Monica Ramakrishnan, Surya Rajasekaran, Barsa Nayak, Akshay Bhagdikar SANTA CLARA UNIVERSITY AUTOMATED LUNG CANCER NODULE DETECTION

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MonicaRamakrishnan,SuryaRajasekaran,BarsaNayak,AkshayBhagdikar
SANTACLARAUNIVERSITY
AUTOMATEDLUNGCANCERNODULEDETECTION
2|P a g e
1 PRE-INTRODUCTION1.1 PREFAFACEThe purpose of this project is to develop a model that utilizes various concepts from imageprocessing, datamining, andmachine learning to detect lung cancer nodules amongst high riskpatients.Variousconceptsof imageprocessingwerealsoutilized.This reporthasbeenmade infulfillmentoftherequirementforthesubject:PatternRecognition&DataMininginJune2017underthesupervisionofDr.Ming-HwaWang1.2 ACKNOWLEDGEMENTSWewouldliketoexpressourheartfeltgratitudetoDr.Ming-HwaWangforprovidinguswithanopportunity to explore our interests in data mining as well as image processing. Without histremendous support, encouragement as well as valuable inputs, this project couldn't havematerialized.Theguidanceandsupportreceivedfromallthememberswhocontributedandwhoarecontributingtothisprojectwasvitalforoursuccess.
3|P a g e
1.3 TABLEOFCONTENTS
1 PRE-INTRODUCTION.......................................................................................................................21.1 PREFAFACE...........................................................................................................................................21.2 ACKNOWLEDGEMENTS........................................................................................................................21.3 TABLEOFCONTENTS............................................................................................................................31.4 LISTOFTABLES&FIGURES...................................................................................................................41.5 ABSTRACT:............................................................................................................................................5
2 INTRODUCTION..............................................................................................................................62.1 OBJECTIVE:...........................................................................................................................................62.2 WHATISTHEPROBLEM:......................................................................................................................62.3 PROJECTRELATIONTOCLASS:.............................................................................................................62.4 WHYOTHERSOLUTIONSAREINADEQUATE:.......................................................................................72.5 WHYOURAPPROACHISBETTER:.........................................................................................................72.6 STATEMENTOFPROBLEM....................................................................................................................82.7 SCOPEOFINVESTIGATION...................................................................................................................8
3 THEORETICALBASESANDLITERATUREREVIEW..........................................................................93.1 DEFINITIONOFTHEPROBLEM:............................................................................................................93.2 THEORETICALBACKGROUNDOFTHEPROBLEM:.................................................................................93.3 RELATEDRESEARCHTOSOLVETHEPROBLEM:....................................................................................93.4 ADVANTAGE/DISADVANTAGEOFTHOSERESEARCH.........................................................................103.5 SOLUTIONTOPROBLEM....................................................................................................................103.6 WHERESOLUTIONISDIFFERENTFROMOTHERS...............................................................................103.7 WHYSOLUTIONISANIMPROVEMENTONCURRENTMETHODS.......................................................113.8 TERMINOLOGY...................................................................................................................................11
4 HYPOTHESIS..................................................................................................................................124.1 MULTIPLEHYPOTHESIS......................................................................................................................124.2 POSITIVE/NEGATIVEHYPOTHESIS:.....................................................................................................12
5 METHODOLOGY............................................................................................................................135.1 HOWTOGENERATE/COLLECTINPUTDATA:......................................................................................135.2 HOWTOSOLVETHEPROBLEM:.........................................................................................................135.3 ALGORITHMDESIGN:.........................................................................................................................145.4 LANGUAGESANDTOOLSUSED:.........................................................................................................205.5 HOWTOGENERATEOUTPUT:............................................................................................................215.6 HOWTOTESTAGAINSTHYPOTHESIS:................................................................................................21
6 IMPLEMENTATION:......................................................................................................................226.1 CODE..................................................................................................................................................226.2 DESIGNDOCUMENT:..........................................................................................................................276.3 DESIGNDOCUMENTANDFLOWCHART.............................................................................................30
7 DATAANALYSISANDDISCUSSION..............................................................................................317.1 OUTPUTGENERATION:......................................................................................................................317.2 OUTPUTANALYSIS:.............................................................................................................................31
4|P a g e
7.3 COMPAREOUTPUTAGAINSTHYPOTHESIS........................................................................................337.4 ABNORMALCASEEXPLANATION........................................................................................................337.5 DISCUSSION:.......................................................................................................................................33
8 CONCLUSIONANDRECOMMENDATIONS.....................................................................................348.1 SUMMARYANDCONCLUSIONS:........................................................................................................348.2 RECOMMENDATIONSFORFUTURESTUDIES:....................................................................................348.3 BIBLIOGRAPHY....................................................................................................................................358.4 PROGRAMFLOWCHART.....................................................................................................................378.5 PROGRAMSOURCECODEWITHDOCUMENTATION..........................................................................378.6 INPUT/OUTPUTLISTING.....................................................................................................................37
1.4 LISTOFTABLES&FIGURES FIGURE1:SAMPLESLICESOFDICOMIMAGE..............................................................................................14
FIGURE2:HOUNDSFIELDUNITSFORVARIOUSSUBSTANCES............................................................................15
FIGURE3:CTSCANSLICECOLORED...........................................................................................................15
FIGURE4:AFTERTHRESHOLDING...............................................................................................................16
FIGURE5:AFTEREROSIONANDDILATION....................................................................................................16
FIGURE6:VGG16ARCHITECTURE............................................................................................................18
FIGURE7:MLPPROCESS........................................................................................................................19
FIGURE8:SAMPLEEPOCHOUTPUT...........................................................................................................32

5|P a g e
1.5 ABSTRACT:Lungcancerisadiseaseofuncontrolledcellgrowthintissuesofthelung.Sincelungcancerisoneoftheleadingcausesofdeath,earlydetectionofmalignanttumorsisimperativeforasuccessfulrecovery.Ingeneral,earlystagelungcancerdiagnosistechniquesmainlyutilizeX-raychestfilms,CT,MRI,etc.Computedtomography(CT)producesaseriesofcross-sectionalimagescoveringapartofthehumanbody.Forourcasespecifically,wewillfocusonthethoracicregion.Visuallyidentifyingandexaminingtheseimagesforpotentialabnormalitiesisachallengingandtimeconsumingtaskduetothelargeamountofinformationthatneedstobeprocessed,andtheshortamountoftimegiven.Thesubjectofmedicalimageminingiscurrentlyanupandcomingtopicandshowsalotofresearchpotentialintheareaofcomputationalintelligence.Byauto-analyzingapatient’srecordsand images throughdataminingand imageprocessing techniques,wewould reduce the riskofhumanerrorinnoduledetection.Byapplyingacombinationoftechniquesindatapreprocessing,featureextraction,andclassification,weultimately seek to increase theaccuracy rateofcancerdetection, while simultaneously reducing the false positive diagnosis rate. In this project, weproposetouseadeepartificialneuralnetworkarchitecture,whichisacombinationofCNNalongwithRNNforthefully-automateddetectionofpulmonarynodulesinCTscans.ThearchitectureoftheVGG16convolutionalneuralnetworkistrainedtodistinguishpixelsacrossimages,andcanbeutilizedinourcasetoextractnoduleinformation.Ourprojectwilldemonstratethatbyleveragingthesetechniques,wesubstantially increasethesensitivitytodetectpulmonarynodules,withoutinflatingthefalsepositiverate.Thus,fromtheavailableLIDC/IDRIdatasetconsistingofaround1500CTscans,wehaveprovidedaninnovativeapproachofimplementingCNNusingthepretrainedVGGmodel for feature extraction and RNN for feature classification for identification of pulmonarynodulesinlungcancerdetection.
6|P a g e
2 INTRODUCTION2.1 OBJECTIVE:Theobjectiveofthisprojectistoimprovethecurrentcancerdetectionratebyreducingthefalsepositives while maintaining a low false negative rate. The false positive detection of cancer isdangerous,asanerroneousdiagnosisutilizespreciousresources,causesunnecessaryapprehensionforthepatient,andfinally,posesavarietyoflegalthreatstothedoctors.Thus,topreventthis,ourobjectiveistodevelopanalgorithmthatefficientlyreducesthefalsepositiverate,whilemaintainingtheoverallcancerdetectionaccuracy.2.2 WHATISTHEPROBLEM:Lungcarcinoma,alsoknownaslungcancer,ischaracterizedbymalignanttumorsfromwhengenechanges intheDNAofthecellsmutateandpromoteunnaturalgrowth.Lungcancer is themostcommontypeofcancerwithapproximately225Knewcasesin2016alone,whichledto$12billioninannualhealthcarecosts.Themostcommonageatdiagnosisis70years.Overall,thelungcancersurvival rate in theUnitedStates isextremely low–only17.4%ofpatientsdiagnosedwith lungcancersurvivefiveyearspostdiagnosis.Further,uncontrolledcellgrowthcanspreadtosurroundingareasormetastasizetootherorgans if itnotdetectedearly.DoctorscurrentlyuseLow-DoseCTscanstohelpassessifapersonisatriskoflungcancer,orevenotherpulmonarydiseases.Using a data set of thousands of high-resolution lung scans provided by the National CancerInstitute,wewilldevelopamodelthataccuratelydetermineswhetherlesionsinthelungsofhighriskpatientsarecancerous.Currentmodelshaveextremelyhighfalsepositiverates,whichdoesnotallowoncologistsandradiologiststofocusonpatientsthathaveanimminentcancerthreat.Further,thehighfalsepositiveratesleadtounnecessarypatientanxiety,additionalfollowupimaging,andinterventionaltreatments.Thus,bybuildingaclassificationmodelthatreducesthenumberofbothfalsepositivesandfalsenegatives,patientscanhaveearlieraccesstolife-savinginterventions,aswellasgivedoctorsanopportunitytoprioritizepatientcare.2.3 PROJECTRELATIONTOCLASS:Theapproachwewilltaketomodelanaccuratepredictionsystemoflungcancerwillutilizemultipletechniques indataminingandpatternrecognition.Classificationproblemsarerooted in featureprocessing,clusteringfeatureextraction,featureengineering,andmachinelearningmodels.First,byminingalargedatasetofCTscans,weutilizetechniquesindataminingandimageprocessingthatarecrucialforaccuratefeatureextraction.Wealsoplantoutilizebothunsupervised(clustering)andsupervised(classification)modelsinordertoextractcharacteristicsofpatients’lungsandfinallyclassifypatientsascancerousornotcancerous.Byusingthesevarioustechniques,wearecombiningwidelyusedtechniquesindataminingandpatternrecognition.

