Autologous transplantation of bone marrow– derived endothelial progenitor cells attenuates monocrotaline-induced pulmonary arterial hypertension in rats Hon-Kan Yip, MD; Li-Teh Chang, PhD; Cheuk-Kwan Sun, MD, PhD; Jiunn-Jye Sheu, MD; Chiang-Hua Chiang, PhD; Ali A. Youssef, MD; Fan-Yen Lee, MD; Chiung-Jen Wu, MD; Morgan Fu, MD P ulmonary artery hypertension (PAH) is a devastating disease (1– 4). Although uncommon, severe pulmonary hyperten- sion can drastically limit physical capac- ity and seriously reduce life expectancy (3, 4). The disease is characterized by a progressive increase in pulmonary vascu- lar resistance caused by vascular cell pro- liferation and obliteration of pulmonary microvasculature, eventually leading to severe PAH and failure of the right side of the heart (5). Treatment of PAH is a formidable challenge for clinicians. A lot of strate- gic managements have been tried, in- cluding long-term therapy with oxygen or inhaled nitric oxide (6), diuretic therapy, anticoagulant agents, vasodila- tors (7), calcium channel blocker agents (8), intravenous prostacyclin (9, 10), phosphodiesterase inhibitors, and endothelin antagonists (11, 12). How- ever, these therapies remain problem- atic due to high cost, limited effective- ness, or serious side effects. Studies have recently demonstrated that circulating bone marrow– derived endothelial progenitor cells (BMDEPCs) play an essential role in repair of endo- thelial damage and participate directly in postnatal vasculogenesis and angiogene- sis in systemic and pulmonary vascular beds (13–17). In addition, two recent studies (14, 18) have shown that gene- transduced EPCs can repair the MCT- damaged lung and restore lung microvas- culature and function. Thus, BMDEPCs seem to be highly advantageous for cell therapy (13–19). However, data regarding the efficacy of EPCs on improvement of PAH and long-term outcome are still lim- ited. Therefore, a thorough understand- ing in the efficiency and mechanisms of EPC therapy is essential before clinical Objectives: Bone marrow– derived endothelial progenitor cells have been shown to circulate to damaged vascular endothelium and differentiate into mature endothelial cells. This study inves- tigated whether bone marrow– derived endothelial progenitor cell therapy ameliorates monocrotaline (MCT)-induced pulmonary ar- terial hypertension in a rat model. Design: Male Sprague-Dawley rats were randomized to re- ceive MCT (75 mg/kg) only (group 1), MCT plus autologous bone marrow– derived endothelial progenitor cell (1.2 10 6 cells) transplantation (group 2), and saline injection only (group 3). Mononuclear cells were obtained from femoral bone marrow of group 2 rats and isolated by Ficoll gradient centrif- ugation. The cells were cultured for 21 days in endothelial culture medium. Setting: An animal research laboratory at Kaohsiung Chang Gung Memorial Hospital. Measurements: Hemodynamics, ventricular weight, expres- sions of connexin43, endothelial nitric oxide synthase messenger RNA gene, Bcl-2, and number of alveolar sacs and small lung arterioles were measured. Results: Hemodynamic measurements on day 28 after MCT treat- ment revealed the development of significantly increased pulmonary arterial hypertension in MCT-treated groups (p < .0001). The bone marrow– derived endothelial progenitor cells were intravenously transplanted in group 2 on day 28 after MCT-induced pulmonary arterial hypertension. By day 90 after MCT treatment, the right ventricular systolic blood pressure and right ventricular hyper- trophy were significantly increased in group 1 compared with groups 2 and 3 (all p values <.01). In addition, connexin43 and endothelial nitric oxide synthase messenger RNA gene expres- sions of lung and right ventricle and Bcl-2 protein expression of right ventricle were significantly lower in group 1 than in groups 2 and 3 (all p values <.01). Furthermore, the number of alveolar sacs and small lung arterioles were significantly lower in group 1 than in groups 2 and 3 (all p values <.01). Conclusions: Autologous bone marrow– derived endothelial pro- genitor cell transplantation effectively ameliorates MCT-induced pul- monary arterial hypertension. (Crit Care Med 2008; 36:873–880) KEY WORDS: pulmonary arterial hypertension; autologous bone marrow– derived endothelial progenitor cell transplantation From the Division of Cardiology (HKY, CJW, MF), Department of General Surgery (CKS), and Department of Cardiovascular Surgery (JJS, FYL), Chang Gung Memorial Hospital–Kaohsiung Medical Center, Chang Gung Univer- sity College of Medicine, Kaohsiung, Taiwan, R.O.C.; Ba- sic Science, Nursing Department, Meiho Institute of Tech- nology, Pingtung, Taiwan (LTC); Department of Veterinary Medicine, National Pingtung University of Science and Technology, Kaohsiung, Taiwan, R.O.C. (CHC); and the Cardiology Department, Suez Canal University Hospital, Ismailia, Egypt (AAY). The authors have not disclosed any potential con- flicts of interest. Supported, in part, by program grant CMRPG 840621 from Chang Gung Memorial Hospital, Chang Gung University, Kaohsiung, Taiwan, ROC. For information regarding this article, E-mail: [email protected] Copyright © 2008 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins DOI: 10.1097/CCM.0B013E318165B7EA 873 Crit Care Med 2008 Vol. 36, No. 3

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Autologous transplantation of bone marrow–derived endothelialprogenitor cells attenuates monocrotaline-induced pulmonaryarterial hypertension in rats
Hon-Kan Yip, MD; Li-Teh Chang, PhD; Cheuk-Kwan Sun, MD, PhD; Jiunn-Jye Sheu, MD;Chiang-Hua Chiang, PhD; Ali A. Youssef, MD; Fan-Yen Lee, MD; Chiung-Jen Wu, MD; Morgan Fu, MD
Pulmonary artery hypertension(PAH) is a devastating disease(1– 4). Although uncommon,severe pulmonary hyperten-
sion can drastically limit physical capac-ity and seriously reduce life expectancy(3, 4). The disease is characterized by aprogressive increase in pulmonary vascu-lar resistance caused by vascular cell pro-liferation and obliteration of pulmonarymicrovasculature, eventually leading to
severe PAH and failure of the right side ofthe heart (5).
