Australian bat lyssavirus infection in three fruit bats from north Queensland Rick Speare 1 , Lee Skerratt 1 , Robert Foster 2 , Lee Berger 1 , Peter Hooper 3 , Ross Lunt 3 , David Blair 4 , Dinah Hansman 5 , Mike Goulet 6 and Sandra Cooper 7 Abstract We report the case findings of Australian bat lyssavirus infection in two black flying foxes (Pteropus alecto ) and one little red flying fox (Pteropus scapulatus) from nor th Queensland between J anuary 1995 and August 1996. Although the P. alecto case in J anuary 1995 is the first recognised case of Australian bat lyssavirus infection in Australia, this was a retrospective diagnosis made after identification of the index case at Ballina in May 1996. E ight persons had exposure to the three bats. Serum antibodies to classical rabies virus were measured in six of these persons; the only one seropositive was a veterinarian who had previously been vaccinated against rabies. Six persons received rabies vaccine following exposure. None of the in-contact humans developed signs of lyssavirus infection. For people exposed to Australian bat lys- savirus-positive bats who have not been scratched or bitten or had mucosal contamination by these bats, we suggest a post-exposur e r egime of five inoculations of the human diploid cell inactivated rabies vaccine. Comm Dis Intell 1997;21:117-120. Introduction Lyssavirus infection was first diagnosed in two black flying foxes (Pteropus alecto) from Ballina, New South Wales in 1996 1,2 . Both bats exhibited neurological signs and had mild to severe encephalitis 2 . The lyssavirus isolated was found to be significantly different from known genotypes in the Lyssavirus genus 2 . In early November 1996, a bat carer from Rockhampton died from a diffuse encephalitis. Australian bat lyssavirus was detected in her cerebrospinal fluid by polymerase chain reaction and her serum contained neutralising antibodies to classical rabies virus 3 . The woman had cared Contents Australian bat lyssavirus infection in three fruit bats from north Queensland 117 Rick Speare, Lee Skerratt, Robert Foster, Lee Berger, Peter Hooper, Ross Lunt, David Blair, Dinah Hansman, Mike Goulet and Sandra Cooper Salmonella in Victoria, 1997: the story so far 120 Rosemary Lester, John Carnie, Lyn McLennan, Stephen Lambert, Helen Kelsall, Catherine Ferreira, Joy Gregory, Bronwen Harries and Graham Rouch Communicable Diseases Surveillance 123 Overseas Briefs 132 ISSN 0725-3141 Volume 21 Number 9 1 May 1997 1. Department of Public Health and Tropical Medicine, James Cook University, Townsville, Queensland 4811. 2. Department of Biomedical and Tropical Veterinary Science, James Cook University, Queensland and Department of Pathobiology, University of Guelph, Ontario Canada. 3. CSIRO Australian Animal Health Laboratory, Geelong, Victoria. 4. Department of Zoology and Tropical Ecology, James Cook University, Queensland. 5. Department of Tropical Plant Science, James Cook University, Queensland. 6. Bayside Veterinary Clinic, Townsville, Queensland. 7. Charters Towers, Queensland.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Australian bat lyssavirus infectionin three fruit bats from north
QueenslandRick Speare1, Lee Skerratt1, Robert Foster2, Lee Berger1, Peter Hooper3, Ross Lunt3, David
Blair4, Dinah Hansman5, Mike Goulet6 and Sandra Cooper7
AbstractWe report the case findings of Australian bat lyssavirus infection in two black flying foxes(Pteropus alecto) and one little red flying fox (Pteropus scapulatus) from north Queenslandbetween January 1995 and August 1996. Although the P. alecto case in January 1995 is the firstrecognised case of Australian bat lyssavirus infection in Australia, this was a retrospectivediagnosis made after identification of the index case at Ballina in May 1996. Eight persons hadexposure to the three bats. Serum antibodies to classical rabies virus were measured in six ofthese persons; the only one seropositive was a veterinarian who had previously been vaccinatedagainst rabies. Six persons received rabies vaccine following exposure. None of the in-contacthumans developed signs of lyssavirus infection. For people exposed to Australian bat lys-savirus-positive bats who have not been scratched or bitten or had mucosal contamination bythese bats, we suggest a post-exposure regime of five inoculations of the human diploid cellinactivated rabies vaccine. Comm Dis Intell 1997;21:117-120.
IntroductionLyssavirus infection was firstdiagnosed in two black flyingfoxes (Pteropus alecto) fromBallina, New South Wales in19961,2. Both bats exhibitedneurological signs and had mild
to severe encephalitis2. Thelyssavirus isolated was found tobe significantly different fromknown genotypes in theLyssavirus genus2.
In early November 1996, a batcarer from Rockhampton died
from a diffuse encephalitis.Australian bat lyssavirus wasdetected in her cerebrospinalfluid by polymerase chainreaction and her serumcontained neutralisingantibodies to classical rabiesvirus3. The woman had cared
ContentsAustralian bat lyssavirus infection in three fruit bats from north Queensland 117
Rick Speare, Lee Skerratt, Robert Foster, Lee Berger, Peter Hooper, Ross Lunt, David Blair, Dinah Hansman, Mike Goulet and Sandra Cooper
Salmonella in Victoria, 1997: the story so far 120
Rosemary Lester, John Carnie, Lyn McLennan, Stephen Lambert, Helen Kelsall, Catherine Ferreira, Joy Gregory, Bronwen Harries and Graham Rouch
Communicable Diseases Surveillance 123
Overseas Briefs 132
ISSN 0725-3141Volume 21Number 91 May 1997
1. Department of Public Health and Tropical Medicine, James Cook University, Townsville, Queensland 4811.
2. Department of Biomedical and Tropical Veterinary Science, James Cook University, Queensland and Departmentof Pathobiology, University of Guelph, Ontario Canada.
3. CSIRO Australian Animal Health Laboratory, Geelong, Victoria.
4. Department of Zoology and Tropical Ecology, James Cook University, Queensland.
5. Department of Tropical Plant Science, James Cook University, Queensland.
6. Bayside Veterinary Clinic, Townsville, Queensland.
7. Charters Towers, Queensland.
for fruit bats in the two to four weekspreceding her illness and had beenscratched by them. She had alsocared for an insectivorous bat sixweeks prior to the onset of clinicalsigns and received a bite from thebat. The woman had also cared for avariety of native animals in the recentpast.
We report three cases of fruit batsinfected with Australian batlyssavirus, and describe the publichealth actions associated with them.
Bat infectionsCase 1 occurred in January 1995 andwas an adult wild female black flyingfox (P. alecto) found behavingaggressively in the back yard of ahouse in Townsville. Intracytoplasmiceosinophilic inclusions in neuroneswere detected in histological sectionsof brain. The bat also had histologicaland biochemical evidence of leadtoxicosis.
Case 2 occurred in May 1996 andwas an adult wild male black flying
fox (P. alecto) with hind limb paresis,found under a tree in ChartersTowers. The brain appearedhistologically normal, but changes inother organs indicated a bacterialsepticaemia.
Case 3 was a little red flying fox(Pteropus scapulatus) found inAugust 1996, with hind limb paresisand clonic muscle spasm, in asuburban garden in Townsville. Anon-suppurative meningoencephalitiswas present on histology.
