Alcoholism: new conception, old challenges Australian Doctors in Recovery Inaugural NZ Doctors in Recovery 18 March 2018 Doug Sellman Professor of Psychiatry & Addiction Medicine National Addiction Centre University of Otago, Christchurch

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Alcoholism
new conception
old challenges
Australian Doctors in Recovery
Inaugural NZ Doctors in Recovery
18 March 2018
Doug Sellman
Professor of Psychiatry amp Addiction Medicine
National Addiction Centre
University of Otago Christchurch
1 What is the new unitary diagnosis of
alcoholism
2 Is alcoholism a brain disease or a
learned habit
3 What is the best treatment advice to
give a person with alcoholism
4 How to reduce the incidence of
alcoholism in New Zealand
Four questions
Trunk and disorderly
Tipsy elephants staggering around South
African Kruger National Park intoxicated after eating
huge quantities of fermented marula fruit
High-volume alcohol-preferring rat
Inhabitants of forests in south-eastern Guinea enjoy rich alcoholic brew
fermented from sugary sap
Chimpanzees observed engaging in habitual drinking (Guardian 2015 quoting Royal Society Open Science)
Life canrsquot be enjoyed without alcohol
Social events arenrsquot proper events without alcohol
To be in the in-crowd means
drinking with the in-crowd
The New Zealand Way of Life
bull 25 of NZ drinkers are heavy drinkers (AUDIT)
bull Half of serious violent crimes relate to alcohol
bull An extraordinary proportion of presentations at Emergency Departments on Friday and Saturday nights are alcohol-related
bull Up to 3000 children born with FASD every year
bull 70000 alcohol-related physical and sexual assaults each year
bull A third of alcohol-related deaths are cancer
Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

1 What is the new unitary diagnosis of
alcoholism
2 Is alcoholism a brain disease or a
learned habit
3 What is the best treatment advice to
give a person with alcoholism
4 How to reduce the incidence of
alcoholism in New Zealand
Four questions
Trunk and disorderly
Tipsy elephants staggering around South
African Kruger National Park intoxicated after eating
huge quantities of fermented marula fruit
High-volume alcohol-preferring rat
Inhabitants of forests in south-eastern Guinea enjoy rich alcoholic brew
fermented from sugary sap
Chimpanzees observed engaging in habitual drinking (Guardian 2015 quoting Royal Society Open Science)
Life canrsquot be enjoyed without alcohol
Social events arenrsquot proper events without alcohol
To be in the in-crowd means
drinking with the in-crowd
The New Zealand Way of Life
bull 25 of NZ drinkers are heavy drinkers (AUDIT)
bull Half of serious violent crimes relate to alcohol
bull An extraordinary proportion of presentations at Emergency Departments on Friday and Saturday nights are alcohol-related
bull Up to 3000 children born with FASD every year
bull 70000 alcohol-related physical and sexual assaults each year
bull A third of alcohol-related deaths are cancer
Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Trunk and disorderly
Tipsy elephants staggering around South
African Kruger National Park intoxicated after eating
huge quantities of fermented marula fruit
High-volume alcohol-preferring rat
Inhabitants of forests in south-eastern Guinea enjoy rich alcoholic brew
fermented from sugary sap
Chimpanzees observed engaging in habitual drinking (Guardian 2015 quoting Royal Society Open Science)
Life canrsquot be enjoyed without alcohol
Social events arenrsquot proper events without alcohol
To be in the in-crowd means
drinking with the in-crowd
The New Zealand Way of Life
bull 25 of NZ drinkers are heavy drinkers (AUDIT)
bull Half of serious violent crimes relate to alcohol
bull An extraordinary proportion of presentations at Emergency Departments on Friday and Saturday nights are alcohol-related
bull Up to 3000 children born with FASD every year
bull 70000 alcohol-related physical and sexual assaults each year
bull A third of alcohol-related deaths are cancer
Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