Treatment of PAH is a formidablechallenge for clinicians. A lot of strate-gic managements have been tried, in-cluding long-term therapy with oxygenor inhaled nitric oxide (6), diuretictherapy, anticoagulant agents, vasodila-tors (7), calcium channel blockeragents (8), intravenous prostacyclin (9,10), phosphodiesterase inhibitors, and
endothelin antagonists (11, 12). How-ever, these therapies remain problem-atic due to high cost, limited effective-ness, or serious side effects.
Studies have recently demonstratedthat circulating bone marrow– derivedendothelial progenitor cells (BMDEPCs)play an essential role in repair of endo-thelial damage and participate directly inpostnatal vasculogenesis and angiogene-sis in systemic and pulmonary vascularbeds (13–17). In addition, two recentstudies (14, 18) have shown that gene-transduced EPCs can repair the MCT-damaged lung and restore lung microvas-culature and function. Thus, BMDEPCsseem to be highly advantageous for celltherapy (13–19). However, data regardingthe efficacy of EPCs on improvement ofPAH and long-term outcome are still lim-ited. Therefore, a thorough understand-ing in the efficiency and mechanisms ofEPC therapy is essential before clinical
Objectives: Bone marrow–derived endothelial progenitor cellshave been shown to circulate to damaged vascular endotheliumand differentiate into mature endothelial cells. This study inves-tigated whether bone marrow–derived endothelial progenitor celltherapy ameliorates monocrotaline (MCT)-induced pulmonary ar-terial hypertension in a rat model.
Design: Male Sprague-Dawley rats were randomized to re-ceive MCT (75 mg/kg) only (group 1), MCT plus autologousbone marrow– derived endothelial progenitor cell (1.2 � 106
cells) transplantation (group 2), and saline injection only(group 3). Mononuclear cells were obtained from femoral bonemarrow of group 2 rats and isolated by Ficoll gradient centrif-ugation. The cells were cultured for 21 days in endothelialculture medium.
Setting: An animal research laboratory at Kaohsiung ChangGung Memorial Hospital.
Measurements: Hemodynamics, ventricular weight, expres-sions of connexin43, endothelial nitric oxide synthase messengerRNA gene, Bcl-2, and number of alveolar sacs and small lungarterioles were measured.
Results: Hemodynamic measurements on day 28 after MCT treat-ment revealed the development of significantly increased pulmonaryarterial hypertension in MCT-treated groups (p < .0001). The bonemarrow–derived endothelial progenitor cells were intravenouslytransplanted in group 2 on day 28 after MCT-induced pulmonaryarterial hypertension. By day 90 after MCT treatment, the rightventricular systolic blood pressure and right ventricular hyper-trophy were significantly increased in group 1 compared withgroups 2 and 3 (all p values <.01). In addition, connexin43 andendothelial nitric oxide synthase messenger RNA gene expres-sions of lung and right ventricle and Bcl-2 protein expressionof right ventricle were significantly lower in group 1 than ingroups 2 and 3 (all p values <.01). Furthermore, the number ofalveolar sacs and small lung arterioles were significantly lowerin group 1 than in groups 2 and 3 (all p values <.01).
Conclusions: Autologous bone marrow–derived endothelial pro-genitor cell transplantation effectively ameliorates MCT-induced pul-monary arterial hypertension. (Crit Care Med 2008; 36:873–880)
KEY WORDS: pulmonary arterial hypertension; autologous bonemarrow–derived endothelial progenitor cell transplantation
From the Division of Cardiology (HKY, CJW, MF),Department of General Surgery (CKS), and Department ofCardiovascular Surgery (JJS, FYL), Chang Gung MemorialHospital–Kaohsiung Medical Center, Chang Gung Univer-sity College of Medicine, Kaohsiung, Taiwan, R.O.C.; Ba-sic Science, Nursing Department, Meiho Institute of Tech-nology, Pingtung, Taiwan (LTC); Department of VeterinaryMedicine, National Pingtung University of Science andTechnology, Kaohsiung, Taiwan, R.O.C. (CHC); and theCardiology Department, Suez Canal University Hospital,Ismailia, Egypt (AAY).
The authors have not disclosed any potential con-flicts of interest.
Supported, in part, by program grant CMRPG840621 from Chang Gung Memorial Hospital, ChangGung University, Kaohsiung, Taiwan, ROC.
For information regarding this article, E-mail:[email protected]
Copyright © 2008 by the Society of Critical CareMedicine and Lippincott Williams & Wilkins
DOI: 10.1097/CCM.0B013E318165B7EA
873Crit Care Med 2008 Vol. 36, No. 3

application of EPC therapy on PAH pa-tients.
Connexin43 (Cx43) plays a key role inelectrical coupling between cardiomyo-cytes (20, 21). An association betweenright ventricular (RV) hypertrophy anddown-regulation of Cx43 expression hasbeen identified (22). In addition, in-creased cardiomyocyte apoptosis anddown-regulated antiapoptotic Bcl-2 geneexpression has been shown in a situationof chronic pressure overload (23).
Accordingly, the purpose of this studywas to evaluate whether autologous BM-DEPC transplantation is effective in at-tenuating PAH and, subsequently, themechanistic basis of biological signalingon recovery lung vascular structure andfunction after the administration ofmonocrotaline (MCT), which is known to
induce selective pulmonary endothelialinjury in rats.
