Avaliação da Função Sisto-diastólica em Doentes Insuficientes Renais em Hemodiálise - Utilidade do Doppler Tissular e do Speckle Tracking para Determinar Parâmetros Independentes de Carga [75] LÍGIA MENDES, REGINA RIBEIRAS, TERESA ADRAGÃO, SÓNIA LIMA, EDUARDA HORTA, CARLA REIS, TIAGO AMARAL, CARLOS AGUIAR, RAQUEL GOUVEIA, ANICETO SILVA Serviço de Cardiologia - Hospital de Santa Cruz, Carnaxide, Portugal Rev Port Cardiol 2008; 27 (9): 1011-1025 ARTIGOS ORIGINAIS 1011 RESUMO Introdução: Os parâmetros ecocardiográficos convencionais por serem dependentes de carga não permitem uma adequada avaliação da função sisto-diastólica ventricular esquerda. As novas metodologias ecocardiográficas têm- -se revelado promissoras, no entanto ainda é controverso se são totalmente independentes da volémia. Objectivo: Os autores pretenderam identificar parâmetros ecocardiográficos independentes de carga para avaliação da função sisto-diastólica em doentes com insuficiência renal terminal (IRT) em programa de hemodiálise (HD). Proposeram-se ainda avaliar a equivalência entre as novas metodologias ecocardiográficas. Métodos: Estudaram-se 20 doentes consecutivos com IRT clinicamente estáveis em programa de HD há mais de 4 meses (idade média 51 ± 12 anos, 14 homens). Todos realizaram ecocardiograma imediatamente antes e após HD. Os volumes das cavidades cardíacas, a fracção de ejecção do ventrículo esquerdo, o fluxo Doppler espectral pulsado transmitral foram avaliados segundo as recomendações da Sociedade Americana de Ecocardiografia. As velocidades longitudinais do anel mitral septal e lateral foram obtidas por Doppler tissular pulsado (DTIp). As velocidades longitudinais miocárdicas sistólicas e diastólicas foram obtidas nas projecções apicais por Doppler tissular codificado por cor (DTIc) e por speckle tracking (STI). Foram calculadas as razões, entre a ABSTRACT Load-independent Parameters of Diastolic and Systolic Function by Speckle Tracking and Tissue Doppler in Hemodialysis Patients Background: Assessment of diastolic function using conventional Doppler techniques is limited by their significant dependence on volume load status. Whether new echocardiographic methods are load- independent in evaluating left ventricular systolic and diastolic function remains controversial. Objective: The aim of this study was to identify load-independent echocardiographic parameters for systolic and diastolic function in end-stage renal disease (ESRD) patients undergoing hemodialysis (HD) and to evaluate agreement between the new methods. Methods: We studied 20 clinically stable patients with ESRD on HD for >4 months (mean age 51±12 years, 14 men, four with coronary disease). All had a transthoracic echocardiogram immediately before and after HD. Cardiac chamber volumes, left ventricular ejection fraction, and transmitral Doppler flow (E/A ratio) were determined according to American Society of Echocardiography guidelines. Pulsed tissue Doppler imaging (TDI) was used to record septal and lateral mitral annular velocities. Longitudinal systolic (Sm), early diastolic (Em) and late diastolic (Am) myocardial velocities and strain were Recebido para publicação: Março de 2008 • Aceite para publicação: Maio de 2008 Received for publication: March 2008 • Accepted for publication: May 2008

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Avaliação da Função Sisto-diastólica emDoentes Insuficientes Renais em
Hemodiálise - Utilidade do Doppler Tissulare do Speckle Tracking para DeterminarParâmetros Independentes de Carga [75]
LÍGIA MENDES, REGINA RIBEIRAS, TERESA ADRAGÃO, SÓNIA LIMA, EDUARDA HORTA, CARLA REIS, TIAGO AMARAL,CARLOS AGUIAR, RAQUEL GOUVEIA, ANICETO SILVA
Serviço de Cardiologia - Hospital de Santa Cruz, Carnaxide, Portugal
Rev Port Cardiol 2008; 27 (9): 1011-1025
ARTIGOS ORIGINAIS
1011
RESUMO
Introdução: Os parâmetros ecocardiográficosconvencionais por serem dependentes de
carga não permitem uma adequada avaliaçãoda função sisto-diastólica ventricular esquerda.As novas metodologias ecocardiográficas têm-
-se revelado promissoras, no entanto ainda écontroverso se são totalmente independentes
da volémia. Objectivo: Os autores pretenderam identificar
parâmetros ecocardiográficos independentes decarga para avaliação da função sisto-diastólica
em doentes com insuficiência renal terminal(IRT) em programa de hemodiálise (HD).
Proposeram-se ainda avaliar a equivalênciaentre as novas metodologias ecocardiográficas.
Métodos: Estudaram-se 20 doentesconsecutivos com IRT clinicamente estáveis
em programa de HD há mais de 4 meses(idade média 51 ± 12 anos, 14 homens). Todos
realizaram ecocardiograma imediatamenteantes e após HD. Os volumes das cavidades
cardíacas, a fracção de ejecção do ventrículoesquerdo, o fluxo Doppler espectral pulsado
transmitral foram avaliados segundo asrecomendações da Sociedade Americana de
Ecocardiografia. As velocidades longitudinaisdo anel mitral septal e lateral foram obtidas por
Doppler tissular pulsado (DTIp). Asvelocidades longitudinais miocárdicas
sistólicas e diastólicas foram obtidas nasprojecções apicais por Doppler tissular
codificado por cor (DTIc) e por speckle tracking(STI). Foram calculadas as razões, entre a
ABSTRACT
Load-independent Parameters of Diastolicand Systolic Function by Speckle Trackingand Tissue Doppler in HemodialysisPatients
Background: Assessment of diastolic functionusing conventional Doppler techniques islimited by their significant dependence onvolume load status. Whether newechocardiographic methods are load-independent in evaluating left ventricularsystolic and diastolic function remainscontroversial.Objective: The aim of this study was to identifyload-independent echocardiographicparameters for systolic and diastolic function inend-stage renal disease (ESRD) patientsundergoing hemodialysis (HD) and to evaluateagreement between the new methods.Methods: We studied 20 clinically stablepatients with ESRD on HD for >4 months(mean age 51±12 years, 14 men, four withcoronary disease). All had a transthoracicechocardiogram immediately before and afterHD. Cardiac chamber volumes, left ventricularejection fraction, and transmitral Doppler flow(E/A ratio) were determined according toAmerican Society of Echocardiographyguidelines. Pulsed tissue Doppler imaging(TDI) was used to record septal and lateralmitral annular velocities. Longitudinal systolic(Sm), early diastolic (Em) and late diastolic(Am) myocardial velocities and strain were
Recebido para publicação: Março de 2008 • Aceite para publicação: Maio de 2008Received for publication: March 2008 • Accepted for publication: May 2008

INTRODUÇÃO
Aecocardiografia é actualmente o método deescolha para avaliação da função sisto-
-diastólica do ventrículo esquerdo (1,2). Os maisvariados índices têm sido adiantados paraestimar as pressões de enchimento, relaxamentoe rigidez. Sabe-se que inúmeras condiçõesfisiológicas como a idade, a volémia, a
INTRODUCTION
Echocardiography is currently the method ofchoice to assess left ventricular (LV) systolic
and diastolic function (1,2). Several differentindices have been proposed to estimate fillingpressures, relaxation and stiffness. The fact thatvarious physiological factors such as age, bloodvolume, heart rate and blood viscosity affect the1012
Rev Port CardiolVol. 27 Setembro 08 / September 08
velocidade de fluxo do enchimento rápidoventricular (E) e a velocidade tissular
diastólica precoce (Em) e entre as velocidadestissulares diastólicas precoce (Em) e tardia
(Am). As potenciais diferenças dasmetodologias Doppler tissular e speckle
tracking foram estudadas. Resultados: A média de volume ultra-filtradofoi 2800 ± 820 ml (entre 1200-4200 ml). Os
volumes tele-diastólicos da aurícula e doventrículo esquerdos, tal como a velocidade
máxima da onda E do fluxo Dopplertransmitral diminuiram significativamente apósa HD. As velocidades longitudinais diastólicas
precoces do anel mitral e miocárdicasdiminuiram significativamente
independentemente do método. A média daspressões de enchimento eram elevadas antes e
não se alterou após variação da volémia. Afracção de ejecção do ventrículo esquerdo era>44% em todos os doentes não se registando
alterações após a HD. Quer as velocidadeslongitudinais de pico sistólico do anel mitral e
miocárdicas (obtidas por qualquer dosmétodos), quer o strain global e longitudinal
foram semelhantes antes e após HD.Conclusão: No nosso estudo grandes variações
de volémia associaram-se a alteraçõessignificativas das velocidades longitudinaisdiastólicas precoces. Pelo contrário a razão
E/Em e os parâmetros de avaliação sistólicarevelaram-se independentes de carga. Os
resultados dos parâmetros de avaliação sisto--diastólica obtidos através dos três métodos
revelaram-se concordantes.