7|P a g e
2.4 WHYOTHERSOLUTIONSAREINADEQUATE:MostofthestandardmechanismsforclassificationgoforeitherPCAorSVMorRandomForestandXboostClassifiertoclassifythedata.Otherclassifiersfailiftheyhaven'ttakenthebelowscenariosintoaccount:
1. Detecting the location of Pulmonary Nodule(s): The current approaches for detectingpulmonarynodulesgenerallyincludemanualintervention.Whenthelocationofthenodulesisnotprovidedinthedataset,itbecomesanextremelytedioustasktomanuallyparsetheimages to findpotentiallymalignantnodules. Thisproves itself evenmoredifficult if theimagesarerotatedortwisted,leadingtofurthererroneousprocessing.
2. FeatureExtraction:Thegenerationofasmallnumberoffeaturesleadstoalossofdata.Oncethenodulepositionisdetermined,thenoduleisthenextractedfromtheentireimage.Then,the features such as total area, average area, maximum area and average eccentricity,averageequivalentdiameter,standardequivalentdiameter,weightedX,weightedY,numberofnodes,andnumberofnodesperslicewerecalculated.Withthisapproach,thereisalotofinformationlost.
2.5 WHYOURAPPROACHISBETTER:Ourproposedapproachhasthefollowingtwosteps:
1. FeatureExtractionPhase:Unlikemanualintervention,wemakeuseoftheimageprocessingtechniquestofirsthighlightthelungregionandthenapplyourstateoftheartpretrainedConvolutionalNeuralNetworkmodelforfeatureextractionfromtheimages.Thisreducesthehumaneffortofthenodulepositiondetection,andsinceourmodelisnotrestrictedtothepositionofthenodule,itdoesnotgetaffectediftheimageisrotatedortwisted.
2. ClassificationPhase:RecurrentNeuralNetworkswithmultilevelperceptronwillbeusedtoclassifytheCTscans.Althoughrandomforestclassificationmodelstypicallyrequiremoredataforasimilaraccuracy,theytypicallygeneratearobustmodel.Thus,wewilluserandomforesttosetabaselineaccuracyforouranalysis.Ontheotherhand,deeplearningismorefavorableascomplexproblemssuchasimageclassificationcanbehandledbetter,andthisisthebaseofpulmonarynoduledetection.
tThebenefitsofusingdeeplearning(RecurrentNeuralNetworks)are:
1. Automaticfeatureextractionwithouthavingtoextractthenodulepositioninformationandotherfeatures.
2. Incaseofdatasetswhicharecomplex3Dimages,deeplearninggivesbetterclassificationresultsascomparedtoothermethods.
3. Treebasedmodels(theonethatXGBoostisgoodat)solvetabulardataverywellbutadeepnetworkcancapturethingslikeimage,audioandpossiblytextquitewellbymodelingthespatialtemporallocality.
4. Neuralnetworkbaseddeeplearningisanaccuracy-focusedmethodwhereasXgboostisaninterpretation-focusedmethod.

8|P a g e
2.6 STATEMENTOFPROBLEMAlthoughCTscansareestablishedmeansfordetectingpulmonarynodules,thesmalllesionsinthelungstillremaindifficulttoidentify–especiallywhenusingasingledetectorCTscan.Thisposesitselfasachallengewhenattemptingearlydetectionoflungcancer.Sinceearlydetectionisthekeyfor a successful remission and recovery, the inability tomanually see the small lesions furtherhindersthepossibilityofearlydetection.CurrentCTscannersproduceupto300cross-sectional2Dimages,eachofwhichmustbeindividuallyevaluatedunderatimeconstraint.DespitethediagnosticbenefitsprovidedbytheCTimaging,theincreasedmanualworkloadthatisrequiredtoread200-300slicesperexamleadstotheincreasingerrorrateofcancerdetection.Giventhatnodulescanappear in different positions, and depending on the patient, the process to detect lung cancerbecomes extremely labor-intensive and manual. This manual process further increases theprobabilityofhumanerror–eitherthedoctordetectscancerinapatientwhoiscancerfree,orthedoctor fails todetect themalignantnodule.Currentstudieshavedemonstrated that therateoferroneousCTinterpretationandanalysisrangesfrom7%-15%whenaradiologistperformsmorethan20CTexaminationsperday(Bechtold,1997).Inordertoaddresstheseissues,therehasbeenasuddenincreaseofresearchanddevelopmentofCAD(computer-aided-diagnosis)systemsforhighaccuracypulmonarynoduledetection.UsingtheCTscans,theadoptionoftheCADsystemsledtoan improvement on the sensitivity of current detection algorithms – present day systems aresuccessfully able to detect nodules with a 3mm diameter. Thus, several approaches are beingproposed to overcome the challenges to detect the pulmonary nodules and thusmaximize thechancesofthesurvivalofthepatients.2.7 SCOPEOFINVESTIGATION Forthepurposesofthisproject,wewillspecificallyfocusonlesionsinthelungsofhighriskpatients.The general approach can potentially be applied to different organs and in patients of variousdemographics,butforthisinvestigation,wewilllimitthescopeofourinvestigation.
9|P a g e
3 THEORETICALBASESANDLITERATUREREVIEW3.1 DEFINITIONOFTHEPROBLEM:Since lungcancer isoneofthe leadingcausesofdeath intheUnitedStatesandgiventhatearlydetection increases the probability of a successful remission, our problem statement revolvesaroundcreatinganautomated,highaccuracymodelfornoduledetection.Currentmethodologiesplace a heavy focus on reducing false negative rates, but at the expense of significantly overpredicting the cancerous class. Further, our research has suggested that current approaches tonoduledetectionallrequiresomelevelofmanualimageprocessing.Thatis,theimagesareparsedbyhandforthecoordinatesofthenodule.Thus,thesolutionwillfocuson1)automatingnoduledetection,and2)reducingthefalsepositiverateofcancerdetectionwhilemaintainingagoodfalsenegativerate.Theavailabilityof largedatagivenbytheNationalCancerAssociationprovidesanopportunityforfurtherresearchindatamining.Theimportantprobleminthisareaistomakeanefficientdetectionalgorithmtoaidwithearlydetection.3.2 THEORETICALBACKGROUNDOFTHEPROBLEM: With the advancement of Technology and Computer Aided Diagnosis (CAD), scientists haveencouraged a lot of automated systems to address the issue of reducing false positive whileestimatingthepresenceofpulmonarynodulesintheCTscansofthepatients.Thus,todaywehaveasurplusofdatapertainingtotheCTscanpatients.Fromhere,wehavetheopportunitytousecurrenttopicsinimageprocessing,datamining,andmachinelearningtoidentifyhiddenpatternsin nodule size, location, structure, etc. and construct a model to increase the probability ofmalignanttumordetection.Withtheadventof thepatternrecognitionandmachine learning,datascientistshaveproposedmanyapproacheswhichwererobustinfindingthehiddenpatternsandreducingthefalsepositives.Withthis,asthedataforthepatientsdetectedwithlungcancerincreased,theCTscanstendtodiffermoresignificantlyfromeachother,acrosspatients.Consequently,thedeeplearninghascomeintopictureforthecompleximageclassificationinordertoensurethatoutliersandanomaliesareproperlyhandledinthemodelandthus,reducingthefalsepositiverateformalignantpulmonarynoduledetection.3.3 RELATEDRESEARCHTOSOLVETHEPROBLEM: Therehasbeenalotofresearchinrecenttimesonthedevelopmentofcomputer-aideddiagnosis(CAD)systemsforpulmonarynoduledetectionusingCTimaging.Advancementsinimageprocessingfield has increased the accuracy in the prediction of cancer fromCT scans. There are plenty ofresearchpaperswhichdiscussthevariousmethodsandoutputs.Afewexamplesinclude:‘RecurrentConvolutionalNetworksforPulmonaryNoduleDetectioninCTImaging’, ‘Combiningdeepneuralnetwork and traditional image features to improve survival prediction accuracy for lung cancerpatientsfromdiagnosticCT’,‘ComputerizedDetectionofLungTumorsinPET/CTImages’,and‘LungcancerclassificationusingneuralnetworksforCTimages’.

10|P a g e
3.4 ADVANTAGE/DISADVANTAGEOFTHOSERESEARCHAdvantages The current research is extremely helpful to many students who would like to implement thefindingsintotheirprojectsandaswellastodofurtherresearch.Theadvantageoftheseresearchfindingsisthatitalsohelpsinimprovingthedetectionofcanceratanearlystageandtoreducethedetectionerror.Disadvantages Thedisadvantagesarethatusuallythedatatrainingsetisveryhugewhichincreasesthetimetakentotrain.Inordertoobtainabeyond-averageaccuracy,wearerequirdtouseanextremelylargedatasetinordertotrainthemodel.Althoughitistimeconsumingforthecodetotrainthenetwork,itisaone-timeprocessthatcanberedoneiftherearenewtypesofcancersthatneedtobetrained.3.5 SOLUTIONTOPROBLEM Inorder todetectcancerous tissue in the lungswitha relativelyhighaccuracy,oursolutionwillincludethefollowingsteps:
1. ImageProcessing2. FeatureExtraction&Engineering3. Clustering4. ClassificationModel
Thishybridapproachallowsustocombinethemostefficientindividualmethodologiesintoanendtoendmodel.Webelievethatthiscombinationwillextracttheadvantagesfromeachapproach,andultimatelyprovidemoreconclusiveresults.Ourgoalistobuildanautomatednoduledetectionmodelwithhighaccuracyinordertoaidthedetectionoflungcancerinpatients.3.6 WHERESOLUTIONISDIFFERENTFROMOTHERS Oursolutionwillutilizeacombinationofmachinelearningtechniquesandplaceauniquefocusonminimizingthefalsepositiverate.Whilemostmodelsplacetheprimaryfocusontotalcancerouslungspredicted,wewillplaceourfocusonreducingthefalsepositiverate,inordertomakeourresultsmorereliable.Further,mostof the techniquesbeingused for lungcancerdetectionpre-processtheCTscanmanually,whichisthemostcriticalstepforhighaccuracydetection.Currentsolutionsrequiremanualfeatureextraction,whichincreasestheprobabilityofhumanerror.Onthecontrary,ourmethodwillinputtheentireCTscanasDICOMimageintotheclassificationsystemandthus,weeliminatetheneedforamanualpreprocess.
11|P a g e
3.7 WHYSOLUTIONISANIMPROVEMENTONCURRENTMETHODS Oursolutionisaimedatreducingthenumberoffalsepositivesintheclassificationmodel.Thiscanbeachievedbyacombinationoffeatureengineering(i.e.selectingfeaturesandcharacteristicsthatarehighlycorrelatedwithlungcancer)aswellastrainingaclassificationmodelusingbootstrappingandvariousotherresamplingtechniquesgivenourunbalanceddataset.Bydoingso,ourdatasetwillevenoutthedistributionbetweentheclassesofpatients.Creatingaweightingfunctionforrareclass(cancerousscans)forcesthemodeltonotoverfittothedata,whichultimatelyresults inaminimalnumberoffalsepositives.Further,aspreviouslymentioned,foranyjobwhich isdoneinapattern,machineshaveamuchlargercapacityandincreasedefficiencyforimageprocessing.Byeliminatingtheneedforhumaninteraction, we have proposed an automated tool which will input raw CT scans, perform therequiredamountofimageprocessing,modeltraining,andfinalclassification.3.8 TERMINOLOGYThissectionhighlightsthecommonterminologyusedinlungcancerandimageprocessing.
Terminology Definition
CT ComputerizedTopologyusescomputer-processedcombinationofX-Rayimagestakenatdifferentanglestoproducethescan
PulmonaryNodule Massinthelungthatusuallyrepresentscancerouslesions
DICOM DigitalImagingandCommunicationsinMedicine
InstanceNumber IdentifiesthesequenceofimagesinaDICOM
SliceThickness ThicknessofslicedependsonthicknessofCTdetectionmachine
HoundsfieldUnits QuantitativeScaleusedtomeasuredensityofsubstancesfoundinbody
ROI RegionofInterest

