Management in the Primary Care Setting Autism Spectrum Disorder and Mental Health Challenges in Youth February 13, 2016 Rebecca Marshall, MD, MPH

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Management in the Primary Care Setting
Autism Spectrum Disorder and Mental Health Challenges in Youth
February 13, 2016 Rebecca Marshal l , MD, MPH
2
Outline• DSM V Criteria
• Comorbidities
• Behavioral treatments
• Pharmacologic treatments
• Resources

3
Autism Spectrum Disorder• DSM IV DSM V• Autistic Disorder, Asperger’s Disorder, and PDD-NOS replaced with Autism
Spectrum Disorder (ASD). • Three core domains of impairment (communication, social interaction, and
restricted interests and repetitive behaviors) changed to two domains of impairment: social/communication deficits and restricted interests and repetitive behaviors.
• Also, a delay in language development is no longer necessary for a diagnosis.
4
DSM V – Autism Spectrum Disorder CriteriaA. Persistent deficits in social communication and social interaction across multiple contexts, as manifested by:
1. Deficits in social-emotional reciprocity, from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
2. Deficits in nonverbal communicative behaviors used for social interaction, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures; to a total lack of facial expressions and nonverbal communication.
3. Deficits in developing, maintaining, and understanding relationships, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
Specify current severity. Severity is based on social communication impairments and restricted repetitive patterns of behavior.
5
DSM V – Autism Spectrum Disorder CriteriaB. Restricted, repetitive patterns of behavior, interests, or activities:
1. Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypies, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns or verbal nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat food every day).
3. Highly restricted, fixated interests that are abnormal in intensity or focus (e.g, strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interest).
4. Hyper- or hyporeactivity to sensory input or unusual interests in sensory aspects of the environment (e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling ortouching of objects, visual fascination with lights or movement).
Specify current severity: Severity is based on social communication impairments and restricted, repetitive patterns of behavior (see Table 2).
6
DSM V – Autism Spectrum Disorder CriteriaC. Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.E. These disturbances are not better explained by intellectual disability or global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.Note: Individuals with a well-established DSM-IV diagnosis of autistic disorder, Asperger’s disorder, or pervasive developmental disorder not otherwise specified should be given the diagnosis of autism spectrum disorder. Individuals who have marked deficits in social communication, but whose symptoms do not otherwise meet criteria for autism spectrum disorder, should be evaluated for social (pragmatic) communication disorder.
7
ASD and Comorbid Psychiatric Disorders• 2008 prevalence study in JAACAP
• 112 children with ASD ages 10-14 were assessed for other psychiatric disorders.
• 70% had at least one comorbid disorder
• 41% had two or more. Emily Simonoff, Andrew Pickles, Tony Charman, Susie Chandler, Tom Loucas, Gillian Baird, Psychiatric Disorders in Children With Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample, Journal of the American Academy of Child & Adolescent Psychiatry, Volume 47, Issue 8, August 2008, Pages 921-929.
8
ASD and Comorbid Psychiatric Disorders• Most common diagnoses:
– social anxiety disorder (29.2%) – attention-deficit/hyperactivity disorder (28.2%)– Oppositional defiant disorder (28.1 %)– Generalized anxiety disorder (13.4%)– Panic disorder (10.1%)– Enuresis (11%)– Low rates of major depressive disorder (0.9%), dysthymic
disorder (0.5%), and conduct disorder (3.2%)
• 84% of those with ADHD had a second comorbid diagnosis.