Palavras-Chave
Insuficiência renal terminal; Hemodiálise; Speckle tracking;
Doppler tissular; Strain; Ecocardiografia, Função sistólica;
Função diastólica
determined by color TDI and also by speckletracking imaging (STI), using apical views. Theratio between the rapid filling wave E andmitral early diastolic filling velocity (E/Em)and the Am/Em ratio were calculated, usingspectral Doppler, pulsed TDI, color TDI, andSTI.Results: Mean ultrafiltration volume was2800±820 ml (range 1200-4200 ml). Left atrial(LA) and left ventricular (LV) end-diastolicvolumes and transmitral pulsed Doppler flowdecreased significantly after HD. Earlydiastolic myocardial velocities also decreasedsignificantly, regardless of the evaluationmethod. Filling pressure ratios were high andremained unchanged after HD. LV ejectionfraction was >44% in all patients and did notchange after HD. Systolic myocardialvelocities, by any method, and global andlongitudinal strain were also similar before andafter HD.Conclusion: Large acute changes in volumeload were associated with significant variationsin early diastolic myocardial longitudinalvelocities, thus demonstrating the dependenceof Em on volume load. By contrast, E/Em ratiosappeared to be load-independent, as weresystolic function parameters. Pulsed TDI, colorTDI, and STI yielded similar results for theassessment of diastolic and systolic myocardialparameters
Key words
End-stage renal disease; Hemodialysis; Speckle tracking;
Tissue Doppler; Strain; Echocardiography; Systolic function;
Diastolic function

frequência cardíaca e a viscosidade sanguínea,modificam o padrão de fluxo espectral pulsadotransmitral, urge pois encontrar parâmetros deavaliação funcional menos dependentes. ODoppler tissular embora dependente dosmovimentos de lateralidade e rotação domiocárdio tem sido adiantado como métodonão invasivo para avaliação da função regionalmiocárdica (3-5). O que ainda se encontra porestabelecer é a sua real independência de cargajá que os resultados dos estudos publicados nãosão consensuais (6-10). Recentemente têm sidoutilizadas novas metodologias de avaliação defunção miocárdica como o strain, que avalia adeformação (11-15), mas a sua correlação com acarga é igualmente desconhecida. Actualmenteexistem dois métodos ultrassonográficos paracalcular a deformabilidade do miocárdio: o strainderivado do Doppler tissular cor (DTIc) e o strainderivado de imagens bidimensionais (speckletracking - STI). Na imagem bidimensional, cadaregião de interesse tem um único padrão de ecos(speckle) que é relativamente estável durante ociclo cardíaco, sendo possível monitorizarimagem a imagem a sua posição (tracking). Omovimento e a alteração de posição dos ‘speckles’fornece-nos informação sobre a deformabilidadedo miocárdio (16).
Muitos dos estudos utilizados para deter-minação de índices ecocardiográficos indepen-dentes de carga, foram realizados com fármacosnão traduzindo uma verdadeira alteração davolémia. Seria portanto útil definir parâmetrosinsensíveis às alterações de carga, através deestudos com variação efectiva da pré-carga.
OBJECTIVOS
Identificar parâmetros ecocardiográficos deavaliação de função sisto-diastólica indepen-dentes de carga, utilizando o modelo do doentehemodialisado (variação de carga controladae comparação com o mesmo doente). Avaliar aequivalência dos resultados obtidos pelasrecentes metodologias ecocardiográficas.
MÉTODOS
População Foram estudados 20 doentes (idade média de
pattern of transmitral Doppler flow has led to asearch for less load-dependent assessmentparameters. Tissue Doppler imaging (TDI),although dependent on the lateral and rotatorymotion of the myocardium, has been proposed asa noninvasive method for evaluation of regionalmyocardial function (3,4,5). What remains to beestablished is whether it is really load-independent, since results of published studiesare conflicting (6-10). New methods of assessingmyocardial function have been explored, such asstrain imaging to measure deformation (11-16), buthow they correlate with load is also unknown. Atpresent there are two ultrasound techniques formeasuring strain: color TDI and two-dimensionalspeckle tracking imaging (STI). In the two-dimensional method, each region of interest has aunique speckle pattern, which is relatively stablethroughout the cardiac cycle and its movementcan be tracked image by image. The positionalchanges of the speckles provide information onmyocardial deformation (17).
Many of the studies used to establish load-independent echocardiographic indices wereperformed with drugs, and therefore do not reflecta real change in blood volume. It would thereforebe useful to define parameters that are notaffected by load conditions through studies ofactual variations in preload.
OBJECTIVES
The aim of the study was to identify load-independent echocardiographic parametersfor systolic and diastolic function in thehemodialysis (HD) patient (with controlledvariation in load and comparison in the samepatient), and to evaluate agreement between theresults obtained by new echocardiographicmethods.
METHODS
PopulationWe studied 20 patients (mean age 51±12
years, 14 men) with end-stage renal diseaseundergoing 3-4 hemodialysis sessions a week formore than four months. Median time of dialysiswas 35 months (P25 12 months, P75 78 months).All the patients were clinically stable and in 1013
LÍGIA MENDES, et alRev Port Cardiol 2008; 27: 1011-25

51±12 anos, 14 homens) com insuficiência renalterminal em programa de hemodiálise de 3 a 4sessões semanais há mais de 4 meses. A medianade tempo da diálise era de 35 meses (P25 12meses, P75 78 meses). Foram incluídos doentesclinicamente estáveis, em ritmo sinusal. Aetiologia da insuficiência renal era nefrosclerosesecundária à hipertensão arterial em oitodoentes, nefropatia da síndrome da imuno-deficiência humana em cinco doentes, nefropatiadiabética em dois doentes, nefropatia secundáriaa doença poliquistica renal em quatro doentes eum doente tinha nefropatia por mieloma mútiplo.Foram critérios de exclusão doença valvularsignificativa, função sistólica significativamentedeprimida (fracção de ejecção ventricularesquerda inferior a 40%), síndrome coronáriaaguda prévia (4 doentes tinham angina estávelcom doença diagnosticada em angiografiacoronária prévia), pericardite aguda ou crónicae/ou síndrome febril. Foi obtido consentimentoinformado de todos os doentes.
ProtocoloA estimativa de peso seco é individualizada
empiricamente para cada doente e baseia-se emsinais clínicos de hidratação e comportamento dapressão arterial durante várias sessões de diálise.Foram usadas máquinas de diálise Gambro AK200F, com filtro de poliamida, regulado parafluxo de sangue de 300 a 400 ml/min e fluxo dedialisante de 500 ml/min.
Foi avaliada a pressão arterial sistólica ediastólica, frequência cardíaca, peso antes edepois da hemodiálise. O ultrafiltrado foiestimado pela diferença de peso antes e depois doprocedimento, assumindo 1 Kg = 1 litro, como emoutros estudos (17).
O ecocardiograma foi realizado imediata-mente antes e trinta minutos após a hemodiálise,os exames foram realizados por um operadorque desconhecia os dados clínicos do doente e acarga retirada.
Em todos os indivíduos foi efectuadoecocardiograma com análise 2D, Modo M,Doppler espectral, Doppler tissular pulsado(DTIp) e Doppler tissular codificado (DTIc).Os exames foram realizados utilizando umecocardiógrafo Vivid 7 Dimension GE® equipadocom sonda de frequência variável (1.7 - 3 MHz) ecom tecnologia para execução de Dopplertissular pulsado e codificado cor, as imagens
sinus rhythm. The etiology of renal failure wasnephrosclerosis secondary to hypertension ineight patients, HIV-related nephropathy in five,diabetic nephropathy in two, nephropathysecondary to polycystic kidney disease in four,and nephropathy due to multiple myeloma in one.Exclusion criteria were significant valve disease,significantly impaired systolic function (leftventricular ejection fraction of <40%), previousacute coronary syndrome (four patients had stableangina with previously diagnosed angiographiccoronary artery disease), and acute or chronicpericarditis and/or fever syndrome. Informedconsent was obtained from all patients.
Study protocolDry weight is estimated empirically for each
individual patient and is based on clinical signsof hydration and blood pressure (BP) behaviorduring several dialysis sessions. Gambro AK 200F dialysis machines fitted with polyamidemembranes were used, with blood flow rate set to300 to 400 ml/min and dialysis fluid flow rate to500 ml/min.
Systolic and diastolic BP, heart rate andweight were measured before and afterhemodialysis. Ultrafiltration volume wasestimated as the difference in weight before andafter the procedure, assuming 1 kg = 1 liter, as inother studies (18).
An echocardiogram was performedimmediately before and 30 minutes afterhemodialysis by an operator who was unaware ofthe patient’s clinical data or of the load removed.
All individuals underwent echocardiographicstudy, with two-dimensional, M-mode, spectralDoppler, pulsed TDI and color TDI analysis. Theexams were performed on a Vivid 7 DimensionGE® scanner, fitted with a variable frequencyprobe (1.7-3 MHz) and able to perform pulsedand color tissue Doppler study; the images weresubsequently analyzed on an EchoPac GE®
workstation equipped for speckle tracking. Theimages were acquired with the patients in leftlateral decubitus during shallow breathing. Thegains and filters were adjusted to obtain the bestquality images.
The exams were performed by fourechocardiographers and the offline analysis bytwo Level III echocardiographers.
1014
Rev Port CardiolVol. 27 Setembro 08 / September 08
foram posteriormente analisadas na workstationEchoPac GE®, com capacidade para a análise despeckle tracking. As imagens foram adquiridascom os doentes em decúbito lateral esquerdo edurante respiração superficial. Os ganhos e osfiltros foram ajustados para adquirir imagens demelhor qualidade.
Os exames foram executados por quatroecocardiografistas e a análise offline foi realizadapor dois ecocardiografistas de nível III.