MATERIALS AND METHODS
Ethics. All animal experimental procedureswere approved by the Institute of Animal Careand Use Committee at our hospital and per-formed in accordance with the Guide for theCare and Use of Laboratory Animals (NationalInstitutes of Health publication 85-23, Na-tional Academy Press, Washington, DC, re-vised 1996).
Bone Marrow Cell Isolation and Cultures.On day 7 after MCT-induced PAH, bone mar-row cells were aspirated from femurs of adultmale Sprague-Dawley rats, weighing 300–320g. The bone marrow cells were buffered in 10mL of culture medium (Iscove modified Dul-becco medium and 10% fetal bovine serum)and centrifuged at 400 � g for 5 mins, di-gested for 40 mins with 0.01% collagenase B
and DNase1, then filtered through a 30-�mnylon mesh. The bone marrow cells were thencentrifuged at 400 � g for 30 mins in Ficollsolution. The bone marrow–derived mononu-clear cells were then isolated by Ficoll-Paque(Amersham Pharmacia Biotech, Uppsala, Swe-den) density-gradient centrifugation. Finally,the interphase of bone marrow– derivedmononuclear cells was collected; the cellswere washed twice with phosphate-bufferedsaline before centrifugation at 400 � g for 5mins. Approximately 2.0 � 106 bone marrow–derived mononuclear cells were obtained ineach animal (both femoral bones) via thismethod. These cells were then cultured indifferential endothelial cells culture medium(endothelial cell basal medium-2, Cambrex,Walkersville, MD) with 10% fetal bovine se-rum, 50 units/mL penicillin, 50 �g/mL strep-tomycin and 2 mmol/L L-glutamine (Invitro-gen, Carlsbad, CA), and vascular endothelial
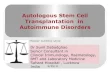
Figure 1. Left, after 21-day culture, spindle-shaped and cobblestone-like morphology typical of endothelial cells were observed under high-power field(�100). Middle and right, endothelial lineage was performed by flow cytometry in bone marrow–derived mononuclear cells after a 21-day cell culture.Endothelia lineage [A � CD31, B � KDR, C � CD29, D � CD90, E � von Willbrand factor (vWF), F � vascular endothelial growth factor (VEGF)] wasperformed by flow cytometry in bone marrow-derived mononuclear cells following 21-day cell culture.
874 Crit Care Med 2008 Vol. 36, No. 3

growth factor and basic fibroblast growth fac-tor (10 ng/mL) plated on gelatin-coated tissueculture flasks and incubated at 37°C with 5%CO2 for 21 days. Culture medium was changedevery 48 hrs. By day 21, plenty (1.0 � 106 to1.2 � 106) of spindle-shaped and cobblestone-like morphology typical of endothelial cellsattached on the plate were obtained (Fig. 1).Next, 3 mL of 4',6-diamidino-2-phenylindole(dissolved in phosphate-buffered saline in 10�M) was added into the culture medium andco-cultured with BMDEPCs (4',6-diamidino-2-phenylindole was specific for labeling nucleus)for 30 mins before 1.0 � 106 to 1.2 � 106
BMDEPCs were intravenously implanted foridentification of these cells in pulmonary ar-teries.
Animal Models of PAH. On day 0, patho-gen-free, male adult Sprague-Dawley rats (n �20), weighing 300–320 g (Charles River Tech-nology, BioLASCO Taiwan), were given onesubcutaneous injection of MCT (75 mg/kg;Sigma, St. Louis, MO). On day 7, MCT-treatedanimals were assigned to one of two experi-mental groups: group 1, MCT alone (n � 10);group 2, BMDEPC therapy (n � 10). Anotherten Sprague-Dawley rats (group 3) receivedonly subcutaneous injection of 3 mL of salineand served as the control group. To evaluatewhether BMDEPCs were trapped and en-grafted in pulmonary arteries, another threeSprague-Dawley rats that were treated withBMDEPCs were killed on day 35 after MCTtreatment (Fig. 2).
Trapping and Engraftment of Fluores-cently Labeled BMDEPCs. Fluorescently la-beled (4',6-diamidino-2-phenylindole) BMDEPCs(1.2 � 106) were intravenously injected fromtail vein into pulmonary circulation of group 2rats on day 28 after MCT-induced PAH. Oneweek later, after the delivery of the BMDEPCs,the fluorescently labeled BMDEPCs were ob-served to be trapped and engrafted into thepulmonary arteries (Fig. 3). However, no fluo-rescently labeled BMDEPC was trapped or en-grafted in RV or inferior vena cava (data notshown).
Hemodynamic Studies. Pulmonary arteryblood flow (PABF) was measured using a com-mercially available echocardiographic system(UF-750XT) equipped with an 8-MHz linear-array transducer for animals (FUKUDA Den-shi, Hongo, Bunkyo-Ku, Tokyo, Japan) beforeMCT treatment on day 35 and on day 90 afterMCT treatment.
On days 28 and 90 after MCT-induced PAH,rats were anesthetized by intraperitoneal in-jections of chloral hydrate (35 mg/kg). Aftershaving the chest, each animal was intubatedwith positive-pressure ventilation (180 mL/min) with room air using a small-animal ven-tilator (SAR-830/A, CWE, Ardmore, PA). Theheart was exposed by left thoracotomy. A ster-ile, 20-gauge, soft plastic–coated needle wasinserted into the left ventricle (LV) and RV ofeach rat and connected to a hemodynamicmonitor (HP M1165A, Model 56S; HewlettPackard, Medical Products Group, Andover,
Figure 2. Schematic representation of experimental setup. *Group 1, monocrotaline (MCT)-treatedonly; *Group 2, MCT-treated plus bone marrow–derived endothelial progenitor cells (BMDEPC)transplantation; *Group 3, control group. †Two rats died in group 1 and group 2 within 3–5 days afterMCT treatment. ‡Two rats in group 1 and one rat in group 2 died 60 days after MCT treatment.Parenthetical letters A–E indicate on which day the individual procedure was performed (days 28, 35,or 90).