Person Date ofexposure
Date ofvaccination
Vaccinationregime
Delay1 Comments
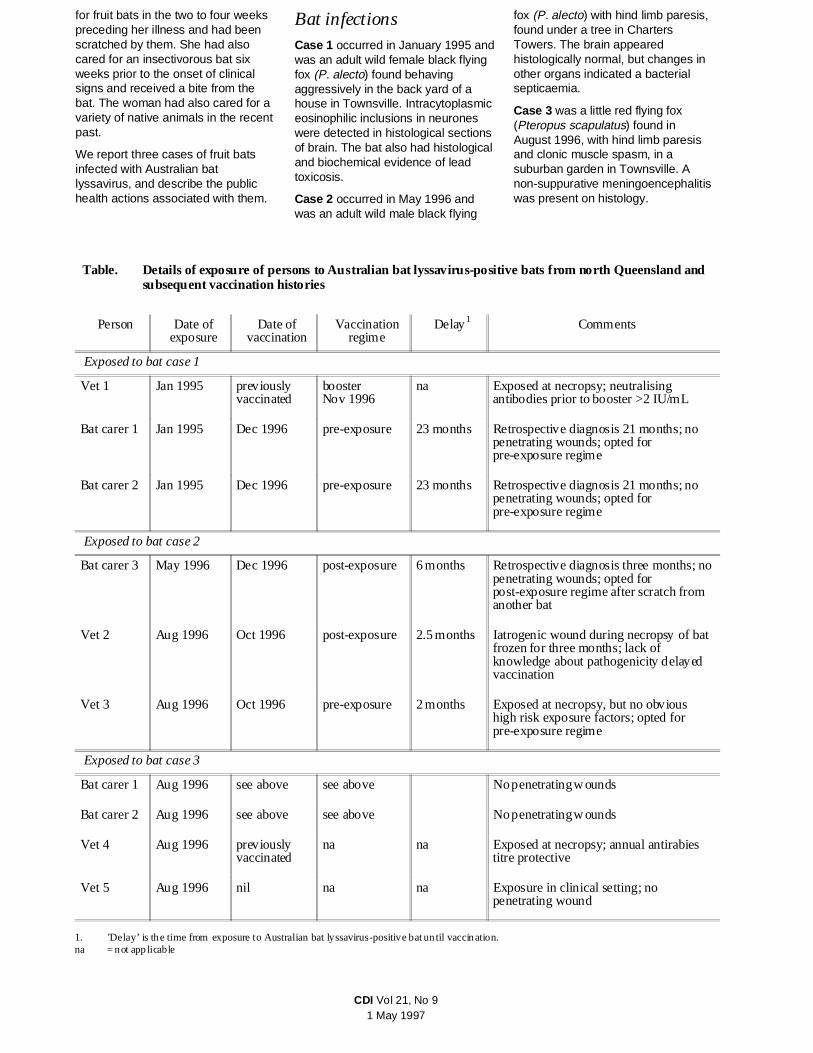
Exposed to bat case 1
Vet 1 Jan 1995 previouslyvaccinated
booster Nov 1996
na Exposed at necropsy; neutralisingantibodies prior to booster >2 IU/mL
Bat carer 1 Jan 1995 Dec 1996 pre-exposure 23 months Retrospective diagnosis 21 months; nopenetrating wounds; opted forpre-exposure regime
Bat carer 2 Jan 1995 Dec 1996 pre-exposure 23 months Retrospective diagnosis 21 months; nopenetrating wounds; opted forpre-exposure regime
Exposed to bat case 2
Bat carer 3 May 1996 Dec 1996 post-exposure 6 months Retrospective diagnosis three months; nopenetrating wounds; opted forpost-exposure regime after scratch fromanother bat
Vet 2 Aug 1996 Oct 1996 post-exposure 2.5 months Iatrogenic wound during necropsy of batfrozen for three months; lack ofknowledge about pathogenicity delayedvaccination
Vet 3 Aug 1996 Oct 1996 pre-exposure 2 months Exposed at necropsy, but no obvioushigh risk exposure factors; opted forpre-exposure regime
Exposed to bat case 3
Bat carer 1 Aug 1996 see above see above No penetrating wounds
Bat carer 2 Aug 1996 see above see above No penetrating wounds
Vet 4 Aug 1996 previouslyvaccinated
na na Exposed at necropsy; annual antirabiestitre protective
Vet 5 Aug 1996 nil na na Exposure in clinical setting; nopenetrating wound
1. ’Delay’ is the time from exposure to Australian bat lyssavirus-positive bat until vaccination.na = not applicable
Table. Details of exposure of persons to Australian bat lyssavirus-positive bats from north Queensland andsubsequent vaccination histories
CDI Vol 21, No 91 May 1997

For all cases, samples of brain storedat -70°C were submitted to theCSIRO Australian Animal HealthLaboratory (AAHL). Brain impressionsmears stained strongly for lyssaviruson the immunofluorescent antibodytest (IFAT), and Australian batlyssavirus was isolated.
Human contactsAt least eight people had closecontact with the three fruit bats(Table). These included three batcarers and five veterinarians, four ofwhom performed post-mortemexaminations on the bats. Time fromcontact with a particular bat toknowledge of the infection status ofthe bat ranged from two weeks to 21months. None of the carers hadsustained obvious penetratingwounds or scratches. Oneveterinarian (Vet 2) had cut a fingerwith a scalpel blade during thenecropsy.
Neutralising antibodies to classicalrabies virus were measured at AAHLfor six of the eight persons afterexposure. One veterinarian (Vet 4)had been vaccinated against rabiesvirus in 1989 and since then had hadannual confirmation of a protectiveantirabies antibody titre. His antibodystatus was not measured on thisoccasion. Five of the six personstested were negative, while oneveterinarian (Vet 1) was stronglypositive with a level >2.0 IU/mL. Hehad received a full course of threedoses of human diploid cell rabiesvaccine in 1985, with three additionalboosters, the last in 1987, and theantibody response was considered tobe due to vaccination. Theveterinarian (Vet 2) who had been cutduring the post-mortem had receivedno rabies vaccinations and had anegative titre against rabies virus tenweeks after the event.
Vet 2 received a post-exposurevaccination regime of fiveinoculations of human diploid cellinactivated rabies vaccinecommencing two and a half monthsafter the injury, while Vet 3 whoassisted in the necropsy received athree-inoculation regime. Bat carer 3received a standard five-inoculationpost-exposure regime six monthsafter caring for Case 2 after she wasscratched by another bat withneurological signs. The latter bat wasAustralian bat lyssavirus-negative,but the regime was started before
infection status was known. The othertwo carers received a three-doseregime 23 months after interactingwith Case 1. These carers were alsoexposed to Case 3. A veterinarianwho had clinical contact with Case 3and had no antibodies to rabies virushas not received any rabiesinoculations to date, six months afterexposure. None of the humancontacts of these bats has shownclinical signs of encephalomyelitis.
DiscussionBat infections
Neurological signs were present in allthree fruit bats from northQueensland infected with Australianbat lyssavirus. Fruit bats will exhibitaggressive behaviour in specifictypes of social interactions, but theaggression shown by Case 1 wasexcessive. Cases 2 and 3 had hindlimb paresis and showed noaggression. The signs of lyssavirusdisease in these cases are similar tothose seen in classical rabies cases4.Paralysis was seen in two of ourcases and paralytic rabies is a morecommon presentation than furiousrabies in most species4.
Case 1 predates the Australian batlyssavirus infections in the blackflying foxes from Ballina, the earliestof which was in March 19952.Currently Case 1 is therefore the firstknown Australian bat lyssavirusinfection in Australia.
Neither of the black flying foxes (P.alecto) from north Queensland(Cases 1 and 2) had an encephalitis,although brain smears from bothreacted strongly to the IFAT forlyssavirus antigen. Case 1 hadhistological and biochemical signs oflead toxicosis, while Case 2 had aterminal septicaemia in addition to theAustralian bat lyssavirus infection.Both of these cases illustrate thatother diagnoses with the potential tocause neurological signs do notexclude the possibility of infectionwith Australian bat lyssavirus.
The occurrence of Australian batlyssavirus infection in Case 3, thelittle red flying fox (P. scapulatus), isthe first report of Australian batlyssavirus in this species. The littlered flying fox (Case 3) had anencephalitis similar to that of theblack flying foxes (P. alecto) fromBallina, and it is thus the third reportof a fruit bat in Australia with
encephalitis caused by Australian batlyssavirus.
Sick and dead bats that arepresented to veterinarians inTownsville are now routinelynecropsied, and specimens are sentto AAHL for testing for lyssavirusinfection. Bat carer coordinators fromTownsville report that in the past twoyears they have seen three other fruitbats which have exhibited abnormalaggressive behaviour prior to death.Two of these flying foxes chased andattacked other flying foxes. One ofthese aggressive flying foxes wasseen at the same release cage asCase 1 and may have been bitten byCase 1 five weeks previously.Necropsies were not performed onthese aggressive bats.