Avaliação por ecocardiografiaconvencional (2D e MM e Dopplerespectral e cor)
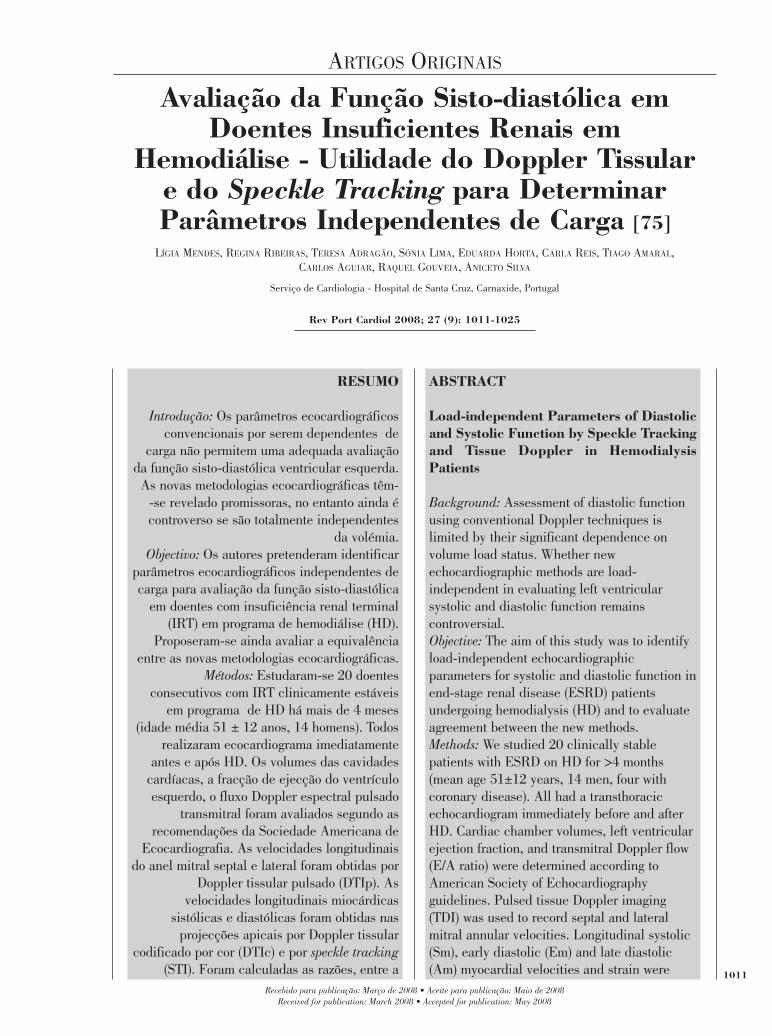
As dimensões das cavidades foram obtidassegundo as recomendações da SociedadeAmericana de Ecocardiografia (18) (Figura 1).
A fracção de ejecção do ventrículo esquerdo(FEVE) foi obtida através da alteração dapercentagem de volumes do ventrículo entre asístole e a diástole em apical 2 e 4 câmaras,utilizando o método de Simpson modificado(média de 3 valores).
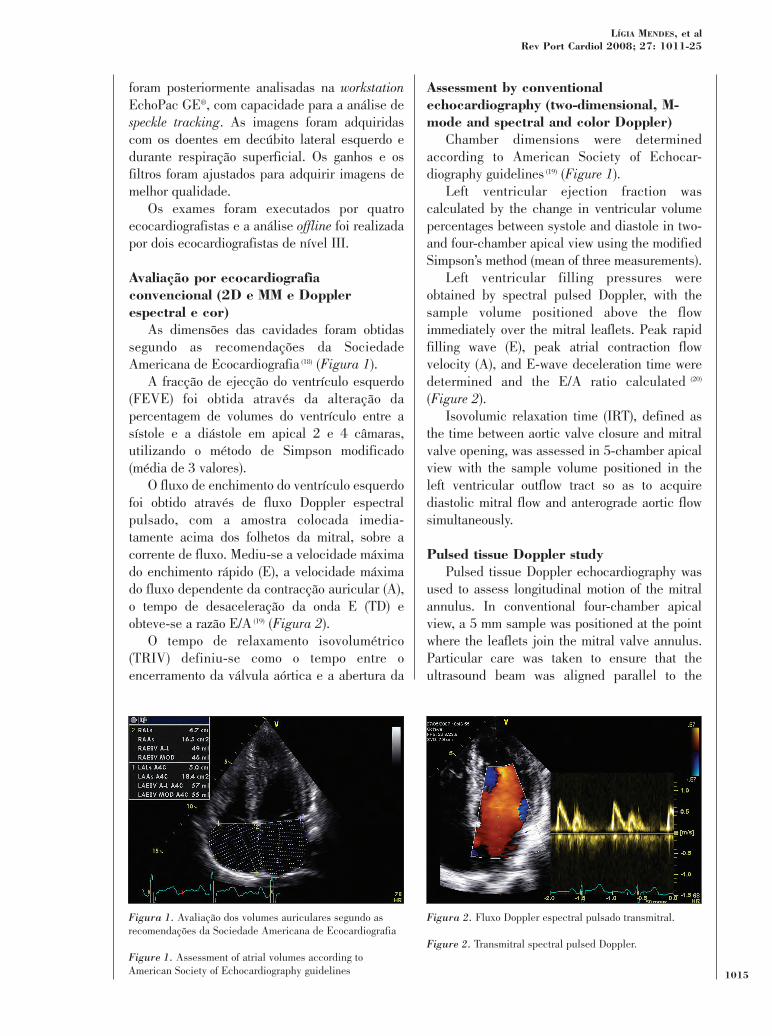
O fluxo de enchimento do ventrículo esquerdofoi obtido através de fluxo Doppler espectralpulsado, com a amostra colocada imedia-tamente acima dos folhetos da mitral, sobre acorrente de fluxo. Mediu-se a velocidade máximado enchimento rápido (E), a velocidade máximado fluxo dependente da contracção auricular (A),o tempo de desaceleração da onda E (TD) eobteve-se a razão E/A (19) (Figura 2).
O tempo de relaxamento isovolumétrico(TRIV) definiu-se como o tempo entre oencerramento da válvula aórtica e a abertura da
Assessment by conventionalechocardiography (two-dimensional, M-mode and spectral and color Doppler)
Chamber dimensions were determinedaccording to American Society of Echocar-diography guidelines (19) (Figure 1).
Left ventricular ejection fraction wascalculated by the change in ventricular volumepercentages between systole and diastole in two-and four-chamber apical view using the modifiedSimpson’s method (mean of three measurements).
Left ventricular filling pressures wereobtained by spectral pulsed Doppler, with thesample volume positioned above the flowimmediately over the mitral leaflets. Peak rapidfilling wave (E), peak atrial contraction flowvelocity (A), and E-wave deceleration time weredetermined and the E/A ratio calculated (20)
(Figure 2).Isovolumic relaxation time (IRT), defined as
the time between aortic valve closure and mitralvalve opening, was assessed in 5-chamber apicalview with the sample volume positioned in theleft ventricular outflow tract so as to acquirediastolic mitral flow and anterograde aortic flowsimultaneously.
Pulsed tissue Doppler studyPulsed tissue Doppler echocardiography was
used to assess longitudinal motion of the mitralannulus. In conventional four-chamber apicalview, a 5 mm sample was positioned at the pointwhere the leaflets join the mitral valve annulus.Particular care was taken to ensure that theultrasound beam was aligned parallel to the
1015
LÍGIA MENDES, et alRev Port Cardiol 2008; 27: 1011-25
Figura 1. Avaliação dos volumes auriculares segundo asrecomendações da Sociedade Americana de Ecocardiografia
Figure 1. Assessment of atrial volumes according toAmerican Society of Echocardiography guidelines
Figura 2. Fluxo Doppler espectral pulsado transmitral.
Figure 2. Transmitral spectral pulsed Doppler.
válvula mitral. Obteve-se numa projecção apical5 câmaras colocando-se a amostra na câmara desaída do ventrículo esquerdo de forma a adquirirsimultaneamente o fluxo mitral diastólico e ofluxo anterógrado aórtico.
Avaliação por Doppler tissular pulsado A ecocardiografia com Doppler tissular
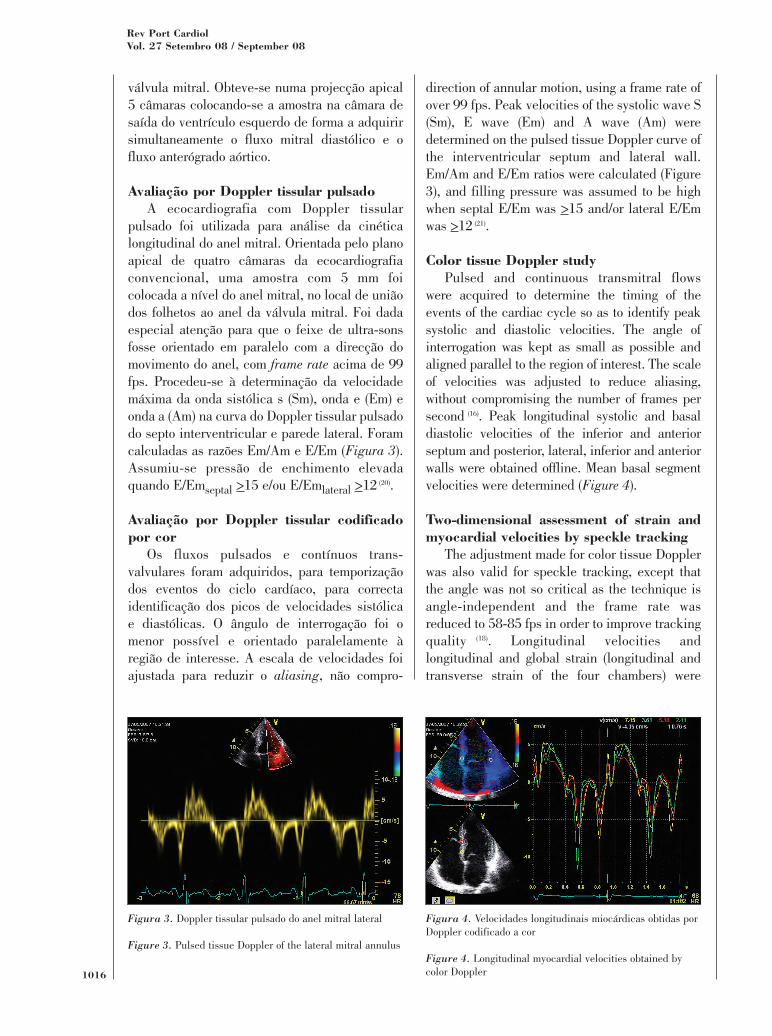
pulsado foi utilizada para análise da cinéticalongitudinal do anel mitral. Orientada pelo planoapical de quatro câmaras da ecocardiografiaconvencional, uma amostra com 5 mm foicolocada a nível do anel mitral, no local de uniãodos folhetos ao anel da válvula mitral. Foi dadaespecial atenção para que o feixe de ultra-sonsfosse orientado em paralelo com a direcção domovimento do anel, com frame rate acima de 99fps. Procedeu-se à determinação da velocidademáxima da onda sistólica s (Sm), onda e (Em) eonda a (Am) na curva do Doppler tissular pulsadodo septo interventricular e parede lateral. Foramcalculadas as razões Em/Am e E/Em (Figura 3).Assumiu-se pressão de enchimento elevadaquando E/Emseptal >15 e/ou E/Emlateral >12 (20).