12|P a g e
4 HYPOTHESIS4.1 MULTIPLEHYPOTHESISHypothesis: By using the solution outlined above, our model will reduce the number of falsepositives,whilemaintainingagoodaccuracyrate.4.2 POSITIVE/NEGATIVEHYPOTHESIS:PositiveHypothesis:WhenextractingandquantifyingfeatureforROI,thefeaturestructuredesignisirrational,hence3Dfeaturesaretakenintoaccountbyrecombiningthesliceswhileextractingthefeaturestogetmoreaccuracy.Negative:Thepulmonarynodulecanbeofanyshapeandcouldmergewiththebloodvessel,whichcouldcause issueswhendetecting thenoduleaccurately. Since theaccuracy isnot100%, thereleavesroomforerror.However,thisisstillbetterthanamanualdetectiondonebyhumans.

13|P a g e
5 METHODOLOGY5.1 HOWTOGENERATE/COLLECTINPUTDATA:OurinputdataistakenfromKaggle,whichhasthedataof1,000highriskpatients.Thedatasetisapproximately130GB–whichrequiredasignificantamountofcomputingpowertoprocess.Inthisdataset,wearegivenoverathousandlow-doseCTimagesfromhigh-riskpatientsinDICOMformat.EachDICOMimagecontainsaseriesof2Dgray-scaleimagesthatcontainmultipleaxialslicesofthechestcavity–thatis,thereareapproximately300imagesperpatient.Eachimagehasavariablenumberof2Dslices,whichcanvarybasedonthetypeofmachineusedinthescan.TheDICOMfileshaveaheaderthatcontainsthenecessaryinformationaboutthepatientid,aswellasotherscanparameterssuchastheslicethickness.Thedatasetalsoincludedacsvcontainingtheclassificationinformationascancerousornon-cancerousperpatientid.Theimagesinourdatasetvaryinquality,depending on when the scan was taken. For example, older scans were imaged with lesssophisticated equipment and thus, have a lower resolution than more recent scans. Thus tosummarizeithasthefollowinginfo–around300imageswhichrepresenttheslicesofthethoracicregionCTscaninslicesinaDICOMformat:
1. PatientID,name,dateofbirthandothermetadataofthepatientandimageinformation2. CSVfilemappingtoeachpatientidmentioningofthepersonhascancerornot
5.2 HOWTOSOLVETHEPROBLEM:Thefollowingflowcharthighlightstheprocessoverviewfordetectingnodulesinlunghypothesis.
Thestepsareoutlinedasfollows:1. DataInput:Downloaddataforaround1,500patientsfromKaggle–gives2DslicesofCTscan
imagesforeachpatient,whichareintheDICOMformat.Thereareapproximately300slicesperpatient.
2. ImageProcessing:Reconstructthe3Dstructureoflungs,removethenoisefromtheimage,andmakethedatasetofallthepatients’uniformandthus,eligibleforfeatureextraction,whichincludessorting,morphological,dilation,erosion,segmentation,maskingetc.
3. Classification:RecurrentneuralNetworkwithMLPasitscoreisusedfortheclassification.MLP,ormulti-levelperceptron,hasamemoryelement,LSTM(longshorttermmemory)associatedwith it. This furtherenhances theclassificationbyemphasizing significant featureswhilede-emphasizingasspectswhichareunimportant.
4. Validation:75%oftrainingdataisgiventotrainthemodeland25%isusedfortestingpurposes.
TheCTscansofallpatienrsarefedintothetoolinDICOMformathaving300imagesperpatients
Imagsofeachpatienttakenasslicsand3Dimagereconstructedandnoisereduction
Imageprocessingdoneontheentirescanforfeatureextraction
75%ofthedataistakenfromtrainingandtheremaining25%isusedfortesting and
validationofthemodel

14|P a g e
5.3 ALGORITHMDESIGN:Asapartofouralgorithmdesign,wewillimplementtwodifferentapproachesinordertodeterminethemodelwith thehighestpredictionaccuracy fordetecting lungcancer.Our imageprocessingstepswill remainconstant throughout theapproaches.Thedifferencewill liewithin the featureextractionandclassificationtechniques.Asourcursoryanalysis,wewilldesignarelativelysimplemethodoffeatureextractionandclassification.1. ImageProcessing:–giventhesetsofCTscans,ouralgorithmwillconstructthe3Dlungscan,and
extractonlythelungregion.Thisisespeciallyimportantthatedgedetectionisdonewithhighaccuracytominimizetheerrorrateofourmodel.Wealsoutilizesegmentationandmachinelearning techniques to pre-process the image, including auto-detecting boundaries thatsurroundthevolumeof interest.Theimagesrepresentthe2Dslicesofthepatient’sthoracicregioninDICOMformat.Thusbeforeprocessing,itisveryimportanttoreconstructtheimagein3Dformasfollows:a. ArrangetheSlices:Arrangetheslicesinthenon-decreasingorderoftheirInstanceNumber
tomakesuretheCTscancanbereconstructed.Asmentioned,theCTscanisintheformofnumerous2Dimages(slices)whichneedtoberearrangedinnumericalordertobeabletorecreatethe3Dstructure.ThisinformationliesintheInstanceNumberoftheslices,whichgivestheorderinwhichithastoappearwhengenerating3Dview.AnexampleofthreeslicesinaparticularDICOMimagecanbeseebelow:
b. CalculateSliceThickness:Oncetheimageisformed,wehavetoensurethatslicethickness
istakenintoaccount.TheslicethicknessiscalculatedbasedonthemetadatapresentintheDICOMformat.Sincetheinputdatahasbeentakenfrommanysources,itsthicknessvariesfordifferentscanners.Thus,wehavetwoformatsofmetadatatocalculatethicknesswhereonecanconsidereithertheImagePositionPatientattributeorSliceLocationattributeoftheDICOMformatbasedonwhichisavailable.
c. ConverttheImageintoHU:TheimageisthenconvertedtoHU(Hounsfieldunits)toisolate
the lungregion.Sincewehavean imageof theentirethoracicregion, it is importanttodistinguishlungregionfromnon-lungregion.Thefirststepoftheconversionissettingthesevaluesto0,whichcorrespondstotheHUunitofair.Then,theHUunitsofeachregionis
Figure 1: Sample slices of DICOM image