Human contacts
Two of the people who had contactwith the three Australian batlyssavirus infected bats received apost-exposure vaccination regime forrabies using the five-inoculationregime. Three of the remaining sixchose to receive the three-inoculationpre-exposure regime, due to the lackof any penetrating wounds. Thisvariation in management of humansexposed to lyssavirus-positive batsmay reflect the lack of informationavailable prior to the November 1996guidelines of the Lyssavirus ExpertGroup. Two veterinarians had alreadybeen fully immunised against rabies,and both had protective levels ofantibody.
The delays between potentialexposure to Australian bat lyssavirusand post-exposure vaccination weredue to several factors. Lyssavirusinfection in two fruit bats wasretrospectively diagnosed on archivedspecimens, leading to a delay indiscovering the infection status of thebats. Lack of knowledge byindividuals about the potential ofAustralian bat lyssavirus to causedisease in humans or animals otherthan bats resulted in poor motivationto seek vaccination. Results frompathogenicity studies on the Ballinaisolate at the Centers for DiseaseControl and Prevention were notavailable until early November 1996,and the death of a human occurredafter the cases described here. Priorto the meeting of the LyssavirusExpert Group in November 19965,protocols concerning actions to betaken after exposure to Australian batlyssavirus were not defined.
CDI Vol 21, No 91 May 1997

The Lyssavirus Expert Group notedthat inapparent exposure tolyssavirus could occur6. The currentguidelines do not offer any definiteadvice for people who have beenexposed to a lyssavirus-positive bat,but who are not aware of receivingany penetrating wound orcontamination of mucous membraneswith secretions5. We suggest thatsuch persons should receive thestandard five-inoculation
post-exposure regime using killedhuman diploid cell rabies vaccine.
References1. Crerar S, Longbottom H, Rooney J,
Thornber P. Human health aspects ofa possible lyssavirus in a black flyingfox. Comm Dis Intell 1996;20:325.
2. Fraser GC, Hooper PT, Lunt, RA et al.Encephalitis caused by a lyssavirus infruit bats in Australia. Emerg Infect Dis1996;2:327-331.
3. Allworth A, Murray K, Morgan J. Ahuman case of encephalitis due to alyssavirus recently identified in fruitbats. Comm Dis Intell 1996;20:504.
4. Geering WA, Forman AJ, Nunn MJ.Exotic diseases of animals: a fieldguide for Australian veterinarians.Canberra: Australian GovernmentPublishing Service, 1995.
5. Lyssavirus Expert Group. Preventionof human lyssavirus infection. CommDis Intell 1996;20:505-507.
6. Update on bat lyssavirus. Comm DisIntell 1996;20:535.
Salmonella in Victoria, 1997: the story so far
Rosemary Lester1, John Carnie1, Lyn McLennan1, Stephen Lambert2, Helen Kelsall1, Catherine Ferreira1, Joy Gregory1, Bronwen Harries3 and Graham Rouch4
AbstractThe Infectious Diseases Unit of the Department of Human Services, Victoria, reported an increased incidenceof Salmonella infections in early 1997. To 21 April 1997, 944 notifications had been received, passing theprevious year’s total of 915. Five outbreaks of five separate serovars have been investigated and traced to theirsources. The outbreaks, their sources and the control measures undertaken are described. Further clusters ofother Salmonella serovars are being investigated. Comm Dis Intell 1997;21:120-122.
IntroductionThe number of notified cases ofSalmonella infections in Victoria hasvaried between 712 and 1,062 in theyears 1991 to 1996. Notification ratesper 100,000 population have been23.7, 21.7 and 20.4 for 1994, 1995and 1996 respectively. Notificationrates to the National SalmonellaSurveillance Scheme for the samethree years were 21.7, 19.7 and 18.1per 100,000 population. TheAustralian average notification rate in1996 was 31.0 per 100,000population.
To 21 April 1997, 944 notifications ofSalmonella had been received inVictoria, passing the previous year’stotal of 915. A number of clusterswere investigated.
Notable outbreaks which have beentraced to a source in the past haveincluded 47 cases of SalmonellaTyphimurium 135 in 1991 associatedwith Italian-style ice cream (usinguncooked eggs), and 54 cases ofSalmonella Mbandaka in 1996associated with peanut butter.
In late 1996, there was an outbreak of36 cases of Salmonella TyphimuriumRDNC A015 traced to a cafe in anouter suburban shopping centre. Theimplicated food in this outbreak wasmayonnaise, which was made on thepremises using raw eggs.
MethodsInvestigations of Salmonella clustersbegin with a weekly review of allnotifications, including Salmonella,compared with historical data. Once itis identified that there is a cluster of
cases of the same serovar, anoutbreak investigation is commenced.A standard questionnaire isadministered by telephone to allnotified cases in the cluster by staff ofthe Infectious Diseases Unit of theDepartment of Human Services. Thequestionnaire asks about theperson’s food history in the threedays prior to becoming ill, and aboutfoods consumed as part of theirroutine diet. Premises nominated bycases where foods have beenpurchased are also recorded. Thedata are constantly reviewed forpossible links, and food samplingeither from cases’ homes or fromnominated premises is undertaken asappropriate.
CDI Vol 21, No 91 May 1997
1. Infectious Diseases Unit, Department of Human Services, 115 Victoria Parade, Fitzroy Victoria 3065.
2. Master of Applied Epidemiology Program, National Centre for Epidemiology and Population Health, Australian National University, Canberra.
3. Food and Water Unit, Department of Human Services, Victoria.
4. Chief Health Officer, Department of Human Services, Victoria.

Outbreaks in 1997Salmonella Muenchen
Twenty-four cases of SalmonellaMuenchen were notified to theDepartment of Human Services frommid-February to mid-March 1997.This is a relatively uncommonserovar, with three to seven casesnotified per year in recent years.Dates of onset of illness varied from21 January to 30 March 1997. Wewere also notified that seven caseshad been reported in South Australia.
The ages of cases ranged from oneyear to 95 years. There wererelatively few young children notifiedcompared with the notification ratesfor all Salmonella. There were twodeaths associated with this outbreak:a 79 year old male and an 86 year oldfemale.
In their food histories, three casesmentioned a retail butcher in thenorthern suburbs of Melbourne.Among samples obtained from thisbutcher, sliced corned beef waspositive for Salmonella Muenchen.The source of the corned beef was asmallgoods manufacturer in thenorthern suburbs. This supplier soldproducts directly from a retail shop,as well as distributing products todelicatessens and smallsupermarkets. A few customers thensold products to other outlets.Extensive samples andenvironmental swabs were obtainedfrom the smallgoods supplier and adistribution list for outlets wasobtained.
Of the 24 cases, 22 mentioned hamand/or corned beef either in theirspecific three day food history, or inthe list of foods generally eaten. Ofthese, 15 cases were shown to havepurchased sliced meats frompremises on the distribution list.Samples and swabs from thesmallgoods supplier were negative.However, the epidemiologicalevidence was such that a recall of theimplicated product was considerednecessary. A voluntary recall ofcorned beef and two types of ham,with a public announcement todiscard these products if the sourcewas unknown, was undertaken on 21March 1997. Preparation of theseproducts involved handling andrepackaging after cooking, andtherefore provided the potential forpost-cooking contamination.
Since the recall, SalmonellaMuenchen has also been isolatedfrom unopened packages of cornedbeef from the factory, both in Victoriaand South Australia.
Salmonella Typhimurium 1
On 23 March 1997, the Departmentof Human Services was notified oflarge numbers of patients seekingtreatment for gastroenteritis at twohospitals in the south-easternsuburbs of Melbourne. Many caseshad eaten Vietnamese pork rolls froma particular hot bread shop in thearea.