Avaliação por Doppler tissular codificadopor cor
Os fluxos pulsados e contínuos trans-valvulares foram adquiridos, para temporizaçãodos eventos do ciclo cardíaco, para correctaidentificação dos picos de velocidades sistólicae diastólicas. O ângulo de interrogação foi omenor possível e orientado paralelamente àregião de interesse. A escala de velocidades foiajustada para reduzir o aliasing, não compro-
direction of annular motion, using a frame rate ofover 99 fps. Peak velocities of the systolic wave S(Sm), E wave (Em) and A wave (Am) weredetermined on the pulsed tissue Doppler curve ofthe interventricular septum and lateral wall.Em/Am and E/Em ratios were calculated (Figure3), and filling pressure was assumed to be highwhen septal E/Em was >15 and/or lateral E/Emwas >12 (21).
Color tissue Doppler studyPulsed and continuous transmitral flows
were acquired to determine the timing of theevents of the cardiac cycle so as to identify peaksystolic and diastolic velocities. The angle ofinterrogation was kept as small as possible andaligned parallel to the region of interest. The scaleof velocities was adjusted to reduce aliasing,without compromising the number of frames persecond (16). Peak longitudinal systolic and basaldiastolic velocities of the inferior and anteriorseptum and posterior, lateral, inferior and anteriorwalls were obtained offline. Mean basal segmentvelocities were determined (Figure 4).
Two-dimensional assessment of strain andmyocardial velocities by speckle tracking
The adjustment made for color tissue Dopplerwas also valid for speckle tracking, except thatthe angle was not so critical as the technique isangle-independent and the frame rate wasreduced to 58-85 fps in order to improve trackingquality (18). Longitudinal velocities andlongitudinal and global strain (longitudinal andtransverse strain of the four chambers) were
1016
Rev Port CardiolVol. 27 Setembro 08 / September 08
Figura 3. Doppler tissular pulsado do anel mitral lateral
Figure 3. Pulsed tissue Doppler of the lateral mitral annulus
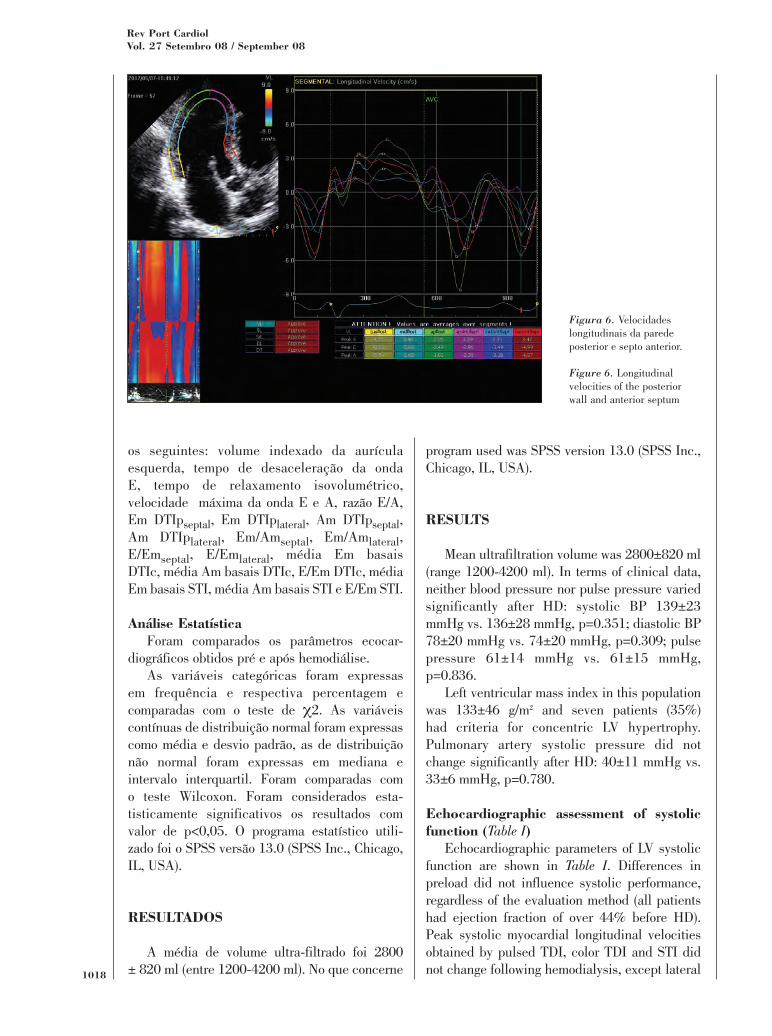
Figura 4. Velocidades longitudinais miocárdicas obtidas porDoppler codificado a cor
Figure 4. Longitudinal myocardial velocities obtained bycolor Doppler
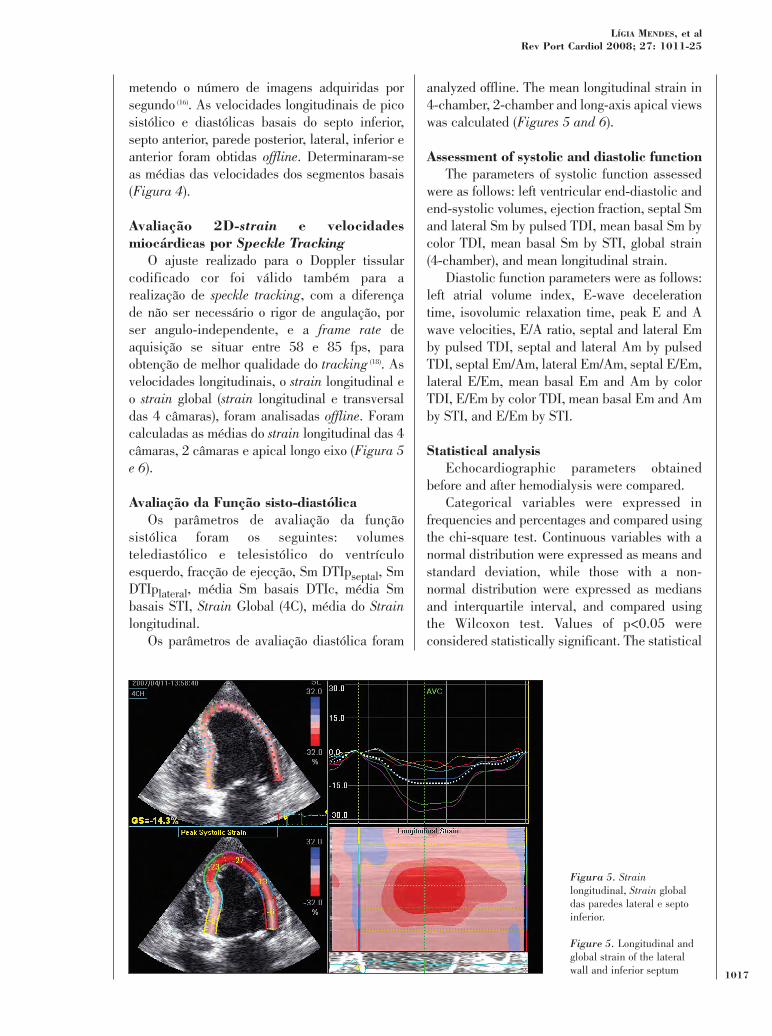
metendo o número de imagens adquiridas porsegundo (16). As velocidades longitudinais de picosistólico e diastólicas basais do septo inferior,septo anterior, parede posterior, lateral, inferior eanterior foram obtidas offline. Determinaram-seas médias das velocidades dos segmentos basais(Figura 4).
Avaliação 2D-strain e velocidadesmiocárdicas por Speckle Tracking
O ajuste realizado para o Doppler tissularcodificado cor foi válido também para arealização de speckle tracking, com a diferençade não ser necessário o rigor de angulação, porser angulo-independente, e a frame rate deaquisição se situar entre 58 e 85 fps, paraobtenção de melhor qualidade do tracking (18). Asvelocidades longitudinais, o strain longitudinal eo strain global (strain longitudinal e transversaldas 4 câmaras), foram analisadas offline. Foramcalculadas as médias do strain longitudinal das 4câmaras, 2 câmaras e apical longo eixo (Figura 5e 6).