Figure 3. Confocal digital images at higher magnification using �63 objective show that thefluorescently labeled (4',6-diamidino-2-phenylindole) bone marrow–derived endothelial progenitorcells (BMDEPC) engrafted into (white arrows in A, B, and C) and were trapped in (white arrowheads,D) the pulmonary arterioles on day 7 after BMDEPC implantation. Green color was positively stainedsmooth-� actin. The scale bars in the right lower corner represent 50 �m.
875Crit Care Med 2008 Vol. 36, No. 3

MA) to measure LV and RV systolic bloodpressures (RVSP). On day 90, after measuringRVSP, the rats were killed and hearts andlungs were harvested. The ratio of right-to-left ventricular plus septum weight was de-termined. Left lung was cut into pieces andembedded in paraffinized sections. The rightlung was dissected into pieces, frozen inliquid nitrogen, then stored at �80°C untilfurther use.
Western Blot Analysis for Lung Tissue andRight Ventricular Myocardium. To evaluatethe anti-apoptotic effect of BMDEPC therapy,equal amounts (30 �g) of protein extractsfrom RV were analyzed by Western blot forBcl-2. In addition, to investigate the effect ofBMDEPC therapy on prevention of down-regulation of Cx43, protein aliquots (30 �g) ofRV and lung were Western blotted for Cx43according to the manufacturer’s instructions.
Immunolabeling of Connexin43 andQuantitative Image Data Analysis. Six serialsections of lung and RV tissues (three longi-tudinal and three transverse) were prepared ata thickness of 4 �m by Cryostat (CM3050S,Leica Microsystems, Nussloch, Germany) forCx43 immunolabeling. To co-localize tropo-nin I and Cx43 in the same sample, tissuesections were first incubated with a mixture of
polyclonal anti-Cx43 (1:200) plus anti-tropo-nin I (1:200) for 24 hrs at 4°C, then incubatedwith anti-mouse fluorescein isothiocyanate (1:200) and anti-rabbit rhodamine (1:200) for 30mins at room temperature.
Calculation of the integrated area of Cx43spots in the slides was achieved using ImageTool 3 (IT3) image analysis software (ImageTool for Windows, Version 3.0, University ofTexas Health Science Center, San Antonio, TX)(24). Three selected slides for each animalwere quantified. The number of pixels in eachCx43 spot per high-power field (HPF) was firstdetermined, followed by summation of thepixels number obtained from the three HPFsin each slide. The mean number of pixels perHPF for each animal was then determined bysummation of all pixel numbers divided bynine. The mean area of Cx43 per HPF wasobtained by adopting a conversion factor of19.24 (1 �m2 represented 19.24 pixels).
Real-Time Quantitative Polymerase ChainReaction Analysis for Endothelial Nitric OxideSynthase Gene Expression in Lung Tissue andRV. Real-time polymerase chain reaction wasconducted using LightCycler TaqMan Master(Roche Diagnostics Corp., Indianapolis, IN) ina single capillary tube according to the man-ufacturer’s guidelines for individual compo-
nent concentrations. Forward and reverseprimers (Table 1) were each designed in adifferent exon of the target gene sequence,eliminating the possibility for amplifyinggenomic DNA. A positive result was deter-mined by identifying the threshold cycle valueat which reporter dye emission appeared abovebackground. If a fluorescence signal was notdetected within 55 cycles, the sample was con-sidered negative.
Distribution of Alveolar Sacs and Vesselsin Lung Parenchyma. Immunohistochemicalstaining of smooth �-actin (Sigma) was per-formed to determine the number of alveolarsacs and arterioles according to the manufac-turer’s instructors. Three lung sections fromeach rat were analyzed to determine numberof alveolar sacs and arterioles. For quantifica-tion, three randomly selected HPFs (�100)were analyzed in each slide. Thus, the meannumber per HPF for each animal was thendetermined by summation of all numbers di-vided by nine.
Statistical Analysis. Data are expressed asmean values (mean � SD). The differences inthe data simply between two groups were de-termined by Student’s t-test. The mean valuesamong groups in Table 2 were compared byone-way analysis of variance or repeated mea-sures of analysis of variance followed by Tukeymultiple comparison procedure. Statisticalanalysis was performed using SAS statisticalsoftware for Windows, version 8.2 (SAS Insti-tute, Cary, NC). A probability value of �.05was considered statistically significant.
RESULTS
In Vitro Characteristics of BMDEPCsAfter 21-Day Culture. After 21 days ofculture in endothelial growth medium,bone marrow–derived mononuclear cellsexhibited spindle-shaped or cobblestone-like morphology typical of endothelialcells (Fig. 1, left). The cells were alsopositive for a panel of endothelial cellmarkers, including CD29, CD31, CD90,KDR, von Willebrand factor, and vascularendothelial growth factor by flow cytom-etry (Fig. 1, middle and right). The cellswere therefore confirmed as BMDEPCs.
Hemodynamic Results and the Ratioof RV to LV plus Septum Weight on day90 After MCT Treatment. On day 0, bodyweight did not differ among the threegroups (Table 2). However, on day 90,body weight was significantly lower ingroup 1 than in groups 2 and 3 andsignificantly lower in group 2 than ingroup 3.
