Azithromycin Pharmacokinetics in Pregnancy James H. Fischer, Pharm.D., FCCP May 17, 2011

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Azithromycin Pharmacokinetics in Pregnancy
James H. Fischer, Pharm.D., FCCP
May 17, 2011
Azithromycin: Background
• Macrolide• Commonly administered for community acquired
respiratory, skin and gynecological infections• Among 15 most frequently prescribed drugs to
pregnant women (2004)• Dose derived from non-pregnant women & men• Practice disregards how dose requirements
affected by pregnancy-related differences:– Pharmacokinetics – Functioning of immune system
Piscitelli et al 1992; Andrade et al 2004; Jamieson 2006

Azithromycin: Pharmacokinetics
• Distinct profile• Incomplete oral absorption (34%)• Extensively distributes into tissues• Eliminated by hepatobiliary excretion
– P-glycoprotein– Multidrug resistance protein-2 (MRP-2)
• Only one previous PK study in pregnancy– Women from Papua-New Guinea receiving
malarial prophylaxis
Ballow et al 1998; Luke & Foulds 1997; Sugie et al 2004; Salmon et al 2010

Objectives
• Compare population pharmacokinetics of azithromycin between pregnant women and nonpregnant women of child bearing age
• Identify factors contributing to the inter-individual variability in azithromycin pharmacokinetics
Research Team• Co-Principal Investigator
Gloria Sarto, M.D., Ph.D.
• Brigham & Women’s Hospital, Harvard – Ruth Tuomala, M.D.– Karen McCarthy, R.N.
• University of Illinois at ChicagoPatricia Fischer, R.N.
Mitra Habibi, Pharm.D.
Sarah Kilpatrick, M.D.
Keith Rodvold, Pharm.D.
• University of WisconsinThomas Jenkins, M.D.
Lori Wollett, R.N.
• University of Michigan– Janet Shier, Pharm.D., M.D.– Zan Daley, R.N.
• FDAMargaret Miller, Ph.D.
Methods: Study Design
• Pilot Study– Goals:
• assist in establishing structural model• provide initial PK parameter estimates
– 12 healthy adult women of child bearing age– Traditional Multi-Dose Pharmacokinetic Study
• 500 mg *1, then 250 mg Q.D. for 4 days• Extensive sampling performed for 96 h following last dose
– Typical eligibility criteria (except allowed OC use)
Methods: Study Design
• Population Pharmacokinetic Study– Prospective, open-label multicenter design– Participants