Avaliação da Função sisto-diastólicaOs parâmetros de avaliação da função
sistólica foram os seguintes: volumestelediastólico e telesistólico do ventrículoesquerdo, fracção de ejecção, Sm DTIpseptal, SmDTIplateral, média Sm basais DTIc, média Smbasais STI, Strain Global (4C), média do Strainlongitudinal.
Os parâmetros de avaliação diastólica foram
analyzed offline. The mean longitudinal strain in4-chamber, 2-chamber and long-axis apical viewswas calculated (Figures 5 and 6).
Assessment of systolic and diastolic functionThe parameters of systolic function assessed
were as follows: left ventricular end-diastolic andend-systolic volumes, ejection fraction, septal Smand lateral Sm by pulsed TDI, mean basal Sm bycolor TDI, mean basal Sm by STI, global strain(4-chamber), and mean longitudinal strain.
Diastolic function parameters were as follows:left atrial volume index, E-wave decelerationtime, isovolumic relaxation time, peak E and Awave velocities, E/A ratio, septal and lateral Emby pulsed TDI, septal and lateral Am by pulsedTDI, septal Em/Am, lateral Em/Am, septal E/Em,lateral E/Em, mean basal Em and Am by colorTDI, E/Em by color TDI, mean basal Em and Amby STI, and E/Em by STI.
Statistical analysisEchocardiographic parameters obtained
before and after hemodialysis were compared.Categorical variables were expressed in
frequencies and percentages and compared usingthe chi-square test. Continuous variables with anormal distribution were expressed as means andstandard deviation, while those with a non-normal distribution were expressed as mediansand interquartile interval, and compared usingthe Wilcoxon test. Values of p<0.05 wereconsidered statistically significant. The statistical
1017
LÍGIA MENDES, et alRev Port Cardiol 2008; 27: 1011-25
Figura 5. Strainlongitudinal, Strain globaldas paredes lateral e septoinferior.
Figure 5. Longitudinal andglobal strain of the lateralwall and inferior septum
os seguintes: volume indexado da aurículaesquerda, tempo de desaceleração da ondaE, tempo de relaxamento isovolumétrico,velocidade máxima da onda E e A, razão E/A,Em DTIpseptal, Em DTIplateral, Am DTIpseptal,Am DTIplateral, Em/Amseptal, Em/Amlateral,E/Emseptal, E/Emlateral, média Em basaisDTIc, média Am basais DTIc, E/Em DTIc, médiaEm basais STI, média Am basais STI e E/Em STI.
Análise EstatísticaForam comparados os parâmetros ecocar-
diográficos obtidos pré e após hemodiálise.As variáveis categóricas foram expressas
em frequência e respectiva percentagem ecomparadas com o teste de χ2. As variáveiscontínuas de distribuição normal foram expressascomo média e desvio padrão, as de distribuiçãonão normal foram expressas em mediana eintervalo interquartil. Foram comparadas como teste Wilcoxon. Foram considerados esta-tisticamente significativos os resultados comvalor de p<0,05. O programa estatístico utili-zado foi o SPSS versão 13.0 (SPSS Inc., Chicago,IL, USA).
RESULTADOS
A média de volume ultra-filtrado foi 2800± 820 ml (entre 1200-4200 ml). No que concerne
program used was SPSS version 13.0 (SPSS Inc.,Chicago, IL, USA).
RESULTS
Mean ultrafiltration volume was 2800±820 ml(range 1200-4200 ml). In terms of clinical data,neither blood pressure nor pulse pressure variedsignificantly after HD: systolic BP 139±23mmHg vs. 136±28 mmHg, p=0.351; diastolic BP78±20 mmHg vs. 74±20 mmHg, p=0.309; pulsepressure 61±14 mmHg vs. 61±15 mmHg,p=0.836.
Left ventricular mass index in this populationwas 133±46 g/m2 and seven patients (35%)had criteria for concentric LV hypertrophy.Pulmonary artery systolic pressure did notchange significantly after HD: 40±11 mmHg vs.33±6 mmHg, p=0.780.
Echocardiographic assessment of systolicfunction (Table I)
Echocardiographic parameters of LV systolicfunction are shown in Table I. Differences inpreload did not influence systolic performance,regardless of the evaluation method (all patientshad ejection fraction of over 44% before HD).Peak systolic myocardial longitudinal velocitiesobtained by pulsed TDI, color TDI and STI didnot change following hemodialysis, except lateral1018
Rev Port CardiolVol. 27 Setembro 08 / September 08
Figura 6. Velocidadeslongitudinais da paredeposterior e septo anterior.
Figure 6. Longitudinalvelocities of the posteriorwall and anterior septum
aos dados clínicos, nem os valores tensionais,nem a pressão de pulso variaram signifi-cativamente após a HD. Tensão arterial sistólica:139 ± 23 mmHg vs 136 ± 28 mmHg, p = 0,351.Tensão arterial diastólica: 78 ± 20 mmHg vs 74± 20 mmHg, p = 0,309. Pressão de pulso: 61 ± 14mmHg vs 61 ± 15 mmHg, p = 0,836.
A massa indexada do ventrículo esquerdodeterminada nesta população foi de 133 ± 46g/m2 e sete doentes (35%) tinham critérios dehipertrofia ventricular esquerda concêntrica. Apressão sistólica da artéria pulmonar não foisignificativamente diferente antes e após a HD,40 ± 11 mmHg vs 33 ± 6 mmHg, p= 0,780.
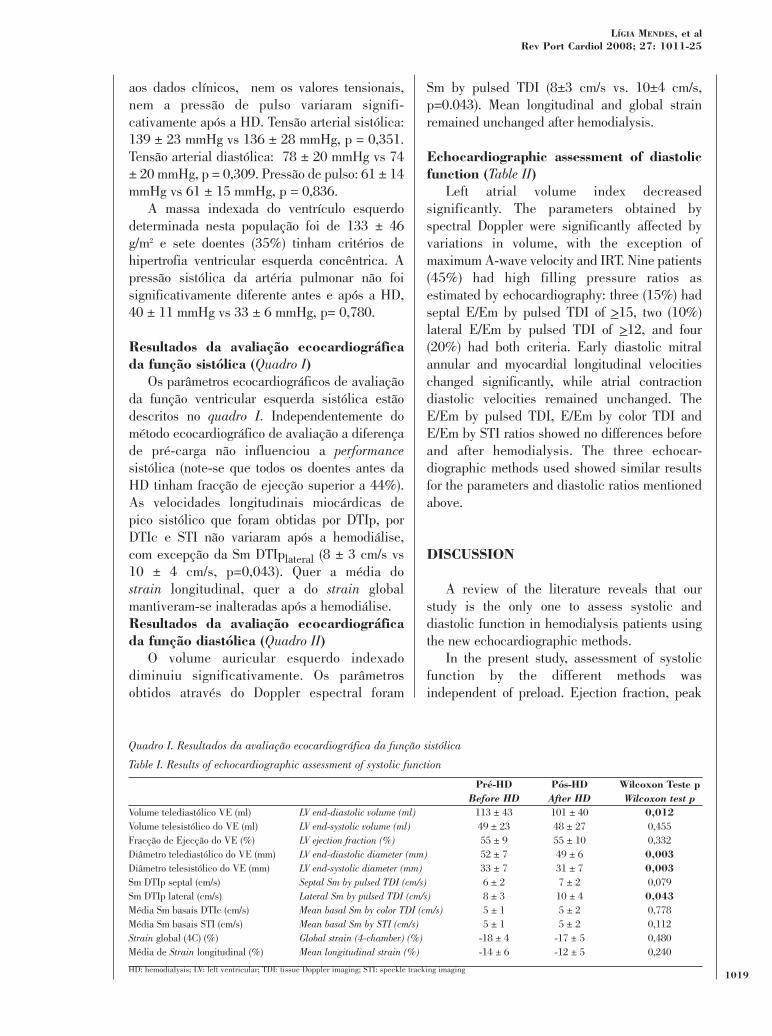
Resultados da avaliação ecocardiográficada função sistólica (Quadro I)
Os parâmetros ecocardiográficos de avaliaçãoda função ventricular esquerda sistólica estãodescritos no quadro I. Independentemente dométodo ecocardiográfico de avaliação a diferençade pré-carga não influenciou a performancesistólica (note-se que todos os doentes antes daHD tinham fracção de ejecção superior a 44%).As velocidades longitudinais miocárdicas depico sistólico que foram obtidas por DTIp, porDTIc e STI não variaram após a hemodiálise,com excepção da Sm DTIplateral (8 ± 3 cm/s vs10 ± 4 cm/s, p=0,043). Quer a média dostrain longitudinal, quer a do strain globalmantiveram-se inalteradas após a hemodiálise.Resultados da avaliação ecocardiográficada função diastólica (Quadro II)
O volume auricular esquerdo indexadodiminuiu significativamente. Os parâmetrosobtidos através do Doppler espectral foram
Sm by pulsed TDI (8±3 cm/s vs. 10±4 cm/s,p=0.043). Mean longitudinal and global strainremained unchanged after hemodialysis.
Echocardiographic assessment of diastolicfunction (Table II)
Left atrial volume index decreasedsignificantly. The parameters obtained byspectral Doppler were significantly affected byvariations in volume, with the exception ofmaximum A-wave velocity and IRT. Nine patients(45%) had high filling pressure ratios asestimated by echocardiography: three (15%) hadseptal E/Em by pulsed TDI of >15, two (10%)lateral E/Em by pulsed TDI of >12, and four(20%) had both criteria. Early diastolic mitralannular and myocardial longitudinal velocitieschanged significantly, while atrial contractiondiastolic velocities remained unchanged. TheE/Em by pulsed TDI, E/Em by color TDI andE/Em by STI ratios showed no differences beforeand after hemodialysis. The three echocar-diographic methods used showed similar resultsfor the parameters and diastolic ratios mentionedabove.
