Approved BFP Initial Test By Certificate Gauge Num Company Phone Final Test By Repair By Service Address Contact Name Install Date Mfr SN Size Type Model Test Report Due: Schedule Code Location ID Map Page Permit Num Hazard Type Haz. Level Assembly ID Meter # Facility Name Acct Number Equip Location Protection Type #2 Ph (Replacement/Correction) Assembly Info R E P A I R Final Test Initial Test Shut Off Valves PVB/SVB Check Valve #1 Check Valve #2 Relief Valve #2 #1 Leaked Leaked PSID Leaked Leaked Did Not Open CLEANED REPLACED CLEANED REPLACED CLEANED REPLACED CLEANED REPLACED CLEANED REPLACED 1A Air Inlet Opened at Air Inlet Disc Airl Inlet Spring Check Disc Check Spring PSID REPORT OF TEST RESULTS Held at PSID Disc Spring Guide Seat Closed Tight PSID Disc Spring Guide Seat Closed Tight Disc Spring Diaphragm Seat Opened at PSID Closed Tight PSID Line pressure at time of test: THE ABOVE REPORT IS CERTIFIED TO BE TRUE: Date: Other/Notes: Held at PSID Opened at PSID PSID PSID Air Inlet CK Valve Closed Tight Did not Open Check Held at Closed Tight Closed Tight Other REPAIR Float Hinge Pin Hinge Pin O-Ring(s) Diaphragm Diaphragm Module Module Module City of Snoqualamish, WA BACKFLOW ASSEMBLY TEST FORM. RETURN ORIGINAL FORM ONLY . Time In Time Out Fail Pass Pass

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Approved BFP
Initial Test By Certificate Gauge Num Company Phone
Final Test By
Repair By
Service Address
Contact Name
Install Date
Mfr
SN
Size
Type
Model
Test Report Due:
Schedule Code
Location ID
Map Page
Permit Num
Hazard Type Haz. Level
Assembly ID
Meter #
Facility Name
Acct Number
Equip Location
Protection Type
#2
Ph
(Replacement/Correction)Assembly Info
R
E
P
A
I
R
Final
Test
Initial
Test
Shut Off ValvesPVB/SVBCheck Valve #1 Check Valve #2 Relief Valve
#2#1
Leaked
Leaked
PSIDLeaked Leaked Did Not Open
CLEANED
REPLACED
CLEANED
REPLACED
CLEANED
REPLACED
CLEANED
REPLACED
CLEANED
REPLACED
1A
Air Inlet Opened at
Air Inlet Disc
Airl Inlet Spring
Check Disc
Check Spring
PSID
REPORT OF TEST RESULTS
Held at
PSID
Disc
Spring
Guide
Seat
Closed Tight
PSID
Disc
Spring
Guide
Seat
Closed Tight
Disc
Spring
Diaphragm
Seat
Opened at
PSID
Closed Tight
PSID
Line pressure at time of test:
THE ABOVE REPORT IS CERTIFIED TO BE TRUE:
Date:
Other/Notes:
Held at
PSID
Opened at
PSID PSID
PSID
Air Inlet
CK Valve
Closed TightDid not Open
Check Held atClosed Tight Closed Tight
Other
REPAIR
FloatHinge Pin Hinge Pin O-Ring(s)
DiaphragmDiaphragm Module Module
Module
City of Snoqualamish, WA
BACKFLOW ASSEMBLY TEST FORM.
RETURN ORIGINAL FORM ONLY .
Time In Time Out
Fail
Pass
Pass

Shut Off ValvesCheck Valve #1 Check Valve #2 Relief Valve
#2#1
Leaked
Leaked
PSIDLeaked Leaked Did Not Open
Air Inlet Opened at
PSID
Held at
PSID PSID
Held at
PSID
Opened at
Initial
Test Closed TightDid not Open
Check Held atClosed Tight Closed Tight
Initial Test By Certificate Gauge Num Company Phone
Final Test By
Repair By
CLEANEDCLEANED CLEANED CLEANED CLEANED
Final
Test
REPORT OF TEST RESULTS
Closed Tight
PSID
Closed Tight
Opened at
PSID Closed Tight
Line pressure at time of test:
THE ABOVE REPORT IS CERTIFIED TO BE TRUE:
Date:
Comments
PSID PSID
PSID
Air Inlet
CK Valve
City of Snoqualamish, WA
BACKFLOW ASSEMBLY TEST FORM.
RETURN ORIGINAL FORM ONLY .
Time In Time Out
0
Service Address
Contact Name
Location
Install Date
Assembly Info
Mfg
SN
Size
Type
Emergency Ph:
Model
Return Form By:
Schedule Code
Location ID
Map Page
Permit Num
Hazard Type Haz. Level
Assembly ID
Meter #
Facility Name
Acct Number
1B
PVB/SVB
FailedPassed
Passed Final Test
Initial Test
TEST
FINAL
TEST
INI-
TIAL
YR
YR
YR
IF DEVICE REPLACED, WHY?
MAP:
GRID
COMMENTS:
PAGE
SITE CONTACT
WORK PERFORMED
TESTING COMPANY PHONE NUMBER
TESTER #
SITE CONTACT PHONE NUMBER
DAY
TESTING COMPANY
MO
WORK PERFORMED
DAYMO
WORK PERFORMED
DAYMOTESTER #
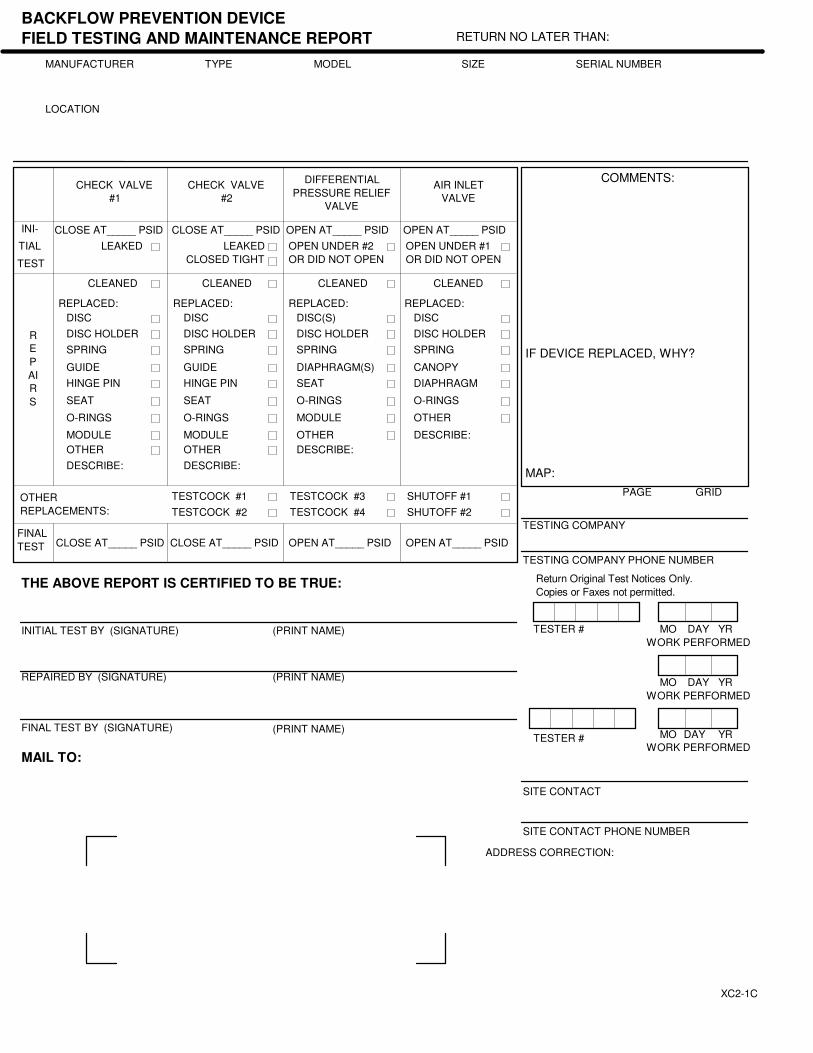
CHECK VALVE
#2
DIFFERENTIAL
PRESSURE RELIEF
VALVE
AIR INLET
VALVE
CHECK VALVE
#1
CLOSE AT_____ PSID
LEAKED
CLOSE AT_____ PSID OPEN AT_____ PSID OPEN AT_____ PSID
LEAKED
CLOSED TIGHT
OPEN UNDER #2
OR DID NOT OPEN
OPEN UNDER #1
OR DID NOT OPEN
CLEANED CLEANED CLEANEDCLEANED
REPLACED: REPLACED: REPLACED: REPLACED:
BACKFLOW PREVENTION DEVICE
FIELD TESTING AND MAINTENANCE REPORT RETURN NO LATER THAN:
MANUFACTURER
LOCATION
MODEL SIZE SERIAL NUMBER
R
E
P
AI
R
S
SPRING
O-RINGS
MODULE
OTHER
DESCRIBE:
DISC
DISC HOLDER
GUIDE
HINGE PIN
SEAT
SPRING
O-RINGS
OTHER
DESCRIBE:
DISC
DISC HOLDER
CANOPY
DIAPHRAGM
(PRINT NAME)
MAIL TO:
ADDRESS CORRECTION:
THE ABOVE REPORT IS CERTIFIED TO BE TRUE:
INITIAL TEST BY (SIGNATURE)
SPRING
O-RINGS
MODULE
OTHER
DESCRIBE:
DISC
GUIDE
SEAT
SPRING
O-RINGS
MODULE
OTHER
DESCRIBE:
DISC(S)
DIAPHRAGM(S)
SEATHINGE PIN
DISC HOLDER DISC HOLDER
OTHER
REPLACEMENTS:
TESTCOCK #1
TESTCOCK #2
TESTCOCK #3
TESTCOCK #4
SHUTOFF #1
SHUTOFF #2
CLOSE AT_____ PSID CLOSE AT_____ PSID OPEN AT_____ PSID OPEN AT_____ PSID
REPAIRED BY (SIGNATURE)
FINAL TEST BY (SIGNATURE)
(PRINT NAME)
(PRINT NAME)
TYPE
XC2-1C
Return Original Test Notices Only.