15|P a g e
obtainedbymultiplyingtherescaleslopeandaddingtheintercept(whichareconvenientlystoredinthemetadataofthescans).Forreference,thetablebelowcontainstheaveragerangeHUspersubstance:
Substance HUAir -1000Lung -500Fat -100to-50Blood +30to+45Water 0Muscle +10to+40
Figure 2: Houndsfield Units for Various Substances
WhenaddingacoloredfiltertoaparticularsliceoftheDICOMimages,wearebetterabletovisualizetheandoutlinevarioussubstancesinthelung:
Figure 3: CT Scan Slice Colored
d. Resampling:Then,weapplyresamplingtoobtainahomogeneousdataset.Uniformityisofprimeconcerninimageprocessing,sowedonotbiasanysetofimages.Acommonmethodofdealingwithproblemistoresamplethefulldatasettoaparticularisotropicresolution.Thus,wegoforaresamplingtechniquetoensurethatthespacingoftheimagesisuniformfortheentireinputdataset.
e. Interpolation:Theprocessofzoominterpolationusingsplinemethodologyisdoneto
smooththeimageandreducevisualdistortion.
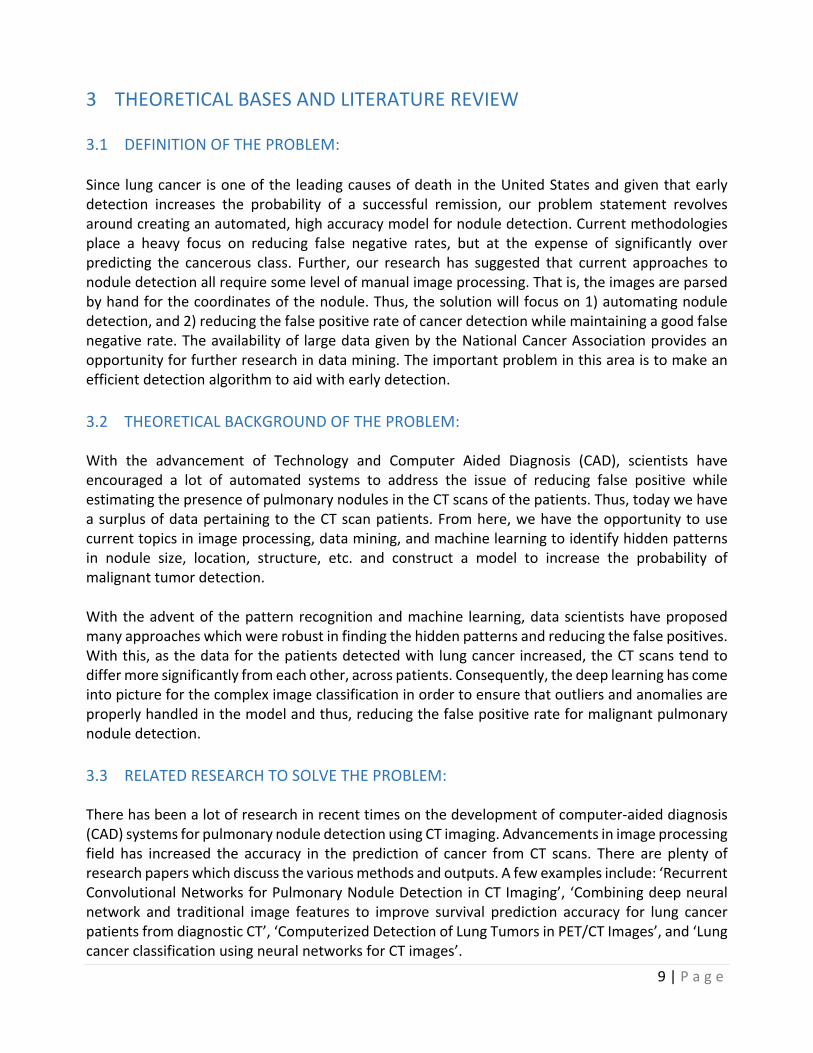
f. Thresholding–Whilethereexistvariouskindsofthresholdingtechniques,forthepurposesofourproject,wewillutilizeaclusteringbasemethod,wherethegray-levelsamplesareclusteredintwopartsasbackgroundandforeground(object).Thus,weapplythek-meansalgorithminordertoseparatethelungregionfromthebackground.Anexampleofaslicepostthresholdingcanbefoundbelow.Notethatwehavesuccessfullyisolatedthelungregion,butcanstillvisiblyseethenoiseintheimage.
16|P a g e
Figure 4: After thresholding
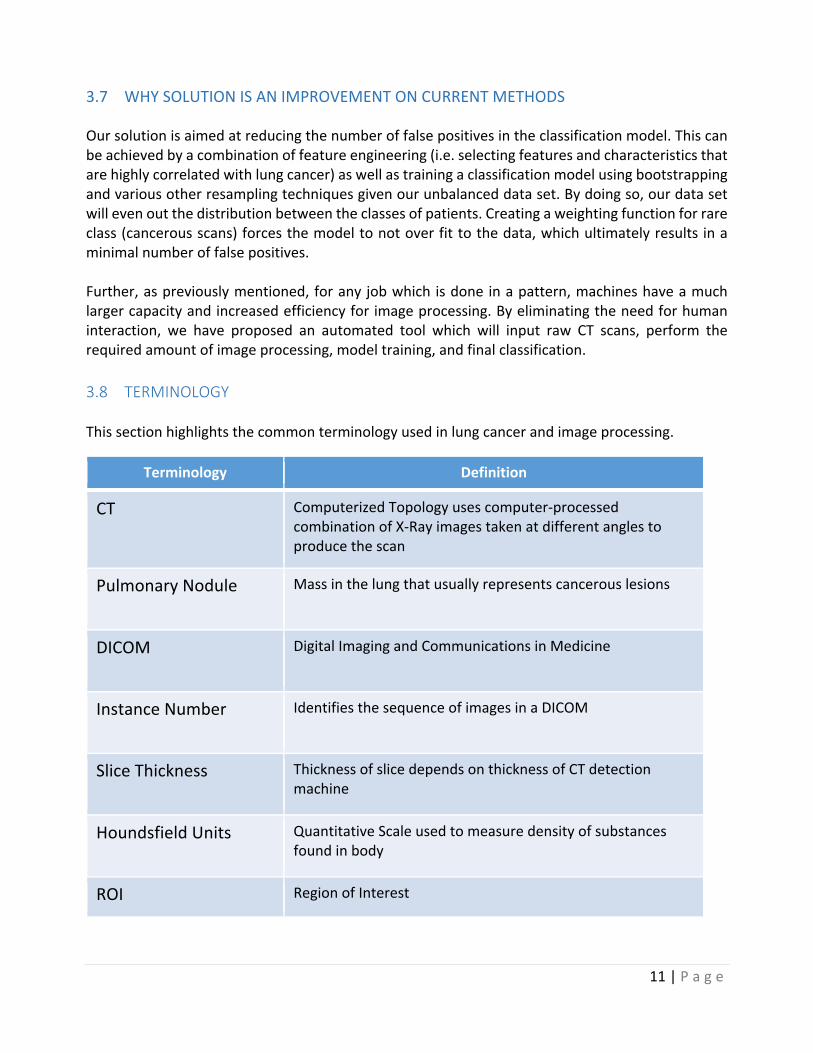
g. ErosionandDilation–Wethenapplyerosion–atechniqueforshrinkingtheimageinorder
to ensure the unwantednoise introduces further diminishes. Then,whenwedilate theimage,weregaintheoriginalsizeofthe image,keepingtheactualsizeof lungsandthenodules intact. These twoprocessesoverall reduce thenoise in the image.ExamplesofnoiseinCTscansincludeveins,capillaries,etc.
Figure 5: After erosion and dilation
h. Segmentation-MaskingoftheimageisdonebyhighlightingROI(RegionofInterest).After
gettingridofnoiseandreducingfalsepositives,theimageissegmented.Thus,amaskismade by outlining the edges of the lung (distinguishing the lung from the muscularsurroundings)aswellasthenodulescontainedwithintheorgan.WethenapplythemasktoisolatetheROI.
17|P a g e
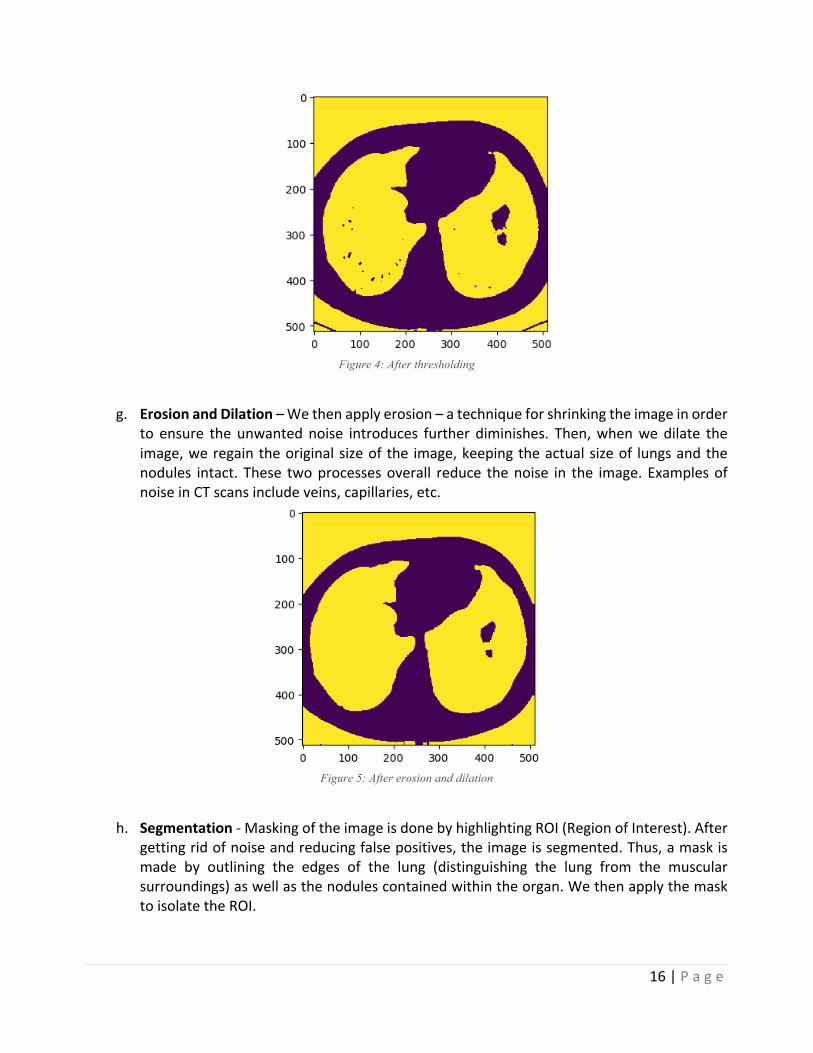
Thebelowimagedemonstratesanoverviewoftheentireprocessdescribedabove:
2. FeatureExtraction&Engineering–Usingthe3Dscanofthelungsallowsustoretainasmuchof
theinformationaspossible.Asexplained,wethenconverttheCTscans(inHounsfieldUnits)topixel,allowingustoinputapixelarrayintoourclassifieraswellasthefeaturesthatweextract.Here,wewillhaveutilizedatwotieredapproach.Thefirstapproachwillfocusonasimplisticmethodoffeatureextraction,thenfollowedbyoursecondapproachwhichwillplaceaheavyemphasisondeep learning.Bydoing so,weallow the simplisticmodel to set abaseline foraccuracy,andwearethenabletofullyunderstandtheimpactthatdeeplearninghasonourprecisionApproach1:a) Foreverypatientwedividedthesetofimagesinto4sections.Forexample,ifthepatient
has 200 images, then divide the set in a section of 50 images each. By doing this weessentiallydividethelunginto4regions–top,twomiddle,andabottom.
b) Afterpreprocessingtheimage,wegetanimagewithbinarypixelvaluesas1or0’s.Wereadeveryimagearrayinasection,thensumthosearraysandfinallyaverageoutandstoretheseaveragedvalues inanewarray.Thisnewarray isamean representationof that specific