DISCUSSION
A review of the literature reveals that ourstudy is the only one to assess systolic anddiastolic function in hemodialysis patients usingthe new echocardiographic methods.
In the present study, assessment of systolicfunction by the different methods wasindependent of preload. Ejection fraction, peak
1019
LÍGIA MENDES, et alRev Port Cardiol 2008; 27: 1011-25
Volume telediastólico VE (ml)Volume telesistólico do VE (ml)Fracção de Ejecção do VE (%)Diâmetro telediastólico do VE (mm)Diâmetro telesistólico do VE (mm)Sm DTIp septal (cm/s)Sm DTIp lateral (cm/s)Média Sm basais DTIc (cm/s)Média Sm basais STI (cm/s)Strain global (4C) (%)Média de Strain longitudinal (%)
LV end-diastolic volume (ml)LV end-systolic volume (ml)LV ejection fraction (%)LV end-diastolic diameter (mm)LV end-systolic diameter (mm)Septal Sm by pulsed TDI (cm/s)Lateral Sm by pulsed TDI (cm/s)Mean basal Sm by color TDI (cm/s)Mean basal Sm by STI (cm/s)Global strain (4-chamber) (%)Mean longitudinal strain (%)
Pré-HDBefore HD
113 ± 4349 ± 2355 ± 952 ± 733 ± 76 ± 28 ± 35 ± 15 ± 1
-18 ± 4-14 ± 6
Pós-HDAfter HD101 ± 4048 ± 2755 ± 1049 ± 631 ± 77 ± 210 ± 45 ± 25 ± 2
-17 ± 5-12 ± 5
Wilcoxon Teste pWilcoxon test p
0,0120,4550,3320,0030,0030,0790,0430,7780,1120,4800,240
Quadro I. Resultados da avaliação ecocardiográfica da função sistólica
Table I. Results of echocardiographic assessment of systolic function
HD: hemodialysis; LV: left ventricular; TDI: tissue Doppler imaging; STI: speckle tracking imaging

marcadamente afectados pela variaçãovolémica, com excepção da velocidade máximada onda A e do TRIV. Nove doentes (45%) tinhampressões de enchimento elevadas estimadaspor ecocardiografia: três doentes (15%) tinhamE/Em DTIpseptal >15, dois doentes (10%) E/EmDTIplateral >12 e quatro doentes (20%)conjugavam os dois critérios. As velocidadeslongitudinais diastólicas precoces do anel mitrale miocárdicas, variaram atingindo significadoestatístico, enquanto que as velocidadesdiastólicas dependentes da contração auricularse mantiveram inalteradas. As razões E/EmDTIp, E/Em DTIc e E/Em STI não registaramdiferenças antes e após hemodiálise. Obser-vou-se concordância entre as três metodologiasecocardigráficas utilizadas, no que respeita aosparâmetros e razões diastólicas acima referidos.
DISCUSSÃO
Revista a literatura o nosso estudo é o únicorealizado para avaliação conjugada da funçãosisto-diastólica em doentes hemodialisados,utilizando as novas metodologias ecocardio-gráficas.
No nosso estudo a avaliação da funçãosistólica, determinada pelos diferentes métodos
systolic mitral annular velocities, systolicmyocardial longitudinal velocities determined bycolor TDI and STI, and longitudinal and globalstrain did not differ significantly before and afterhemodialysis. It should be noted that althoughsystolic function as assessed by ejection fractionwas preserved or only mildly impaired and thepatients were free of symptoms of heart failure,systolic longitudinal velocities and myocardialstrain were lower than normal values (22).
It is generally assumed that a heart withpreserved systolic function obeys the Frank-Starling law (23), that is, a reduction in end-diastolic volume results in decreased inotropism(lower peak systolic longitudinal velocities andstrain). This was not the case in our population.In our patients, such a reduction in inotropismsecondary to lower end-diastolic volume mayhave been canceled out by the increasedinotropism arising from removal of cardiotoxicmetabolites. The reductions seen in longitudinaland global strain were far from reachingstatistical significance, which does not supportthe idea put forward by some authors of a closerelationship between strain and end-diastolicvolume (24).
In contrast to our results, in the studies ofBauer et al. (25) and Barberato et al. (26), also ofpatients undergoing hemodialysis, systolic mitral
1020
Rev Port CardiolVol. 27 Setembro 08 / September 08
Volume da aurícula esquerda (ml/m2)Tempo de desaceleração da onda E (m/s)Tempo de relaxamento isovolumétrica (m/s)Velocidade máxima onda E (m/s)Velocidade máxima onda A (m/s)E/AEm DTIp septal (cm/s)Em DTIp lateral (cm/s)Am DTIp septal (cm/s)Am DTIp lateral (cm/s)Em/Am septalEm/Am lateralE/Em septalE/Em lateralMédia Em basais DTIc (cm/s)
Média Am basais DTIc (cm/s)E/Em DTIc Média Em basais STI (cm/s)Média Am basais STI (cm/s)E/Em STI
Left atrial volume (ml/m2)E-wave deceleration time (m/s)Isovolumic relaxation time (m/s)Peak E-wave velocity (m/s)Peak A-wave velocity (m/s)E/A ratioSeptal Em by pulsed TDI (cm/s)Lateral Em by pulsed TDI (cm/s)Septal Am by pulsed TDI (cm/s)Lateral Am by pulsed TDI (cm/s)Septal Em/Am Lateral Em/Am Septal E/Em Lateral E/Em Mean basal Em by color TDI (cm/s)Mean basal Am by color TDI (cm/s)E/Em by color TDI Mean basal Em by STI (cm/s)Mean basal Am by STI (cm/s)E/Em by STI
Pré-HDBefore HD
32 ± 13214 ± 6092 ± 2797 ± 3987 ± 391.2 ± 0.5
-7 ± 3-10 ± 4-9 ± 2-9 ± 2
0.8 ± 0.31.2 ± 0.716 ± 1010 ± 7-6 ± 3-6 ± 2
-22 ± 23-6 ± 2-6 ± 1
-22 ± 19
Pós-HDAfter HD24 ± 14270 ± 8499 ± 2676 ±4082 ± 461 ± 0.8-6 ± 2-7 ± 5-9 ± 3-8 ± 6
0.7 ± 0.31.1 ± 0.8 15 ± 1110 ± 9-5 ± 2-6 ± 3-17 ± 8-4 ± 1-6 ± 2-18 ± 9
Wilcoxon Teste pWilcoxon test p
0,0010,0010,2860,0010,4330,0300,0130,0140,7880,8870,0840,0030,1780,1330,0300,9700,8810,0400,7630,502
Quadro II. Resultados da avaliação ecocardiográfica da função diastólica
Table II. Results of echocardiographic assessment of diastolic function
HD: hemodialysis; TDI: tissue Doppler imaging; STI: speckle tracking imaging

foi independente da pré-carga. A fracção deejecção, as velocidades do anel mitral de picosistólico, as velocidades miocárdicas longitu-dinais sistólicas determinadas por DTIc eSTI, o strain longitudinal, e o strain global nãoforam diferentes pré e pós hemodiálise. Importasalientar que, embora a função sistólica avaliadapela fracção de ejecção estivesse conservada oucom disfunção de grau muito ligeiro e os doenteslivres de sintomas de insuficiência cardíaca, asvelocidades longitudinais sistólicas e o strainforam inferiores aos parâmetros normais (21).
Assume-se actualmente que um coraçãocom função sistólica preservada obedece à lei deFrank-Starling (22): a uma diminuição do volumetelediastólico corresponde uma diminuição deinotropismo (menores velocidades longitudinaisde pico sistólico e strain). Tal não se verificouna nossa população. Nos nossos doentes adiminuição de inotropismo secundário aomenor volume telediastólico, poderá ter sidoantagonizado pelo ganho do mesmo, decorrenteda depuração de metabolitos cardiotóxicos. Adiminuição observada quer no Strainlongitudinal, quer global esteve longe de atingirsignificado estatístico não corroborando a ideia,defendida por alguns autores, da existência deuma relação estreita entre o Strain e o volumetelediastólico (23).
Contrariamente ao nosso estudo, nos trabalhosde Bauer et al (24) e Barberato et al (25) realizadostambém em doentes hemodialisados, asvelocidades longitudinais sistólicas do anelmitral e miocárdicas aumentaram significa-tivamente. Nestes estudos talvez o ganho doinotropismo secundário à eliminação dosmetabolitos tenha superado a reduçãoinotrópica secundária à diminuição do volumetelediastólico. Note-se que as médias deultra-filtrados destes últimos, foram inferioresàs do nosso estudo, podendo ser esta, uma dasrazões para estes resultados.
Abali et al (26), avaliou ecocardiograficamente101 indivíduos saudáveis pré e pós doação desangue (500ml). Aqui as (Sm) permaneceramconstantes, registando-se apenas diminuiçãodo strain sistólico (28 ± 8 vs 21 ± 4 %, p=0,03).
Noutros protocolos (6,8), em que se utilizou anitroglicerina para diminuir a pré-carga emindivíduos saudáveis, a função sistólica foideterminada através da fracção de ejecção e dasvelocidades longitudinais sistólicas do anel
annular and myocardial longitudinal velocitiesincreased significantly. It is possible that in thesestudies the gain in inotropism secondary toelimination of metabolites was greater than thereduced inotropic action secondary to reducedend-diastolic volume. Mean ultrafiltrationvolumes were also lower than in our study, whichmay partly explain their results.
