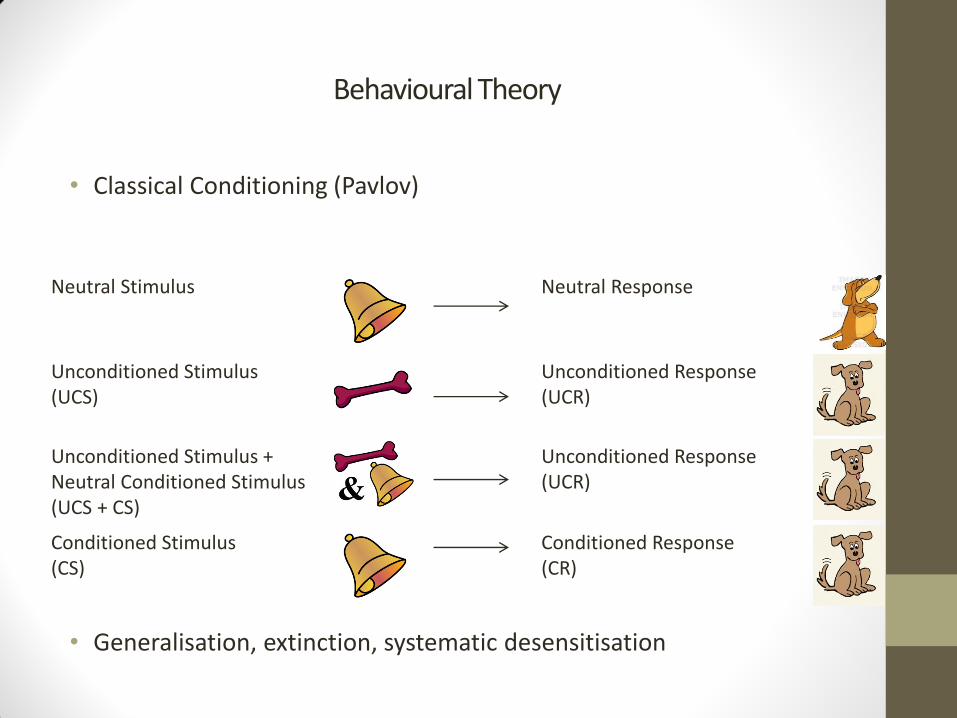
Behavioural Theory
• Classical Conditioning (Pavlov)
• Generalisation, extinction, systematic desensitisation
Neutral Stimulus Neutral Response
Unconditioned Stimulus (UCS)
Unconditioned Response (UCR)
Unconditioned Stimulus + Neutral Conditioned Stimulus (UCS + CS)
Unconditioned Response (UCR)
Conditioned Stimulus (CS)
Conditioned Response (CR)
Cognitive Theory
• Focus on distal developmental factors
• How we feel and behave is dependent upon how we interpret an event
• How we interpret an event is dependent upon what we believe about the world, and assumptions we make
• Emotional disorders stem from maladaptive patterns of interpretation and behaviour
• Therapy involves evaluating and modifying dysfunctional beliefs with healthier and more adaptive beliefs
(Johnstone & Dallos)
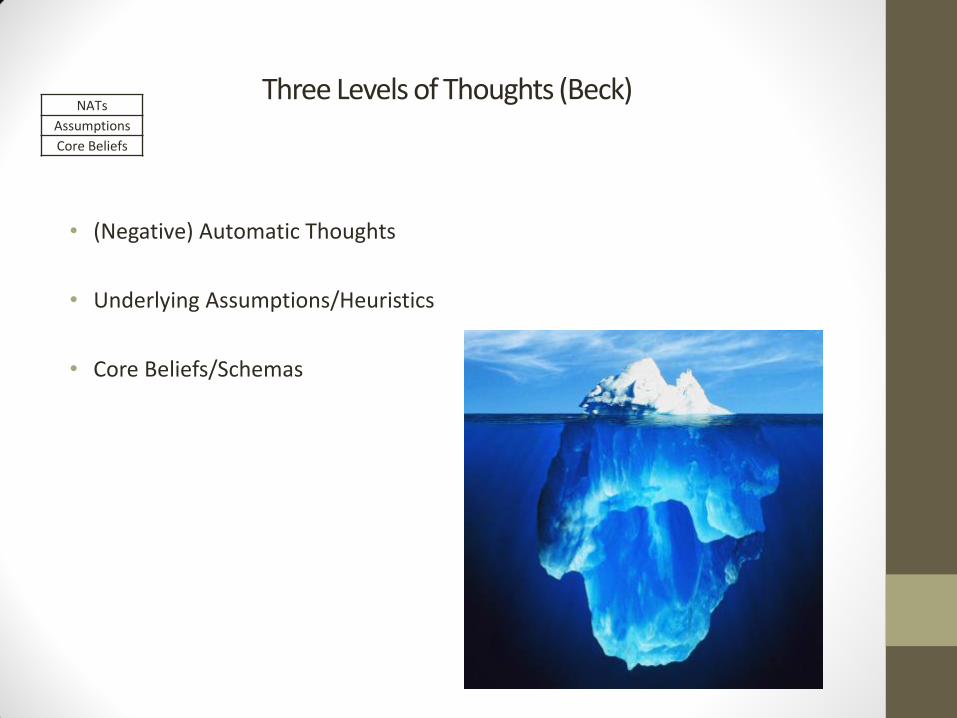
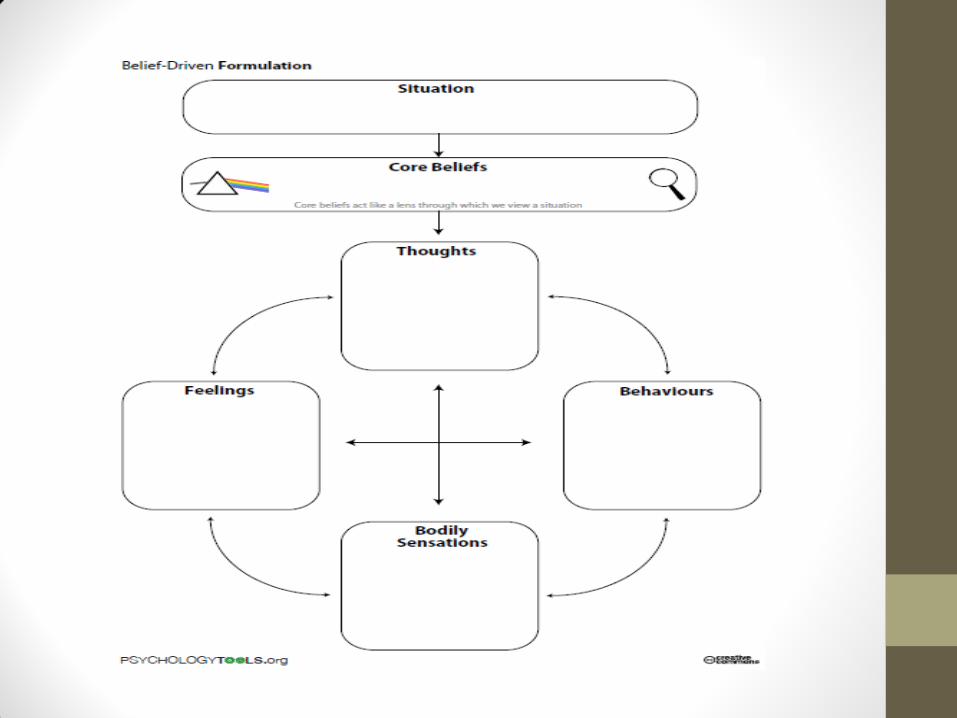