Copies or Faxes not permitted.
O-RING(S)OTHEROTHER
Initial Test by (Signature) Tester Number MO DAY YR
DISC(S) DISCDISC DISC(S)
FLOATSEATSEAT DIAPHRAGM(S)
MODULE OTHERMODULE SEAT(S)
SPRING SPRINGSPRING SPRING
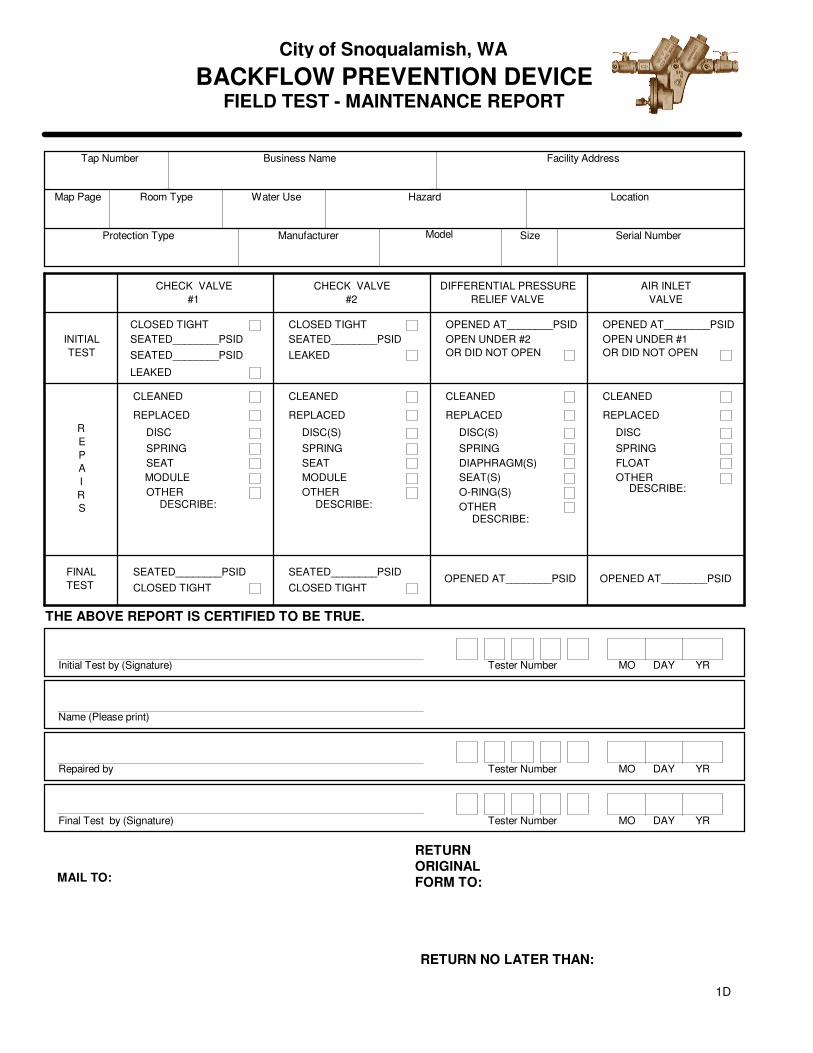
CLOSED TIGHT CLOSED TIGHT
SEATED________PSIDSEATED________PSID
CLEANED
CHECK VALVE
#2
DIFFERENTIAL PRESSURE
RELIEF VALVE
AIR INLET
VALVE
CHECK VALVE
#1
LEAKED
OPEN UNDER #2
OR DID NOT OPEN
OPEN UNDER #1
OR DID NOT OPEN
INITIAL
TEST
CLEANED CLEANEDCLEANED
REPLACED REPLACED REPLACED REPLACED
R
E
P
A
I
R
S DESCRIBE:DESCRIBE:
DESCRIBE:
FINAL
TEST
DESCRIBE:
SEATED________PSID
OPENED AT________PSID OPENED AT________PSID
LEAKED
SEATED________PSID
CLOSED TIGHT
SEATED________PSID
CLOSED TIGHT OPENED AT________PSID OPENED AT________PSID
THE ABOVE REPORT IS CERTIFIED TO BE TRUE.