Abali et al. (27) assessed 101 healthyindividuals echocardiographically before andafter blood donation (500 ml), and found thatpeak systolic velocities remained unchanged,with a decrease in systolic strain only (28±8 vs.21±4%, p=0.03).
Other protocols (6, 8), using nitroglycerin todecrease preload in healthy individuals, assessedsystolic function by ejection fraction and systolicmitral annular and myocardial longitudinalvelocities. In these, there was no reduction inblood volume and thus no changes in ventricularvolumes, with parameters of systolic functionremaining unchanged.
To summarize, small changes in preload donot alter echocardiographic parameters of systolicfunction, as shown in studies of blood donors andpharmacological protocols. Improvement mayeven be seen in hemodialysis patients with lowultrafiltration volumes, in whom increasedinotropism due to clearance of cardiotoxicmetabolites is observed. A balance is maintainedwith larger ultrafiltration volumes, with nochanges in systolic function parameters.
The morphology of transmitral spectral pulsedDoppler flows depends on different variables,such as left atrial pressure, preload, afterload,respiratory rate, heart rate and alterations inleft ventricular relaxation. Reduced preloaddecreases E and A wave velocities, and so theseare of no use to assess diastolic function whenthere are changes in volume. Although tissueDoppler imaging has shown promise inidentifying load-independent diastolic param-eters (3, 4, 5), it is not known whether their behaviorwill be affected by significant changes in preload.
In our study, transmitral early filling velocity(E) and Em by pulsed TDI, color TDI and STIdecreased significantly, while transmitral atrialvelocity (A) and Am by pulsed TDI, color TDIand STI did not change. As would be expected,E/A and Em/Am ratios also decreased, thedifference reaching statistical significance, whilethe E/Em ratio remained unchanged. With the 1021
LÍGIA MENDES, et alRev Port Cardiol 2008; 27: 1011-25
mitral e miocárdicas. Neste contexto não houveperda de volémia, não ocorrendo alterações dosvolumes ventriculares, mantendo-se inalteráveisos parâmetros de avaliação da função sistólica.
Resumindo, as pequenas alterações depré-carga, não alteram os parâmetrosecocardiográficos de avaliação sistólica(estudos em dadores de sangue e protocolosfarmacológicos). Pode mesmo haver melhoriaem doentes hemodialisados com ultrafiltradospouco significativos, cujo ganho de inotropismopor depuração de metabolitos cardiotóxicos setorna evidente. Perante ultrafiltrados demaiores dimensões existe um equilíbrio, nãoexistindo modificações no que respeita aosparâmetros de avaliação da função sistólica.
Sabe-se que a morfologia do fluxo Dopplerespectral pulsado transmitral depende dediversas variáveis como: pressão da aurículaesquerda, pré-carga, pós-carga, respiração,frequência cardíaca e alterações do relaxamentoventricular esquerdo. A diminuição da pré-cargadiminui as velocidades das ondas E e A, sendoestas inúteis para avaliar a diástole na presençade alterações de volume. Muito embora oDoppler tissular se tenha revelado promissor naidentificação de parâmetros diastólicosindependentes de carga (3,4,5), desconhece-se seeste comportamento persistirá na presença dealterações muito significativas da pré-carga.
No nosso estudo, a velocidade de enchimentoprecoce transmitral (E), a Em DTIp, a Em DTIce a Em STI, diminuiram significativamente,enquanto que a velocidade transmitraldependente da contracção auricular (A), a AmDTIp, a Am DTIc e a Am STI não semodificaram. Logicamente as razões E/A eEm/Am também diminuiram atingindosignificado estatístico, enquanto que a razãoE/Em se manteve inalterável. Com aexcepção dos resultados E/Em (nunca tinhasido estudada) os restantes foram idênticos aosobtidos em outros ensaios (27,24,7) com populaçõessemelhantes à nossa. O que o nosso estudoacrescenta é a inalterabilidade da razão E/Emavaliada por qualquer uma das metodologiasecocardiográficas em estudo: DTIp, DTIc e STI.
Muitos têm sido os trabalhos (28,29), com vista adeterminar a melhor velocidade longitudinaldiastólica precoce, se a do segmento lateral, sea do septal do anel mitral. No nosso estudonenhuma das razões E/Em DTIp se alterou.
exception of the E/Em ratio (which had not beenstudied previously), results were similar to thoseobtained in other studies on populations similarto ours (28, 24, 7). The contribution of our study is thefinding that the E/Em ratio did not change whenassessed by any of the echocardiographicmethods used - pulsed TDI, color TDI and STI.
Several works (29, 30) have set out to determinewhether the best early diastolic velocity to assessis that of the lateral or septal segment of themitral annulus. In our study, neither of the E/Emratios by pulsed TDI changed. It is thus assumedthat either can be used to assess diastolicfunction, regardless of the volume status of thepatient. The septal E/Em ratio by pulsed TDI washigher than the lateral ratio, as has been reportedpreviously (20).
Almost half of the patients studied hadechocardiographic criteria for high fillingpressures, reflecting at least grade 2 diastolicdysfunction, which is not surprising in apopulation with a high prevalence ofhypertension and left ventricular hypertrophy.
Studies in hemodialysis patients (31, 22) thatfound no differences in Em by pulsed TDIinvolved lower ultrafiltration volumes, and thesmall reduction in preload could mask itsdependence on volume status. The same may betrue of the results obtained in the study of blooddonors (27).
It should be stressed that in our study theresults for systolic and diastolic myocardiallongitudinal velocities by the three differentmethods (pulsed TDI, color TDI and STI) weresimilar. This suggests that tissue Doppler orspeckle tracking can be used in clinical practiceto assess left ventricular systolic and diastolicfunction (32).
The present study is the largest to assesssystolic and diastolic function in hemodialysispatients not only by conventional methods butalso by tissue Doppler and speckle tracking. Anycomparison between blood donors and HDpatients is bound to be only approximate, firstlybecause the former are healthy, and secondlybecause the volume loss in donors is only 500 ml,while in hemodialysis the ultrafiltration volumecan be as high as 4000 ml. Our results shouldalso not be compared to those in studies in whichpreload is reduced by vasodilators such asnitroglycerin, since these drugs are associatedwith increased circulating and myocardial levels1022
Rev Port CardiolVol. 27 Setembro 08 / September 08

Assume-se assim que possam ser utilizadasindiferentemente para avaliação da funçãodiastólica, independentemente do estadovolémico do doente. A razão E/Em DTIpseptal foi superior à lateral, tal como já tinhasido descrito anteriormente (20).
Quase metade dos doentes estudados tinhamcritérios ecocardiográficos de elevação daspressões de enchimento, correspondendo a umestadio de disfunção diastólica de pelo menosgrau 2, o que não é surpreendente neste tipode população com elevada prevalência dehipertensão arterial e hipertrofia ventricularesquerda.
Os estudos (30,22) em doentes hemodialisadosem que não se obtiveram diferenças para o EmDTIp envolveram ultrafiltrados menores, podendoa pequena diminuição de pré-carga mascarar asua dependência do estado volémico. A mesmajustificação pode ser adiantada para os resultadosobtidos no estudo de dadores de sangue (23).
É importante apontar, que no nosso trabalhoa determinação das velocidades longitudinaismiocárdicas, sistólicas e diastólicas, pelasdiferentes metodologias (DTIp, DTIc e STI) foramsobreponíveis. Tal facto permite antever autilização clínica de Doppler tissular ou speckletracking, no estudo da função sistólica ediastólica ventricular esquerda (31).
O presente trabalho é pois o maior estudode avaliação da função sisto-diastólica, utili-zando metodologia convencional, mas tambémDoppler tissular e speckle tracking, em doentesem hemodiálise. A comparação será sempregrosseira entre os dadores de sangue e oshemodialisados, primeiro porque estes sãosaudáveis, segundo porque a volémia perdida éde apenas 500 ml, enquanto que na hemodiáliseo ultrafiltrado chega a atingir os 4000 ml.Também não é lícito comparar os nossosresultados com os encontrados nos ensaios emque se obtém diminuição da pré-carga através defármacos como a nitroglicerina. É conhecido, queestes vasodilatadores cursam com aumento dosníveis circulantes e transmiocárdicos deepinefrina, alterando os índices de contrac-tilidade e da pós-carga nos doentes seminsuficiência cardíaca (32).
of norepinephrine, which alters indices ofcontractility and afterload in patients withoutheart failure (33).
LIMITATIONS
Although there is no other way to reducevolume load so significantly, an obviouslimitation of the present study is that our resultscannot be extrapolated to healthy populations.Moreover, besides the small sample size,another limitation is the lack of invasivemonitoring of right chambers and pulmonarycapillary wedge pressures in order to validate ourechocardiographic results. Lastly, it should benoted that the echocardiographers were aware ofthe pre- or post-dialysis status of the patientsduring image acquisition and no evaluation wasmade of inter- and intra-observer variation in theoffline analysis.
CONCLUSION
In our study, large acute changes in volumeload were associated with significant variationsin early diastolic myocardial longitudinalvelocities. By contrast, E/Em ratios were load-independent, as were systolic function param-eters, enabling these indices to be used toevaluate left ventricular systolic and diastolicfunction independently of the volume load statusof renal failure patients.
The results for systolic and diastolicparameters assessed by new echocardiographictechniques (pulsed TDI, color TDI and STI) weresimilar, and any of them can thus be used toassess systolic and diastolic function in patientswith end-stage renal disease.