The RVSP was significantly higher ingroups 1 and 2 than in group 3 on day 28after MCT treatment. Moreover, RVSPwas markedly increased in group 1 com-pared with groups 2 and 3 on day 90 after
Table 1. Primer used for real-time polymerase chain reaction (PCR) amplification
Gene GenBank Accession NumberForward Primer (5�-3�)Reverse Primer (5�-3�) PCR Product Size (base pair)
eNOS NM_021838-2 TGGAAATTAACGTGGCTGTG 112GCCTTCTGCTCATTTTCCAA
�-Actin U19893-1 CTGGGGCCTGAGGAGTTC 87CCGGTTGAACTCAGCATCA
eNOS, endothelial nitric oxide synthase.
Table 2. Summarized data of body weight, ratio of right ventricle (RV) to left ventricle (LV) plusseptum weight, and hemodynamics in three groups of rats
Variables Group 1 Group 2 Group 3 p Value
Body weight on day 0, g 312.3 � 8.1 313.4 � 7.7 310.9 � 8.4 .667Body weight on day 90, g 343.4 � 10.1† 385.5 � 8.9‡ 478.2 � 10.6¶ �.0001RVSP on day 28, mm Hg 55.4 � 2.6† 54.9 � 2.4† 25.8 � 3.2‡ �.0001RVSP on day 90, mm Hg 70.6 � 6.1† 58.6 � 4.6‡ 26.8 � 3.6¶ �.0001RV/LV S on day 90 0.73 � 0.08† 0.59 � 0.11‡ 0.26 � 0.10¶ �.0001LVSB, mm Hg 81.7 � 3.3† 82.6 � 3.8† 71.3 � 2.6‡ �.001DT-PABF on day 0§, msecs a65.4 � 2.2 a66.4 � 1.9 65.8 � 1.4 .779DT-PABF on day 35§, msecs b54.5 � 1.91 b54.3 � 1.91 66.1 � 2.22 �.001DT-PABF on day 90§, msecs c40.8 � 3.11 b51.6 � 2.12 65.8 � 2.33 �.0001p Value of DT-PABF in the same
group among days 0, 35, and 90�.0001 �.0001 .747
Group 1, monocrotaline-treated only; Group 2, monocrotaline plus bone marrow–derived endo-thelial progenitor cells; Group 3, control group; RVSP, right ventricular systolic blood pressure; LV S, left ventricle plus septum; LVSP, left ventricular systolic blood pressure; DT-PABF, decelerationtime of pulmonary artery blood flow. Data are expressed as mean � SD. §Letters (a, b, c) among days(by repeated-measures analysis of variance) and numbers (1, 2, 3) among groups (by one-way analysisof variance) of DT-PABF indicate significant difference (p � .05 level) by Tukey multiple comparisonsprocedure. Mean values of the groups with significant difference (p � .0001) by one-way analysis ofvariance: p � .05 for ¶ vs. †, ¶ vs. ‡, and ‡ vs. †; p � .05 for a vs. b, a vs. c, and b vs. c; p � .05 for 1
vs. 2, 1 vs. 3, and 2 vs. 3.
876 Crit Care Med 2008 Vol. 36, No. 3

MCT-induced PAH. Although RVSP wasstill higher in group 2 than in group 3 onday 90 after MCT treatment, comparedwith day 28 after MCT treatment, RVSPwas not significantly increased on day 90after BMDEPC implantation in group 2rats. Furthermore, the LVSP was signifi-cantly higher in groups 1 and 2 than ingroup 1.
By day 90, the ratio of right-to-leftventricular plus septum weight was re-markably higher in group 1 than ingroups 2 and 3 and significantly higher ingroup 2 than in group 3.
On day 0, the deceleration time (DT)of PABF did not differ among the threegroups before MCT-induced PAH. How-ever, the DT-PABF was significantly de-creased in groups 1 and 2 in comparisonwith group 3 on day 35 after MCT treat-ment. Moreover, the DT-PABF was sub-stantially decreased in group 1 comparedwith groups 2 and 3 on day 90 after MCTtreatment. Although the DT-PABF wasstill higher in group 2 than in group 3 byday 90 after BMDEPC implantation, com-
pared with day 35 after MCT treatment,the DT-PABF did not significantly in-crease by day 90 after BMDEPC implan-tation in group 2 rats.
Western Blot Results. The Cx43 pro-tein expression of RV and lung was sub-stantially lower in group 1 than in groups2 and 3 on day 90 after MCT treatment(Fig. 4, left and middle). In addition, Cx43protein expression of RV was significantlylower in group 2 than in group 3 (Fig. 4,left). Moreover, Bcl-2 protein expressionof RV was significantly lower in group 1than in groups 2 and 3 by day 90 afterMCT treatment (Fig. 4, right).
Connexin43 Expression. Figure 5shows the results of quantification of in-tegrated area of clustered Cx43 spots ineach group of RV tissue on day 90 afterMCT treatment. The summation area ofCx43 was significantly lower in group 1than in groups 2 and 3 and significantlylower in group 2 than in group 3 (Fig. 5,left). In addition, expression of Cx43 gapjunctions exhibited greater down-regula-
tion in group 1 than in groups 2 and 3(Fig. 5, right).
Endothelial Nitric Oxide SynthaseGene Expression in Lung and RV.Changes in lung and RV endothelial ni-tric oxide messenger RNA expressionwere measured by real-time polymerasechain reaction. On day 90 after MCTtreatment, expression of endothelial ni-tric oxide messenger RNA in both lung(Fig. 6, left) and RV (Fig. 6, right) weresignificantly lower in group 1 than ingroups 2 and 3 and significantly lower ingroup 2 than in group 3.