RETURNORIGINALFORM TO:
RETURN NO LATER THAN:
MAIL TO:
Name (Please print)
Repaired by Tester Number MO DAY YR
Final Test by (Signature) Tester Number MO DAY YR
BACKFLOW PREVENTION DEVICEFIELD TEST - MAINTENANCE REPORT
City of Snoqualamish, WA
Tap Number Business Name Facility Address
Map Page Room Type Water Use Hazard Location
Protection Type Manufacturer Model Size Serial Number
OTHER
1D

CHECK VALVE #1
CHICAGO WATER DEPARTMENT
BACKFLOW PREVENTER TEST REPORT
PLUMBING INSPECTION DEPARTMENT FAXPHONE
PERMIT # ORIGINAL TEST
DISTRICTAM. PM. DATE RETESTTIME PASS FAIL
CALIBRATION DATETEST KIT
ADDRESS OWNER
CONTACT PHONE FAX
DEVICE = SUPPLY PRESSUREDCDADCRP PVB PSIG
CONTRACTOR PHONE
MFR SIZE MODEL# SERIAL#
ON LINE TO
LEAKED
DID NOT OPEN
OPENED @
OPENED @
COMMENTS
COMPLETETYPE TYPE
PSID / RP ZONE
PSID
RELIEF VALVE
TEST COCKS
MISSING #RWRW
DAMAGEDCLOSED TIGHTCLOSED TIGHT
COMMENTSLEAKEDLEAKED
PSIDPSID
INITIAL TEST CLOSED TIGHT CLOSED TIGHT
LEAKED
COMMENTSCOMMENTS
CLOSED TIGHT
CHECK VALVE #2
CONTROL VALVE #2
COMMENTSCOMMENTS
FINAL TEST
COMMENTS
CCCDI# XC PLUMBING LICENSE#
CCCDI NAME (PRINT) SIGNATURE
CLOSED TIGHT
CONTROL VALVE #1
EXACT LOCATION
1E
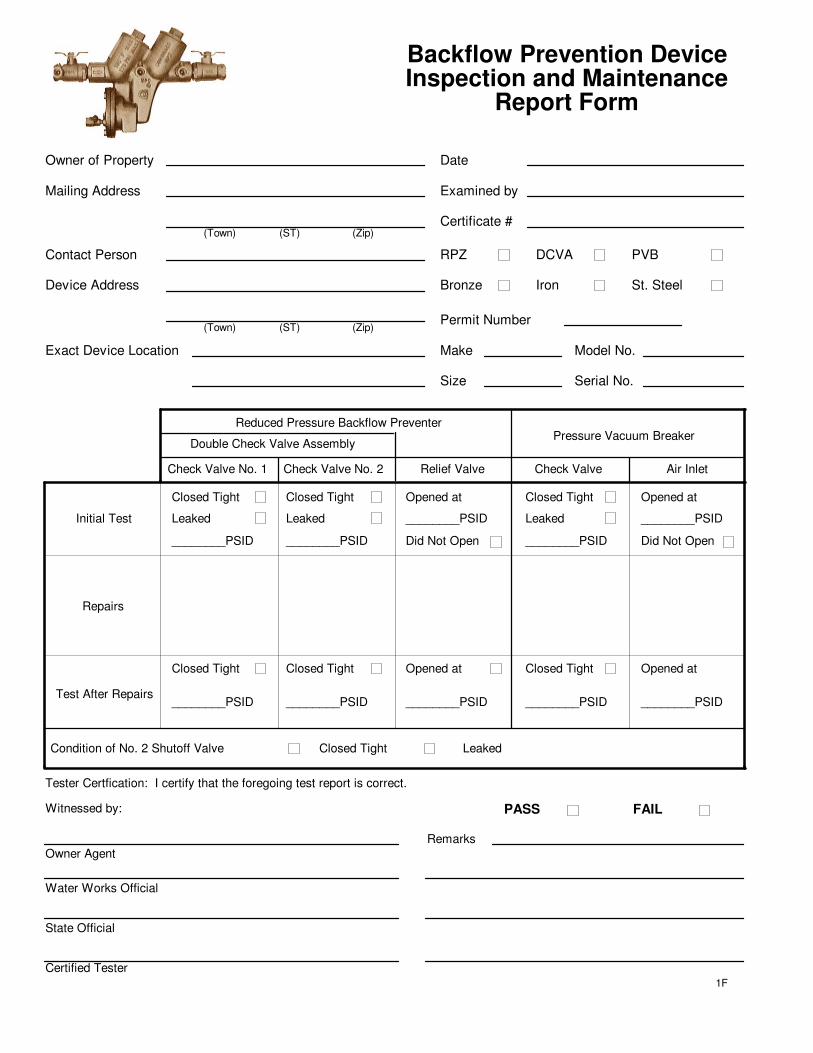
Owner of Property
Mailing Address
Device Address
Contact Person
Exact Device Location
Date
Examined by
Certificate #
RPZ DCVA PVB
(Town) (Zip)(ST)
Bronze Iron St. Steel
(Town) (ST) (Zip)
Size
Model No.Make
Serial No.
Reduced Pressure Backflow Preventer
Double Check Valve Assembly
Check Valve No. 1 Check Valve No. 2 Relief Valve
Pressure Vacuum Breaker
Check Valve Air Inlet
Initial Test
Closed Tight
Leaked
________PSID
Opened at
Did Not Open
Repairs
Test After Repairs
Condition of No. 2 Shutoff Valve
________PSID
Opened atClosed Tight
Leaked
________PSID Did Not Open
________PSID
Closed Tight Closed Tight Closed TightOpened at Opened at
________PSID________PSID ________PSID ________PSID________PSID
Closed Tight
Closed Tight Leaked
Leaked ________PSID
Inspection and Maintenance Backflow Prevention Device
Report Form
1F
Owner Agent
Witnessed by: PASS FAIL
Water Works Official
State Official
Certified Tester
Remarks
Tester Certfication: I certify that the foregoing test report is correct.
Permit Number

Repairs
Exact Device Location
Reduced Pressure Backflow Preventer
Double Check Valve Assembly
Check Valve No. 1 Check Valve No. 2 Relief Valve
Pressure Vacuum Breaker
Check Valve Air Inlet
Initial Test/Routine Test
Closed Tight
Leaked
________PSID
Opened at
Did Not Open
Test AfterRepairs
Condition of No. 2 Shutoff Valve
________PSID
Opened atClosed Tight
Leaked
________PSID Did Not Open
________PSID
Closed Tight Closed Tight Closed TightOpened at Opened at
________PSID________PSID ________PSID ________PSID________PSID
Closed Tight
Closed Tight Leaked
Leaked ________PSID
Backflow Prevention Device
Inspection and Maintenance
Report Form
1FB
MA License Plumbers/FSF Name (Print)
Repair Person: These devices must be repaired by a Massachusetts Licensed Plumber or a Fire Sprinkler Fitter.
PASS FAIL
The Above Test/Inspection is Certified to be True
TEST RESULT
Plumber/FSF Lic # Cert. Exp Date Signature
Initial
Re-Test
Annual
Semi-Annual
Test Status
Public Water System Name PWS City/Town PWS ID Number
City of Snoqualamish, WA Snoqualamish
Date
MA-DEP Certified Tester Name (Print) MA-DEP Cert Tester ID Cert. Exp Date Signature Date
Backflow Device Test Conducted by: (MA - DEP Backflow Prevention Device Tester)
Backflow Device Test Witnessed By: (Facility Owner/Representative)
Facility Owner/Representative (Print) Signature Date
Date
Date
Date
Owner of Property
Mailing Address
Device Address
Contact Person
RPZ DCVA PVB
(Town) (Zip)(ST)
Bronze Iron St. Steel
(Town) (ST) (Zip)
Size
Model No.Make
Serial No.
Permit Number
Valve Type: OS&Y Butterfly Other
Domestic Line Fire Sprinkler Line
Ball
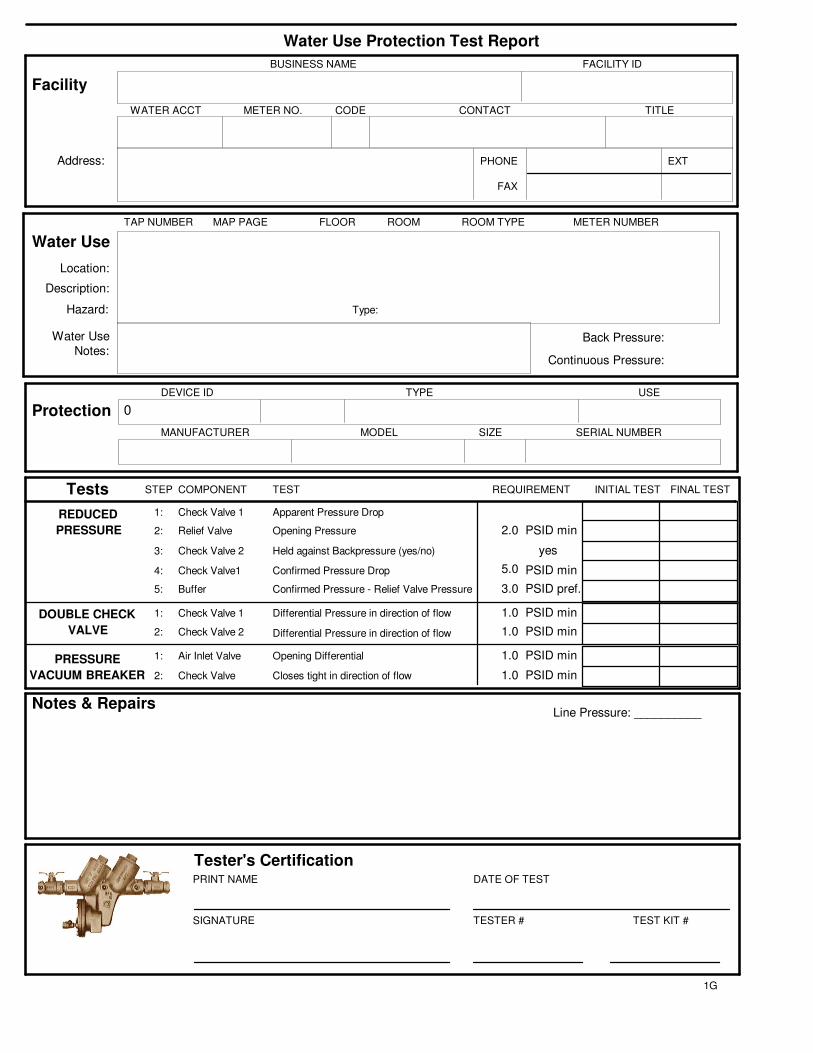
Line Pressure: __________
Tester's Certification
Water Use Protection Test Report
Notes & Repairs
PRINT NAME
SIGNATURE
DATE OF TEST
TESTER # TEST KIT #
1G
Tests COMPONENTSTEP TEST REQUIREMENT INITIAL TEST FINAL TEST
REDUCED
PRESSURE
DOUBLE CHECK
VALVE
PRESSURE
VACUUM BREAKER
Relief Valve Opening Pressure2: PSID min
Check Valve 2 Held against Backpressure (yes/no)3: yes
Buffer5: Confirmed Pressure - Relief Valve Pressure PSID pref.