• Women at least 18 years of age, • Capable of bearing children, • Receiving azithromycin for treatment of infection, and• Either
– Pregnant and at least 12 weeks gestational age, or– Nonpregnant and at least 3 months postpartum.
Methods: Study Design
• Sparse sampling strategy– 5 samples collected within 4 sampling windows– First 3 with any dose, last 2 with final dose
• Drug intake assessed by diary and interviews
Methods: Laboratory Analysis
• Azithromycin Plasma Concentrations– HPLC with electrochemical detection– linear: 10 – 505 ng/ml– LLOQ: 10 ng/ml– inter-assay precision: 3.2% to 5.8%

Methods: Pharmacokinetic Analysis
• Nonlinear mixed effects modeling (NONMEM) with FOCE method
• Subjects with at least one evaluable azithromycin plasma concentration
• Data from healthy women included in population PK database
• Step 1: Identify structural (base) model • Step 2: Covariate Analysis• Step 3: Model validation
Covariates• Body Size Measures
total body weightlean body weightbody mass index
body surface area
• Continuous Variablesagegestational agecreatinine clearanceazithromycin dose
• Categorical Variablespregnancy statusEthnicitystudy sitetype of infectionconcurrent medicationsoral contraceptivesrenal/hepatic diseaseadministration with foodhealthy volunteer