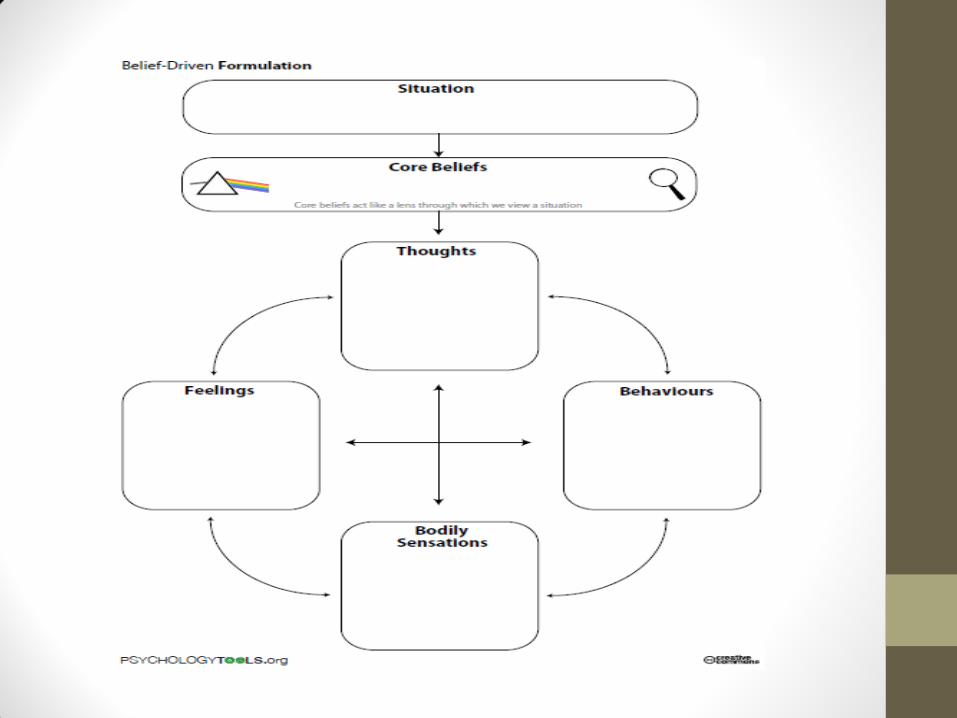
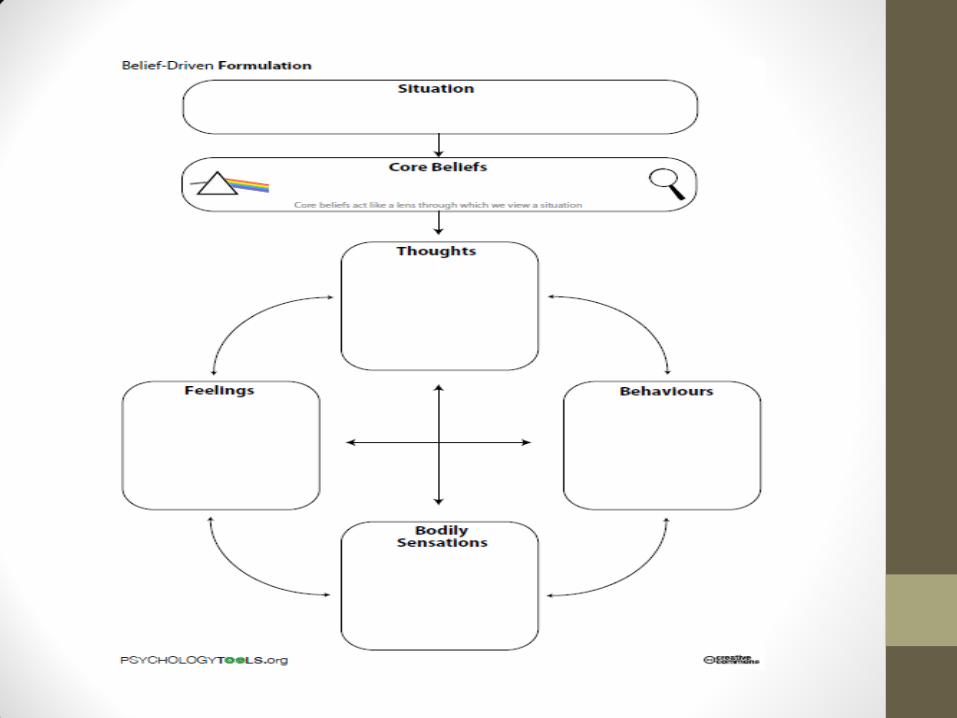
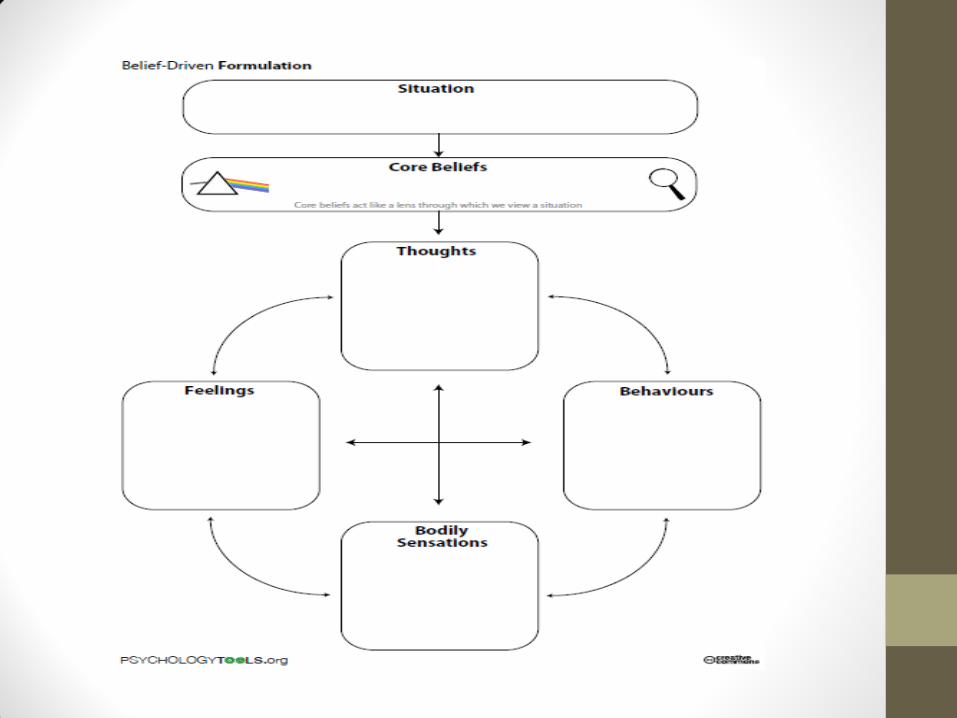
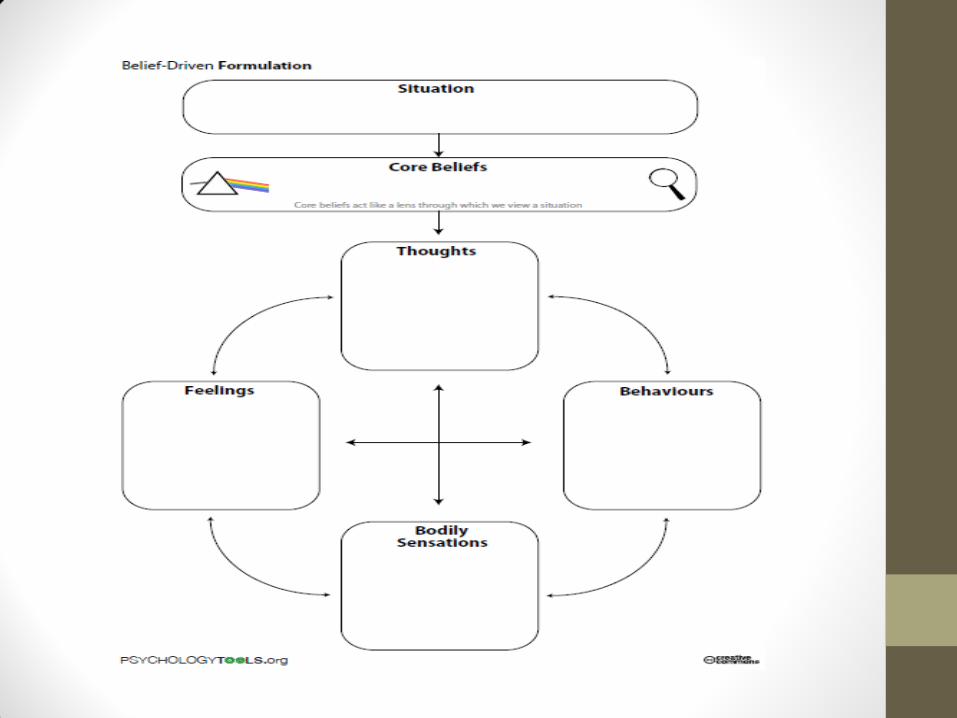
Three Levels of Thoughts (Beck)
• (Negative) Automatic Thoughts
• Underlying Assumptions/Heuristics
• Core Beliefs/Schemas
NATs
Assumptions
Core Beliefs
Core Beliefs (schemas)
• Built up through early experiences, including significant events, interactions with parents, siblings, teachers, peers, developmental experiences
• Define a person
• Pervasive and enduring (characterise aspects of personality)
• Fundamental and absolute
• Cognitive triad – thoughts and expectations about world, self and others
NATs
Assumptions
Core Beliefs
Core Beliefs (schemas)
• A schema is a cluster of core beliefs
• Beliefs can be active, inactive or latent
• Most people have core beliefs on a continuum,
- eg “I/others/world are sometimes...”