Air Inlet Valve1: Opening Differential PSID min
Check Valve2: Closes tight in direction of flow PSID min
Apparent Pressure DropCheck Valve 11:
4: Check Valve1 Confirmed Pressure Drop PSID min
1: Check Valve 1 Differential Pressure in direction of flow PSID min
2: Check Valve 2 Differential Pressure in direction of flow PSID min
5.0
2.0
1.0
1.0
1.0
1.0
3.0
Protection
USETYPE
SIZEMODELMANUFACTURER SERIAL NUMBER
DEVICE ID
Facility
Water Use
BUSINESS NAME FACILITY ID
WATER ACCT CONTACT TITLE
PHONE
FAX
EXT
CODEMETER NO.
TAP NUMBER MAP PAGE FLOOR ROOM ROOM TYPE METER NUMBER
Water Use
Notes:Back Pressure:
Continuous Pressure:
Address:
Hazard:
Location:
Description:
Type:
0
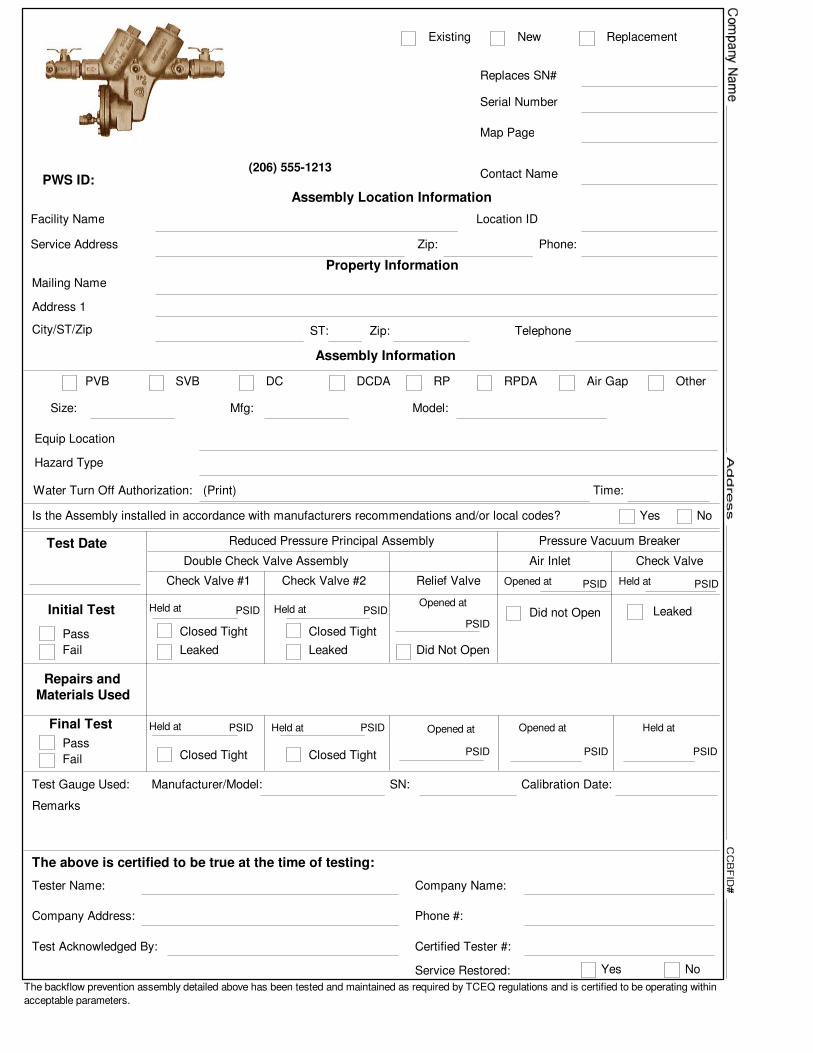
Test Gauge Used: Manufacturer/Model: SN: Calibration Date:
Tester Name:
Company Address:
Test Acknowledged By:
Company Name:
Phone #:
Certified Tester #:
The above is certified to be true at the time of testing:
Service Restored:
Remarks
The backflow prevention assembly detailed above has been tested and maintained as required by TCEQ regulations and is certified to be operating within
acceptable parameters.
Pressure Vacuum Breaker
Final Test
Initial Test
Repairs andMaterials Used
Test Date Reduced Pressure Principal Assembly
Double Check Valve Assembly Check Valve
Check Valve #1 Check Valve #2
Air Inlet
Relief Valve
Leaked
PSID
PSID
Leaked Leaked Did Not Open
Contact Name
Mfg:
Serial Number
Size: Model:
Map Page
PSID
Held at PSID
PSID
Held at PSIDOpened at
Did not Open
Closed Tight Closed Tight
PVB SVB DC DCDA RP RPDA Air Gap Other
Held at PSID
PSID
Held at PSID Opened at
Closed Tight Closed Tight
Existing New Replacement
Replaces SN#
PSID
Opened at Held at
Opened at Held at
Is the Assembly installed in accordance with manufacturers recommendations and/or local codes? Yes No
Water Turn Off Authorization: (Print) Time:
Yes No
Service Address
Location IDFacility Name
Phone:
Mailing Name
City/ST/Zip Telephone
Address 1
ST: Zip:
Assembly Information
Assembly Location Information
Zip:
Hazard Type
Equip Location
Property Information
Fail
Pass
Fail
Pass
PWS ID:(206) 555-1213
PSID PSIDPSID
. . .
Check Valve #1 Check Valve #2 Relief Valve
RPP
DCV
Opened atClosed Tight Closed Tight
Leaked Leaked Did Not Open
Opened Under 2.0 PSID
(Replacement/Correction)
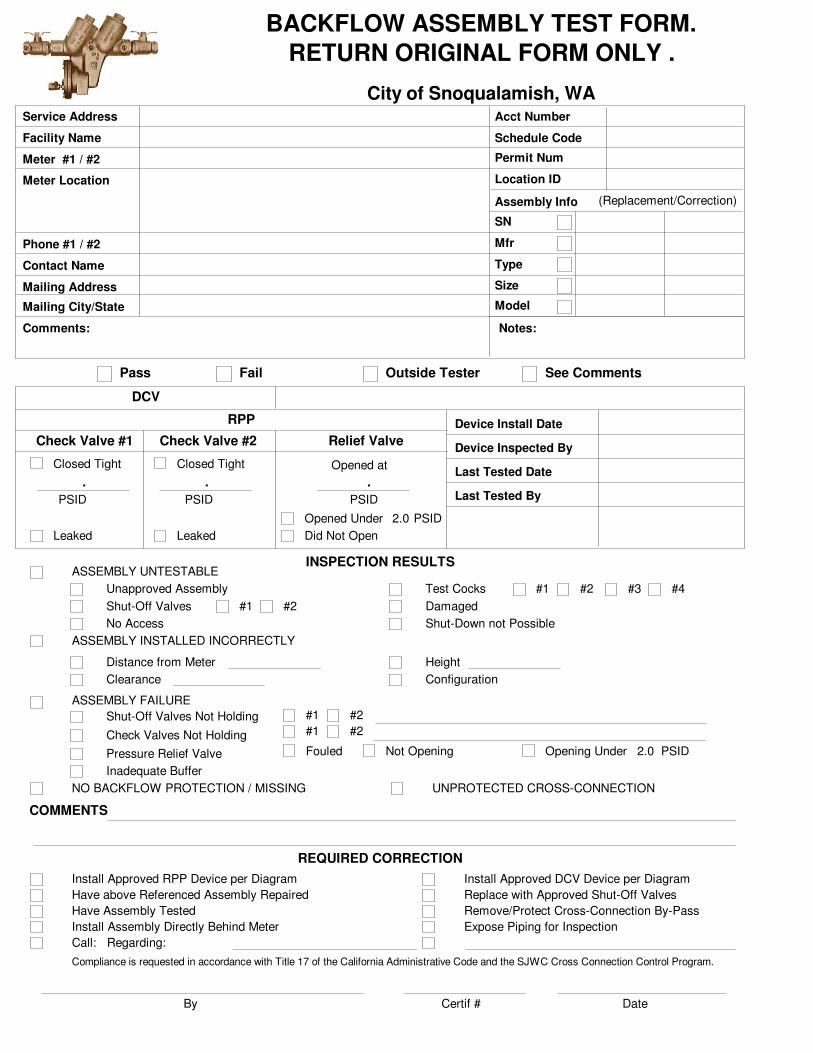
City of Snoqualamish, WA
Fail
Service Address
Device Install Date
Mfr
SN
Size
Type
Model
Schedule Code
Location ID
Permit Num
Acct Number
Assembly Info
BACKFLOW ASSEMBLY TEST FORM.