9
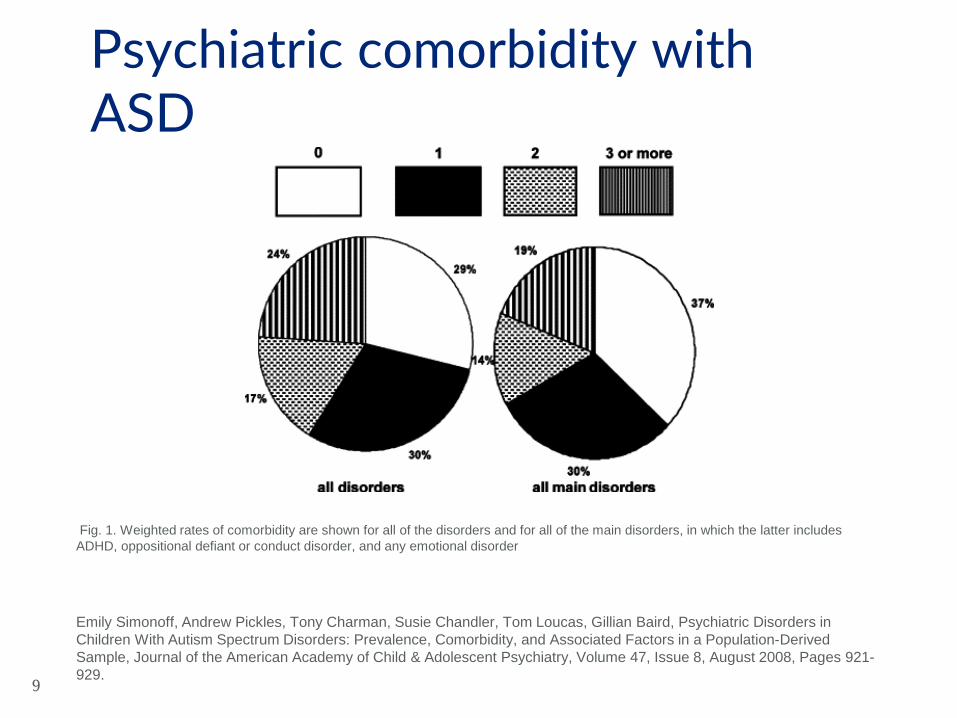
Fig. 1. Weighted rates of comorbidity are shown for all of the disorders and for all of the main disorders, in which the latter includes ADHD, oppositional defiant or conduct disorder, and any emotional disorder
Emily Simonoff, Andrew Pickles, Tony Charman, Susie Chandler, Tom Loucas, Gillian Baird, Psychiatric Disorders in Children With Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample, Journal of the American Academy of Child & Adolescent Psychiatry, Volume 47, Issue 8, August 2008, Pages 921-929.
Psychiatric comorbidity with ASD
10
Intellectual disability in those with ASD• approximately 50% exhibit severe or
profound intellectual disability • 35% exhibit mild to moderate
intellectual disability, and the remaining
• 20% have IQs in the normal range.18 Fred Volkmar, Matthew Siegel, Marc Woodbury-Smith, Bryan King, James McCracken, Matthew State, and the AACAP Committee on Quality Issues. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Autism Spectrum Disorder. JAACAP, 53 (2) 2014.
11
Behavioral difficulties in those with ASD• A range of behavioral difficulties can be observed in
ASD:– hyperactivity– obsessive-compulsive phenomena– self-injury– aggression– stereotypies– Tics– affective symptoms (lability, inappropriate affective
responses, anxiety, and depression)
12
Behavioral Treatments for ASD• Core feature of ASD is
difficulty with social interactions.
• Therapy / behavioral treatments therefore critical with strong evidence base for improved outcomes.
13
Applied Behavior Analysis• Based on concept of understanding how events influence and change
behavior. • Requires assessment of how events influence an individual’s behavior.
Includes:– contextual factors such as the setting in which a behavior occurs; – motivational variables such as the need to attain something; – antecedent events, such as a request to do something from another person; – Consequences following the behavior
• Progress is measured by direct observations over time. • Early Intensive Behavioral Intervention (EIBI) -- comprehensive ABA
program for young children– Intensive and highly individualized– Up to 40 hours per week of one-to-one direct teaching
Reichow, B. & Volkmar, F.R. Social skills interventions for individuals with autism: evaluation for evidence-based practices within a best evidence synthesis framework. Autism Dev Disord (2010) 40: 149.
14
Naturalistic treatment• Used to structure parent child interactions or
to teach imitation and/or joint attention behaviors
• Intervening in the natural environment with natural reinforcers during interactions guided by the child
• Evidence strongest for use with young children
Reichow, B. & Volkmar, F.R. Social skills interventions for individuals with autism: evaluation for evidence-based practices within a best evidence synthesis framework. Autism Dev Disord (2010) 40: 149.
15
Parent Training
Reichow, B. & Volkmar, F.R. Social skills interventions for individuals with autism: evaluation for evidence-based practices within a best evidence synthesis framework. Autism Dev Disord (2010) 40: 149.
• Important element of intervention programs for children with autism
• Accumulating evidence that parent training is an effective method for increasing the social skills of young children
16
Peer training• The use of peers to help teach children with autism
has been a commonly used method that has significant research support
• Used for both preschool and school-aged children• Like-aged individuals with and without individuals• Peers taught to provide specific elements of therapy
including visual supports and prompting
Reichow, B. & Volkmar, F.R. Social skills interventions for individuals with autism: evaluation for evidence-based practices within a best evidence synthesis framework. Autism Dev Disord (2010) 40: 149.
17
Other modalities• Visual supports (social stories, visual
schedules)• Social skills groups• Video modeling• Occupational / physical therapy
18
Communication • Typically addressed in the child’s IEP in
coordination with the speech-language pathologist.
• Nonverbal children: alternative communication modalities, i.e., sign language, communication boards, visual supports, picture exchange.