1023
LÍGIA MENDES, et alRev Port Cardiol 2008; 27: 1011-25

LIMITAÇÕES
Embora não houvesse outra forma desubmeter indivíduos a tão significativa alteraçãode carga, o nosso estudo apresenta as óbviaslimitações da impossibilidade de extrapolar osnossos resultados para uma população saudável.Além do tamanho da amostra, outra limitaçãoé a ausência de monitorização invasiva dascavidades direitas e pressões de encravamentocapilar pulmonar com o objectivo de validar osnossos resultados ecocardiográficos. Finalmenteimporta referir que durante a aquisição dasimagens havia conhecimento do status pré ou pósdialitico dos doentes e não foi avaliada avariabilidade inter e intra-observador da análiseoffline.
CONCLUSÃO
No nosso estudo grandes variações de volémiaassociaram-se a alterações significativas dasvelocidades longitudinais diastólicas precoces.Pelo contrário a razão E/Em e os parâmetros deavaliação sistólica revelaram-se independentes
de carga. Permitindo-nos utilizar estes índicespara aferir a função sisto-diastólica do ventrículoesquerdo independentemente do estado volémicono doente insuficiente renal.
Acresce que os resultados dos parâmetrosde avaliação sisto-diastólica obtidos atravésdas recentes e metodologias ecocardiográficas(TDIp, TDIc e STI) foram semelhantes, sendopossível utilizá-los indiferentemente na ava-liação da função sisto-diastólica no doentecom insuficiência renal terminal.
Pedidos de separatas para:
Address for reprints:
LÍGIA LOPES MENDES
Serviço de Cardiologia
Hospital de São Bernardo
Rua Camilo Castelo Branco
2910-146 SETÚBAL
Tel/Fax: +351.265.549.082
e-mail: [email protected]
1024
Rev Port CardiolVol. 27 Setembro 08 / September 08
1. Pinto FJ. Echocardiography in left ventricular dysfunction.Ital Heart J 2004; 5: 1745-54.
2. Paulus JW at al. How to diagnose diastolic heart failure: aconsensus statement on the diagnosis of heart failure withnormal left ventricular ejection fraction by the Heart Failureand Echocardiography Associations of the European Society ofCardiology. Eur Heart J 2007; 28: 2539-2550.
3. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA,Quiñones MA. Doppler tissue imaging: a non-invasive techniquefor evaluation of left ventricular relaxation and estimation offilling pressures. J Am Coll Cardiol 1997; 15: 1527-33.
4. Yu CM, Sanderson JE, Marwick TH, Oh JK. Tissue Dopplerimaging: a new prognosticator for cardiovascular diseases. J AmColl Cardiol 2007 May 15;49(19):1903-14.
5. Ho CY, Solomon SD. A Clinician’s Guide to Tissue DopplerImaging. Circulation 2006;113;e396-e398
6. Amà R, Segers P, Roosens C, Claessens T, Verdonck P,Poelaert J. The effects of load on systolic mitral annularvelocity by tissue Doppler imaging. Anesth Analg 2004 Aug;99(2):332-8.
7. Hung KC, Huang HL, Chu CM, Chen CC, Hsieh IC, ChangST, Fang JT, Wen MS. Evaluating preload dependence of a
novel Doppler application in assessment of left ventriculardiastolic function during hemodialysis. Am J Kidney Dis 2004Jun;43(6):1040-6.
8. Andersen NH, Terkelsen CJ, Sloth E, Poulsen SH. Influenceof preload alterations on parameters of systolic left ventricularlong-axis function: a Doppler tissue study. J Am SocEchocardiogr 2004 Sep;17(9):941-7.
9. Pelà G, Regolisti G, Coghi P, Cabassi A, Basile A, CavatortaA, Manca C, Borghetti A. Effects of the reduction of preload onleft and right ventricular myocardial velocities analyzed byDoppler tissue echocardiography in healthy subjects. Eur JEchocardiogr 2004 Aug;5(4):262-71.
10. Yalçin F, Kaftan A, Muderrisoglu H, Korkmaz ME,Flachkampf F, Garcia M, et al. Is Doppler tissue velocity duringearly ventricular filling preload independent? Heart 2002; 87:336-9.
11. Perk G, Tunick PA, Kronzon I. Non-Doppler two-dimensional strain imaging by echocardiography-from technicalconsiderations to clinical applications. J Am Soc Echocardiogr2007 Mar;20(3):234-43.
12. Marwick TH. Measurement of strain and strain rate byechocardiography: ready for prime time? J Am Coll Cardiol2006 Apr 4;47(7):1313-27.
BIBLIOGRAFIA / REFERENCES
13. Pislaru C, Pellikka PA. Tissue Doppler and strain-rateimaging in cardiac ultrasound imaging: valuable tools orexpensive ornaments? Expert Rev Cardiovasc Ther 2005Jan;3(1):1-4.
14. Sutherland GR, Di Salvo G, Claus P, D’hooge J, Bijnens B.Strain and strain rate imaging: a new clinical approach toquantifying regional myocardial function. J Am SocEchocardiogr 2004 Jul;17(7):788-802.
15. D’hooge J, Heimdal A, Jamal F, KuKulski T, Bijnens B,Rademakers F, Hatle L, Suetens P, Sutherland GR. Regionalstrain and strain rate measurements by cardiac ultrasound:principles, implementation and limitations. Eur J Echocardiog2000; 1: 154-170.
16. Teske AJ et al. Echocardiographic quantification ofmyocardial function using tissue deformation, a guide to imageacquisition and analysis using tissue Doppler and speckletracking. Card Ultrasound 2007; 5:27.
17. Agmon Y, Oh JK, McCarthy JT, Khandheria BK, BaileyKR, Seward JB. Effect of volume reduction on mitral annulardiastolic velocities in hemodialysis patients. Am J Cardiol. 2000Mar 1;85(5):665-8, A11.
18. Lang RM et al. Recommendations for ChamberQuantification: A Report from the American Society ofEchocardiography’s Guidelines and Standards Committee andthe Chamber Quantification Writing Group, Developed inConjunction with the European Association ofEchocardiography, a Branch of the European Society ofCardiology. J Am Soc Echocardiogr 2005;18:1440-1463.
19. Nishimura RA, Abel MD, Hatle LK, Tajik AJ. Assessment ofthe heart, background and current applications of Dopplerechocardiography (Part II: Clinical studies). Mayo Clin Proc1989:990-1003
20. Oh JK. Echocardiography in heart failure: beyonddiagnosis. Eur J Echocardiogr 2007 Jan; 8(1):4-14.
21. Gilman G, Khanderia BK, Hagen ME, Abraham TP, SewardJB, Belohlavek M. Strain rate and strain: a step-by-stepapproach to image and data acquisition. J Am Soc Echocardiogr1004;17: 1011-20.
22. Zipes DP, Libby P, Bonow RO, Braunwald E. Braunwald’sheart disease. Elsevier Saunders 2005: 7th ed: 476
23. Stoylen A. Strain Rate imaging. http://ntu.no/stoylen/strainrate 2006
24. Bauer F, Jamal F, Douillet R, Le Roi F, Bouchoule I, Bizet-Nafeh C, Godin M, Cribier A, Derumeaux G. Acute changes inload: effects of myocardial velocities measured by Doppler tissueimaging. Arch Mal Coeur Vaiss 2001 Nov; 94 (11): 1155-60.
25. Barberato SH, Filho RP. Influence of preload reduction onTei index and other Doppler echocardiographic parameters ofleft ventricular function. Arq Bras Cardio 2006 Jun; 86 (6):425-31
26. Abali G, Tokgozoglu L, Ozcebe OI, Aytemir K, Nazli N.Which Doppler parameters are load independent? A study innormal volunteers after blood donation. J Am Soc Echocardiogr2005; 18:1260-1265.
27. Oguzhan A, Arinç H, Abaci A, Topsakal R, Kemal E,Ozdogru I, Basar E, Ergin A. Preload dependence of Dopplertissue imaging derived indexes of left ventricular diastolicfunction. Echocardiogr 2005 Apr; 22(4):320-5.
28. Srivastava P, Burrell L, Calafiori P. Lateral vs medialannular tissue Doppler in the echocardiographic assessment ofdiastolic function and filling pressures: which should we use?Eur J Echocardiogr 2005; 6:97-106.
29. Khouri SJ, Maly GT, Suh DD, Walsh TE. A practicalapproach to the echocardiographic evaluation of diastolicfunction. J Am Soc Echocardiogr 2004;17:290-7.
30. Fijalkowski M, Koprowski A, Gruchala M, Galaska R,Debska-Slizien A, Rogowski J, Rutkowski B, Rynkiewicz A.Effect of preload reduction by hemodialysis on myocardialultrasonic characterization, left atrial volume, and Dopplertissue imaging in patients with end-stage renal disease. J Am SocEchocardiogr 2006; 19: 1359-1364.
31. Stefani L, Toncelli L, Gianassi M, Manetti P, Di Tante V,Vono MRC, Moretti A, Cappelli B, Pedrizzetti G, Galanti G.Two-dimensional tracking and TDI are consistent methods forevaluating myocardial longitudinal peak strain in left and rightventricle basal segments in athletes. Cardiovascular Ultrasound2007, 5:7.
32. Ros M, Azevedo ER, Newton GE, Parker JD, Effects ofnitroprusside on cardiac norepinephrine spillover andisovolumic left ventricular relaxation in the normal and thefailing human left ventricle. Can J Cardiol 2002;18:1211-6.
1025
LÍGIA MENDES, et alRev Port Cardiol 2008; 27: 1011-25
Related Documents