“I am generally ok”
“Other people are mostly alright”
“The world usually provides”
• Problem experiences can lead to the development of maladaptive schemas
NATs
Assumptions
Core Beliefs
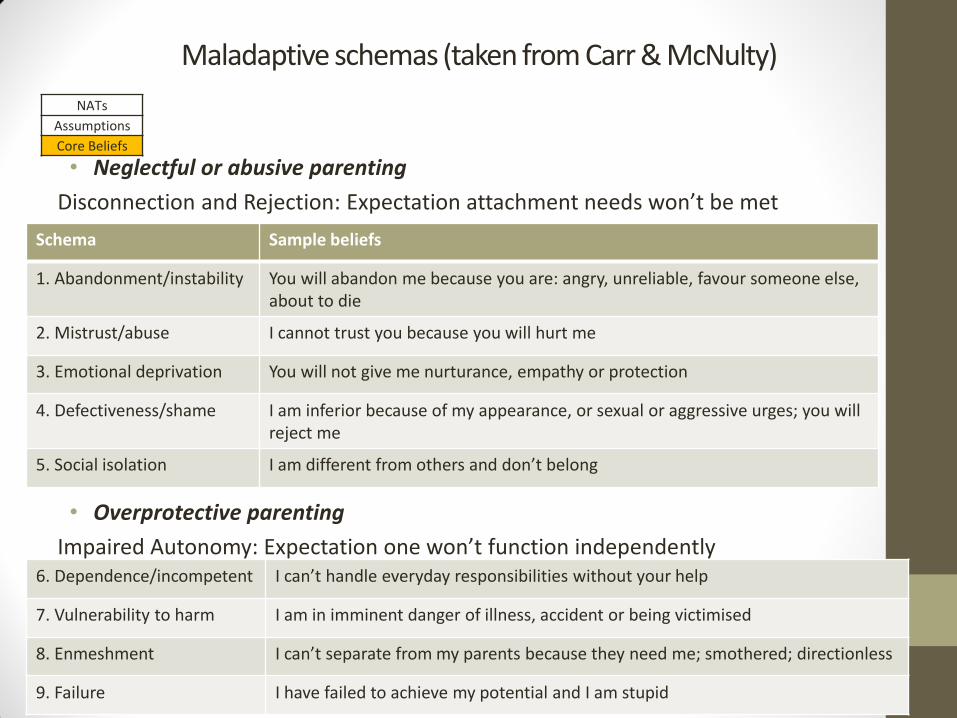
Maladaptive schemas (taken from Carr & McNulty)
• Neglectful or abusive parenting
Disconnection and Rejection: Expectation attachment needs won’t be met
• Overprotective parenting
Impaired Autonomy: Expectation one won’t function independently
Schema Sample beliefs
1. Abandonment/instability You will abandon me because you are: angry, unreliable, favour someone else, about to die
2. Mistrust/abuse I cannot trust you because you will hurt me
3. Emotional deprivation You will not give me nurturance, empathy or protection
4. Defectiveness/shame I am inferior because of my appearance, or sexual or aggressive urges; you will reject me
5. Social isolation I am different from others and don’t belong
6. Dependence/incompetent I can’t handle everyday responsibilities without your help
7. Vulnerability to harm I am in imminent danger of illness, accident or being victimised
8. Enmeshment I can’t separate from my parents because they need me; smothered; directionless
9. Failure I have failed to achieve my potential and I am stupid
NATs
Assumptions
Core Beliefs
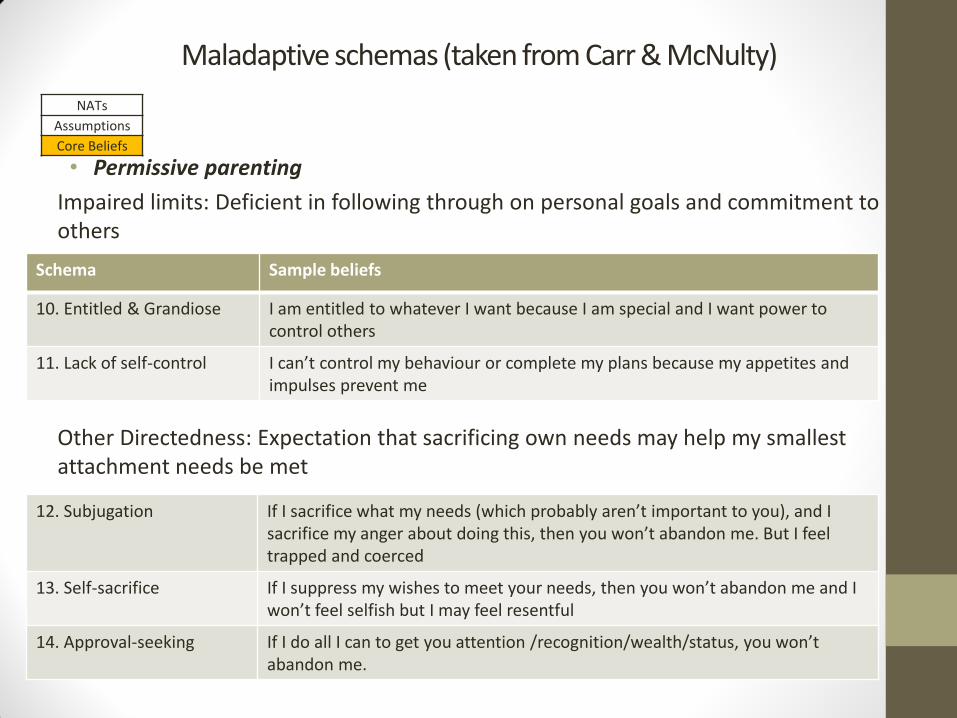
Maladaptive schemas (taken from Carr & McNulty)
• Permissive parenting
Impaired limits: Deficient in following through on personal goals and commitment to others
Other Directedness: Expectation that sacrificing own needs may help my smallest attachment needs be met
Schema Sample beliefs
10. Entitled & Grandiose I am entitled to whatever I want because I am special and I want power to control others
11. Lack of self-control I can’t control my behaviour or complete my plans because my appetites and impulses prevent me
12. Subjugation If I sacrifice what my needs (which probably aren’t important to you), and I sacrifice my anger about doing this, then you won’t abandon me. But I feel trapped and coerced
13. Self-sacrifice If I suppress my wishes to meet your needs, then you won’t abandon me and I won’t feel selfish but I may feel resentful