Quantitative Analysis of Number ofAlveolar Sacs and Small Arteriolar Den-sity of Lung Parenchyma. The numberof arterioles (�100 �m) of lung paren-chyma was substantially lower in group1 than in groups 2 and 3 on day 90 afterMCT treatment (Fig. 7, left). In addi-tion, histopathological findings showedarteriolar wall thickness was notably in-creased in group 1 compared withgroups 2 and 3 (Fig. 7, middle). Fur-thermore, microscopic findings re-
Figure 4. Left, connexin43 (Cx43) protein expression of right ventricle in each group of rats on day 90 after monocrotaline (MCT) treatment. BMDEPCs,bone marrow–derived endothelial progenitor cells. ‡Normal vs. †MCTBMDEPCs, p � .006; ‡Normal vs. *MCT, p � .0006; †MCTBMDEPCs vs. *MCT,p � .027. Middle, Cx43 protein expression of lung in each group of rats on day 90 after MCT treatment. ‡Normal vs. †MCTBMDEPCs, p � .762; ‡Normalvs. *MCT, p � .004; †MCTBMDEPCs vs. *MCT, p � .026. Right, Bcl-2 expression of right ventricle in each group of rats on day 90 after MCT treatment.‡Normal vs. †MCTBMDEPCs, p � .682; ‡Normal vs. *MCT, p � .022; †MCTBMDEPCs vs. *MCT, p � .041.
Figure 5. Left, integrated area of positively stained connexin43 (Cx43) of right ventricle in each group of rats on day 90 after monocrotaline (MCT)treatment. BMDEPCs, bone marrow–derived endothelial progenitor cells. Mean values of the groups with significant difference (p � .0001) by one-wayanalysis of variance; in addition, p � .05 for ‡Normal vs. †MCTBMDEPCs, ‡Normal vs. *MCT, and †MCTBMDEPCs vs. *MCT. Right, semiquantitativeimmunofluorescence images identifying fewer spots of Cx43-positive staining (red color) located between cardiomyocytes in MCT-treated rats (A) than inMCT-treated plus BMDEPC therapy (B) and normal control rats (C). In addition, as compared with the MCT plus BMDEPC treatment and normal control,the appearance of the Cx43 gap junctions (yellow arrows) in the MCT-treated group was not homogeneously distributed, with reduced numbers of intactCx43 gap junctions. The scale bars in right lower corner represent 50 �m (A and B) and 100 �m (C).
877Crit Care Med 2008 Vol. 36, No. 3

vealed that the lung parenchyma wasmore crowded together and the septumwas thickened more in group 1 than ingroups 2 and 3 (Fig. 7, middle). More-over, the number of alveolar sacs wasremarkably lower in group 1 than ingroups 2 and 3 on day 90 after MCTtreatment (Fig. 7, right).
Histopathological Finals of Kidneyand Mortality in Three Groups. By day35, histopathological examination (Fig.8) of kidneys from three groups re-vealed changes consistent with early re-nal disease, including glomerular hy-percellularity and diffuse increase inmesangial matrix in group 1 and group2 rats.
On day 90, four rats had died in group1, three in group 2, and none in group 3.The mortality rate was therefore signifi-
cantly higher in groups 1 and 2 than ingroup 3.
DISCUSSION
A recent study demonstrated that in-travenously administrated BMDEPCs areattracted to sites of cerebral injury (25–27) and accumulated in ischemic myo-cardium after myocardial infarction (28).In addition, circulating BMDEPCs play akey role in repairing damaged endothelialcells and participate in angiogenesis insystemic and pulmonary vascular beds(13–15, 17). These findings (13–15, 17,27, 28) support the principle that BMDEPCshave the ability of homing to the injuredvessels for repair of endothelial functionand to the ischemic organ for angiogen-esis (16, 17, 27). This activity, in turn,
improves ischemia-related organ dys-function (13, 14, 28).
An important finding of this study isthat intravenous administration of autol-ogous BMDEPCs is first trapped in thepulmonary arterioles and capillary net-works and then engrafted into the MCT-damaged pulmonary arterioles and capil-laries. On the other hand, BMDEPCs werenot trapped or engrafted in the RV orsystemic venous circulation. Interest-ingly, two recent studies also found thatintravenously implanted EPCs circulateinto distal pulmonary arteries and areincorporated into the endothelial liningin a MCT-injured lung to repair its func-tion after MCT-induced PAH (14, 18).These two recent studies (14, 18) provideadded support to the current experimen-tal findings. Taking these findings into
Figure 6. Left, endothelial nitric oxide synthase (eNOS) messenger (m)RNA expression in lung of each group of rats on day 90 after monocrotaline (MCT)treatment. BMDEPCs, bone marrow–derived endothelial progenitor cells. ‡Normal vs. †MCTBMDEPCs, p � .0005; ‡Normal vs. *MCT, p � .0001;MCTBMDEPCs vs. *MCT, p � .0004. Right, eNOS mRNA expression in RV of each group of rats on day 90 after MCT treatment. ‡Normal vs.†MCTBMDEPCs, p � .0001; ‡Normal vs. *MCT, p � .0001; †MCTBMDEPCs vs. *MCT, p � .007.
Figure 7. Left, number of lung vessels in high-power field (HPF) (�100) on day 90 after monocrotaline (MCT) treatment. BMDEPCs, bone marrow–derivedendothelial progenitor cells. Small vessels: ‡Normal vs. †MCTBMDEPCs, p � .461; ‡Normal vs. *MCT, p � .005; †MCTBMDEPCs vs. *MCT, p � .003.Total number of vessels: **Normal vs. ¶MCTBMDEPCs, p .5; **Normal vs. §MCT, p � .01; ¶MCTBMDEPCs vs. §MCT, p � .001. Middle,immunohistochemical staining (A–C) and hematoxylin and eosin staining (D–F) of the lung tissue on day 90 after MCT treatment. There are fewer smallvessels (�100 �m) in the MCT-treated group (A) than in the MCTBMDEPC-treated group (B) and normal control group (C). In addition, the vessel wall(an index of smooth muscle proliferation) was observed to be more thickened in the MCT-treated group than in the other two groups (black arrows). Thenumber of alveolar sacs was remarkably lower in the MCT-treated group (D) than in the MCTBMDEPC-treated group (E) and normal control group (F).Moreover, the lung parenchyma crowded together and the septum was more thickened in the MCT-treated group (D) than in the other two groups (E andF). Scale bars represent 200 �m. Right, number of alveolar sacs in HPF (�100) on day 90 after MCT treatment. ‡Normal vs. †MCTBMDEPCs, p � .631;‡Normal vs. *MCT, p � .002; †MCTBMDEPCs vs. *MCT, p � .003.