• Children with fluent speech: language skills training, for example targeting pragmatic language skills. Fred Volkmar, Matthew Siegel, Marc Woodbury-Smith, Bryan King, James McCracken, Matthew State, and the
AACAP Committee on Quality Issues. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Autism Spectrum Disorder. JAACAP, 53 (2) 2014.
19
Educational • Children with ASD need a structured educational approach with
explicit teaching.• Programs should involve planned, intensive, individualized
intervention with an experienced interdisciplinary team of providers, and family involvement
• Educational plan should include an assessment of child’s strengths and vulnerabilities, with a description of services to be provided, goals and objectives, and monitoring plan
• Curricula should enhance verbal and nonverbal communication, academic skills, and social, motor, and behavioral capabilities.
Fred Volkmar, Matthew Siegel, Marc Woodbury-Smith, Bryan King, James McCracken, Matthew State, and the AACAP Committee on Quality Issues. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Autism Spectrum Disorder. JAACAP, 53 (2) 2014.

20
Pharmacotherapy• Target specific symptom or comorbid condition • Combining medication with parent / behavioral training is more
efficacious than medication alone for decreasing serious behavioral disturbance and improving adaptive functioning.
• Individuals with ASD may be nonverbal, so treatment response is often judged by caregiver report and observation of specific behaviors.
• Use objective rating scales to help monitor treatment response.• SSRIs, atypical antipsychotic agents, stimulants, and α2-
adrenergic agonist antihypertensive agents are the most commonly prescribed classes of psychotropic medications for children with ASDs.Fred Volkmar, Matthew Siegel, Marc Woodbury-Smith, Bryan King, James McCracken, Matthew State, and the AACAP
Committee on Quality Issues. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Autism Spectrum Disorder. JAACAP, 53 (2) 2014.
21
SSRIs
• Double-blind, placebo-controlled trials have demonstrated efficacy of the SSRIs fluoxetine and fluvoxamine in the treatment of repetitive and other maladaptive behaviors in patients with ASDs
• Open-label trials of these and other SSRIs have shown improvements in target symptoms, including repetitive behaviors, irritability, depressive symptoms, tantrums, anxiety, aggression, difficulty with transitions, and aspects of social interaction and language.
• Potential adverse effects of SSRIs include but are not limited to nausea, drowsiness, sexual dysfunction, constipation, abdominal discomfort, fatigue, headache, dizziness, dry mouth, agitation, behavioral activation, hypomania or mania, apathy, suicidal ideation, and alteration of sleep.
Myers, SM, Plauche Johnson, C. Management of children with autism spectrum disorders. Pediatrics 120 (5), 2007, http://pediatrics.aappublications.org/content/120/5/1162#ref-162
22
Antipsychotics• Risperidone (2006) and aripiprazole (2009) FDA approved for
symptomatic treatment of irritability– Includes aggressive behavior, deliberate self-injury, and temper
tantrums in children and adolescents with ASDs. – Two large, multisite, randomized, controlled trials have confirmed the
short-term efficacy of risperidone for these severe disruptive behaviors in youth with ASDs
• Potential adverse effects include but are not limited to excessive appetite and weight gain, insulin resistance, dyslipidemia, hyperprolactinemia, extrapyramidal symptoms, tardive dyskinesia, neuroleptic malignant syndrome, QTc prolongation, dry mouth, urinary retention, constipation, seizures, hematologic abnormalities, and sedation.
Myers, SM, Plauche Johnson, C. Management of children with autism spectrum disorders. Pediatrics 120 (5), 2007, http://pediatrics.aappublications.org/content/120/5/1162#ref-162
23
Stimulants
• A double-blind, placebo-controlled study conducted by the Research Units on Pediatric Psychopharmacology (RUPP) Autism Network (Posey et al.,
2004) confirmed earlier findings that about half (49 percent) of children with
autism responded to methylphenidate with decreased hyperactivity and
inattention. • Significantly lower response than for children with ADHD without
autism. • A large percentage (18 percent) of children with autism treated with
methylphenidate experienced significant side effects that were intolerable.
• Potential adverse effects include appetite reduction, inhibition of growth, delayed sleep onset, jitteriness, exacerbation of tics, abdominal discomfort, increased blood pressure, increased heart rate, irritability, increased anxiety, and repetitive behaviors.