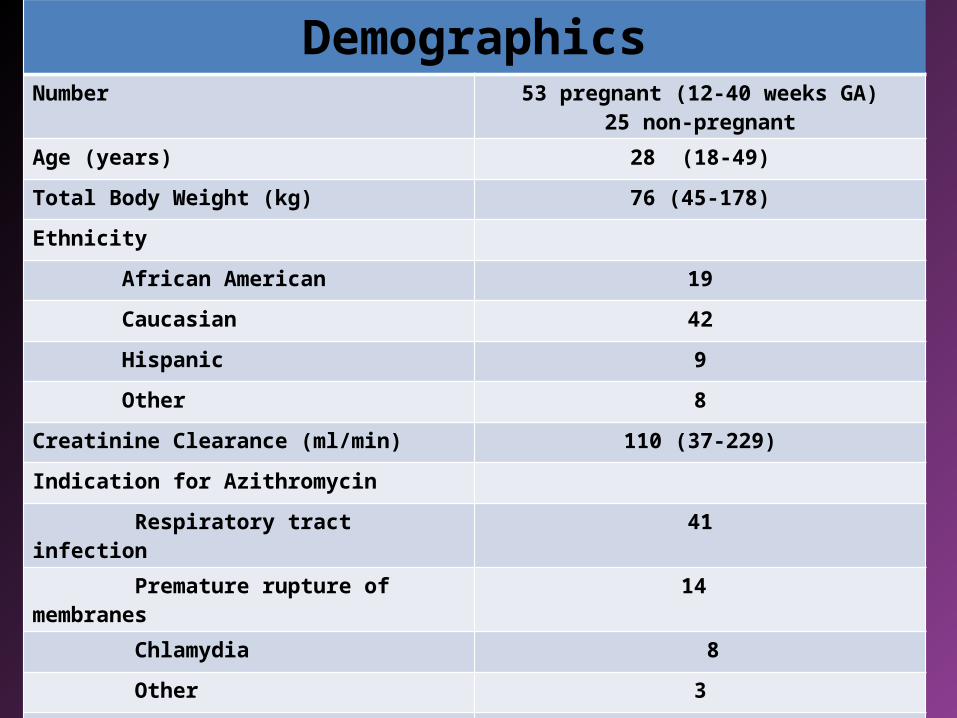
DemographicsNumber 53 pregnant (12-40 weeks GA)
25 non-pregnant
Age (years) 28 (18-49)
Total Body Weight (kg) 76 (45-178)
Ethnicity
African American 19
Caucasian 42
Hispanic 9
Other 8
Creatinine Clearance (ml/min) 110 (37-229)
Indication for Azithromycin
Respiratory tract infection 41
Premature rupture of membranes 14
Chlamydia 8
Other 3
Healthy volunteer 12
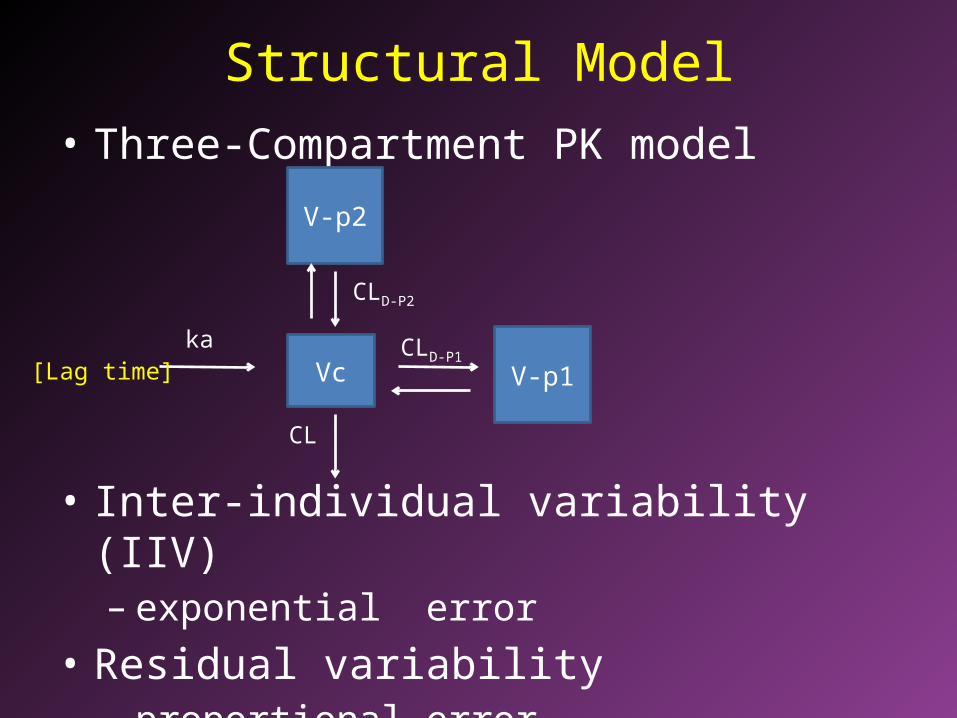
Structural Model• Three-Compartment PK model
• Inter-individual variability (IIV)– exponential error
• Residual variability– proportional error
Vcka
V-p1CLD-P1
CL
V-p2
[Lag time]
CLD-P2
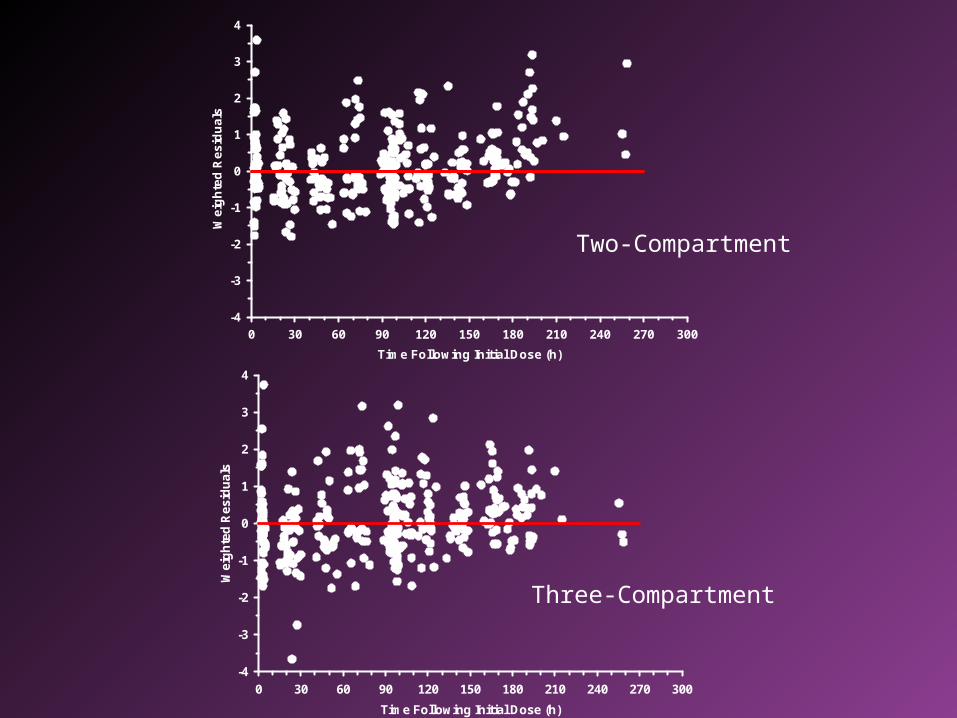
Time Following Initial Dose (h)
0 30 60 90 120 150 180 210 240 270 300
We
igh
ted
Resid
uals
-4
-3
-2
-1
0
1
2
3
4
Time Following Initial Dose (h)
0 30 60 90 120 150 180 210 240 270 300
We
igh
ted
Re
sid
ua
ls
-4
-3
-2
-1
0
1
2
3
4
Two-Compartment
Three-Compartment
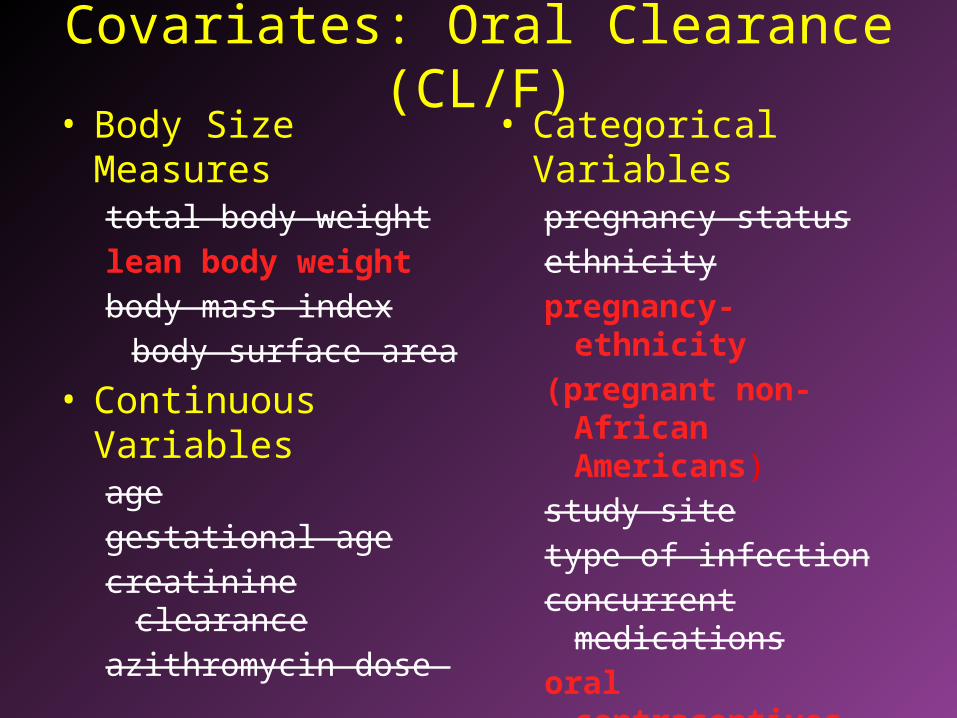
Covariates: Oral Clearance (CL/F)• Body Size Measures
total body weightlean body weightbody mass index