18|P a g e
section of lung area. By doing so, we average out the dark areas per region, with thehypothesisthatthehighertheaveragevalue,thelargertheprobabilityfornoduledetection.
c) Similarly,wefindaveragedarrayforeverysection.Thevaluesstored inthisarrayrangesfrom0to1.Weroundoffthesevaluesandfinallygetfourarrayswith0sand1sforeverypatient.
d) Wecalculatethenumberof1sineveryarray.Sofinally,foreverypatientwegetfourvalues–numberof1sineverysection.
e) Thesevaluesarethenusedasthefeatureinputforourclassificationmodel.
Approach2:First,featureextractionislargelydependentonimageidentification.ThusanycustomizedCNNmodelfirsthavetofedwithlotoftrainingdataunlikehumanbeingsforittounderstandwhichcategorythe imagebelongsto. Intheprocess itdoessobyupdating itsweights i.e.applyingappropriatefilters,andthusemphasizingonthefeaturetobeconsideredforrecognition.Thisprocessistimeconsumingaswitheachinput,itupdatestheweightsandlearnstoidentifythefeature.TheprocessoutlinedbelowwascreatedbyVisualGeometryGroup(VGG)whohavetrainedaCNNmodelwithatleast22,000categoriestohavethebestpossibleweightsforfeatureextraction.Forourcase,wecanusethemodeldirectlyforfeatureextractionwithouthavingtomanuallyupdatetheweights.With16layers,VGG16isanextremelyefficientimageprocessingalgorithm.Usingapre-trainedmodelallowsustoutilizethemostuptodatetechnologies inmachinelearninganddatamining.ByrunningthisCNNonthedata,weareabletoautodetectfeatures in each DICOM image. Thus, our output from the CNN is a data frame withapproximately40,000processedfeaturesperpatient.ThearchitectureforVGGisbelow:
Figure 6: VGG16 Architecture
ThismodelisavailableforboththeTheanoandTensorFlowbackend,andcanbebuiltbothwith"channels_first"dataformat(channels,height,width)or"channels_last"dataformat(height,width,channels).
19|P a g e
3. Classification–Finally,wecan inputourdata intoaclassificationmodel.Thedataframewillhaveeachindividualpatientasarow,andthedifferentfeaturesasacolumn.Thefinalcolumninthedataframewillbeabinaryvalue:1ifthepatienthascancer,and0ifthepatientdoesnothavecancer.Forvalidationpurposes,wewilluse75%percentofouroriginaldatafortrainingtheclassifier,and25%forvalidation.Frompreviousdiscussion,wementionedwearetakingtwodifferenttracksinordertofurtheranalyzetheaccuracydifferencesbetweenusingasimplevscomplexmodel.Thus,ourclassificationstepsforbothapproachesareasfollows:Approach1:OnceourimagesareprocessedandthepixelarrayisextractedfromeachCTscanfromapproach1mentionedabove,wecan feedthedata frame intoaclusteringalgorithmtogroupsimilarpatientstogether.Assuch,usingthefourfeaturespreviouslygenerated,weutilizedtheK-Meansclustering algorithm in order to partition the ~1,500 patients into k=2 clusters – positive ornegativeforcancer–whereeachpatientwillbelongtotheclusterwiththenearestmean.Bypartitioning the data space as such,we are able to gain a preliminary understanding of thedistinguishingcharacteristicsbetweenthetwogroups.TheK-Meansalgorithmpartitionedthedataintothetwogroupswithrelativelyhighaccuracy.WewerethenabletoaddtheK-Meansclusteringclassificationasaninputparametertoournextclassificationmethod:RandomForest.SinceRandomForestsareknowntoperformwellonvarious tasks, including unscaled data and variable selection, we decided to employ thisapproachinordertounderstandtheeffectivenessofourfeatureextractionmethodology.IfourRandom Forest returns a low accuracy, we can conclude that our feature extraction is notadequate,settingabasisforourdeeplearningapproach.
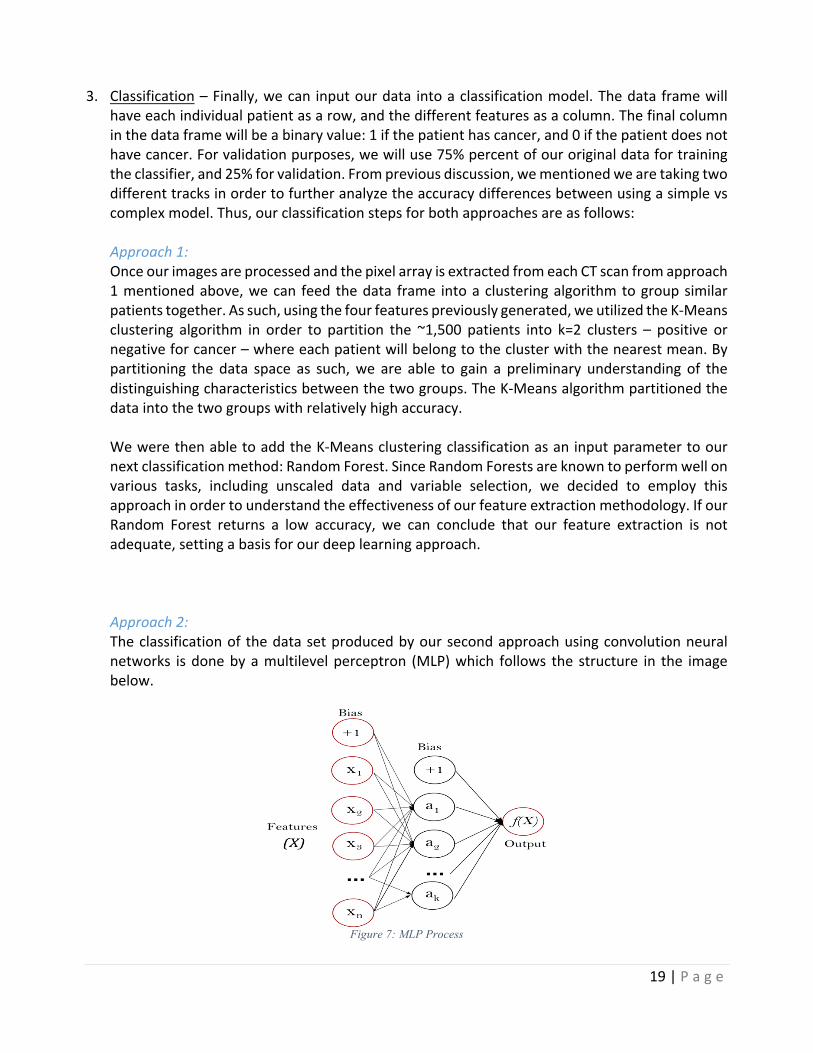
Approach2:Theclassificationof thedatasetproducedbyoursecondapproachusingconvolutionneuralnetworks isdonebyamultilevelperceptron (MLP)which follows the structure in the imagebelow.
Figure 7: MLP Process

20|P a g e
Using amultilevel perceptron has various advantages, including the capability to learn bothlinearandnon-linearmodels,andmostimportantly,thecapabilitytolearnmodelsinreal-time(on-linelearning)usingpartialfit.TheMLPthenfollowsthestepshighlightedbelow:
• Checksifthereapretrainedmodeltoloaditbeforetraining.• Sequentialmodelusedfortrainingthemodel.• Modelusesreluactivationwithvariousactivationlayers• Dropoutaftereverystagetopreventoverfitting• Model is compiled with ‘binary_crossentropy’ - loss which is the best for binary
classification,optimizer–RMSPROPbeingused• Checkpointer-usedtosavethebestmodelbasedonaccuracymetrics• Aftertraining,evaluationisdonetoshowtheefficiencyofthetrainedmodel.
5.4 LANGUAGESANDTOOLSUSED:Ourprojectwillutilize libraries frombothRandpython.Wewillprimarilyusepythontodothemajorityofourdataextractionandimageprocessing,whiletheclassificationmodelswillbebuiltandanalyzedusingbothRandpython.
21|P a g e
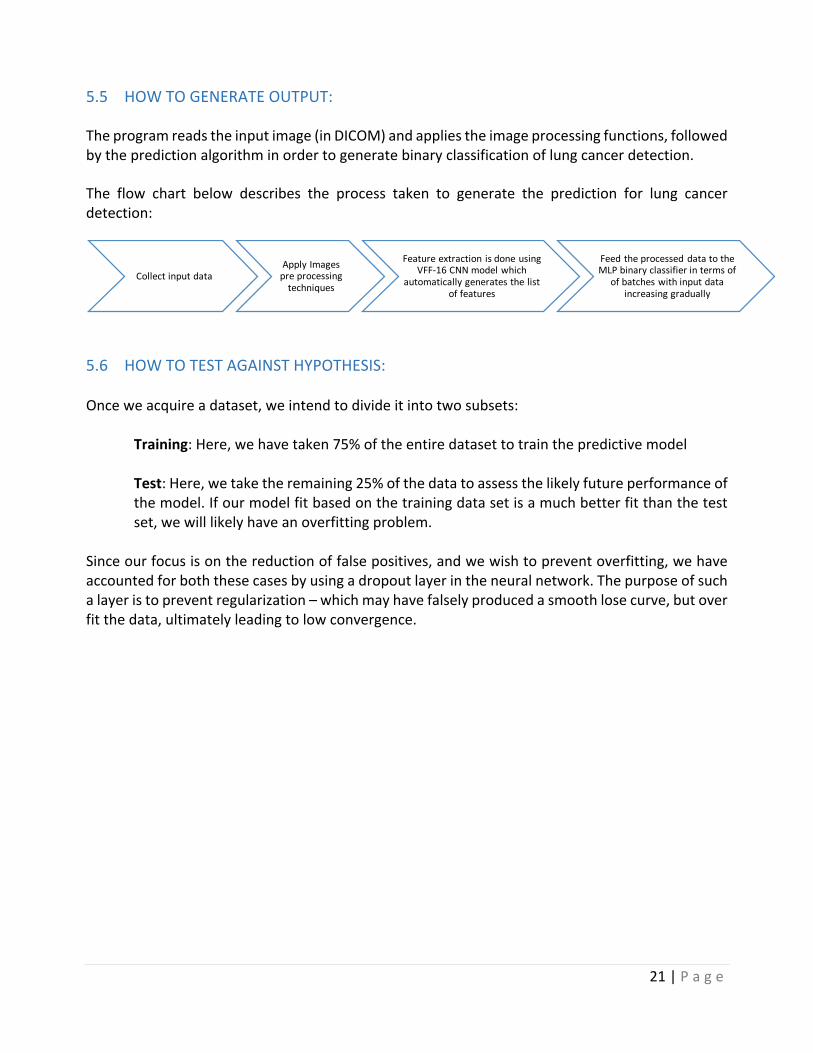
5.5 HOWTOGENERATEOUTPUT:
Theprogramreadstheinputimage(inDICOM)andappliestheimageprocessingfunctions,followedbythepredictionalgorithminordertogeneratebinaryclassificationoflungcancerdetection.
The flow chart below describes the process taken to generate the prediction for lung cancerdetection:
5.6 HOWTOTESTAGAINSTHYPOTHESIS:Onceweacquireadataset,weintendtodivideitintotwosubsets: Training:Here,wehavetaken75%oftheentiredatasettotrainthepredictivemodel
Test:Here,wetaketheremaining25%ofthedatatoassessthelikelyfutureperformanceofthemodel.Ifourmodelfitbasedonthetrainingdatasetisamuchbetterfitthanthetestset,wewilllikelyhaveanoverfittingproblem.
Sinceourfocusisonthereductionoffalsepositives,andwewishtopreventoverfitting,wehaveaccountedforboththesecasesbyusingadropoutlayerintheneuralnetwork.Thepurposeofsuchalayeristopreventregularization–whichmayhavefalselyproducedasmoothlosecurve,butoverfitthedata,ultimatelyleadingtolowconvergence.
CollectinputdataApplyImagespreprocessingtechniques
FeatureextractionisdoneusingVFF-16CNNmodelwhich
automaticallygeneratesthelistoffeatures
FeedtheprocesseddatatotheMLPbinaryclassifierintermsof
ofbatcheswithinputdataincreasinggradually
22|P a g e
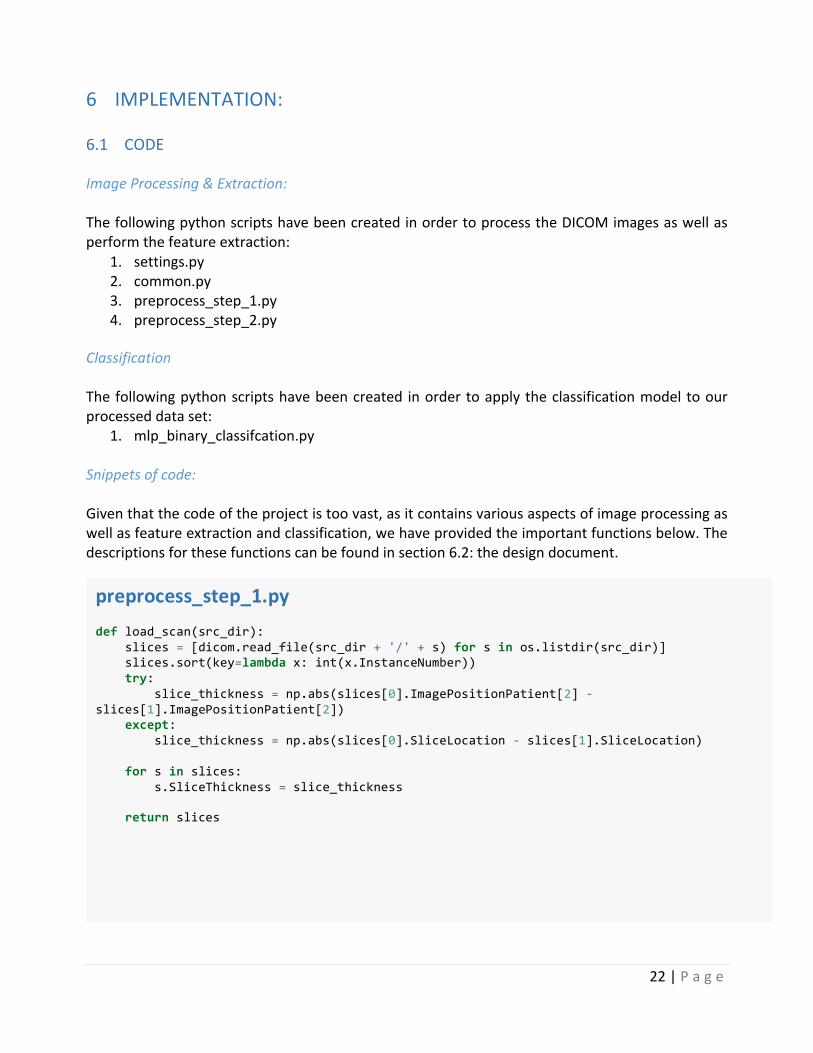
6 IMPLEMENTATION:6.1 CODE ImageProcessing&Extraction:ThefollowingpythonscriptshavebeencreatedinordertoprocesstheDICOMimagesaswellasperformthefeatureextraction:
1. settings.py2. common.py3. preprocess_step_1.py4. preprocess_step_2.py
ClassificationThefollowingpythonscriptshavebeencreated inordertoapplytheclassificationmodeltoourprocesseddataset:
1. mlp_binary_classifcation.py
Snippetsofcode:Giventhatthecodeoftheprojectistoovast,asitcontainsvariousaspectsofimageprocessingaswellasfeatureextractionandclassification,wehaveprovidedtheimportantfunctionsbelow.Thedescriptionsforthesefunctionscanbefoundinsection6.2:thedesigndocument.
preprocess_step_1.py def load_scan(src_dir): slices = [dicom.read_file(src_dir + '/' + s) for s in os.listdir(src_dir)] slices.sort(key=lambda x: int(x.InstanceNumber)) try: slice_thickness = np.abs(slices[0].ImagePositionPatient[2] - slices[1].ImagePositionPatient[2]) except: slice_thickness = np.abs(slices[0].SliceLocation - slices[1].SliceLocation) for s in slices: s.SliceThickness = slice_thickness return slices