High-volume alcohol-preferring rat
Inhabitants of forests in south-eastern Guinea enjoy rich alcoholic brew
fermented from sugary sap
Chimpanzees observed engaging in habitual drinking (Guardian 2015 quoting Royal Society Open Science)
Life canrsquot be enjoyed without alcohol
Social events arenrsquot proper events without alcohol
To be in the in-crowd means
drinking with the in-crowd
The New Zealand Way of Life
bull 25 of NZ drinkers are heavy drinkers (AUDIT)
bull Half of serious violent crimes relate to alcohol
bull An extraordinary proportion of presentations at Emergency Departments on Friday and Saturday nights are alcohol-related
bull Up to 3000 children born with FASD every year
bull 70000 alcohol-related physical and sexual assaults each year
bull A third of alcohol-related deaths are cancer
Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Inhabitants of forests in south-eastern Guinea enjoy rich alcoholic brew
fermented from sugary sap
Chimpanzees observed engaging in habitual drinking (Guardian 2015 quoting Royal Society Open Science)
Life canrsquot be enjoyed without alcohol
Social events arenrsquot proper events without alcohol
To be in the in-crowd means
drinking with the in-crowd
The New Zealand Way of Life
bull 25 of NZ drinkers are heavy drinkers (AUDIT)
bull Half of serious violent crimes relate to alcohol
bull An extraordinary proportion of presentations at Emergency Departments on Friday and Saturday nights are alcohol-related
bull Up to 3000 children born with FASD every year
bull 70000 alcohol-related physical and sexual assaults each year
bull A third of alcohol-related deaths are cancer
Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges
Life canrsquot be enjoyed without alcohol
Social events arenrsquot proper events without alcohol
To be in the in-crowd means
drinking with the in-crowd
The New Zealand Way of Life
bull 25 of NZ drinkers are heavy drinkers (AUDIT)
bull Half of serious violent crimes relate to alcohol
bull An extraordinary proportion of presentations at Emergency Departments on Friday and Saturday nights are alcohol-related
bull Up to 3000 children born with FASD every year
bull 70000 alcohol-related physical and sexual assaults each year
bull A third of alcohol-related deaths are cancer
Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Social events arenrsquot proper events without alcohol
To be in the in-crowd means
drinking with the in-crowd
The New Zealand Way of Life
bull 25 of NZ drinkers are heavy drinkers (AUDIT)
bull Half of serious violent crimes relate to alcohol
bull An extraordinary proportion of presentations at Emergency Departments on Friday and Saturday nights are alcohol-related
bull Up to 3000 children born with FASD every year
bull 70000 alcohol-related physical and sexual assaults each year
bull A third of alcohol-related deaths are cancer
Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

To be in the in-crowd means
drinking with the in-crowd
The New Zealand Way of Life
bull 25 of NZ drinkers are heavy drinkers (AUDIT)
bull Half of serious violent crimes relate to alcohol
bull An extraordinary proportion of presentations at Emergency Departments on Friday and Saturday nights are alcohol-related
bull Up to 3000 children born with FASD every year
bull 70000 alcohol-related physical and sexual assaults each year
bull A third of alcohol-related deaths are cancer
Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

The New Zealand Way of Life
bull 25 of NZ drinkers are heavy drinkers (AUDIT)
bull Half of serious violent crimes relate to alcohol
bull An extraordinary proportion of presentations at Emergency Departments on Friday and Saturday nights are alcohol-related
bull Up to 3000 children born with FASD every year
bull 70000 alcohol-related physical and sexual assaults each year
bull A third of alcohol-related deaths are cancer
Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Jordan is 39 years old married with two sons aged 12 and
10 and works night-shifts as a nurse He also owns and part-
runs a restaurant as well as renovating a house he and his
wife recently bought
He is currently ldquotaking a breakrdquo from his marriage following a
late night drunken altercation when out of frustration he
pushed his wife Sally who fell badly twisting her ankle
When Sally threatened to call the Police Jordan went and
stayed with a close friendcolleague for the night Sally took
out a non-molestation order out on him the next day Jordan
subsequently went and lived in their half-renovated house
Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Jordan first got drunk at age 10 and began drinking regularly on
Friday and Saturday nights at age 15 when he and friends
normally each drank six 750ml bottles (18 standard drinks) each
night He got into several fights had ldquoone or two blackoutsrdquo but
mainly recalls having a great time
His heaviest period of drinking was when he was in Australia in his
early 30s ndash about 10 sds five days a week
During that time he showed evidence of hazardous use
tolerance use despite interpersonal conflict and a lot of time
taken up with drinking
He is currently three months abstinent aiming to prove to his wife
he isnrsquot an alcoholic
Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Other Addiction History nil of note
Other Psychiatric History currently low in mood but still working
hard despite lowered motivation decreased enjoyment of life
and not feeling as sharp as usual
Family History heavy drinking family but no one diagnosed as
alcoholic
Personal History warm family upbringing felt loved did well at
school optimistic personality good marriage overall but two
strong personalities who often argue about trivialities even when
neither been drinking
MSE low mood evident but could raise a smile just no evidence
of cognitive impairment or any other psychiatric phenomenology
What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