body surface area
• Continuous Variablesagegestational agecreatinine clearanceazithromycin dose
• Categorical Variablespregnancy statusethnicitypregnancy-ethnicity (pregnant non-African
Americans) study sitetype of infectionconcurrent medicationsoral contraceptivesrenal/hepatic diseaseadministration with foodhealthy volunteer
Covariate Models
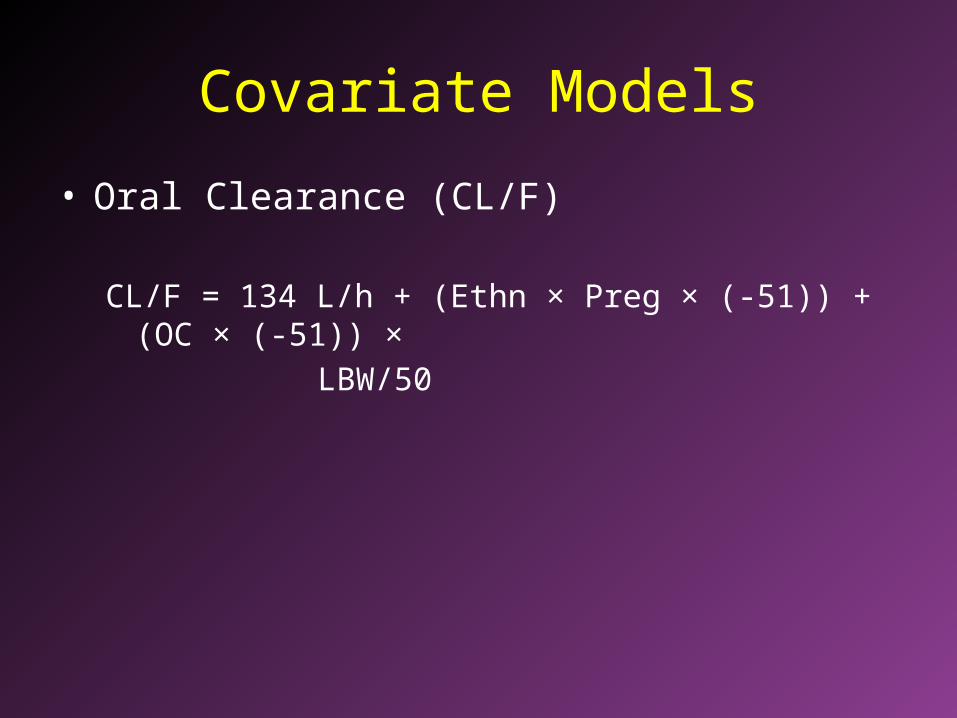
• Oral Clearance (CL/F)
CL/F = 134 L/h + (Ethn × Preg × (-51)) + (OC × (-51)) ×
LBW/50
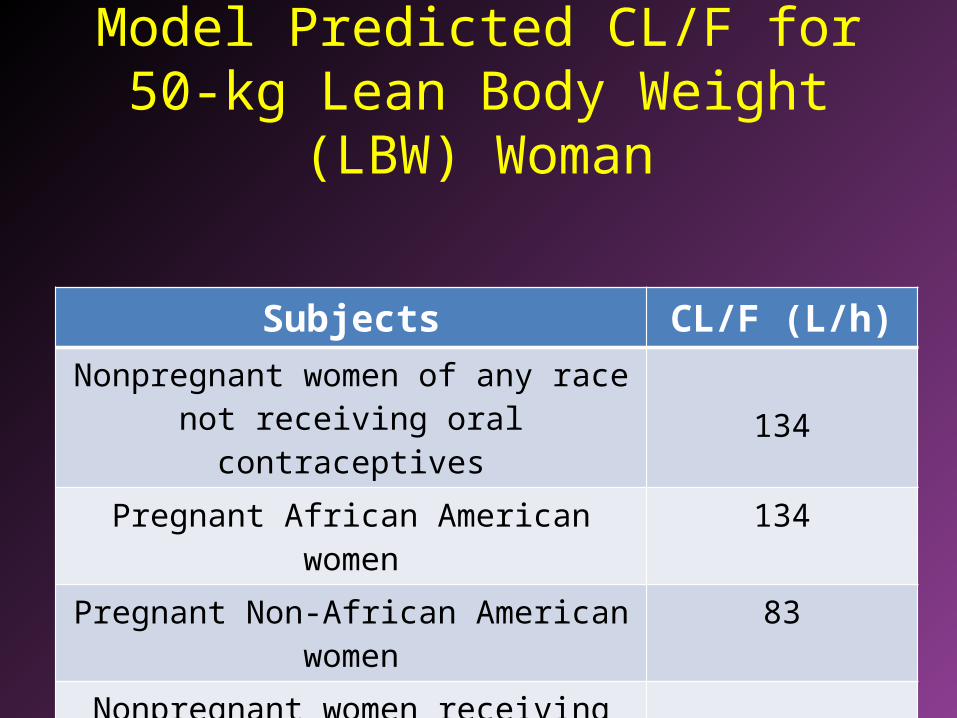
Model Predicted CL/F for 50-kg Lean Body Weight (LBW) Woman
Subjects CL/F (L/h)
Nonpregnant women of any race not receiving oral contraceptives 134
Pregnant African American women 134
Pregnant Non-African American women 83
Nonpregnant women receiving oral contraceptives (OC) 83
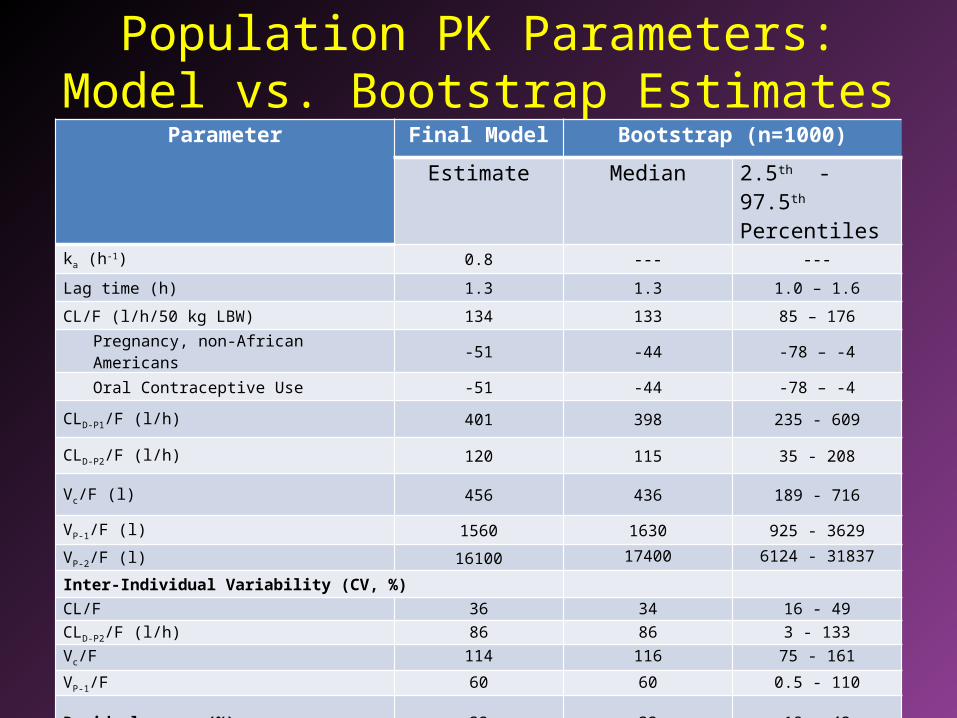
Population PK Parameters: Model vs. Bootstrap Estimates
Parameter Final Model Bootstrap (n=1000)
Estimate Median 2.5th - 97.5th Percentiles
ka (h-1) 0.8 --- ---
Lag time (h) 1.3 1.3 1.0 – 1.6
CL/F (l/h/50 kg LBW) 134 133 85 – 176
Pregnancy, non-African Americans -51 -44 -78 – -4