23|P a g e
def resample(image, scan, new_spacing=[1, 1, 1]): # Determine current pixel spacing spacing = map(float, ([scan[0].SliceThickness] + scan[0].PixelSpacing)) #print spacing spacing = np.array(list(spacing)) resize_factor = spacing / new_spacing new_real_shape = image.shape * resize_factor new_shape = np.round(new_real_shape)
real_resize_factor = new_shape / image.shape new_spacing = spacing / real_resize_factor image = scipy.ndimage.interpolation.zoom(image, real_resize_factor) return image, new_spacing
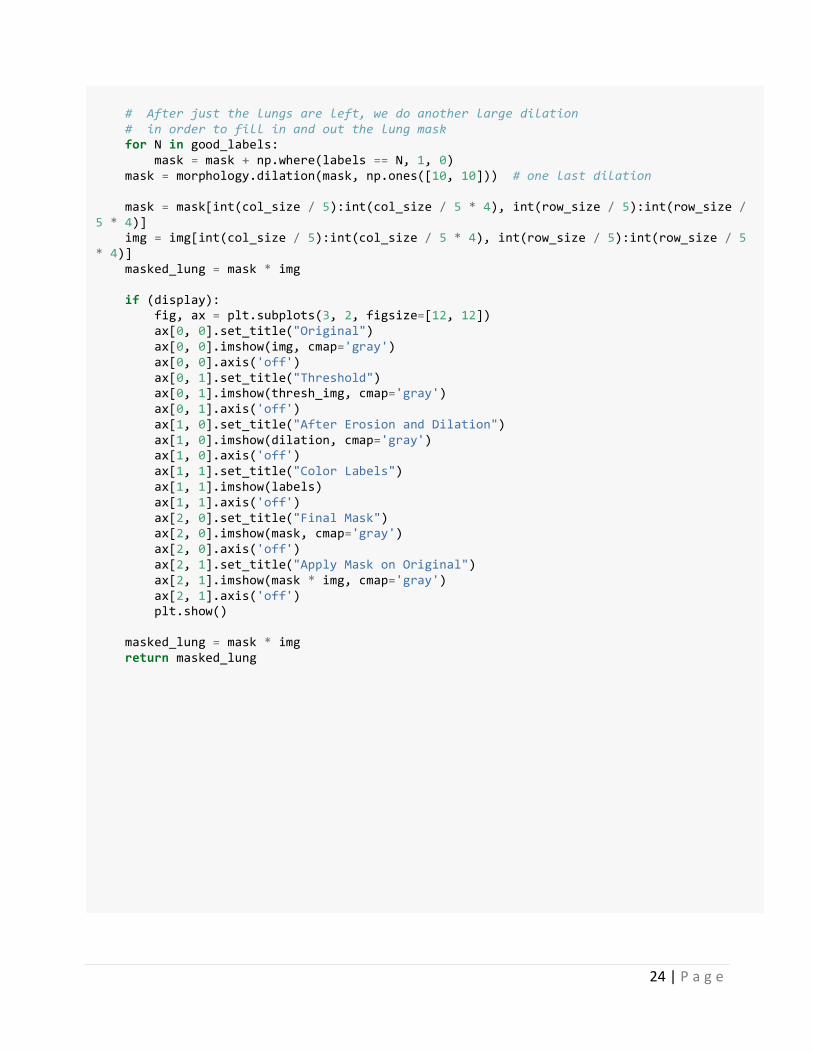
def make_lungmask(img, display=False): row_size = img.shape[0] col_size = img.shape[1] mean = np.mean(img) std = np.std(img) img = img - mean if std > 0: img = img / std # Find the average pixel value near the lungs to renormalize washed out images middle = img[int(col_size / 5):int(col_size / 5*4),
int(row_size / 5):int(row_size / 5 * 4)] mean = np.mean(middle) max = np.max(img) min = np.min(img) #To improve threshold finding,move underflow and overflow to pixel spectrum img[img == max] = mean img[img == min] = mean # Use Kmeans to separate foreground(soft tissue/bone) and background(lung/air) kmeans = KMeans(n_clusters=2).fit(np.reshape(middle,
[np.prod(middle.shape), 1])) centers = sorted(kmeans.cluster_centers_.flatten()) threshold = np.mean(centers) thresh_img = np.where(img < threshold, 1.0, 0.0) # threshold the image # First erode away the finer elements, then dilate to include some of the pixels surrounding the lung as we don't want to accidentally clip the lung. eroded = morphology.erosion(thresh_img, np.ones([3, 3])) dilation = morphology.dilation(eroded, np.ones([8, 8])) labels = measure.label(dilation) # Different labels are displayed in different colors label_vals = np.unique(labels) regions = measure.regionprops(labels) good_labels = [] for prop in regions: B = prop.bbox if B[2] - B[0] < row_size / 10 * 9 and B[3] - B[1] < col_size / 10 * 9 and B[0] > row_size / 5 and B[ 2] < col_size / 5 * 4: good_labels.append(prop.label) mask = np.ndarray([row_size, col_size], dtype=np.int8) mask[:] = 0
24|P a g e
# After just the lungs are left, we do another large dilation # in order to fill in and out the lung mask for N in good_labels: mask = mask + np.where(labels == N, 1, 0) mask = morphology.dilation(mask, np.ones([10, 10])) # one last dilation mask = mask[int(col_size / 5):int(col_size / 5 * 4), int(row_size / 5):int(row_size / 5 * 4)] img = img[int(col_size / 5):int(col_size / 5 * 4), int(row_size / 5):int(row_size / 5 * 4)] masked_lung = mask * img if (display): fig, ax = plt.subplots(3, 2, figsize=[12, 12]) ax[0, 0].set_title("Original") ax[0, 0].imshow(img, cmap='gray') ax[0, 0].axis('off') ax[0, 1].set_title("Threshold") ax[0, 1].imshow(thresh_img, cmap='gray') ax[0, 1].axis('off') ax[1, 0].set_title("After Erosion and Dilation") ax[1, 0].imshow(dilation, cmap='gray') ax[1, 0].axis('off') ax[1, 1].set_title("Color Labels") ax[1, 1].imshow(labels) ax[1, 1].axis('off') ax[2, 0].set_title("Final Mask") ax[2, 0].imshow(mask, cmap='gray') ax[2, 0].axis('off') ax[2, 1].set_title("Apply Mask on Original") ax[2, 1].imshow(mask * img, cmap='gray') ax[2, 1].axis('off') plt.show() masked_lung = mask * img return masked_lung

25|P a g e
preprocess_step_2.py def dump_features(patient_id): patient_id = patient_id[:-2] try: global COUNT COUNT = COUNT + 1 print("{}, {}".format(patient_id, COUNT)) model = applications.VGG16(include_top=False, weights='imagenet', input_shape=(settings.ct_width, settings.ct_height, 3)) features_train = model.predict_generator(generator(patient_id), steps=settings.ct_depth/3) features_train = np.reshape(features_train, (1, -1)) if settings.is_csv: np.savetxt("{}/{}.csv".format(settings.preprocess_step2_csv, patient_id), features_train, fmt ='%.2f', delimiter=',') else: pickle.dump(features_train, open("{}/{}.b".format(settings.preprocess_step2, patient_id), 'wb')) except Exception as e: print e mlp_binary_classifcation.py def create_model(): model = Sequential() model.add(Dense(128, input_dim=input_dim, activation='relu', kernel_initializer="normal", #kernel_regularizer=regularizers.l1(), # activity_regularizer=regularizers.l1(0.0001) )) model.add(Dropout(0.3)) model.add(Dense(64, activation='relu', kernel_initializer="normal")) model.add(Dropout(0.3)) model.add(Dense(32, activation='relu', kernel_initializer="normal")) model.add(Dropout(0.3)) model.add(Dense(16, activation='relu', kernel_initializer="normal")) model.add(Dropout(0.3)) model.add(Dense(8, activation='relu', kernel_initializer="normal")) model.add(Dropout(0.3)) model.add(Dense(1, activation='sigmoid')) sgd = SGD(lr=0.01, decay=1e-2, momentum=0.9) model.compile(loss='binary_crossentropy', optimizer='adam', metrics=['accuracy']) return model