What is Jordanrsquos alcohol diagnosis
What is the best advice to give
Jordan regarding his drinking
Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Sociopathic Personality
Disturbance
Alcoholism Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial PersonalityAntisocial Personality
Disorder
DSM1(1952)
DSM2 ICD 8(1968) (1969)
ICD9 DSM3 DSM3-R ICD10 DSMIV(1977) (1980) (1987) (1992) (1994)
Shifts in the diagnosis of alcoholism over the past 50 years
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges
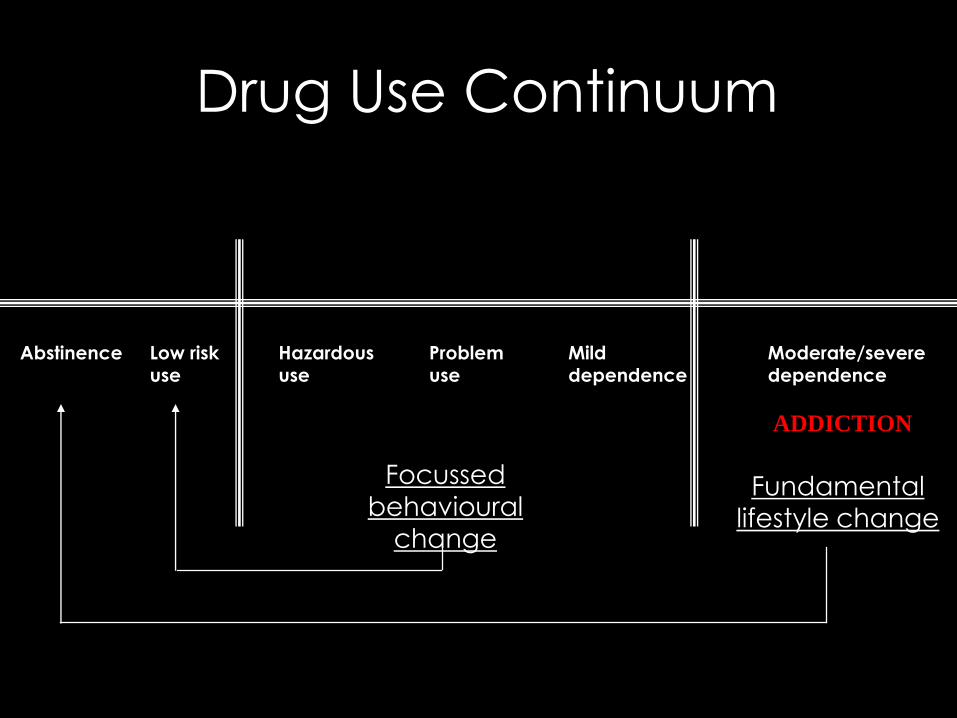
Drug Use Continuum
Abstinence Low risk Hazardous Problem Mild Moderatesevereuse use use dependence dependence
ADDICTION
Focussed
behavioural
change
Fundamental
lifestyle change
Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Shifts in the diagnosis of alcoholism over the past 60 years
DSM-I(1952)
DSM-II ICD8(1968) (1969)
ICD9 DSM-III DSM-IIIR ICD10 DSM-IV(1977) (1980) (1987) (1991) (1994)
DSM5(2013)
Sociopathic Personality Disturbance
Alcoholism
Alcohol Abuse
Alcohol Dependence
Antisocial Personality
Alcohol Use Disorder
Antisocial Personality
Disorder
Alcoholism
Antisocial Personality
Disorder
Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Drinking Continuum
No Low risk Hazardous Mild alcohol use Moderate Severe
drinking drinking drinking disorder (AUD) AUD AUD
ADDICTION
Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Proposed grouping of DSM-5 criteria for alcohol use disorder
based on severity weightings (Saha et al 2006)
DyscontrolUse is often longer than intended
Unsuccessful attempts to cut downstop
Use when physically hazardous
134
170
172
Physiological changes
Withdrawal evidence
Acquired tolerance
176
180
Compulsion to useCraving
Use despite physicalpsychological problems
Social and interpersonal problems
-
204
243
SalienceA lot of time spent
Neglect of roles
Activities given up
229
285
302
What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