14. Approval-seeking If I do all I can to get you attention /recognition/wealth/status, you won’t abandon me.
NATs
Assumptions
Core Beliefs
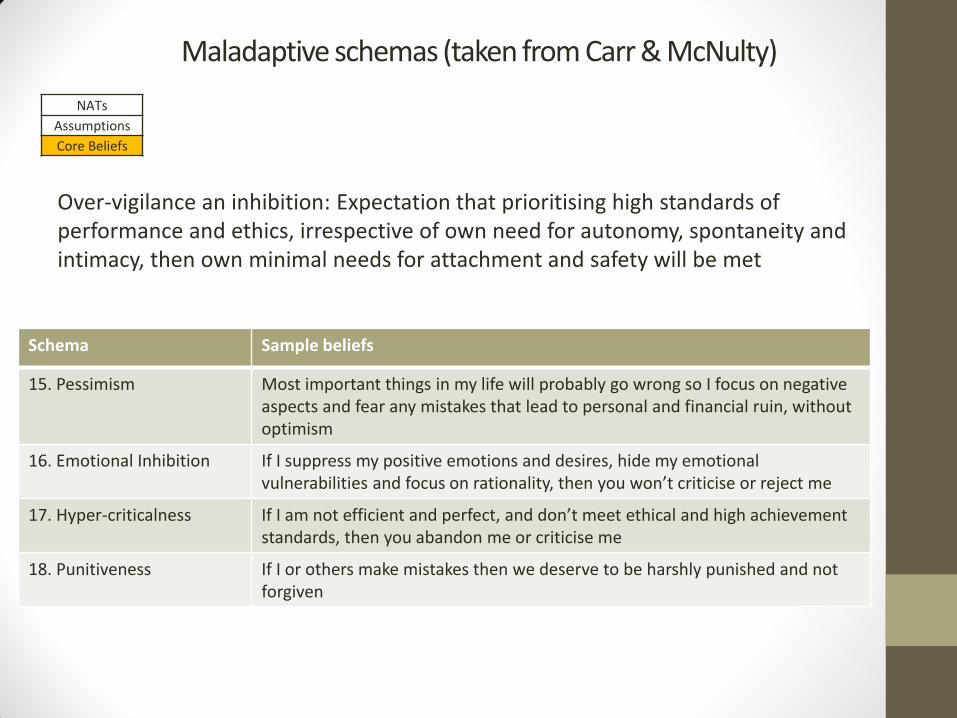
Maladaptive schemas (taken from Carr & McNulty)
Over-vigilance an inhibition: Expectation that prioritising high standards of performance and ethics, irrespective of own need for autonomy, spontaneity and intimacy, then own minimal needs for attachment and safety will be met
Schema Sample beliefs
15. Pessimism Most important things in my life will probably go wrong so I focus on negative aspects and fear any mistakes that lead to personal and financial ruin, without optimism
16. Emotional Inhibition If I suppress my positive emotions and desires, hide my emotional vulnerabilities and focus on rationality, then you won’t criticise or reject me
17. Hyper-criticalness If I am not efficient and perfect, and don’t meet ethical and high achievement standards, then you abandon me or criticise me
18. Punitiveness If I or others make mistakes then we deserve to be harshly punished and not forgiven
NATs
Assumptions
Core Beliefs
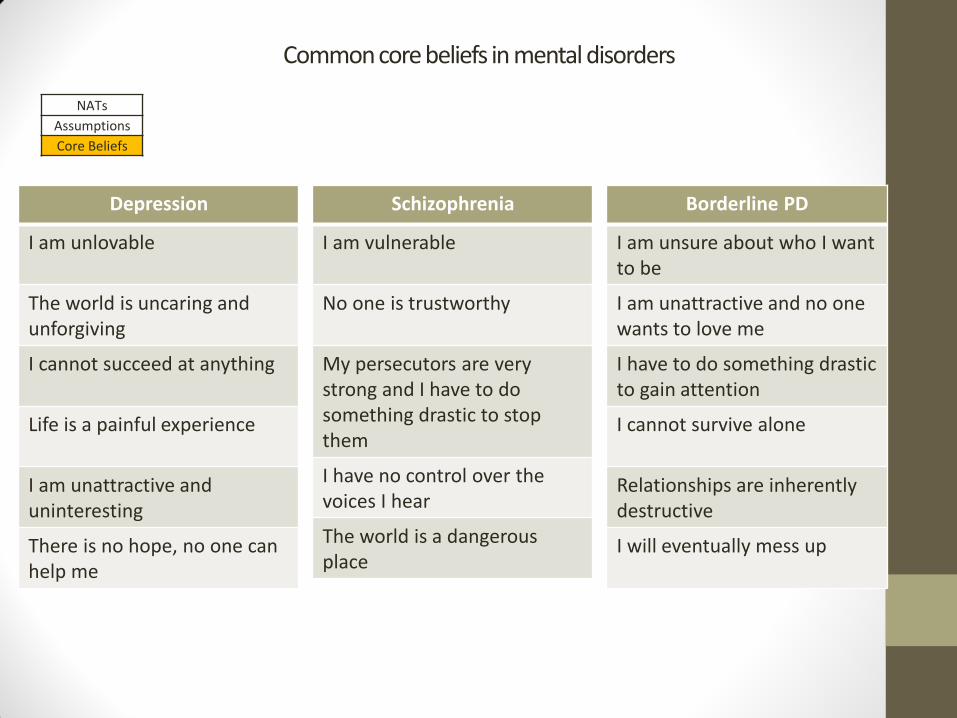
Common core beliefs in mental disorders
Depression
I am unlovable
The world is uncaring and unforgiving
I cannot succeed at anything
Life is a painful experience
I am unattractive and uninteresting
There is no hope, no one can help me
Schizophrenia
I am vulnerable
No one is trustworthy
My persecutors are very strong and I have to do something drastic to stop them
I have no control over the voices I hear
The world is a dangerous place
Borderline PD
I am unsure about who I want to be
I am unattractive and no one wants to love me
I have to do something drastic to gain attention
I cannot survive alone
Relationships are inherently destructive
I will eventually mess up
NATs
Assumptions
Core Beliefs
Assumptions/Heuristics
• Assumptions and rules emerge which are consistent with our core beliefs.