26|P a g e
def train_model(): model = get_model() patient_ids = common.get_patient_ids() train_pct = 0.7 steps_per_epoch = int(len(patient_ids)*train_pct/settings.batch_size) validation_steps = max(1, steps_per_epoch * (1 - train_pct)) checkpointer = ModelCheckpoint(filepath=settings.model_filename, monitor='acc', verbose=1, save_best_only=True) early_stopping = EarlyStopping(monitor='acc', min_delta=0.001, patience=10, verbose=1, mode='auto') history = model.fit_generator( common.generate_arrays_from_file(input_shape=(input_dim,), train_pct=train_pct), steps_per_epoch=steps_per_epoch, epochs=settings.epochs, validation_data=common.generate_arrays_from_file(input_shape=(input_dim,), train_pct=train_pct, is_test=True), validation_steps=validation_steps, #validation_data=read_validation_data(30, input_shape=(input_dim,)), workers=4, pickle_safe=False, callbacks=[checkpointer]) score = model.evaluate_generator( common.generate_arrays_from_file(input_shape=(input_dim,), train_pct=0.80, is_test=True), steps=1) print score return model, history #score = model.evaluate(x_test, y_test) #print score model, history = train_model() model.save(settings.model_filename) pickle.dump(history.history, open(settings.model_dump_dir + "/cnn_history.b", "wb")) #plot_model(model, to_file=settings.output_dir + "/" + "mip_model.png") common.plot_history(history)

27|P a g e
6.2 DESIGNDOCUMENT:
DocumentationofFunctionsUsed:
Common.py
Method Description
get_patient_ids() ThisfunctionfetchesthepatientIDsforallthepatients
threadsafe_generator(f) Thisisadecoratorthattakesageneratorfunctionandmakesitthreadsafe
generate_arrays_from_file(input_shape,train_pct=0.9,is_test=False) Generatesanarrayfromvaluesinthefile
plot_history(history) Thisfunctionisusedtoplotthetrainingaccuracyandthetestaccuracy
preprocess_step_1.py
Method Description
load_scan(src_dir) Thisfunctionloopsovertheimagefilesandstoreseverythingintoalist.
get_pixels_hu(scans) ThisfunctionisusedforsegregatingthelungpartbyconvertingpixelstoHUunits
sample_stack(stack,rows=6,cols=6,start_with=10,show_every=3)
Usedsamplethestackof2Dimagesanddisplaythem
resample(image,scan,new_spacing=[1,1,1])
Resamplingisdonebythisfunctiontomakesurethatthedistancebetweentheslicesisuniform
reshape_ct(image,new_shape=[settings.ct_depth,settings.ct_width,settings.ct_height])
Reshapethe2Dimagesasperthedesiredshapeforthenextinput
make_lungmask(img,display=False) Functiontostandardizethepixelvalues

28|P a g e
preprocess(data_path) Thisfunctionprocessesalltheabovefunctionsdefined
dump_preprocess_data(patient_id)Usedtosavethepreprocessedimageintheformofbinaryfile/csvtobeusedbythefeatureextractionmodel
preprocess_all():
Functionusedtoiterateovereverypatientandpreprocesseachsliceperpatienttomakesureitisreadyforfeatureextraction
Pre_process_step_2.py
Method Description
read_preprocess_1(patient_id): Thisfunctionisusedtoloadthepreprocessedimages
generator(patient_id):
Thisfunctiontakesthepreprocessedimageandgeneratesnewimageswithdimension,whichcanbefedinto#VGG-16model.
dump_features(patient_id):
ThefeaturesextractedusingtheCNNmodel(VGG-16)aresavedtobefedtotheclassifierinthenextstageinthisfunction
preprocess2_all():
FunctionusedtoextractthefeaturesforeachofthescansbyVGG16model
Mlp_binary_clasification.py
Method Description
create_model()Thisfunctionisusedtocreateasequentialmodelthatisusedforsimplebinaryclassification.
get_model(): Functionusedtoloadapre-existingtrainedmodel

29|P a g e
train_model():
Thisfunctiongetapretrainedmodelifpresentorcreatesatrainingmodelandthentrainsitinepochs(asperthenumberofepochsmentioned)
evaluate_model(): Oncethemodelistrained,thisfunctionisusedtoevaluatethetestdata

30|P a g e
6.3 DESIGNDOCUMENTANDFLOWCHART Thefollowingsectionoutlinestheflowchartofouranalysis.
Start
Loadtheinput CTScanimagesofeachpatient
PreprocessingoftheImagewithImageprocessingmethods foruniformityandnoisereduction
FeatureExtractionusingVGG-16CNNmodel
Divideinputdataintotraindataandtestdata
Checkifthereisapretrainedmodelandthenloadsitbeforeproceedingwithtraining
Trainthemodelusingtrainingdataset
Findtheaccuracyandupdatethemodelifthelatestaccuracyisbetterthanearlier
Givethetestdataforevaluationofthemodel
DisplaytheOutput
Stop

31|P a g e
7 DATAANALYSISANDDISCUSSION7.1 OUTPUTGENERATION:TheprogramreadstheinputofaCTscanintheformofaDICOMimageperpatient,andappliesthepredictionalgorithmtoittogeneratetheoutput.Theimagesare2DslicesoftheCTscan.Wethentrainthemodelandanalyzetheaccuracyagainsttheactualresultforeachpatient(i.e.cancerousornon-cancerous).Wethenfindthedifferenceoftheoutputsandupdatetheweightsby-30%toavoidoverfitting.Thefinaloutputofouralgorithmisaclassificationofeachpatientaseitherpositiveornegativeforcancer.Thisoutputisgeneratedforallselectedpatients.7.2 OUTPUTANALYSIS: Approach 1:Aspreviouslymentioned,ourfirstapproachutilizestheRandomForestclassifieronthesimplisticfeatureextractionmodel.Assuch,theconfusionmatrixisasfollows:
PREDICTED:NOCANCER PREDICTED:YESCANCERACTUAL:NOCANCER 301 383ACTUAL:YESCANCER 117 128
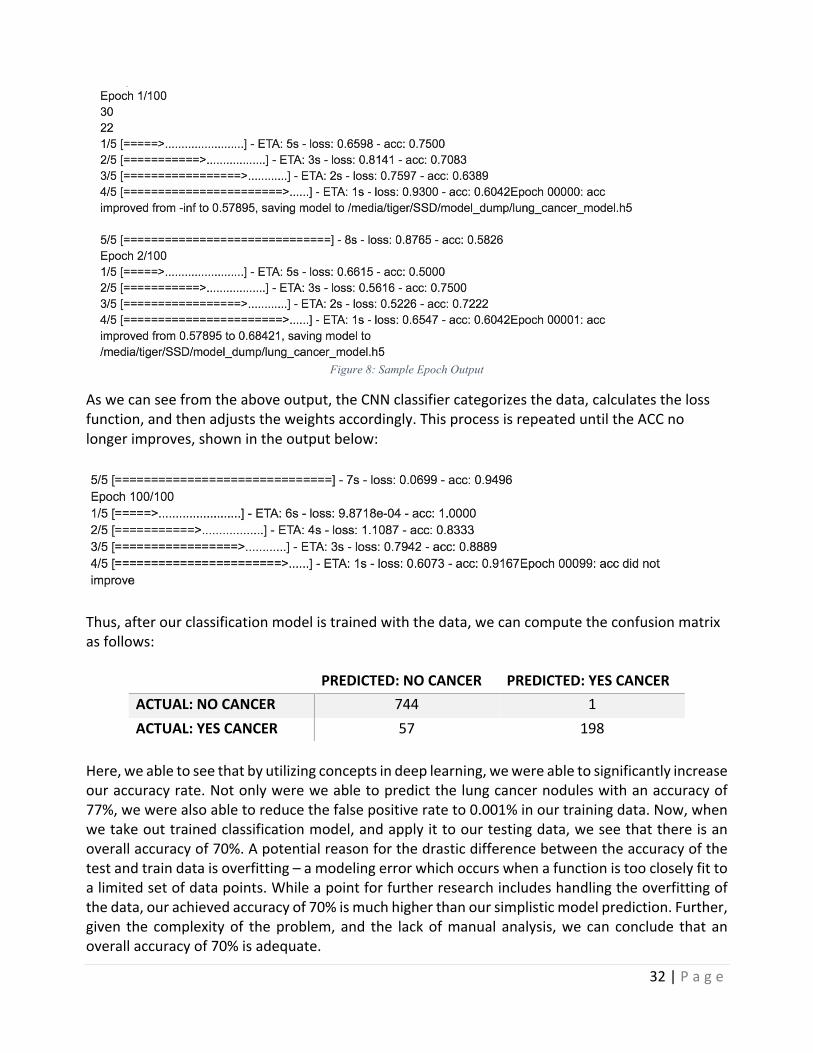
Here,confusionmatrixdisplaysthetotalnumberofcorrectandincorrectpredictionsmadebytheclassificationmodelincomparisontotheactualoutcomes.Forourpurposes,theperformanceofourmodelswillbeevaluatedusingthedatainthematrix.Fromtheaboveoutput,wecanseethatoutof684patientswhodidnothavecancer,383werepredictedincorrectly, indicatingthatourfalse positive rate is 56%. Similarly, out of the 245 patients who have cancer, only 128 werepredictedcorrectly,indicatingthatourfalsenegativerateis47%.Aswecansee,theaboveinputindicatesthatourfeatureextractionprocessisclearlyinadequatefordetectinglungcancernodules.Ouraccuracyrateisaround50%forboththefalsepositivesandfalsenegatives,andthus,wecanconcludethatthesimplisticmodelbasedonhigh-levelfeatureextractionandbasicclassificationisnotabletopredictlungcancernodulesatadesirableaccuracy.However,thesimplisticapproachprovidesuswithabaselineforfurtheranalysis.Asweproceedtoanalyzeourmorecomplexmodelinvolvingapre-trainedfeatureextractionconvolutionalneuralnetwork,wecanjudgeouraccuracynotonlybyarawpercentage,butalsoasarelativeincreasecomparedtooursimplisticmodel.Approach 2:Now,aswemoveforwardwiththedeeplearningapproachaspreviouslymentioned,weusedaconvolutionalneuralnetworktoclassifypatientsaseithercancerousornon-cancerous.Throughtheprocessoftrainingtheclassifier,welookattheepochoutputasfollowed:Ateachstep,theCNNcalculatestheEstimateTimeofArrival,loss,accuracyineachstage,totaltime,totallossandtotalaccuracyforentirestep.Sampleoutputisfoundbelow:
32|P a g e
Figure 8: Sample Epoch Output
Aswecanseefromtheaboveoutput,theCNNclassifiercategorizesthedata,calculatesthelossfunction,andthenadjuststheweightsaccordingly.ThisprocessisrepeateduntiltheACCnolongerimproves,shownintheoutputbelow:
Thus,afterourclassificationmodelistrainedwiththedata,wecancomputetheconfusionmatrixasfollows:
PREDICTED:NOCANCER PREDICTED:YESCANCERACTUAL:NOCANCER 744 1ACTUAL:YESCANCER 57 198
Here,weabletoseethatbyutilizingconceptsindeeplearning,wewereabletosignificantlyincreaseouraccuracyrate.Notonlywereweabletopredictthelungcancernoduleswithanaccuracyof77%,wewerealsoabletoreducethefalsepositiverateto0.001%inourtrainingdata.Now,whenwetakeouttrainedclassificationmodel,andapplyittoourtestingdata,weseethatthereisanoverallaccuracyof70%.Apotentialreasonforthedrasticdifferencebetweentheaccuracyofthetestandtraindataisoverfitting–amodelingerrorwhichoccurswhenafunctionistoocloselyfittoalimitedsetofdatapoints.Whileapointforfurtherresearchincludeshandlingtheoverfittingofthedata,ourachievedaccuracyof70%ismuchhigherthanoursimplisticmodelprediction.Further,given the complexityof theproblem, and the lackofmanual analysis,we can conclude that anoverallaccuracyof70%isadequate.