Oral Contraceptive Use -51 -44 -78 – -4
CLD-P1/F (l/h) 401 398 235 - 609
CLD-P2/F (l/h) 120 115 35 - 208
Vc/F (l) 456 436 189 - 716
VP-1/F (l) 1560 1630 925 - 3629
VP-2/F (l) 16100 17400 6124 - 31837
Inter-Individual Variability (CV, %)CL/F 36 34 16 - 49
CLD-P2/F (l/h) 86 86 3 - 133
Vc/F 114 116 75 - 161
VP-1/F 60 60 0.5 - 110
Residual error (%) 32 32 18 - 42
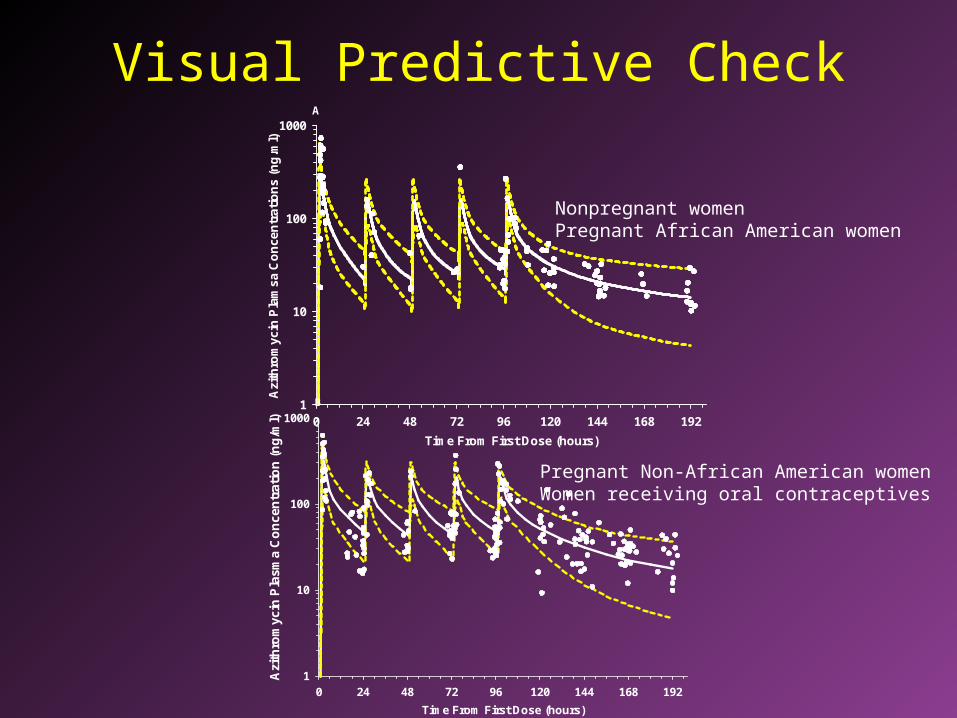
Visual Predictive Check
Time From First Dose (hours)
0 24 48 72 96 120 144 168 192
Azi
thro
myc
in P
lam
sa C
on
cen
trat
ion
s (n
g.m
l)
1
10
100
1000A
Time From First Dose (hours)
0 24 48 72 96 120 144 168 192
Azi
thro
myc
in P
lasm
a C
on
cen
trat
ion
(n
g/m
l)
1
10
100
1000B
Nonpregnant womenPregnant African American women
Pregnant Non-African American womenWomen receiving oral contraceptives
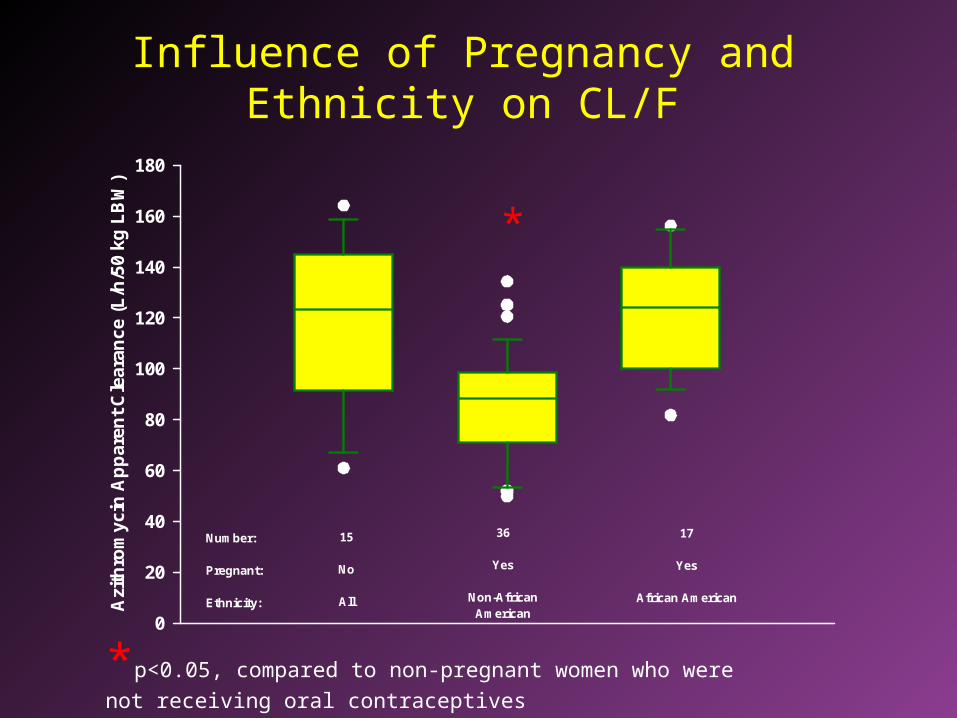
Influence of Pregnancy and Ethnicity on CL/FA
zith
rom
ycin
Ap
par
ent
Cle
aran
ce (
L/h
/50
kg L
BW
)
0
20
40
60
80
100
120
140
160
180
Number:
Pregnant:
Ethnicity:
15
No
All
36
Yes
Non-AfricanAmerican
17
Yes
African American
*
*p<0.05, compared to non-pregnant women who were
not receiving oral contraceptives