• Theories about how we and the world should operate
• Conditional:
“If…., then…”
• Example
Belief: I am unlovable
Assumption: If I am not in a relationship, then I am unlovable
Rule: I must be in a relationship, otherwise I am unlovable
• “If a client doesn’t improve, then…”
NATs
Assumptions
Core Beliefs
Assumptions/Heuristics
• Heuristics are rules for living which form from our underlying assumptions
- I should/I must…
- If I do…, then…will happen
- If I don’t…, then I am…
NATs
Assumptions
Core Beliefs
(Negative) Automatic Thoughts
• “Hot thoughts”
• Internal dialogue
• Triggered by specific situations (precipitating event)
• Emotionally-laden
• Immediate
• Seem real and logical to the client
• Typically accompanied by physiological response
• Inform our behaviour
What goes through your mind when walking into a room full of people you don’t know
Fight or flight
NATs
Assumptions
Core Beliefs
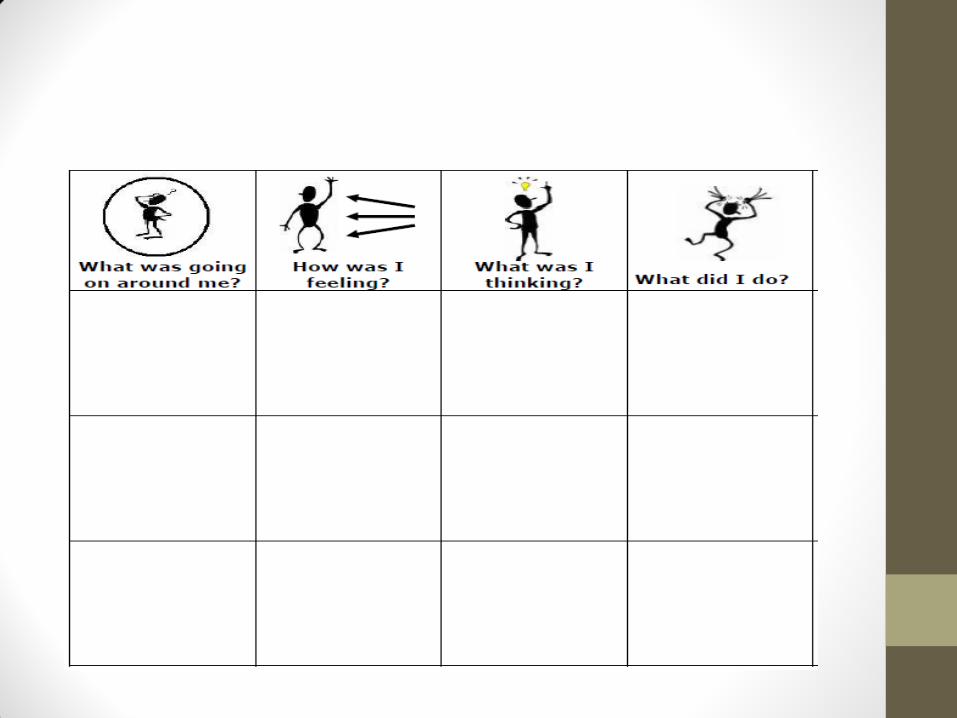
Spotting our own automatic thoughts
• What goes through your mind? • Words…
• Pictures…
• Sounds…
• Memories…
• How do you feel physically?
• Do you have any urges?
Automatic Thoughts?
Automatic Thoughts?
Automatic Thoughts?
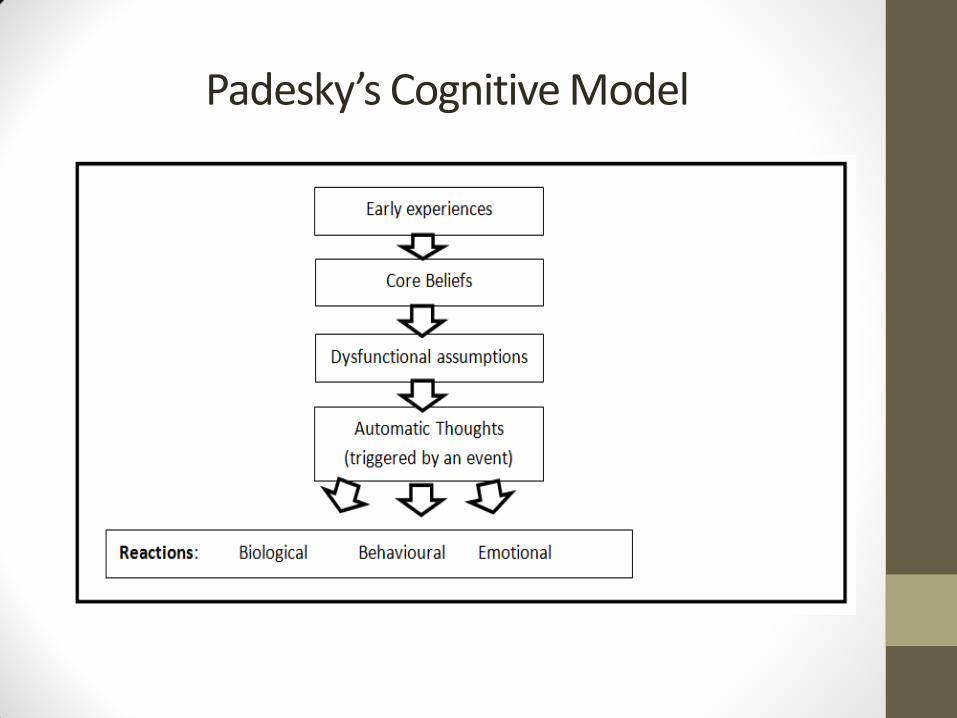
Padesky’s Cognitive Model
Compensatory Strategies (behaviour)
• Behaviour serves a function. Antecedent – Behaviour - Consequences
Eg - Child gets a biscuit after screaming and shouting – he is likely to repeat the behaviour the next time he wants one
• We act to compensate for our core beliefs
Eg – I am unlovable. If I am not in a relationship then I am unlovable. Try to establish relationship
• Sometimes the behaviour is functional but maladaptive (problematic or risky).
Eg’s
- deliberate self-harm
- promiscuity
- withdrawal (isolation)
- eating disorders
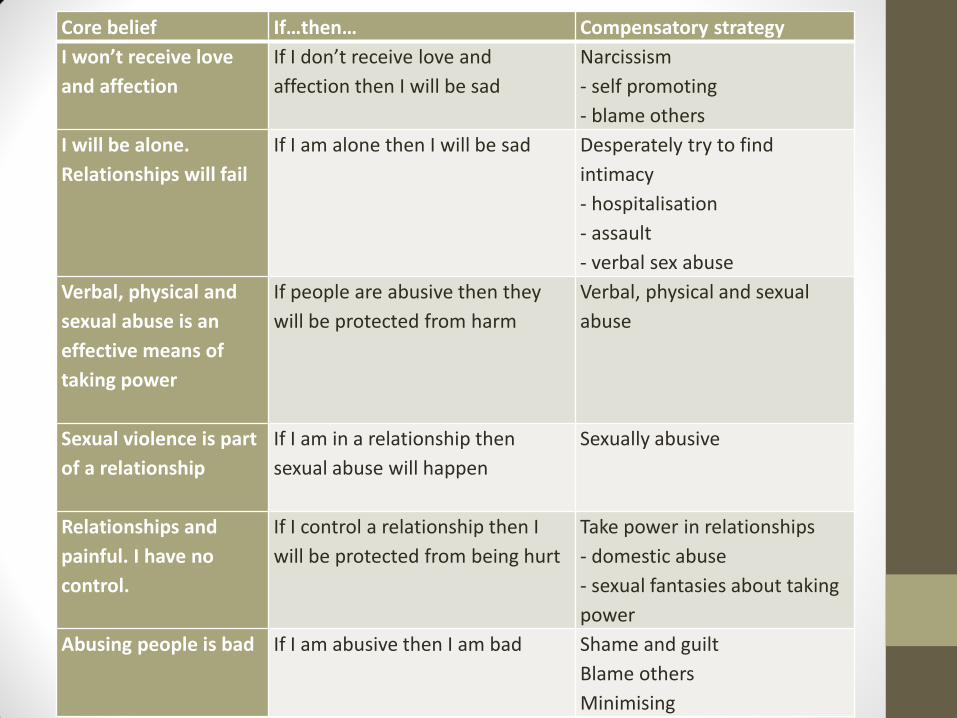
Core belief If…then… Compensatory strategy
I won’t receive love
and affection
If I don’t receive love and
affection then I will be sad
Narcissism
- self promoting
- blame others
I will be alone.
Relationships will fail
If I am alone then I will be sad Desperately try to find
intimacy
- hospitalisation
- assault
- verbal sex abuse
Verbal, physical and
sexual abuse is an
effective means of
taking power
If people are abusive then they
will be protected from harm
Verbal, physical and sexual
abuse
Sexual violence is part
of a relationship
If I am in a relationship then
sexual abuse will happen
Sexually abusive
Relationships and
painful. I have no
control.