The Department of Human Servicesreceived 808 reports. Of these, 598were reported from hospitalemergency departments, and 79cases required hospitalisation. To 21April 1997, 415 isolations ofSalmonella Typhimurium 1 had beenofficially notified to the departmentsince the weekend of the outbreak.No deaths were reported inconjunction with this outbreak.
The hot bread shop identified as thesource was closed on the evening ofthe day on which the outbreak wasnotified, and remains closedindefinitely. Seven hundred andseventy-four of the cases had adefinite association with eatingVietnamese rolls. Three otherpremises which sold the rolls from thehot bread shop had cases associatedwith them.
Salmonella Anatum
Nineteen cases of SalmonellaAnatum were notified to theDepartment of Human Services inMarch 1997. The age range of thecases was one to 74 years. Caseswere scattered through the suburbsof Melbourne, and four cases werefrom two towns in north-easternVictoria. None of the cases requiredhospitalisation, although one caseacquired her infection while inhospital for an unrelated complaint.Dates of onset varied from 1February to 13 March. Seventeen ofthe 19 cases mentioned consumptionof ham in their specific three day foodhistory; all 19 reported consumptionof ham in their routine diet. Fourteenof the 19 also mentionedconsumption of corned beef.Sampling of smallgoods from adelicatessen nominated by three ofthe cases revealed SalmonellaAnatum in unopened corned beef andtwo types of ham. A recall of the
affected products was commencedon 2 April.
Six further cases have been notifiedsince the recall was announced.Dates of onset are available for fourof these cases; all were prior to theannouncement of the recall.
Salmonella Chester
Five cases of Salmonella Chesterinfection occurred in the southernbayside suburbs of Melbourne inFebruary - March 1997. One caserequired hospitalisation. Four of thefive cases revealed a link with adelicatessen in a large localsupermarket. The delicatessen wasclosed for cleaning and sanitising.Food and environmental samples andfaecal specimens from staff werecollected. Two further cases havebeen notified since the secondcluster, but neither has links with thedelicatessen.
Investigations into this outbreak arecontinuing and the delicatessenremains closed. A more completedescription of this outbreak will bereported separately.
Salmonella Typhimurium 43
Seven cases of this serovar occurredin March 1997, with three of thecases being from one family. Theseventh case was a notification fromthe State coroner. The organism wasisolated from the bowel of a 27 yearold man at post mortem. This manhad a four day history of moderategastroenteritis. He had visited hisgeneral practitioner on two occasionsin the several days prior to beingfound dead at home. The cause ofdeath as reported by the coroner wasindeterminate, as there was noevidence that the Salmonellainfection was the cause.
Five of the cases had a definitehistory of having eaten at aVietnamese/Chinese restaurant in thesouth-eastern suburbs of Melbourne.The deceased man had recently beenemployed at a fish shop two doorsaway from this restaurant. Theowners of the fish shop used toregularly order food for theiremployees, or send them to thisrestaurant for lunch. No one coulddefinitely confirm whether this manhad eaten food from the restaurantbefore becoming ill, but this seemslikely to have occurred. The seventhcase reported no association with therestaurant. The shop was closed for
CDI Vol 21, No 91 May 1997

cleaning and sanitising, and faecaltests on staff were carried out.
ConclusionsDetailed investigation of Salmonellaclusters by a team of public healthofficers has shown that successfulresults can be obtained, even whenthe source of an outbreak is anunlabelled, distributed product, aswas the case with the two outbreaksinvolving smallgoods. The time takento find the source in these twooutbreaks contrasts with the ease offinding a cause in the case of a pointsource outbreak with a very highattack rate.
The high incidence of Salmonella inVictoria in 1997 may be due to ahigher load of organisms beingpresent in meat coming fromabattoirs. This has been combinedwith gross errors of food handling insome cases, and minor errors inothers. Undoubtedly, mishandling byconsumers has also contributed to
the increased incidence. The majorityof these outbreaks occurred duringand shortly after the hottest summerever recorded in Melbourne.
The high success rate in tracking thesources of outbreaks, and theassociated publicity, probably led tomore testing and more reporting ofoutbreaks which may previously havegone unreported. A lowered thresholdof suspicion has led to investigationof small clusters with successfulresults, as with SalmonellaTyphimurium 43. All such successesadd to our knowledge of theepidemiology of this type offood-borne disease, and add toprospects for prevention.
AcknowledgmentsWe wish to thank Geoff Hogg, AgnesTan, Diane Lightfoot and all the staffof the Microbiological Diagnostic Unitfor their enormous contribution tothese investigations. The volume ofwork undertaken, and the advicefreely given at all hours, has beenmuch appreciated by the Departmentof Human Services team. Similarly,the work of Tony Harrison and thedepartment’s Food and Water Unithas been greatly valued. The supportof the senior management of thePublic Health Branch, especiallyGeoff Lavender and William Hart, hasbeen invaluable. The rapid andprofessional response provided byregional environmental health officersand local government teams involvedin these outbreaks has made the taskmuch easier. Finally, thanks go tothose hospitals and generalpractitioners who have been diligentin notifying us promptly, and forproviding follow-up information whererequested.
CDI Vol 21, No 91 May 1997

Communicable Diseases SurveillanceMeningococcal infectionNeisseria meningitidis is the most common cause ofbacterial meningitis in Australia. Between 5% and 10% ofthe population asymptomatically carry Neisseriameningitidis in the nasopharynx. In a small proportion ofthese individuals infection progresses to an acute invasivedisease such as septicaemia, meningitis or pneumonia.
Neisseria meningitidis is spread by direct contact with aninfected person through respiratory droplets from the noseand throat. The incubation period is 3 to 4 days.Symptoms and signs may include fever, headache,nausea, stiff neck and petechial rash.
There are 13 different serogroups of Neisseriameningitidis. Of these, three, serogroups A, B and C,account for 90% of invasive infections. While serogroup Aorganisms are rarely isolated in Australia, outbreaks havebeen reported in Aboriginal communities in centralAustralia. Serogroup B organisms account for most casesof sporadic disease in Australia. However the isolation ofserogroup C organisms has increased in recent years.
From 1994 to 1996 the Australian MeningococcalSurveillance Program of the National Neisseria Networktested 750 islolates of Neisseria meningitidis associatedwith invasive disease. Of these, approximately 95% wereserogroups B and C. Serogroup B predominated nationallyand in most States and Territories, with the exception of1994 when serogroup C was more prominent in NewSouth Wales, Tasmania and South Australia. Group Cwas also more prevalent in the Northern Territory in 1994and 1995.
Vaccines containing groups A, C, Y and W135 areavailable in Australia, and can be used in the control ofoutbreaks due to these serogroups. However, they do notprotect against the more commonly isolated group Borganisms. Outbreaks of any serogroup can be controlledby the prophylactic use of rifampicin or other suitableantibiotics. These reduce or eliminate the carriage of theorganism in the nasopharynx. Close contacts, includinghousehold contacts, those in nurseries and those exposedto oral secretions (for example, by kissing) should receivechemoprophylaxis.
Meningococcal infection is a notifiable disease in all Statesand Territories. The notification rate recorded by theNational Notifiable Diseases Surveillance Scheme rosefrom 1.6 cases per 100,000 population in 1991 to 2.1 per100,000 population in 1995. The number of reports hasrisen in recent months but remains similar to previousyears (Figure 1). Meningococcal infection is mostcommonly reported for those in the 0 - 4 years age group,with a further peak for those aged 15 - 24 years (Figure 2).
National Notifiable DiseasesSurveillance SystemThe NNDSS is conducted under the auspices of theCommunicable Diseases Network Australia New Zealand.The system coordinates the national surveillance of morethan 40 communicable diseases or disease groupsendorsed by the National Health and Medical ResearchCouncil (NHMRC). Notifications of these diseases aremade to State and Territory health authorities under theprovisions of their respective public health legislations.De-identified core unit data are supplied fortnightly forcollation, analysis and dissemination. For furtherinformation, see CDI 1997;21:5.