Myers, SM, Plauche Johnson, C. Management of children with autism spectrum disorders. Pediatrics 120 (5), 2007, http://pediatrics.aappublications.org/content/120/5/1162#ref-162
24
Atomoxetine• Some recent studies have suggested that
atomoxetine may be effective for attention-deficit/hyperactivity disorder–like symptoms in children and adolescents with ASDs
• Potential side effects include appetite suppression, nausea, fatigue, mood swings, suicidal ideation, dizziness, and liver injury
Myers, SM, Plauche Johnson, C. Management of children with autism spectrum disorders. Pediatrics 120 (5), 2007, http://pediatrics.aappublications.org/content/120/5/1162#ref-162
25
Alpha-2 agonists• Two small double-blind, placebo-controlled trials have documented modest
benefits of clonidine in reducing hyperarousal symptoms including hyperactivity, irritability and outbursts, impulsivity, and repetitive behaviors in children with ASDs.
• Small studies suggested that guanfacine was similarly effective in some patients.
• Potential adverse effects of these centrally acting α2-agonists include but are not limited to drowsiness, sedation, dry mouth, decreased blood pressure, dizziness, constipation, and irritability, and these drugs can be dangerous in overdose.
Myers, SM, Plauche Johnson, C. Management of children with autism spectrum disorders. Pediatrics 120 (5), 2007, http://pediatrics.aappublications.org/content/120/5/1162#ref-162
26
Omega-3s
• Hypothesis that Omega-3 supplementation should improve symptoms of ASD have not been borne out by research including 2011 Cochrane review. However larger controlled trials are needed.
Amminger, GP, Berger, GE, Schafer, MR, Klier, C, Friedrich, MH, Feucht, M. Omega-3 Fatty Acids Supplementation in Children with Autism: A Double-blind Randomized, Placebo-controlled Pilot Study. Biological Psychiatry 61(4); 2001 (551-553).
27
Sleep Problems• There is some evidence of abnormality of melatonin regulation
in children with ASDs• Melatonin may be effective for improving sleep onset in
children with ASDs • A recent open-label study suggested that controlled-release
melatonin improved sleep in a group of 25 children with ASDs and that treatment gains were maintained at 1- and 2-year follow-up
• Antihistamines, α2-agonists, benzodiazepines, chloral hydrate, trazodone, and newer nonbenzodiazepine hypnotic agents, such as zolpidem and zaleplon, can be trialed
Myers, SM, Plauche Johnson, C. Management of children with autism spectrum disorders. Pediatrics 120 (5), 2007, http://pediatrics.aappublications.org/content/120/5/1162#ref-162

28
ASPEN TM, Inc. (Asperger Syndrome Education Network) (http://www.aspennj.org)
A regional nonprofit organization providing families and those individuals affected with Asperger syndrome and related disorders with information, support, and advocacy.
Autism Society of America (http://www.autism- society.org)
The mission of the Autism Society of America is to promote lifelong access and opportunities for persons within the autism spectrum and their families to be fully included, participating members of their communities through advocacy, public awareness, education, and research related to autism.
Autism Speaks (http://www.autismspeaks.org)
Autism Speaks is an autism science and advocacy organization dedicated to funding research into the causes, prevention, treatments, and a cure for autism; increasing awareness of autism spectrum disorders; and advocating for the needs of individuals with autism and their families.
Division TEACCH (Treatment and Education of Autism and related Communication handicapped Children, University North Carolina at Chapel Hill) (www.teacch.com)
The TEACCH Web site includes information about their program, educational and communication approaches to teaching individuals with autism, their research and training opportunities, and information and resources on autism.
LDAA (Learning Disabilities Association of America) (http://www.ldanatl.org)
The LDAA site includes information and resources on many learning disabilities, including learning disabilities involving a significant social component, such as autism and Asperger syndrome.
OASIS (Online Asperger Syndrome Information and Support) (http://www.asperger.org)
General information on Asperger syndrome and related disorders, including resources and materials, announcements of major pertinent events and publications, and being the major “intersection” for communication among parents, clinicians, educators, and individuals with social disabilities
Yale Child Study Center (www.autism.fm)
Information on autism, Asperger syndrome, and related disorders, lists of resources organized by state, and parent support organizations and advocacy agencies.
Resources for Providers and Parents
29
Simonoff E, Pickles A, Charman T, Chandler S, Loucas T, Baird G. Psychiatric Disorders in Children With Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample, Journal of the American Academy of Child & Adolescent Psychiatry, 47 (8), 2008, 921-929.
Myers, SM, Plauche Johnson, C. Management of children with autism spectrum disorders. Pediatrics 120 (5), 2007, http://pediatrics.aappublications.org/content/120/5/1162#ref-162
Reichow B. & Volkmar, F.R. Social skills interventions for individuals with autism: evaluation for evidence-based practices within a best evidence synthesis framework. Autism Dev Disord (2010) 40: 149.
Volkmar F, Siegel M, Woodbury-Smith M, King B, McCracken J, State M and the AACAP Committee on Quality Issues. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Autism Spectrum Disorder. JAACAP, 53 (2) 2014.
References
30
Thank you!
Related Documents