If I control a relationship then I
will be protected from being hurt
Take power in relationships
- domestic abuse
- sexual fantasies about taking
power
Abusing people is bad
If I am abusive then I am bad Shame and guilt
Blame others
Minimising
BREAK
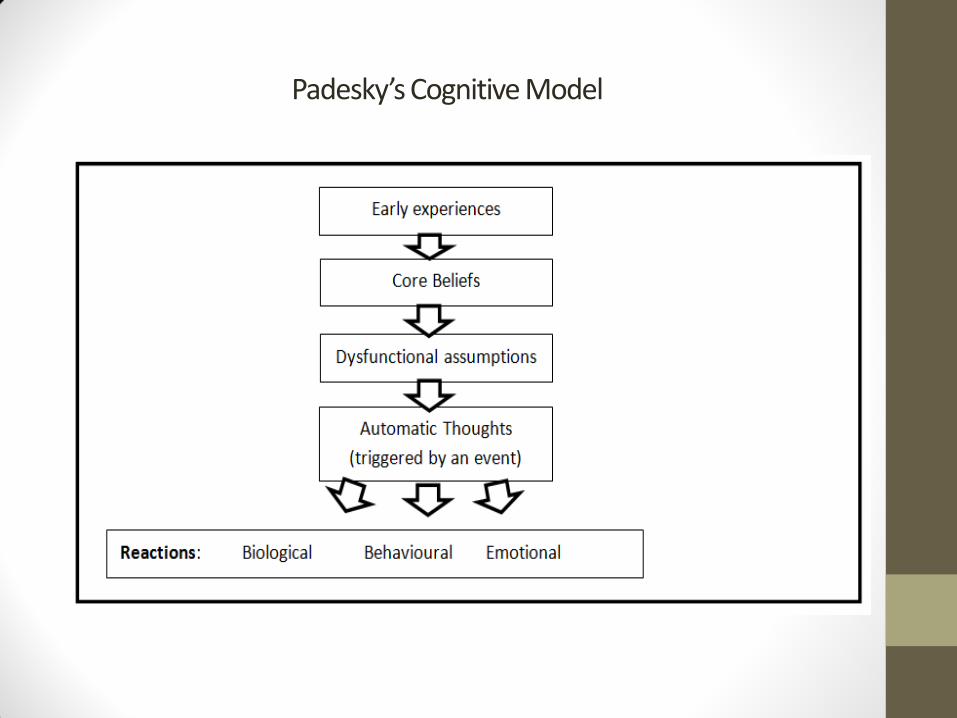
Padesky’s Cognitive Model
Delivering Therapy
• Principles of CBT:
1. Ever-evolving formulation and cognitive conceptualisation
2. Sound therapeutic alliance
3. Collaboration and active participation
4. Goal-orientated and problem-focused
5. Initially emphasises the present
6. Teaches client to be their own therapist; emphasises relapse prevention
7. Time-limited
8. Structured
9. Identify, evaluate and respond to dysfunctional thoughts and beliefs
10. Variety of changing thinking, mood and behaviour
Delivering Therapy
• 5-20 weekly sessions
• 30-60 minutes
• 1:1, group, self-help programmes and computerised programmes
• Forms basis of many condition-specific programmes
How therapy works
• Form an alliance based on shared goals
• Explore the client’s experience in Socratic terms
• Generate hypotheses about stuck states
• Functional Analysis – what purpose does a behaviour serve (A-B-C; Behavioural Theory)
• Promote learning which breaks stuck cycles and opens new learning

Assessment
• Begin with assessment which leads to individualised case formulation. Use to plan treatment
• Set of hypotheses about development and maintenance of problem list. There may be one for each disorder
• Good practice to form contract for assessment of number of sessions, venue, timing, importance of homework

Assessment continued: Presenting problem list
• Orientate to referral and time-frame available
• Invite client to explain difficulties with limited interruption
• Helpful prompts:
“What led you to come here today?”
“How long have you been feeling like this?”
“Can you tell me more about that?”
“Can you give an example?”
• Validate as you go to build alliance! Show understanding of their difficulty. Repeat, paraphrase
• Group and prioritise problems in a clinically meaningful way: (i) life-threatening behaviour, (ii) therapy-interfering behaviour, (iii) quality-of-life interfering behaviour
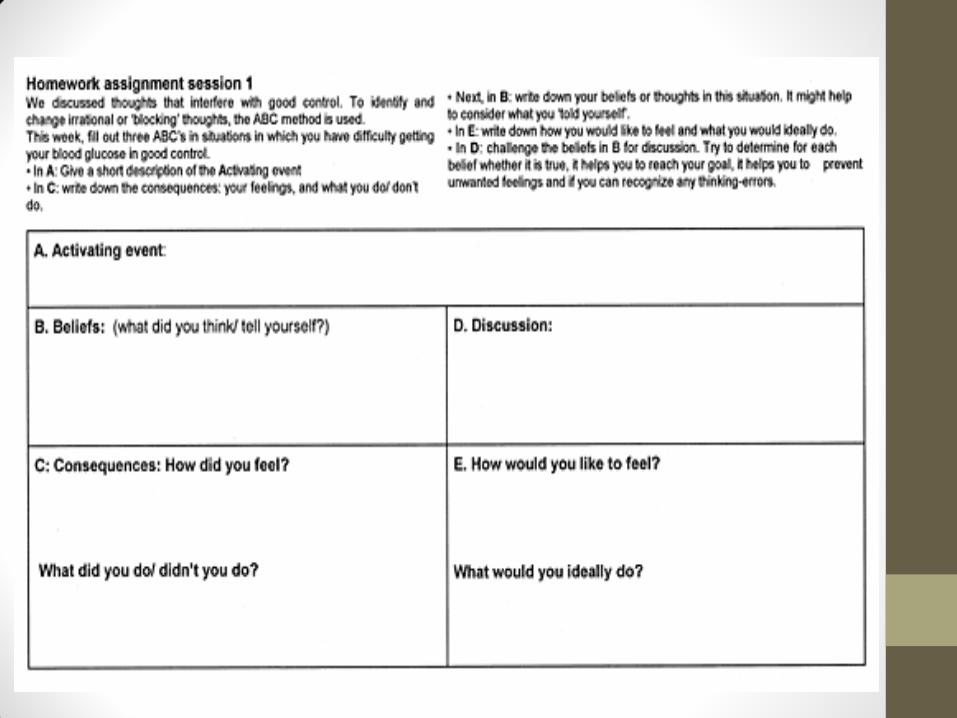
Assessment continued: ABC problem analysis
• Most psychological problems are amenable to ABC analysis
• The way antecedent factors (A), intervening beliefs (B), and emotional, cognitive, physiological and behavioural consequences (C) maintain problems
• Conduct by observing the client go through a micro-episode of the problem in the therapy room, request they complete self-monitoring homework task or ask about it:
“Can you describe the last time the problem happened?”
“What happened next?” “What went through your mind?”
“What did you do/want to do?” “How did that make you feel?”
“What did your body do?” “How did other people react?”
• After you have completed an ABC analysis, summarise it, and check it with the client for accuracy
• Clients can find it hard to capture their automatic thoughts. The therapist must teach them to thought-catch
• Strategies:
- Direct questions
- Strong affect
- Imagery
- Role plays
Assessment continued: ABC problem analysis
• Events which prompt episodes of the problem can be identified by a lifeline exercise.
• They can be classified as:
- Exits
- Entrances
- Illnesses/injuries
- Other transitions
Assessment continued: precipitating factors
Assessment continued: Predisposing factors
• Core beliefs triggered by precipitating event
• Distal external/internal factors vulnerability factors
• Focus for more in-depth treatment (Schema Therapy)
• Stress-Vulnerability Model
• Can be identified using Socratic questioning and the downward arrow technique
“If that were true, why would it be a problem?
What would it mean about you?”
Eg what would it mean if you were to fail an exam?