0
10
20
30
40
50
60
70
80
Jan1993
Jul Jan1994
Jul Jan1995
Jul Jan1996
Jul Jan1997
Not
ifica
tions
Figure 1. Notifications of meningococcal infection,1993 to 1995, by month of onset
0
10
20
30
40
50
60
70
80
90
100
0-4 10-14 20-24 30-34 40-44 50-54 60-64 70-74 >80
Age group
Not
ifica
tions
FemaleMale
Figure 2. Notifications of meningococcal infection,1996, by age group and sex
CDI Vol 21, No 91 May 1997
NN Not Notifiable.
1. No notifications of poliomyelitis have been reported since 1986.
2. Totals comprise data from all States and Territories. Cumulativefigures are subject to retrospective revision, so there may bediscrepancies between the number of new notifications and the increment in the cumulative figure from the previous period.
Disease1,2 ACT NSW NT Qld SA Tas Vic WA
Thisperiod1997
Thisperiod1996
Year todate1997
Year todate1996
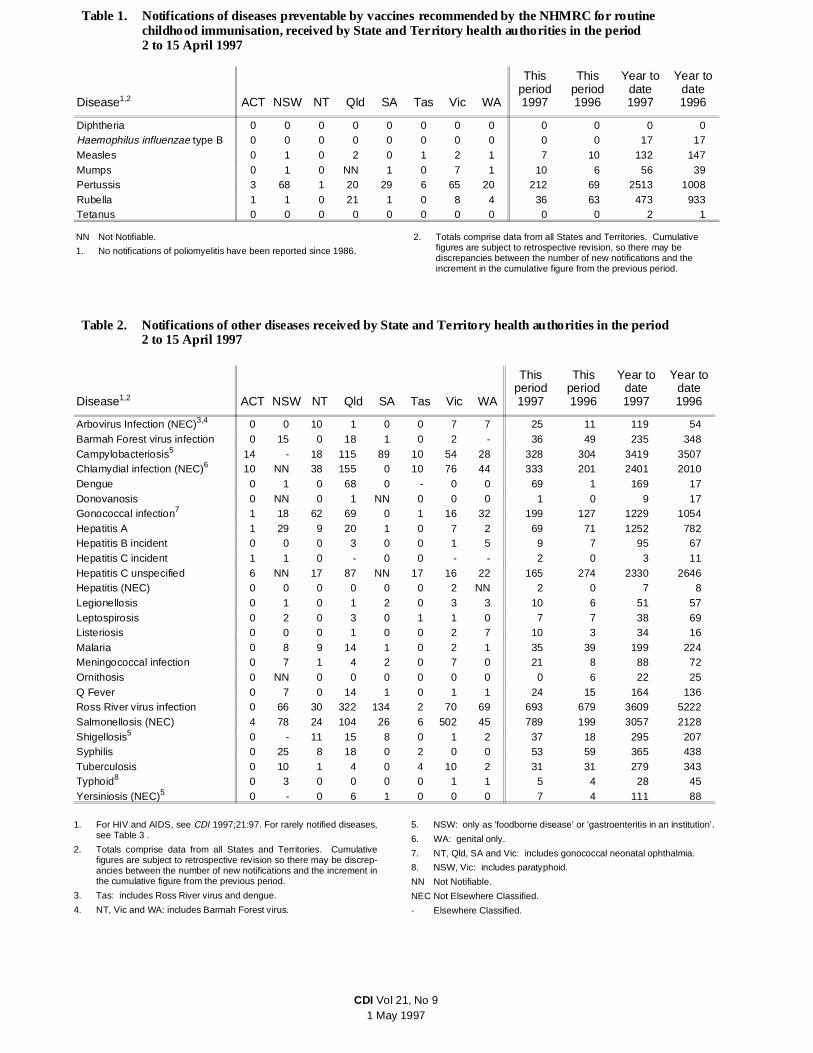
Diphtheria 0 0 0 0 0 0 0 0 0 0 0 0Haemophilus influenzae type B 0 0 0 0 0 0 0 0 0 0 17 17Measles 0 1 0 2 0 1 2 1 7 10 132 147Mumps 0 1 0 NN 1 0 7 1 10 6 56 39Pertussis 3 68 1 20 29 6 65 20 212 69 2513 1008Rubella 1 1 0 21 1 0 8 4 36 63 473 933Tetanus 0 0 0 0 0 0 0 0 0 0 2 1
Table 1. Notifications of diseases preventable by vaccines recommended by the NHMRC for routinechildhood immunisation, received by State and Ter ritory health authorities in the period2 to 15 April 1997
Disease1,2 ACT NSW NT Qld SA Tas Vic WA
Thisperiod1997
Thisperiod1996
Year todate1997
Year todate1996
Arbovirus Infection (NEC)3,4 0 0 10 1 0 0 7 7 25 11 119 54Barmah Forest virus infection 0 15 0 18 1 0 2 - 36 49 235 348Campylobacteriosis5 14 - 18 115 89 10 54 28 328 304 3419 3507Chlamydial infection (NEC)6 10 NN 38 155 0 10 76 44 333 201 2401 2010Dengue 0 1 0 68 0 - 0 0 69 1 169 17Donovanosis 0 NN 0 1 NN 0 0 0 1 0 9 17Gonococcal infection7 1 18 62 69 0 1 16 32 199 127 1229 1054Hepatitis A 1 29 9 20 1 0 7 2 69 71 1252 782Hepatitis B incident 0 0 0 3 0 0 1 5 9 7 95 67Hepatitis C incident 1 1 0 - 0 0 - - 2 0 3 11Hepatitis C unspecified 6 NN 17 87 NN 17 16 22 165 274 2330 2646Hepatitis (NEC) 0 0 0 0 0 0 2 NN 2 0 7 8Legionellosis 0 1 0 1 2 0 3 3 10 6 51 57Leptospirosis 0 2 0 3 0 1 1 0 7 7 38 69Listeriosis 0 0 0 1 0 0 2 7 10 3 34 16Malaria 0 8 9 14 1 0 2 1 35 39 199 224Meningococcal infection 0 7 1 4 2 0 7 0 21 8 88 72Ornithosis 0 NN 0 0 0 0 0 0 0 6 22 25Q Fever 0 7 0 14 1 0 1 1 24 15 164 136Ross River virus infection 0 66 30 322 134 2 70 69 693 679 3609 5222Salmonellosis (NEC) 4 78 24 104 26 6 502 45 789 199 3057 2128Shigellosis5 0 - 11 15 8 0 1 2 37 18 295 207Syphilis 0 25 8 18 0 2 0 0 53 59 365 438Tuberculosis 0 10 1 4 0 4 10 2 31 31 279 343Typhoid8 0 3 0 0 0 0 1 1 5 4 28 45Yersiniosis (NEC)5 0 - 0 6 1 0 0 0 7 4 111 88
Table 2. Notifications of other diseases received by State and Territory health authorities in the period2 to 15 April 1997
1. For HIV and AIDS, see CDI 1997;21:97. For rarely notified diseases,see Table 3 .
2. Totals comprise data from all States and Territories. Cumulativefigures are subject to retrospective revision so there may be discrep-ancies between the number of new notifications and the increment inthe cumulative figure from the previous period.
3. Tas: includes Ross River virus and dengue.
4. NT, Vic and WA: includes Barmah Forest virus.
5. NSW: only as ’foodborne disease’ or ’gastroenteritis in an institution’.6. WA: genital only.
7. NT, Qld, SA and Vic: includes gonococcal neonatal ophthalmia.
8. NSW, Vic: includes paratyphoid.
NN Not Notifiable.
NEC Not Elsewhere Classified.
- Elsewhere Classified.
CDI Vol 21, No 91 May 1997

Reporting period 2 to 15 April 1997
There were 3,413 notifications received for this two-weekperiod (Tables 1, 2 and 3). The numbers of reports forselected diseases have been compared with average datafor corresponding periods in the previous three years(Figure 3).
Reports of Ross River virus infection continued to rise,with 693 notifications received this period. The majority ofnotifications were from Queensland (322) and SouthAustralia (134). Fifty per cent of reports were for the 25 -44 years age range. The total numbers received for thisyear are still below the levels reported for the same periodin 1996.