878 Crit Care Med 2008 Vol. 36, No. 3

consideration, we suggest that BMDEPCshave intrinsic ability to migrate to theMCT-damaged pulmonary vascular endo-thelial layer, where they differentiate intomature endothelial cells and restore theintegrity of vascular endothelial function.
The most important finding in thesetwo recent studies (14, 18) is that trans-plantation of EPCs or vasodilator gene-transduced EPCs significantly attenuatedthe PAH in MCT-treated rats. However,these studies (14, 18) did not further ad-dress the molecular–cellular biologicalsignaling of reversed PAH after EPCtransplantation. In the present study, themost important finding is that intrave-nous administration of autologous BM-DEPCs significantly reduced RV mass,RVSP, apoptosis of RV, thickness of arte-riolar smooth muscle layer, and attenu-ated the decreased numbers of alveolarsacs and arteriolar-capillary density andintegrity of Cx43. Therefore, our findings,in addition to supporting the results fromthese two recent studies (14, 18), furtherextend the findings obtained by these tworecent studies (14, 18).
This study showed that endothelial ni-tric oxide messenger RNA expression inlung and RV was significantly higher ingroup 2 than in group 1. The BMDEPCs
are known to express endothelial nitricoxide and produce nitric oxide (14). Ac-cordingly, we speculate that engraftedBMDEPCs in the pulmonary artery endo-thelia thereafter improve nitric oxide pro-duction. This, in turn, exerts vasodilata-tion effects, inhibits platelet aggregationand leukocyte migration to subendothe-lial layers, and attenuates vascularsmooth muscle proliferation, resulting inreduced severity of PAH.
Association between pressure overloadand down-regulated expression of anti-apoptotic Bcl-2 gene in RV and LV hasbeen reported by previous studies (23,29). In the present study, we also foundthat Bcl-2 protein expression was mark-edly suppressed in MCT-treated rats. In-terestingly, transplantation of BMDEPCscaused a significant up-regulation ofBcl-2 protein expression. Moreover, im-plantation of BMDEPCs revealed signifi-cant protection of lung parenchymal ar-chitecture and the integrity of alveolarsac and its apparatus from MCT damage.This in turn, improves nutrient and oxy-gen exchanges between alveolar sac andcapillary bed in the alveolar septum andameliorates the hypoxia-induced PAH.Furthermore, the finding of preservedCx43 expression in RV hypertrophy after
BMDEPC transplantation suggests re-duced RV pressure overload and RV hy-pertrophy. This suggestion is supportedby a recent study (22) showing that Cx43expression was substantially down-regulated by RV hypertrophy resultingfrom PAH in rats. Accordingly, our exper-imental results explain why the RVSP, areflex of pulmonary arterial systolic bloodpressure, was significantly decreased,whereas the DT-PABF, an index of pul-monary artery resistance, was notablyimproved in MCT-induced PAH rats afterautologous BMDEPC transplantation.Conclusively, our findings further inves-tigation of histopathological findings andmolecular– cellular biological signalingof BMDEPC therapy, in addition to he-modynamic measurement, strengthenthose of recent studies (14, 18) andprovide a rationale for investigating thepossibility of application of this noveltherapeutic paradigm that has beenpreliminarily reported to be beneficialin PAH patients (30).
By day 90, the LVSP, an index of sys-tolic arterial blood pressure, was notablyincreased in groups 1 and 2. In addition,proliferative glomerulonephritis was alsoobserved in these two groups of rats. Fur-thermore, markedly hemodynamic im-provement in pulmonary circulation afterBMDEPC treatment did not translate toimprove 90-day mortality in group 2 rats.This could be, at least in part, due to theMCT-induced extra-pulmonary organdamage.
This study has limitations. First, it didnot test the effect of administering largeror repeated doses of BMDEPCs. Second,although the reversal model of this studyprovides striking implications, the find-ings are still not predictive of response totherapy in PAH patients.
In conclusion, autologous transplan-tation of BMDEPCs is feasible and effec-tive for attenuating MCT-induced PAH ina rat model. This study revealed the needfor further elucidation of the safety andeffectiveness of BMDEPC therapy for PAHin human subjects.
REFERENCES
1. Rubin LJ: Primary pulmonary hypertension.N Engl J Med 1997; 336:111–117
2. Branzi A, Manes A, Galie N: Emerging med-ical therapies for pulmonary arterial hyper-tension. Prog Cardiovasc Dis 2002; 45:213–224
3. Runo JR, Loyd JE: Primary pulmonary hy-pertension. Lancet 2003; 361:1533–1544
Figure 8. Proliferative glomerulonephritis on day 21 after monocrotaline (MCT) treatment. Periodicacid-Schiff stain shows normal glomerulus (A); proliferative glomerulonephritis is observed in MCT-treated only (B) and MCT plus bone marrow–derived endothelial progenitor cells (BMDEPC)–treated(C) rats. Under high-power field (�400), glomerular hypercellularity and diffuse increase in mesangialmatrix are observed; some nuclear fragmentation (black arrows) is present in glomerulus ofMCTBMDEPC–treated rat (D). Scale bars represent 100 �m.