Assessment continued: Protective factors and Goal-setting
Protective factors
• Need to be considered because they have an impact on the efficacy of therapy
• Capacity to form therapeutic relationship is important
• Motivation to engage (do homework)
• Internal locus of control
Goal-setting
• Goals can be: short-term (this session), mid-term (this couple of sessions), long-term (for life)
• SMART
• Measure routinely, e.g. psychometric scores or increased/decreased behaviours
Assessment: Contracting
• Agree contract once intake assessment is complete and working formulation model has been constructed
• Client must understand and (collaboratively) agree with formulation and treatment goals. Establish:
1. Problems
2. ABC analysis
3. Predisposing factors – core beliefs
4. Precipitating factors
5. Protective factors
6. Therapy Goals
Session structure
- Orientation to session structure
- Check-in
- Set agenda
- Work through agenda, including review of homework
- Agree homework
- Summarise and request feedback
Treatment strategies
• Cognitive strategies aim to modify NATs and cognitive distortions to alter problem mood states
• They aim to reduce vulnerability to relapse by modifying core beliefs
• Modify assumptions rather than replace them with opposites
• Behavioural strategies aim to help clients alter activating events or engage them in activities which have a direct and positive impact on emotion states which are intrinsically reinforcing (Carr & McNulty)
• Clinicians draw from an menu of strategies when tailoring individualised programmes for particular clients. This depends on formulation, although specific protocols exist for particular disorders
Cognitive treatment: Socratic questioning
• “cornerstone of cognitive therapy”
• Use questions to elicit adaptive responses from clients. Planned questions to identify how problems are maintained and how they might be altered
• “guided discovery” Asking, rather than telling the problem, aids self-discovery and greater commitment to altering underlying problem belief
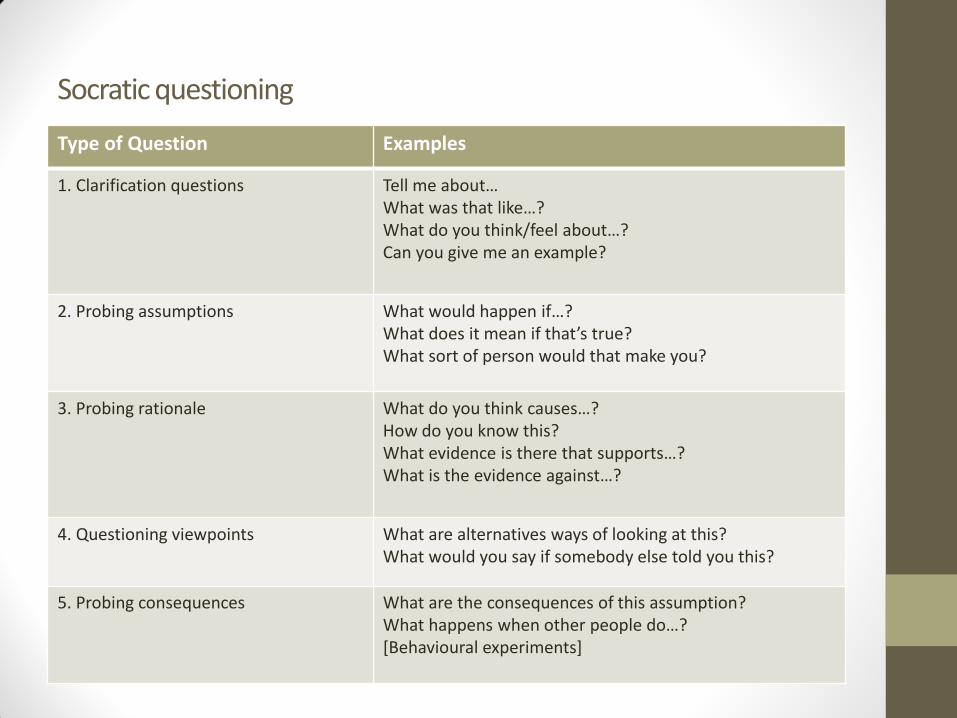
Socratic questioning
Type of Question Examples
1. Clarification questions Tell me about… What was that like…? What do you think/feel about…? Can you give me an example?
2. Probing assumptions What would happen if…? What does it mean if that’s true? What sort of person would that make you?
3. Probing rationale What do you think causes…? How do you know this? What evidence is there that supports…? What is the evidence against…?
4. Questioning viewpoints What are alternatives ways of looking at this? What would you say if somebody else told you this?
5. Probing consequences What are the consequences of this assumption? What happens when other people do…? [Behavioural experiments]
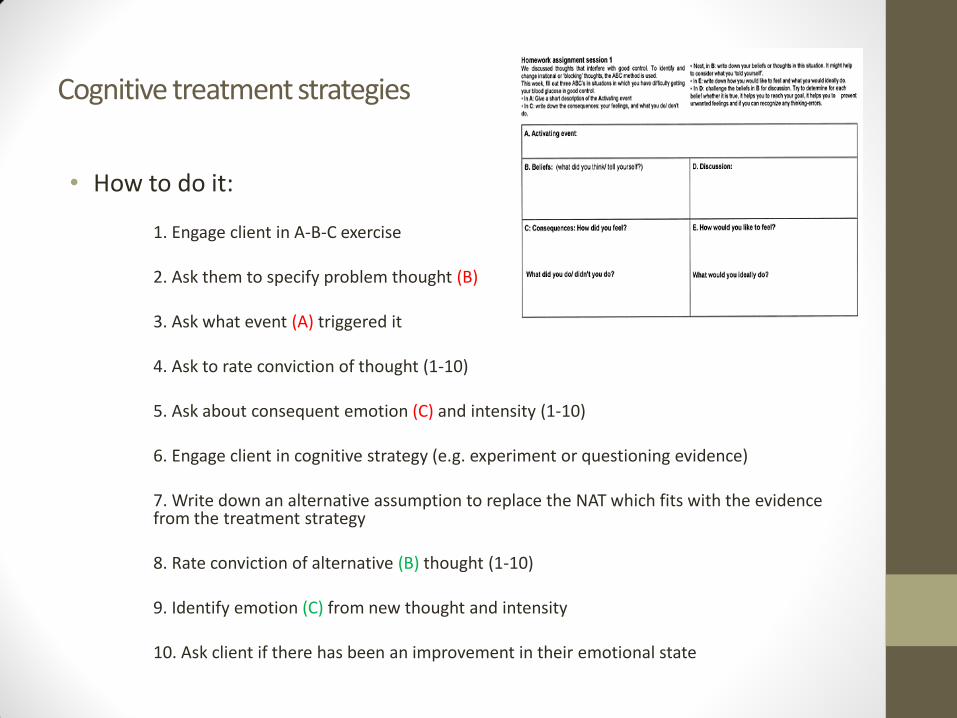
Cognitive treatment strategies
• How to do it: 1. Engage client in A-B-C exercise 2. Ask them to specify problem thought (B) 3. Ask what event (A) triggered it 4. Ask to rate conviction of thought (1-10) 5. Ask about consequent emotion (C) and intensity (1-10) 6. Engage client in cognitive strategy (e.g. experiment or questioning evidence) 7. Write down an alternative assumption to replace the NAT which fits with the evidence from the treatment strategy 8. Rate conviction of alternative (B) thought (1-10) 9. Identify emotion (C) from new thought and intensity 10. Ask client if there has been an improvement in their emotional state
Cognitive treatment strategies
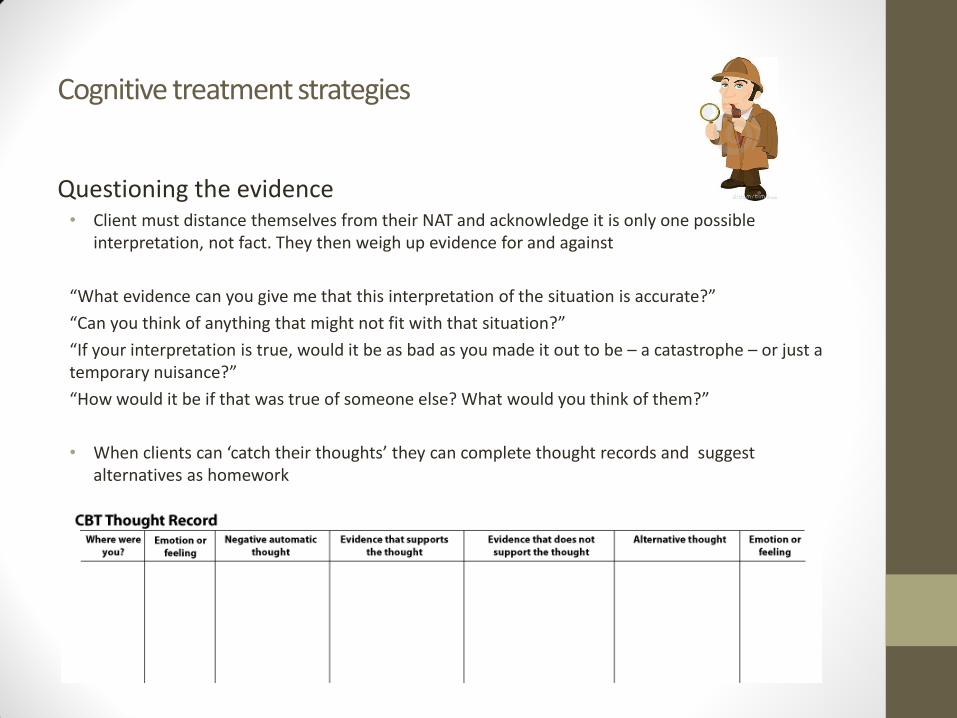
Questioning the evidence • Client must distance themselves from their NAT and acknowledge it is only one possible
interpretation, not fact. They then weigh up evidence for and against
“What evidence can you give me that this interpretation of the situation is accurate?”