Notifications of salmonellosis have increased markedly inrecent weeks and reports received so far in 1997 are
abovethenumbersforth
e same period in 1996. The highest number of cases forthis period was reported from Victoria (502), with themajority having dates of onset during March. Recentoutbreaks detected in Victoria (see page 120) havecontributed to the high number of notifications.
Thirty-seven reports of shigellosis were received thisperiod. The number of notifications in 1997 is higher thanthe number for the same period in 1996, but the trend isconsistent with the higher incidence seen in spring andsummer in recent years (Figure 4). In 1997, the highestnumber of reports has been in the 0 - 4 years (104), 5 - 9years (37) and 25 - 29 years (25) age groups.
0
20
40
60
80
100
120
Jan1994
Jul Jan1995
Jul Jan1996
Jul Jan1997
Not
ifica
tions
Figure 4. Notifications of shigellosis, 1994 to 1997,by month of onset
1. The historical data are the averages of the number of notifications in 9 previous 2-week reportingperiods: the corresponding periods of the last 3 years and the periods immediately preceding andfollowing those.
0 100 200 300 400 500 600 700 800
Salmonellosis
Rubella
Q fever
Pertussis
Meningococcal infection
Measles
Legionellosis
Hepatitis A
Campylobacteriosis
Ross River virus infection
Historical Data
Reporting Period 2/04/97 to 15/04/97
Notifications
Figure 3. Selected National Notifiable Diseases Surveillance System reports, and historicaldata1
Disease2Total this
period
ReportingStates orTerritories
Totalnotifications
1997
Brucellosis 12Chancroid 1Cholera 1Hydatid infection 1 Tas 7Leprosy 2 Qld 6
1. Fewer than 60 cases of each of these diseases were notified each yearduring the period 1988 to 1996.
2. No notifications have been received during 1997 for the following rarediseases: botulism, lymphogranuloma venereum, plague, rabies, yellowfever, or other viral haemorrhagic fevers.
Table 3. Notifications of rare1 diseases received byState and Territory health authorities inthe period 2 to 15 April 1997
CDI Vol 21, No 91 May 1997

National Influenza Surveillance,1997Australian Sentinel Practice Research Network;Communicable Diseases Intelligence Virology andSerology Laboratory Reporting Scheme ContributingLaboratories, New South Wales Department of Health;Victorian Department of Health; World HealthOrganization Collaborating Centre for Influenza Referenceand Research.
Three types of data are included in National InfluenzaSurveillance, 1997. These include Sentinel GeneralPractitioner Surveillance, Laboratory Surveillance andAbsenteeism Surveillance. These are described below.
Sentinel General Practitioner Surveillance
Data will be included from four sources this season:ASPREN (the Australian Sentinel Practice ResearchNetwork); the Department of Health and CommunityServices, Victoria; the Department of Health, New SouthWales; and Tropical Influenza Surveillance of the
Department of Health and Community Services, NorthernTerritory.
The ASPREN consultation rate for influenza-like illnesshas remained below 5% so far for 1997, which is usual forthe time of year (Figure 5). However, Tropical InfluenzaSurveillance in the Northern Territory recorded a peak inthe consultation rate in mid-January, and after falling inearly February has risen again in recent weeks.
No data are available from Victoria and New South Walesthis fortnight.
Laboratory Surveillance
Laboratory surveillance data from the CommunicableDiseases Intelligence Virology and Serology LaboratoryReporting Scheme will be included in National InfluenzaSurveillance, 1997. The World Health OrganizationCollaborating Centre for Influenza Reference andResearch will also contribute information on strainsisolated.
This fortnight 9 reports of influenza A were received.Thirty-five reports have been received for the year to date,which is similar to previous years.
Nineteen reports of influenza B have been received thisfortnight, bringing the total number of reports for the yearto date to 70. This is the highest number recorded by thisscheme for the time of year (Figure 6). The male:femaleratio was 1.1:1 and 30% of reports were for children underthe age of 5 years.
Absenteeism Surveillance
National absenteeism data will continue to be supplied byAustralia Post and included in National InfluenzaSurveillance, 1997.
The national absenteesim rate has remained stablethroughout February and March at approximately 2.5%.
Australian Sentinel PracticeResearch NetworkThe Australian Sentinel Practice Research Network(ASPREN) comprises 99 sentinel general practitionersfrom throughout the country. Approximately 9,000consultations are recorded each week for 12 conditions.Of these, CDI reports the consultation rates forchickenpox, HIV testing (doctor initiated), HIV testing(patient initiated), influenza, measles, pertussis, RossRiver virus infection, rubella and gastroenteritis. Forfurther information including case definitions see CDI1997;21:6.
Data for weeks 14 and 15 ending 6 and 13 Aprilrespectively are included in this issue of CDI (Table 4).The consultation rate for gastroenteritis has continued todecline during the last 3 months. The rate for chickenpoxhas declined from the higher consultation rate reportedduring the summer, to a rate comparable with the 1996autumn period (Figure 7). Patient-initiated HIV testing hasshown a significantly reduced consultation rate over thelast 4 reporting weeks to little more than half the rateexperienced during the previous 10 weeks; consultation
0
5
10
15
20
25
30
35
Jan Feb Mar
Rat
e pe
r 1,
000
cons
ulta
tions
ASPRENNT
Apr May
Figure 5. Sentinel general practitioner influenzaconsultation rates, 1997, by week andscheme
0
20
40
60
80
100
120
140
160
180
Jan1993
May Sep Jan1994
May Sep Jan1995
May Sep Jan1996
May Sep Jan1997
Labo
rato
ry r
epor
ts
Figure 6. Influenza B laboratory reports, 1997, byweek
CDI Vol 21, No 91 May 1997

rates for doctor-initiated testing have not variedappreciably. Consultation rates for Ross River virusinfection have remained low during 1997. The numbers ofreported cases of measles, rubella and pertussis haveremained low.
Sentinel Chicken SurveillanceProgrammeAnnette Broom, Brenda Van Heuzen and Suzan Caulfield,Department of Microbiology, The University of WesternAustralia, QEII Medical Centre, Nedlands WesternAustralia 6009
There have been a number of seroconversions to MurrayValley encephalitis and Kunjin viruses in the sentinelchicken flocks in the north of Western Australia during the1997 wet season. A summary of the number of confirmedpositives recorded from the Kimberley and Pilbara flocksin March and early April 1997 is presented in Table 5.
There are still a number of possible seroconversions fromboth regions waiting to be confirmed. To date, there havebeen no cases of Australian encephalitis reported from theKimberley or Pilbara regions.
0
1
2
3
4
5
1 5 9 13 17 21 25 29 33 37 41 45 49 1 5 9 13
Reporting week
Rat
e pe
r 1,
000
cons
ulta
tions
Jan 1996 Jan 1997
Figure 7. ASPREN consultation rate for chickenpox,1996 to 1997, by week
Week 14, to 6 April 1997 Week 15, to 13 April 1997
Condition ReportsRate per 1,000
encounters ReportsRate per 1,000
encounters
Chickenpox 15 2.3 9 1.3
Gastroenteritis 71 10.9 64 9.3
HIV testing (doctor initiated) 6 0.9 8 1.2
HIV testing (patient initiated) 10 1.5 7 1.0
Influenza 26 4.0 27 3.9
Measles 0 0.0 0 0.0
Pertussis 1 0.2 2 0.3
Ross River virus infection 4 0.6 1 0.1
Rubella 1 0.2 0 0.0
Table 4. Australian Sentinel Practice Research Network reports, weeks 14 and 15, 1997
March April
MVE Kunjin MVE and Kunjin MVE Kunjin MVE and Kunjin Total
KimberleyKununurra 3 1 5 9Derby (town) 2 1 3Broome 2 1 3
PilbaraHarding Dam (Karratha) 6 1 7Tom Price 2 1 3Paraburdoo 1 1Ophthalmia (Newman) 1 1 1 2 1 6Whaleback Mine (Newman) 1 2 3
Table 5. Sentinel Chicken Surveillance Programme seroconversions, Western Australia, March and April1997
CDI Vol 21, No 91 May 1997

LabVISEThe Virology and Serology Laboratory Reporting Scheme,LabVISE, is a sentinel reporting scheme. Twenty-onelaboratories contribute data on the laboratory identificationof viruses and other organisms. Data are collated andpublished in Communicable Diseases Intelligence eachfortnight. These data should be interpreted with caution asthe number and type of reports received is subject to anumber of biases. For further information, see CDI1997;21:8-9.