RETURN ORIGINAL FORM ONLY .
Pass Outside Tester See Comments
INSPECTION RESULTSASSEMBLY UNTESTABLE
Unapproved Assembly
Shut-Off Valves
No Access
#1 #2
Test Cocks
Damaged
Shut-Down not Possible
#1 #2 #3 #4
ASSEMBLY INSTALLED INCORRECTLY
Distance from Meter
Clearance
Height
Configuration
ASSEMBLY FAILURE
Shut-Off Valves Not Holding
Check Valves Not Holding
Pressure Relief Valve
#1 #2
#1 #2
Inadequate Buffer
Fouled Not Opening Opening Under
NO BACKFLOW PROTECTION / MISSING UNPROTECTED CROSS-CONNECTION
COMMENTS
REQUIRED CORRECTION
Install Approved RPP Device per Diagram
Have above Referenced Assembly Repaired
Have Assembly Tested
Install Assembly Directly Behind Meter
Call: Regarding:
Install Approved DCV Device per Diagram
Replace with Approved Shut-Off Valves
Remove/Protect Cross-Connection By-Pass
Expose Piping for Inspection
2.0 PSID
By Certif # Date
Compliance is requested in accordance with Title 17 of the California Administrative Code and the SJWC Cross Connection Control Program.
Device Inspected By
Last Tested Date
Last Tested By
Facility Name
Meter #1 / #2
Meter Location
Phone #1 / #2
Contact Name
Mailing Address
Mailing City/State
Comments: Notes:

Final
TestApparent Air Inlet
CK Valve
PSID
PSID Closed TightClosed Tight
PSID Opened at
PSIDActual
Initial
Test
Leaked
Check Held at
PSID Leaked
Closed Tight
Leaked
Closed Tight
Leaked
Did Not OpenActual
Did not Open
PSIDPSIDPSIDApparent
PVB/SVB Shut Off ValvesRelief ValveCheck Valve #2Check Valve #1
Air Inlet Opened at #2#1 Held atHeld at PSID Opened at
R
E
P
A
I
R
CLEANED
REPLACED
Air Inlet Disc
Airl Inlet Spring
Check Disc
Check Spring
Float
Diaphragm
CLEANED
REPLACED
Other
REPAIR
CLEANED
REPLACED
Disc
Spring
Guide
Seat
Hinge Pin
Module
CLEANED
REPLACED
Disc
Spring
Guide
Seat
Other/Notes:
Hinge Pin
Diaphragm
Module
CLEANED
REPLACED
Disc
Spring
Diaphragm
Seat
O-Ring(s)
Module
THE ABOVE REPORT IS CERTIFIED TO BE TRUE:
Initial Test By
Final Test By
Repair By
Line pressure at time of test:
Protection Type
1. Is the device installed per:
2. Is there a strainer or Pressure Regulator
between Meter and Backflow Preventer?
REQUIREMENTS
CompanyTime Out PhoneGauge Num Time InDate:Certificate
Yes No
3. Is there PVC Pipe
between Meter and Backflow Preventer?
4. Is there a Tee
between Meter and Backflow Preventer?
Yes No
City of Snoqualamish, WA
0
Service Address
Contact Name
Install Date
Mfr
SN
Size
Type
Model
Return Form By:
Schedule Code
Location ID
Map Page
Permit Num
Hazard Type Haz. Level
Assembly ID
Meter #
Facility Name
Acct Number
Equip Location
#2
Ph
(Replacement/Correction)Assembly Info
1H
BACKFLOW ASSEMBLY TEST FORM.
RETURN ORIGINAL FORM ONLY .
Held at PSID
Check Valve #1 Check Valve #2Differential
Pressure Relief Valve
Air Inlet Opened at
PSID
R
E
P
A
I
R
S
Initial
TestPSID
REPLACED REPLACED REPLACED
PSID PSID
Opened at Check Held at
PSID
REPLACED
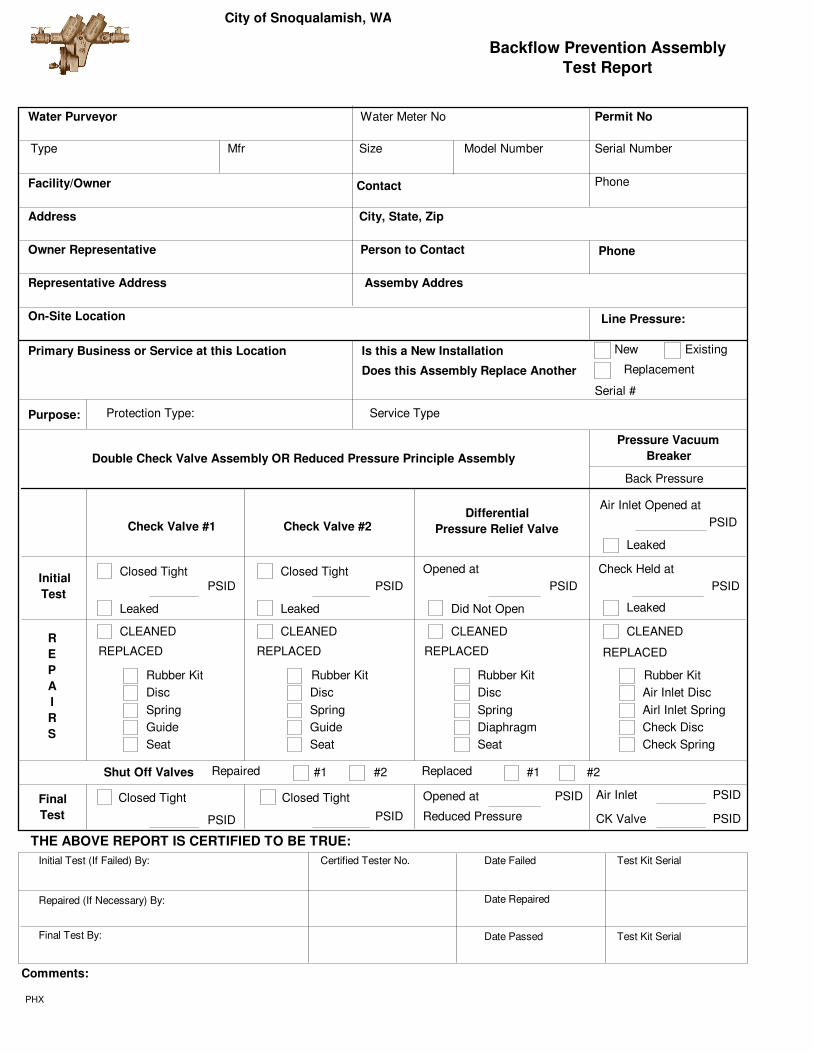
Double Check Valve Assembly OR Reduced Pressure Principle Assembly
Back Pressure
Pressure Vacuum
Breaker
Water Purveyor
Mfr Serial NumberSize Model Number
Phone
Assemby Addres
Permit No
Facility/Owner
Address
Owner Representative
Representative Address
On-Site Location
Water Meter No
City, State, Zip
ExistingNew
Serial #
Phone
Backflow Prevention Assembly
Test Report
Line Pressure:
Replacement
Protection Type: Service Type
Contact
Person to Contact
Primary Business or Service at this Location Is this a New Installation
Does this Assembly Replace Another
Purpose:
Final
Test
PHX
PSID
PSID
Air Inlet
CK Valve
Comments:
PSID
PSID
PSID
Opened at
Reduced Pressure
Repaired ReplacedShut Off Valves
Date FailedCertified Tester No.Initial Test (If Failed) By:
Repaired (If Necessary) By:
Final Test By:
Test Kit Serial
Date Repaired
Date Passed Test Kit Serial
THE ABOVE REPORT IS CERTIFIED TO BE TRUE:
Type
Leaked
Leaked Leaked Did Not Open
CLEANEDCLEANED CLEANED CLEANED
Air Inlet Disc
Airl Inlet Spring
Check Disc
Check Spring
Disc
Spring
Guide
Seat
Closed Tight
Disc
Spring
Guide
Seat
Closed Tight
Disc
Spring
Diaphragm
Seat
Closed Tight Closed Tight
Leaked
Rubber Kit Rubber Kit Rubber Kit Rubber Kit
#1 #2 #1 #2
City of Snoqualamish, WA

Owner of Property
Mailing Address
Device Address
Contact Person
Exact Location
Test Date
(Town) (Zip)(ST)
(Town) (ST) (Zip)
Size
Model No.Make
Serial No.