“Can you think of anything that might not fit with that situation?”
“If your interpretation is true, would it be as bad as you made it out to be – a catastrophe – or just a temporary nuisance?”
“How would it be if that was true of someone else? What would you think of them?”
• When clients can ‘catch their thoughts’ they can complete thought records and suggest alternatives as homework
Cognitive treatment strategies
Behavioural experiments • These can take the form of: observational (monitoring activities), graded task/graded
exposure, direct test of core beliefs, interview others, perspective-taking (what would someone else do?), video-recording
- Identify underlying assumptions
- Make very specific predictions
- Plan the experiment
- Anticipate problems
- Do the experiment (multiple times if necessary)
- Record outcomes
- Analyse outcome patterns
- Be alert for disqualifiers (eg it only turned out like that because…)
Cognitive treatment strategies
Safety Behaviour Experiments • Establish what the client does to avoid an aversive outcome. Invite them to give up the
safety behaviour and test whether feared consequence occurs. If so, why. If not, observe reduced anxiety
Belief surveys • Ask friends to what extent they believe in the client’s NAT. Discuss verbatim responses
in next session
Think in shades of grey • Rephrase one NAT or assumption in less concrete language (mindfulness helps address
assumptions
Re-attribution • Rephrase problem assumption to practise shifting blame between internal and
external factors
Cognitive treatment strategies
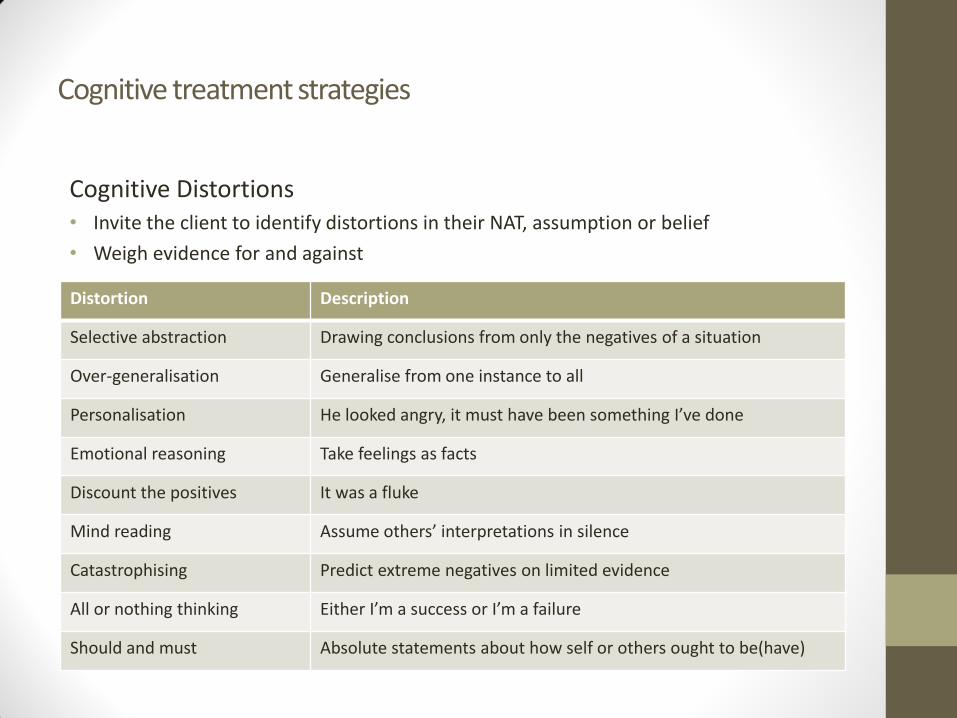
Cognitive Distortions • Invite the client to identify distortions in their NAT, assumption or belief
• Weigh evidence for and against
Distortion Description
Selective abstraction Drawing conclusions from only the negatives of a situation
Over-generalisation Generalise from one instance to all
Personalisation He looked angry, it must have been something I’ve done
Emotional reasoning Take feelings as facts
Discount the positives It was a fluke
Mind reading Assume others’ interpretations in silence
Catastrophising Predict extreme negatives on limited evidence
All or nothing thinking Either I’m a success or I’m a failure
Should and must Absolute statements about how self or others ought to be(have)
Cognitive treatment strategies
Cost-benefit analysis • What are the costs and benefits of holding problematic thoughts and giving them up
Pie chart analysis • Apportion responsibility amongst all parties involved for a perceived negative event to
break perception of being solely responsible
Core belief test • Downward-arrow to core beliefs then list evidence which shows core belief is not
universally true
Show self-compassion
Focus on the positives
Positive daily log
Take control of mood:
• set up situations which are less distressing
• learn to tolerate being in difficult situations with certain coping strategies
How: complete ABC and rate intensity. Invite coping skill then measure intensity of consequent emotion
Behavioural treatment strategies
Distraction/thought-stopping/grounding
• Identify activating event then temporarily focus on another aspect of the situation, distracting technique. Actively postpone rumination, flashcard, wristband, bang on table, say STOP (Distress Tolerance)
Relaxation
• Progressive muscle relaxation, paced breathing (5 in, 5 out)
Imagery
• Relaxation and distraction used in systematic desensitisation. Relax in advance then bring distressing image to mind. Imagine positive not negative outcome
Behavioural treatment strategies
Physical Activity • Part of PLEASE skills to reduce vulnerability to problematic emotions
Pleasant event • Fill diary with all obligations, pleasant events can be filled into the vacant slots
Graded challenges • Construct hierarchies of graded challenges, including increasingly fear-inducing or
anger-provoking situations
Self-reward • Use self-praise and tangible award
Behavioural treatment strategies
Relapse Prevention
• Identify triggers
- risky thoughts, emotions and situations
• Look for early warning signs
• Recognise distortions
• Plan how to cope (effective strategies) when you recognise these signs
- If this happens…, then I will do this…
Related Documents