879Crit Care Med 2008 Vol. 36, No. 3

4. Gaine SP, Rubin LJ: Primary pulmonary hy-pertension. Lancet 1998; 352:719–725
5. Pietra GG, Edwards WD, Kay JM, et al: His-topathology of primary pulmonary hyperten-sion. Circulation 1989; 80:1198–1206
6. Anand IS, Prasad BAK, Chugh SS, et al: Ef-fects of inhaled nitric oxide and oxygen inhigh-altitude pulmonary edema. Circulation1998; 98:1441–1445
7. Barst RJ, Maislin G, Fishman AP: Vasodilatortherapy for primary pulmonary hypertensionin children. Circulation 1999; 99:1197–1208
8. Kalra L, Bone MF: Effect of nifedipine onphysiologic shunting and oxygenation inchronic obstructive pulmonary disease.Am J Med 1993; 94:419–423
9. Badesch DB, Tapson VF, McGood MD, et al:Continuous intravenous epoprostenol forpulmonary hypertension due to sclerodermaspectrum of disease: A randomized, con-trolled trial. Ann Intern Med 2000; 132:425–434
10. Barst RJ, Rubin LJ, Long WA, et al: A com-parison of continuous intravenous epopro-stenol (prostacyclin) with conventional ther-apy for primary pulmonary hypertension.N Engl J Med 1996; 334:296–301
11. Channick R, Simonneau G, Sitbon O, et al:Effects of dual endothelin-receptor antago-nist bosentan in patients with pulmonaryhypertension: A randomized placebo-con-trolled study. Lancet 2001; 358:1119–1123
12. Rubin LJ, Badesch DB, Barst RJ, et al: Bosen-tan therapy for pulmonary arterial hyperten-sion. N Engl J Med 2002; 346:896–903
13. Yoon CH, Hur J, Park KW, et al: Synergisticneovascularization by mixed transplantationof early endothelial progenitor cells and lateoutgrowth endothelial cells: The role of an-giogenic cytokines and matrix metallopro-teinases. Circulation 2005; 112:1618–1627
14. Zhao YD, Courtman DW, Deng Y, et al: Res-cue of monocrotaline-induced pulmonary ar-terial hypertension using bone marrow-derived endothelial-like progenitor cells:Efficacy of combined cell and eNOS genetherapy in established disease. Circ Res 2005;96:442–450
15. Luttun A, Carmeliet G, Carmeliet P: Vascularprogenitors: from biology to treatment.Trends Cardiovasc Med 2002; 12:88–96
16. Asahara T, Kawamoto A: Endothelial progen-itor cells for postnatal vasculogenesis.Am J Physiol Cell Physiol 2004; 287:C572–C579
17. Rocher AA, Schuster MD, Bonaros N, et al:Myocardial homing and neovascularizationby human bone marrow angioblasts is regu-lated by IL-8/Gro CXC chemokines. J MolCell Cardiol 2006; 40:455–464
18. Nagaya N, Kangawa K, Kanda M, et al: Hybridcell-gene therapy for pulmonary hyperten-sion based on phagocytosing action of endo-thelial progenitor cells. Circulation 2003;108:889–895
19. Davani S, Marandin A, Merisin N, et al: Mes-enchymal progenitor cells differentiate intoan endothelial phenotype, enhance vasculardensity, and improve heart function in a ratcellular cardiomyoplasty model. Circulation2003; 108(suppl II):II-253–II-258
20. Jalife J, Morley GE, Vaidya D: Connexins andimpulse propagation in the mouse heart. J Car-diovasc Electrophysiol 1999; 10:1649–1663
21. Vozzi C, Dupont E, Coppen SR, et al: Cham-ber-related differences in connexin expres-sion in human heart. J Mol Cell Cardiol1999; 31:991–1003
22. Uzzaman M, Honjo H, Takagishi Y, et al:Remodeling of gap junctional coupling inhypertrophied right ventricles of rats with
monocrotaline-induced pulmonary hyper-tension. Circ Res 2000; 86:871–878
23. Condorelli G, Morisco C, Stassi G, et al: In-creased cardiomyocyte apoptosis andchanges in proapoptotic and antiapoptoticgene bax and Bcl-2 during left ventricularadaptations to chronic pressure overload inthe rat. Circulation 1999; 99:3071–3078
24. Sheu JJ, Chang LT, Chiang CH, et al: Impactof diabetes on cardiomyocyte apoptosis andconnexin43 gap junction integrity. IntHeart J 2007; 48:48:233–245
25. Sanchez O, Humbert M, Sibon O, et al: Treat-ment of pulmonary hypertension secondaryto connective tissue diseases. Thorax 1999;54:273–277
26. D’Alonzo GE, Barst RJ, Ayres SM, et al: Sur-vival in patients with primary pulmonary hy-pertension: Results from a national prospectiveregistry. Ann Intern Med 1991; 115:343–349
27. Priller J, Flugel A, Wehner T, et al: Targetinggene-modified hematopoietic cells to thecentral nervous system: Use of green fluores-cent protein uncovers microglial engraft-ment. Nat Med 2001; 7:1356–1361
28. Kawamoto A, Gwon HC, Iwaguro H, et al:Therapeutic potential of ex vivo expandedendothelial progenitor cells for myocardialischemia. Circulation 2001; 103:634–637
29. Ecarnot-Laubriet A, Assem M, Poirson-Bichat F, et al: Stage-dependent activation ofcell cycle and apoptosis mechanisms in theright ventricle by pressure overload. BiochimBiophy Acta 2002; 1586:233–242
30. Wang XX, Zhang FR, Shang YP, et al: Trans-plantation of autologous endothelial progen-itor cells may be beneficial in patients withidiopathic pulmonary arterial hypertension.J Am Coll Cardiol 2007; 49:1566–1571
880 Crit Care Med 2008 Vol. 36, No. 3
Related Documents