Reduced Pressure Backflow Preventer
Double Check Valve Assembly
Check Valve No. 1 Check Valve No. 2 Relief Valve
Pressure Vacuum Breaker
Check Valve Air Inlet
Initial Test Closed Tight
Leaked
________PSID
Opened at
Did Not Open
Repairs
Final Test
Condition of No. 2 Shutoff Valve
________PSID
Opened atClosed Tight
Leaked
________PSID Did Not Open
________PSID
Closed Tight Closed Tight Closed TightOpened at Opened at
________PSID________PSID ________PSID ________PSID________PSID
Closed Tight
Closed Tight Leaked
Leaked ________PSID
Inspection and Maintenance
Backflow Prevention Device
Report Form
1L
PASS
FAIL
Certification: On this date, the above device was tested per applicable codes and the required performance standards.
Permit Number
Test Type
Tester Name
Gauge No. Testing Firm
Tester Certification No.
Tester Signature:
Contact Signature:
Date:
Date:
Notes:
Line PSI
PVB
SVB
DCV
DDCV
RPBP
RPDA
PASS
Return Form By:
Test Report Due:

Test Gauge Used: Manufacturer/Model: SN:
Tester Name:
Company Address:
Tester Signature:
Company Name:
Phone #:
Certified Tester #:
The above is certified to be true at the time of testing Service Restored:
Remarks
Pressure Vacuum Breaker
Final Test
Initial Test
Repairs andMaterials Used
Test Date Reduced Pressure Principal Assembly
Double Check Valve Assembly Check Valve
Check Valve #1 Check Valve #2
Air Inlet
Relief Valve
Leaked
PSID
PSID
Leaked Leaked Did Not Open
Contact Name
Mfg:
Serial Number
Size: Model:
Map Page
PSID
Held at PSID
PSID
Held at PSIDOpened at
Did not Open
Closed Tight Closed Tight
Held at PSID
PSID
Held at PSID Opened at
Closed Tight Closed Tight
Existing New Replacement
Replaces SN#
PSID
Opened at Held at
Opened at Held at
Is the Assembly installed in accordance with manufacturers recommendations and/or local codes? Yes No
Water Turn Off Authorization: (Print) Time:
Yes No
Service Address
Location IDFacility Name
Phone:
Mailing Name
City/ST/Zip Telephone
Address 1
ST: Zip:
Assembly Information
Assembly Location Information
Zip:
Hazard Type
Equip Location
Property Information
Fail
Pass
Pass
PWS ID:(206) 555-1213
Type:
1M
Assembly ID
Calib/Accur Date:
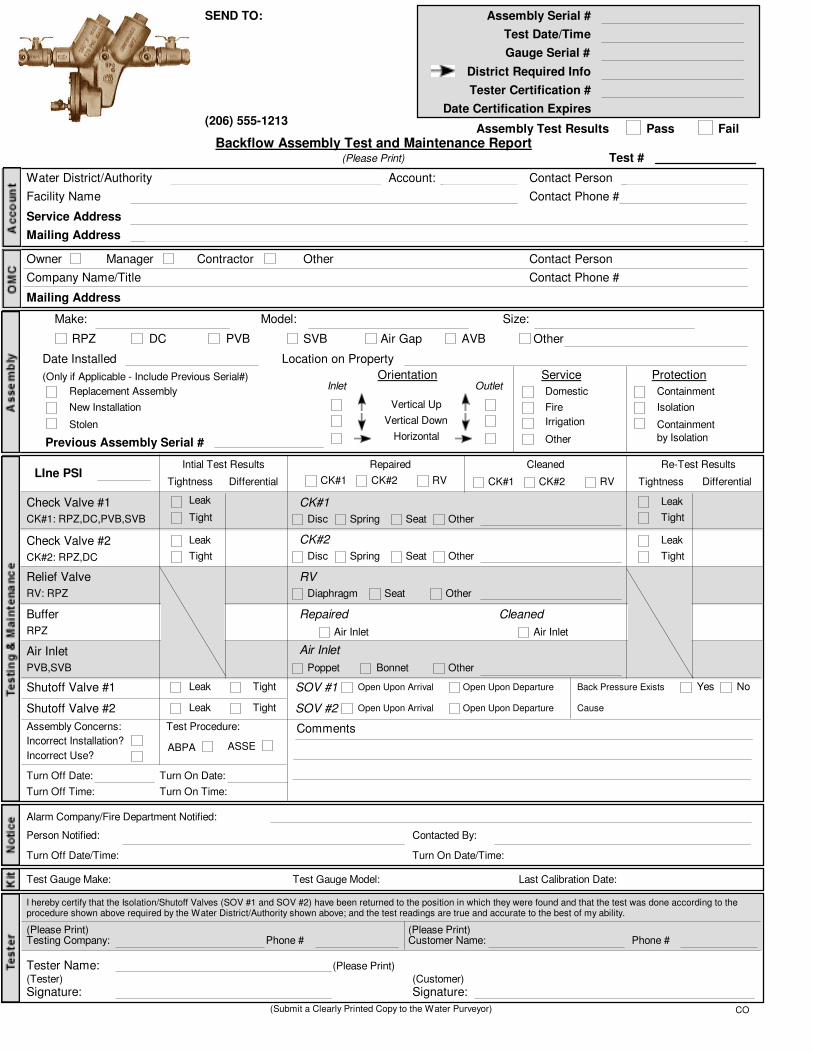
I hereby certify that the Isolation/Shutoff Valves (SOV #1 and SOV #2) have been returned to the position in which they were found and that the test was done according to theprocedure shown above required by the Water District/Authority shown above; and the test readings are true and accurate to the best of my ability.
Protection
Domestic
Containment
by Isolation
Isolation
Containment
Assembly Serial #
Test Date/Time
Gauge Serial #
District Required Info
Tester Certification #
Date Certification Expires
Date Installed
Re-Test Results
Tight
Leak
Tight
Leak
Tightness Differential
Intial Test Results Repaired Cleaned
Tight
Leak
Tight
Leak
Tightness Differential
CK#1
CK#2
RV
Repaired
Air Inlet
Disc Spring Seat Other
Disc Spring Seat Other
Diaphragm Seat Other
Other
Air Inlet
Cleaned
Air Inlet
LIne PSI
Check Valve #1
CK#1: RPZ,DC,PVB,SVB
Check Valve #2
CK#2: RPZ,DC
Relief Valve
RV: RPZ
Buffer
RPZ
Air Inlet
PVB,SVB
Leak Tight
Leak Tight
SOV #1
SOV #2
Open Upon Arrival
Open Upon Arrival
Open Upon Departure
Open Upon Departure
Back Pressure Exists
Cause
Backflow Assembly Test and Maintenance Report(Please Print)
Assembly Test Results Pass Fail
Test #
Water District/Authority
Facility Name
Service Address
Mailing Address
Account: Contact Person
Contact Phone #
Owner
Company Name/Title
Mailing Address
Contact Person
Contact Phone #
Manager Contractor Other
Make: Size:Model:
PVB SVBDCRPZ AVBAir Gap Other
Location on Property
Stolen
New Installation
Replacement Assembly
(Only if Applicable - Include Previous Serial#)
Previous Assembly Serial #
Orientation Service
Irrigation
Fire
OtherHorizontal
Vertical Down
Vertical Up
Inlet Outlet
SEND TO:
Shutoff Valve #1
Shutoff Valve #2
Yes No
Assembly Concerns:
Incorrect Installation?