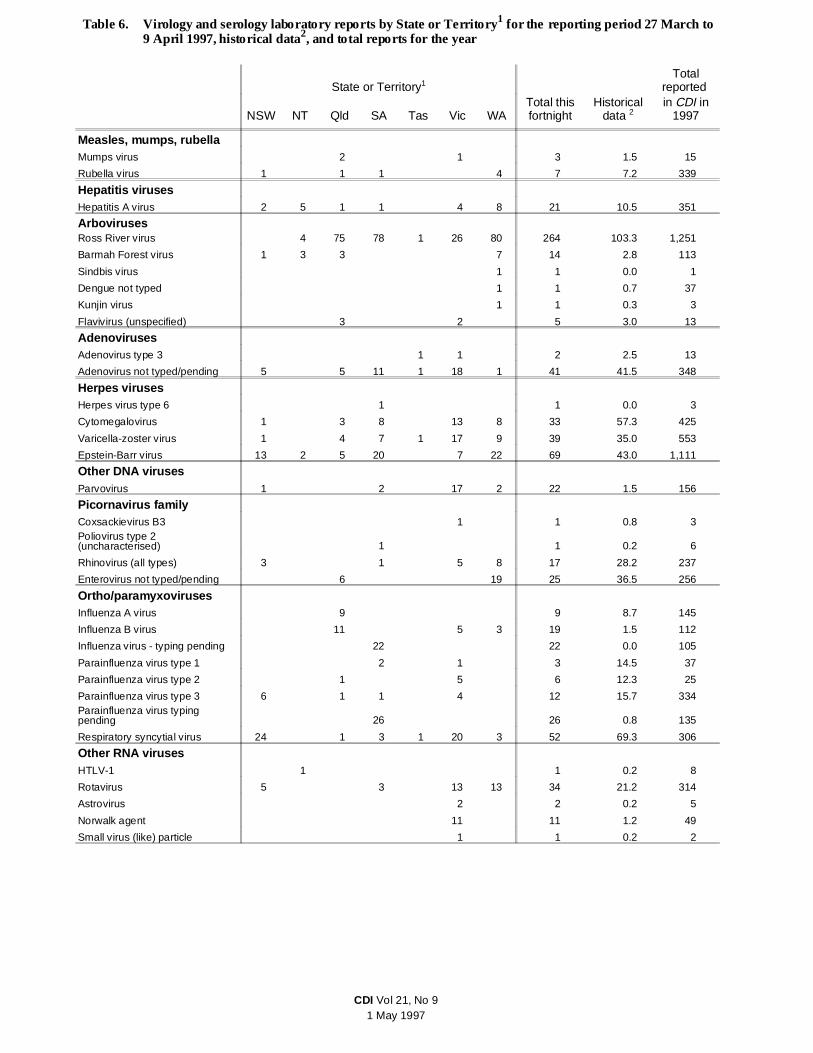
There were 1,058 reports received in the CDI Virology andSerology Laboratory Reporting Scheme this period(Tables 6 and 7). The largest number of reports (264) wasof Ross River virus infection. Diagnosis was by IgMdetection (249), four-fold rise in titre (14) and single hightitre (1). Reports of Ross River virus infection arecontinuing to increase as reported in CDI 1997;21:107-108.
Reports of respiratory syncytial virus infection are alsoincreasing as expected (Figure 8). There were 52 reportsreceived this fortnight, with diagnosis by antigen detection(28), virus isolation (22) and single high titre (1). Onereport did not indicate the method of diagnosis.
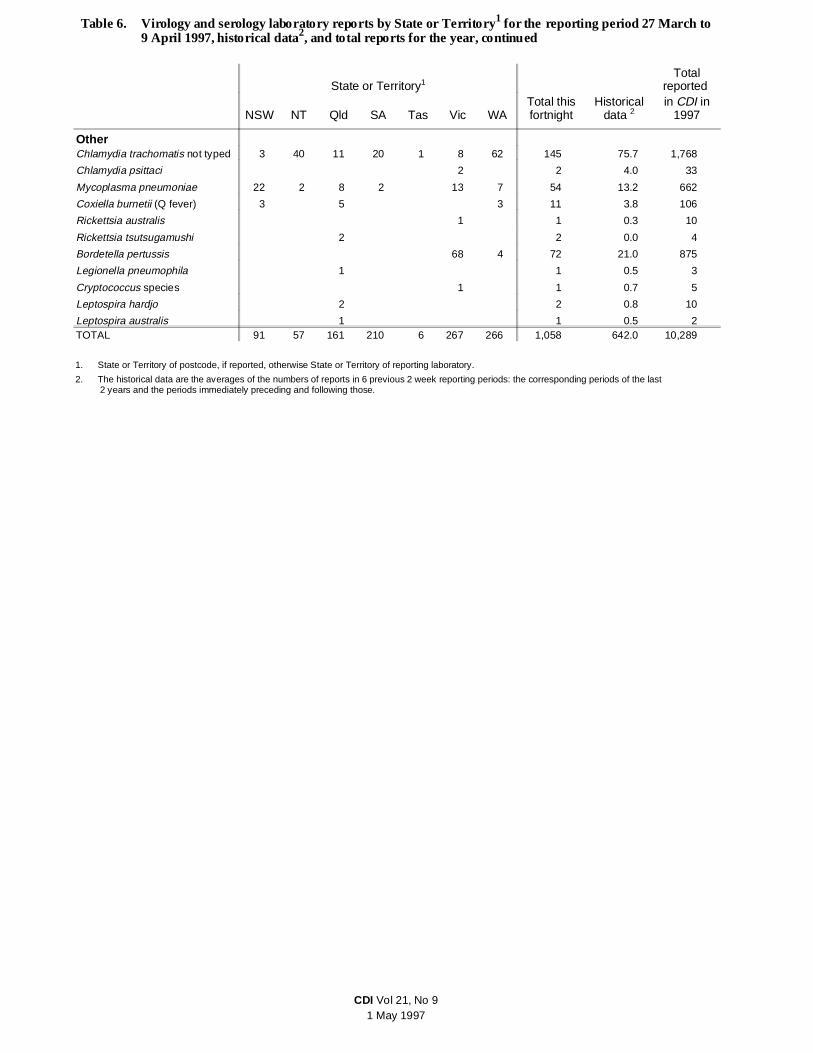
Laboratory reports of Mycoplasma pneumoniae arecontinuing to decline but are well above those received incorresponding periods over the last two years (Figure 9).There were 54 reports received in the last fortnight, withdiagnosis by IgM detection (35), single high titre (11), totalantibody (6) and four-fold rise in titre (2).
A similar pattern is evident in the number of laboratoryreports of parvovirus (Figure 10). Although the number ofreports of parvovirus is declining, the number reported forMarch is the highest recorded for that month in theprevious five years.