33|P a g e
7.3 COMPAREOUTPUTAGAINSTHYPOTHESIS The efficiency of the model depends on the preprocessing, the feature extraction and theclassificationmodel.Italsolargelydependsonthedatasetused,thequalityofCTscanimagesandalsothevolumeofdataorthenumberofpatients.Withincreasingrateoflungcancerwithtime,moredatawillbeavailableandthusitcanimprovetheefficiencyofthemodelaccordingly.Withthedatasetofaround1,500patientswithlowdoseCTscanimages(thathasaround300imagesperpatient)where75%ofdataistakenasinputand25%asoutput,wemanagedtogeta90%accuracywith our training data and a 70% accuracy rate with our test data with complete automatedpulmonarynoduledetection.7.4 ABNORMALCASEEXPLANATIONSince thedata availablewasof lowdoseCT scan, the imagequality could alsohavepotentiallyaffected the efficiency. With the advancement of technology, better CT scanners have beendevelopedwhichcouldtakeCTscanswithultimateprecisionandimagequality,hencebeingabetterinputforthemodel.7.5 DISCUSSION:We selected 1,000 patients to train our CNN classificationmodel, and used the remaining 200patientstotestthealgorithm.Manyiterationsortestingvariousparameterswereattemptedbeforeconcludingwiththeabovemodel.Asseen,wemayhaveapotentialproblemwithoverfitting,butfornow,wewillconcludethatourmodelisadequateforpredictingthedetectionoflungcancernodules.

34|P a g e
8 CONCLUSIONANDRECOMMENDATIONS8.1 SUMMARYANDCONCLUSIONS:Inthispaper,westudytheuseofimageprocessing,datamining,andmachinelearningtechniquestopredictlungcancernodulesinhighriskpatients.Basedontheresearchandanalysisconductedfor this project using a publicly available data set of lung CT scans,wewere able to develop asuccessful model for lung cancer nodule detection. By using a hybrid of approaches in imageprocessing and classification,wewere able todevelop anend to endprocess that detects lungcancernoduleswithhighaccuracy.Further,byplacingaheavyemphasisonautomationofimageprocessingaswellasareductionoffalsepositives,wewereabletodevelopafullmodelthatrunswith 70% accuracy on test data. Given the difficult nature of the problem, we faced variouschallengesthroughouttheprocess.First,thesegmentationoflungsisaverychallengingproblemduetoinhomogeneityinthelungregion,pulmonarystructuresofsimilardensitiessuchasarteries,veins,bronchi,andbronchioles,anddifferentscannersandscanningprotocolsanddifference inqualityoftheCTscans,theimageshadtobemadeuniformbeforeprocessing.TheCTscansbeinginhundredsofimagesperpatienthadamemoryconstraintwhileprocessingandalsowasatimeconsumingprocesssincedataperpatientwasrelativelyhigh(around300imagesperpatientwitharound1,500patients).8.2 RECOMMENDATIONSFORFUTURESTUDIES: Forfeatureextraction,wehaveuseVGG16thesimplicityofthemodelmakesiteasytoimplement.However, there are other pre-trained CNN models available too for feature extraction. Forcomplicatedprocesslikeimageclassification,manyotherdeeplearningtechnologiesareproposed.Ateachstage,onecoulduseanovelapproachtoretainthemaximumfeatures,whichwouldoveralllead toabettermodel.Otherpre-trainedmodelscouldbeused likeResnet,Googlenet,etc. forfeature extraction and othermodules for deep learning could be combined with deferent lossfunction, layers and optimization techniques for better results. As previously mentioned, ourclassificationmodelispotentiallyoverfittingthedata,andthus,thereexistsaclearopportunitytoresearchdifferentmethodologies to combat thisproblem.Finally, the imageclassificationbeingused is MLP classifier with sequential model, however, other regularization techniques andfunctionscouldbeexploredtoupdateweightsinordertoincreasetheaccuracyofthemodel.

35|P a g e
8.3 BIBLIOGRAPHY
"1.17.NeuralNetworkModels(supervised)"1.17.NeuralNetworkModels(supervised)—Scikit-learn0.18.1Documentation.Google,n.d.Web.12June2017.
AmericanCancerSociety.Cancerfactsandfigures,2015.URLhttp://www.
cancer.org/research/cancerfactsstatistics/index.Bechtold,RobertE.,MichaelY.M.Chen,DavidJ.Ott,RonaldJ.Zagoria,EricS.Scharling,NeilT.
Wolfman,andDavidJ.Vining."InterpretationofAbdominalCT:AnalysisofErrorsandTheirCauses."JournalofComputerAssistedTomography21.5(1997):681-85.Web.
Chauhan,Divya,andVarunJaiswal."AnEfficientDataMiningClassificationApproachforDetecting
LungCancerDisease."2016InternationalConferenceonCommunicationandElectronicsSystems(ICCES)(2016):n.pag.Web.
"GettingStartedwiththeKerasSequentialModel."GuidetotheSequentialModel-Keras
Documentation.N.p.,n.d.Web.12June2017.Golan,Rotem,ChristianJacob,andJorgDenzinger."LungNoduleDetectioninCTImagesUsing
DeepConvolutionalNeuralNetworks."2016InternationalJointConferenceonNeuralNetworks(IJCNN)(2016):n.pag.Web.
Hawkins,SamuelH.,JohnN.Korecki,YoganandBalagurunathan,YuhuaGu,VirendraKumar,
SatrajitBasu,LawrenceO.Hall,DmitryB.Goldgof,RobertA.Gatenby,andRobertJ.Gillies."PredictingOutcomesofNonsmallCellLungCancerUsingCTImageFeatures."IEEEAccess2(2014):1418-426.Web.
Jafar,Iyad,HaoYing,AnthonyF.Shields,andOttoMuzik."ComputerizedDetectionofLung
TumorsinPET/CTImages."2006InternationalConferenceoftheIEEEEngineeringinMedicineandBiologySociety(2006):n.pag.Web.
Juma,Kassimu,MaHe,andYueZhaoc."LungCancerDetectionandAnalysisUsingDataMining
Techniques,PrincipalComponentAnalysisandArtificialNeuralNetwork."AmericanScientificResearchJournalforEngineering,Technology,andSciences(n.d.):n.pag.Web.
Kuruvilla,Jinsa,andK.Gunavathi."LungCancerClassificationUsingNeuralNetworksforCT
Images."ComputerMethodsandProgramsinBiomedicine113.1(2014):202-09.Web.Paul,Rahul,SamuelH.Hawkins,LawrenceO.Hall,DmitryB.Goldgof,andRobertJ.Gillies.
"CombiningDeepNeuralNetworkandTraditionalImageFeaturestoImproveSurvivalPredictionAccuracyforLungCancerPatientsfromDiagnosticCT."2016IEEEInternationalConferenceonSystems,Man,andCybernetics(SMC)(2016):n.pag.Web.

36|P a g e
Rao,R.Bharat,JinboBi,GlennFung,MarcosSalganicoff,NancyObuchowski,andDavidNaidich."LungCAD."Proceedingsofthe13thACMSIGKDDInternationalConferenceonKnowledgeDiscoveryandDataMining-KDD'07(2007):n.pag.Web.
Raschka,Sebastian."KDnuggets."KDnuggetsAnalyticsBigDataDataMiningandDataScience.
N.p.,n.d.Web.12June2017.Rosebrock,Adrian."ImageNet:VGGNet,ResNet,Inception,andXceptionwith
Keras."PyImageSearch.Pyimagesearch,03May2017.Web.12June2017.Srivastava,Nitish,GeoffreyHinton,AlexKrizhevsky,IlyaSutskever,andRuslanSalakhutdinov.
"Dropout:ASimpleWaytoPreventNeuralNetworksfromOverfitting."JournalofMachineLearningResearch(2014):n.pag.Web.
Ypsilantis,Petros-Pavlos,andGiovanniMontana."RecurrentConvolutionalNetworksfor
PulmonaryNoduleDetectioninCTImaging."(2016):1-36.Https://arxiv.org/pdf/1609.09143.pdf.Web.May2017.
Zisserman,Andrew,andKarenSimonyan."VeryDeepConvolutionalNetworksforLarge-Scale
VisualRecognition."VisualGeometryGroupHomePage.VisualGeometryGroupDepartmentofEngineeringScience,UniversityofOxford,n.d.Web.12June2017.

37|P a g e
8.4 PROGRAMFLOWCHART Theprogramflowchartcanbefoundinsection6.3anddetailedinstructionsforrunningthecodecanbefoundinthesubmittedREADMEfile.
8.5 PROGRAMSOURCECODEWITHDOCUMENTATION Thecodecanbefoundinthesubmittedfiles,alongwithaREADMEfilecontainingthefulldocumentation.
8.6 INPUT/OUTPUTLISTING Input:Aspreviouslymentioned,theinputfilesareintheformofaDICOMimage.ExamplesofslicesinaDICOMimageforonepatientcanbefoundbelow.
Output:Thefinaloutputisaclassificationvalue:1forcancerous,and0fornon-cancerous.
Related Documents