Incorrect Use?
Turn Off Date:
Turn Off Time:
CK#1 CK#2 RV CK#1 CK#2 RV
Turn On Date:
Turn On Time:
Test Procedure:
ABPA ASSE
Comments
Alarm Company/Fire Department Notified:
Person Notified:
Turn Off Date/Time:
Contacted By:
Turn On Date/Time:
Test Gauge Make: Test Gauge Model: Last Calibration Date:
Testing Company:
Tester Name:
Signature:
(Please Print)
(Tester)
Phone # Customer Name:(Please Print)
Phone #
Signature:(Customer)
(Submit a Clearly Printed Copy to the Water Purveyor)
(Please Print)
CO
(206) 555-1213
Poppet Bonnet
Make/Model Gauge #Calibration Date:
Tester Signature: Cert. No.:
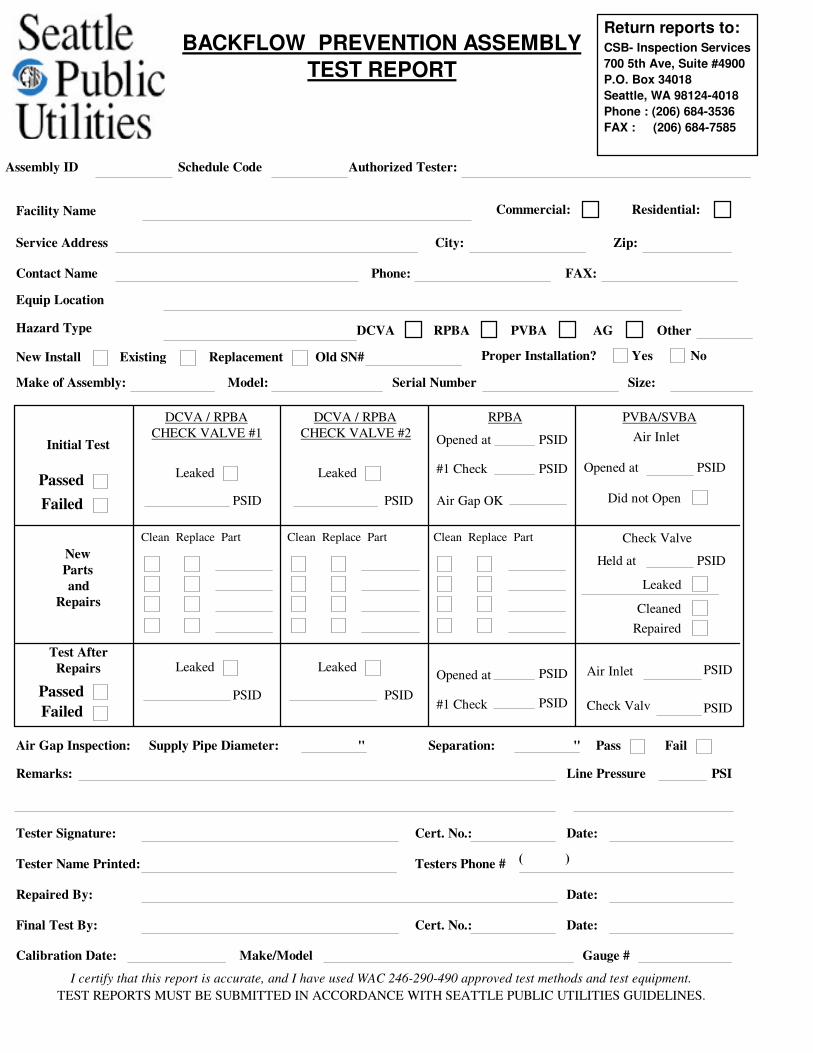
I certify that this report is accurate, and I have used WAC 246-290-490 approved test methods and test equipment.
PVBA/SVBA
Initial Test
DCVA / RPBA
CHECK VALVE #1 Air Inlet
Leaked Leaked
PSID
PSID
PSID
Opened at
Did not Open
Opened at
Failed
Passed
DCVA / RPBA
CHECK VALVE #2
RPBA
PSID#1 Check
Air Gap OK
Check Valve
PSIDHeld at
Leaked
Cleaned
Repaired
Test After
Repairs
New
Parts
and
Repairs
Contact Name Phone: FAX:
Make of Assembly: Serial Number Size:Model:
ExistingNew Install Replacement Old SN# Proper Installation? Yes No
Hazard Type PVBA AGDCVA RPBA Other
Service Address Zip:City:
Facility Name
Equip Location
Failed
Passed
Leaked Leaked PSID
PSID
PSID
PSID
Opened at Air Inlet
PSID#1 Check PSIDCheck Valv
Clean Replace Part Clean Replace Part Clean Replace Part
Authorized Tester:
Line PressureRemarks: PSI
Date:
Tester Name Printed: Testers Phone #( )
Repaired By: Date:
Final Test By: Cert. No.: Date:
Air Gap Inspection: Supply Pipe Diameter: Separation: FailPass""
TEST REPORTS MUST BE SUBMITTED IN ACCORDANCE WITH SEATTLE PUBLIC UTILITIES GUIDELINES.
Commercial: Residential:
PSID
Schedule Code
Return reports to:BACKFLOW PREVENTION ASSEMBLY
TEST REPORTCSB- Inspection Services
700 5th Ave, Suite #4900
P.O. Box 34018
Seattle, WA 98124-4018
Phone : (206) 684-3536
FAX : (206) 684-7585
Assembly ID

Annual Test & Maintenance Report for Backflow Prevention Assemblies
STATE OF OHIO
(All applicable fields must be filled out completely in order for test results to be accepted)
Facility Name:
Contact Person:
Address:
Phone No.
Make:
Model:
Size:
Serial Number:
Assembly Information
Meter Pit
Penthouse
Mechanical Room
Basement
Boiler Room
Protection Provided
Floor Number:
Room Number:
Installation Information
Containment Isolation
Double Check Valve Assembly
Initial
Test
Outer
Valve
1st
Check
Valve
2nd
Check
Valve
psid
psid
Pass
Fail
Pass
Fail
Pass
Fail
Reduced Pressure Assembly
1st
Check Valve
Relief Valve
Opening Point
2nd
Check Valve
psid
psid
Pass
Fail
Pass
Fail
Pass
Fail
Outlet Valve Pass Fail
Pass
Fail
Pass
Fail
Pressure Vacuum Breaker
Air Inlet Valve
Check Valve
psid
psid
Repairs &
Materials
Used
Date
Double Check Valve Assembly
Re-Test
After
Repairs
Outer
Valve
1st
Check
Valve
2nd
Check
Valve
psid
psid
Pass
Fail
Pass
Fail
Pass
Fail
Reduced Pressure Assembly
1st
Check Valve
Relief Valve
Opening Point
2nd
Check Valve
psid
psid
Pass
Fail
Pass
Fail
Pass
Fail
Outlet Valve Pass Fail
Pass
Fail
Pass
Fail
Pressure Vacuum Breaker
Air Inlet Valve
Check Valve
psid
psid
Date
TESTER CERTIFICATION I certify that the above data is correct and that the backflow prevention device is in proper working
condition.
Tester Name (Printed)
Company Name
Signature
OH Cert. No.
Phone No.
DateContractor No.
FACILITY
CERTIFICATION
I hereby certify that the above backflow prevention device has been in constant use at this location during the entire
prescribed interval between test periods and during that period this device was not bypassed, made inoperative or
removed without proper authorization. I further certify that I have the authority and responsibility to ensure the
above.
Owner/Officer (Printed)
Title
Signature Phone No.