0
5
10
15
20
25
30
35
40
45
Jan1994
Apr Jul Oct Jan1995
Apr Jul Oct Jan1996
Apr Jul Oct Jan1997
Labo
rato
ry r
epor
ts
Figure 10. Parvovirus laboratory reports, 1994 to1997, by month of specimen collection
0
200
400
600
800
1000
1200
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Labo
rato
ry r
epor
ts
1995
1996
1997
Figure 8. Respiratory syncytial virus laboratoryreports, 1995 to 1997, by month ofspecimen collection
0
20
40
60
80
100
120
140
160
Jan1994
May Sep Jan1995
May Sep Jan1996
May Sep Jan1997
Labo
rato
ry r
epor
ts
Figure 9. Mycoplasma pneumoniae laboratoryreports, 1994 to 1997, by month ofspecimen collection
CDI Vol 21, No 91 May 1997
State or Territory1Total
reported
NSW NT Qld SA Tas Vic WATotal thisfortnight
Historicaldata 2
in CDI in1997
Measles, mumps, rubellaMumps virus 2 1 3 1.5 15
Rubella virus 1 1 1 4 7 7.2 339
Hepatitis virusesHepatitis A virus 2 5 1 1 4 8 21 10.5 351
ArbovirusesRoss River virus 4 75 78 1 26 80 264 103.3 1,251
Barmah Forest virus 1 3 3 7 14 2.8 113
Sindbis virus 1 1 0.0 1
Dengue not typed 1 1 0.7 37
Kunjin virus 1 1 0.3 3
Flavivirus (unspecified) 3 2 5 3.0 13
AdenovirusesAdenovirus type 3 1 1 2 2.5 13
Adenovirus not typed/pending 5 5 11 1 18 1 41 41.5 348
Herpes virusesHerpes virus type 6 1 1 0.0 3
Cytomegalovirus 1 3 8 13 8 33 57.3 425
Varicella-zoster virus 1 4 7 1 17 9 39 35.0 553
Epstein-Barr virus 13 2 5 20 7 22 69 43.0 1,111
Other DNA virusesParvovirus 1 2 17 2 22 1.5 156
Picornavirus familyCoxsackievirus B3 1 1 0.8 3Poliovirus type 2(uncharacterised) 1 1 0.2 6
Rhinovirus (all types) 3 1 5 8 17 28.2 237
Enterovirus not typed/pending 6 19 25 36.5 256
Ortho/paramyxovirusesInfluenza A virus 9 9 8.7 145
Influenza B virus 11 5 3 19 1.5 112
Influenza virus - typing pending 22 22 0.0 105
Parainfluenza virus type 1 2 1 3 14.5 37
Parainfluenza virus type 2 1 5 6 12.3 25
Parainfluenza virus type 3 6 1 1 4 12 15.7 334Parainfluenza virus typingpending 26 26 0.8 135
Respiratory syncytial virus 24 1 3 1 20 3 52 69.3 306
Other RNA virusesHTLV-1 1 1 0.2 8
Rotavirus 5 3 13 13 34 21.2 314
Astrovirus 2 2 0.2 5
Norwalk agent 11 11 1.2 49
Small virus (like) particle 1 1 0.2 2
Table 6. Virology and serology laboratory reports by State or Territory1 for the reporting period 27 March to9 April 1997, historical data2, and total reports for the year
CDI Vol 21, No 91 May 1997
State or Territory1Total
reported
NSW NT Qld SA Tas Vic WATotal thisfortnight
Historicaldata 2
in CDI in1997
OtherChlamydia trachomatis not typed 3 40 11 20 1 8 62 145 75.7 1,768
Chlamydia psittaci 2 2 4.0 33
Mycoplasma pneumoniae 22 2 8 2 13 7 54 13.2 662
Coxiella burnetii (Q fever) 3 5 3 11 3.8 106
Rickettsia australis 1 1 0.3 10
Rickettsia tsutsugamushi 2 2 0.0 4
Bordetella pertussis 68 4 72 21.0 875
Legionella pneumophila 1 1 0.5 3
Cryptococcus species 1 1 0.7 5
Leptospira hardjo 2 2 0.8 10
Leptospira australis 1 1 0.5 2TOTAL 91 57 161 210 6 267 266 1,058 642.0 10,289
Table 6. Virology and serology laboratory reports by State or Territory1 for the reporting period 27 March to9 April 1997, historical data2, and total reports for the year, continued
1. State or Territory of postcode, if reported, otherwise State or Territory of reporting laboratory.
2. The historical data are the averages of the numbers of reports in 6 previous 2 week reporting periods: the corresponding periods of the last 2 years and the periods immediately preceding and following those.
CDI Vol 21, No 91 May 1997

State or Territory Laboratory Reports
New South Wales Institute of Clinical Pathology & Medical Research, WestmeadThe New Children’s Hospital, WestmeadSouth West Area Pathology Service, Liverpool
402026
Queensland Queensland Medical Laboratory, West EndState Health Laboratory, Brisbane
34127
South Australia Institute of Medical and Veterinary Science, Adelaide 208
Tasmania Royal Hobart Hospital, Hobart 4
Victoria Microbiological Diagnostic Unit, University of MelbourneMonash Medical Centre, MelbourneRoyal Children’s Hospital, MelbourneVictorian Infectious Diseases Reference Laboratory, Fairfiel
820
133114
Western Australia PathCentre Virology, PerthPrincess Margaret Hospital, PerthWestern Diagnostic Pathology
17922
123
TOTAL 1,058
Table 7. Virology and serology laboratory reports by contributing laboratories for the reporting period 27March to 9 April 1997
CDI Vol 21, No 91 May 1997

Overseas briefsSource: World Health Organization (WHO)
CholeraSomalia . Outbreaks of acute diarrhoea and cholera havecontinued to occur in various parts of Somalia since late1996. Cholera has been confirmed and continues to bereported in Mogadishu and Merca and new outbreakshave been reported in Lower Shabelle region. The totalnumber of cholera cases (including suspect cases)reported since the first case on 30 November 1996 is1,535, with 47 deaths.
The number of cases in Mogadishu North has almosttripled in the last weeks following recent heavy rainfalls.Although the treatment centre there is coping well with theincreased cases, medical supplies are running short andWHO is trying to purchase these elsewhere. ECHO(European Community for Humanitarian Action) is alsoproviding support and sending supplies. A WHOconsultant who was in Mogadishu to study choleratransmission and assist in setting up a cholera committeewill now extend his stay to help deal with the increasingnumber of cases. However, in recently affected rural areascoordination of control activities is difficult.
Based on trends of cholera outbreaks in previous years, adecline in numbers is expected in the next six to eightweeks. The remote areas affected continue to be difficultto reach. Cholera task forces are meeting regularly toreview the situation.
Zaire. A confirmed cholera outbreak has been reported inKasese refugee camp near Kinsangani in Haut-ZaireProvince. A WHO team in Kinsangani together with teamsfrom Médecins sans Frontières and UNICEF are currentlyassisting in the implementation of control measures forthis outbreak.
Since the beginning of 1997 suspected cholera outbreakshave been reported in several regions of Zaire, particularlyKinshasa and Equateur Provinces. Cholera treatment kitshave been sent to Kinshasa and a WHO consultant isvisiting the area affected.
Acting Editor: Ana Herceg
Deputy Editor: Graham Andrews
Assistant Edi tor: Margaret Curran
Editorial Advisory Board
Charles Watson (Chair), Margaret Burgess, Scott Cameron,Jeffrey Hanna, John Kaldor, Margery Kennett, Cathy Mead,Christine Roberts
Editorial and Production Staff
Ross Andrews, Scott Crerar, David Evans, Kim Moser, HtooMyint, Graeme Oliver, Irmgard Wilkins, Corina Yong
Contributions covering any aspects of communicable disease areinvited. Instructions to authors can be found in CDI 1997;21:9.
CDI is produced fortnightly by the National Centre for DiseaseControl, Department of Health and Family Services, GPO Box9848 Canberra ACT 2601; fax: (06) 289 7791, telephone: (06)289 1555. For subscriptions or change of address please fax (06)269 1212 or write to PO Box 462, Fyshwick ACT 2609.
Opinions expressed in CDI are those of the authors and notnecessarily those of the Department of Health and FamilyServices or the Communicable Diseases Network Australia NewZealand. Data may be subject to revision.
CDI is available on the CDI Bulletin Board System on (06) 2816695, and via Internet on ’ftp://ftp.health.gov.au’ in directory/pub/CDI and on ’http://www.health.gov.au’ in/hfs/pubs/cdi/cdihtml.htm.
Consent for copying in all or part can be obtained from theManager, Commonwealth Information Services, AustralianGovernment Publishing Service, GPO Box 84 Canberra ACT2601.
Related Documents