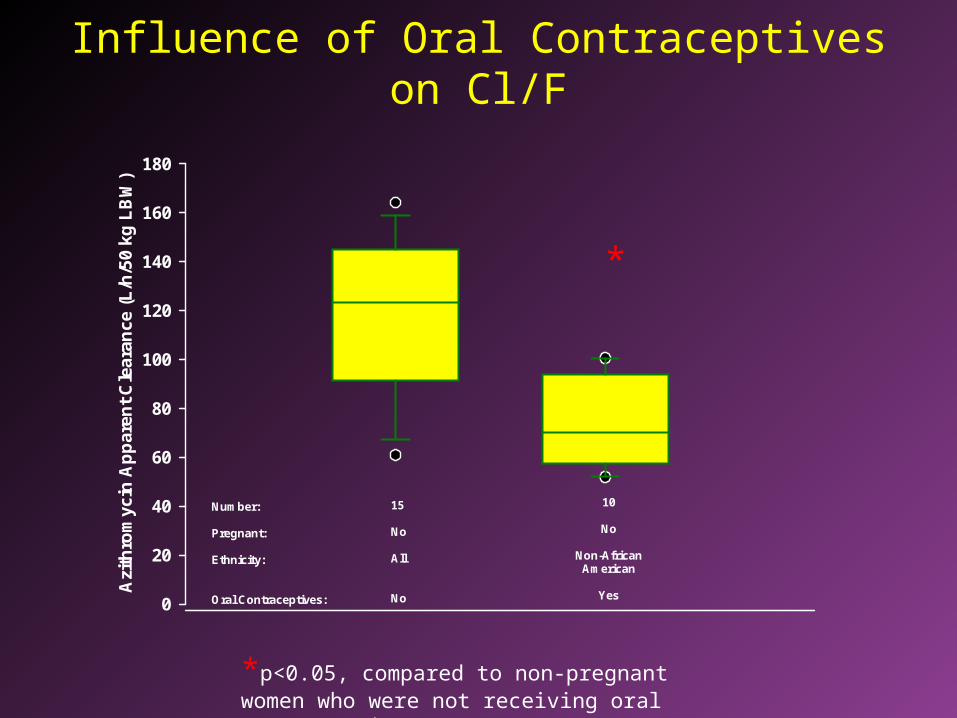
Influence of Oral Contraceptives on Cl/FA
zith
rom
ycin
Ap
par
ent
Cle
aran
ce (
L/h
/50
kg L
BW
)
0
20
40
60
80
100
120
140
160
180
Number:
Pregnant:
Ethnicity:
Oral Contraceptives:
15
No
All
No
10
No
Non-AfricanAmerican
Yes
*
*p<0.05, compared to non-pregnant women who were not receiving oral contraceptives
Conclusions• Ethnicity influences the effect of pregnancy
on azithromycin CL/F• Compared to non-pregnant women,
azithromycin CL/F during pregnancy is unchanged in African American women and 40% lower in non-African Americans
• Concurrent administration of oral contraceptives (OCs) also reduced azithromycin CLoral
Conclusions
• Whether ethnicity also impacts the effect of OCs on CL/F requires further study as no African American women were in the OC cohort.
• These findings suggest that estrogen or progesterone mediate the effects of pregnancy and OCs on azithromycin CL/F.
Research in Pregnant Women
Lessons Learned

IRB Challenges• Vulnerable Population• Options to Participation (other drug options)• Coercion/Undue Influence• Inclusions of subjects < 18 y/o• Risks of Drug Therapy• Restrictions on concurrent drug therapy• Data Safety Monitoring Committee
IRB Challenges• Frequency of Blood Sampling• Translated consent forms• Certificate of Confidentiality• Follow up Data Collection on Newborn
– Consent– Blood sampling
Overcoming Challenges
• Request Pre-review with IRB staff• Study design: Population PK – missed clinic
visit or time limitations have no impact on study integrity
• Be prepared for additional scrutiny

Reasons for not participating
• Time commitment• Illness in addition to pregnancy – did not want
additional burden• Aversion to needle sticks• Discomfort with 24 hr blood pressure monitor
– Staff wore first to develop strategies
Subject Recruitment Strategies
• Involve Primary Physician– Assure physician that research is independent of
clinical care– Provide overview to potential subject
• Experienced Study Coordinator• Coordination with clinical care services
– Other labs– Ultrasounds– Prolonged monitoring
Subject Recruitment Strategies
• Multiple sites– Adequate number of subjects– Diversity of population
• Age• Ethnicity• Diagnosis• Liver/renal function• Body size
Related Documents