What is Jordanrsquos alcohol diagnosis
At his heaviest period of use evidence of
bull dyscontrol (hazardous use)
bull physiological features (tolerance)
bull compulsion to use (use despite interpersonal
conflict)
bull salience (a lot of time taken up with drinking)
Diagnosis moderate alcohol use disorder
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges
What is the best advice to give
Jordan regarding his drinking
Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Mark and Linda Sobell (1995)
ldquoControlled drinking after 25 years
How important was the great debaterdquo
Sanchez-Craig et al (1984)
bull Mildly dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at two years
bull Majority of successful outcomes involved moderation
Foy et al (1984)
bull Severely dependent drinkers
bull Randomly assigned to abstinence or controlled drinking
bull No difference in outcome at five years
bull Majority of successful outcomes involved abstinence
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges
Suggested abstinence advice in relation to
severity of alcohol use disorder (DSM-5)
Sellman et al Aust N Z J Psychiatry 201448507-511
Copyright copy by The Royal Australian and New Zealand College of Psychiatrists
What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

What is the best advice to give
Jordan regarding his drinking
The best strategy is not to
give (unsolicited) advice
but rather
facilitate discovery
Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Alcoholism
Brain disease or learned habit
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges
Alcoholism Disease or Habit
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges
Brain Disease
(Volkov)
Learned Habit
(Lewis)
Caricature Person canrsquot help it
Person needs medical
treatment
Person simply chose it
Person can simply choose
not to be addicted
In practice Progressive brain changes
underlying disordered
behaviour
Medications and therapy can
assist a persons recovery
Normal learning processes
lead to changes in neural
pathways
Self-empowerment is critical
to a re-learning process of
moving on
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges
Behind every addiction is an industry pushing a moreish
engineered product
Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Behind every addiction there is an industry
scheming to make you and your children
one of their favourite customers for life
Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Alcohol No Ordinary Commodity
(2010)
5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

5+ Solution MPAAD+bull Marketing
bull Pricing
bull Accessibility
bull Age of purchase
bull Drink-driving
PLUS Increase treatment opportunities for heavy drinkers
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges
Five main reforms
1 End alcohol advertising and sponsorship
2 End ultra cheap alcohol
3 End anytime-anywhere alcohol
4 End teenage purchase of alcohol
5 End legal drunk driving
Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

Combination of effectiveness and public support of these reforms
Effectiveness Public Support(0 + ++ +++)
1 Dismantle marketing +++ 77 - 96
2 Raise the price +++ 76
3 Reduce trading hours ++ 84
4 Raise purchase age +++ 87
5 Lower drink driving limit +++ 65 - 75
The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

The Alcohol NON-Reform Bill
1 Marketing - some limited restriction of TINKERINGadvertising to minors only
2 Pricing NOTHING
3 Accessibility ndash no alcohol from convenience stores COULD YIELDamp voluntary local alcohol policies SOMETHING
4 Age of purchase ndash maintain 18 years for both on-licence NOTHINGand for off-licence
5 Drink driving limits NOTHING
British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

British American Tobacco NZ
1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges

1 The new unitary diagnosis of alcoholism is a return to the 1960s
2 ldquoAddiction interruptionrdquo using abstinence for a variable amount
of time depending on the severity of alcoholism is compatible
with both alcoholism conceived as a brain disease and as a
learned habit
3 The old challenge remains - working alongside a person with alcoholism and conducting individualised therapeutic
experiments together
4 The old challenge remains - advocating for effective alcohol
reform to reduce alcohol-related harm including the incidence of alcoholism when governments tend to place higher value on
Big Business than Public Health
Alcoholism New conception old challenges
Related Documents