Date
Return Original To: Email:
All applicable fields must be filled out completely in order for test results to be accepted
Phone:
Fax:
(206) 555-1213
(206) 555-2121
Make/Model: Gauge #Calibration Date:
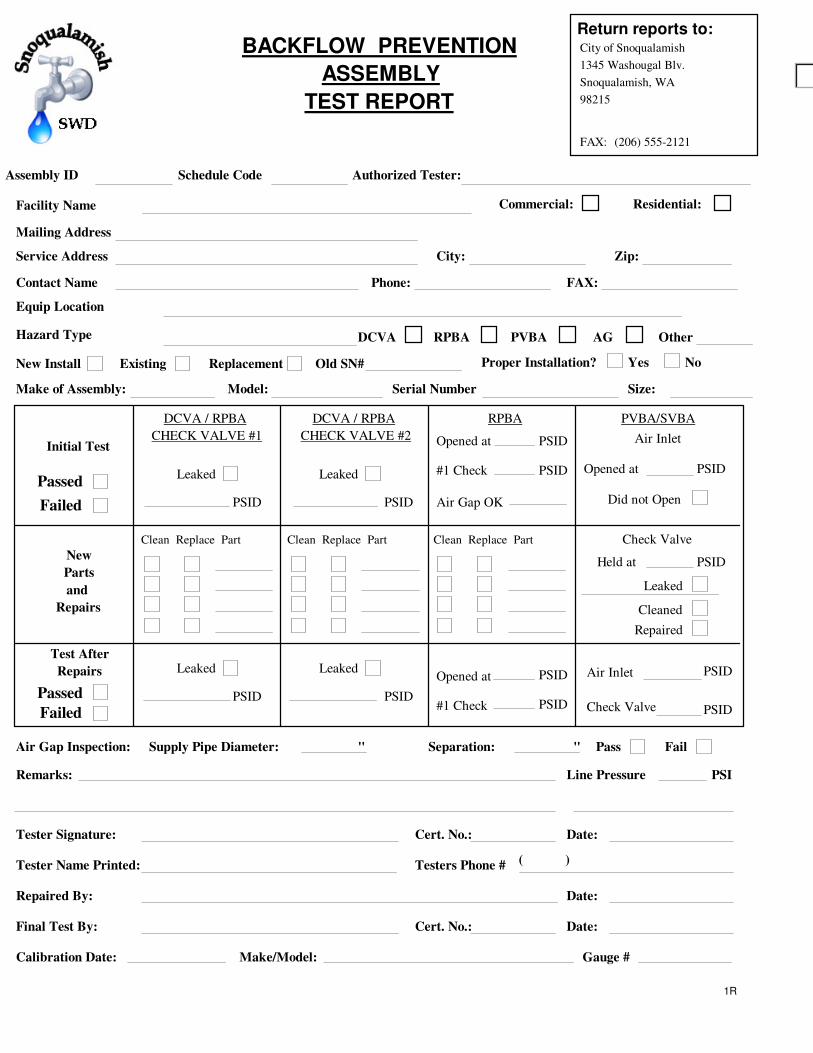
Tester Signature: Cert. No.:
PVBA/SVBA
Initial Test
DCVA / RPBA
CHECK VALVE #1 Air Inlet
Leaked Leaked
PSID
PSID
PSID
Opened at
Did not Open
Opened at
Failed
Passed
DCVA / RPBA
CHECK VALVE #2
RPBA
PSID#1 Check
Air Gap OK
Check Valve
PSIDHeld at
Leaked
Cleaned
Repaired
Test After
Repairs
New
Parts
and
Repairs
Yes No
City of Snoqualamish
1345 Washougal Blv.
Snoqualamish, WA
98215
(206) 555-2121
Failed
Passed
Leaked Leaked PSID
PSID
PSID
PSID
Opened at Air Inlet
PSID#1 Check PSIDCheck Valve
Clean Replace Part Clean Replace Part Clean Replace Part
Line PressureRemarks: PSI
Date:
Tester Name Printed: Testers Phone #( )
Repaired By: Date:
Final Test By: Cert. No.: Date:
Air Gap Inspection: Supply Pipe Diameter: Separation: FailPass""
PSID
FAX:
Return reports to:BACKFLOW PREVENTION
ASSEMBLY
TEST REPORT
1R
Contact Name Phone: FAX:
Make of Assembly: Serial Number Size:Model:
ExistingNew Install Replacement Old SN# Proper Installation?
Hazard Type PVBA AGDCVA RPBA Other
Service Address Zip:City:
Facility Name
Equip Location
Commercial: Residential:
Authorized Tester:Schedule CodeAssembly ID
Mailing Address
0
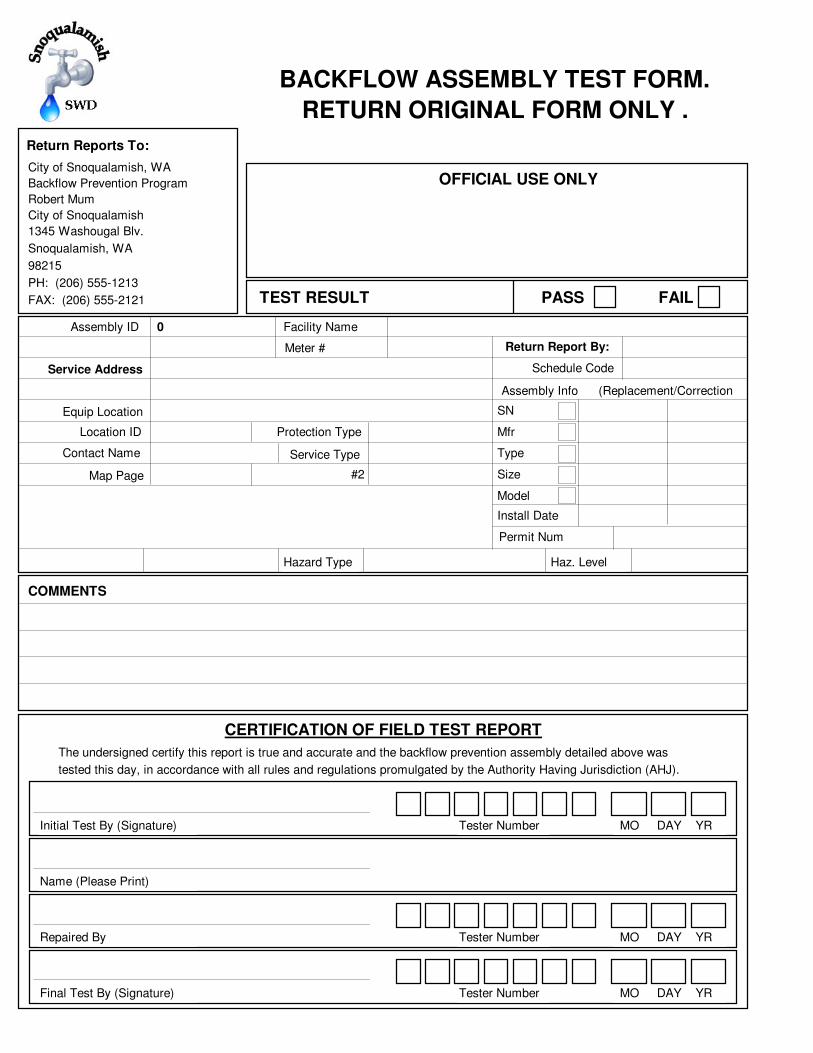
BACKFLOW ASSEMBLY TEST FORM.
RETURN ORIGINAL FORM ONLY .
Service Address
Contact Name
Install Date
Mfr
SN
Size
Type
Model
Return Report By:
Schedule Code
Location ID
Map Page
Permit Num
Hazard Type Haz. Level
Assembly ID
Meter #
Facility Name
Equip Location
Protection Type
#2
Assembly Info
OFFICIAL USE ONLY
TEST RESULT PASS FAIL
COMMENTS
CERTIFICATION OF FIELD TEST REPORT
The undersigned certify this report is true and accurate and the backflow prevention assembly detailed above was
tested this day, in accordance with all rules and regulations promulgated by the Authority Having Jurisdiction (AHJ).
Initial Test By (Signature) Tester Number MO DAY YR
Name (Please Print)
Repaired By Tester Number MO DAY YR
Final Test By (Signature) Tester Number MO DAY YR
Return Reports To:
Service Type
(Replacement/Correction
City of Snoqualamish, WA
Backflow Prevention Program
Robert Mum
City of Snoqualamish
1345 Washougal Blv.
Snoqualamish, WA
98215
PH: (206) 555-1213
FAX: (206) 555-2121
Related Documents











